

Supplemental Digital Content is available in the text.
Key Words: health workforce, COVID-19, contact tracing, pandemic preparedness
Abstract
Background:
As coronavirus disease 2019 (COVID-19) rapidly progressed throughout the United States, increased demand for health workers required health workforce data and tools to aid planning and response at local, state, and national levels.
Objective:
We describe the development of 2 estimator tools designed to inform health workforce planning for COVID-19.
Research Design:
We estimated supply and demand for intensivists, critical care nurses, hospitalists, respiratory therapists, and pharmacists, using Institute for Health Metrics and Evaluation projections for COVID-19 hospital care and National Plan and Provider Enumeration System, Provider Enrollment Chain and Ownership System, American Hospital Association, and Bureau of Labor Statistics Occupation Employment Statistics for workforce supply. We estimated contact tracing workforce needs using Johns Hopkins University COVID-19 case counts and workload parameters based on expert advice.
Results:
The State Hospital Workforce Deficit Estimator estimated the sufficiency of state hospital-based clinicians to meet projected COVID-19 demand. The Contact Tracing Workforce Estimator calculated the workforce needed based on the 14-day COVID-19 caseload at county, state, and the national level, allowing users to adjust workload parameters to reflect local contexts.
Conclusions:
The 2 estimators illustrate the value of integrating health workforce data and analysis with pandemic response planning. The many unknowns associated with COVID-19 required tools to be flexible, allowing users to change assumptions on number of contacts and work capacity. Data limitations were a challenge for both estimators, highlighting the need to invest in health workforce data and data infrastructure as part of future emergency preparedness planning.
In March 2020, coronavirus disease 2019 (COVID-19) began a rapid spread across the United States—initially in Washington, California, and New York—followed by outbreaks across the country. As cases and hospitalizations began to overwhelm health care systems, concerns turned to the availability of intensive care unit (ICU) beds, ventilators, and the health workforce needed to meet rising COVID-19 demands. Throughout the spring, the public health response to COVID-19 evolved, and strategies initially focused on strict community mitigation turned to contact tracing, requiring significant expansion of the public health workforce.
While earlier and less severe pandemics have provided a blueprint for future scenarios, the national reach of COVID-19 has been unprecedented. Historically, much of the onus has been on individual health systems to develop surge plans in the event of a pandemic.1 Prior planning tools ranged from spreadsheets to predict hospital admissions and staffing needs to more sophisticated models used to understand the spread of disease.2–5 As new strategies emerged to meet health workforce needs, it quickly became apparent that health workforce data and tools were needed to inform coordinated local, state, and national response. The Fitzhugh Mullan Institute for Health Workforce Equity developed 2 tools to inform health workforce planning for COVID-19—the State Hospital Workforce Deficit Estimator and the Contract Tracing Workforce Estimator. We describe the 2 workforce estimators, including the data, requirements, and limitations of each tool, and the implications for effective pandemic response.
STATE HOSPITAL WORKFORCE DEFICIT ESTIMATOR
At the height of the massive outbreak in New York City in March 2020, it was unclear whether the existing health care workforce would be sufficient to care for COVID-19 patients. In addition, there was concern that the hospital workforce might temporarily or permanently decline due to workers becoming ill and possibly dying or needing to quarantine. One early estimate indicated that up to 380,000 health care workers in the United States could die from the virus.6
Several health workforce strategies emerged to meet hospital staffing requirements for COVID-19. Temporary staffing companies helped fill the initial spike in need for nurses and other clinicians in New York and other early hotspots.7 Many states moved to relax requirements to allowing recent retirees and health professionals licensed in other states to practice.8 The federal government deployed military medical personnel,9 as well as the National Disaster Medical System10 and the US Public Health Service Commissioned Corps to hotspots. However, these strategies and others, such as transitioning to surge capacity staffing, redeployment of existing health workers, and calls for volunteer retired and other workers11,12 require advanced planning and time to implement effectively.
