

Abstract
We tested the link between COVID‐19 conspiracy theories and health protective behaviours in three studies: one at the onset of the pandemic in the United Kingdom (UK), a second just before the first national lockdown, and a third during that lockdown (N = 302, 404 and 399). We focused on conspiracy theories that did not deny the existence of COVID‐19 and evaluated the extent to which they predicted a range of health protective behaviours, before and after controlling for psychological and sociodemographic characteristics associated with conspiracy theory belief. COVID‐19 conspiracy beliefs were positively correlated with beliefs in other unrelated conspiracies and a general conspiracy mind‐set, and negatively correlated with trust in government and a tendency towards analytical thinking (vs. intuitive thinking). Unexpectedly, COVID‐19 conspiracy believers adhered to basic health guidelines and advanced health protective measures as strictly as non‐believers. Conspiracy believers were, however, less willing to install the contact‐tracing app, get tested for and vaccinated against COVID‐19, and were more likely to share COVID‐19 misinformation—all of which might undermine public health initiatives. Study 3 showed conspiracy theory believers were less willing to undertake health protective behaviours that were outside of their personal control, perceiving these as having a negative balance of risks and benefits. We discuss models explaining conspiracy beliefs and health protective behaviours, and suggest practical recommendations for public health initiatives.
Keywords: conspiracy theory, COVID‐19, fake‐news, health protective behaviours, pandemic
“Covid‐19, an ocean of misinformation…” (Stein et al., 2021).
1. INTRODUCTION
Viruses are not the only things that run wild during a pandemic. Conspiracy theories also spread rapidly far and wide via social networks (Larson et al., 2019; Vosoughi et al., 2018). In fact, conspiracy‐related content has prompted greater user engagement than content from qualified sources such as the World Health Organisation and national health services, such as the Centre for Disease Control in the United States (Mian & Khan, 2020; Stein et al., 2021). The ‘infodemic’ of conspiracy theory content is particularly worrying because it may represent a serious threat to public health initiatives. In this article, we evaluate this threat by testing whether conspiracy beliefs are negatively related to health protective behaviours that are critical for safeguarding and managing a pandemic.
The emergence of the novel coronavirus in late 2019 and early 2020 quickly gave rise to a range of new conspiracy theories, positing that the pandemic was caused by the secret acts of powerful malevolent individuals, despite most evidence suggesting it was caused by a zoonotic spillover (transmission from animal to human) (WHO, 2021). Some declared the pandemic a plot by pharmaceutical companies, others argued that it was an artificially created bioweapon—some even attributed the virus to 5G. The use of face masks, temperature checks, testing, therapies, and medicines were all the targets of misinformation at one point or another on social media. These beliefs are, however, not mere abstract inaccuracies that are harmlessly shared; some can have a profound impact on people's real‐life behaviours. For instance, the falsification of the virus’ severity broadcast on TV in March 2020 which downplayed it as a ‘little cold’ has been linked with lower compliance with safeguarding behaviours and a rise in death rates (Bursztyn et al., 2020). Ideally, when faced with a pandemic, citizens should comply with the public health guidance of medical experts, but research indicates that conspiracy beliefs could undermine this response. The question remains, however, to what extent this generalises across different types of conspiracy theories and health protective behaviours. In our work, we examine whether conspiracy theories that acknowledge the existence of the new coronavirus are associated with a range of protective behaviours and, where an association exists, whether it is dependent on psychological and sociodemographic characteristics of conspiracy believers.
A large body of research shows that health‐related conspiracy beliefs can undermine health protective behaviours. For example, people who believe in HIV conspiracy theories are less likely to attend regular medical check‐ups (Oliver & Wood, 2014), get vaccinated (Hornsey et al., 2018; Jolley & Douglas, 2014; Setbon & Raude, 2010), use a condom (Grebe et al., 2012; Ross et al., 2006), or comply with prescribed treatments (Mattocks et al., 2017). Research is, however, not unanimous regarding the nature of the link between conspiracy theories and COVID‐19 health protective behaviours. While most studies have found a negative relationship between conspiratorial beliefs and support for government COVID‐19 health guidelines (Allington et al., 2020; Freeman et al., 2020; Nowak et al., 2020; Romer & Jamieson, 2020; Swami & Barron, 2020), others have not (Čavojová et al., 2020; Fuhrer & Cova, 2020).
The type of health protective behaviour could explain the link between health conspiracy beliefs and compliance. For example, although conspiracy believers actively endorse alternative ‘therapies’ in general (e.g., homeopathy; Lamberty & Imhoff, 2018) and unproven treatments against COVID‐19 (e.g., chloroquine, colloidal silver; Bertin et al., 2020; Teovanović et al., 2020), they consistently judge vaccines negatively (Allington et al., 2020; Freeman et al., 2020; Meuer & Imhoff, 2021; Romer & Jamieson, 2020; see also van Mulukom et al., 2020 for a review of evidence). Contrasting relationships have also been found within single studies, with conspiracy beliefs being negatively related to social distancing, but not to hand hygiene (Biddlestone et al., 2020). The link between conspiracy theories and health protective behaviours is therefore not always negative and difficult to explain.
Evidence indicates that the link between conspiracy belief and adherence to health guidelines could be contingent on the nature of the belief—that is, whether it accepts or refutes the existence of the virus. Specifically, evidence suggests that conspiracy theories that denied the existence of the virus were connected with lower adherence to basic health guidelines, whereas those that did not deny the existence of the virus were not (Imhoff & Lamberty, 2020). At the time we conducted our first study, we were not aware of this particular finding, and therefore, based on pre‐pandemic evidence of health‐related conspiracy beliefs undermining health protective behaviours, we believed that even conspiracy beliefs that acknowledged the existence of COVID‐19 would be negatively related to health protective behaviours. Given that conspiracy theorists believe in powerful malevolent individuals (Sunstein & Vermeule, 2009) and have low trust in government and science (Lamberty & Imhoff, 2018), it was plausible to assume that advice from often villainised sources such as politicians and ‘big pharma’ could result in lower compliance with health protective behaviours, even when people believed the threat to be real. For example, exposure to a health conspiracy theory increased hesitancy to be vaccinated against viruses which people believe in, such as the seasonal influenza virus (Craciun & Baban, 2012). We therefore expected that conspiracy beliefs would be related to lower likelihood to follow health protective behaviours because the guidelines for these behaviours came from distrusted government and private pharmaceutical authorities.
To untangle the complex connection between conspiracy beliefs and health protective behaviours, we turn to the psychological characteristics of people who believe in conspiracy theories. Examining the characteristics of conspiracy believers may help to better explain their behaviour, since their behaviours could either be directly tied to their (incorrect) beliefs or better explained by underlying psychological characteristics. Identifying the psychological characteristics of conspiracy theorists could be a real advantage for public health initiatives. For instance, narratives could be tailored to reach out to conspiracy believers with information that resonates with them and campaigns could be designed to negotiate the value of adhering to health guidelines via a personalised and targeted approach.
There exists a clear set of individual characteristics associated with conspiracy belief. So much so that believing in a single conspiracy theory is one of the best predictors of beliefs in other (unrelated) conspiracy theories (Goertzel, 1994; Miller, 2020; Swami et al., 2011). What characteristics predispose people to believing in conspiracy theories, and could these characteristics explain the engagement (or lack thereof) with health protective behaviours? First, and foremost, conspiracy theory beliefs seem to emerge from a set of higher order general beliefs characterised as a conspiracy mind‐set (also known as conspiracy worldview, mentality, or thinking); these general beliefs predispose people to believe in conspiracy theories (Brotherton et al., 2013; Dagnall et al., 2015; Imhoff & Bruder, 2014). These include the beliefs that: (1) governments are maleficent, (2) small, secret, and powerful organisations control the world order, and (3) that these ill‐intentioned organisations cover‐up the existence of extra‐terrestrial lives, (4) threaten people's health and freedom and (5) control the flow of information (Brotherton et al., 2013). Having a conspiracy mind‐set predicts beliefs in health‐related conspiracy theories, such as those connected with the Zika virus (Klofstad et al., 2019). At the heart of these beliefs is the notion that ill‐intentioned groups are acting behind the scenes, pointing out the major role that trust plays in conspiracy beliefs.
Trust is an important contributor to conspiracy theory beliefs (Imhoff & Lamberty, 2018; Meuer & Imhoff, 2021). Different facets of trust, such as interpersonal trust (e.g., Goertzel, 1994), trust in healthcare (e.g., Mattocks et al., 2017), as well as political trust (e.g., Jasinskaja‐Lahti & Jetten, 2019) and trust in government (Pierre, 2020), have all been linked with conspiracy beliefs, and many with COVID‐19 conspiracy theories (Freeman et al., 2020; Pummerer et al., 2021). Trust in government is particularly relevant to better understand COVID‐19 conspiracy theories and their link to health protective behaviours because governments are often painted as malevolent in conspiracy theories, which may in turn shape whether people heed official health advice (or not). At the same time, it is hard to resolve whether it is specifically distrust in government that pushes people towards conspiracy theories (e.g., Kim & Cao, 2016; Pierre, 2020) or if it is believing in conspiracy theories that reduces trust (e.g., Pummerer et al., 2021). By contrast, cognitive factors can be more clearly understood as predictors of conspiracy belief, since the relationship is less likely to be reverse causal.
Some cognitive attributes might indeed make people more vulnerable to misinformation and conspiracy beliefs. In the dual process model of human cognition, analytical thinking is conceptualised as a slower and more in‐depth evaluation of information, as opposed to intuition, which is a faster and shallower form of information processing (De Neys & Pennycook, 2019; Epstein et al., 1996; Evans & Stanovich, 2013). Analytical thinking (as opposed to intuition) has been linked with a greater ability to reason, with for example the ability to avoid logical inaccuracies in a range of tasks (Toplak et al., 2011), less gullibility towards pseudo profound nonsense statements (Pennycook et al., 2015), lower endorsement of scientifically unfounded beliefs (e.g., paranormal belief; Pennycook et al., 2012), greater likelihood to share information from reliable sources (Mosleh et al., 2021) and more real‐life positive outcomes (Juanchich et al., 2016). In particular, analytical thinking reduces people's likelihood to fall prey to misinformation (Pennycook & Rand, 2020), including conspiracy theory beliefs (Čavojová et al., 2020; Denovan et al., 2020; Georgiou et al., 2019; Pytlik et al., 2020; Šrol et al., 2020 Preprint; Ståhl & van Prooijen, 2018; Swami & Barron, 2020; Swami et al., 2014; van der Wal et al., 2018). For example, more analytical participants (as measured by the Cognitive Reflection Test; Frederick, 2005) were less likely to believe that “5G electromagnetic field exposure played a role in the coronavirus pandemic” (Teovanović et al., 2020). Experimental evidence further supports the link between analytical thinking and conspiracy belief, with a nudge increasing analytical processing leading to a reduction of conspiratorial beliefs (Swami et al., 2014).
1.1. The present research
In summary, although we can expect conspiracy beliefs to undermine health protective behaviours, this relationship may not hold for conspiracy theories that acknowledge the new coronavirus does exist (vs. beliefs that it is a hoax for example), or across different types of protective behaviours. The reason why health conspiracy beliefs predict health behaviours also remains unclear—and could be explained by specific socio‐psychological and cognitive characteristics. In three studies we tested the extent to which COVID‐19 conspiracy theories (which acknowledge existence of the virus) related to health protective behaviours over and above their socio‐psychological profile. In Studies 1 and 2, we evaluate the extent to which some known socio‐psychological characteristics are associated with COVID‐19 conspiracy beliefs (e.g., conspiracy mind‐set, trust, analytical thinking style) and test whether those characteristics could explain the link between conspiracy theories and health protective behaviours (e.g., handwashing, social distancing, and vaccination). Study 2 extends our approach by focusing on four new behaviours: the adoption of advanced and non‐traditional health protective behaviours (e.g., wearing gloves), the intention to be tested for, or vaccinated against COVID‐19, and the tendency to share COVID‐19 misinformation. Finally, Study 3 tests the hypothesis that conspiracy theory believers are only reluctant to undertake the behaviours over which they do not have personal control, perceiving those as having a negative balance of risk and benefits. The studies were conducted at a critical time, over the first 3 months of the COVID‐19 pandemic in the United Kingdom (UK) (see timeline Figure 1).
FIGURE 1.
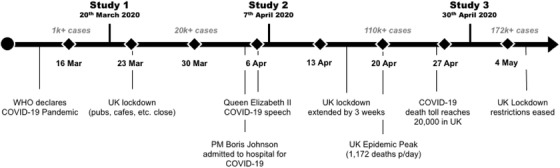
Timeline of the three studies where we evaluated the link between COVID‐19 conspiracy beliefs and health protective behaviours in the United Kingdom. Cases are cumulative cases for the UK (Worldometer, 2021)
Open Science Statement. All the studies were preregistered, with hypotheses, materials and analyses submitted to AsPredicted. Preregistration, data, and questionnaires are available on the Open Science Framework: https://osf.io/ujsrc/?view_only = 820fda53fc28401092a498766cea2ec1. The sample sizes were selected to maximise statistical power within budget. We conducted preregistered analyses as planned, and where the normality assumptions were not met, we conducted the equivalent non‐parametric analysis. The authors have no conflict of interest to declare, and the studies received ethical approval from the institution of the first author.
