

Abstract
Objective:
The presence of unlocked firearms in the home is associated with increased risk of suicide and unintentional injury in youth. We adapted an evidence-based program for promoting safe firearm storage, Safety Check, to enhance its acceptability as a universal suicide prevention strategy in pediatric primary care.
Methods:
We applied ADAPT-ITT, an established adaptation framework, to guide iterative program adaptation with ongoing input from key stakeholders. The present study describes two phases of ADAPT-ITT: the Production phase (generating adaptations) and the Topical Experts phase (gathering stakeholder feedback on adaptations). After generating proposed program adaptations based on three inputs (stakeholder feedback collected in a prior study, the behavioral science literature, and best practices in pediatric medicine), we elicited feedback from stakeholders with firearm expertise. The adaptations included changes such as clarifying firearm ownership will not be documented in the medical record and offering follow-up reminders. We also crowdsourced feedback from 337 parents to select a new name and program logo.
Results:
Saturation was reached with 9 stakeholders. Feedback confirmed the value of adaptations that: a) considered context (e.g., reason for ownership), b) promoted parent autonomy in decision-making, and c) ensured privacy. The most preferred program name was Suicide and Accident prevention through Family Education (SAFE) Firearm.
Conclusions:
Guided by an established adaptation framework that prioritized multi-stage stakeholder feedback, adaptations to the original Safety Check were deemed acceptable. We plan to test the SAFE Firearm program as a universal suicide prevention strategy in pediatric primary care via a hybrid effectiveness-implementation trial.
Keywords: suicide prevention, firearm safety, pediatric primary care
Firearms are the second leading cause of death for young people (1-19 years old) in the United States (U.S.).1 Because unlocked firearms are associated with higher likelihood of both suicide and unintentional injury,2,3 safe firearm storage is key to preventing firearm injuries and may be a promising universal suicide prevention strategy. The American Academy of Pediatrics4 and Society for Adolescent Health and Medicine5 have issued recommendations encouraging pediatricians to counsel parents on safe firearm storage and there is evidence that such counseling can affect storage behavior,6 but these discussions are not a routine part of well-child visits.7 The sensitive national debate surrounding firearms highlights the importance of ensuring that safety programs incorporate the perspectives of firearm-owning parents and firearm experts. The current study applied an established adaptation framework (i.e., ADAPT-ITT)8 to incorporate such stakeholder input into an existing evidence-based program for promoting safe firearm storage, Safety Check (SC). Our goals were to enhance its acceptability and to facilitate widespread use in pediatric primary care.
Safe Storage as a Means to Prevent Youth Firearm Injury and Mortality
Firearms are present in one in three homes in the U.S.9 Among firearm-owning households with children, about three out of 10 store all guns unloaded and locked.10 Simulation research has found that a modest increase in safe firearm storage could prevent as many as 32% of youth firearm deaths in the U.S.11 With documented increases in firearm purchases during the COVID-19 pandemic,12 there is an urgent need for safe firearm storage programs.
Primary Care as an Optimal Setting for Firearm Safety Interventions
Primary care is an ideal setting for universal prevention programs, since many children and adolescents attend annual well-care visits.13 Prior research has found that the majority of parents, both firearm owners and non-owners, believe pediatricians should provide advice about safe firearm storage14 and that it is appropriate to receive a firearm safety lock at a pediatric office.15 Moreover, many primary care providers (PCPs) view firearm safety programs as within their scope of practice.7,16 Yet, many pediatric PCPs do not deliver firearm safety programs, representing a missed opportunity.17
The Safety Check Program
SC is an evidence-based violence prevention program designed to reach parents of young children (ages 2-11 years), with a focus on discipline, media use, and firearm safe storage. Its firearm injury harm reduction approach includes: (a) screening for presence of firearms, firearm storage, and parental concerns about firearm injuries where children live and/or play; (b) counseling using brief motivational interviewing18; and (c) providing firearm safe storage tools, such as a cable lock.6 A randomized controlled trial conducted in 137 pediatric clinics found a 10% increase in parent-reported use of cable locks to store firearms in the intervention group and a 12% decrease in the control group.6
Adapting Safety Check for Expanded Use
In keeping with recommendations from the implementation science literature regarding adaptation of evidence-based interventions for use with new populations,19,20 we chose the ADAPT-ITT framework8 to guide our efforts to adapt SC’s safe storage component to reach a broader age group (i.e., youth up to age 18) and to serve as a universal suicide prevention strategy. The framework integrates stakeholder feedback during sequential, iterative phases of adaptation. Although ADAPT-ITT8 was first developed in the context of HIV prevention and intervention research, it has been used to guide adaptations to other behavioral interventions (e.g., a brief adolescent substance use intervention),21 making it well-suited for the current investigation. As summarized in Figure 1, the model8 includes eight steps: Assessment, Decision, Adaptation, Production, Topical Experts, Integration of Feedback, Training, and Testing. As described in detail elsewhere,7,16,22 we previously surveyed or interviewed a range of stakeholders including parents, pediatric primary care providers, and firearm owners and experts as part of the Assessment, Decision, and Adaptation phases and found greater acceptability and use of the screening and counseling components of SC, compared to giving out cable locks.7,22 The present study describes the subsequent two steps: the Production phase (generating proposed adaptations) and the Topical Experts phase (gathering stakeholder feedback on proposed adaptations). The remaining ADAPT-ITT steps (Integration of feedback, Training, and Testing) will be completed in our future work. To our knowledge, this is the first application of ADAPT-ITT to a firearm safety program.
Figure 1.
