

Abstract
Background:
Coronavirus disease (COVID-19), an acute respiratory syndrome caused by a novel severe acute respiratory syndrome coronavirus (SARS-CoV-2), has rapidly spread worldwide, significantly affecting the outcome of a highly vulnerable group such as cancer patients. The aim of the present study was to evaluate the clinical impact of COVID-19 infection on outcome and oncologic treatment of cancer patients.
Patient and methods:
We retrospectively enrolled cancer patients with laboratory and/or radiologic confirmed SARS-CoV-2 infection, admitted to our center from February to April 2020. Descriptive statistics were used to summarize the clinical data and univariate analyses were performed to investigate the impact of anticancer treatment modifications due to COVID-19 outbreak on the short-term overall survival (OS).
Results:
Among 61 patients enrolled, 49 (80%) were undergoing anticancer treatment and 41 (67%) had metastatic disease. Most patients were men; median age was 68 years. Median OS was 46.6 days (40% of deaths occurred within 20 days from COVID-19 diagnosis). Among 59 patients with available data on therapeutic course, 46 experienced consequences on their anticancer treatment schedule. Interruption or a starting failure of the oncologic therapy correlated with significant shorter OS. Anticancer treatment delays did not negatively affect the OS. Lymphocytopenia development after COVID was significantly associated with worst outcome.
Conclusions:
COVID-19 diagnosis in cancer patients may affect their short-term OS, especially in case of interruption/starting failure of cancer therapy. Maintaining/delaying cancer therapy seems not to influence the outcome in selected patients with recent COVID-19 diagnosis.
Keywords: Cancer, COVID-19, treatment delay, outcome
Introduction
Coronavirus disease (COVID-19) is an acute respiratory syndrome due to a novel severe acute respiratory syndrome coronavirus (SARS-CoV-2) which bursted in China at the end of 2019.1 COVID-19 quickly spread worldwide and was formally declared a pandemic by the World Health Organization on March 11, 2020.2 Because of the high contagiousness of the infection caused by SARS-CoV-2, associated with significant lethality, a large number of countries approved strict contagion restriction measures. Among European countries, Italy was the first to detect the disease, and it experienced an explosive growth of the contagion.
It seems that cancer patients are more susceptible to COVID-19 because of the immunosuppressive state induced by both anticancer treatment and cancer disease, and their recurrent accesses to the hospital.3 Moreover, cancer patients are regarded as a highly vulnerable group in the COVID-19 crisis. Chinese investigations found that patients with cancer had a higher risk of severe clinical events than those without cancer.4,5 Among cancer patients, those who had undergone recent chemotherapy or surgery had a higher risk of clinically severe events (admission to Intensive Care Unit or death) than those who had not received the treatments.6,7 An ECOG (Eastern Cooperative Oncology Group) performance status of 2 or higher was associated with an increased risk of worse outcome.8
There is an urgent need to understand if COVID-19 infected cancer patients would have distinct clinical courses and worse outcomes, such as death from the infection or severe pneumonia. The choice of delivering standard antitumoral treatments to cancer patients during COVID-19 pandemia is subject to further debate. Moreover, it has been suggested that anticancer immunotherapy could give some hope to protect against COVID-19.9
Hence, a retrospective, observational, single-center study was performed to evaluate the clinical course of COVID-19 infection in cancer patients, and the impact of COVID-19 on anticancer treatment schedules.
Materials and Methods
Patient eligibility
The present study included adult patients with diagnosis of solid cancer, who were consecutively admitted to the Medical Oncology Unit of University Hospital of Parma (Parma, Italy) from February 20, 2020, to April 20, 2020. We censored our study in May 2020, due to the urgent clinical need to acquire useful information about the outcome of cancer patients during COVID-19 emergency.
Patients were eligible if they had cytologically or histologically confirmed diagnosis of any primary cancer, regardless of stage (locally advanced/metastatic disease). Any type of systemic anticancer treatment (chemotherapy, immunotherapy, hormone-therapy, molecular targeted therapy) and radiotherapy were allowed, both planned and current, across different settings (adjuvant/neoadjuvant/advanced). Patients undergoing surgery as exclusive treatment were excluded. Patients who were not on active treatment (ie, follow-up) were included. Radiologic diagnosis of SARS-CoV-2-related interstitial pneumonia by computed tomography (CT) scan and/or nasopharyngeal swab positive for SARS-CoV-2 infection was the inclusion criterion. It has also to be acknowledged that radiologic imaging and/or nasopharyngeal swab were performed only in presence of signs and/or symptoms suspected for COVID-19. All patients provided written informed consent to receive the anticancer treatment. All the patients who were alive at the time of the data collection for the study provided written informed consent to be included in the analysis. The study procedures were in accordance with the Declaration of Helsinki. The study (ID 656/2020/OSS*/AOUPR) was approved by the Local Ethical Committee (Comitato Etico dell’Area Vasta Emilia Nord) on September 24, 2020.
