

Abstract
Aim:
To systematically review the reported techniques, for evaluating the risk and difficulty encountered in the management of fractured abutment screw in accordance with the location of fracture, and to develop a logical sequence in managing an implant abutment screw fracture.
Settings and Design:
Systematic review following PRISMA guidelines.
Materials and Methods:
A systematic search of the PubMed/MEDLINE database for articles published between January 2000 and March 2020 was performed by 2 independent reviewers. Case reports and case series that described the management of fractured implant abutment screw were included. Published articles were qualitatively analyzed employing CARE guidelines and were classified according to the location of screw fracture with respect to implant platform, risk of damage to the implant, and intervention for managing the fractured screw.
Statistical Analysis Used:
Qualitative analyisis.
Results:
A total of 28 articles were included in the review. Two of them explained the management of screw fracture at or above the implant platform and required only mild approach with low risk while the others explained the management of screw fracture below the level of implant platform. Among them, 6 were considered mild approach with low risk, 13 moderate approach with moderate risk, and 8 of them severe approach with high risk.
Conclusion:
Irrespective of the technique, any attempt to retrieve abutment screw fragment poses some risk to the implant which is varying from mild to severe. As the location of fracture is more gingival to the implant platform, difficulty of retrieval as well as risk to the implant increases. The proposed decisionmaking tree will be a useful tool in helping clinicians to manage abutment screw fracture.
Keywords: Complication, implant, management, screw fracture
INTRODUCTION
Implantology has emerged as the most successful treatment modality for the replacement of missing teeth. This wide popularity enjoyed is mostly due to the fact that it eliminates the need for preparation of the adjacent teeth. On long-term functioning, success of an implant-retained or implant-supported prosthesis depends primarily on biological and mechanical factors.[1] The implant failure can be classified into early or late failures. Early failures occur immediately after implant placement and result in a lack of osseointegration whereas late failures occur after prosthetic rehabilitation and a period of function. Biological and mechanical complications are the two main causes of late implant failures. Biological complication is due to the loss of supporting tissues, secondary to infection or periimplantitis whereas mechanical complications arise as a result of loosening/or fracture of abutment or prosthetic screws and the wear and fracture of the prosthesis or various components in the system.[1,2] A recent study has shown that abutment screw loosening ranges between 7% and 11%, while the incidence of abutment screw fracture was found to be 0.6%.[3] Abutment screw loosening and fracture are one of the most serious and prevalent problems associated with the restorative aspect of dental implants. Inadequate biomechanical design and/or occlusal overloading are found to be the major contributing factors for screw loosening which eventually leads to fracture.[4] The management of fractured abutment screw is challenging and time-consuming and also poses various degrees of risk to implant and prosthesis, which must be analyzed.[5] When an abutment screw fractures, the aim of management is removal of the fragment without causing damage to internal threads of the implant and replacing the fractured one with a new one. Sometimes, it may not be possible and may require implant modifications to receive prosthesis. In such situations, some techniques cause irreversible damage to the implant components. The possible risk should be assessed before planning an intervention to salvage the implant and this intervention should always improve the prognosis. Different techniques are reported to manage abutment screw fracture, but literature that describes a structured approach for clinical management of abutment screw fracture is still limited. The purpose of this article is to review the various retrieval techniques and to extract a methodical approach in managing fractured abutment screw.
MATERIALS AND METHODS
Protocol and registration
This systematic review was performed and reported according to the guidelines prescribed by the preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines (Moher et al. 2010).
Target question
How will you methodically approach and manage an abutment screw fracture with minimal damage to the implant?
Review question
The following PICO question was used to frame search strategy:
Population: Patients with fractured implant abutment screw
Intervention: Retrieval of the fractured abutment screw without impairing the implant survival
Comparison: Risk of damage to implants with different techniques employed for retrieving fractured abutment screw in accordance with location of fracture.
Primary outcomes
To evaluate the risk and difficulty encountered in the management of fractured abutment screw in accordance with the location of fracture, i.e., at, above, or below the implant platform.
Secondary outcomes
To develop a logical sequence in managing implant abutment screw fracture.
Information sources
All studies reporting on the management of perishing implants with abutment screw fracture were searched in online electronic databases (PubMed and Google Scholar). Relevant publications which were not accessible online were hand searched. Other sources such as online search engines (Google, Yahoo, etc.), online research community websites (https://www.researchgate.net/), and reference cross-checks were all assessed for generating a maximum pool of relevant studies.
Eligibility criteria
Inclusion criteria
Case reports and case series explaining clinical management of fractured abutment screw of single or multiple unit implant-supported prosthesis with follow-up time up to 6 years
Techniques for salvaging implants with abutment screw fracture
Restoration type ranging from implant-supported fixed dental prosthesis to implant-retained complete denture.
Exclusion criteria
Case reports of implant-abutment connections other than internal hexagon or external hexagon
Case reports which failed to attain successful rehabilitation of implants with abutment screw fracture
Techniques involving management of fracture of implant components other than abutment screw
Review articles
Irrelevant articles.
Search strategy
The two investigators performed the searches based on the identified medical subject headings (MeSH) search terms “abutment screw,” “fractured,” “broken,” “damaged,” “unsalvageable,” “screw retrieval,” “screw complication,” “implant,” and “dental implant “ as dictated by the search design and strategy. The terms were then applied using the appropriate Boolean operators, “OR” or “AND,” to perform the search in the databases and the filters set ((Language – English, Species – Human, Journal categories – Dental journals) while performing the searches in the above-mentioned databases. The search was performed from January 2000 to March 2020.
