

Abstract
The United States currently ranks last among high-income countries for life expectancy. Since 2014, U.S. life expectancy has declined. By now, these alarming trends are well known to researchers, the public, and policymakers. Nevertheless, there is no consensus among researchers on the causes of the trends, and there has been no serious and effective bipartisan effort to solve the problem. The dominant narrative has implicated Americans’ behaviors, such as smoking, illicit drug use, and suicide; yet, this narrative is misguided and counterproductive. It also exonerates the key structural drivers of behaviors and health, namely the U.S. policy context and the outsized influence of corporations and big donors on those policies. The U.S. policy context has changed dramatically since the 1970s, particularly at the state level. State policies have hyperpolarized along partisan lines. These changes have likely had a profound impact on nearly every aspect of Americans’ lives, cutting short many of them. Consequently, this Essay argues that state policies increasingly affect life and death in the United States. It raises concerns about how the polarization of state policies will further deteriorate the health of many Americans. It points to three significant forces behind the polarization and the growing importance of state policy contexts on Americans’ lives—(1) New Federalism; (2) the new type of state preemption laws; and (3) the emergence of organizations, such as the American Legislative Exchange Council, through which corporations and big donors influence policies.
Introduction
Americans are losing in the game of life expectancy. Since the 1980s, gains in U.S. life expectancy have lagged behind other high-income countries and now the United States ranks last among those countries.1 In 2010 U.S. life expectancy plateaued, and in 2014 it started to decline.2 By 2017 U.S. life expectancy was similar to or shorter than some middle-income countries, including Costa Rica, Cuba, and Lebanon.3 The trends are especially alarming among Americans without a college degree and those living in southern and midwestern states.4
Although scientists have repeatedly reported the troubling U.S. trends for over a decade,5 these trends have become part of national awareness only in recent years. In fact, presidential candidates Hillary Clinton and Bernie Sanders mentioned the trends on national television during a 2016 Democratic debate.6 Clinton remarked, “People with a high school education or less are not even living as long as their parents lived. This is a remarkable and horrifying fact.”7 Sanders followed by implicating disastrous trade policies and decisions of corporate America, stating, “And that’s why this study, which shows that if you can believe it today, for white working class people between 45 and 54, life expectancy is actually going down.”8 However, as those remarks illustrate, the wide reach and long history of the U.S. problem in life expectancy appear to be generally unknown and greatly underappreciated because, in reality, the problem reaches beyond any single demographic group and has deep historical roots.9
Even though the disconcerting trends are well-documented, the robust scientific evidence available to date has not adequately explained these trends.10 Nevertheless, media coverage has consistently fed the narrative that the behaviors of (some) Americans—for example, sedentary lifestyles, smoking, illicit drug and alcohol use, homicides, suicides—lie at the root of the problem.11 For example, a CNN reporter stated,
While there are public health initiatives to address these issues, the negative trends in life expectancy are not likely to change any time soon, because the underlying drivers remain. For example, about 80% of adults don’t meet physical activity guidelines, studies show, and the vast majority of American adults are overweight or obese—some 71%, according to the CDC.12
The narrative conveniently aligns with Americans’ sense of personal responsibility for their own health.13 However, it is misguided and counterproductive, and it exonerates the actual “manufacturers of illness.”14 These manufacturers predominately include political decisions, policies, and corporations. They affect nearly every aspect of Americans’ lives, such as the air they breathe, the food they consume, the money in their pockets, their access to medical care, and, most certainly, their personal health behaviors.15
Some researchers have sought to reorient the narrative and direction of research to put a spotlight on the roles of the U.S. political economy and the dramatic changes in the U.S. policy context in recent decades, most especially at the state level.16 These changes have pulled the social and economic rug out from under many Americans. This Essay argues that state policies increasingly affect life and death in the United States. It raises concerns about how the polarization of state policies will further deteriorate the health and longevity of many Americans.
Section I reviews how and when the scientific evidence on the alarming trends in life expectancy emerged as well as why it took so long for researchers to believe the evidence and for the public to become aware of it. It also compares the U.S. trends to those of other high-income countries to illustrate that the U.S. situation is unique. Section II illustrates how the trends at the national level obscure more dramatic trends at the state level. It describes how numerous state policies affect Americans’ lives. It also shows how the policy polarization across states corresponds with the growing disparities in life expectancy across states. Section III provides a historical backdrop to explain the roots of the polarization, pointing to three main factors: (1) “New Federalism”; (2) the new type of state preemption laws; and (3) the growing influence of corporations, big donors, and organizations such as the American Legislative Exchange Council (ALEC) on U.S. state policymaking. An appreciation of the historical roots is necessary for designing effective policy and communication strategies. Section IV discusses the health consequences of polarization for Americans and the deteriorating position of the country in international rankings of life expectancy. In response to these consequences, Section V provides recommendations for moving forward.
I. Life Expectancy in the United States: The Canary is Dead
This Section begins with an overview of how, when, and for whom the current troubles with U.S. life expectancy unfolded.17 This information is essential for developing informed hypotheses about the causes of the trends. It illustrates that low-educated18 white women have been the canary in the coal mine: their life expectancy started to decline as early as the mid-1980s, three decades before it started to deteriorate for the nation as a whole. Next, this Section highlights key debates in the scientific literature to help explain why a broader recognition of the trends has been slow to emerge.19 It concludes by comparing the U.S. trends to those in other high-income countries to demonstrate that the U.S. trends are unique in many ways.20
A. First Signs of the Problem
Life expectancy is a “social mirror”; it reflects the overall well-being of a population in a single measure.21 Mirroring the many advancements of the twentieth century—such as improvements in standard of living, compulsory schooling, public health interventions like water chlorination, and medicine22—U.S. life expectancy increased from 47.3 years in 1900 to 76.8 years in 2000.23 By 2014 it had climbed to 78.9 years.24 Accompanying those steady gains in longevity were major improvements in health across multiple bodily systems, such as cardiovascular, respiratory, and musculoskeletal systems.25
Despite the favorable historical trends, it is unclear what the future holds. In the last few decades, U.S. life expectancy increased little each year.26 And since 2014, it has declined.27 Specifically, between 2014 and 2017 it fell from 78.9 to 78.6 years,28 effectively erasing all of the gains that had been made since 2009.29 Accompanying those disconcerting trends in longevity, the prevalence of some health issues, such as obesity and diabetes, has increased.30 These recent trends paint a troubling portrait of life and death in the twenty-first century United States.
Disturbing signs about U.S. longevity are not new, however. In 2005, demographer Jay Olshanksy and colleagues published a report in the New England Journal of Medicine warning that life expectancy may soon decline.31 A few years later, in 2008, scientists first reported that it had, in fact, declined for women with at most a high school credential.32 Scores of studies have replicated and refined those findings.33 A crucial point here is that signs that something was amiss emerged over a decade ago; if the troubling trends started back then, so too did the root causes.