2. STUDY 1
We tested the prevalence of five conspiracy beliefs at the onset of the pandemic in the UK and how those beliefs related to basic health protective behaviours over and above two psychological characteristics connected with conspiracy theory beliefs: general conspiracy mind‐set and trust in governments. We hypothesised that general conspiracy mind‐set and trust in governments would be associated with COVID‐19 conspiracy beliefs and that these beliefs would be associated with fewer health protective behaviours and more stockpiling. The study was conducted on 20 March, 10 days after COVID‐19 was officially declared a pandemic by the WHO (2020) and “urgent and aggressive action” was recommended. Three days after, on 23 March 2020, the UK entered its first national lockdown.
2.1. Method
2.1.1. Participants
Three hundred and two participants completed the study online via the Prolific platform—their personal characteristics are shown in Table 1 and more details can be found in supplementary materials Table SM 1. We preregistered a sample of 400 participants to identify a correlation magnitude of ρ = |.12| (with alpha = .05 and .80 power, one tail), but following institutional budget cuts due to the pandemic, we reduced our sample size to 300 before launching data collection. According to a sensitivity analysis, this gave us enough power to detect ρ = |.14| correlations.
TABLE 1.
Sociodemographic characteristics of participants in Study 1, 2 and 3
| Study 1, n = 302 | Study 2, n = 404 | Study 3, n = 399 | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Gender | ||||||
| Female | 206 | 68% | 225 | 56% | 248 | 62% |
| Male | 95 | 32% | 174 | 43% | 144 | 36% |
| Other | 1 | 0% | 5 | 1% | 7 | 2% |
| Ethnicity | ||||||
| Asian British | 16 | 5% | 27 | 7% | 23 | 6% |
| Asian/Other | 2 | 1% | 7 | 2% | 1 | 0% |
| Black British | 9 | 3% | 21 | 5% | 11 | 3% |
| Black/Other | 0 | 0% | 5 | 1% | 2 | 1% |
| White British | 252 | 83% | 291 | 72% | 328 | 82% |
| White/Other | 9 | 3% | 25 | 6% | 18 | 5% |
| Other | 11 | 4% | 28 | 7% | 8 | 2% |
| Age | ||||||
| 18–25 | 64 | 21% | 57 | 14% | 107 | 27% |
| 26–40 | 140 | 47% | 135 | 34% | 176 | 44% |
| 41–55 | 66 | 22% | 101 | 25% | 83 | 21% |
| 55+ | 31 | 10% | 108 | 27% | 33 | 8% |
| Education | ||||||
| Less than high school | 3 | 1% | 9 | 2% | 4 | 1% |
| High school | 113 | 37% | 148 | 37% | 135 | 34% |
| Bachelor's Degree | 128 | 42% | 160 | 40% | 172 | 43% |
| Master's Degree or more | 42 | 14% | 68 | 17% | 69 | 17% |
| Other | 15 | 5% | 17 | 4% | 19 | 5% |
| Income | ||||||
| Less than $10,000 | 78 | 26% | 92 | 23% | 115 | 29% |
| $10,000–$30,000 | 127 | 43% | 166 | 41% | 146 | 37% |
| $30,000–$60,000 | 68 | 23% | 89 | 22% | 80 | 21% |
| Over $60,000 | 0 | 0% | 14 | 4% | 16 | 4% |
| Not disclosed | 22 | 7% | 42 | 10% | 42 | 11% |
| Political Preference | ||||||
| Labour | 121 | 40% | 140 | 35% | 146 | 37% |
| Conservative | 74 | 25% | 109 | 27% | 81 | 20% |
| Liberal Democrat | 26 | 9% | 35 | 9% | 45 | 11% |
| UK Independence Party | 4 | 1% | 6 | 2% | 3 | 1% |
| Other political party | 22 | 7% | 42 | 10% | 56 | 14% |
| No political preference | 41 | 14% | 49 | 12% | 45 | 11% |
| Not disclosed | 14 | 5% | 22 | 5% | 23 | 6% |
| Employment | ||||||
| Unemployed | 87 | 29% | 130 | 32% | 131 | 33% |
| Employed and working | 186 | 61% | 212 | 53% | 186 | 47% |
| Employed but furloughed | 29 | 10% | 61 | 15% | 82 | 21% |
| Works on the “frontline”* | 65 | 21% | 39 | 10% | 40 | 10% |
* Note: individuals working in their “normal” setting which is not home (vs. working from home, being furloughed or unemployed). This includes for example some health workers, teachers, checkout operators in essential shops, or refuse collectors. More details about the sample are provided in supplementary materials.
2.1.2. Materials and procedure
Participants were paid £0.75 to complete the survey online (plus a £0.27 bonus for a 9‐minute survey duration), which consisted of informed consent followed by five scales: trust in government, conspiracy mind‐set, past conspiracy theory belief, COVID conspiracy theory beliefs, and adherence to safeguarding behaviours, including basic health guidelines scale and tendency to stockpile scale. The measure of trust was presented either before or after the three measures related to conspiracy theories, and those were followed by the safeguarding measure. The six scales all reached a good reliability (Cronbach's alpha ranged from .82 to .94), and we computed an average score for each.
Belief in COVID‐19 conspiracy theories . We identified five COVID‐19 conspiracy beliefs by searching the key terms “conspiracy theory” and “coronavirus” (see Table 2). Participants indicated the degree to which they believed in each of those five COVID‐19 conspiracy theories on a 5‐point Likert scale (1: Definitely not true and 5: Definitely true, with 3: Not sure/cannot decide).
TABLE 2.
To what extent do people believe in COVID‐19 conspiracy theory beliefs? We evaluated thepredictors and behavioural correlates of the following COVID‐19 conspiracy beliefs
| No | COVID‐19 conspiracy theories |
|---|---|
| 1 | The new coronavirus was leaked from a high security lab in Wuhan, and China is trying to cover it up. |
| 2 | The new coronavirus was part of an effort by pharmaceutical companies to profit by selling vaccines for it. |
| 3 | The new coronavirus was released as part of a Chinese covert biological weapons programme to destabilise Western countries. |
| 4 | The new coronavirus has been bioengineered by people who plot to cull certain populations. |
| 5 | The new coronavirus has been created by China, to harm the economy of Western countries. |
| 6 | There is a vaccine or cure for the coronavirus that the government won't release/authorise. (Studies 2 and 3) |
| 7 | Many governments let the coronavirus spread so that they could take dictatorial powers. (Studies 2 and 3) |
| 8 | Chinese tech companies are using 5G to weaken our immune system and/or spread the coronavirus. (Study 3) |
Note: These conspiracy theory beliefs were measured in Study 1, 2, and 3 unless indicated otherwise in the parentheses.
Belief in other conspiracy theories . Participants rated their agreement with 13 conspiracy beliefs adapted from the scale of Douglas et al., and Harvey (2016). Participants indicated the degree to which they believed in each of those conspiracy theories on a 7‐point Likert scale (1: Strongly disagree and 5: Strongly agree). The scale included conspiracy theories related to climate change, celebrities and the HIV epidemics (e.g., Scientists are creating panic about climate change because it is in their interests to do so).
General conspiracy mind‐set . We measured the five facets of conspiracy belief mind‐set using the 15 items of the Generic Conspiracist Beliefs Scale (Brotherton et al., 2013). The facets included: governmental maleficence, small international organisations control the world order, cover‐up the existence of extra‐terrestrial lives, threat to people's health and freedom and control of information (e.g., The government is involved in the murder of innocent citizens and/or well‐known public figures, and keeps this a secret). Participants indicated the degree to which they believed in each statement on a 5‐point Likert scale (1: Definitely not true and 5: Definitely true, with 3: Not sure/cannot decide).
Trust in government . We used an adapted version of the Trust in Government Scale (Grimmelikhuijsen & Knies, 2017) and measured perceived competence, benevolence, and integrity as dimensions of trust (e.g., In general, I believe that governments and governmental bodies are capable). Participants reported their agreement on a 5‐point Likert scale (1: strongly disagree to 5: strongly agree).
Basic health protective behaviours . Participants rated on a 4‐point scale how often (1: not at all, 2: some of the time, 3: most of the time, 4: all of the time; 99: not applicable) they performed a list of 10 behaviours in the last 24 hours (e.g., I used hand sanitizer gel if soap and water were not available).
Stockpiling behaviours . Participants reported whether in the last 7 days they had bought, or attempted to buy, more of any regular items that they would usually buy (e.g., pasta, long life milk, toilet paper) and the specific additional amount (0: No, 1: Yes, one or two extra, 2: Yes, three or four extra, or 3: Yes, five or more extra).
Self‐isolation commitment . Participants reported whether they would self‐isolate if they showed symptoms consistent with COVID‐19. Out of 302 participants, only 1 answered “no” (0.3%) and 18 reported “maybe”. So, for lack of variability, this was not included in our analysis.
Personal characteristics and situation . Participants also reported a range of sociodemographic characteristics and personal information reported in Table 1. Finally, participants completed two additional questions concerning risk perception that were unrelated to the present study (Holford et al., 2021).
2.2. Results
2.2.1. Socio‐psychological antecedents of COVID‐19 conspiracy theory beliefs
Overall, 27% of the participants endorsed at least one of the five COVID‐19 conspiracy beliefs listed in our study, judging that the conspiracy theory was either “probably” or “definitely” true. Between 10% and 20% of the participants agreed that each of the five COVID‐19 conspiracy theories was “likely” or “definitely” true (see Table 3). A correlation analysis showed that, in line with our expectation, conspiracy mind‐set was correlated with believing in COVID‐19 conspiracy theories (and beliefs in other conspiracy theories), while trust was negatively correlated with COVID‐19 conspiracy belief (see Figure 2). Some sociodemographic characteristics were also positively related to COVID‐19 conspiracy theory beliefs: being part of an ethnic minority, being more educated (continuous variable from no formal education to PhD degree), and being a frontline worker were all positively related to conspiracy theory beliefs. 1 A full correlation table showing all the study variables is shown in Supplementary Materials (Table SM2).
TABLE 3.
Proportion of individuals who agreed/disagreed with COVID‐19 conspiracy theory beliefs across studies (Study 1, n = 302, 20/02/2020; Study 2, n = 396, 07/04/2020, Study 3, n = 399, 30/04/2020)
| Study 1 | Study 2 | Study 3 | ||||
|---|---|---|---|---|---|---|
| COVID‐19 conspiracy theories | Agree | Disagree | Agree | Disagree | Agree | Disagree |
| China cover‐up of Coronavirus leak from high security lab | 23% | 62% | 22% | 56% | 24% | 56% |
| Coronavirus was created by pharmaceutical companies | 7% | 81% | 5% | 85% | 5% | 86% |
| Coronavirus is a Chinese covert biological weapon | 9% | 74% | 10% | 76% | 10% | 72% |
| Coronavirus has been bioengineered to cull certain populations. | 13% | 70% | 10% | 76% | 11% | 77% |
| China created the coronavirus to harm Western economies | 12% | 74% | 10% | 77% | 11% | 73% |
| The government has a vaccine but won't release it | – | – | 9% | 83% | 8% | 83% |
| Governments use the virus to take dictatorial powers | – | – | 10% | 76% | 11% | 75% |
| 5G network is causing or fuelling the epidemics | – | – | – | – | 3% | 91% |
Note : The remainder % chose the answer “not sure”.
FIGURE 2.