Data extraction and analysis
The investigators initially assessed the search results by a thorough title and abstract screening. After the initial assessment, the shortlisted studies were included for a full-text analysis only after a mutual agreement between the two investigators. Disagreements, if present, were resolved by a consensus meeting with the third investigator. The final list was mutually agreed upon by the two investigators before data extraction. Data extraction was performed independently by both investigators and was reciprocally blinded. The investigators used Microsoft Excel spreadsheets for tabulating the extracted information. The following parameters were extracted from the included studies: authors' names, year of publication, study design, location in the arch, abutment material/type, restoration material, location of fractured abutment screw at, above, or below the platform of the implant, technique, and different retrieval methodologies. The outcome was not evaluated according to the prosthetic rehabilitation.
Risk of bias and quality assessment of the included studies
Risk of bias was assessed in the included case reports and case series using ROBIS (Risk Of Bias In Systematic reviews) tool for systematic reviews.[6] The case reports and case series were assessed using the recommended checklist for report writing following CARE guidelines. The reports were analyzed based on the 13 item checklist, and subsequently, a score was assigned to the report. Thus, each report was assessed out of the total score of 13.
Summary measures
The primary outcome set for this review was to evaluate the risk and difficulty encountered in accordance with the location of fractured abutment screw at, above, or below the platform of the implant. Secondary outcome measures targeted in developing a logical sequence and technique for managing an implant abutment screw fracture.
RESULTS
Study selection and characteristics
The details of the search and selection processes are described in the PRISMA flow diagram [Figure 1]. The systematic database search yielded a total of 642 eligible studies. From this total, 535 studies were eliminated after an initial title and abstract screening, thus identifying a total of 107 studies for full-text analysis; 55 studies were shortlisted for inclusion in the review. After reference cross-checks and hand searches, 35 studies were shortlisted for a final evaluation. A reapplication of the inclusion and exclusion criteria was performed to this final list resulting in a further elimination of 7 studies. Finally, a total of 28 methodologically sound publications were included in this review for statistical analyses. The list of studies included for analyses comprised of 27 case reports and 1 case series. Tables 1 and 2 show the characteristics of the included studies.
Figure 1.
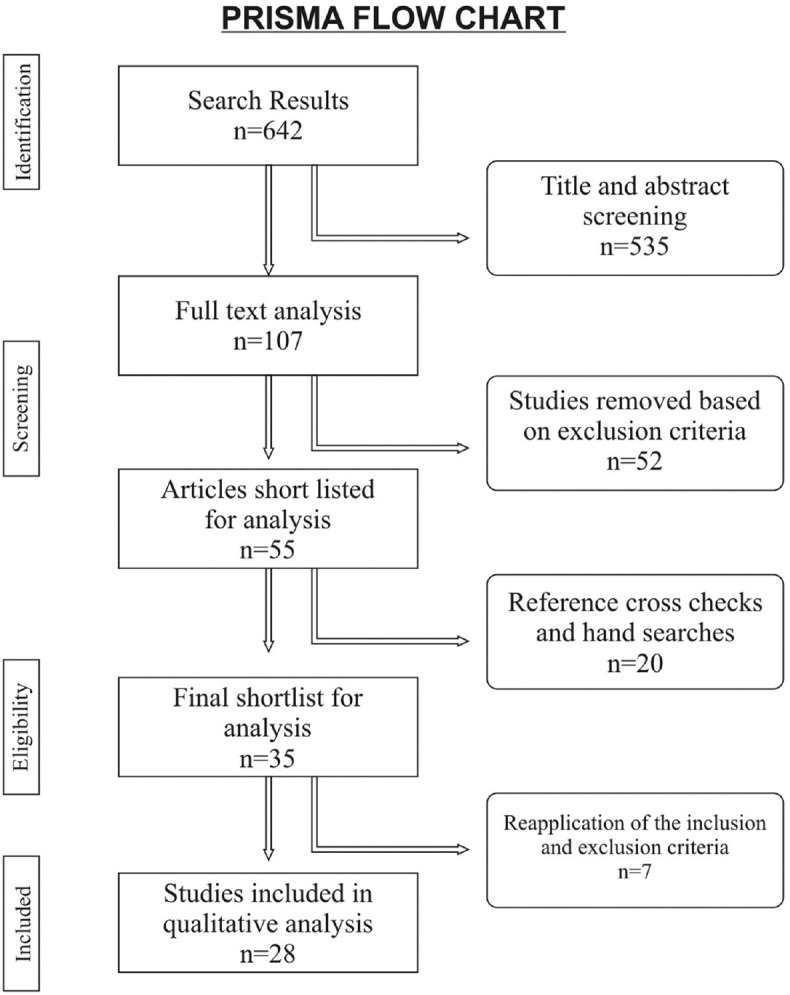
PRISMA flow chart
Table 1.
Screw retrieval techniques for fracture at or above the platform of the implant
| Mild approach with low risk | |||||
|---|---|---|---|---|---|
| Author and year | Study design and title | Location in arch | Abutment material/type | Restoration material | Technique andretrieval methodology |
| Barbosa et al., 2014[7] | DescriptiveThe cotton driver: An alternative technique for removing fractured screw fragments | Not available | Titanium abutment | Not available | Modified cotton swabPressing the cotton swab into the implant head and twist the fractured abutment screw slowly counter clockwise |
| Yang and Wu 2019[8] | DescriptiveA technique to retrieve a fractured implant abutment screw by using a screwdriver fashioned from a needle | Not available | Prefabricated Titanium abutment | Not available | Modified hypodermic needleAppropriate sized needle is bending to form screwdriver. After engaging the fractured end, turned counter clockwise for removal |
Table 2.