To help states and federal actors plan for workforce needs across the country, we developed the State Hospital Workforce Deficit Estimator. The aim was to anticipate potential shortages at the state level and give them time to prepare. While various research centers endeavored to predict the course of COVID-19 cases and deaths, no other source was examining whether the hospital workforce would be adequate across the United States and at the state level. Our tool provides information on the supply of active and inactive clinicians in each state and examines the sufficiency of the workforce to meet projected COVID-19 demand.
METHODS
The State Hospital Workforce Deficit Estimator estimates whether the supply of respiratory therapists, intensivists, hospitalists, critical care nurses, and pharmacists would be sufficient to meet demand for COVID-19 care in each state. We focus on these professions since they are critical to hospital care and because supply data was available.
We utilized data from the Institute for Health Metrics and Evaluation (IHME) COVID-19 Health Care Utilization Projections to estimate the need for COVID-19 hospital care.13 IHME projections included projected COVID-19 hospitalizations as well as ICU cases. The IHME models projected lower bound, mean, and upper bound estimates to reflect uncertainty, were updated every 3−10 days, and generally projected 4−5 months out from the date of update. We also estimated demand for non-COVID-19 care based on the Medicare Hospital Cost Report, applying a 25% reduction in bed occupancy (except for ICU occupancy) to account for the cancellation of elective procedures.14
We estimated the supply of different health care professions using various datasets. For intensivists, we used the Provider Enrollment, Chain and Ownership System file as of January 2020,15 the National Plan and Provider Enumeration System registry as of March 2020,16 and the Medicare Part B public use file from 2017.17 The Provider Enrollment, Chain and Ownership System files and National Plan and Provider Enumeration System registry provided information on self-reported intensivists, which we cross-referenced with billing activity for any ICU services using the Medicare Part B public use file. We used a similar methodology to identify hospitalists. To identify respiratory therapists, we used the American Hospital Association Annual Survey from 2018, aggregating hospital numbers to the state level. For both critical care nurses and pharmacists, we used the Bureau of Labor Statistics Occupational Employment Statistics (OES) from 2019.18 OES data reported hospital-based registered nurses and clinical nurse specialists (advanced practice registered nurses) together as registered nurses, and it does not report how many hospital-based nurses are critical care nurse specialists. Therefore, we applied the ratio of hospital-based registered nurses to clinical nurse specialist and the ratio of critical care to hospital-based registered nurses from the National Sample Survey of Registered Nurses to the OES state data.19
For each profession, we calculated baseline and surge clinician capacity COVID-19 workforce requirements based on surge capacity staffing recommendations from the University of California, San Francisco Healthforce Center.20 We based our main estimates on active clinicians, but also provided estimates of clinicians active in other clinical settings (intensivists not billing in ICU settings and hospitalists billing less than our threshold of 90% inpatient service) and inactive clinicians, when possible. The estimator allowed users to adjust provider attrition rates to reflect their local contexts and plan for different rates, and provided a downloadable excel file for each type of health care worker, providing all data and a calculator where users could adjust workforce assumptions, for example, number of health worker shifts per week, hours per shift, and provider to patient ratios (see Appendix, Supplemental Digital Content 1, http://links.lww.com/MLR/C299, which provides additional information on the methodology including an example of this calculator).
RESULTS
The State Hospital Workforce Deficit Estimator, first released on April 8, 2020, reported whether states’ hospital worker supply would be sufficient to meet the peak demand for COVID-19 care using IHME’s lower bound, mean, and upper bound estimates. The most severe level of shortage corresponded to states that had insufficient providers to meet IHME’s lower bound estimation of peak COVID-19 hospital demand. Figure 1 shows an example map of shortages projected for intensivists as of early August 2020.
FIGURE 1.
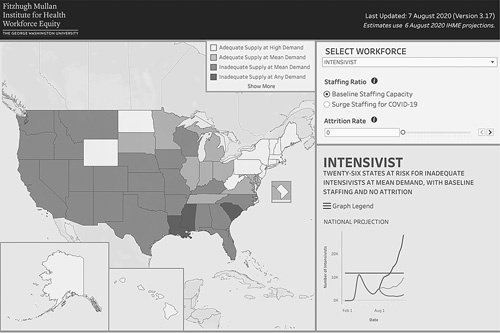
State Hospital Workforce Deficit Estimator for Intensivists, August 7, 2020. COVID-19 indciates coronavirus disease 2019; IHME, Institute for Health Metrics and Evaluation.