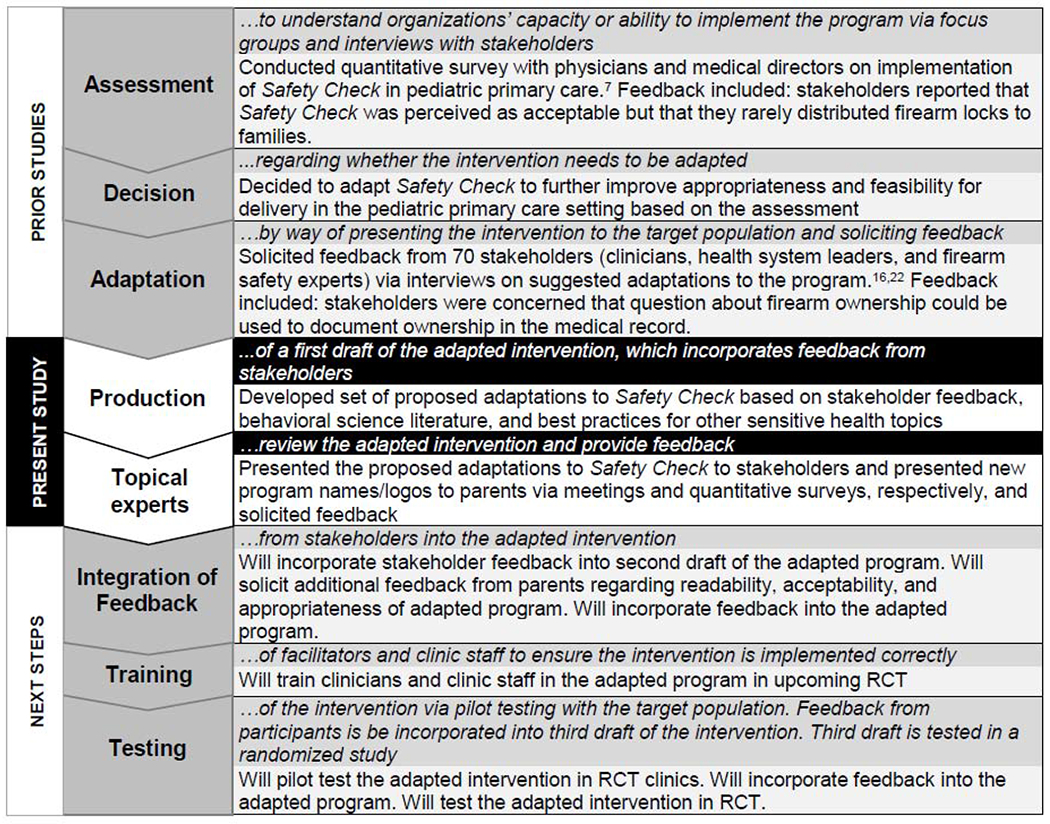
Steps of adaptation of Safety Check via the ADAPT-ITT model8
METHOD
All study procedures were approved by the University of Pennsylvania’s Institutional Review Board. We followed Consolidated Criteria for Reporting Qualitative Research (CORE-Q) reporting guidelines.23
Generating Proposed Adaptations (“Production”)
Our proposed program adaptations were based on stakeholder input from prior stages,7,16,22 literature regarding health behavior change, and best practices from other primary care-based interventions on sensitive health topics (e.g., HPV vaccination). For example, some components of the intervention were adjusted to accommodate stakeholder concerns and preferences (e.g., clarifying that ownership will not be documented in the medical record), whereas others were added based on their ability to promote behavior change (e.g., incorporating reminders). An initial group of potential adaptations was discussed and refined in collaboration with the research team before being presented to stakeholders.
Initial Stakeholder Feedback on Proposed Adaptations (“Topical Experts, Part 1”)
Recruitment and Participants.
We recruited a convenience sample of individuals who expressed interest in participating in research related to firearm safety and suicide prevention with the research team and/or the Firearm Safety Among Children and Teens (FACTS) Consortium (https://www.icpsr.umich.edu/web/pages/facts/index.html) to confirm acceptability of the proposed adaptations. All participants were firearm owners who were highly engaged in firearm safety promotion, including some who had a specific focus on suicide prevention. They also represented various perspectives based on other roles and backgrounds (i.e., firearm safety instructors or experts, mental health clinician, educator, military veterans, and law enforcement). Stakeholders were located across the U.S. (e.g., Midwest, Southwest, Mid-Atlantic) and provided urban, suburban, and rural perspectives. Eight stakeholders were invited to participate in the initial wave of recruitment; one additional stakeholder was recommended by another stakeholder. All who were invited chose to participate. Thematic saturation was an explicit goal of recruitment. A priori, we planned for a sample size of 9-15 stakeholders, similar to sample size recommendations in the literature.24 Recent work by Guest and colleagues25 suggests that 6-7 interviews is enough to gather most themes in a homogenous sample.
Procedure.
Individuals participated in a one-hour small group discussion or individual interview, based on schedule and/or preference. Members of the research team with experience conducting qualitative interviews (RSB, ARP, and/or CJ; two psychologists and one graduate-level research coordinator; all women) conducted two small group discussions (comprised of three people each) and three individual interviews via a secure virtual meeting platform. Participants were sent the informed consent document to review ahead of the interview. During the meetings, we obtained verbal consent for participation and permission to audio-record. We then summarized the original SC program, presented each proposed adaptation with a brief rationale for the change, and asked stakeholders to provide feedback. Following the meeting, participants were given the option of submitting additional anonymous comments via a secure online survey platform, though no new information was gleaned this way. Audio recordings were transcribed and uploaded into the NVivo Qualitative Data Analysis Software, version 10 (QSR International). Field notes were not taken and transcriptions were not reviewed by participants. Participants did not provide feedback on the findings.
Data Analysis.
We used an integrated analysis approach to coding,26,27 which involved identifying a priori constructs related to each program component (e.g., “locks”) and adding codes upon review of all transcripts based on emergent themes. Two members of the research team (AL, CJ) developed a structured codebook by open coding each transcript and then met to refine the codebook (available upon request). After codebook development, two members of the research team (MD, CJ) independently coded each transcript and met to resolve discrepancies, refine the codebook, and analyze consensus codes. All transcripts were double coded (Cohen’s kappa = 0.91).
Additional Stakeholder Feedback on Proposed Adaptations (“Topical Experts, Part 2”)
Recruitment and Participants.