Screw retrieval techniques for fracture below the platform of the implant
| Author and year | Study design and title | Location in arch | Abutment type/material | Restoration material | Technique and retrieval methodology |
|---|---|---|---|---|---|
| Mild approach with low risk | |||||
| Fauvell et al., 2006[9] | DescriptiveThe lumen technique. Retrieval of broken goldscrews in dental implants | Not available | Not available | Not available | Instrument modificationAn applicator tip was seated with apical pressure in implant fixture, wedged it between implant and screw surface and then counterturned to retrieve the retention screw |
| Satterthwaite and Rickman, 2008[10] | DescriptiveRetrieval of a fractured abutment screw thread from an implant: a case report | Anterior maxillaMaxillary central incisor | Esthetic abutment | Not available | Visualization and basic instrumentationVisualized through a clinical microscope and fragment was removed using endodontic instruments |
| Bhandari et al., 2013[11] | DescriptiveUltrasonic oscillations for conservative retrieval of a rare fracture of implant healing abutment | Posterior mandibleMandibular first and second molars | Healing abutment | Porcelain fused to metal | OscillationsPiezoelectric ultrasonic scaler tip in a gentle reverse torque was employed for abutment screw retrieval |
| Chen and Cho, 2018[12] | DescriptiveAn accessory technique for the intraoral removal of a fractured implant abutment screw | Posterior maxillaMaxillary second Premolar | Not available | Porcelain fused to metal | Ultrasonic oscillationPerformed with a combination of ultrasonic device and a dental restoration holder |
| Azpiazu-Flores and Lee, 202013] | DescriptiveUsing the screw shank as a retrieval tool: A straightforward approach to removing screws with diagonal fractures | Anterior mandibleMandibular central incisors | Not available | Not available | Basic instrumentation with screw shankAfter engaging the shank mounted in hexagon driver with fractured screw it is rotated counter clockwise. |
| Moderate approach with moderate risk | |||||
| Luterbacher et al., 2000[14] | DescriptiveFractured prosthetic abutments in osseointegrated implants: A technical complication to cope with | Anterior mandibleMandibular anterior teeth | Prefabricated Titanium abutment | Porcelain fused to metal | Screw modificationRepair set of the ITI Dental Implant System is used to retrieve the fragment. The service set consists of burs, tap sets of three instruments, drill guides etc. |
| Williamson and Robinson, 2001[15] | DescriptiveRetrieval technique for fractured implant screws | Not available | Not available | Not available | Screw modificationA groove was made on the surface of the screw with ¼ round bur and number 1 round bur is modified to be used as a screwdriver |
| Nergiz et al., 2004[16] | DescriptiveRemoval of a fractured implant abutment screw: A clinical report | Anterior mandibleMandibular canines | Magnetic implant abutment | Magnet retained acrylic overdenture | Screw modificationAbutment screw was retrieved using repair kit (IMZ Twin Plus Repair Set). First, fragment was perforated and achieved retention to unscrew it |
| Reyhanian et al., 2010[17] | DescriptiveThe use of the Er: YAG in laser-assisted broken abutment screw treatment | Anterior maxillaMaxillary central incisor | Prefabricated Titanium abutment | Not available | Laser and screw modificationLaser is used for exposing implant platform, ablate granulation tissue and for decontamination. Screw is retrieved after modifying with surgical drill |
| Yilmaz and McGlumphy, 2011[18] | DescriptiveA technique to retrieve fractured implant screw | Not available | Not available | Not available | Screw modificationStainless steel fork shaped instrument is used in slow-speed hand piece for screw retrieval |
| Walia et al., 2012[19] | DescriptiveRemoval of fractured dental implant screw using a new technique: A case report | Posterior mandibleMandibular first molar | Prefabricated Titanium abutment | Not available | Screw modification and oscillationsNotch made on the fragment and ultrasonic scaler tip is moved in counter clockwise direction to retrieve implant abutment screw |
| Yohsuke and Sawase, 2012[20] | DescriptiveA modified technique for removing a failed abutment screw from an implant with a custom guide tube | Anterior maxillaMaxillary central incisors | Angled abutment | Metal with resin veneering | Screw modification through a custom made guide tubeFailed abutment screw is modified with a high speed air-turbine and the tungsten carbide bur was insertedthrough the guide tube |
| Kurt et al., 2013[21] | DescriptiveA Technique for Removal of a Fractured ImplantAbutment Screw | Anterior mandibleMandibular canine | Ball attachment | Implant-supported acrylic overdenture | Screw modification with modified bursGroove on the fractured screw with modified flame shaped bur and a handmade screw driver with tungsten carbide bur |
| Satwalekar et al., 2013[22] | DescriptiveA simple and cost-effective method used for removal of a fractured implant abutment screw: A case report | Posterior mandibleMandibular first Premolar | Titanium abutment | Not available | Screw modification and custom made screw driverA groove was made on the upper end of the broken screw using an airotor and a modified spoon excavator was used as screw driver |
| Gooty et al., 2014[23] | DescriptiveNoninvasive method for retrieval of broken dental implant abutment screw | Posterior mandibleMandibular first molar | Prefabricated titanium abutment | Not available | Screw modification and oscillationsDeep pit made on the fragment and an ultrasonic tip was engaged in counter clockwise direction |
| Carneiro et al., 2016[24] | DescriptiveA conservative approach to retrieve a fractured abutment screw – A case report | Posterior mandible | Abutment screw with diamond-likecarbon DLCcoating | Not available | Screw modification through titanium guide sleeveTitanium guide sleeve guided-drilling of the fractured screw and re-tapping the implant internal threads with a retapping tool |
| Yoon et al., 2016[25] | DescriptiveSafe removal of a broken abutment screw with customized drill guide and rotary instrument: A Clinical Report | Posterior mandibleMandibular second molar | Prefabricated Titanium abutment | Porcelain fused to metal | Screw modification through a custom made guide tubeAn access hole on top of the broken screw made through a customized drill guide which was fabricated from an implant impression coping |
| Flanagan, 2016[26] | DescriptiveManagement of a fractured implant abutment screw | Posterior maxilla (Maxillary first premolar)Posterior maxillaAnterior mandible (Mandibular canine) | Prefabricated titanium abutments | Not availableAcrylic maxillary overdentureAcrylic mandibular overdenture | Screw modificationFragment removal is accomplished with festooned #557 bur in counter clockwise rotation and #33 1/3 bur in clockwise rotation |