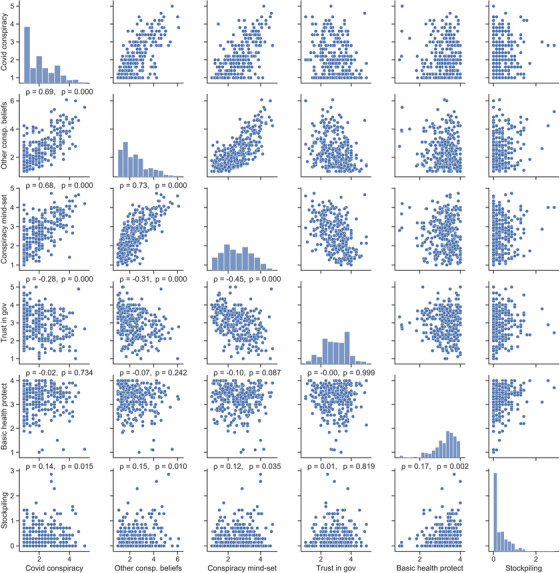
Relationship between beliefs in Covid‐19 conspiracy theories, psychological predictors, behaviours and sociodemographic characteristics in Study 1 (n = 302). The correlation coefficients in the lower quadrant are Spearman ρ and the variables distributions are shown in the diagonal
2.2.2. Does endorsing COVID‐19 conspiracy theories predict safeguarding behaviour?
A correlation analysis showed that conspiracy belief was not statistically significantly associated with basic health protective behaviours, indicating that conspiracy theory believers reported following health guidelines as much as others. However, we found a small positive statistically significant correlation between conspiracy beliefs and stockpiling. To evaluate whether that relationship held over and above the psychological characteristics of conspiracy believers, and relevant sociodemographic characteristics, we conducted a two‐step hierarchical regression reported in Table 4. The analysis showed that COVID‐19 conspiracy beliefs did not predict stockpiling behaviour over and above conspiracy mind‐set and trust in government. The final model shows that only belonging to ethnic minority groups and working on the frontline were associated with more stockpiling.
TABLE 4.
Regression analyses evaluating the extent to which COVID‐19 conspiracy beliefs predict stockpiling behaviours over and above conspiracy predictors and selected sociodemographic characteristics
| Outcome: Stockpiling | Model step 1 | Model step 2 |
|---|---|---|
| COVID conspiracy beliefs | .04 (.04) [–.04, .11] | .03 (.03) [−.04, .10] |
| Consp. mind‐set | .06 (.04) [−.03, .14] | .02 (.04) [−.06, .10] |
| Trust | .06 (.04) [−.01, .13] | .06 (.03) [−.00, .13] |
| Ethnic minority | .34 *** (.07) [.21, .48] | |
| Education | .02 (.04) [−.05, .09] | |
| Frontline work | .19 ** (.06) [.07, .30] | |
| F change model summary | F(3, 279) = 2.69, p = .047, | F(3, 276) = 11.66, p < .001, |
| R2, R2 change | .03, .03 | .14, .11 |
** p < .01, *** p < .001. Sociodemographic variables that had statistically significant correlations with conspiracy theory beliefs (p < .05) were included in the model.
2.3. Discussion
Contrary to our expectations, COVID‐19 conspiracy beliefs were not negatively related with adherence to basic health protective behaviours. Overall, participants reported a strong compliance with basic health protective behaviours, such as hand washing and social distancing, suggesting limited variability and that a possible ceiling effect for these basic behaviours may have occurred. In Study 2, we broaden our scope to new, more advanced health protective behaviours, for which we expected answers to be less skewed. In line with our predictions, we found that attitudinal variables, such as having a conspiracy mind‐set and low trust in government, were related to beliefs in COVID‐19 conspiracy theories and that those attitudes explained away the small correlation between conspiracy theory beliefs and stockpiling behaviour. In Study 2 we extended our approach of the correlates of conspiracy theories to a cognitive factor: people's tendency to rely on analytical thinking (vs. intuition).
3. STUDY 2
Study 2 was conducted on 7 April 2020 during the first UK lockdown. The virus had not yet reached the peak of the first epidemic wave (see timeline in Figure 1 for global context). We extended our scope to new health‐related measures and cognitive predictors of conspiracy beliefs. We added a measure of advanced health protective behaviours, intention to get tested for and vaccinated against COVID‐19 and a measure of the likelihood to share COVID misinformation online. We also added a measure of analytical thinking which was expected to be negatively related with conspiracy theory beliefs (Šrol et al., 2020 Preprint; Swami & Barron, 2020; Swami et al., 2014).
We hypothesised that about 15% of participants would endorse each conspiracy theory and that those beliefs would be negatively related to trust in government and positively related to analytical thinking and education. We hypothesised that COVID‐19 conspiracy beliefs would be associated with regular and advanced health protective behaviours, but we did not specify the direction of this relationship given our findings in Study 1. We also expected COVID‐19 conspiracy beliefs to be positively related to stockpiling and likelihood to share COVID‐19 misinformation online, and negatively related to intention to be tested for or vaccinated against COVID‐19.
3.1. Method
Participants. Of the 412 individuals who completed the study online via the Prolific platform, we excluded data from eight respondents who answered in less than 2 minutes (n = 1) or failed the attention check (n = 7). The characteristics of the 404 remaining participants are shown in Table 1. Out of this sample we purposefully included 100 participants from Study 1, to evaluate the stability of conspiracy beliefs.
3.2. Materials and procedure
The study lasted about 14 minutes and participants were paid £1.16 (£0.75 and a £0.41 bonus to reach £5/hour). Participants started with either the COVID‐19 conspiracy theory questions or the two main predictors: trust and analytical thinking. These were followed by the predicted behaviours and intentions presented in a fixed order: basic health protective behaviours, including outings and face‐to‐face interactions, stockpiling, advanced health protective behaviours, intention to get tested and vaccinated, and likelihood to share misinformation online. Our behavioural measures focused on the past 3 days to minimise distorted memories. The scales all had good reliability (Cronbach's alpha between .76 and .94) and we computed the average score for all of them, except for the analytical thinking measure for which we used a sum of correct answers.
Belief in COVID‐19 conspiracy theories . To the same measure as Study 1, we added two new COVID‐conspiracy beliefs that rose in reaction to the lockdown measures and were more political in nature; “There is a vaccine or cure for the coronavirus that the government won't release/authorise”, “Many governments let the coronavirus spread so that they could take dictatorial powers”. The task also included an attention check question (select “I do not agree at all”).
Trust in government . We used the same measure of trust as in Study 1.
Analytical thinking . We measured participants’ tendency to rely on analytical thinking (vs. intuition) with the Cognitive Reflection Test (CRT). The test measures the ability to inhibit intuitive thinking processes to adopt analytical thinking (Frederick, 2005). We used the seven‐item CRT (Toplak et al., 2014), an expanded version of the original three‐item version (Frederick, 2005) but featuring multiple‐choice answers (validated by Sirota & Juanchich, 2018). To answer the CRT questions correctly, participants must inhibit the first answer that springs to mind, and think more carefully (i.e., analytically) about what the correct answer may be. Each of the seven questions was presented with four possible answers, including the intuitive incorrect one, two decoys, and the correct one presented in a random order to each participant. An example item is: “A baseball bat and a ball cost £1.10 together, and the bat costs £1.00 more than the ball, how much does the ball cost?” The answers available included the intuitive incorrect answer (10 pence), two alternative incorrect answers (9 pence and 1 pence) along with the correct answer that required analytical thinking to be chosen (5 pence). This CRT format using multiple choices was validated as being as effective as the original test to measure cognitive reflection while taking less time to complete and avoiding coding errors (Sirota & Juanchich, 2018). A higher sum score of correct answers indicates stronger analytical thinking.
Basic health protective behaviours . We used a similar measure as for Study 1, but we made three minor changes to reflect the developments in government guidance: the distance between people was adjusted from 1 meter to 2 meters and we replaced the item “I avoided public gatherings of more than 5 people” with “I only went out for essential needs, including food, exercise or medical supply/appointment”. Participants answered on a 4‐point scale with 1: Not at all, 2: Some of the time, 3: Most of the time, 4: All the time, with the added option: 99: Not applicable (excluded from the analyses). Participants also reported the number of outings and face‐to‐face interactions they had over the last 3 days (outside their household) by selecting a number between 0 and “6 or more” in increments of 1 or “Prefer not to say” (coded 99 and excluded from the analyses).
Advanced health protective behaviours . Participants rated how often they performed eight behaviours in the last 3 days. The behaviours related to three specific situations: when participants left their home [2 items, e.g., “I wore a face mask”], when they came back home [2 items; e.g., “I undressed and put my clothes to wash straight away”], and what they did with their grocery shopping [3 items; e.g., “I washed all of the products that I could with soap”]). Note that in early April 2020 when Study 2 was conducted, wearing a face mask was considered an advanced protection measure because it was still not recommended by the UK national health authorities; in fact, masks were not readily available in the UK at that time, and it was advised not to wear one to avoid depleting scarce resources that were urgently needed for frontline healthcare workers. Participants answered using the same 4‐point scale as for basic health protective behaviours (1: Not at all—4: All the time, 99: Not applicable). Overall, 37% of participants answered the items “did not apply” to them, due to either not leaving their home or not doing grocery shopping (coded 99 and excluded).
Intention to get tested and vaccinated . Participants reported whether they would get tested for and vaccinated against COVID‐19 if the government was recommending them to do so. We described the vaccine as 70% effective (similar to the flu). For both questions, participants responded on a 7‐point scale ranging from 1: Certain that I would not do it to 7: Certain I would do it with “possible” as a middle point (4).
Stockpiling behaviours . We adapted our stockpiling measure given the restrictions that supermarkets had placed on buying items (e.g., no more than three of the same product could be purchased) and we instead focused our question on “building a stockpile” of long‐life items that could be used in case of food shortages or the need to self‐isolate. Participants rated how much they had tried to stock seven items (e.g., sugar, flour, cans) on a 4‐point scale (1: No, not at all, 2: Yes, a little bit, 3: Yes, quite a bit, 4: Yes, completely).
Sharing COVID‐19 misinformation . Participants read eight social media posts (one per page, randomised order for each participant) and evaluated their likelihood to share each post (adapted from Pennycook et al., and Rand (2020). Six posts were COVID‐19 misinformation: three referred to conspiracy theories (e.g., the virus was deliberately released from a Chinese lab) and three were medical misinformation regarding bogus protective measures (being in the sun) and cures (coconut oil and salted water). Finally, we also included two real news posts taken from Pennycook et al. (2020) to obscure our particular focus on misinformation. The likelihood to share the news item was measured on a 6‐point scale (1: Extremely unlikely to 6: Extremely likely). Overall, participants differentiated well between the real and false information and were more likely to share real news than the misinformation posts, M = 2.08, SD = 1.21 and M = 1.63, SD = 0.94, t(402) = 9.79, p < .001, Cohen's d = .49 (r = .66, p < .001). We used the average likelihood to share the misinformation across the six misinformation posts.
Personal characteristics. Participants answered the same questions as in Study 1 (see Table 1).
3.3. Results
3.3.1. Socio‐psychological antecedents of COVID‐19 conspiracy theory beliefs
Overall, 27% of the participants endorsed at least one of the seven COVID‐19 conspiracy theories listed (see Table 2). Focusing on the subsample of participants who took part in both Study 1 and Study 2 (n = 103) showed that COVID‐19 conspiracy beliefs were fairly stable over time, M March = 1.99, SD = 0.83 vs. M April 1.88, SD = 0.83, t(102) = 1.58, p = .117, with a large correlation, Spearman ρ = .71, p < .001. This supports past findings that conspiracy beliefs are stable over time (Sanche et al., 2020).
In line with our expectation, trust in government and analytical thinking were statistically significantly correlated with belief in COVID‐19 conspiracy theories (see Figure 3). In terms of sociodemographic characteristics, being part of an ethnic minority and voting for a conservative party were associated with a greater uptake of conspiracy beliefs, while using the national broadcaster (BBC) as a news source and having a higher level of education were linked with a lower uptake of those beliefs. 2 A full correlation table showing all the study variables is shown in Supplementary Materials (Table SM3).
FIGURE 3.
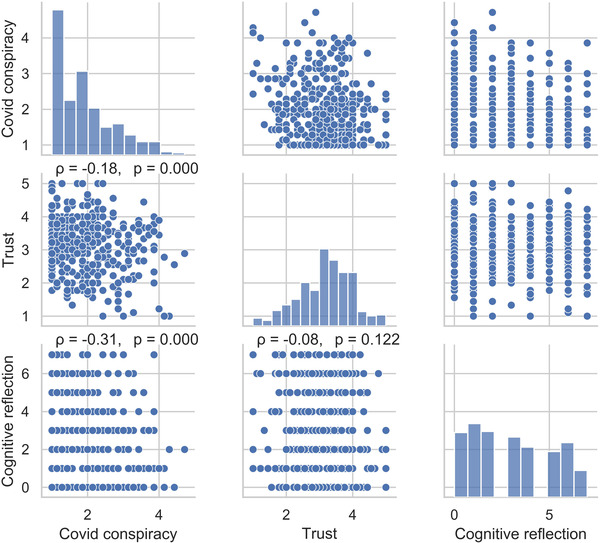
Correlations between COVID‐19 conspiracy beliefs and psychological characteristics in Study 2 (n = 404). The correlation coefficients in the lower quadrant are Spearman ρ and the variables distributions are shown in the diagonal
3.3.2. COVID‐19 conspiracy beliefs and health protective behaviours
The correlations analysis showed that believing in COVID‐19 conspiracy theories was not correlated with classic safeguarding behaviours including basic health behaviours, outings, face‐to‐face interactions and stockpiling (see Figure 4). There was a tendency for conspiracy believers to undertake more advanced health protective behaviours, but it was not statistically significant. The only health‐related behaviours that were statistically related to conspiracy beliefs were COVID‐19 diagnostic testing and vaccination and the tendency to spread COVID‐19 misinformation. People who believed in COVID‐19 conspiracy theories were less likely to agree to get tested for or vaccinated against COVID‐19 and were more likely to share misinformation about the virus. An exploratory analysis reported in Supplementary Materials C showed that conspiracy believers were more likely to share any type of news (real or false) compared to non‐believers, indicating that non‐believers discriminated better between the real and false information.