Study design
We conducted a retrospective, observational, single-center study. The primary objective was to describe the clinical characteristic of COVID-19 positive patients with cancer and SARS-CoV-2 infection course. Secondary objectives included (1) to investigate the time between the last administration of any anticancer treatment and the onset of COVID-19 pneumonia and (2) to evaluate the putative modification of the standard course of anticancer treatment due to SARS-CoV-2 infection. An interval of 14 days was used as a cut-off to explore the correlation between the last treatment administration and COVID-19 diagnosis and outcome, according to recently published data.10
We collected data from clinical records regarding patients characteristics (sex, age, Eastern Cooperative Oncology Group Performance Status [ECOG PS], smoking habits, body mass index [BMI], blood type, comorbidities, pharmacologic history), cancer characteristics (primary tumor site, stage, type of treatment, and date of the last administration), COVID-19 features (symptoms, imaging techniques performed for the diagnosis, pneumonia radiologic features, swab results, need of hospitalization, or admission to Intensive Care Unit), and course of cancer treatment (ie, discontinuation, delay or not starting of planned therapy).
Overall survival (OS) was defined as the time from radiologic and/or laboratory COVID-19 diagnosis (whichever occurred first) until death from any cause. Patients without event (death) at the time of data cut-off (May 20, 2020) were considered as censored.
Due to the limited evidence about the topic of our study, when the study was planned, it was not possible to estimate the sample size. We used descriptive statistics to describe the study population characteristics and to estimate the time between the last administration of oncologic treatment and the onset of pneumonia, to evaluate the frequency of discontinuation/delay of therapy. Patients and disease characteristics were described using rates (percentages), median values, and ranges. Comparisons between clinical-laboratory features and COVID-19 outcome were conducted using the χ2 test, contingency table, and Fisher exact test (as appropriate) for categorical variables. Overall survival was estimated using the Kaplan–Meier method, and it was correlated to covariates of interest by log-rank test. The median follow-up was calculated using reverse Kaplan–Meier method.11 All statistical tests were 2-sided, and P < .05 was considered as statistically significant.
The SPSS Statistics 25.0 software (IBM Corporation, NY, USA) was used to carry out the statistical analyses.
Imaging technique
Non-contrast high-resolution computed tomography (HRCT) was performed with either a 128-slice scanner (SOMATOM Definition Edge, Siemens Healthineers, Erlangen, Germany) or a 16-slice mobile scanner on truck (SOMATOM Emotion, Siemens Healthineers, Erlangen, Germany). High-resolution computed tomography images were acquired with patients in supine position during end-inspiration breath-hold, without intravenous administration of contrast media.
The acquisition parameters were set at 110 to 120 kVp, 80 reference mAs, pitch 0.9 to 1.2, and collimation 0.625 to 1.0 mm. Lung images were reconstructed as follows: slice thickness 1.0 mm, increment 0.7 to 1.0 mm, sharp reconstruction algorithm (Bl57 for SOMATOM Definition Edge or B70s for SOMATOM Emotion), lung window (width, 1600 HU; level, –600 HU). Advanced Modeled Iterative Reconstruction (ADMIRE) strength 3 on SOMATOM Definition Edge, filtered back projection (FBP) on SOMATOM Emotion.
Computed tomography reading
Two chest radiologists (M.S., with >10 years of experience; G.M., with 6 years of experience) and 1 radiology resident (R.E.L., with 3 years of experience in chest CT) independently reviewed HRCT scans. The readers were aware that the study population included only cancer patients. Readers were allowed to evaluate previous CT scans available on the local Picture Archiving and Communication System (PACS) for comparison with HRCT performed within the COVID-19 diagnostic path.
Description of the pattern was tabulated into the various HRCT categories of our local COVID-19 protocol,12 and the extent of combined ground glass opacities (GGO) and consolidation was visually scored at the nearest 5% on the whole lungs. Furthermore, all HRCT were categorized accordingly to the structured report proposed by the Radiological Society of North America (RSNA).13
Results
Patient characteristics
Between February 2020 and April 2020, 61 cancer patients with laboratory and/or CT-confirmed SARS-CoV-2 infection were enrolled in the present study. Among them, none was newly diagnosed with cancer. In the same time, 2722 patients with cancer were in charge to our Center. The COVID-19 incidence in our cancer population was 2.2%. Patients’ characteristics are summarized in Table 1 and Figure 1s in the Supplementary Material. Overall, 31 patients (51%) were men and median age was 68 years (range, 36-90 years). Thirty-one patients (51%) were current/former smokers and 27 (44%) had at least one comorbidity among cardiovascular, metabolic, and respiratory disorders. Eastern Cooperative Oncology Group Performance Status was 0 in 34 patients (56%), 1 in 22 patients (36%), and 2 in 5 patients (8%). Median BMI was 26 kg/m2 (range, 17-36). Among patients with available data, the most represented blood type was O (n = 31, 54%). Regarding concurrent medications, 18 patients (29%) were receiving corticosteroids, 15 (25%) were on treatment with angiotensin-converting enzyme inhibitors (ACEi), while 4 (7%) were assuming angiotensin II receptor blockers (ARBs). At the time of enrollment in the present study, most patients (n = 49, 80%) were undergoing anticancer treatment, which consisted of chemotherapy, targeted therapy, hormone therapy, immunotherapy, and radiotherapy in 28 (46%), 13 (21%), 10 (16%), 8 (13%), and 3 patients (5%), respectively. Among different clinical settings, metastatic stage was the most represented (n = 41, 67%) and one-third of our cohort (n = 20, 33%) was made of lung cancer patients.