The estimator tool provided state level workforce data for each profession and estimates of sufficiency, which we updated based on the most current IHME projections of hospitalizations, every 3−10 days. The number of states with projected shortages changed over the course of the project. Table 1 provides workforce supply and COVID-19 demand for the state of Arizona in April and August. On April 22, Arizona was projected to have sufficient intensivists with an estimated 70% available for non-COVID patients when demand peaked, at baseline staffing. By August 7, the state was estimated to have insufficient intensivists with none available for non-COVID patients when demand peaked.
TABLE 1.
State Hospital Workforce Deficit Estimator—Arizona Hospital Workforce Example
| Projected COVID-19 Workforce Demand, Baseline Staffing | |||||||
|---|---|---|---|---|---|---|---|
| Workforce Supply | April 22, 2020 | August 7, 2020 | |||||
| Profession | Active | Active—Billing Other Areas | Nonactive | Mean Demand | % Available for Non-COVID | Mean Demand | % Available for Non-COVID |
| Intensivists | 208 | 82 | 121 | 63 | 70 | 237 | −14 |
| Hospitalists | 902 | 115 | 208 | 111 | 88 | 403 | 55 |
| Critical Care Nurses | 6647 | NA | NA | 444 | 93 | 1656 | 75 |
| Respiratory Therapists | 1933 | NA | NA | 245 | 87 | 918 | 53 |
| Pharmacists | 1490 | NA | NA | 192 | 87 | 711 | 52 |
COVID-19 indicates coronavirus disease 2019; NA, not applicable.
LIMITATIONS
The development of the State Hospital Workforce Deficit Estimator faced several challenges and limitations. All COVID-19 projections have limitations.21 We selected the IHME model as our source of demand data because it provided estimates at the state rather than the national level, and it was a prevailing model at the time of development.
Available workforce data and information on COVID-19 specific health care demand and staffing needs was also limited. We have the most confidence in our estimates of the supply of hospitalists and intensivists since we were able to use claims data to confirm clinicians’ practice. However, the most recent claims data is from 2017, and we were unable to fully account for nurse practitioners and physician assistants working in critical care and hospitalist settings. Estimates for other professions were mainly based on survey data. These data sources were the best nationally available estimates. Licensure data for pharmacists, respiratory therapists and critical care nurses in some states may be better than our national estimates. For example, North Carolina licensing data identified 4658 respiratory therapists with active licenses in the state, although 500 were identified as unemployed and 50 as retired.22 In comparison, American Hospital Association survey data identified 2717 respiratory therapists working in hospitals in North Carolina. Further work comparing the 2018 National Sample Survey of Registered Nurses to licensure data in North Carolina suggests the 2 datasets produce similar estimates of nurses working in emergency, inpatient, and outpatient setting.23 Our findings on intensivists and hospitalists could be more accurate than licensure data since some licensed professionals could be inactive. Similarly, physicians often list multiple specialties, and the claims data allows us to see who is actually providing the services associated with a specific specialty.
We also could not fully account for changing COVID-19 health care demands or how the workforce might adapt under different surge scenarios. Our estimates did not include nurse practitioners and physician assistants. We assumed that clinicians would care for more patients per shift when COVID-19 cases surged, however, we could not account for how professionals might have skillsets that would allow them to take on new roles. For example, critical care nurses can be trained to fulfill tasks usually performed by respiratory therapists. Nurse practitioners and physician assistants who currently work in outpatient settings might have past experience in critical care. To address this issue, we provided a downloadable tool to allow users to adjust workforce assumptions to align with their local contexts.
A final limitation is that, given the absence of data for both projected hospital care demand and clinician supply, we could not go below that state level. Nevertheless, we know that the severity of the pandemic varied widely within states, making substate analyses desirable. Thus, while our estimates could inform decisions at the state and national levels, they could not inform distributional decisions within states.