| Severe approach with high risk | |||||
| Pipko et al., 2004[27] | DescriptiveRetrofitting a cast dowel-core on salvaged dental implant | Anterior mandibleMandibular central incisor | Titanium abutment | Not available | Implant modificationRemoval is accomplishedby using number 2 and number 4 friction grip carbide bur and an accurate cast dowel core is retrofitted into the implant |
| Pow and Wat, 2006[28] | DescriptiveA technique for salvaging an implant-supported crown with a fractured abutment screw | Posterior mandibleMandibular first molar | Not available | Not available | Implant modificationFractured end is removed and elimination of the internal threads were done with rotary cutting instrument followed by postcore crown |
| Maalhagh-fard and Jacobs, 2010[29] | DescriptiveRetrieval of a stripped abutment screw: A clinical report | Anterior maxillaMaxillary central incisor | Titanium abutments | Not available | Implant and screw modificationA trough is made betweenabutment head and internal aspect of implant to facilitate abutment screw accessibility and retrieval is accomplished using fine forceps |
| Yilmaz and McGlumphy, 2013[30] | DescriptiveA technique to salvage a single implant-supported fixed dental prosthesis having a nonretrievable implant screw fragment | Not available | Prefabricated titanium abutment | Not available | Implant modificationA flat stainless steel washer with a new implant screw was employed to rehabilitate the implant |
| Canpolat et al., 2014[31] | DescriptiveManagement of a Fractured Implant Abutment Screw: A Clinical Report | Anterior mandibleMandibular canine | Ball attachment | Implant-supported acrylic mandibular overdenture | Implant modificationInterior of the implant and the fractured screw were machined with high speed hand piece and a custom made cast dowel with ball attachment for rehabilitation |
| Gupta et al., 2014[32] | DescriptiveA new restorative technique for the perishing implantdue to abutment screw fracture | Posterior mandibleMandibular first molar | Prefabricated titanium abutment | Not available | Implant modificationFractured screw was removed with high speed hand piece and a custom made cast post is fabricated |
| Harshakumar et al., 2014[33] | DescriptiveSalvaging an implant with abutment screw fracture by a custom titanium post and core supported prosthesis - A novel technique | Anterior maxillaMaxillary central incisor | Prefabricated titanium abutment | Not available | Implant modificationInternal threads and the fractured screw were removed using tungsten carbide bur and titanium cast post for rehabilitation |
| Shah and Lee, 2016[34] | DescriptiveAn alternative approach for the management of fractured implant abutment screws on a mandibular implant - retained overdenture: A clinical report | Anterior mandibleMandibular canine | Locator abutments | Implant-supported acrylic mandibular overdenture | Implant modification and laser weldingScrew chamber converted into a dowel space for a dowel-core and locator bar attachments were laser welded into the cast custom made abutments |
Risk of bias/quality assessment of the included studies
Risk of bias assessment was done using ROBIS tool for studies included in the systematic review. The tool is completed in 3 phases: (1) assess relevance (optional), (2) identify concerns with the review process, and (3) judge risk of bias in the review. Signaling questions were included to help assess specific concerns about potential biases within the review. The ratings from these signaling questions helped assessors to judge overall risk of bias. All signaling questions were rated as “Yes” or “Probably Yes,” and hence, a low risk of bias was identified. The review processes of data collection and study appraisal are therefore unlikely to have introduced bias into this review [Figure 2]. Although the case reports, case series, and reported techniques included in this systematic review compared different retrieval methodologies in mild, moderate, or severe risk cases of implant abutment screw fracture, a meta-analysis could not be performed due to the heterogeneity of the data between the included studies. The 28 methodologically sound publications were qualitatively assessed using CARE guidelines, and the mean quality score of the papers was 11.29 ± 0.71.
Figure 2.
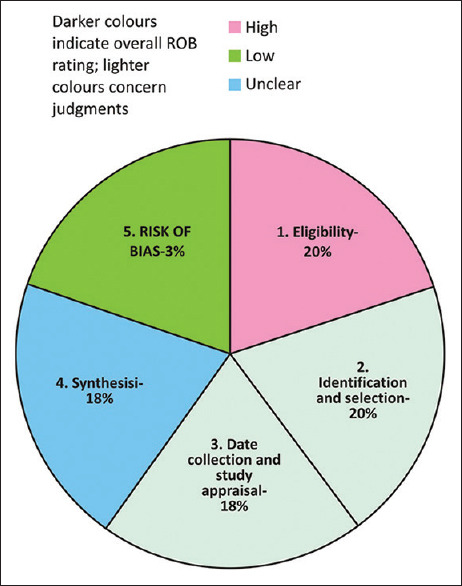
Graphical representation of ROBIS from multiple reviews
Statistical analysis
The overall Kappa scores calculated using the GraphPad Prism software (Version 11, San Diego, California, USA) from extracted data by the two investigators were found to be 0.78 indicating an substantiate degree of inter-investigator agreement.
Dicussion
The first step in managing any fractured screw is to obtain a detailed history and perform a thorough clinical examination. Every attempt should be made to determine the cause of the screw fracture to minimize the risk of subsequent complications. In most of the cases, abutment screw loosening preceded the fracture of the same. The etiology is multifactorial and can range from inadequate treatment plan and design, component misfit, inadequate screw tightening, excessive loading, and/or inadequate screw design.[35] Inadequate treatment design and planning can attributed to patient assessment and insufficient number and location of implants. Patient parameters such as age and sex can have an influence on the prevalence of screw loosening and fracture. The included case reports and case series showed sex predilection for males and age wise for the elderly (50–65 years) and were in accordance with the previous study conducted by Lee et al.[36] Literature shows that the incidence of screw fracture is more frequent in posterior region compared to anterior.[3] In the present study involving case reports and case series, incidence of abutment screw fracture in the anterior region was more prevalent than the posterior region. This may be due to esthetic concern and frequency in seeking treatment in the case of anteriors. Usually, in terms of retention, a higher incidence of screw loosening has been observed in screw-retained implant prostheses than cement-retained implant prostheses. Single crowns are more prone to screw loosening followed by cantilever bridges, splinted crowns, and implant-retained overdenture.[36]
The types of abutments included in this study were prefabricated metallic ones which comprise straight abutments, angled abutments, ball with locator abutment, multiunit abutment, and anatomic/esthetic abutment. The restorative materials metal-ceramic and zirconia-based all ceramic were included in the study.