Table 1.
Clinical characteristics of cancer patients with COVID-19.
| Demographic and clinical characteristics (N = 61 patients) | n (%) | Value (range) |
|---|---|---|
| Sex | ||
| Male | 31 (51) | |
| Female | 30 (49) | |
| Median age (years) | 68 (36-90) | |
| Blood type | ||
| Type O | 31 (51) | |
| Type A | 12 (20) | |
| Type B | 9 (15) | |
| Type AB | 5 (8) | |
| Unknown | 4 (6) | |
| Pre-existing conditions | ||
| Current/former smokers | 31 (51) | |
| Median BMI (kg/m2) | 26 (17-36) | |
| BMI < 25 | 18 (30) | |
| BMI 25-30 | 25 (41) | |
| BMI > 30 | 13 (21) | |
| BMI unknown | 5 (8) | |
| At least one comorbiditya | 27 (44) | |
| Concurrent medications | ||
| Corticosteroids | 18 (29) | |
| ACE-inhibitors | 15 (25) | |
| ARBs | 4 (7) | |
| ECOG type | ||
| ECOG 0 | 34 (56) | |
| ECOG 1 | 22 (36) | |
| ECOG 2 | 5 (8) | |
| Tumor stage | ||
| Metastatic stage | 41 (67) | |
| Non-metastatic stage | 20 (33) | |
| Cancer type | ||
| Lung cancer | 20 (33) | |
| Non-lung cancer | 41 (67) | |
| Anticancer treatmentb | ||
| Chemotherapy | 28 (46) | |
| Targeted therapy | 13 (21) | |
| Hormone therapy | 10 (16) | |
| Immunotherapy | 8 (13) | |
| Radiotherapy | 3 (5) | |
| No ongoing treatment | 8 (13) | |
ACE-inhibitors, angiotensin-converting enzyme inhibitors; ARBs, angiotensin II receptor blockers; BMI, body mass index; ECOG, Eastern Cooperative Oncology Group Performance Status.
Cardiovascular, metabolic, and respiratory disorders.
The sum of % is not 100 because some patients received more than 1 treatment concurrently (eg, chemo-immunotherapy).
Clinical course of SARS-CoV-2 infection
Overall, 57 individuals (93%) experienced a symptomatic infection, which consisted of fever (n = 51, 84%), dyspnea (n = 32, 52%), cough (n = 26, 43%), anosmia, and/or dysgeusia (n = 2, 3%) (Table 2). The SARS-CoV-2 infection was diagnosed by CT scan in 57 patients (93%). Nasopharyngeal swab was performed in 54 individuals (89%), among whom 39 (72% of 54) were positive (Table 2). At the time of diagnosis, considering patients who underwent both diagnostic procedures (CT scan and nasopharyngeal swab; n = 51), 16 patients (31% of 51) had a negative nasopharyngeal swab in the presence of a CT scan suggestive for a SARS-CoV-2 pneumonia. Fifty-two patients (85%) were admitted to the Hospital, and 1 case was relocated to Intensive Care Unit. At the time of data cut-off (May 20, 2020), 30 patients (49%) died, 25 (41%) of whom died due to SARS-CoV-2 infection.
Table 2.
Symptoms and diagnostics.
| Symptomatic patients and diagnosis (N = 61 patients) | n (%) |
|---|---|
| Symptoms | |
| Symptomatic patientsa | 57 (93) |
| Asymptomatic patients | 4 (7) |
| CT scan | |
| Yes | 57 (93) |
| SARS-CoV-2 pneumonia | 46 (87)b |
| Nasopharyngeal swab | |
| Yes | 54 (89) |
| Positive | 39 (72) |
CT, computed tomography; SARS-CoV-2, severe acute respiratory syndrome coronavirus-2.
Fever, dyspnea, cough, anosmia, and/or dysgeusia.
Assessed on 53 patients with CT scan available for revision.
Imaging features of SARS-CoV-2 pneumonia
Eight patients (13.1%) did not have HRCT studies available for imaging review. For the remaining 53 patients, a CT imaging revision was performed, and HRCT categories were defined by the 3 chest radiologists (Table 2s in the Supplementary Material).