CONTACT TRACING WORKFORCE ESTIMATOR
Contact tracing is a core public health strategy to control infectious diseases. Most states and counties have some contact tracing staff to deal with sexually transmitted diseases and other infectious diseases, but the staff needed for these diseases are far less than the number needed to deal with the COVID-19 pandemic. Conceptually, contact tracing seeks to quickly identify anyone who has come into close contact with a person who tests positive for an infectious disease and prevent further spread of the disease. Total shutdowns of communities are the blunt instrument to slow the spread by preventing any contact in the community; contact tracing is the targeted alternative.
Initial estimates for the contact tracing workforce were high-level and based on a strict per-capita approach. The National Association of County and City Health Officials (NACCHO) recommended 15 health workers per 100,000 at baseline and 30 per 100,000 during a pandemic, the equivalent of nearly 100,000 contact tracers when applied to the United States population.24 Other estimates used other countries’ strategies. China deployed 1800 teams of 5 in Wuhan to serve a population of 11 million for a ratio of 81 contact tracers per 100,000 people, translating into a need for about 300,000 contact tracers in the United States.25 Other countries where the virus was successfully controlled, including Iceland and New Zealand, used smaller ratios of 13.7 and 3.9 per 100,000 people, respectively.26,27
The pandemic was not affecting the United States uniformly, however, and a purely population-based method to approximate contact tracers risked underestimating or disproportionately allocating the workforce. Around this time, Resolve to Save Lives released a spreadsheet to help calculate staffing needs for contact tracing for individual jurisdictions but did not provide a state or national snapshot of workforce needs, which might inform policy and planning.28 We developed the Contact Tracing Workforce Estimator (CT Estimator) as a more nuanced tool to inform federal, state, and county officials in their planning for this new workforce.
METHODS
The CT Estimator uses a baseline of 15 CTs per 100,000 population and increases, as needed, the number of contact tracers required to address the prior 14-day COVID-19 case count for each county over a week and provides aggregates at the state and national level. We used case data imported from the Center for Systems Science and Engineering at Johns Hopkins University to update the CT Estimator weekly with new 14-day case counts.29
We initially reviewed available literature, including guidance from governmental agencies, organizations engaged in contact tracing, and media reports. We also consulted with public health experts (eg, county health departments) and partnered with the Association of State and Territorial Health Officials and NACCHO to guide our understanding of the workflow and specific steps and tasks for the contact tracing workforce. Figure 2 summarizes the effort required to trace 1 case. The workforce needed relates to the number of cases, the number of contacts, and the time needed to interview each case and to reach and talk with those coming into contact with people who tested positive. Several contextual factors impact the variables determining the number of contact tracers that are needed. The level of social distancing and stay-at-home orders affects the number of contacts while the social needs of contacts and the ability to self-isolate may affect the time required in follow up. The use of technology and other apps may shorten the time required with contacts. The CT Estimator includes default variables for all factors in the algorithm. The default values were based on discussions with experts in the field. For example, the default value for the number of contacts per positive case was set at 10. If a community is generally shut down, this is likely to be high; if there are few or no constraints on social interactions, this is a low estimate.
FIGURE 2.

Contact Tracing Effort.
The CT Estimator allows local planners to adjust assumptions according to the unique needs of their population. To inform user decision making when modifying workforce capacity variables, we included data on local cases per day (with trends over the last 14 d period), population demographics, and the Centers for Disease Control and Prevention Social Vulnerability Index which takes into consideration 15 social factors, such as poverty status and English-language proficiency, to identify communities with higher needs.30 The CT Estimator also provides geolocations of local health departments, which used data from NACCHO as of 2016. The map also provides an analogous display for Tribal Nations areas with locations of Indian Health Services facilities. For Tribal nations, 14-day case counts were unavailable, and the tool requires users to enter daily COVID-19 case counts.