FIGURE 4.
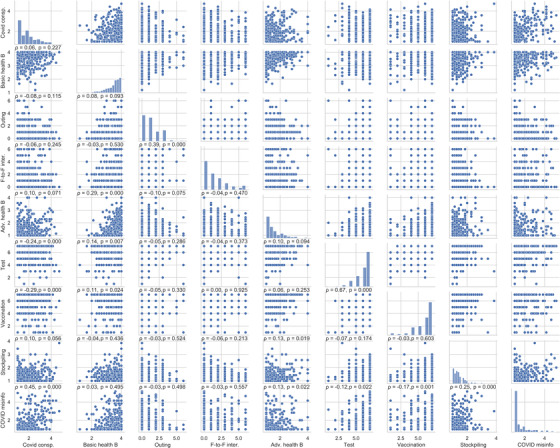
Correlations between COVID‐19 conspiracy beliefs and health protective behaviours in Study 2 (n = 404). The correlation coefficients in the lower quadrant are Spearman ρ and the variables distributions are shown in the diagonal
The predictive value of COVID‐19 conspiracy belief for testing, vaccination, and misinformation sharing was further tested in a series of two‐step hierarchical regression analyses, to see whether cognitive reflection and trust in government or sociodemographic characteristics could help to explain the relationships. The analyses shown in Table 5 revealed that COVID‐19 conspiracy beliefs remained a statistically significant predictor for testing, vaccination, and misinformation sharing even after we controlled for cognitive reflection, trust, and for key sociodemographic characteristics that correlated with conspiracy theories (see model 2).
TABLE 5.
How much do conspiracy theory beliefs predict COVID‐19 screening tests, COVID‐19 vaccination intentions and COVID misinformation sharing tendencies (n = 378)
| Model 1 | Model 2 | |
|---|---|---|
| Outcome: Intention to get tested | ||
| COVID conspiracy belief | −.39*** (.08) [−.55, −.24] | −.34*** (.08) [−.50, −.18] |
| Analytical thinking | −.01 (.03) [−.07, .04] | −.02 (.03) [−.08, .04] |
| Trust in government | .23** (.08) [.08, .38] | .26** (.08) [.10, .42] |
| Ethnic minority | −.16 (.14) [−.44, .13] | |
| BBC news | .13 (.15) [−.17, .42] | |
| Conservative | .22 (.14) [−.50, .06] | |
| Model summary | ||
| F change (df) | (3, 367) = 15.15, p < .001 | (3, 364) = 1.28, p = .280 |
| R2, R2 change | .13, .13 | .15, .01 |
| Outcome: Intention to get vaccinated | ||
| COVID‐19 conspiracy belief | −.49*** (.10) [−.68, −.30] | −.41*** (.10) [−.62, −.22] |
| Analytical thinking | .00 (.04) [−.07, .08] | −.00 (.04) [−.07, .07] |
| Trust in government | .37*** (.10) [.18, .56] | .33** (.10) [.13, .53] |
| Ethnic minority | −.53** (.18) [−.88, −.18] | |
| BBC news | .13 (.18) [−.23, .49] | |
| Conservative | .05 (.18) [−.40, .29] | |
| Model summary | ||
| F change (df) | (3, 367) = 18.35, p < .001 | (3, 364) = 1.28, p = .024 |
| R2, R2 change | .12, .03 | .14, .02 |
| Outcome: Spreading COVID misinformation | ||
| COVID‐19 conspiracy belief | .52*** (.06) [.41, .62] | .48*** (.06) [.36, .59] |
| Analytical thinking | −.04 (.02) [−.08, .01] | −.03 (.02) [−.07, .01] |
| Trust in government | .02 (.05) [−.09, .13] | .03 (.06) [−.09, .14] |
| Ethnic minority | .11 (.10) [−.09, .31] | |
| BBC news | −.29 (.10)** [−.49, −.08] | |
| Conservative | .04 (.10) [−.16, .23] | |
| Model summary | ||
| F change (df) | (3, 367) = 2.11, p < .001 | (4, 364) = 3.92, p = .027 |
| R2, R2 change | .25, .25 | .27, .02 |
* p < .05, ** p < .01, *** p < .001. Sociodemographic variables that had statistically significant correlations with conspiracy theory beliefs (p < .05) were included in the model.
3.4. Discussion
Overall, Study 2 showed that conspiracy believers reported an equal likelihood of following basic and advanced health guidance when compared to non‐believers, but a lower likelihood to agree to get tested for, or vaccinated against, COVID‐19 and a greater tendency to share COVID misinformation, even after we controlled for socio‐cognitive characteristics. The findings highlight that, on the one hand, people who believed in conspiracy theories were following guidelines to the same extent as others. On the other hand, paradoxically, they were also reluctant to undertake some other safeguarding behaviours, such as being tested or vaccinated. In Study 3, we aimed to reconcile this apparent contradiction.
4. STUDY 3
The study was conducted on 30 April 2020, 10 days after the highest number of daily deaths had occurred—commonly called the peak of the first epidemic wave—with 1,172 deaths in 24 hours (see timeline in Figure 1). In this study, our goal was to test the robustness of the findings of Study 2 and to explain the links found between conspiracy beliefs and health protective behaviours, as well as add two new COVID‐19 relevant behaviours: antibodies testing and using a contact‐tracing app.
We aimed to test two non‐exclusive explanations for why conspiracy believers follow some health protective behaviours but not others. First, we noticed that health protective behaviours differed in terms of agency, which is the degree to which people have autonomy and control over the behaviour. All the behaviours that conspiracy believers performed as much or more than other people provide autonomy and control: one chooses to wash their hands, or to wear a mask, and the extent to which this is done well does not rely on anybody else. By contrast, being tested or vaccinated cannot be performed autonomously: it requires the involvement of others one needs to trust to get the job well done. This necessary intrusion may generate a particularly distressing worry for conspiracy believers since they tend to score low on trust and higher than others on interpersonal paranoia (Freeman et al., 2020; Goreis & Voracek, 2019). In particular, lacking the power to make autonomous decisions has been shown to deter conspiracy theory believers from some safeguarding behaviours, such as vaccination (Jolley & Douglas, 2014). A second and non‐exclusive explanation focuses on the perceived value of different protective behaviours. According to this hypothesis, vaccination and testing would be perceived as having a more negative balance of risks and benefits by conspiracy believers compared to others, whereas basic and advanced health behaviours would be perceived as having a similar balance of risks and benefits. The utility of different options is essential to decision‐making theoretical models (Morgenstern & von Neumann, 1943) and indeed to shaping decisions (McDowell et al., 2016). Medical interventions, and in particular vaccinations, are often the target of false information campaigns which may distort the perception of their risks and benefits (e.g., immunisations cause autism; Kata, 2012). Conspiracy believers tend to perceive that vaccines are dangerous, which partly explains their reluctance to be vaccinated (Jolley & Douglas, 2014).
We hypothesised that control and utility would explain the uptake of health protective behaviours. We expected COVID‐19 conspiracy beliefs would not to be associated with basic health protective behaviours but would be associated with more advanced health protective behaviours and stockpiling behaviours and a lower intention to take a COVID‐19 diagnostic test, a COVID‐19 antibodies test, the COVID‐19 vaccine and to use a contact‐tracing app. We expected that people would judge that they have control over basic health behaviours, advanced health behaviours, and stockpiling, but that this would not be the case for vaccination, taking an antibodies test, a diagnostic test, and using the contact tracing app. We hypothesised that events perceived as controllable (basic health behaviours, advanced health behaviours, and stockpiling) would be perceived as having a greater utility than less controllable behaviours (tests, vaccination, and using the app), in particular for those with stronger conspiracy beliefs. We also hypothesised that the utility and controllability of a behaviour would positively predict its uptake and that this would partly explain the relationship between conspiracy beliefs and behaviours.
4.1. Methods
4.1.1. Participants
The characteristics of the 399 participants are shown in Table 1. These participants had not taken part in Study 1 or Study 2.
4.1.2. Materials and procedure
The study took 10 minutes on average and participants were paid £0.84 (an initial £0.75 for an estimated duration of 7 minutes, adjusted upward via a bonus to £0.84 to reach £5/hour).
Belief in COVID‐19 conspiracy theories . The measure was the same as in Study 2, except we added a new viral conspiracy theory: “Chinese tech companies are using 5G to weaken our immune system and/or spread the coronavirus” (see Table 2).
Sharing COVID‐19 misinformation . To measure the tendency to share COVID‐19 misinformation, participants reported their likelihood to share three social media posts hinting at a conspiracy: one post declaring that the virus was released from a Chinese lab, and two that referred to the possibility that the virus was being intentionally fuelled via the 5G network. These three misinformation posts were supplemented with two real recent news articles published in the national press: one announcing the first human trial for a coronavirus vaccine and one announcing the beginning of a trial testing the benefits of nicotine in coronavirus treatment. As in Study 2, overall, participants discriminated well between the real and the false information and were more likely to share real information, M = 2.00, SD = 0.86 and M = 1.51, SD = 0.76, t(398) = 11.39, p < .001, Cohen's d = .85 (r = .45, p < .001).
Health protective behaviours and intentions . We measured 11 health protective behaviours. We used a selection of the basic and advanced health questions and extended their focus to the last 7 days (instead of the last day only) to avoid a floor effect. We measured three basic health behaviours: increased handwashing, staying at home, and social distancing, and three advanced health behaviours: wearing facemasks, gloves, and washing grocery products with soap. An item asking about unpacking groceries and handwashing was also included but was judged redundant with general handwashing and was not included in the analysis (results were the same). We also measured stockpiling with 1 item where participants reported for how long they could live off the food and first‐necessity items they currently had at home (response: for less than 7 days, 7, 10, or 14 days and more).
We used the same materials to measure intention to vaccinate and to take a diagnostic test and we introduced two new behavioural intentions: the intention to get tested for COVID‐19 antibodies (based on a blood test, which may seem more invasive than the swab needed for the diagnostic test) and the intention to instal the contact tracing app that was about to be released by the National Health Service (NHS). The intentions were measured with a 5‐point Likert scale ranging from ‘very unlikely’ to ‘very likely’. For the contact tracing app, participants were randomly allocated to one of two conditions: a control condition where they were simply asked about their likelihood to instal and use the app after a brief description of its utility or the same description together with a control boost message that was expected to increase its acceptability (‘Take back control and stop the spread thanks to the contact tracing app’). The manipulation did not affect participants’ likelihood to accept to use the app (M control = 3.46, SD = 1.24, M boost = 3.64, SD = 1.36, t(397) = 1.36, p = .174, Cohen's d = 0.14), and data were pooled together.
Perception of personal control . Participants rated their perceived control and autonomy for all of the 11 health protective behaviours and intentions: staying at home, social distancing, handwashing, wearing facemasks, wearing gloves, washing groceries with soap, keeping enough essential items at home, getting vaccinated, getting the COVID‐19 diagnostic test, getting the COVID‐19 antibodies test, and using the NHS contact tracing app. Participants read that protective measures varied in terms of how much control people had over undertaking them and how well they were done. Then, participants evaluated whether, “yes” or “no”, they had control over the behaviours listed.
Utility perception: risks and benefits. For each of the 11 behaviours of interest, participants reported the extent to which the behaviour was risky, defined as “could have negative consequences that could affect you, people around you or society in general, possibly involuntarily”. On a separate page, participants reported the extent to which each behaviour could be beneficial, defined as having “positive consequences for you, people around you or society in general”. Participants reported their perception on a 4‐point scale ranging from Not at all risky/beneficial to 4: Very risky/beneficial. We computed a utility score for each behaviour by taking away the risk responses form the benefits responses (Utility = Benefits—Risks).
Personal situation and characteristics . We measured the same personal characteristics as before but we added a measure of political conservatism by asking participants where they stood regarding economic issues and social issues on a Likert scale ranging from 1: Strongly liberal to 5: Strongly conservative.
4.2. Results
4.2.1. Beliefs in and sharing of COVID‐19 conspiracy theories
Overall, 31% of the participants endorsed at least one of the eight COVID‐19 conspiracy theories (see Table 3). This shows a slight increase over time from 27% in February and early April. As expected, the theory that China bioengineered the virus was endorsed by more than 20% of participants, p = .035. The other conspiracy theories were endorsed by about 10% of the participants, except the theory that the virus was created by pharmaceutical companies and the theory that the 5G network spreads the virus, which both had lower endorsement, p < .001. As we found in Study 2, people who believed more in conspiracy theories were also more likely to share COVID misinformation in their network, highlighting the risks of further spread, ρ = .46, p < .001. An exploratory analysis reported in supplementary materials showed that, as in Study 2, non‐believers discriminated better than conspiracy believers between the different types of news; conspiracy believers were more likely to share both real of false information compared to non‐believers.