The extent of combined GGO and consolidation was ⩽25% for 21 patients, between 26% and 50% for 11 patients and between 51% and 75% for 11 patients. Ten patients had a CT scan negative for the presence of GGO and consolidations. The mean GGO and consolidation extension was 27% (range 4%-75%), median was 30%, and the mode was 20%. The mean of lung lobes involvement was 3.7 and the mode was 4.
According to RSNA score,13 10 patients were negative for pneumonia, 2 had atypical appearance, 9 had indeterminate appearance, and 32 typical appearance. While using our local COVID-19 protocol,12 10 patients belonged to category 1, 4 patients to category 2, and 39 patients to category 3.
Clinico-laboratory-radiologic parameters and outcome
Considering all causes mortality, median OS (mOS) was 46.6 days (95% confidence interval [CI], 37.7-54.0) (Figure 1A). Within 20 days from COVID-19 diagnosis, 40% of deaths occurred. Out of 31 dead patients, 25 died for COVID-19 and 6 due to cancer progression (Figure 1s in the Supplementary Material). Among clinical features, BMI was not significantly related to OS, although a trend toward a worse prognosis was observed in patients with a higher BMI (Figure 1B). Tumor type did not affect COVID-19 outcome (lung vs non-lung cancer, P = .855).
Figure 1.
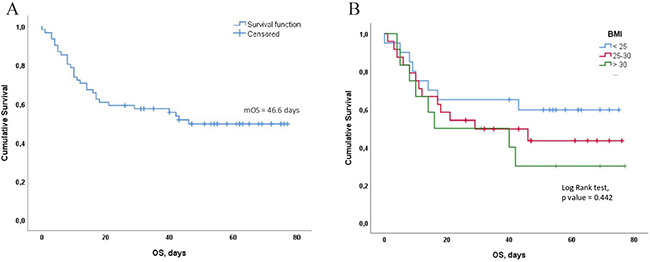
(A) Median OS. (B) Correlation between BMI and OS.
BMI indicates body mass index; mOS, median OS; OS, overall survival.
Concurrent medications did not show significant correlation with outcome (corticosteroids, P = .649; ACEi, P = .670). Nevertheless, it was observed a trend (of OS) in favor of patients who were receiving corticosteroids before COVID-19 diagnosis (P = .649: the 30-day OS after COVID-19 diagnosis was 67% in patients on steroid treatment vs 49% in patients not receiving steroids).
Patients with negative nasopharyngeal swab in the presence of a CT scan suggestive for a SARS-CoV-2 pneumonia showed a trend toward a longer OS compared with the concordant counterpart (mOS not reached [NR] vs 18.0 days, P = .097) (Figure 2A). Other clinical parameters (ie, sex, age, ECOG PS) did not affect the outcome.
Figure 2.

(A) Correlation between CT scan, nasopharingeal swab, and OS. (B) Correlation between blood type and OS.
CT indicates computed tomography; OS, overall survival.
A positive correlation between A blood type and OS was noticed (P = .174) (Figure 2B). Changes in the lymphocytes count are illustrated in Figure 3A. Blood lymphocytes and hemoglobin significantly decreased after COVID-19 diagnosis (median lymphocytes pre vs post: 1270/mm3 vs 900/mm3, P < .001; median hemoglobin pre vs post 12.0 g/dL vs 11.1 g/dL, P = .009). Conversely, LDH values increased after COVID-19 diagnosis (median LDH pre vs post 205 UI/L vs 350 UI/L, P < .001). When stratifying patients according to the trend of laboratory parameters, cases who experienced a decrease in the lymphocytes count had a significantly worse OS compared with the counterpart (mOS 18.0 vs NR days, P = .019, odds ratio [OR] = 4.76 95% CI 1.1-20.3) (Figure 3B). Changes in hemoglobin and LDH levels did not affect OS.
Figure 3.

(A) Changes in the lymphocytes count. (B) Correlation between lymphocytes count and OS.
OS indicates overall survival.
No correlation between radiologic chest CT features and outcome was found.
Impact of SARS-CoV-2 infection on the therapeutic course
Among 53 patients who were under anticancer treatment at the time of COVID-19, 23 (43%) received the therapy within 14 days of COVID-19 diagnosis. We found that OS was not affected by the time between the last antitumor therapy and COVID-19 diagnosis (P = .767). In 59 patients with available data on therapeutic course, 46 (78%) experienced consequences on their anticancer treatment approach, resulting in 29 (49%) interruptions of the ongoing therapy, 12 (20%) delays and 5 (8%) failures of the treatment beginning. Seven patients (13%) out of 53 patients who were on treatment continued the anticancer therapy during COVID-19 without delay/interruption. Among these, 5 cases were receiving either endocrine therapy or immunotherapy or target therapy, which are not immunosuppressive. Concerning treatment delays, the median time from the planned date to the real subsequent administration was 36.0 days (95% CI, 17.3-54.7). Patients who had a consequence on their active anticancer treatment, including interruptions, delays, or starting failures, (n = 46) showed a worse OS compared with whom did not (n = 13), although this finding did not reach the statistical significance (mOS 29.0 vs NR, P = .103) (Figure 4A).