Next, we used an online platform to crowdsource name and logo design ideas for the adapted program. After receiving 1,419 name entries and 299 logo entries, the research team chose the 10 names and 10 logos that best fit the program content, context, and prior stakeholder feedback, and obtained quantitative feedback from firearm-owning and non-owning parents via Amazon Mechanical Turk (MTurk) in two separate surveys.28 Participant selection criteria are detailed in Figure 2.
Figure 2. Surveys completed on Amazon Mechanical Turk (MTurk).
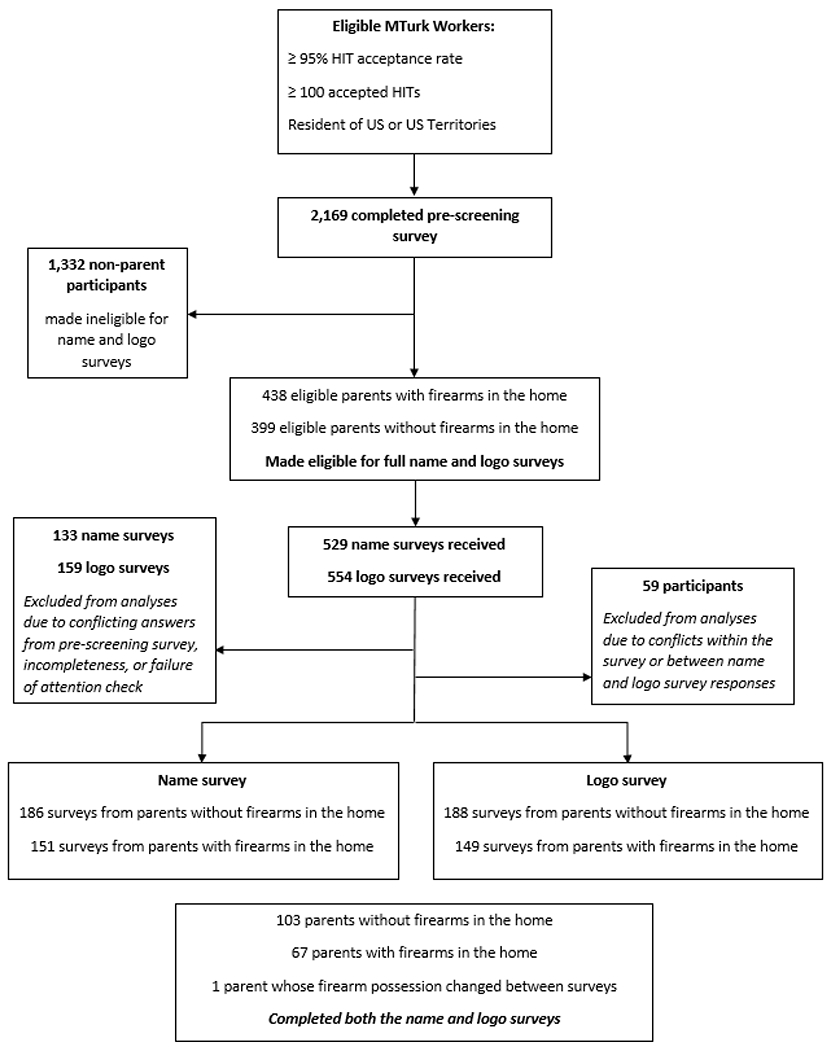
HIT indicates human intelligence task. Additional details are available in part one of the Appendix.
Measures.
Background information included self-reported age, gender, race, number of children, and number of firearms owned. Acceptability and appropriateness of each name and logo option were assessed with one question each from the Acceptability of Intervention Measure (AIM; “I like this name/logo”) and Intervention Appropriateness Measure (IAM; “This name/logo is suitable for the pediatric primary care setting”)29 – each of which were rated on a 1-5 Likert scale. Preferences were assessed by presenting eight sets of five randomly selected program name and logo options, respectively, and asking participants to pick the best and worst options using best-worst scaling, a preference elicitation approach.30
Data Analysis.
We used a number of strategies to ensure data quality prior to analysis (see the Appendix Part One). Descriptive statistics were used to analyze demographic data. We analyzed mean acceptability and appropriateness scores and used independent samples t-tests to compare responses across firearm owner and non-owner subgroups. We calculated a best and a worst frequency score for each name and logo choice, representing the number of times each choice was selected best and worst, respectively, divided by the number of times each choice was displayed. Overall preference scores were calculated by subtracting the worst frequency from the best frequency. These scores were calculated separately for firearm owners and non-owners.
RESULTS
Production Phase: Generating Proposed Adaptations
Proposed adaptations centered on a number of key changes: 1) remove screening for firearm ownership to emphasize the goal of universal implementation; 2) clarify for parents that firearm ownership will not be documented in the medical record, to reduce privacy concerns; 3) change the program name; 4) provide cable locks but also offer information on other storage options to accommodate different firearms and uses (e.g., personal protection vs. hunting); 5) use evidence-based behavior change strategies to boost follow-through (e.g., setting an intention, reminder sticker); 6) emphasize the shared goal of keeping young people safe (i.e., use gain-framed messaging to offset perceived disadvantages of changing storage behavior); 7) offer additional resources from firearm experts to increase the credibility of the message; and 8) follow up after the visit to aid follow-through. A detailed list of proposed adaptations and supporting rationales is provided in the Appendix Part Two.
Topical Experts Phase: Stakeholder Feedback on Proposed Adaptations
Table 1 lists the proposed adaptations alongside examples of related stakeholder feedback. Saturation was achieved by the third discussion; however, we continued conducting additional interviews to further ensure saturation as well as geographic representation. Stakeholders were in favor of a safe firearm storage program as a universal suicide prevention strategy and agreed with the importance of delivering the program to all families, irrespective of firearm ownership status. They highlighted the need for safety education among new firearm owners as well as the need for reminders among some established owners, and found value in owners receiving safety messaging from multiple sources, including pediatric providers.