Conspiracy theory beliefs were correlated with five sociodemographic characteristics. Conspiracy beliefs were negatively related with age (ρ = ‐.11, p = .036), education (ρ = ‐.11, p = .031), and using the national broadcaster (BBC) as a news source (ρ = ‐.16, p = .001) and positively related with conservatism (ρ = .23, p < .001), belonging to an ethnic minority group (ρ = .14, p = .006), as well as self‐identifying as a key worker (ρ = .14, p = .003). 3 The full correlation table is available in supplementary materials (Table SM4).
4.2.2. Levels of personal control in health protective behaviours
As expected, participants felt that some behaviours were under their control, giving them more autonomy, while others were perceived as providing low levels of control (see Table 6). A large majority rated the basic and advanced behaviours as giving personal control, whereas the diagnostic test, the antibodies test, and the vaccination were deemed outside of their personal control by a majority of participants. The social distancing and contact‐tracing app received mixed judgments. Perception of control was mostly not related to conspiracy beliefs—as shown in the second column of Table 6. There was only a small and positive correlation between conspiracy beliefs and perception of control for three of the six behaviours providing high levels of control, and no statistically significant correlations with perception of control for the other five behaviours (see Table 6, third column).
TABLE 6.
Proportion of participants who judged protective behaviours as under their control and correlation with conspiracy beliefs
| Correlation with conspiracy beliefs (Spearman ρ) | |||||
|---|---|---|---|---|---|
| Uptake M (SD) | control (% yes) | Control (0/1) | Utility | Behaviour uptake/intention | |
| High in control | |||||
| Hand‐washing (1‐4; n = 396) | 3.63 (0.74) | 99% | .06 | −.16** | .02 |
| Staying home (1‐4; n = 382) | 3.73 (0.55) | 96% | .07 | −.01 | .03 |
| Face masks (1‐4; n = 334) | 1.47 (0.95) | 92% | .10* | −.03 | .14** |
| Gloves (1‐4; n = 336) | 1.55 (0.95) | 93% | .13* | −.10* | .11* |
| Washing groceries (1‐4; n = 349) | 1.69 (1.69) | 94% | .13* | −.01 | .05 |
| Stockpiling (1‐4; n = 399) | 2.74 (0.99) | 87% | .08 | −.01 | −.04 |
| Mixed perception of control | |||||
| Social distance (1‐4; n = 368) | 3.63 (0.58) | 63% | −.00 | −.14** | −.07 |
| Contact tracing app (1‐5; n = 399) | 3.55 (1.30) | .60% | .08 | −.10* | −.13** |
| Low in control | |||||
| Diagnostic test (1‐5; n = 399) | 4.28 (0.92) | .25% | −.02 | −.18*** | −.20*** |
| Antibodies test (1‐5; n = 399) | 4.16 (1.07) | .24% | −.05 | −.19*** | −.26*** |
| Vaccination (1‐5; n = 399) | 3.55 (1.30) | .24% | −.05 | −.29*** | −.33*** |
Note: * p < .05, ** p < .01, *** p < .001. The proportion of judgments that the behaviours were under one's control were all significantly greater than 50% for the high and mixed control behaviours (binomial test p < .005), and lower than 50% for the low control behaviours.
4.2.3. Conspiracy beliefs and health protective behaviours
Conspiracy belief was statistically correlated with six out of eleven of the health protective behaviours measured: wearing a face‐mask, wearing gloves, the intention to instal the contact tracing app of the NHS, the intention to get a diagnostic test, the intention to get an antibodies test, and the intention to be vaccinated against Covid‐19 (see the behaviour uptake column in Table 6). The pattern of results was consistent with our expectation that COVID‐19 conspiracy believers would perform as much or even more of the behaviours that afforded them some control and less of the behaviours that did not. For both social distancing and using the contact‐tracing app, which showed mixed perceptions of controllability, the relationship was negative but only statistically significant for the contact‐tracing app.
4.2.4. Utility perception of health protective behaviours
To showcase the role of control, we compared the average utility and uptake of the behaviours deemed under personal control and those deemed outside of personal control. As shown in Figure 5, we found that on average the utility of the protective behaviours deemed controllable had a more positive balance of risks and benefits and a greater uptake, compared to low control behaviours. When we assessed the effect of control on utility together with whether participants believed in at least one conspiracy theory or not in a variance analysis, 4 we found a clear interaction effect indicating that for conspiracy theory believers, the gap in the average utility as a function of control was larger than for non‐conspiracy believers, F interaction(1, 397) = 30.92, p < .001, η2 p = .07. In this analysis, whether the behaviours provided personal control or not and whether people believed in conspiracy beliefs or not both also had a main effect on utility perception, F(1, 397) = 61.60, p < .001, η2 p = .13, F(1, 397) = 41.27, p < .001, η2 p = .09.
FIGURE 5.
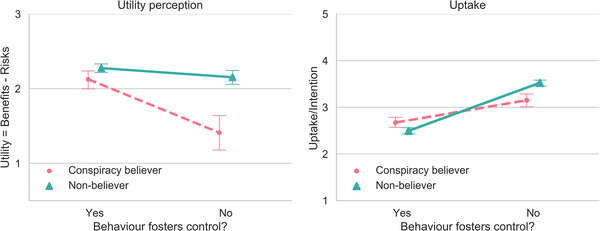
Perceived utility for (balance of risks and benefits) and uptake of behaviours that foster personal control or not as a function of conspiracy belief
Note: Behaviours that foster control included handwashing, staying home, wearing a mask, wearing gloves, and stockpiling. Behaviours that did not foster control included antibodies testing, diagnostic testing, and vaccinations
A correlational analysis between conspiracy beliefs and utility perceptions for each behaviour provided a more detailed description of the overall effect. As shown in Table 6 in the utility column, conspiracy beliefs were negatively related to the utility perception of all of the low or mixed control behaviours, but were not statistically significantly correlated with most of the behaviours that gave a strong sense of personal control: four out of six behaviours were not statistically significantly correlated with conspiracy beliefs.
4.2.5. Can utility perception explain the behaviours of conspiracy believers?
Clearly, conspiracy believers are more sceptical about the utility of some health protective behaviours compared to non‐believers, especially those that did not provide personal control. Could this difference in utility perception explain away the predictive power of conspiracy belief on people's behaviour? We tested this possibility in a hierarchical regression analysis (see Table 7). The analyses showed that the perceived utility of the protective behaviours explained some of the predictive value of conspiracy belief for the four behaviours that did not afford participants a clear sense of control: the contact tracing app, the diagnostic test, the antibodies test, and the vaccination—and for two of those behaviours, the predictive value of conspiracy theory beliefs became statistically not significant (see Step 2, Table 7). For controllable behaviours, gloves and face‐masks, the positive relationship between conspiracy beliefs and behaviour remained similar and statistically significant after we controlled for utility perception and sociodemographic characteristics. Across models, adding the sociodemographic characteristics associated with conspiracy beliefs to the models did not change the pattern of results.
TABLE 7.
To what extent does conspiracy theory belief predict behaviour uptake, without and with control for the balance of risks and benefits (standardised regression coefficient Beta)
| Advanced health behaviour fostering high control | Low control health behaviours | |||||
|---|---|---|---|---|---|---|
| Face masks | Gloves | Contact tracing | Diag. test | Antib. test | Vaccine | |
| Step 1 | ||||||
| Conspiracy | .17** | .14* | −.12* | −.16** | −.24*** | −.33*** |
| Step 2 | ||||||
| Conspiracy | .19*** | .19*** | −.02 | −.05 | −.13** | −.12* |
| Risks/benefits | .28*** | .40*** | .74*** | .44*** | .45*** | .59*** |
| R2 change | .08*** | .16*** | .55*** | .18*** | .19*** | .31*** |
| Step 3 | ||||||
| Conspiracy | .18** | .17** | .00 | −.02 | −.10* | −.09 |
| Risks/benefits | .24*** | .40*** | .73*** | .43*** | .44*** | .58*** |
| Age | −.02 | −.07 | .06 | .05 | .06 | .08 |
| Ethnicity | .22*** | .03 | −.03 | −.11* | −.11* | −.04 |
| Education | −.01 | −.03 | .01 | .02 | −.06 | .01 |
| BBC | .05 | .02 | .06 | .02 | .04 | .01 |
| Keyworker | .01 | −.02 | −.04 | −.02 | .04 | −.03 |
| Conservatism | −.05 | .06 | −.02 | −.03 | −.04 | −.04 |
| R2 change | .05** | .01 | .01 | .01 | .02 | .01 |
Note: we only included here the behaviours that were correlated with conspiracy beliefs, in an attempt to explain those. For the contact tracing app, the regression model also included the interaction conspiracy belief * control as a predictor variable but it was not statistically significant, Beta = –.03 for Step 2, and –.04 for Step 3.
*p < .05, **p < .01, ***p < .001
4.3. Discussion
Results confirmed that conspiracy theory believers were reluctant to undertake actions for which they had lower levels of personal control, and they felt these actions were riskier and less beneficial. This highlights that the involvement of others could be perceived as a threat and echoes results linking conspiracy theory beliefs with interpersonal distrust (Goertzel, 1994) and paranoid tendencies (Goreis & Voracek, 2019; Imhoff & Lamberty, 2018). By contrast, conspiracy theory believers showed no difference from non‐believers in performing health protective behaviours over which they had control.
5. DISCUSSION
At the beginning and during the peak of the first wave of the COVID‐19 pandemic in the UK, around one third of the people surveyed believed in at least one COVID‐19 conspiracy. In three studies, we consistently found that people who believed in conspiracy theories were not less likely to follow classic public health guidance to mitigate the spread of COVID‐19 compared to non‐believers. Conspiracy believers were even more likely to follow some advanced health protective behaviours, such as wearing masks or gloves, at a time when these were not officially recommended. However, conspiracy believers reported a reluctance to undertake health behaviours over which they did not have personal control, such as taking COVID‐19 diagnostic or antibodies tests, being vaccinated, and using the contact tracing application, judging these as more risky and less beneficial than non‐believers. We identified a triad of psychological antecedents to conspiracy theory beliefs: conspiracy mind‐set, trust in governmental institutions, and analytical thinking and specific sociodemographic characteristics linked with conspiracy beliefs, but those did not explain away why conspiracy theory believers were more reluctant to undertake some health protective behaviours.
5.1. Conspiracy theory beliefs and how they spread
We found that COVID‐19 conspiracy beliefs were fairly prevalent and stable over time in the UK population. We also found, as in past research (Allington et al., 2020), that some conspiracy theories were more likely to be endorsed than others, with, for example, the belief that the virus is a weapon engineered by China more prevalent than the belief that the 5G network is used to spread the illness. This prevalence estimate deserves cautious interpretation since our samples came from an online panel (Prolific) that tends to be biased towards younger, more liberal, and more educated individuals than the general population (Gosling & Mason, 2015). However, larger‐scale surveys with quota representative sampling found a similar level of endorsement (Freeman et al., 2020). Relying on an online sample can also be considered as appropriate to study conspiracy theories as those mostly spread online. Incidentally, social media users, who are particularly exposed to conspiracy theories and therefore more likely to endorse them, share similar socio‐demographics as our sample: younger, more educated and more liberal than the general population (Mellon & Prosser, 2017).
Echoing recent findings, we found that the prevalence of conspiracy beliefs varied across segments of the population, being more common in people with a conservative ideology (Bruder et al., 2013), individuals from ethnic minorities (van Prooijen et al., 2018), and those with lower formal education attainment (Lobato et al., 2014; van Prooijen, 2017). An addition to this list was that, being a frontline worker was associated with believing in conspiracy theories in two studies out of three. These trends highlight some potential vulnerability factors and could help to scope interventions to curb the infodemic. The increased prevalence of conspiracy theories in frontline workers and individuals from ethnic minorities may explain the greater hesitancy to be vaccinated against COVID‐19 observed in both of those groups (Martin et al., 2021). Similar links have been shown in the past where people from ethnic minorities were more likely to endorse conspiracy theories and less likely to get vaccinated against the flu (Quinn et al., 2017). It is important to work with vaccine hesitant groups with “engagement, understanding, and trust” (Razai et al., 2021), and it is especially important for key workers and individuals from ethnic minorities to be vaccinated because they might have a greater risk of contracting COVID‐19 (Martin et al., 2020) with, in addition, a heightened risk of clinical complications for specific ethnic groups (Sze et al., 2020).