Figure 4.

(A) Correlation between anticancer treatment modification and OS. (B) Correlation between oncology treatment interruption or starting failure and OS. (C) Correlation between treatment delay and OS.
OS indicates overall survival.
Individuals who experienced either the interruption or a starting failure of the oncologic therapy (n = 34) had a statistically significant shorter mOS than those who remained on treatment (delayed or not, n = 25) (mOS 14.0 vs NR days, P < .001, OR 8.51; 95% CI 2.92-24.72) (Figure 4B).
Focusing on patients who continued the anticancer treatment (n = 25), those who delayed (n = 12) the subsequent administration had a significantly longer OS than those who continued according to the pre-planned schedule (mOS NR for both groups, P = .040, OR = 0.30, 95% CI 0.0-45.25) (Figure 4C). All the patients who delayed the treatment had a good ECOG PS (0-1) and were mostly young adults (median age range, 36-73 years) with locally advanced or metastatic cancer under chemotherapy treatment. Forty-two percent of patients who delayed treatment had only one comorbidity among hypertension, diabetes, and chronic obstructive pulmonary disease (COPD). For all of them, lung GGO and consolidation extension diagnosticated by chest CT scan was equal or less than 15%.
We then explored whether the distribution of previously tested clinico-immunologic variables (blood type, age, sex, smoking status, BMI, concordance between CT scans and nasopharyngeal swab, lymphocyte count) was different among the 2 distinct groups based on consequences on anticancer treatment. Significant correlations were documented between blood type (A vs non-A) and consequence on treatment (continued vs interrupted/not started), as a higher proportion of blood type A patients were present among those who interrupted/not started anticancer treatment (Fisher exact test, P = .004). Moreover, a trend toward higher incidence of cases displaying a median age superior to 68 years and a decreased lymphocyte count was observed in the subgroup of patients who interrupted/not started anticancer treatment. Conversely, when we focused on treatment delay, no statistically relevant associations with clinico-immunologic parameters were identified.
A multivariate analysis was not carried out due to the small sample size.
Discussion
In the present study, we described the clinical characteristics and course of COVID-19 in 61 cancer patients from the University Hospital of Parma (Italy). To the best of our knowledge, this is the first study to assess the impact of anticancer treatment delays and/or interruptions during COVID-19 on the short-term OS in cancer patients.
The province of Parma was a high endemic area of COVID-19; as of the data cut-off (May 20, 2020), the overall COVID-19 incidence rate in the general population was 0.7%.14 We accounted a high COVID-19 mortality rate in our population (41%). Moreover, 40% of deaths occurred within 20 days from COVID-19 diagnosis suggesting a rapidly progressive disease course in cancer patients. The mortality rate was higher than that observed in general population (about 2%),6 in previous reports on cancer patients (9%-29%)5,6 as well as in the TERAVOLT study on thoracic cancer patients (33%).7 Nonetheless, it must be highlighted that 67% of our population had an advanced disease, and 86% of patients were on active treatment. The high risk of death for metastatic cancer patients during COVID-19 could be due to known cancer and treatment-related complications, such as anemia, leukopenia, hypoproteinemia, or dyspnea, that worsen after the SARS-CoV-2 infection. The high mortality accounted in our analysis supports the choice of reducing the follow-up visits and postponing the treatments during the pandemia, as suggested by the oncology society guidelines.15 Indeed, a balance of the cost–benefit ratio should be taken into account for each patients, according to age, comorbidities, and treatment impact on outcome.15
As in previous reports,5,10 in our population, lung cancer was the most frequent cancer type (33%).
We did not identify additional risk factors for COVID-19 outcome in our cohort of cancer patients. Body mass index, cancer type, cancer treatment, and previous medications (ACEi and ARBs) did not contribute to the severity of the disease. Nevertheless, we noticed a positive trend for OS in patients undergoing chronic steroid treatment. Of note, on the basis of the current knowledge, the benefit of systemic steroids in COVID-19 infection is limited only to patients who are receiving either invasive mechanical ventilation or oxygen supply.16
Our cancer patients developed COVID-19 clinical features similarly to the general population. Typical symptoms included fever, cough, and dyspnea. Furthermore, patients who experienced the greatest decrease in the lymphocytes count during the course of the infection had a worse outcome, in accordance with previous reports.17,18 Several hypotheses have been advanced to elucidate the mechanism by which SARS-CoV-2 might cause lymphocytopenia.19,20 Zhu et al speculated that the virus could directly infect the lymphocytes and lymphatic organs, resulting in lymphocyte death. In fact, lymphocytes express the coronavirus receptor ACE2 and may be a direct target of the virus.19 On the contrary, Liao et al20 demonstrated that inflammatory cytokines, like tumor necrosis factor-α (TNF-α) or interleukin-6 (IL-6), could induce lymphocyte deficiency during COVID-19 disease. To date, it is still not clear whether cancer treatment could represent an important risk factor for severe SARS-CoV-2 infection due to the risk of reducing lymphocyte count itself. Based on our results, given the worse outcome of patients who experienced a decrease in the lymphocyte count, we assume that anticancer treatments that induce lymphocytopenia should be avoided, when feasible.