B. Skepticism
Those early studies showing that life expectancy had deteriorated among low-educated adults (mainly among white women) received surprisingly little fanfare outside of academic circles.34 One exception was a 2012 study led by Olshansky, which found staggering declines in longevity for whites without a high school credential.35 Between 1990 and 2008 life expectancy of these individuals reportedly fell by 5.3 years for women and 3.3 years for men.36
Nevertheless, the scientific community was slow to embrace those early reports that longevity had declined among low-educated adults. In fact, the findings were met with outright disbelief among many researchers. Skeptics levied one main (and entirely fair) criticism: the studies were comparing apples to oranges.37 They pointed to the fact that the percentage of adults who did not graduate from high school has declined over time, so nongraduates today are a very different group than nongraduates of the past.38 The assumption is that nongraduates today disproportionately include people who suffered from early-life adversities,39 such as congenital health issues, behavioral problems, cognitive limitations, poverty, teenage pregnancy, and parental abuse. Consequently, so the argument goes, those early disadvantages—not the lack of a high school credential—explain why nongraduates today die sooner.40
To examine whether the longevity decline among low-educated adults simply boiled down to this apples-to-oranges error, some researchers altered the way that they measured education in their studies.41 Instead of using people’s actual level of education (e.g., fourteen years of schooling), they used people’s relative level of education (e.g., bottom quintile).42 In practice, this alternative method means ranking people according to the number of years of schooling that they had completed among people born in the same year.43
These newer studies using relative levels of education also found that life expectancy had declined after 1990 among low-educated individuals—again, mainly among white women.44 However, the decline was smaller than previously reported.45 For example, in a 2015 study, economist John Bound and colleagues reported that, between 1990 and 2010, life expectancy of low-educated white women declined by 3.9 years when low-educated was defined as zero to eleven years of education, but it declined by 1.2 years when it was defined as the bottom quartile.46
These newer studies had an unfortunate side effect, however. They seemed to provide a sense of comfort that things were not so bad after all. In fact, things might still be quite good. This side effect stemmed from two issues. First, these studies were comparing their results to the massive decline in life expectancy reported by Olshanksy and colleagues.47 By comparison, declines of approximately one year reported in the new studies might seem like good news and were sometimes couched as such.48 For example, the 1.2-year decline was characterized as “modest.”49
The second issue concerned inconsistencies in what is considered a meaningful decline in life expectancy. It is helpful to put these numbers in perspective. One way to do that is to consider the number of years in which white women’s life expectancy would change if major causes of death, such as diabetes, were completely eradicated.50 If all deaths due to diabetes were eliminated, white women’s life expectancy would increase by just 0.26 years.51 If their deaths due to breast cancer were eliminated, the estimated gain in life expectancy is 0.59 years.52 The estimated gain is also 0.59 years for stroke, 0.41 years for Alzheimer’s disease, and 0.81 years for lung cancer.53 The only cause of death whose total elimination would raise white women’s longevity by 1.2 years or more is coronary heart disease (a gain of 2.2 years).54 Clearly then, even a seemingly small decline—let alone a 1.2-year decline—in life expectancy is truly alarming.
C. Recognition of the Problem
It took until late 2015—nearly eight years and dozens of replication studies after the decline was initially reported—for skepticism about the decline in life expectancy among low-educated adults to wane. Two events were instrumental. The first was a study published in December 2015 by economists Anne Case and Angus Deaton that corroborated earlier studies55 and received unprecedented attention from scientists and the media.56 The second event occurred a year later when the U.S. Centers for Disease Control and Prevention reported that life expectancy for the nation declined from 78.9 to 78.8 years between 2014 and 2015.57 With the country as a whole showing signs of trouble, it seemed that something real was indeed happening.
While scientists were heatedly debating whether the longevity decline among low-educated adults was real, the machinery of injustice and premature death kept operating full steam ahead. In fact, the troubling signs are now seen in more segments of the population. Demographer Isaac Sasson recently reported that life expectancy among whites has continued to decline for those with zero to eleven years of schooling, but it has also started to decline for high school graduates and those who attended college but did not obtain a four-year degree.58
D. Is the United States Unique?
Are the troubling trends in life expectancy also occurring in other high-income countries? Has the United States’ international ranking in life expectancy changed? What do the answers imply about the reasons for the trends and inequalities in U.S. life expectancy? To glean insights into those questions, this Part provides an overview of the U.S. trends in an international context.
The United States ranks forty-fifth in the world in terms of life expectancy at birth.59 In 2017 Americans could expect to live 78.5 years on average, which is more than four years shorter than people in Italy, Spain, Switzerland, Luxembourg, Singapore, Hong Kong, and Japan.60 If the United States is ranked only against comparable high-income countries, it is in last place.61 In fact, a recent analysis of eleven high-income countries reported that the United States not only had the lowest life expectancy, it also had the highest infant and maternal mortality rates despite spending roughly twice as much as those countries on medical care.62 Even more sobering, the United States has a similar or shorter life expectancy than some middle-income countries: in 2017, U.S. life expectancy was similar to Albania (78.3 years), Cuba (78.7 years), and Lebanon (78.8 years).63 The future does not look much brighter. By 2040 the United States is projected to make fewer gains than other countries and fall more than any other high-income country to sixty-fourth place.64
The downward fall of the United States in international rankings of life expectancy is not a recent phenomenon, however. It began decades ago, as shown in Figure 1.65
Figure 1.