Table 1.
Stakeholder Feedback on Proposed Adaptations and Themes Across Adaptations
| Proposed Adaptation or Theme | Example Quotes |
|---|---|
| Proposed Adaptations | |
|
| |
| 1: Remove Screening Step | 203: When somebody feels like you’re
trying to single them out as a gun owner, then some of that dialogue
starts to shut down, but if you generalize a little bit, and at the same
time you’re kind of making it more…cause you’re
talking about, “I don’t care where the gun is, you need to
be thinking safety.” 103: I know from where I’m at…there definitely has been a lot of, from what we’ve seen recently or generally, concern from individuals about being asked about owning firearms… |
| 2: State that Firearm Ownership Status Will Not be Documented | 301: … I know there are some people out there that feel very strongly about having [firearm ownership] documented. They feel it’s their personal right to bear a firearm, regardless if it’s a handgun, a long rifle shotgun, that sort of thing. And they don’t want it documented. |
| 3: Change the Program Name | 101: And so if it’s generic, and just
descriptive, that makes me a little bit more comfortable. 401: It’s not about the gun. It’s about, it’s one more child. Lock up the guns. Because one is too many. I’ve been using that phrase a lot. One is too many. |
| 4: Provide Free Cable Locks and Resources Describing Alternative Locking Options | 201: So there are a lot of options out there.
And I suppose, you know, you can’t have one size fitting all,
obviously. Firearms are different, people are different, homes are
different, locations are different. 101: So I think having the lock on hand is, there is value in that. It’s often a conversation starter, even if it’s not the preferred method of secure storage. And it can lead people to a discussion of, say, a lock box, which we can’t assume, we have some focus group research that says we can’t assume that people know about lock boxes because we found out that many people didn’t, when we assumed that they did. |
| 5: Use Strategies from Behavioral Science to Promote Behavior Change | 101: …about the sticker, the date-time to use the lock—I wasn’t quite sure. I mean, really that only works one time, right? That’s—when you give them the lock you put down “install this at 5 PM today” or something like that. Well that—the lock is going to go on the gun, and then off the gun, and then on the gun, and then off the gun. You know, the number of times that people are using the firearm. Or, like I said, it only sort of works one time. And it’s a little—seems a little odd. It seems to me that if you’re going to do something like that, that maybe a verbal pledge or something like that might suffice. A written pledge might be, some people might respond to that, and for others, that might be a little off-putting. |
| 6: Emphasize the Shared Goal of Keeping Children Safe | 401: …you wear a seatbelt, because
it’s safer. Lock up the gun, because it’s
safer. 501: And the main thing I say is, regardless of what your stance is on firearms, don’t come across from a judgmental or a critical perspective. And find common ground, which is the safety of the child. You know, that’s the main thing, the safety of the child. |
| 7: Offer Additional Resources from Firearm Experts | 201: … information is power and I think
that the informed decision on the part of the parents and I see us as
being the facilitators of resources, making it available. 501: …give parents a link to a video that includes credible firearms experts talking about the importance—fantastic. But I think that as important as credible sources, there should also be individuals that have been affected by gun tragedies. Nothing speaks to that population as people who have been there and have done that. So parents of kids who have gotten hurt, individuals that have hurt themselves because of improperly stored firearms. |
| 8: Follow-up | 101: But I think it’s more palatable if it’s optional. Somebody gives you permission or asks you to follow up. I think that makes it much more palatable. |
|
Overarching
Themes Autonomy |
201: So, I guess the goal would be to provide as much information as possible, and let the parent decide what fits for their situation. |
| Privacy | 301: But I think of it this way…Are you more likely to ask for condoms or ask for other sorts of prophylactics or you know, “Hey, there’s a bin there, I can grab a few of them.” You know what I mean? Without having to have that conversation. |
| Communication | 102: I would just caution against anything
that’s going to make people think you are being cute with the
language, you know. I think it should be very
transparent… 301: …at least having it in in print material and having a set script, because what I’ve also experienced is that everybody has their own personal opinions. I’ve had some pretty opinionated physicians of my own and for my children over time. You don’t want them to be interjecting their own personal feelings into it. |
| Knowledge | 101: …And I think, you know,
particularly the suicide angle may be something that some parents have
not thought about. I think it’s a much more powerful argument.
Not that, obviously, keeping a young child safe from accessing a gun is
not a powerful argument. But the fact that those numbers are growing rapidly, and there are a lot of external factors… |
| Safe Storage | 202: So safe storage to me is different than what 201 just said. Just not allowing, you know I have a young [child], access to my weapon and knowing where my weapon is at all times and making sure it’s in a position where [they] can’t get ahold of it. |
| Situational Awareness | 202: I think it is important to do at your
well checks, because I think at times we do get complacent. So, and you
know, we need to be reminded that we need to put these things away
too. 501: You think your kids don’t know where your guns are? That is just a fallacy. |
| Environment | 301: The culture that is coming through is so
scared of firearms. You know, that’s just my opinion, but I see a
lot of this fear of firearms instead of [recognizing] it has a purpose.
You know, respect it, treat it appropriately, and it’s not an
issue. But, there’s so many people that just have this fear, like
the gun is going to jump up and do something to you. It’s
not. 401: Because certainly a doctor knows his patients, and some of them hunt together. You get some of these communities and it’s like, “hey, I know ‘Jim’ has all these guns. Tell him to lock them up, and there’s ten gun locks in there. Take them home to ‘Jim,’ and tell him I’m going to be over for bourbon, and I’m going to make sure they’re locked up.” I mean some of these doctors have this kind of relationship… |
Stakeholders noted that asking about firearm ownership status prior to universal counseling could elicit defensiveness and that allowing parents to choose whether to disclose ownership was preferable. Similarly, they agreed that proactively clarifying that providers would document only that a conversation took place (not whether families owned a firearm) would increase privacy and acceptability and reduce concerns that the information would be used in an unanticipated manner (e.g., to create a national firearm registry). Stakeholders also suggested that a new program name should be succinct and specific, with branding maintaining a focus on safety. One stakeholder suggested a “name the campaign contest” to arrive at the new program name.