A positive correlation between blood group A and OS was found in our study. This result seems contradictory when compared with the findings by Zhao et al,21 who reported a higher risk of acquiring SARS-CoV-2 infection in people with blood group A. To date, the relationship between blood group and the risk of infection or outcome is indeterminate.
Defining the relationship between cancer treatment delay/interruption during COVID-19 and the clinical course of cancer patients is fundamental to assess the risk–benefit balance when planning routine cancer treatment. Our data suggest that anticancer treatment administered within or over 14 days before the diagnosis of COVID-19 did not affect survival in cancer patients. Of interest, in our population, 13% of patients who were on treatment continued the anticancer therapy despite COVID-19, without delay, even though most of them were not receiving chemotherapy or radiotherapy. This is in contrast with the retrospective study by Zhang et al10 (28 patients enrolled), where patient who received anticancer therapy within 14 days preceding COVID-19 diagnosis had an increased risk of severe events (admission to Intensive Care Unit, need for mechanical ventilation, or death).
According to our results, individuals who experienced either an interruption or a starting failure because of COVID-19 infection had a statistically shorter OS than patients who remained on treatment (Figure 4B). This could be due to a severe SARS-CoV-2 infection or an aggressive cancer disease that rapidly changed patients’ clinical condition, thus not allowing the starting of treatment, as supported by the high percentage of deaths occurred within 20 days from COVID-19 diagnosis.
Concerning individuals who continued anticancer treatment during COVID-19, patients who delayed the subsequent treatment administration had a significantly longer OS than those who continued according to the pre-planned schedule. This result might have been influenced by the relatively good conditions of patients who delayed the treatment (mild COVID-19 infection, ECOG PS 0-1, absence of comorbidities). In this specific group, the deferral of anticancer treatment did not compromise the short-term oncology outcome.
Like previously published studies,7,22 we included both patients with laboratory-confirmed SARS-CoV-2 infection by Real-Time Polymerase Chain Reaction (RT-PCR) and radiologically diagnosed cases with lung imaging features consistent with COVID-19 pneumonia. In our population, 16 patients had a negative nasopharyngeal swab in the presence of a CT scan suggestive for a SARS-CoV-2 pneumonia. This finding supports the King’s College Hospital Intensive Care Unit guidelines for critical care that highlighted a greater sensibility of both CT scan and clinical criteria than RT-PCR at an early stage of disease.23 Even though the analysis of nasopharyngeal swab by RT-PCR constitutes the current standard method for the diagnosis of SARS-CoV-2 infection, it is indeed overburdened by the high false negative rate.24,25 Different factors could contribute to a false negative result, such as the technique of sample collection, poor quality/low volume of samples, low viral load, time of collection, handling and storage of the sample, or technical limitations of the test. We could speculate that our patients with a negative nasopharyngeal swab, in the presence of a CT scan suggestive for COVID-19 pneumonia, had a better outcome because their SARS-CoV-2 load was low.
Because cancer patients periodically undergo CT scans, an emerging amount of COVID-19 suspicious imaging is likely to increase in the next months, even in the absence of symptoms. Of note, COVID-19 pneumonia might mimic interstitial pneumonia induced by anticancer treatments, such as immunotherapy.26 In this regard, a differential diagnosis is crucial to implement the best therapeutic strategy. A bronchoscopy could be considered in uncertain cases, as the onset of new GGO in the presence of a negative swab test. Indeed, among different specimens of patients with radiologically confirmed COVID-19, bronchoalveolar lavage fluid showed the highest positive rates (93%).27
We are aware of the limitations of our study, including the retrospective nature and the limited sample size. Moreover, we enrolled only patients with a good ECOG PS (while patients with ECOG 3-4 were directly admitted to the Emergency Department) and, due to the state of emergency, it was not feasible to collect the data about resuscitation of the patients. To overcome the limited sample size point, our group planned to perform a wider multicenter provincial study (ID: 290/2020/OSS/AOUPR—CANCERCOV) aimed at providing a real-life portray of COVID-19 epidemiology in cancer patients. Nonetheless, the in-depth analysis of the various patient characteristics and therapeutic course described in the present study may offer useful hints to manage patients with cancer and COVID-19. However, a larger population is warranted to confirm our findings. Moreover, there are potential confounders related to some of the results, such as the impact of a less aggressive disease on treatment delay and the observation that most patients continuing their anticancer treatment were not having chemotherapy.