Our results show that people who believe in conspiracy theories disseminate those beliefs: They were more likely to share COVID‐19 misinformation than non‐believers. In fact, those who believed in conspiracy theories reported a greater likelihood to share news in general, both real and fake, without distinguishing between the two. Sharing misinformation is likely to “contaminate” receivers since the mere exposure to (false) information increases its perceived veracity (Fazio et al., 2015; Hasher et al., 1977; Pennycook et al., 2018). Exposure to conspiracy views increases the perception that they are true (Béna et al., 2019) and may even change subsequent behaviours so it is essential to slow their spread. For example, exposure to climate change conspiracy theories reduced science acceptance and pro‐environmental behaviours (van der Linden, 2015).
5.2. Socio‐cognitive psychological antecedents of beliefs in COVID‐19 conspiracy theories
Conspiracy theory beliefs seem to be fuelled by a foundational set of beliefs assuming that governments are maleficent and that there exist small international organisations that control the world order, covering‐up critical events and controlling information (Brotherton et al., 2013). Our results highlight in particular the role of trust in government institutions: people who express lower trust in governments were more likely to believe in COVID‐19 conspiracy theories—believing that the crisis was intentionally caused for nefarious purposes. This is consistent with past work showing a connection between different facets of trust and conspiracy theory beliefs (Goertzel, 1994; Jasinskaja‐Lahti & Jetten, 2019; Mattocks et al., 2017; Pierre, 2020) and replicates recent work conduct on COVID‐19 conspiracy theories (Freeman et al., 2020; Pummerer et al., 2021). Interpersonal trust more generally could also play a role in conspiracy beliefs and adherence to health protective behaviours, albeit slightly differently from trust in government, since individuals scoring low in interpersonal trust would be more likely to consider people in general, as a threat (e.g., neighbours) rather than specific groups (e.g., health professionals). We could therefore expect interpersonal trust to be associated with a greater compliance with autonomous health behaviours (e.g., wearing masks) and a lower compliance with behaviours involving cooperation with others, even when they are not health professionals (e.g., social distancing). Future research could test the role of different facets of trust—in government, in people in general, and in healthcare professionals. While we could expect all of these to be negatively related to conspiracy theory belief, they may have a different connection with adherence to health protective behaviours. Research focusing on how to restore trust between conspiracy theory believers and expert figures could also make a strong contribution to the field. For instance, in our study, all the behaviours that required the involvement of others concerned health professionals, thereby creating a possible confound: conspiracy believers could have been reluctant to interact with healthcare professionals. It also seems paramount that pharmaceutical companies signal their trustworthiness more clearly, for example, by adopting more transparent data sharing practices to foster trust (Warren et al., 2020). Indeed, we are seeing the fragility of this trust play out in the current European resistance to the Oxford‐AstraZeneca vaccine, with a number of countries suspending the use of this vaccine, partly due to reporting errors in clinical trials (Bendix, 2021), and reports of rare severe side effects (Smith, 2021). Trust, especially in vaccines, requires transparent testing practices and honest reporting.
While it is difficult to ascertain whether trust causes belief in conspiracy theories or the other way around, some cognitive characteristics can be more clearly seen as having a directional and causal effect—and therefore explaining why people endorse conspiracy theory beliefs. Our findings support previous research by highlighting the role of analytical thinking (vs. intuition) in the development of conspiracy theory beliefs (Čavojová et al., 2020; Denovan et al., 2020; Fuhrer & Cova, 2020; Georgiou et al., 2019; Ståhl & van Prooijen, 2018; van der Wal et al., 2018). This link is important because it suggests a route to help people resist false information: prompting analytical thinking could help people recognise correct information and fend off conspiracy theories (Pennycook et al., 2020) and increase the sharing of information from reliable sources (Mosleh et al., 2021). Overall, our findings support the view that both social (e.g., trust) and cognitive (e.g., analytical thinking) factors are linked with the endorsement of new conspiracy theories. Our findings suggest that a two‐pronged approach, aimed at capitalising on trusted sources of information and triggering analytical evaluations of evidence, is likely to be needed to tackle the spread of conspiracy theories.
5.3. Behaviours associated with conspiracy theory beliefs: are conspiracy believers careless or careful?
It is important to note here that, consistent with recent evidence (Moussaoui et al., 2020), UK residents who took part in our studies largely reported following government health guidelines, such as staying home and social distancing, and we observed more variability in more advanced health behaviours (e.g., wearing gloves) or recently introduced behaviours (e.g., being tested/vaccinated). Building on past research on conspiracy beliefs and health behaviours, we expected that conspiracy believers would be less likely to follow public health recommendations, but our results showed a different picture. In contrast, we consistently found that believing in conspiracy theories did not reduce the adoption of basic health protective measures either before or after they were formally enforced by the government. Across more than one thousand respondents, our results showed that conspiracy believers were equally as likely to social distance and stay at home as non‐believers. They were even extra cautious and more likely to adopt advanced health protective behaviours that were controversial at the time (e.g., wearing gloves and face‐masks). These findings are at odds with some of the recent research conducted in the UK showing that conspiracy beliefs were negatively related to the adoption of basic health protective behaviours (Allington et al., 2020; Freeman et al., 2020; Swami & Barron, 2020; but see also Fuhrer & Cova, 2020 for opposite results), but are in line with findings showing that the conspiracy theories that acknowledge the existence of the virus were not connected with the adoption of basic health behaviours (Imhoff & Lamberty, 2020). A similar lack of connection was found in research focusing on AIDS—where several studies failed to find a link between beliefs in HIV conspiracy theories and lower protective behaviours (Westergaard et al., 2014) and some studies even found a positive link (e.g., with HIV testing; Ford et al., 2013). Those studies—like ours—focused on conspiracy theories that recognise the existence of the virus and not on conspiracy theories that deny its existence, for which those beliefs seem consistently connected to lower compliance with health protective behaviours.
Apparently in contradiction with the idea that conspiracy believers are equally cautious as others, conspiracy believers reported lower intentions to be tested and vaccinated. This is in line with recent findings on COVID‐19 conspiracy theories and COVID‐19 vaccination (Allington et al., 2020; Freeman et al., 2020; Meuer & Imhoff, 2021; see also van Mulukom et al., 2020 for a review of evidence) and more generally on medical conspiracy theories and vaccines (Jolley & Douglas, 2014; Jolley & Douglas, 2017; Oliver & Wood, 2014). Here we extend these findings by showing that this resistance applies to a range of medical interventions critical to controlling the spread of contagious illnesses—such as diagnostic and antibodies testing and using a contact‐tracing application. The explanation for this reluctance does not seem to be a mere negative reaction to official recommendations. Indeed, findings from Study 3 suggest that this is rooted in the precise belief that those procedures can be dangerous, possibly because they cannot be performed autonomously and depend on an external agent (in this case, healthcare professionals who may have insidious motives according to conspiracy believers).
Overall, the literature on health conspiracy theories and health protective behaviours shows that the link between conspiracy belief and health protective behaviours is contradictory depending on the nature of the conspiracy theory and the nature of the behaviour. Often, conspiracy believers are presented as risk‐taking individuals who refuse to follow official health recommendations (Allington et al., 2020), but here we provide evidence that this is not the case. Conspiracy believers seem to endorse as much, or even more, the protective behaviours that afford them a sense of personal control, whereas they are reluctant to undertake the behaviours that offer low levels of control and autonomy, because they are perceived as risky. The misalignment of conspiracy believers with (some) public health measures should therefore not be interpreted as recklessness or negligence towards their own health, but rather as a failure to adequately communicate the risks and benefits of those procedures. Developing communications tailored to speak more inclusively to conspiracy believers is imperative to increase the uptake of testing and vaccination.
5.4. Limitations
While we focused on several meaningful antecedents, there was still unexplained variance in conspiracy theory beliefs and health protective behaviours. Future research may include other factors known to predict conspiracy theory beliefs such as personality traits (e.g., the dark triad) (Nowak et al., 2020), and clinical or social measures (e.g., sense of social integration) (Stoica & Umbreș, 2020).
5.5. Applied implications
We draw three practical implications from our findings. First, our results suggest that lower trust in government could fuel conspiracy beliefs and the reluctance to undertake important health protective behaviours, such as being tested or vaccinated. Therefore, creating health messages that are delivered by trusted sources could increase adherence to testing and vaccination. Information coming from trusted (rather than less trusted) sources is more influential (Thorpe et al., 2020). Second, we found that conspiracy believers undertook behaviours that they could accomplish on their own and had control over in equal measure to non‐believers, and therefore, could be more open to autonomy‐supportive health advice. For example, using autonomy‐supportive messages to invite health care professionals for a flu shot has been effective in reducing vaccine hesitancy (Moon et al., 2021). Third, our findings offer insights into how to fight online misinformation, with evidence highlighting the role of analytical thinking in keeping conspiracy beliefs at bay, supporting recent findings showing that nudging people to be analytical helps them to differentiate between real and false information (Pennycook et al., 2020). Some health messages are difficult to understand well (Holford et al., 2021), which might fuel ill‐informed decisions and health inequalities. Designing simpler and clearer messages is essential to being inclusive and supporting a greater number of citizens to make more informed decisions.
6. CONCLUSION
In three studies, we found that COVID‐19 conspiracy believers followed most basic health guidelines and some advanced health protective measures as strictly as non‐believers, but they were less likely to adopt a number of health behaviours that they could not perform independently, such being tested for and vaccinated against COVID‐19. This negative link between conspiracy beliefs and health protective behaviours was not explained away by the socio‐psychological characteristics associated with COVID‐19 conspiracy beliefs, but seemed driven by the perception that they were less beneficial and more risky.
Supporting information
Supplementary information
Juanchich Marie, Sirota Miroslav, Jolles Daniel, Whiley Lilith A.. Are COVID‐19 conspiracies a threat to public health? Psychological characteristics and health protective behaviours of believers. European Journal of Social Psychology. 2021;51:969–989. 10.1002/ejsp.2796
NOTES
Being part of an ethnic minority was defined broadly as not belonging to the White British majority, which accounted for 16% of the participants (vs. 84% White British). Being a frontline worker was defined as any individuals who work in their “normal” workplace, which is not home, and those represented 22% of the participants.
Overall 26% of our participants were categorised as belonging to an ethnic minority (vs. White British). For the conservative political parties, we summed participants who reported being affiliated with UKIP or the Conservative Party, which accounted for 31% of the participants. Finally, most participants reported using the BBC (app/radio/TV) as news source, with 79% of the participants. Education was a continuous measure ranging from no formal education to PhD education level.
78% used BBC as news source; 18% belonged to an ethnic minority (defined as not White British) and 21% reported being Conservative/UKIP (21%).
The variance analysis was deemed preferable to the preregistered regression analysis to better accompany the differences shown in the graphical display than a regression analysis in this context.