After assessing the reason for fracture, the next step is to confirm that the screw is fractured and to determine the location of the fracture. Fractures mostly occur at the junction of the screw head and screw shank or at the junction of the screw shank and screw thread.[20,37] Screw fracture may be confirmed by direct visualization, radiographic examination, tactile sensation through the use of an instrument, comparison with an undamaged screw of the same system, or by using other undamaged components of the same system to see if an obstruction is prohibiting complete seating. If the restoration has been missing for an extended period, the periimplant soft tissue may overgrow, making access to and visualization of the implant difficult. In this situation, a low-frequency diode laser is ideal to trim the tissue, since the scratching of the implant surface with surgical blade or scalpel has to be avoided. The use of an electrosurgery unit should be avoided to expose the implant platform since it causes heat transfer within the implant. Other techniques that may help to improve visualization include the use of dental loupes with a coaxial or light-emitting diode headlamp or a dental surgical microscope, especially in situations with deep screw fracture.[21,38]
Management of abutment screw fracture is challenging since the preloading and occlusal loading could wedge the fractured abutment into the implant and require high pull-out force. Saliva, blood, and the limited visibility make it difficult to access.[39] In this situation, initial treatment in the form of conservative retrieval is always the first and most preferable option. Sometimes, it may not prove successful, then we have to consider other options. The uncertainty in decision on type of treatment and sequence of treatment make it more arduous. Therefore, the formation of a decision tree can be useful in managing situations that range from routine to highly complex. This review highlights the need of a decision-making tree on the basis of risk and difficulty involved, in relation to the various reported techniques for managing fractured screws.[40] Application of the proposed decision-making tree may allow for a logical and structured approach in managing fractured abutment screws [Figure 3]. According to the proposed decision-making tree, methods employed to grasp the broken fragments or screw are determined by the location of the fracture abutment – above or below the head of the implant.
Figure 3.
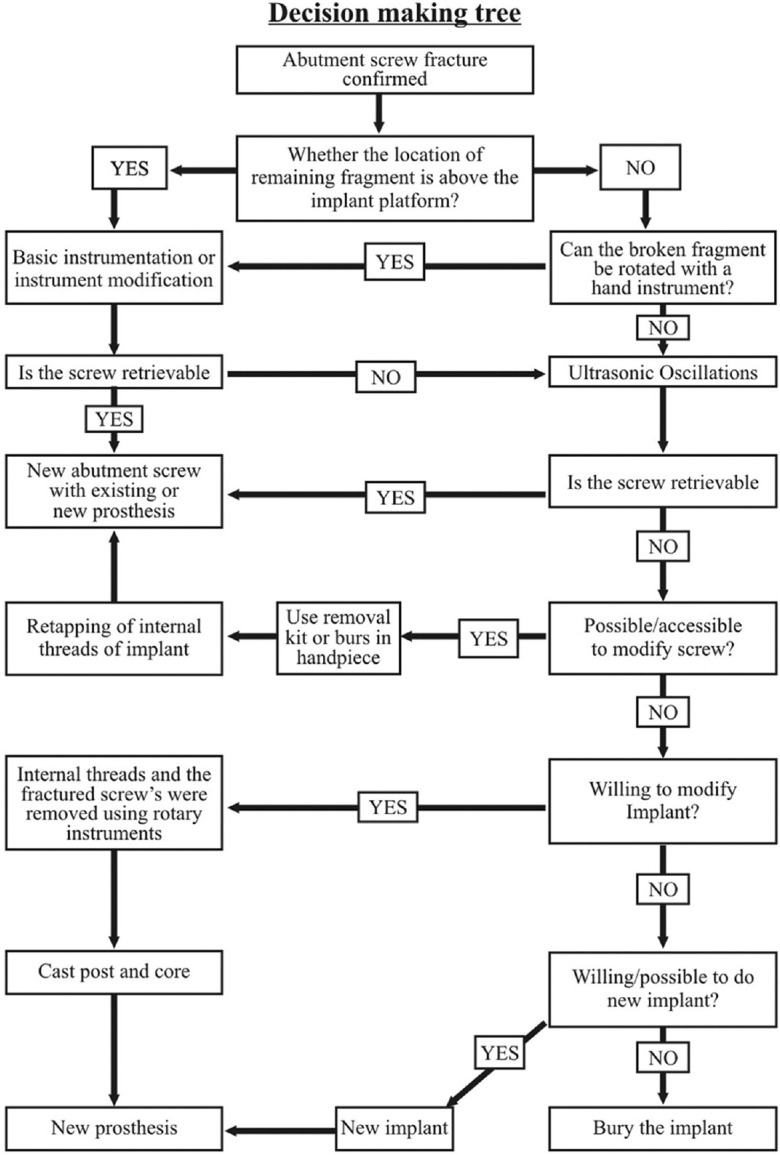
Decision making tree
If an abutment screw fractures above the head of the implant, an explorer, a straight probe, or hemostat might be successful.[7,8] The tip of the instrument is moved carefully in a counter-clockwise direction over the surface of the screw segment until it loosens. In the case of abutment screw fracture below the implant platform as well, the first choice of intervention is use of rigid instruments such as a scaler, sickle explorer, or endodontic explorer in the same fashion.[9,10,13] Care must be taken to avoid instrument tip breakage. Sometimes, even if the screw gets loosened, it may be difficult to remove it completely out of the fixture, then the use of a cotton swab might be helpful to pull out the fragment.[7] Oblique fractures may be easier to manage with this technique because a purchase point usually exists in which the instrument can be engaged. Ultrasonic oscillation assisted by hand instruments is an accessory method to remove a fractured abutment screw fragment which is not possible with hand instruments alone.[11,12] Thin scaler tips in counter-clockwise oscillation may be helpful to back out the fragment, but care should be taken to avoid wedging of the screw into the implant. These are mild approaches which pose only low risk since it will not damage internal threads of the implant and will not increase temperature which affects bone around it.