Conclusions
Our results suggest that cancer patients are at high risk of developing severe events from COVID-19, including high mortality rate within 20 days from COVID-19 diagnosis. Cancer therapy seemed not to affect the outcome in selected patients, when it was administered closely to COVID-19 diagnosis. Some factors, such as blood type, lymphocyte count, age, BMI, and concordance between CT scans and nasopharyngeal swab, may help the oncologist to personalize the decision about continuation or delaying or stopping the anticancer treatment for each single patient. Our data did not allow to draw definitive conclusions about the impact of different cancer treatments (targeted therapy, chemotherapy, immunotherapy) and cancer type on COVID-19 outcome.
Supplemental Material
Supplemental material, sj-docx-1-onc-10.1177_11795549211043427 for Clinical Impact of COVID-19 Outbreak on Cancer Patients: A Retrospective Study by Sebastiano Buti, Fabiana Perrone, Teresa Zielli, Giulia Mazzaschi, Chiara Casartelli, Alessandro Leonetti, Gianluca Milanese, Mario Silva, Roberta Eufrasia Ledda, Antonino Musolino, Francesca Pucci, Melissa Bersanelli and Marcello Tiseo in Clinical Medicine Insights: Oncology
{kind=link}
Supplemental material, sj-jpg-1-onc-10.1177_11795549211043427 for Clinical Impact of COVID-19 Outbreak on Cancer Patients: A Retrospective Study by Sebastiano Buti, Fabiana Perrone, Teresa Zielli, Giulia Mazzaschi, Chiara Casartelli, Alessandro Leonetti, Gianluca Milanese, Mario Silva, Roberta Eufrasia Ledda, Antonino Musolino, Francesca Pucci, Melissa Bersanelli and Marcello Tiseo in Clinical Medicine Insights: Oncology
Footnotes
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions: SB and MT contributed to the original idea and study planning. SB, FaPe, TZ, GM, CC, AL, GM, MS, REL, AM, FrPu, and MB contributed to the study planning and data acquisition. GM, MS, and REL were responsible for independent and blinded imaging revision. SB, FaPe, TZ, GM, CC, AL, GM, MS, REL, MB, and MT did the analysis and interpretation of data. SB, FaPe, TZ, GM, AL, MB, and MT contributed to drafting the manuscript and revising it critically for important intellectual content; SB, FaPe, TZ, GM, CC, AL, GM, MS, REL, AM, FrPu, MB, and MT contributed to the final approval of the version to be published. SB was responsible for study supervision.
Ethics Statement: This study was approved by the ethic committees of the center (University Hospital of Parma) where it was conducted. Written informed consent was obtained for each subject included and alive at the time of the study initiation and data collecting.
ORCID iDs: Sebastiano Buti  https://orcid.org/0000-0003-0876-0226
https://orcid.org/0000-0003-0876-0226
Teresa Zielli
https://orcid.org/0000-0002-2212-3605
Alessandro Leonetti
https://orcid.org/0000-0001-5415-6703
Marcello Tiseo
https://orcid.org/0000-0002-9553-8465
Data Availability: All datasets generated for this study are included in the manuscript and/or in the supplementary files.
Supplemental Material: Supplemental material for this article is available online.
References
- 1.Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395:507-513. doi: 10.1016/S0140-6736(20)30211-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Adhanom Ghebreyesus T. WHO: director-general’s opening remarks at the media briefing on COVID-19-11 March 2020. https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020.
- 3.Wang H, Zhang L.Risk of COVID-19 for patients with cancer. Lancet Oncol. 2020;21:e181. doi: 10.1016/S1470-2045(20)30149-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Liang W, Guan W, Chen R, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. 2020;21:335-337. doi: 10.1016/S1470-2045(20)30096-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dai M, Liu D, Liu M, et al. Patients with cancer appear more vulnerable to SARS-CoV-2: a multicenter study during the COVID-19 outbreak. Cancer Discov. 2020;10:783-791. doi: 10.1158/2159-8290.CD-20-0422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wu Z, McGoogan JM.Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323:1239-1242. doi: 10.1001/jama.2020.2648. [DOI] [PubMed] [Google Scholar]
- 7.Garassino MC, Whisenant JG, Huang LC, et al. TERAVOLT investigators. COVID-19 in patients with thoracic malignancies (TERAVOLT): first results of an international, registry-based, cohort study. Lancet Oncol. 2020;21:914-922. doi: 10.1016/S1470-2045(20)30314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kuderer NM, Choueiri TK, Shah DP, et al. Clinical impact of COVID-19 on patients with cancer (CCC19): a cohort study. Lancet. 2020;395:1907-1918. doi: 10.1016/S0140-6736(20)31187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chakraborty A, Roy U, Shankar A, Biswas A, Aziz F.Cancer immunotherapy and COVID-19: mind the gap. Asian Pac J Cancer Care. 2020;5:213-218. [Google Scholar]
- 10.Zhang L, Zhu F, Xie L, et al. Clinical characteristics of COVID-19-infected cancer patients: a retrospective case study in three hospitals within Wuhan, China. Ann Oncol. 2020;31:894-901. doi: 10.1016/j.annonc.2020.03.296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Schemper M, Smith TL.A note on quantifying follow-up in studies of failure time. Control Clin Trials. 1996;17:343-346. doi: 10.1016/0197-2456(96)00075-X. [DOI] [PubMed] [Google Scholar]
- 12.Sverzellati N, Milanese G, Milone F, Balbi M, Ledda RE, Silva M.Integrated radiologic algorithm for COVID-19 pandemic. J Thorac Imaging. 2020;35:228-233. doi: 10.1097/RTI.0000000000000516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Simpson S, Kay FU, Abbara S, et al. Radiological Society of North America expert consensus statement on reporting chest CT findings related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA—Secondary Publication. J Thorac Imaging. 2020;35:219-227. doi: 10.1097/RTI.0000000000000524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Protezione Civile. https://www.open.online/2020/04/30/coronavirus-bollettino-protezione-civile-30-aprile/.