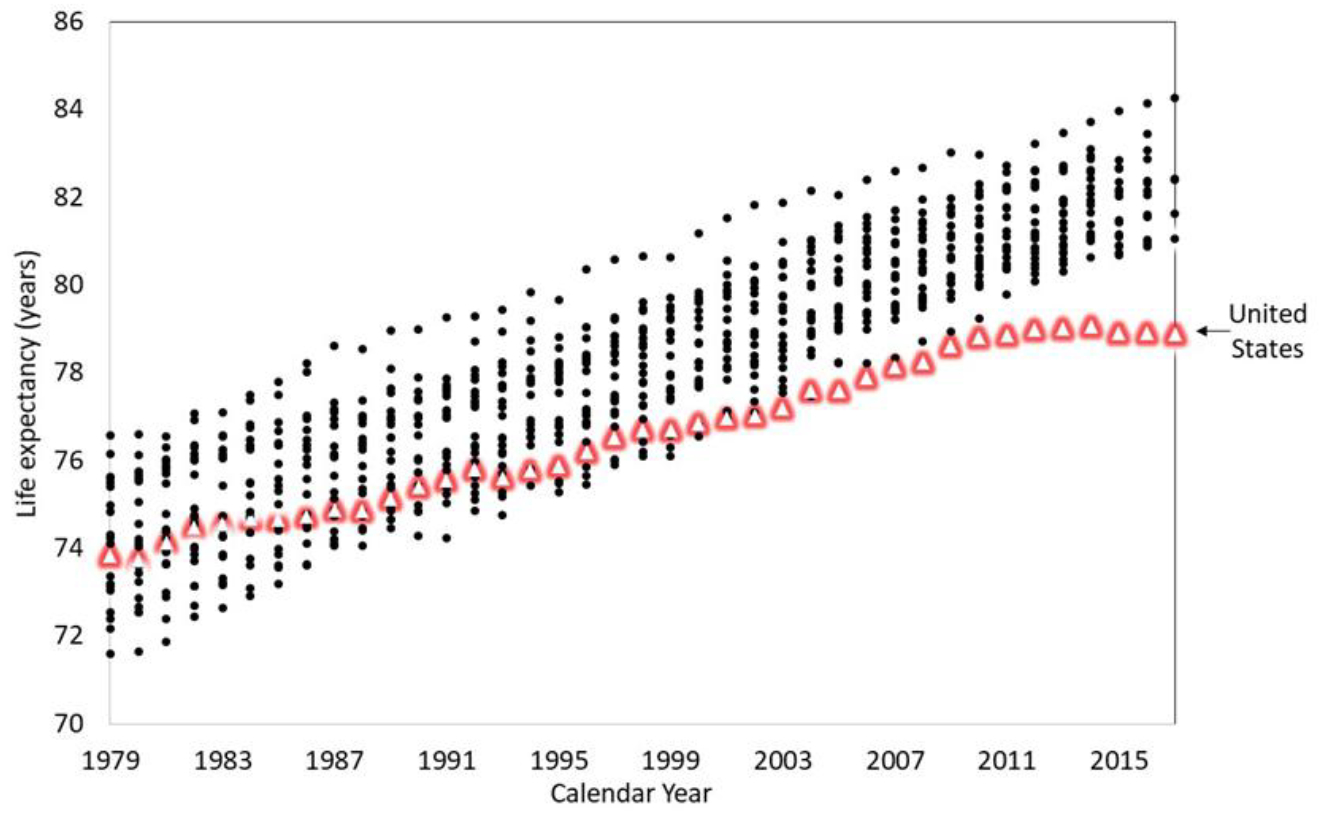
Life Expectancy in Twenty-Two High-Income Countries, 1979–2017
Each vertical set of dots in the figure marks the life expectancy twenty-two high-income countries, with the United States identified as the triangles. The figure illustrates that, around 1980, U.S. life expectancy was roughly in the middle of the twenty-two countries. Subsequent U.S. gains have lagged behind other countries. An important but often unrecognized fact is that U.S. women were the first to experience slower gains; men followed suit around 2010.66 After 2010, U.S. life expectancy of both women and men took a notably different trajectory than did other countries, first with a stagnation and then, after 2014, a decline.67
To be clear, the United States was not alone in experiencing a longevity decline in recent years.68 A study by demographers Jessica Ho and Arun Hendi examined eighteen high-income countries and found that, between 2014 and 2015, life expectancy declined in twelve countries for women and eleven countries for men.69 However, most countries that experienced these declines also saw increases during 2015 and 2016 that more than compensated for that prior decline.70 The United States and the United Kingdom, to a lesser extent, were notable exceptions.71
Although there is no consensus on why gains in U.S. life expectancy have not kept pace with other high-income countries since the 1980s, several hypotheses have been put forth. A 2013 report that the National Research Council commissioned pointed to five hypotheses: (1) public health and medical care systems, (2) behaviors such as smoking, (3) social and economic factors, (4) physical and social environments, and (5) policies and social values.72 Scientific studies and the public narrative have focused mostly on the first three explanations. All three appear to play some role but do not adequately explain the U.S. longevity disadvantage. For example, researchers have pointed out that the U.S. disadvantage exists even among individuals with medical insurance.73 Additionally, historically high smoking rates among Americans cannot explain why the disadvantage is pronounced below age fifty (when smoking-related deaths are rare).74 Further, even high-educated and high-income Americans are less healthy and die sooner than peers in many other high-income countries.75
Scientific studies have identified several additional features of the U.S. longevity disadvantage.76 It does not appear to be due to the demographic diversity of the population. In fact, non-Hispanic white Americans, who are one of the most advantaged groups in the United States, die sooner than their peers in many other countries.77 Another important and telling feature is that the U.S. disadvantage starts at an early age, well before individuals have the agency to make choices about their lives.78 For example, a 2011 study found that among zero- to three-year-old children, 7.5% of American girls had asthma compared to 1.8% of English girls.79 Among four- to eleven-year-old children, 12.1% of American girls were obese compared to 7.3% of English girls.80 Taken together, evidence indicates that Americans’ longevity disadvantage is multifaceted, systemic, and affects all ages and population groups—although it is most pronounced among marginalized populations, such as women, persons of color, and low-educated individuals.
Nevertheless, much scientific and media attention persists in its focus on Americans’ lifestyle behaviors as the explanation for the U.S. crisis.81 A 2018 study reported that behaviors related to “external causes” (e.g., drug overdoses, homicides, suicides) greatly contributed to the U.S. shortfall in life expectancy between 2014 and 2015.82 Although those findings are indisputable, it is essential to recognize that, even if Americans’ behaviors fully explained why they die sooner than people in peer countries, such an explanation would be woefully inadequate and misguided. As public health scholars Mauricio Avendano and Ichiro Kawachi argued, “[A]n approach that focuses solely on behavioral differences is impoverished by its focus on ‘proximal’ individual choices.”83 It does not explain why Americans more often engage in unhealthy behaviors, and it neglects the central role of social, economic, legal, and policy contexts that drive those behaviors.84
In fact, some researchers have explicitly implicated the U.S. policy environment as a major contributor to the disconcerting trends and inequalities in U.S. life expectancy.85 Professor Clare Bambra and colleagues recently argued that policies and politics are “the causes of the causes of the causes of geographical inequalities in health.”86 Compared to countries in Europe, the social safety net in the United States has historically been much weaker.87 The United States has weaker social transfers, such as unemployment compensation and sick pay; fewer redistributive policies, which exacerbates economic inequalities; and limited eligibility for economic supports by relying heavily on means-tested programs.88 In addition, Bambra and colleagues pointed out that Americans’ unhealthy behaviors can be partly linked to the country’s “limited regulation of unhealthy products, such as tobacco, alcohol and ultra-processed food and drinks, and the industries that produce and market these products.”89 The next Section explains how the U.S. policy context, focusing on states, increasingly influences Americans’ life and death.