If the fractured abutment screw fragment is not possible to remove with hand instruments or combination of ultrasonic oscillation and hand instruments, other options must be considered. Burs or drills mounted on a handpiece in counter-clockwise rotation may unwind the fragment. Sometimes, access points or grooves are created on the occlusal aspect of fragment for the mechanical interlocking of scaler tip or customized screwdrivers made from burs or instruments.[15,16,17,18,21,22,26] Furthermore, burs or drills may be modified to avoid damage to internal threads of the implant and better engagement. Screw modification with rotary instruments drilling should be performed intermittently at a reduced speed and under copious irrigation to avoid thermal damage to the surrounding bone. Fabrication of custom-made drill guides employing a high-speed air turbine or a high-speed micro-motor handpiece ensures protection of the internal threads against drilling.[20,25] There are several available implant repair kits including ITI® Dental Implant System (Institut Straumann AG, Switzerland), IMZ® TwinPlus Implant System1 (DENTSPLY Friadent, Germany), Screw Removal Kit Replace (Nobel Biocare™, Yorba Linda, California, USA), and Certain® Screw Removal Kit (Biomet 3i™, Florida, USA31). The application of these systems is to permit a hole to be drilled into the center of the broken screw and drive a removal wedge into the hole that engages the broken screw when reverse torque is applied by removing the instrument.[14]
If all the attempts of mild and moderate approach have failed and the internal aspect is significantly damaged, the clinician may choose either to remove the implant and replace it with a new one or abandon the implant and cover it with soft tissue. Many patients may not prefer replacement with new implant since it is an expensive option and require surgical procedures. Abandoning the implant and covering it with soft tissue may lead to compromised function, phonation, or esthetics. Intentional modification of the implant may be necessary to keep the implant serviceable. In cases where irretrievable screw fragment is drilled out, attempts can be made to retap the internal threads to salvage the implant.
If implant's screw threads have been damaged irreversibly and the patient is still unwilling to sacrifice the implant, it is possible to fabricate a custom cast post and core for the implant.[27,28,29,30,31,32,33,34] These techniques generally start with the removal of remaining screw fragment, followed by removal of the internal threads of the implant by using a diamond rotary instrument or tungsten carbide bur in a high-speed handpiece under copious irrigation. Pattern for casting can either be made directly on the prepared implant or indirectly on a stone cast. The pattern is then cast using nickel-or cobalt-chromium alloys, although other types of metal alloys have also been reported. Once the seating of the custom cast post and core has been confirmed, it can be cemented. The appropriate restoration can then be fabricated following conventional prosthodontic protocols. This technique has a few disadvantages such as weakening of the implant body and excessive heat production during cutting of the fractured screw; hence, it is last choice of management.
Prevention is better than cure, and the correct measures should be taken to ensure that screw fracture does not happen. Abutment screw loosening preceded the fracture of the same. For prevention of screw loosening and fracture, clinician should know mechanics of abutment screw. A screw is tightened by applying a torque and it develops a force within the screw called the preload. Elastic recovery of the screw pulls the two parts together, creating a clamping force. The preload in the screw, from elongation and elastic recovery, is equal in magnitude to the clamping force.[41] Preload depends on the torque applied, material, and design of the screw, and surface roughness.[42] Joint separating forces and settling effect cause loosening of initially tightened screw by making loss of preload. Intraoral separating forces include off-axis occlusal contacts, parafunctional forces, and nonpassive frameworks that attach to the implants. Once external forces exceed the screw joint preload, the joint becomes unstable whereas settling occurs as the rough spots flatten under load, since they are the only contacting surfaces when the initial tightening torque is applied. It has been reported that 2% to 10% of the initial preload is lost as a result of settling.[41] It is recommended in clinical practice that to reduce the settling effect, abutment screws should be retightened 10 min after the initial torque application.[42,43] Mechanical torque gauges should be used instead of hand drivers to ensure a consistent tightening of the implant components to recommended torque values.[41] Joint separating or bending forces can be minimized by placing the implants perpendicular to the occlusal plane and frameworks with minimal cantilever lengths. Furthermore, the use of implant components with anti-rotational features and low tolerance levels for component misfit will help in reducing the abutment screw loosening and further complications.[44]
The limitations of the present study include (a) the study was not able to review all the relevant literature, (b) the study attempted to identify those publications relevant for our purpose, (c) publication bias, and (d) over interpretation of case series and case reports dealt with could be a limiting factor.