- 15.Curigliano G, Banerjee S, Cervantes A, et al. Panel members. Managing cancer patients during the COVID-19 pandemic: an ESMO multidisciplinary expert consensus. Ann Oncol. 2020;31:1320-1335. doi: 10.1016/j.annonc.2020.07.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.RECOVERY Collaborative Group, Horby P, Lim WS, et al. Dexamethasone in hospitalized patients with Covid-19: preliminary report. N Engl J Med. 2021;384:693-704. doi: 10.1056/NEJMoa2021436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tan L, Wang Q, Zhang D, et al. Lymphopenia predicts disease severity of COVID-19: a descriptive and predictive study. Signal Transduct Target Ther. 2020;5:33. doi: 10.1038/s41392-020-0148-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Terpos E, Ntanasis-Stathopoulos I, Elalamy I, et al. Hematological findings and complications of COVID-19. Am J Hematol. 2020;95:834-847. doi: 10.1002/ajh.25829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zhu N, Zhang D, Wang W, et al. China novel coronavirus investigating and research team: a novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382:727-733. doi: 10.1056/NEJMoa2001017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Liao YC, Liang WG, Chen FW, Hsu JH, Yang JJ, Chang MS.IL-19 induces production of IL-6 and TNF-alpha and results in cell apoptosis through TNF-alpha. J Immunol. 2002;169:4288-4297. doi: 10.4049/jimmunol.169.8.4288. [DOI] [PubMed] [Google Scholar]
- 21.Zhao J, Yang Y, Huang H, et al. Relationship between the ABO blood group and the COVID-19 susceptibility. Clin Infect Dis. 2021;73:328-331. doi: 10.1093/cid/ciaa1150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.He W, Chen L, Chen L, et al. COVID-19 in persons with haematological cancers. Leukemia. 2020;34:1637-1645. doi: 10.1038/s41375-020-0836-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.King’s Critical Care. King’s Critical Care: evidence summary clinical management of COVID-19. https://wspidsoc.kenes.com/wp-content/uploads/sites/95/2020/03/KCC-Covid19-evidence-summary.pdf. Updated 2020.
- 24.Woloshin S, Patel N, Kesselheim AS.False negative tests for SARS-CoV-2 infection: challenges and implications. N Engl J Med. 2020;383:e38. doi: 10.1056/NEJMp2015897. [DOI] [PubMed] [Google Scholar]
- 25.Ai T, Yang Z, Hou H, et al. Correlation of chest CT and RT-PCR testing for coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases. Radiology. 2020;296:E32-E40. doi: 10.1148/radiol.2020200642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Dingemans AC, Soo RA, Jazieh AR, et al. Treatment guidance for patients with lung cancer during the coronavirus 2019 pandemic. J Thorac Oncol. 2020;15:1119-1136. doi: 10.1016/j.jtho.2020.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wang W, Xu Y, Gao R, et al. Detection of SARS-CoV-2 in different types of clinical specimens. JAMA. 2020;323:1843-1844. doi: 10.1001/jama.2020.3786. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-docx-1-onc-10.1177_11795549211043427 for Clinical Impact of COVID-19 Outbreak on Cancer Patients: A Retrospective Study by Sebastiano Buti, Fabiana Perrone, Teresa Zielli, Giulia Mazzaschi, Chiara Casartelli, Alessandro Leonetti, Gianluca Milanese, Mario Silva, Roberta Eufrasia Ledda, Antonino Musolino, Francesca Pucci, Melissa Bersanelli and Marcello Tiseo in Clinical Medicine Insights: Oncology
Supplemental material, sj-jpg-1-onc-10.1177_11795549211043427 for Clinical Impact of COVID-19 Outbreak on Cancer Patients: A Retrospective Study by Sebastiano Buti, Fabiana Perrone, Teresa Zielli, Giulia Mazzaschi, Chiara Casartelli, Alessandro Leonetti, Gianluca Milanese, Mario Silva, Roberta Eufrasia Ledda, Antonino Musolino, Francesca Pucci, Melissa Bersanelli and Marcello Tiseo in Clinical Medicine Insights: Oncology