Stakeholders saw benefits to providing locks as part of the program in order to motivate behavior change. Nonetheless, they noted both advantages and disadvantages of cable locks and agreed that resources describing alternative locking options would be helpful to provide alongside the cable locks. While stakeholders acknowledged the potential value of reminders to use the locks, feedback was mixed on the best method (e.g., a sticker to record the date the parent plans to lock their firearm). Stakeholders felt some parents could find such tools helpful, whereas others might find them intrusive. Stakeholders generally agreed that instructional tools to clarify the steps of locking a firearm (e.g., videos) would be acceptable.
Stakeholders agreed that emphasizing the program’s intention of promoting child safety would be important, as would ensuring that parents not feel singled out or judged for owning firearms. There was also recognition that family engagement in safe storage is a process and that even small steps toward safer storage are valuable, consistent with a harm reduction approach. Stakeholders recommended consideration of a range of formats (e.g., videos, infographics) for resources to be incorporated into the program. Their primary feedback was about the importance of attending to content and framing (e.g., wording of messages, credibility of speakers).
Finally, stakeholders varied in their beliefs about whether there should be a follow-up component and how that communication should occur (e.g., calls, texts, flyers). They highlighted the importance of maintaining parent autonomy and avoiding follow-up that could be perceived as monitoring or an invasion of privacy. Follow-up was generally considered more acceptable if it was optional and part of broader safety check-ins.
Qualitative analysis revealed several themes that cut across adaptations:
Autonomy.
The need to prioritize parents’ autonomy was repeatedly emphasized. Stakeholders indicated that bringing information to parents and letting them make independent decisions about firearm safety would be optimal.
Privacy.
Stakeholders supported adaptations that were focused on maximizing respect for parent privacy, such as allowing parents not to disclose firearm ownership or permitting them to take program resources without clinic staff knowing (e.g., from a basket in a common area).
Communication.
Stakeholders supported the use of nonjudgmental language to help offset concerns that medical providers would be against firearm ownership. Use of a script for how to broach the topic of firearm safety was recommended. Multiple stakeholders commented on the utility of grouping firearm safety with other safety guidance that primary care clinicians provide to families, consistent with the original SC.
Knowledge.
Stakeholders cited several anticipated knowledge gaps for parents and children, including the risk of suicide and other injuries associated with firearms and ways to handle and store firearms safely. While stakeholders often suggested clinicians deliver this information to parents, some stakeholders also referenced the duty of parents to educate their children.
Safe Storage.
In responding to questions about what safe storage means to them, stakeholders noted that safe storage carries a different meaning depending on the person and their circumstances (e.g., whether someone owns a firearm for protection or hunting). However, the general consensus was that safe storage involves preventing unauthorized access to firearms by people who should not have access to them, including children.
Situational Awareness.
Stakeholders commented on the importance of being aware of the location of one’s firearm and cautioned about the possibility of firearm owners forgetting to consider how someone might gain unauthorized access. Several stakeholders indicated that it should not be assumed that children or visitors would be unable to find firearms in a home.
Environment.
A number of environmental factors, including firearm and hunting cultures and the culture of a given clinic or geographic region, were mentioned as critical to consider in the delivery of the adapted program.
Topical Experts Phase: Eliciting Further Feedback on Program Name and Logo
Survey participant demographics were similar across firearm ownership subgroups (Table 2). Parents had children ranging from under one year to 18 years and older. SAFE (Suicide and Accident prevention through Family Education) Firearm was the most preferred name by both firearm owners and non-owners based on best-worst scaling scores (Table 3). Additionally, SAFE Firearm had the highest average acceptability and appropriateness scores across ownership subgroups. There were no significant differences in acceptability, t(335) = .12, P =.91, or appropriateness, t(335) = −.40, P =.69, between firearm owners and non-owners for the winning name.
Table 2.
Survey Participant Demographic Characteristics
| Full Sample | Firearm Owners | Non-Firearm Owners | ||||
|---|---|---|---|---|---|---|
| Program Name Survey Participants | ||||||
| N | 337 | 151 | 186 | |||
| Mean Age (SD), years | 37.50 (7.82) | 36.87 (8.29) | 38.01 (7.40) | |||
| Gender | ||||||
| Female | 67% | 68% | 66% | |||
| Male | 33% | 32% | 34% | |||
| Race | ||||||
| American Indian or Alaska Native | 1% | 1% | 0.5% | |||
| Asian | 6% | 3% | 8% | |||
| Black or African American | 7% | 7% | 8% | |||
| Native Hawaiian or Other Pacific Islander | 0.3% | 0% | 0.5% | |||
| White | 81% | 85% | 79% | |||
| Other | 2% | 3% | 2% | |||
| Multiple | 2% | 1% | 3% | |||
| Ethnicity | ||||||
| Non-Hispanic/Latino | 93% | 92% | 95% | |||
| Hispanic/Latino | 7% | 8% | 5% | |||
| Number of Children, mean (SD) | 1.89 (1.05) | 1.96 (1.09) | 1.83 (1.02) | |||
| Number of Firearms, mean (SD) | N/A | 2.79 (2.68) | N/A | |||
| Program Logo Survey Participants | ||||||
| N | 337 | 149 | 188 | |||
| Mean Age (SD), years | 37.71 (7.78) | 37.03 (8.05) | 38.25 (7.53) | |||
| Gender | ||||||
| Female | 62% | 60% | 63% | |||
| Male | 38% | 40% | 37% | |||
| Race | ||||||
| American Indian or Alaska Native | 1% | 1% | 2% | |||
| Asian | 10% | 7% | 13% | |||
| Black or African American | 9% | 7% | 10% | |||
| Native Hawaiian or Other Pacific Islander | 1% | 1% | 0.5% | |||
| White | 77% | 82% | 73% | |||
| Other | 1% | 1% | 0.5% | |||
| Multiple | 2% | 2% | 2% | |||
| Ethnicity | ||||||
| Non-Hispanic/Latino | 93% | 93% | 94% | |||
| Hispanic/Latino | 7% | 7% | 7% | |||
| Number of Children | 1.85 (.97) | 1.87 (1.02) | 1.83 (.94) | |||
| Number of Firearms | N/A | 2.54 (2.45) | N/A | |||
Note. Number of children can include those > 18. Number of guns included all guns in the home (regardless of who owned them). There were no significant differences on these demographic variables between firearm owners and non-owners. Some percentage totals do not sum to 100% due to rounding.