RESULTS
The CT Estimator presets the number of contacts per case to account for social distancing and the CT work capacity (number of case interviews, contact notifications, and contact follow-ups a CT can conduct daily) to include some social needs evaluation, case management, and daily follow up for all contacts for a 14-day total period. The user can modify all of these variables. The estimator also supports a daily case override, which allows a user to set the number of anticipated daily cases to support planning for future needs (eg, anticipated surge or decreasing cases). For example, adjusting the percent contact follow-up expected from 100% to 50% in early August reduced the national estimate of contact tracers needed from 369,558 to 273,107. Increasing the number of contact notifications a contact tracer can complete in a day from 12 to 24, perhaps working in a community with greater CT technology engagement, further decreased the national estimate to 202,052 contact tracers. Figure 3 shows an example map of the state of Florida in early August.
FIGURE 3.
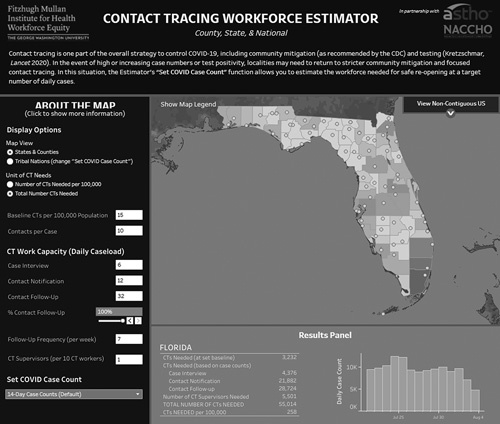
Contact Tracing Workforce Estimator—Florida, August 4, 2020. CDC indicates Centers for Disease Control and Prevention; COVID-19, coronavirus disease 2019; CT, Contact Tracing; NACCHO, National Association of County and City Health Officials.
LIMITATIONS
We note several challenges and limitations in the development of the CT Estimator. Initially, limited information regarding the number of contacts per case and work capacity of contact tracers was mostly a function of the novelty surrounding COVID-19. With time, however, there remained a lack of data around the workflows and efficiencies of contact tracing, limiting our ability to update assumptions and preset variables to increase the utility of the tool. While we recognized that population demographics and use of technology would affect workflow, there was little information available regarding these effects to refine the CT Estimator further.
Workforce needs, as calculated by the CT Estimator, correlate directly with the number of cases at a discrete point in time. As locations began to see a surge in cases following phased reopening, the number of CTs needed also increased—sometimes to a level where contact tracing no longer seemed feasible. While locations were encouraged to continuously reevaluate and plan for the required workforce at a target number of daily cases, additional data surrounding these metrics (proportion of new contacts notified, percent of new cases arising from contacts) would strengthen the utility of the CT Estimator and help guide decision making in localities.
Finally, planning a workforce inherently depends upon an understanding of the existing workforce. Before COVID-19, contact tracing was primarily focused on sexually transmitted diseases and carried out by Disease Intervention Specialists in settings where need and funding could support a position. In smaller health departments, the role may fall within the job description of a variety of public health workers. This ambiguity limits the ability to estimate the actual size of the existing contact tracing workforce, and therefore the use of this workforce was not included when calculating the workforce needed to support contact tracing for COVID-19.
DISCUSSION
The 2 health workforce estimators demonstrate the potential value of bringing existing health workforce data and analysis to real-time local, state, and national pandemic response (Fig. 4). At the local level, workforce data can direct needed resources to support existing health workers, target the recruitment, training, and deployment of high need health workers, and support cross-community coordination and partnerships, such as local health departments, universities, and health centers partnering to train, support, and coordinate the contact tracing workforce. The flow of data and information from organizations up to the state and national levels can inform policies and programs to meet local needs, including the strategic deployment of state and national health workforce and resources. The broad geographic impact of COVID-19 has been unlike any recent disasters, creating a critical need for better information to target limited resources.
FIGURE 4.