CONCLUSION
Within the limitations of the study, the following conclusions were drawn:
Irrespective of the technique, any attempt to retrieve abutment screw fragment poses a certain risk to the implant which varies from mild to severe. Twenty-five percent of the case reports used a mild approach that involved the use of hand instruments or combination of hand instruments and ultrasonic oscillation. This technique produces only minimal damage to the implant such as abrading of the implant surface. Forty-five percent of the case reports used a moderate approach that involved the use of retrieval kits and modified burs. This technique produces damage to internal threads of the implant. Remaining case reports used high-risk approach that involved the modification of implant itself. This technique may lead to implant body weakening and damage to surrounding bone
As the location of fracture is more gingival to the implant platform, difficulty of retrieval as well as risk to the implant increases. Irrespective of the location, more conservative approach should be attempted first, before considering invasive procedures
The proposed decision-making tree will be a useful tool in guiding the clinicians for the management of abutment screw fracture and successful rehabilitation of the implant
More extensive studies are needed to propose the most appropriate technique in a particular clinical situation for the retrieval of fractured abutment screw.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Hanif A, Qureshi S, Sheikh Z, Rashid H. Complications in implant dentistry. Eur J Dent. 2017;11:135–40. doi: 10.4103/ejd.ejd_340_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Balshi TJ. Preventing and resolving complications with osseointegrated implants. Dent Clin North Am. 1989;33:821–68. [PubMed] [Google Scholar]
- 3.Katsavochristou A, Koumoulis D. Incidence of abutment screw failure of single or splinted implant prostheses: A review and update on current clinical status. J Oral Rehabil. 2019;46:776–86. doi: 10.1111/joor.12817. [DOI] [PubMed] [Google Scholar]
- 4.Winkler S, Ring K, Ring JD, Boberick KG. Implant screw mechanics and the settling effect: Overview. J Oral Implantol. 2003;29:242–5. doi: 10.1563/1548-1336(2003)029<0242:ISMATS>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 5.Gupta S, Gupta H, Tandan A. Technical complications of implant-causes and management: A comprehensive review. Natl J Maxillofac Surg. 2015;6:3–8. doi: 10.4103/0975-5950.168233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Whiting P, Savović J, Higgins JP, Caldwell DM, Reeves BC, Shea B, et al. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol. 2016;69:225–34. doi: 10.1016/j.jclinepi.2015.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Barbosa JM, Ascenso J, Hirata R, Caramês J. The cotton driver: An alternative technique for removing fractured screw fragments. J Prosthet Dent. 2014;112:1601–2. doi: 10.1016/j.prosdent.2014.07.012. [DOI] [PubMed] [Google Scholar]
- 8.Yang CH, Wu AY. A technique to retrieve a fractured implant abutment screw by using a screwdriver fashioned from a needle. J Prosthet Dent. 2019;121:709–10. doi: 10.1016/j.prosdent.2019.01.001. [DOI] [PubMed] [Google Scholar]
- 9.Fauvell SA, Gialanella G, Penna KJ. The Lumen Technique. Retrieval of broken gold screws in dental implants. N Y State Dent J. 2006;72:43. [PubMed] [Google Scholar]
- 10.Satterthwaite J, Rickman L. Retrieval of a fractured abutment screw thread from an implant: A case report. Br Dent J. 2008;204:177–80. doi: 10.1038/bdj.2008.99. [DOI] [PubMed] [Google Scholar]
- 11.Bhandari S, Aggarwal N, Bakshi S. Ultrasonic oscillations for conservative retrieval of a rare fracture of implant healing abutment. J Oral Implantol. 2013;39:475–8. doi: 10.1563/AAID-JOI-D-11-00126. [DOI] [PubMed] [Google Scholar]
- 12.Chen JH, Cho SH. An accessory technique for the intraoral removal of a fractured implant abutment screw. J Prosthet Dent. 2018;120:812–5. doi: 10.1016/j.prosdent.2018.01.026. [DOI] [PubMed] [Google Scholar]
- 13.Azpiazu-Flores FX, Lee DJ. Using the screw shank as a retrieval tool: A straightforward approach to removing screws with diagonal fractures. J Prosthet Dent. 2020;123:535–6. doi: 10.1016/j.prosdent.2019.12.003. [DOI] [PubMed] [Google Scholar]
- 14.Luterbacher S, Fourmousis I, Lang NP, Brägger U. Fractured prosthetic abutments in osseointegrated implants: A technical complication to cope with. Clin Oral Implants Res. 2000;11:163–70. [PubMed] [Google Scholar]
- 15.Williamson RT, Robinson FG. Retrieval technique for fractured implant screws. J Prosthet Dent. 2001;86:549–50. doi: 10.1067/mpr.2001.118922. [DOI] [PubMed] [Google Scholar]
- 16.Nergiz I, Schmage P, Shahin R. Removal of a fractured implant abutment screw: A clinical report. J Prosthet Dent. 2004;91:513–7. doi: 10.1016/j.prosdent.2004.03.010. [DOI] [PubMed] [Google Scholar]
- 17.Reyhanian A, Parker S, Moshonov J, Fuhrman N. The use of Er: YAG in laser-assisted broken abutment screw treatment. Case Rep Er YAG Lasers. 2010;3:6–11. [Google Scholar]
- 18.Yilmaz B, McGlumphy E. A technique to retrieve fractured implant screws. J Prosthet Dent. 2011;105:137–8. doi: 10.1016/S0022-3913(11)60015-2. [DOI] [PubMed] [Google Scholar]
- 19.Walia MS, Arora S, Luthra R, Walia PK. Removal of fractured dental implant screw using a new technique: A case report. J Oral Implantol. 2012;38:747–50. doi: 10.1563/AAID-JOI-D-10-00195. [DOI] [PubMed] [Google Scholar]
- 20.Taira Y, Sawase T. A modified technique for removing a failed abutment screw from an implant with a custom guide tube. J Oral Implantol. 2012;38:165–9. doi: 10.1563/AAID-JOI-D-10-00162. [DOI] [PubMed] [Google Scholar]