II. Role of State Policies in Shaping Life and Death
Progress in rectifying the troubling trends in U.S. life expectancy requires shifting the unit of analysis from the country as a whole to its states and examining their changing policy contexts. National analyses of life expectancy obscure substantial differences across states. This Section describes trends in longevity across states and how they have diverged during the last forty-five years.90 Then it reviews scientific evidence on how state policies affect population health and longevity.91 Finally, this Section illustrates how states’ policy contexts have polarized since the 1970s.92
A. Trends in Life Expectancy Across States
In 2017 life expectancy in the fifty states ranged from 74.7 years in West Virginia93 to 81.6 years in Hawaii.94 If West Virginia were a nation, it would be ranked ninety-third in the world in terms of life expectancy, right in between Lithuania and Mauritius.95 In fact, life expectancy in Mississippi falls below that of many middle-income countries.96 It is even below four countries that are classified as lower middle income: Vietnam, Morocco, Honduras, and Tunisia.97 If Hawaii were a nation, it would be ranked twenty-third in the world in terms of longevity.98 Life expectancy in Hawaii is within 0.8 years of world leaders such as Sweden, Iceland, Ireland, New Zealand, and Canada.99
Life expectancy has differed across states for as long as such data have been recorded; however, those differences have been widening since around 1980, particularly for women.100 As an illustration, Figure 2 shows trends in life expectancy for each state from 1970 through 2014.101
Figure 2.
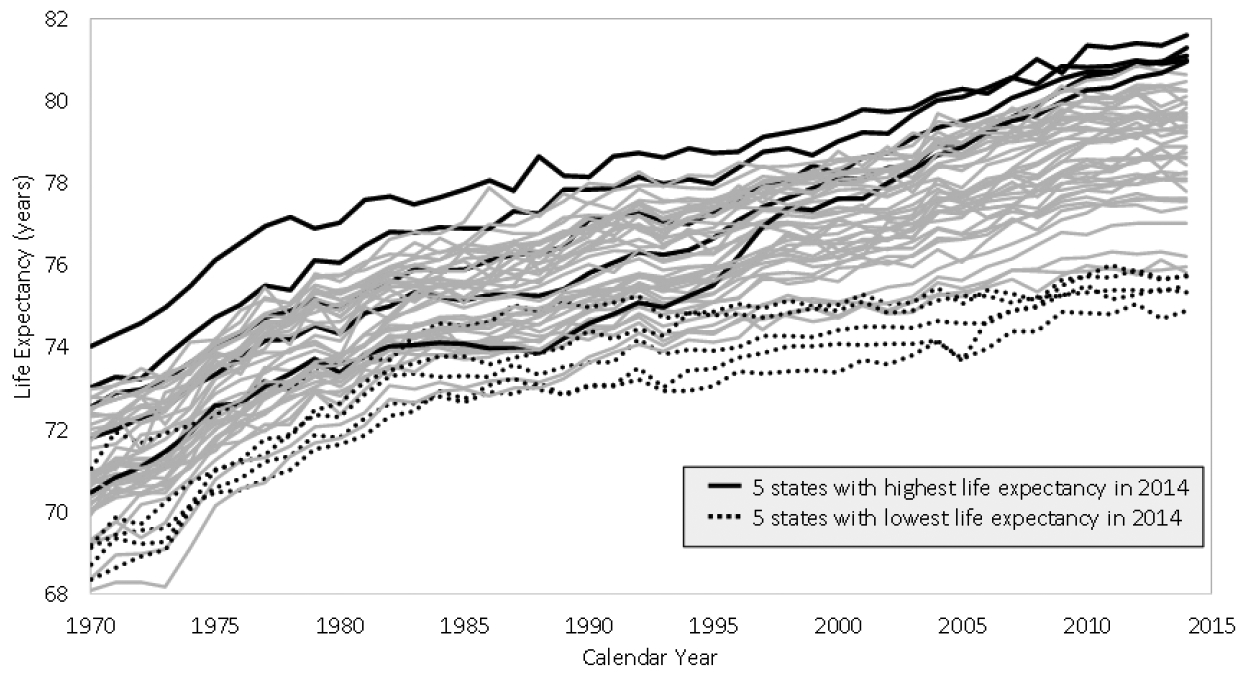
Trends in Life Expectancy by U.S. State, 1970–2014
During the 1960s (not shown) and 1970s, life expectancy was actually becoming more equal across states.102 The smallest range in life expectancy across states was 4.9 years in 1984.103 Since the 1980s, the range has expanded.104 By 2014 it had increased to 6.7 years.105
Figure 2 also illustrates that states have experienced vastly different trajectories. For instance, in 1970, life expectancy was 71.1 years in Oklahoma and 72.6 years in Connecticut, a 1.5-year difference.106 By 2014 life expectancy was 75.7 years in Oklahoma and 81.1 years in Connecticut, a 5.4-year difference.107 The substantial gains in life expectancy in Connecticut propelled them to be among the top five states in 2014, leaving behind Oklahoma, which fell into the bottom five.108 Figure 2 demonstrates that the relatively stagnant national-level trend in longevity in recent years mask highly dynamic and diverging trends at the state level. It also suggests that the life expectancy crisis in the United States is not so much a national crisis (at least not yet) as it is a crisis within certain states. Consequently, explaining and rectifying the alarming trends and inequalities in U.S. life expectancy demands that attention be directed to the states. What lessons can be drawn from states like Connecticut that rose to the top during the past forty-five years and from states like Oklahoma that made little progress?
B. U.S. State Policies Affect Well-Being
State policies play a decisive role in Americans’ lives, affecting opportunities for employment, economic well-being, family relationships, education, safe and affordable housing, lifestyles, medical care, and so on. State policies also shape the social determinants of health.109 As an example, states can shape the importance of gender, race, sexuality, and educational attainment on health through policies such as those aimed to address gender discrimination in pay and paid family leave, civil rights, labor protections, and Medicaid.110 This Part highlights a handful of the state policies of which effects on population health are well established.
State policies such as minimum wage, paid leave, and earned income tax credit (EITC) affect economic well-being, stress, and health behaviors that, in turn, shape health. Raising the minimum wage reduces infant mortality, the risk of low birth weight and preterm birth, adolescent fertility, smoking, body mass index, and heart disease mortality among working-age adults.111 Studies of states that have mandated paid leave find a host of positive effects on population health.112 It increases maternal attachment to the labor force, reduces poverty rates after childbirth, increases breastfeeding, and consequently improves birth outcomes and infant health.113
States influence Americans’ lifestyles and behaviors through multiple policies, such as tobacco control, nutrition labeling, Supplemental Nutrition Assistance Program (SNAP) eligibility, marijuana legalization, and public transportation.114 As one example, excise taxes on tobacco sales and indoor clean air laws are particularly powerful mechanisms for reducing smoking,115 the leading preventable cause of death.116 As another example, SNAP has been shown to improve health-related outcomes for infants and adults by reducing food insecurity and freeing up resources that can be used to purchase other necessities such as medical care.117
State policies also affect family structures and psychological well-being, which both have significant implications for health.118 For instance, more restrictive abortion laws elevate women’s risk of poverty, unemployment, anxiety, poor physical health, and violence from the man involved in the pregnancy.119 Further, whether or not state civil rights protections for marginalized populations exist has consequences for population health.120 For example, residing in a state that has weak or no protections for lesbian, gay, and bisexual populations increases the risk of generalized anxiety disorder, posttraumatic stress disorder, and dysthymia among these populations.121
State policies are disproportionately relevant for marginalized populations, including women, persons of color, and low-educated adults. To illustrate, women comprise the majority of workers making minimum wage or less, Medicaid enrollees, and EITC recipients.122 In fact, state policy contexts may be more important in shaping women’s risk of dying than men’s.123 State contexts also appear to have disproportionate consequences on the health and longevity of low-educated adults but have little effect on college-educated adults.124 In sum, state policies touch nearly every aspect of people’s lives, providing both opportunities and risks for living long, healthy lives.