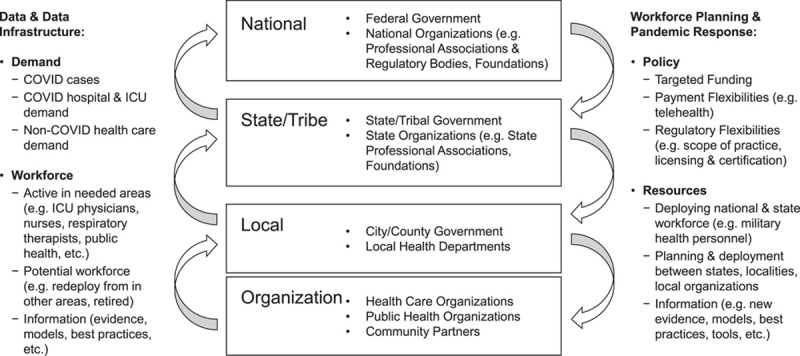
Health Workforce Data, Planning, and Pandemic Response Framework.
The health workforce estimators also demonstrate significant gaps and needs for a more effective pandemic response. The estimators highlight the need to build tools that are flexible to accommodate significant unknowns, for example, allowing communities to adjust workforce assumptions based on their local context (eg, health worker attrition or contact tracing workload), and that support ongoing reevaluation as the situation changes. In the case of a novel and rapidly developing pandemic, much will be unknown in the early days. The availability of health care and public health service needs, staffing models, and health workforce data created significant limitations for pandemic response and persisted well into the course of COVID-19. Inconsistent data across health professions and localities and limited infrastructure for data flow up to local, state, and national levels resulted in no national datasets in many cases. In the case of the public health workforce, lack of consistent data led to ongoing challenges as states, and the nation struggled to understand the sufficiency of the contact tracing workforce.31
The health workforce is a critical component of the health care and public health systems that we will need for any future pandemic response. Increased investment in health workforce data and data infrastructure is required to ensure future preparedness. The success of past efforts to establish minimum datasets with consistent core data has been variable by profession and state, and national databases remain limited.32 While the federal National Center for Health Workforce Analysis supports health workforce research and data, 2 additional federal vehicles to support workforce planning—the National Health Care Workforce Commission and State Health Care Workforce Development Grants—were authorized by the Patient Protection and Affordable Care Act, but never funded. COVID-19 has shown us that this infrastructure, as well as engagement by local health care organizations, local health departments, states, and national organizations, are needed to ensure the health workforce is ready and able to respond in times of emergency.
The experience with the estimators clearly demonstrates the need for a national response to meet workforce needs in a pandemic. As the number of cases rise rapidly in a community, there is an urgent need for workers, but local communities and states do not have the time, expertise or resources to rapidly recruit, train and hire staff to meet peak needs. Given that different communities and states experience high need at different times, the ability to move the workforce to communities where need is high would be more effective than expecting local communities to be able to ramp up quickly. This calls for state and national efforts to bolster local communities.
Supplementary Material
Supplemental Digital Content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal's website, www.lww-medicalcare.com.
Footnotes
The State Health Workforce Deficit Estimator and the Contact Tracing Workforce Estimator are supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) as part of an award totaling $450,000 with zero percentage financed with non-governmental sources.
The authors declare no conflict of interest.
Contributor Information
Candice Chen, Email: cpchen@gwu.edu.
Qian Luo, Email: qluo@gwu.edu.
Nicholas Chong, Email: nchong@gwmail.gwu.edu.
Sara Westergaard, Email: swestergaard@gwu.edu.
Erin Brantley, Email: ebrantley@email.gwu.edu.
Edward Salsberg, Email: esalsberg@email.gwu.edu.
Clese Erikson, Email: cerikson@email.gwu.edu.
Drishti Pillai, Email: drishti_pillai@email.gwu.edu.
Katherine Green, Email: greenk@email.gwu.edu.
Patricia Pittman, Email: ppittman@gwu.edu.
REFERENCES
- 1.U.S. Department of Health and Human Services. Pandemic Influenza Plan 2017 Update [CDC web site]. 2017. Available at: www.cdc.gov/flu/pandemic-resources/pdf/pan-flu-report-2017v2.pdf. Accessed March 23, 2021.