Table 3.
Top Five Names and Logos Based on Preference Elicitation and Corresponding Acceptability and Appropriateness Ratings, by Firearm Ownership Status*
| Best-Worst Scaling | Acceptability Mean (SD) |
Appropriateness Mean (SD) |
||||
|---|---|---|---|---|---|---|
|
| ||||||
| Names and Logos | Owners | Non-Owners | Owners | Non-Owners | Owners | Non-Owners |
| Name | ||||||
| SAFE Firearm | 0.58 | 0.60 | 4.22 (0.99) | 4.23 (0.94) | 4.18 (1.05) | 4.13 (0.99) |
| Name 2 | 0.16 | 0.19 | 3.45 (1.12) | 3.51 (0.95) | 3.76 (1.07) | 3.84 (0.93) |
| Name 3 | 0.14 | 0.10 | 3.35 (1.27) | 3.32 (1.21) | 3.59 (1.18) | 3.50 (1.13) |
| Name 4 | 0.05 | 0.02 | 3.36 (1.27) | 3.03 (1.13) | 3.22 (1.23) | 3.02 (1.22) |
| Name 5 | 0.03 | 0.09 | 3.11 (1.24) | 3.43 (1.06) | 3.51 (1.17) | 3.74 (1.01) |
| Logo | ||||||
| Selected Logo | 0.26 | 0.24 | 3.77 (1.10) | 3.66 (1.11) | 4.35 (0.77) | 4.21 (0.84) |
| Logo 2 | 0.12 | 0.07 | 3.68 (1.19) | 3.59 (1.12) | 4.28 (0.86) | 4.14 (0.85) |
| Logo 3 | 0.09 | 0.13 | 3.51 (1.14) | 3.63 (1.07) | 4.06 (0.91) | 4.13 (0.84) |
| Logo 4 | 0.09 | 0.07 | 3.54 (1.19) | 3.51 (1.20) | 4.26 (0.80) | 4.26 (0.81) |
| Logo 5 | 0.07 | 0.12 | 3.52 (1.12) | 3.61 (0.96) | 4.12 (0.87) | 4.12 (0.79) |
151 firearm owners and 186 non-firearm owners responded to the name survey. 149 firearm owners and 188 non-firearm owners responded to the logo survey. Best-worst scaling scores reflect the total best frequency minus the total worst frequency. Alternate names and logos are masked due to intellectual property restrictions.
Figure 3 displays the logo that scored highest on appropriateness for firearm owners and second highest for non-firearm owners, while also receiving the highest acceptability rating in both groups. There were no significant differences in acceptability, t(335) = −.83, P =.41, or appropriateness, t(353) = −1.50, P =.13, between groups for the winning logo.
Figure 3.

Grayscale version of top logo selection across firearm owners and non-firearm owners.
DISCUSSION
The primary objective of this study was to adapt SC (now called SAFE Firearm) using an established adaptation framework in order to increase the acceptability of the program, maximize the program-setting fit, and optimize effectiveness for our goal of universal suicide prevention. Via the two stages of the ADAPT-ITT8 process described here, we received valuable confirmatory stakeholder feedback on proposed adaptations that were developed based on previous stakeholder feedback,7,16,22 the behavioral science literature, and best practices for addressing sensitive health topics. Stakeholders were in favor of the majority of our proposed adaptations and supported the program’s aim of employing a harm reduction approach.31 Important themes related to autonomy, privacy, communication, and attention to the broader national environment were also reinforced, consistent with previous work.16,22 Additionally, we were able to demonstrate the potential of the ADAPT-ITT8 framework to facilitate thoughtful and systematic adaptation of a firearm safety program, and the value of online crowdsourcing marketplaces to rapidly and systematically brand programs to maximize their acceptability. Notably, while our adaptation of SC focused on adapting it to be a universal suicide prevention strategy, both firearm-owning and non-firearm owning parents preferred a program name that included “accident prevention,” which aligns with stakeholder feedback on the importance of inclusive branding that broadly emphasizes safety to support universal implementation.
Much of the feedback gathered in the current study confirms findings from prior research,14,32 suggesting that major themes such as privacy are essential and have been appropriately identified and infused into the proposed program adaptations. It will be particularly important to apply these insights to planned future adaptations of SAFE Firearm, and to integrate them into the development and/or refinement of other firearm safety programs, to ensure such programs are as acceptable and effective as possible. Interestingly, the adaptations that evoked equivocal responses were those that related to evidence-based strategies to boost behavior change, such as use of follow-up reminders. As Hoskins and colleagues33 noted when advocating for the application of behavioral economics to understanding firearm storage, “parental decision-making is complex, inevitably value laden, and not cleanly bounded by behavioral science” (p.5). Our findings point to the nuanced factors that may influence decision-making regarding firearm storage and the varied ways in which attempts to intervene upon those factors may be perceived. They also highlight that even universal interventions are delivered in the context of a specific patient-provider relationship, and programs are likely to be most effective when providers are sensitive to each family’s culture, attitudes, and needs. It will be important for future research to continue to engage stakeholders to determine how to increasingly leverage behavioral science in ways that are not only likely to lead to safe firearm storage but are also are perceived as being respectful of autonomy (consistent with motivational interviewing18 approaches), and as minimally intrusive as possible. Emerging options for gathering parent feedback in an economical and efficient way, such as the MTurk methods described here, could facilitate such efforts and coincide with calls in the literature to include parent and patient perspectives in dissemination and implementation efforts and to target marketing of interventions directly to these individuals.34
Our study has several limitations. First, while similar to sample sizes recommended in the literature,24,25 our qualitative interviews included a relatively small number of stakeholders. Nonetheless, thematic saturation was reached around the main proposed adaptations, particularly when considering the current results in conjunction with prior work in this area involving other stakeholder groups.7,16,22 The only exception was the lack of consensus on reminder strategies. Second, given the involved, iterative nature of the ADAPT-ITT process, we present our findings in stages to allow other researchers to replicate this adaptation process more readily and increase the likelihood of successful adaptation and implementation efforts. In future research, it may be helpful to distill or combine certain phases to accelerate the time from adaptation to implementation, in line with calls for rapid implementation science35 to efficiently bridge the research-to-practice gap. It will be important to balance thoughtful, rigorous adaptation with the need to move quickly on deploying critical healthcare interventions in real-world settings.