DATA AVAILABILITY STATEMENT
The preregistration, materials and data for the three studies reported here are openly available in Open Science Framework at https://osf.io/ujsrc/?view_only=820fda53fc28401092a498766cea2ec1
REFERENCES
- Allington, D. , Duffy, B. , Wessely, S. , Dhavan, N. , & Rubin, J. (2020). Health‐protective behaviour, social media usage and conspiracy belief during the COVID‐19 public health emergency. Psychological Medicine, 1–7. 10.1017/S003329172000224X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Béna, J. , Carreras, O. , & Terrier, P. (2019, October 2). On Believing Conspiracy Theories We Remember: Analyses of Two Large‐Scale Surveys of Conspiracism in the French General Public. 10.31234/osf.io/tf76n. [DOI]
- Bendix, A. (2021). AstraZeneca's missteps and murky data sowed worldwide confusion that undermined trust—but don't rule the shot out yet. Insider, https://www.businessinsider.com/astrazeneca‐vaccine‐mistakes‐confusing‐data‐eroded‐trust‐2021‐2?r=US&IR=T. Published online February 11, 2021. [Google Scholar]
- Bertin, P. , Nera, K. , & Delouvée, S. (2020). Conspiracy beliefs, rejection of vaccination, and support for hydroxychloroquine: A conceptual replication‐extension in the COVID‐19 pandemic context. Frontiers in Psychology, 11, 565128. 10.3389/fpsyg.2020.565128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Biddlestone, M. , Green, R. , & Douglas, K. M. (2020). Cultural orientation, power, belief in conspiracy theories, and intentions to reduce the spread of COVID‐19. British Journal of Social Psychology, 59(3), 663–673. 10.1111/bjso.12397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brotherton, R. , French, C. , & Pickering, A. (2013). Measuring belief in conspiracy theories: The generic conspiracist beliefs scale. Frontiers in Psychology, 4(279). 10.3389/fpsyg.2013.00279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bruder, M. , Haffke, P. , Neave, N. , Nouripanah, N. , & Imhoff, R. (2013). Measuring individual differences in generic beliefs in conspiracy theories across cultures: Conspiracy mentality questionnaire. Frontiers in Psychology, 4(225),. 10.3389/fpsyg.2013.00225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bursztyn, L. , Rao, A. , Roth, C. , & Yanagizawa‐Drott, D. (2020). Misinformation During a Pandemic. University of Chicago, Becker Friedman Institute for Economics Working Paper 2020–44 . https://ssrn.com/abstract=3580487
- Čavojová, V. , Šrol, J. , & Ballová Mikušková, E. (2020). How scientific reasoning correlates with health‐related beliefs and behaviors during the COVID‐19 pandemic? Journal of health psychology, 0(0), 1359105320962266. 10.1177/1359105320962266. [DOI] [PubMed] [Google Scholar]
- Čavojová, V. , Šrol, J. , & Jurkovič, M. (2020). Why should we try to think like scientists? Scientific reasoning and susceptibility to epistemically suspect beliefs and cognitive biases. Applied Cognitive Psychology, 34(1), 85–95. [Google Scholar]
- Craciun, C. , & Baban, A. (2012). Who will take the blame?”: Understanding the reasons why Romanian mothers decline HPV vaccination for their daughters. Vaccine, 30(48), 6789–6793. 10.1016/j.vaccine.2012.09.016 [DOI] [PubMed] [Google Scholar]
- Dagnall, N. , Drinkwater, K. , Parker, A. , Denovan, A. , & Parton, M. (2015). Conspiracy theory and cognitive style: A worldview [Original Research]. Frontiers in Psychology, 6(206). 10.3389/fpsyg.2015.00206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Neys, W. , & Pennycook, G. (2019). Logic, fast and slow: Advances in dual‐process theorizing. Current Directions in Psychological Science, 28(5), 503–509. 10.1177/0963721419855658 [DOI] [Google Scholar]
- Douglas, K. M. , Sutton, R. M. , Callan, M. J. , Dawtry, R. J. , & Harvey, A. J. (2016). Someone is pulling the strings: Hypersensitive agency detection and belief in conspiracy theories. Thinking & Reasoning, 22(1), 57–77. 10.1080/13546783.2015.1051586 [DOI] [Google Scholar]
- Epstein, S. , Pacini, R. , Denes‐Raj, V. , & Heier, H. (1996). Individual differences in intuitive‐experiential and analytical‐rational thinking styles. Journal of Personality and Social Psychology, 71, 390–405. 10.1037/0022-3514.71.2.390 [DOI] [PubMed] [Google Scholar]
- Evans, J. S. , & Stanovich, K. E. (2013). Dual‐process theories of higher cognition: Advancing the debate. Perspectives on Psychological Science, 8(3), 223–241. 10.1177/1745691612460685 [DOI] [PubMed] [Google Scholar]
- Fazio, L. K. , Brashier, N. M. , Payne, B. K. , & Marsh, E. J. (2015). Knowledge does not protect against illusory truth. Journal of Experimental Psychology: General, 144(5), 993–1002. 10.1037/xge0000098 [DOI] [PubMed] [Google Scholar]
- Ford, C. L. , Wallace, S. P. , Newman, P. A. , Lee, S.‐J. , & Cunningham, W. E. (2013). Belief in AIDS‐related conspiracy theories and mistrust in the government: Relationship with HIV testing among at‐risk older adults. The Gerontologist, 53(6), 973–984. 10.1093/geront/gns192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frederick, S. (2005). Cognitive reflection and decision making. Journal of Economic Perspectives, 19(4), 25–42. 10.1257/089533005775196732 [DOI] [Google Scholar]
- Freeman, D. , Waite, F. , Rosebrock, L. , Petit, A. , Causier, C. , East, A. , Jenner, L. , Teale, A.‐L. , Carr, L. , Mulhall, S. , Bold, E. , & Lambe, S. (2020). Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psychological Medicine, 1–13. 10.1017/S0033291720001890 ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fuhrer, J. , & Cova, F. (2020). “Quick and dirty”: Intuitive cognitive style predicts trust in Didier Raoult and his hydroxychloroquine‐based treatment against COVID‐19. Judgment and Decision Making, 15(6), 889–908. [Google Scholar]
- Georgiou, N. , Delfabbro, P. , & Balzan, R. (2019). Conspiracy beliefs in the general population: The importance of psychopathology, cognitive style and educational attainment. Personality and Individual Differences, 151, 109521. 10.1016/j.paid.2019.109521. [DOI] [Google Scholar]
- Goertzel, T. (1994). Belief in conspiracy theories. Political Psychology, 15(4), 731–742. 10.2307/3791630 [DOI] [Google Scholar]
- Goreis, A. , & Voracek, M. (2019). A Systematic Review and Meta‐Analysis of Psychological Research on Conspiracy Beliefs: Field Characteristics, Measurement Instruments, and Associations With Personality Traits. Frontiers in Psychology, 10(205). 10.3389/fpsyg.2019.00205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gosling, S. D. , & Mason, W. (2015). Internet research in psychology. Annual Review of Psychology, 66(1), 877–902. 10.1146/annurev-psych-010814-015321 [DOI] [PubMed] [Google Scholar]
- Grebe, E. , & Nattrass, N. (2012). AIDS conspiracy beliefs and unsafe sex in Cape Town. Journal of Acquired Immune Deficiency Syndromes, 16(3), 761–773. [DOI] [PubMed] [Google Scholar]
- Grimmelikhuijsen, S. , & Knies, E. (2017). Validating a scale for citizen trust in government organizations. International Review of Administrative Sciences, 83(3), 583–601. 10.1177/0020852315585950 [DOI] [Google Scholar]
- Hasher, L. , Goldstein, D. , & Toppino, T. (1977). Frequency and the conference of referential validity. Journal of Verbal Learning and Verbal Behavior, 16(1), 107–112. 10.1016/S0022-5371(77)80012-1 [DOI] [Google Scholar]
- Holford, D. L. , Juanchich, M. , & Sirota, M. (2021). Ambiguity and unintended inferences about risk messages for COVID‐19. Journal of Experimental Psychology: Applied. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hornsey, M. J. , Harris, E. A. , & Fielding, K. S. (2018). The psychological roots of anti‐vaccination attitudes: A 24‐nation investigation. Health Psychology, 37(4), 307–315. 10.1037/hea0000586 [DOI] [PubMed] [Google Scholar]
- Imhoff, R. , & Bruder, M. (2014). Speaking (un‐) truth to power: Conspiracy mentality as a generalised political attitude. European Journal of Personality, 28(1), 25–43. 10.1002/per.1930 [DOI] [Google Scholar]
- Imhoff, R. , & Lamberty, P. (2018). How paranoid are conspiracy believers? Toward a more fine‐grained understanding of the connect and disconnect between paranoia and belief in conspiracy theories, 48(7), 909–926. 10.1002/ejsp.2494 [DOI] [Google Scholar]
- Imhoff, R. , & Lamberty, P. (2020). A Bioweapon or a Hoax? The link between distinct conspiracy beliefs about the coronavirus disease (COVID‐19) Outbreak and Pandemic Behavior. Social Psychological and Personality Science, 11(8), 1110–1118. 10.1177/1948550620934692 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jasinskaja‐Lahti, I. , & Jetten, J. (2019). Unpacking the relationship between religiosity and conspiracy beliefs in Australia. British Journal of Social Psychology, 58(4), 938–954. 10.1111/bjso.12314 [DOI] [PubMed] [Google Scholar]
- Jolley, D. , & Douglas, K. M. (2014). The effects of anti‐vaccine conspiracy theories on vaccination intentions. Plos One, 9(2), e89177. 10.1371/journal.pone.0089177 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jolley, D. , & Douglas, K. M. (2017). Prevention is better than cure: Addressing anti‐vaccine conspiracy theories. Journal of Applied Psychology, 47(8), 459–469. 10.1111/jasp.12453 [DOI] [Google Scholar]
- Juanchich, M. , Dewberry, C. , Sirota, M. , & Narendran, S. (2016). Cognitive reflection predicts real‐life decision outcomes, but not over and above personality and decision‐making styles. Journal of Behavioral Decision‐Making, 29, 52–59. 10.1002/bdm.1875 [DOI] [Google Scholar]
- Kata, A. (2012). Anti‐vaccine activists, Web 2.0, and the postmodern paradigm: An overview of tactics and tropes used online by the anti‐vaccination movement. Vaccine, 30(25), 3778–3789. 10.1016/j.vaccine.2011.11.112 [DOI] [PubMed] [Google Scholar]
- Kim, M. , & Cao, X. (2016). The impact of exposure to media messages promoting government conspiracy theories on distrust in the government: Evidence from a two‐stage randomized experiment. International Journal of Communication, 10, 3808–3827. [Google Scholar]
- Klofstad, C. A. , Uscinski, J. E. , Connolly, J. M. , & West, J. P. (2019). What drives people to believe in Zika conspiracy theories? Palgrave Communications, 5(1), 36. 10.1057/s41599-019-0243-8 [DOI] [Google Scholar]
- Lamberty, P. , & Imhoff, R. (2018). Powerful pharma and its marginalized alternatives? Effects of individual differences in conspiracy mentality on attitudes toward medical approaches. Social Psychology, 49(5), 255–270. 10.1027/1864-9335/a000347 [DOI] [Google Scholar]
- Larson, H. J. , Hartigan‐Go, K. , & de Figueiredo, A. (2019). Vaccine confidence plummets in the Philippines following dengue vaccine scare: Why it matters to pandemic preparedness. Human Vaccines & Immunotherapeutics, 15(3), 625–627. 10.1080/21645515.2018.1522468 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lobato, E. , Mendoza, J. , Sims, V. , & Chin, M. (2014). Examining the relationship between conspiracy theories, paranormal beliefs, and pseudoscience acceptance among a university population. 28(5), 617–625. 10.1002/acp.3042 [DOI] [Google Scholar]
- Martin, C. A. , Jenkins, D. R. , Minhas, J. S. , Gray, L. J. , Tang, J. , Williams, C. , Sze, S. , Pan, D. , Jones, W. , Verma, R. , Knapp, S. , Major, R. , Davies, M. , Brunskill, N. , Wiselka, M. , Brightling, C. , Khunti, K. , Haldar, P. , & Pareek, M. (2020). Socio‐demographic heterogeneity in the prevalence of COVID‐19 during lockdown is associated with ethnicity and household size: Results from an observational cohort study. EClinicalMedicine, 25, 100466. 10.1016/j.eclinm.2020.100466 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin, C. A. , Marshall, C. , Patel, P. , Goss, C. , Jenkins, D. R. , Ellwood, C. , Barton, L. , Price, A. , Brunskill, N. J. , Khunti, K. , & Pareek, M. (2021). Association of demographic and occupational factors with SARS‐CoV‐2 vaccine uptake in a multi‐ethnic UK healthcare workforce: A rapid real‐world analysis. medRxiv, 2021.2002.2011.21251548. 10.1101/2021.02.11.21251548 medRxiv [DOI] [Google Scholar]
- Mattocks, K. M. , Gibert, C. , Fiellin, D. , Fiellin, L. E. , Jamison, A. , Brown, A. , & Justice, A. C. (2017). Mistrust and endorsement of human immunodeficiency virus conspiracy theories among human immunodeficiency virus–infected African American veterans. Military Medicine, 182(11–12), e2073–e2079. 10.7205/MILMED-D-17-00078%J [DOI] [PubMed] [Google Scholar]
- McDowell, M. , Rebitschek, F. G. , Gigerenzer, G. , & Wegwarth, O. (2016). A simple tool for communicating the benefits and harms of health interventions: A guide for creating a fact box. Medical Decision Making Policy & Practice, 1(1), 2381468316665365. 10.1177/2381468316665365 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mellon, J. , & Prosser, C. (2017). Twitter and Facebook are not representative of the general population: Political attitudes and demographics of British social media users. Research & Politics, 4(3), 2053168017720008. 10.1177/2053168017720008 [DOI] [Google Scholar]