- 2.Centers for Disease Control and Prevention. FluSurge Special Edition [CDC web site]. 2009. Available at: www.cdc.gov/h1n1flu/tools/flusurge/. Accessed March 23, 2021.
- 3.Abramovich MN, Toner ES, Matheny J. Panalysis: a new spreadsheet-based tool for pandemic planning. Biosecur Bioterror. 2008;6:78–92. [DOI] [PubMed] [Google Scholar]
- 4.Eichner M, Schwehm M, Duerr HP, et al. The influenza pandemic preparedness planning tool InfluSim. BMC Infect Dis. 2007;7:1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Germann TC, Kadau K, Longini IM, Jr, et al. Mitigation strategies for pandemic influenza in the United States. Proc Natl Acad Sci USA. 2006;103:5935–5940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Frogner B. How many health care workers are at risk of being sacrificed to COVID-19 in the US? [Center for Health Workforce Studies, University of Washington web site]. 2020. Available at: https://depts.washington.edu/fammed/chws/how-many-health-care-workers-are-at-risk-of-being-sacrificed-to-covid-19-in-the-us/. Accessed August 7, 2020.
- 7.Higgins-Dunn N. Travel nurses race to New York and other coronavirus hot spots: ‘They are literally in a war zone’ [CNBC web site]. 2020. Available at: www.cnbc.com/2020/04/06/travel-nurses-race-to-new-york-and-other-coronavirus-hot-spots-they-are-literally-in-a-war-zone.html. Accessed August 9, 2020.
- 8.Federation of State Medical Boards. U.S. states and territories modifying licensure requirements for physicians in response to COVID-19 [FSMB web site]. 2020. Available at: www.fsmb.org/siteassets/advocacy/pdf/state-emergency-declarations-licensures-requirementscovid-19.pdf. Accessed August 20, 2020.
- 9.Bowman T. U.S. military is sending medical staff to COVID-19 hotspots [NPR web site]. 2020. Available at: www.npr.org/sections/coronavirus-live-updates/2020/07/13/890553905/u-s-military-is-sending-medical-staff-to-covid-19-hotspots. Accessed August 11, 2020.
- 10.Dawson L. The National Disaster Medical System (NDMS) and the COVID-19 pandemic. [Kaiser Family Foundation web site]. 2020. Available at: www.kff.org/coronavirus-covid-19/issue-brief/the-national-disaster-medical-system-ndms-and-the-covid-19-pandemic/. Accessed August 9, 2020.
- 11.Spetz J. There are not nearly enough nurses to handle the surge of coronavirus patients: here’s how to close the gap quickly [Health Affairs blog web site]. 2020. Available at: www.healthaffairs.org/do/10.1377/hblog20200327.714037/full/. Accessed August 20, 2020.
- 12.Chen C Pittman P Westergaard S, et al. Emerging health workforce strategies to address COVID-19 [Health Affairs blog web site]. 2020. Available at: www.healthaffairs.org/do/10.1377/hblog20200414.197056/full/. Accessed August 20, 2020.
- 13.Institute for Health Metrics and Evaluation. COVID-19 Projections. Institute for Health Metrics and Evaluation [IHME web site]. 2020. Available at: https://covid19.healthdata.org/. Accessed August 10, 2020.
- 14.Centers for Medicare & Medicaid Services. Cost Reports [CMMS web site]. 2020. Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Downloadable-Public-Use-Files/Cost-Reports. Accessed August 10, 2020.
- 15.Center for Medicare & Medicaid Services. Provider Enrollment, Chain, and Ownership System [CMMS web site]. Available at: https://pecos.cms.hhs.gov. Accessed March 10, 2021.
- 16.Center for Medicare & Medicaid Services. National Plan and Provider Enumeration System [CMMS web site]. Available at: https://npiregistry.cms.hhs.gov/. Accessed March 10, 2021.
- 17.Center for Medicare & Medicaid Services. Medicare Provider Utilization and Payment Data: Physician and Other Supplier Data CY 2017 [CMMS web site]. 2020. Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Provider-Charge-Data/Physician-and-Other-Supplier2017. Accessed March 10, 2021.