C. U.S. State Policies Have Hyperpolarized Since the 1970s
In a 2018 study, political scientist Jacob Grumbach documented the polarization in U.S. state policy contexts along partisan lines during the 1970–2014 period.125 By 2014 the polarization was so striking that he characterized it as “hyper-polarization.”126 He collected information on 135 policies for each state and year from 1970 through 2014.127 The policies spanned sixteen major domains: “[A]bortion, campaign finance, civil rights and liberties, criminal justice, drug policy, education, environment, gun control, health and welfare, housing and transportation, immigration, labor (private sector), labor (public sector), LBGT rights, taxes, and voting.”128 He summarized the information into a “policy liberalism” score for each state and year.129 The scores ranged from zero to one, where zero indicated that a state had the most conservative configuration of policies in that year across all states and years; one indicated the most liberal configuration.130 Grumbach defined liberal policies as those that (1) “expand the use of state power for economic regulation and redistribution, or to increase or protect the rights of historically marginalized groups in society,” and (2) “restrict the use of state power for the punishment of deviant social behavior”; he defined conservative policies as the opposite.131
Using data from Grumbach, Figure 3 shows how states’ policy contexts have polarized.132
Figure 3.
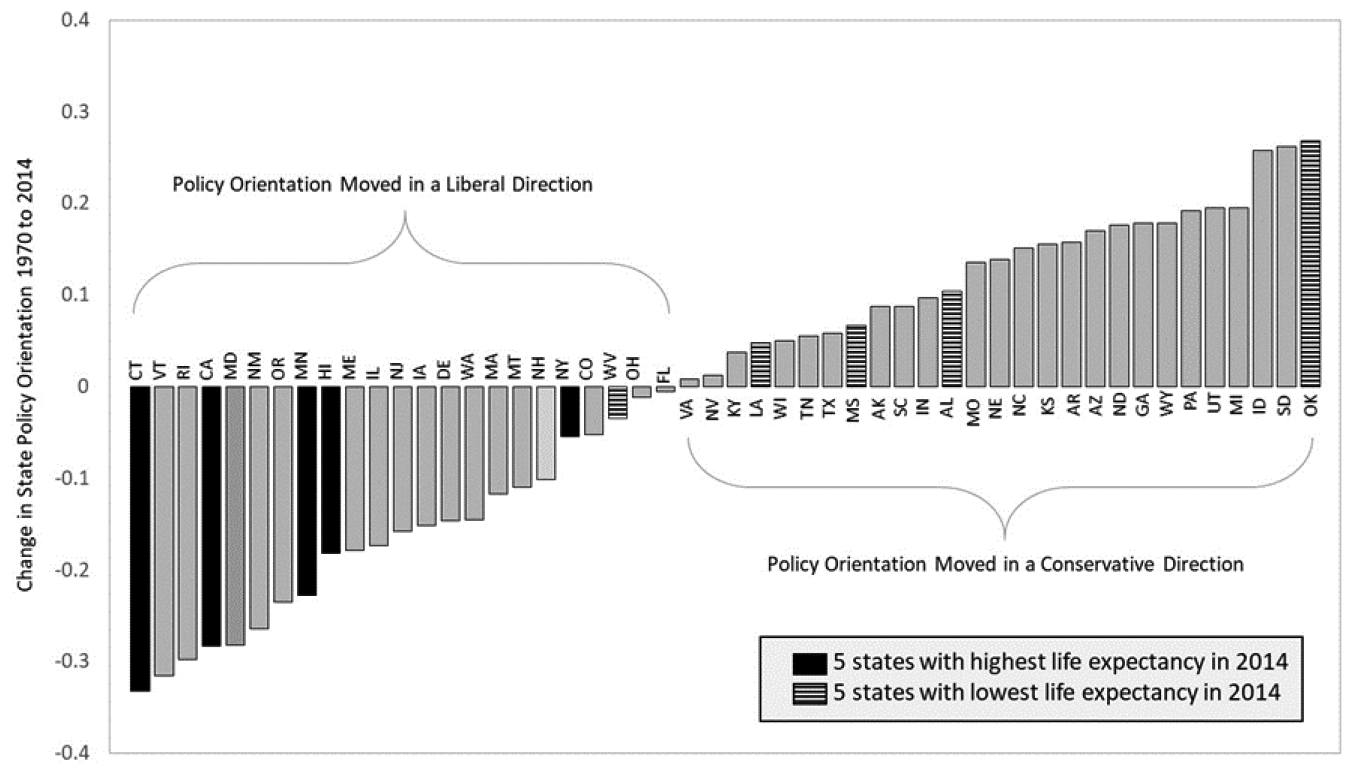
Policy Polarization Across States, 1970–2014
Each bar shows how a state’s overall policy liberalism score changed from 1970 to 2014. The change in the score is negative for states who moved their overall policy context toward a more liberal direction. The change in the score is positive for states who moved in a conservative direction. Figure 3 shows considerable movement among states in either a liberal or conservative direction. It also hints that the polarization in states’ policies may undergird the growing divergence in states’ life expectancies. The five states with the highest life expectancy in 2014 are identified by black bars. The policy contexts of those states moved in a liberal direction between 1970 and 2014. The five states with the lowest life expectancy in 2014 are identified by striped bars; they tended to become more conservative during the time period.
Since the 1970s, many states transitioned from having a mix of policies that were liberal in some domains and conservative in others to a mix that is either liberal or conservative across most or all domains.133 Again, this can be seen using the data Grumbach compiled.134 He calculated a zero to one score for each of the sixteen policy domains just as he had for the states’ overall policy orientations.135 In 1970 there was little relationship between how liberal or conservative a state was on one policy domain and how liberal or conservative it was on another domain.136 For instance, at this time there was no relationship between how conservative or liberal a state was on its immigration-related policies and its gun control policies: the correlation between these two policy domains was -0.01.137 By 2014 the correlation had increased to 0.56, meaning that states with conservative immigration-related policies also tended to have conservative gun control policies, and the same for those with liberal policies. As another example, the correlation between states’ abortion policies and their labor policies also grew much stronger, from 0.27 in 1970 to 0.70 in 2014.