Conclusions
The present study provides a methodological roadmap for applying an established adaptation method that can guide future programming related to firearm safety as well as other sensitive health topics. This work also shows the benefit of triangulating multiple sources of qualitative and quantitative data to arrive at an adapted program in a confirmatory fashion. The adapted program will be tested in a hybrid effectiveness-implementation trial.
Supplementary Material
What’s New.
We adapted Safety Check, an evidence-based firearm safe storage program delivered in pediatric primary care, to enhance acceptability as a universal suicide prevention strategy. Stakeholders viewed the adapted program, SAFE Firearm, as a promising approach to promoting safe storage.
ACKNOWLEDGEMENTS
We would like to thank our stakeholder participants, the broader FACTS Consortium, and Drs. Brian Ahmedani, Arne Beck, Jennifer Boggs, Joel Fein, and John Zeber for their valuable contributions to this project and related work. This work was supported by the National Institute of Child Health and Human Development (5R24HD087149-03; Cunningham PI) and the National Institute of Mental Health (1R01MH123491-01; Beidas PI). Molly Davis is supported by a National Institute of Mental Health Training Fellowship (T32 MH109433; Mandell/Beidas MPIs). The granting agencies were not involved in the study design; data analysis, collection, or interpretation; the writing of the manuscript; or the decision to submit this manuscript for publication.
The asterisk denotes that Molly Davis and Christina Johnson are co-first authors. This work was supported by the National Institute of Child Health and Human Development Firearm-safety Among Children and Teens Consortium (5R24HD087149-03; Cunningham and Zimmerman PI) and the National Institute of Mental Health (1R01MH123491-01; Beidas PI). Molly Davis is supported by a National Institute of Mental Health Training Fellowship (T32 MH109433; Mandell/Beidas MPIs). The granting agencies were not involved in the study design; data analysis, collection, or interpretation; the writing of the manuscript; or the decision to submit this manuscript for publication. Rinad Beidas receives royalties from Oxford University Press, has provided consultation to the Camden Coalition of Health Care Providers, and currently provides consultation to United Behavioral Health. She also serves on the Optum Behavioral Health Clinical Scientific Advisory Council. Cheryl King serves on the Scientific Advisory Council of the American Foundation for Suicide Prevention. The authors have no other conflicts of interest to disclose.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- 1.Cunningham RM, Walton MA, Carter PM. The major causes of death in children and adolescents in the United States. New England Journal of Medicine. 2018;379(25):2468–2475. 10.1056/NEJMsr1804754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Grossman DC, Mueller BA, Riedy C, et al. Gun storage practices and risk of youth suicide and unintentional firearm injuries. JAMA. 2005;293(6):707–714. 10.1001/jama.293.6.707. [DOI] [PubMed] [Google Scholar]
- 3.Kposowa A, Hamilton D, Wang K. Impact of firearm availability and gun regulation on state suicide rates. Suicide and Life-Threatening Behavior. 2016;46(6):678–696. 10.1111/sltb.12243. [DOI] [PubMed] [Google Scholar]
- 4.Dowd MD, Sege RD, Council on Injury Violence and Poison Prevention Executive Committee. Firearm-related injuries affecting the pediatric population. Pediatrics. 2012;130(5):e1416–1423. 10.1542/peds.2012-2481. [DOI] [PubMed] [Google Scholar]
- 5.The Society for Adolescent Health and Medicine. Preventing firearm violence in youth through evidence-informed strategies. Journal of Adolescent Health. 2020;66(2):260–264. 10.1016/j.jadohealth.2019.11.295. [DOI] [PubMed] [Google Scholar]
- 6.Barkin SL, Finch SA, Ip EH, et al. Is office-based counseling about media use, timeouts, and firearm storage effective? Results from a cluster-randomized, controlled trial. Pediatrics. 2008;122(1):e15–e25. 10.1542/peds.2007-2611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Beidas RS, Jager-Hyman S, Becker-Haimes E, et al. Acceptability and use of evidence-based practices for firearm storage in pediatric primary care. Academic Pediatrics. 2019;19(6):670–676. 10.1016/j.acap.2018.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wingood GM, DiClemente RJ. The ADAPT-ITT model: a novel method of adapting evidence-based HIV interventions. Journal of Acquired Immune Deficiency Syndromes. 2008;47(suppl 1):S40–S46. 10.1097/QAI.0b013e3181605df1. [DOI] [PubMed] [Google Scholar]
- 9.Miller M, Azrael D, Barber C. Suicide mortality in the United States: the importance of attending to method in understanding population-level disparities in the burden of suicide. Annual Review of Public Health. 2012;33:393–408. 10.1146/annurev-publhealth-031811-124636. [DOI] [PubMed] [Google Scholar]
- 10.Azrael D, Cohen J, Salhi C, Miller M. Firearm storage in gun-owning households with children: results of a 2015 national survey. Journal of Urban Health. 2018;95(3):295–304. 10.1007/s11524-018-0261-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Monuteaux MC, Azrael D, Miller M. Association of increased safe household firearm storage with firearm suicide and unintentional death among US youths. JAMA Pediatrics. 2019;173(7):657–662. 10.1001/iamapediatrics.2019.1078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Collins K, Yaffe-Bellany D. About 2 million guns were sold in the U.S. as virus fears spread. The New York Times. April 1, 2020. https://www.nytimes.com/interactive/2020/04/01/business/coronavirus-gun-sales.html. Accessed August 28, 2020. [Google Scholar]