- 18.United States Department of Labor Bureau of Labor Statistics. Occupational Employment Statistics [U.S. Bureau of Labor Statistics web site]. Available at: www.bls.gov/oes/. Accessed March 10, 2021.
- 19.Health Resources and Services Administration National Center for Health Workforce Analysis. Nursing Workforce Survey Data [HRSA web site]. Available at: https://data.hrsa.gov/topics/health-workforce/nursing-workforce-survey-data. Accessed March 10, 2021.
- 20.University of California San Francisco Healthforce Center. Staffing Plans for Surge Hospitals [University of California, San Francisco web site]. 2020. Available at: https://healthforce.ucsf.edu/file/staffing-plans-surge-hospitals-public-apr-7-updatexlsx. Accessed August 9, 2020.
- 21.Holmdahl I, Buckee C. Wrong but useful—What Covid-19 epidemiologic models can and cannot tell us. N Engl J Med. 2020;383:303–305. [DOI] [PubMed] [Google Scholar]
- 22.Fraher E Galloway E Spero J, et al. North Carolina’s Respiratory Therapist Workforce: Availability to treat COVID-19 [Sheps Health Workforce NC web site]. 2020. Available at: https://nchealthworkforce.unc.edu/blog/respiratory_therapist_nc/. Accessed February 22, 2021.
- 23.Patel E. Comparing Hospital Nurse Settings from the 2018 NSSRN vs. 2008-2013 North Carolina Licensure Data [Sheps Health Workforce NC web site]. 2020. Available at: https://nchealthworkforce.unc.edu/briefs/nssrn_hospital_setting/. Accessed February 22, 2021.
- 24.National Association of City and County Health Officials. NACCHO Position Statement: Building COVID-19 Contact Tracing Capacity in Health Departments to Support Reopening American Society Safely [NACCHO web site]. 2020. Available at: www.naccho.org/uploads/full-width-images/Contact-Tracing-Statement-4-16-2020.pdf. Accessed August 6, 2020.
- 25.World Health Organization. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) [WHO web site]. 2020. Available at: www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf. Accessed August 6, 2020.
- 26.The Directorate of Health and The Department of Civil Protection and Emergency Management. Iceland’s response [Iceland government web site]. 2020. Available at: www.covid.is/sub-categories/icelands-response. Accessed August 6, 2020.
- 27.New Zealand Ministry of Health. Contact tracing at forefront of fight against COVID-19 [New Zealand Ministry of Health web site]. 2020. Available at: www.health.govt.nz/news-media/media-releases/contact-tracing-forefront-fight-against-covid-19. Accessed August 6, 2020.
- 28.Prevent Epidemics. Contact tracing staffing calculator [Prevent Epidemics web site]. 2020. Available at: https://preventepidemics.org/covid19/resources/contact-tracing-staffing-calculator/. Accessed March 23, 2021.
- 29.Johns Hopkins University and Medicine. COVID-19 Dashboard by the Center for Systems Science and Engineering (CCSE) at Johns Hopkins [JHU web site]. 2020. Available at: https://coronavirus.jhu.edu/map.html. Accessed August 6, 2020.
- 30.Agency for Toxic Substances and Disease Registry. CDC Social Vulnerability Index [CDC web site]. 2020. Available at: www.atsdr.cdc.gov/placeandhealth/svi/index.html. Accessed March 10, 2021.
- 31.Simmons-Duffin S.Coronavirus cases are surging. The contact tracing workforce is not [NPR web site]. 2020. Available at: www.npr.org/sections/health-shots/2020/08/07/899954832/coronavirus-cases-are-surging-the-contact-tracing-workforce-is-not. Accessed August 11, 2020.
- 32.Clifford M, Armstrong DP. Inventory of State Health Workforce Data Collection. Rensselaer, NY: Center for Health Workforce Studies, School of Public Health, University at Albany, State University of New York; 2019. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Digital Content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal's website, www.lww-medicalcare.com.