What are the roots of this polarization? What forces explain the dramatic divergence in the policy direction of states and the “packaging” of either conservative or liberal policies after the 1970s?
III. Roots of State Policy Polarization
The policy contexts of states have become more polarized and central in shaping Americans’ lives since the late 1970s. States have gained considerable policymaking authority in large part through two policy movements—devolution138 and preemption139—and an infusion of big money from corporations and big donors via policy-influencing organizations such as ALEC.140 This Section reviews these three forces.
A. States Gained Policymaking Authority from the Federal Government
The first movement, coined the “devolution revolution” or “New Federalism,” transitioned certain authorities from the federal government down to the states.141 The movement started with President Richard Nixon but became a defining feature of President Ronald Reagan’s political ideology and administration.142 It returned much of the policymaking power to the states that they had lost as a result of President Franklin Roosevelt’s New Deal and President Lyndon Johnson’s Great Society.143 The Reagan administration cut federal aid to states, and the aid it did provide increasingly came in the form of block grants instead of categorical grants.144 That is, instead of providing funds to support specific programs, such as welfare or Medicaid, with strings attached, the federal government gave states more discretion on how to spend the funds and loosened the strings that were previously attached to them.145 The devolution revolution was re-energized after the historic 1994 midterm elections, when Republicans gained control of the House for the first time in forty years, with Speaker Newt Gingrich at the helm.146
Warnings about the profound consequences that this decentralization of policymaking authority would have on the United States were prescient. Sharing his own concerns in a 1995 New York Times article, Senator Daniel Patrick Moynihan recounted testimony given before the Senate Finance Committee by Richard P. Nathan, Director of the Rockefeller Institute of Government.147 According to Moynihan, Nathan claimed that the devolution revolution would be far more consequential than the Great Society and underscored his point by stating, “As economist Joseph Schumpeter once said … it is in fiscal issues like this that you can hear the thundering hoofbeats of history.”148 Consistent with those predictions, the decentralization of political authority set in motion wildly disparate economic and policy contexts across states, particularly those related to economic safety nets.149
B. States Removed Policymaking Authority from Local Governments
The second policy movement transitioned certain policymaking authorities from local to state governments through the increasing use of state preemption laws.150 These laws forbid or limit local governments from creating legislation on any number of issues, such as antismoking ordinances, paid sick days, or hydraulic fracking.151 Industry lobbyists and ALEC have pushed state preemption laws for decades on the grounds that they prevent a patchwork of local regulations.152 Since the 1980s, the tobacco industry has been successful in lobbying states to stop the growing tide of local antismoking legislation by preempting localities from implementing such legislation.153 Similarly, since the 1990s, the National Rifle Association (NRA) has been successful in lobbying states to preempt local gun control laws.154 In fact, the NRA’s Institute for Legislative Action openly boasted in 2019 that “[t]he NRA has led the fight to enact state preemption laws across the country to ensure uniformity in state gun laws.”155
The past decade has seen a rapid expansion of state preemption laws as a tool to prevent progressive-leaning local legislation and appease trade associations, corporate interests, and conservative donors.156 Legal scholar Richard Briffault asserted that this new era of preemption is closely tied to the political polarization between conservative state governments and liberal local governments.157 Accordingly, Briffault explained that, rather than harmonizing state and local law (historically a main function of preemption), preemption increasingly consists of “sweeping state laws that clearly, intentionally, extensively, and at times punitively bar local efforts to address a host of local problems.”158 For example, after the City of Birmingham passed legislation to raise the city’s minimum wage from $7.25 to $10.10 per hour, the Alabama state legislature immediately reacted by preempting municipal authority to raise the minimum wage and then returned the wage back to $7.25 per hour.159 The fact that predominately white state lawmakers preempted a law that would have disproportionately benefitted Black Birmingham residents was not lost on the U.S. Court of Appeals for the Eleventh Circuit, which criticized the preemption as “rushed, reactionary, and racially polarized.”160
The emergence of this new type of preemption over the last decade means that people living in some states (mainly those in Republican-dominated state governments) have seen opportunities for economic well-being and health stripped away by their state legislators, while people living in many other states have experienced the opposite.161 For example, as of 2000, only two states (Louisiana and Colorado) preempted their localities from raising the minimum wage and no state preempted localities from mandating paid leave.162 By 2019, twenty-six states had preempted localities from raising minimum wages and twenty-three states had preempted them from mandating paid leave.163 Given the well-established benefits of policies such as these on population health, states that preempt localities from enacting these policies are also limiting their constituents’ well-being and health, as Part II.B discusses.
Until recently, the potential impact of preemption on population health had gone largely unnoticed among public health researchers. In 2017, legal scholars Jennifer Pomeranz and Mark Pertschuk published an important article that alerted researchers to the “[s]ignificant and [q]uiet [t]hreat to [p]ublic [h]ealth.”164 Since then, evidence on the threat for public health has been slowly emerging. For instance, a 2017 policy brief found that states that have more actively engaged in the new type of preemption during the past decade have made the smallest gains in life expectancy.165
C. The Influence of Corporations, Big Donors, and the “Troika” on States
In his 2019 book, State Capture, political scientist Alexander Hertel-Fernandez outlined how the policy environments of many states—particularly conservative states—since the mid-1980s have been intentionally molded by the money and power of three policy-influencing organizations.166 He referred to these three organizations collectively as the “troika”: ALEC, State Policy Network, and Americans for Prosperity.167 The troika and its funders (mainly corporations and wealthy donors) have had profound consequences on U.S. state policies.168
According to Hertel-Fernandez, ALEC is the dominant player within the troika.169 As a coalition of (mainly conservative) politicians, businesses, wealthy donors, and activists, it writes model bills that are corporate friendly and socially conservative and then persuades state legislatures to enact them.170 ALEC’s focus on states rather than national or local politics was a deliberate and strategic move.171 States are more vulnerable to pressures from corporations because of fears that the companies will move out of the state.172 Moreover, it is easier to mold state-level than national-level policies because of the gridlock in Washington, D.C., and to do so under the radar because media attention is generally focused on national politics.173 ALEC is also closely tied to the two other forces proposed in this Essay to undergird state policy polarization: Reagan’s devolution revolution174 and preemption.175
ALEC started having real success in implementing its corporate-friendly policy agenda within many states during the mid-1980s.176 A longstanding and central objective of ALEC and other troika members is the dismantling of labor rights and power through model bills such as ALEC’s Right to Work Act.177 Starting in the mid-2000s, ALEC ramped up its focus on enacting conservative policies related to immigration, voting access, and gun rights (such as the castle doctrine or stand-your-ground laws).178 Hertel-Fernandez explained that ALEC’s success really took off after the 2010 midterm elections, with an unprecedented and striking pace in which (mainly Republican) states began enacting a nearly identical set of hardline conservative policies.179 In sum, ALEC’s policy priorities have been stamped on the state policy landscape, sharpening the divide between states and their policy priorities.180 Additional evidence on the outsized influence of organized probusiness groups like ALEC on U.S. policymaking came from political scientists Martin Gilens and Benjamin Page.181 They found that, between 1981 and 2006, the two main forces driving U.S. policymaking boiled down to very wealthy individuals and organized interest groups that represent business interests, and that the average American had “only a minuscule, near-zero, statistically non-significant impact upon public policy.”182
IV. Consequences of State Policy Polarization
Polarization means that the state in which one resides increasingly influences their economic opportunities, well-being, and health.183 Compare Mississippi and New York for example. As this comparison shows, in 1970, these two states differed little in many policies that are well known to affect health.184 Minimum wage was $1.60 in MS185 and $1.85 in NY,186 state excise tax on tobacco sales was $0.09 per pack in MS and $0.12 per pack in NY,187 and neither state offered their own EITC.188 By 2016, minimum wage was $7.25 in MS189 but $9.70 in NY,190 state excise tax on tobacco were just $0.68 per pack in MS but $4.35 per pack in NY,191 and NY but not MS offered their own EITC.192 The polarization may explain why some states have made much greater gains in life expectancy than other states. In fact, Figure 4 suggests such a relationship.193
Figure 4.