- Meuer, M. , & Imhoff, R. (2021). Believing in hidden plots is associated with decreased behavioral trust: Conspiracy belief as greater sensitivity to social threat or insensitivity towards its absence? Journal of Experimental Social Psychology, 93, 104081. 10.1016/j.jesp.2020.104081 [DOI] [Google Scholar]
- Mian, A. , & Khan, S. (2020). Coronavirus: The spread of misinformation. BMC Medicine, 18(1), 89–90. 10.1186/s12916-020-01556-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller, J. M. (2020). Do COVID‐19 conspiracy theory beliefs form a monological belief system? Canadian Journal of Political Science, 53(2), 319–326. 10.1017/S0008423920000517 [DOI] [Google Scholar]
- Moon, K. , Riege, A. , Gourdon‐Kanhukamwe, A. , & Vallée‐Tourangeau, G. (2021). The moderating effect of autonomy on promotional health messages encouraging healthcare professionals to get the influenza vaccine. Journal of experimental Psychology: Applied, 27(2), 187–200. 10.1037/xap0000348. [DOI] [PubMed] [Google Scholar]
- Morgenstern, O. , & von Neumann, J. (1943). Theory of games and economic behavior. Princeton University Press. [Google Scholar]
- Mosleh, M. , Pennycook, G. , Arechar, A. A. , & Rand, D. G. (2021). Cognitive reflection correlates with behavior on Twitter. Nature Communications, 12(1), 921. 10.1038/s41467-020-20043-0 ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moussaoui, L. S. , Ofosu, N. D. , & Desrichard, O. (2020). Social psychological correlates of protective behaviours in the COVID‐19 Outbreak: Evidence and recommendations from a nationally representative sample. Applied Psychology: Health and Well‐Being, 12(4), 1183–1204. 10.1111/aphw.12235 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nowak, B. , Brzóska, P. , Piotrowski, J. , Sedikides, C. , Żemojtel‐Piotrowska, M. , & Jonason, P. K. (2020). Adaptive and maladaptive behavior during the COVID‐19 pandemic: The roles of Dark Triad traits, collective narcissism, and health beliefs. Personality and Individual Differences, 167, 110232. 10.1016/j.paid.2020.110232 ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oliver, J. E. , & Wood, T. (2014). Medical conspiracy theories and health behaviors in the United States. JAMA Internal Medicine, 174(5), 817–818. 10.1001/jamainternmed.2014.190%J [DOI] [PubMed] [Google Scholar]
- Pennycook, G. , Cannon, T. D. , & Rand, D. G. (2018). Prior exposure increases perceived accuracy of fake news. Journal of Experimental Psychology: General, 147(12), 1865–1880. 10.1037/xge0000465 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pennycook, G. , Cheyne, J. A. , Barr, N. , Koehler, D. J. , Fugelsang, J. A. J. J. , & making, D. (2015). On the reception and detection of pseudo‐profound bullshit. Judgment and Decision Making, 10(6), 549–563. [Google Scholar]
- Pennycook, G. , Cheyne, J. A. , Seli, P. , Koehler, D. J. , & Fugelsang, J. A. (2012). Analytic cognitive style predicts religious and paranormal belief. Cognition, 123, 335–346. 10.1016/j.cognition.2012.03.003. [DOI] [PubMed] [Google Scholar]
- Pennycook, G. , McPhetres, J. , Zhang, Y. , Lu, J. G. , & Rand, D. G. (2020). Fighting COVID‐19 misinformation on social media: Experimental evidence for a scalable accuracy‐nudge intervention. Psychological Science, 31(7), 770–780. 10.1177/0956797620939054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pennycook, G. , & Rand, D. G. (2020). Who falls for fake news? The roles of bullshit receptivity, overclaiming, familiarity, and analytic thinking. Journal of personality, 88, 185–200. 10.1111/jopy.12476 [DOI] [PubMed] [Google Scholar]
- Pierre, J. M. (2020). Mistrust and misinformation: A two‐component, socio‐epistemic model of belief in conspiracy theories. Journal of Social and Political Psychology, 8(2), 617–641. 10.5964/jspp.v8i2.1362 [DOI] [Google Scholar]
- Pummerer, L. , Böhm, R. , & Sassenberg, K. (2021). Conspiracy theories and their societal effects during the COVID‐19 pandemic. Social Psychological and Personality Science, 10.1177/19485506211000217 ] [DOI] [Google Scholar]
- Pytlik, N. , Soll, D. , & Mehl, S. (2020). Thinking preferences and conspiracy belief: Intuitive thinking and the jumping to conclusions‐bias as a basis for the belief in conspiracy theories. Frontiers in Psychiatry, 11, 987. 10.3389/fpsyt.2020.568942 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quinn, S. C. , Jamison, A. , Freimuth, V. S. , An, J. , Hancock, G. R. , & Musa, D. (2017). Exploring racial influences on flu vaccine attitudes and behavior: Results of a national survey of White and African American adults. Vaccine, 35(8), 1167–1174. 10.1016/j.vaccine.2016.12.046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Razai, M. S. , Osama, T. , McKechnie, D. G. J. , & Majeed, A. (2021). Covid‐19 vaccine hesitancy among ethnic minority groups. BMJ (Clinical Research Ed.), 372, n513. 10.1136/bmj.n513 [DOI] [PubMed] [Google Scholar]
- Romer, D. , & Jamieson, K. H. (2020). Conspiracy theories as barriers to controlling the spread of COVID‐19 in the US. Social Science & Medicine, 263, 113356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ross, M. W. , Essien, E. J. , & Torres, I. (2006). Conspiracy beliefs about the origin of HIV/AIDS in four racial/ethnic groups. Journal of Acquired Immune Deficiency Syndromes (1999), 41(3), 342–344. 10.1097/01.qai.0000209897.59384.52 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanche, S. , Lin, Y. T. , Xu, C. , Romero‐Severson, E. , Hengartner, N. , & Ke, R. (2020). High contagiousness and rapid spread of severe acute respiratory syndrome coronavirus 2. Emerging Infectious Diseases, 26(7), 1470–1477. 10.3201/eid2607.200282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Setbon, M. , & Raude, J. (2010). Factors in vaccination intention against the pandemic influenza A/H1N1. European Journal of Public Health, 20(5), 490–494. 10.1093/eurpub/ckq054%J [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sirota, M. , & Juanchich, M. (2018). Effect of response format on cognitive reflection: Validating a two‐ and four‐option multiple choice question version of the Cognitive Reflection Test. Behavior Research Methods, 50(6), 2511–2522. 10.3758/s13428-018-1029-4 [DOI] [PubMed] [Google Scholar]
- Smith, M. (2021). Europeans now see AstraZeneca vaccine as unsafe, following blood clots scare . https://yougov.co.uk/topics/international/articles-reports/2021/03/22/europeans-now-see-astrazeneca-vaccine-unsafe-follo
- Šrol, J. , Ballová Mikušková, E. , & Čavojová, V. (Preprint). (2020). When we are worried, what are we thinking? Anxiety, lack of control, and conspiracy beliefs amidst the COVID‐19 pandemic. Applied Cognitive Psychology, 35(3), 720–729. https://psyarxiv.com/f9e6p/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ståhl, T. , & van Prooijen, J.‐W. (2018). Epistemic rationality: Skepticism toward unfounded beliefs requires sufficient cognitive ability and motivation to be rational. Personality and Individual Differences, 122, 155–163. 10.1016/j.paid.2017.10.026 [DOI] [Google Scholar]
- Stein, R. A. , Ometa, O. , Pachtman Shetty, S. , Katz, A. , Popitiu, M. I. , & Brotherton, R. (2021). Conspiracy theories in the era of COVID‐19: A tale of two pandemics. International Journal of Clinical Practice, 75(2), e13778. 10.1111/ijcp.13778 ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stoica, C. A. ,& Umbreș, R. (2020). Suspicious minds in times of crisis: Determinants of Romanians’ beliefs in COVID‐19 conspiracy theories. European Societies, 23(sup1), S246–S261. 10.1080/14616696.2020.1823450] [DOI] [Google Scholar]
- Sunstein, C. R. , & Vermeule, A. (2009). Conspiracy Theories: Causes and Cures, 17(2), 202–227. 10.1111/j.1467-9760.2008.00325.x [DOI] [Google Scholar]
- Swami, V. & Barron, D. (2020). Analytic thinking, rejection of coronavirus (COVID‐19) conspiracy theories, and compliance with mandated social‐distancing: Direct and indirect relationships in a nationally representative sample of adults in the United Kingdom.
- Swami, V. , Coles, R. , Stieger, S. , Pietschnig, J. , Furnham, A. , Rehim, S. , & Voracek, M. (2011). Conspiracist ideation in Britain and Austria: Evidence of a monological belief system and associations between individual psychological differences and real‐world and fictitious conspiracy theories. British Journal of Psychology, 102(3), 443–463. 10.1111/j.2044-8295.2010.02004.x [DOI] [PubMed] [Google Scholar]
- Swami, V. , Voracek, M. , Stieger, S. , Tran, U. S. , & Furnham, A. (2014). Analytic thinking reduces belief in conspiracy theories. Cognition, 133(3), 572–585. 10.1016/j.cognition.2014.08.006 [DOI] [PubMed] [Google Scholar]
- Sze, S. , Pan, D. , Nevill, C. R. , Gray, L. J. , Martin, C. A. , Nazareth, J. , Minhas, J. S. , Divall, P. , Khunti, K. , & Abrams, K. R. (2020). Ethnicity and clinical outcomes in COVID‐19: A systematic Review and Meta‐analysis. EClinicalMedicine, 29, 1–17. 10.1016/j.eclinm.2020.100630 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teovanović, P. , Lukić, P. , Zupan, Z. , Lazić, A. , Ninković, M. , & Žeželj, I. (2020). Irrational beliefs differentially predict adherence to guidelines and pseudoscientific practices during the COVID‐19 pandemic. Applied Cognitive Psychology, 35(2), 486–496. 10.1002/acp.3770 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thorpe, A. , Sirota, M. , Juanchich, M. , & Orbell, S. (2020). ‘Always take your doctor's advice’: Does trust moderate the effect of information on inappropriate antibiotic prescribing expec10.1111/bjhp.12411tations? British Journal of Health Psychology, 25(2), 358–376 10.1111/bjhp.12411 [DOI] [PubMed] [Google Scholar]
- Toplak, M. E. , West, R. F. , & Stanovich, K. E. (2011). The Cognitive Reflection Test as a predictor of performance on heuristics‐and ‐biases tasks. Memory and Cognition, 39, 1275–1289. 10.3758/s13421-011-0104-1 [DOI] [PubMed] [Google Scholar]
- Toplak, M. E. , West, R. F. , & Stanovich, K. E. (2014). Assessing miserly information processing: An expansion of the Cognitive Reflection Test. Thinking & Reasoning, 20(0), 147–168. 10.1080/13546783.2013.844729. [DOI] [Google Scholar]
- van der Linden, S. (2015). The conspiracy‐effect: Exposure to conspiracy theories (about global warming) decreases pro‐social behavior and science acceptance. Personality and Individual Differences, 87, 171–173. 10.1016/j.paid.2015.07.045 [DOI] [Google Scholar]
- van der Wal, R. C. , Sutton, R. M. , Lange, J. , & Braga, J. P. N. (2018). Suspicious binds: Conspiracy thinking and tenuous perceptions of causal connections between co‐occurring and spuriously correlated events. European Journal of Social Psychology, 48(7), 970–989. 10.1002/ejsp.2507 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Mulukom, V. , Pummerer, L. , Alper, S. , Cavojova, V. , Farias, J. E. M. , Kay, C. S. , Lazarevic, L. , Lobato, E. J. C. , Marinthe, G. , & Banai, I. P. (2020). Antecedents and consequences of COVID‐19 conspiracy theories: A rapid review of the evidence. 10.31234/osf.io/u8yah [DOI] [PMC free article] [PubMed]
- van Prooijen, J.‐W. (2017). Why education predicts decreased belief in conspiracy theories. Applied Cognitive Psychology, 31(1), 50–58. 10.1002/acp.3301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Prooijen, J.‐W. , Staman, J. , & Krouwel, A. P. M. (2018). Increased conspiracy beliefs among ethnic and Muslim minorities. Applied Cognitive Psychology, 32(5), 661–667. 10.1002/acp.3442 [DOI] [Google Scholar]
- Vosoughi, S. , Roy, D. , & Aral, S. (2018). The spread of true and false news online. Science, 359, 1146–1151. 10.1126/science.aap9559 [DOI] [PubMed] [Google Scholar]
- Warren, R. C. , Forrow, L. , Hodge, D. A. , & Truog, R. D. (2020). Trustworthiness before trust: Covid‐19 vaccine trials and the Black community. New England Journal of Medicine, 383(22), e121. 10.1056/NEJMp2030033 ] [DOI] [PubMed] [Google Scholar]
- Westergaard, R. P. , Beach, M. C. , Saha, S. , & Jacobs, E. A. (2014). Racial/ethnic differences in trust in health care: HIV conspiracy beliefs and vaccine research participation. Journal of General Internal Medicine, 29(1), 140–146. 10.1007/s11606-013-2554-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organisation . (2020). WHO Director‐General's opening remarks at the media briefing on COVID‐19 ‐ 11 March 2020. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020
- World Health Organization . (2021). WHO‐convened global study of origins of SARS‐CoV‐2: China Part.
- Worldometer . (2021). Total Coronavirus Cases in the United Kingdom. Retrieved 07/06/2021 from https://www.worldometers.info/coronavirus/country/uk/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary information
Data Availability Statement
The preregistration, materials and data for the three studies reported here are openly available in Open Science Framework at https://osf.io/ujsrc/?view_only=820fda53fc28401092a498766cea2ec1