- 21.Kurt M, Güler AU, Duran İ. A technique for removal of a fractured implant abutment screw. J Oral Implantol. 2013;39:723–5. doi: 10.1563/AAID-JOI-D-11-00017. [DOI] [PubMed] [Google Scholar]
- 22.Satwalekar P, Chander KS, Reddy BA, Sandeep N, Sandeep N, Satwalekar T. A Simple and Cost Effective Method used for Removal of a Fractured Implant Abutment Screw: A Case Report. J Int Oral Health. 2013;5:120–3. [PMC free article] [PubMed] [Google Scholar]
- 23.Gooty JR, Palakuru SK, Guntakalla VR, Nera M. Noninvasive method for retrieval of broken dental implant abutment screw. Contemp Clin Dent. 2014;5:264–7. doi: 10.4103/0976-237X.132382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Carneiro TA, Prudente MS, E Pessoa RS, Mendonça G, das Neves FD. A conservative approach to retrieve a fractured abutment screw-Case report. J Prosthodont Res. 2016;60:138–42. doi: 10.1016/j.jpor.2015.09.003. [DOI] [PubMed] [Google Scholar]
- 25.Yoon JH, Lee H, Kim MY. Safe removal of a broken abutment screw with customized drill guide and rotary instrument: A clinical report. J Prosthodont. 2016;25:170–3. doi: 10.1111/jopr.12291. [DOI] [PubMed] [Google Scholar]
- 26.Flanagan D. Management of a fractured implant abutment screw. J Oral Implantol. 2016;42:508–11. doi: 10.1563/aaid-joi-D-16-00105. [DOI] [PubMed] [Google Scholar]
- 27.Pipko DJ, Kukunas S, Ismail YH. Retrofitting a cast dowel-core on salvaged dental implants. J Prosthodont. 2004;13:52–4. doi: 10.1111/j.1532-849X.2004.04006.x. [DOI] [PubMed] [Google Scholar]
- 28.Pow EH, Wat PY. A technique for salvaging an implant-supported crown with a fractured abutment screw. J Prosthet Dent. 2006;95:169–70. doi: 10.1016/j.prosdent.2005.12.005. [DOI] [PubMed] [Google Scholar]
- 29.Maalhagh-Fard A, Jacobs LC. Retrieval of a stripped abutment screw: A clinical report. J Prosthet Dent. 2010;104:212–5. doi: 10.1016/S0022-3913(10)00133-2. [DOI] [PubMed] [Google Scholar]
- 30.Yilmaz B, McGlumphy E. A technique to salvage a single implant-supported fixed dental prosthesis having a nonretrievable implant screw fragment. J Oral Implantol. 2013;39:81–3. doi: 10.1563/AAID-JOI-D-11-00051. [DOI] [PubMed] [Google Scholar]
- 31.Canpolat C, Ozkurt-Kayahan Z, Kazazoğlu E. Management of a fractured implant abutment screw: A clinical report. J Prosthodont. 2014;23:402–5. doi: 10.1111/jopr.12111. [DOI] [PubMed] [Google Scholar]
- 32.Gupta V, Prithviraj DR, Muley N. A new restorative technique for the perishing implant due to abutment screw fracture. J Oral Implantol. 2014;40:755–7. doi: 10.1563/AAID-JOI-D-12-00231. [DOI] [PubMed] [Google Scholar]
- 33.Harshakumar K, Bhatia S, Ravichandran R, Joy PT. Salvaging an implant with abutment screw fracture by a custom titanium post and core supported prosthesis-a novel technique. Int J Sci Study. 2014;2:36–9. [Google Scholar]
- 34.Shah K, Lee DJ. An alternative approach for the management of fractured implant abutment screws on a mandibular implant-retained overdenture: A clinical report. J Prosthet Dent. 2016;115:402–5. doi: 10.1016/j.prosdent.2015.09.027. [DOI] [PubMed] [Google Scholar]
- 35.Cecchini-259 J. Review of Implant Screw Fractures: Their Causes and Methods of Retrieval. Oral Health Group. 2017. [Last accessed on 2020 Dec 08]. Available from: https://www.oralhealthgroup.com/features/review-implant-screw-fractures-causes-methods-retrieval/
- 36.Lee KY, Shin KS, Jung JH, Cho HW, Kwon KH, Kim YL. Clinical study on screw loosening in dental implant prostheses: A 6-year retrospective study. J Korean Assoc Oral Maxillofac Surg. 2020;46:133–42. doi: 10.5125/jkaoms.2020.46.2.133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Quek CE, Tan KB, Nicholls JI. Load fatigue performance of a single-tooth implant abutment system: Effect of diameter. Int J Oral Maxillofac Implants. 2006;21:929–36. [PubMed] [Google Scholar]
- 38.Patel RD, Kan JY, Jonsson LB, Rungcharassaeng K. The use of a dental surgical microscope to aid retrieval of a fractured implant abutment screw: A clinical report. J Prosthodont. 2010;19:630–3. doi: 10.1111/j.1532-849X.2010.00644.x. [DOI] [PubMed] [Google Scholar]
- 39.Lee JH, Park JH, Park CJ, Cho LR. Technique to retrieve implant abutment fragments. J Prosthet Dent. 2015;114:486–9. doi: 10.1016/j.prosdent.2014.04.033. [DOI] [PubMed] [Google Scholar]
- 40.Mizumoto RM, Jamjoom FZ, Yilmaz B. A risk-based decision making tree for managing fractured abutment and prosthetic screws: A systematic review. J Prosthet Dent. 2018;119:552–9. doi: 10.1016/j.prosdent.2017.05.016. [DOI] [PubMed] [Google Scholar]
- 41.Abdelfattah MY. Different mechanical complications of implant prosthodontics: Review article. Int J Dent Sci Res. 2014;2:190–6. [Google Scholar]
- 42.Bakaeen LG, Winkler S, Neff PA. The effect of implant diameter, restoration design, and occlusal table variations on screw loosening of posterior single-tooth implant restorations. J Oral Implantol. 2001;27:63–72. doi: 10.1563/1548-1336(2001)027<0063:TEOIDR>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 43.Siamos G, Winkler S, Boberick KG. Relationship between implant preload and screw loosening on implant-supported prostheses. J Oral Implantol. 2002;28:67–73. doi: 10.1563/1548-1336(2002)028<0067:TRBIPA>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 44.Cho SC, Small PN, Elian N, Tarnow D. Screw loosening for standard and wide diameter implants in partially edentulous cases: 3- to 7-year longitudinal data. Implant Dent. 2004;13:245–50. doi: 10.1097/01.id.0000140459.87333.f8. [DOI] [PubMed] [Google Scholar]