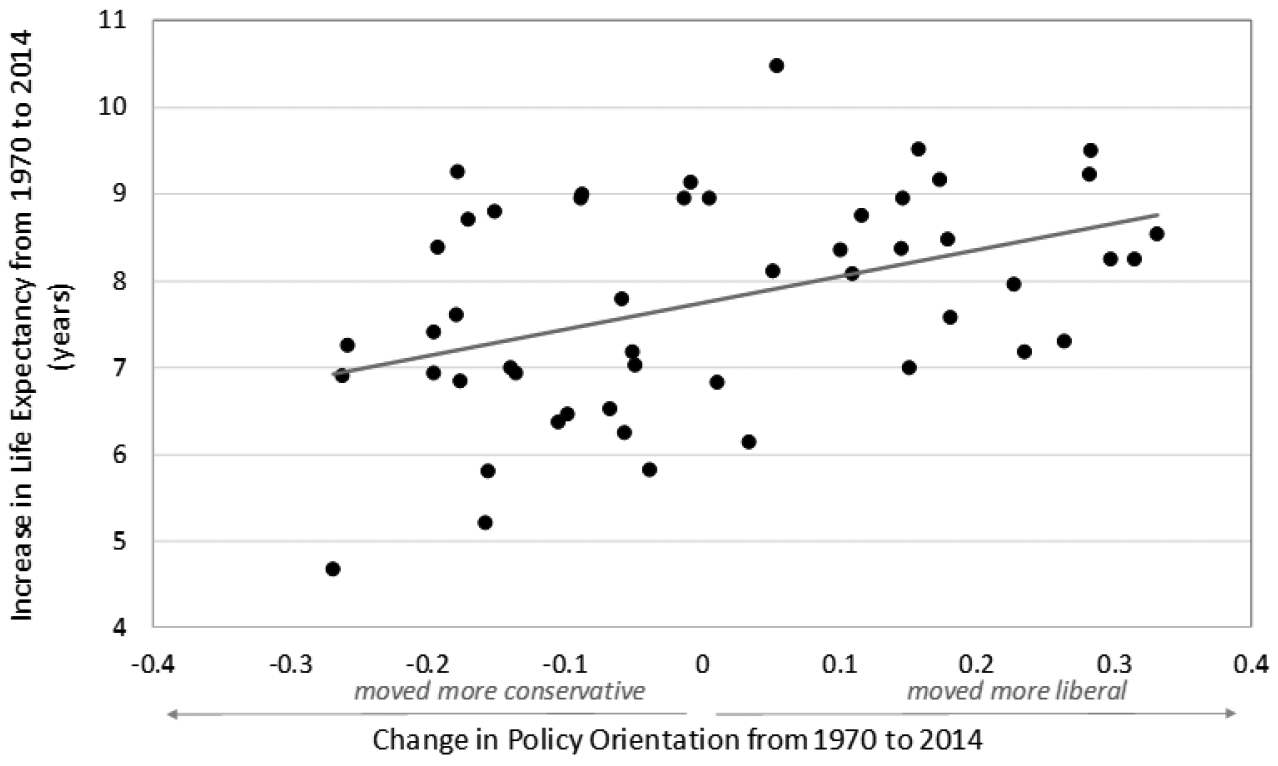
Changes in Policy Orientation and Life Expectancy Among States, 1970–2014
Figure 4 contains a dot for each state. Each dot represents the difference in the state’s overall policy orientation score from 1970 to 2014 (a difference greater than zero means the state’s overall policy orientation moved in a liberal direction) against the difference in the state’s life expectancy from 1970 to 2014. There is a positive and statistically significant correlation of 0.43, implying that states who moved in a more liberal policy direction tended to make greater gains in life expectancy across the forty-five-year period.
Policy polarization may also have contributed to the deteriorating position of the United States in international rankings of life expectancy. Demographer John Wilmoth and colleagues examined life expectancy at age fifty in the United States, Canada, France, Germany, and Japan from 1980 to 2000.194 They concluded that 10% to 50% of the deteriorating position of the United States against those countries is due to widening differences in life expectancy across states, plus shrinking differences within other countries, with the former contributing the most.195
Another hint that the changes in state policies may underlie the changes in U.S. life expectancy is suggested by the timeline of activity of policy-influencing organizations. ALEC’s initial success in the mid-1980s corresponds with the time that U.S. longevity started to fall behind other high-income countries and when longevity started to diverge across states.196 A step change in ALEC’s success occurred with the 2010 midterm elections, which corresponds to the time that U.S. longevity noticeably plateaued and departed from other high-income countries.197 Another hint can be seen by comparing states of highest and lowest ALEC activity. Take Oklahoma and Connecticut. As discussed above, in 1970 life expectancies in these two states were rather average, as compared to the rest of the United States,198 and differed by 1.5 years.199 Subsequently, OK became one of the most active states in enacting ALEC legislation200 and by 2014 had fallen to forty-seventh place in terms of life expectancy;201 CT was among the least active in enacting ALEC legislation202 and by 2014 had risen to third place.203
V. Resuscitating the Canary
“The time for half measures and talk is over, Senator.”