- 13.Uddin SG, O’Connor KS, Ashman JJ. Physician office visits by children for well and problem-focused care: United States, 2012. 2016; https://www.cdc.gov/nchs/data/databriefs/db248.pdf. Accessed August 28, 2020. [PubMed]
- 14.Garbutt JM, Bobenhouse N, Dodd S, et al. What are parents willing to discuss with their pediatrician about firearm safety? A parental survey. Journal of Pediatrics. 2016;179:166–171. 10.1016/i.ipeds.2016.08.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.DeMello AS, Rosenfeld EH, Whitaker B, et al. Keeping children safe at home: parent perspectives to firearms safety education delivered by pediatric providers. Southern Medical Journal. 2020;113(5):219–223. 10.14423/SMJ.0000000000001096. [DOI] [PubMed] [Google Scholar]
- 16.Wolk CB, Van Pelt AE, Jager-Hyman S, et al. Stakeholder perspectives on implementing a firearm safety intervention in pediatric primary care as a universal suicide prevention strategy: a qualitative study. JAMA Network Open. 2018;1(7):e185309–e185309. 10.1001/iamanetworkopen.2018.53Q9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Roszko PJ, Ameli J, Carter PM, et al. Clinician attitudes, screening practices, and interventions to reduce firearm-related injury. Epidemiologic Reviews. 2016;38(1):87–110. 10.1093/epirev/mxv005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Colby SM, Monti PM, Tevyaw TO, et al. Brief motivational intervention for adolescent smokers in medical settings. Addictive Behaviors. 2005;30(5):865–874. 10.1016/j.addbeh.2004.10.001. [DOI] [PubMed] [Google Scholar]
- 19.Aarons GA, Sklar M, Mustanski B, et al. “Scaling-out” evidence-based interventions to new populations or new health care delivery systems. Implementation Science. 2017;12. 10.1186/sl3012-017-064Q-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Stirman SW, Baumann AA, Miller CJ. The FRAME: an expanded framework for reporting adaptations and modifications to evidence-based interventions. Implementation Science. 2019;14. 10.1186/s13012-019-Q898-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Carney T, Chimbambo V, Johnson K, et al. The adaptation of an evidence-based brief intervention for substance-using adolescents and their caregivers. Psychotherapy Research. 2020;30(6):728–738. 10.1080/10503307.2Q19.1656352. [DOI] [PubMed] [Google Scholar]
- 22.Jager-Hyman S, Wolk CB, Ahmedani BK, et al. Perspectives from firearm stakeholders on firearm safety promotion in pediatric primary care as a suicide prevention strategy: a qualitative study. Journal of Behavioral Medicine. 2019;42(4):691–701. 10.1007/s10865-019-00074-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care. 2007;19(6):349–357. 10.1093/intqhc/mzm042. [DOI] [PubMed] [Google Scholar]
- 24.Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82. 10.1177/1525822X05279903. [DOI] [Google Scholar]
- 25.Guest G, Namey E, Chen M. A simple method to assess and report thematic saturation in qualitative research. PLoS One. 2020;15(5):e0232076. 10.1371/iournal.pone.0232076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bradley EH, Curry LA, Devers KJ. Qualitative data analysis for health services research: developing taxonomy, themes, and theory. Health Services Research. 2007;42(4):1758–1772. 10.1111/i.1475-6773.2006.00684.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Charmaz K Grounded theory: objectivist and constructivist methods. In: Denzin NK, Lincoln YS, eds. Handbook of Qualitative Research. 2nd ed. Thousand Oaks, CA: Sage; 2000:509–535. [Google Scholar]
- 28.Rothman EF, Paruk J, Espensen A, et al. A qualitative study of what US parents say and do when their young children see pornography. Academic Pediatrics. 2017;17(8):844–849. 10.1016/j.acap.2017.04.014. [DOI] [PubMed] [Google Scholar]
- 29.Weiner BJ, Lewis CC, Stanick C, et al. Psychometric assessment of three newly developed implementation outcome measures. Implementation Science. 2017;12(1). 10.1186/sl3012-017-0635-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Finn A, Louviere JJ. Determining the appropriate response to evidence of public concern: the case of food safety. Journal of Public Policy & Marketing. 1992;11(2):12–25. 10.1177/0743915692011002Q2. [DOI] [Google Scholar]
- 31.Beidas R, Rivara F, Rowhani-Rahbar A. Safe firearm storage: a call for research informed by firearm stakeholders. Pediatrics. 2020;146(5):e20200716. 10.1542/peds.2020-0716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hinnant A, Boman CD, Hu S, et al. The third rail of pediatric communication: discussing firearm risk and safety in well-child exams. Health Communication. 2019. 10.1080/10410236.2019.170Q883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hoskins K, Paladhi UR, McDonald C, Buttenheim A. Applying behavioral economics to enhance safe firearm storage. Pediatrics. 2020;145(3):e20192268. 10.1542/peds.2019-2268. [DOI] [PubMed] [Google Scholar]
- 34.Becker SJ. Direct-to-consumer marketing: a complementary approach to traditional dissemination and implementation efforts for mental health and substance abuse interventions. Clinical Psychology: Science and Practice. 2015;22(1):85–100. 10.1111/cpsp.12086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Smith J, Rapport F, O’Brien TA, et al. The rise of rapid implementation: a worked example of solving an existing problem with a new method by combining concept analysis with a systematic integrative review. BMC Health Services Research. 2020;20(449). 10.1186/sl2913-020-05289-Q. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.