–Maximus Decimus Meridius, Gladiator204
Despite widespread recognition that Americans are dying prematurely, no serious and effective bipartisan effort has been undertaken to rectify the problem. A glimpse of hope did occur on October 5, 2018, when Representative Debbie Wasserman Schultz proposed the National Strategy To Increase Life Expectancy Act of 2018.205 The proposed legislation directed the U.S. Department of Health and Human Services to “develop a strategy that will analyze the causes of the falling life expectancy in the United States and propose solutions to those causes.”206 Nevertheless, the legislation was never enacted and died with the 115th Congress.207
Given the extent of the problem and its structural and historical roots, the solution will need to be bold. Anything less would be putting a bandage on a severed limb. Structural solutions focused on state policy contexts are required. Yet, it is unclear precisely what those solutions should look like and how they should be rolled out. Consequently, a necessary first step toward identifying effective and bold solutions is a fundamental reorientation of scientific research on the topic that targets the structural factors (e.g., state policies, corporations, policy-influencing organizations) that undergird the problem and identifies the best course of action.208 This is not to suggest that efforts to tackle the longevity crisis should wait until numerous comprehensive studies have been published, or until expert panels have been commissioned, or after researchers and policymakers have agreed on a single course of action. On the contrary, as Part II.B reviews, extensive evidence on the health benefits and harms of specific state-level policies already exists. For instance, there is abundant evidence that higher minimum wages improve health; many more states could implement such policies now to help stem the longevity crisis.209
To be sure, continued efforts to address behavioral factors will also be important, but they cannot be the sole focus. A singular focus on the health behavior crisis du jour (e.g., smoking, obesity, opioids, vaping) is ineffective as it leaves intact the structural machinery that continually generates such behaviors.210 This crucial fact is compellingly illustrated by the following parable,
There I am standing by the shore of a swiftly flowing river and I hear the cry of a drowning man. So I jump into the river, put my arms around him, pull him to shore and apply artificial respiration. Just when he begins to breathe, there is another cry for help. So I jump into the river, reach him, pull him to shore, apply artificial respiration, and then just as he begins to breathe, another cry for help. So back in the river again, reaching, pulling, applying, breathing and then another yell. Again and again, without end, goes the sequence. You know, I am so busy jumping in, pulling them to shore, applying artificial respiration, that I have no time to see who the hell is upstream pushing them all in.211
Researchers must turn their attention to examining the upstream forces that are pushing people in the river. This Essay argues that the polarization in U.S. state policies and the forces behind those changes (e.g., big donors, corporations, groups representing business interests) are pushing people in the river. Nevertheless, the information this Essay presents simply outlines the contours of that argument and provides preliminary supporting evidence, especially Figures 3 and 4. That argument or any counter argument must be rigorously tested and validated.
This new generation of studies should be interdisciplinary and bring together perspectives from disciplines that have heretofore not had much voice on the topic. Mostly demographers and economists have contributed to our understanding of the trends.212 While their perspectives and methods are essential, they alone are unlikely to move the needle on solving the problem. For instance, countless studies have used demographic methods that identify the major causes of death (e.g., suicide, drug overdose) contributing to the longevity decline.213 Such an estimation is vital, but it is simply a means to an end: causes of death explain how, not why, Americans are dying. To understand “why,” researchers need to ask new and different questions and integrate perspectives from political science and especially legal epidemiology—“the scientific study and deployment of law as a factor in the cause, distribution, and prevention of disease and injury in a population.”214 The importance of integrating these perspectives cannot be exaggerated. As public health scholar Nicholas Freudenberg proclaimed, the United States’ health woes have its roots “in corporate boardrooms[,] advertising and lobbying firms, and legislative and judicial chambers.”215 Likewise, legal epidemiologists who want to investigate the troubling trends in U.S. life expectancy should work with demographers and economists who can bring a strong social determinants of health perspective, extensive background knowledge about the longevity trends, and a sophisticated set of methodological techniques to empirically investigate potential explanations.216
A compelling, coordinated, and clear communication strategy is also needed to persuade policymakers and the public about the root causes of the longevity decline and the solutions needed to rectify the problem. The dominant narrative that health is primarily a result of personal responsibility and decisions (e.g., decisions to smoke, decisions to not attend college) needs correcting.217 Stakeholders with vested interests in the public believing in personal responsibility for health have been very effective, often rallying around terms like liberty and individual freedom that are hard to argue with.218 A communication strategy to combat this false narrative needs to be equally savvy and difficult to argue with. Unfortunately, it is unclear whether a rallying cry around health equity remains compelling in today’s environment; many policymakers and ordinary Americans appear to be unmoved by rallying cries around health or health equity, and such appeals may even be counterproductive.219 Nevertheless, it will be essential to develop a compelling message. All of the robust scientific evidence brought to bear on the topic may be entirely ineffective if it is not communicated in a clear, coordinated, and compelling way that can shape the hearts and minds of Americans across demographic groups and political affiliations.
The onus to change the narrative rests first and foremost with scientists who study and write about the health of the U.S. population. In order for journalists, policymakers, and the public to appreciate the centrality of structural factors in shaping population health, scientists must clearly and consistently communicate that centrality and “walk the walk” with their own research agendas. If the overriding focus is individual Americans’ health behaviors, it is irrational to hope that policymakers will understand the fundamental importance of law and policy in shaping Americans’ health and legislate accordingly.
Conclusion
Americans’ health and longevity are in trouble. Americans are sicker and die sooner than their peers in many other high-income countries and this disadvantage cuts across all demographic groups. It is less certain as to how the country ended up in this predicament. This Essay developed the hypothesis that the changing policy context of the United States—in particular, the polarizing policy environment across states—has played a significant and underappreciated role. It argued that state policies increasingly affect life and death in the United States and raised concerns that the continued polarization of state policies will further deteriorate the health and longevity of many Americans. Although the data in this Essay provide preliminary support for the argument, a significant amount of collaborative and interdisciplinary research is needed to test and refine those hypotheses. A new generation of research integrating principles of legal epidemiology will be instrumental, as well as an aggressive and bold communication strategy, to move the needle on changing U.S. policies, public perception, and improving Americans’ lives.
Notes
Jessica Y. Ho & Arun S. Hendi, Recent Trends in Life Expectancy Across High Income Countries: Retrospective Observational Study, BMJ, Aug. 15, 2018, at 1.
Id. at 3.
Life Expectancy at Birth, Total (Years), World Bank, http://data.worldbank.org/indicator/sp.dyn.le00.in?name_desc=false [https://perma.cc/93AC-YFZT] (last visited May 1, 2020) (providing life expectancy figures for various countries and regions through 2017).
Jennifer Karas Montez et al., Educational Disparities in Adult Mortality Across U.S. States: How Do They Differ, and Have They Changed Since the Mid-1980s?, 56 Demography 621, 638–39 (2019) [hereinafter Montez et al., Disparities in Adult Mortality].
For a review of the literature, see generally id. at 622–26
Transcript of the Democratic Presidential Debate in Milwaukee, N.Y. Times (Feb. 11, 2016), http://www.nytimes.com/2016/02/12/us/politics/transcript-of-the-democratic-presidential-debate-in-milwaukee.html [https://perma.cc/U7LH-U58D].
Id.
Id.
See Nancy MacLean, Democracy in Chains: The Deep History of the Radical Right’s Stealth Plan for America (2017); Steven H. Woolf & Heidi Schoomaker, Life Expectancy and Mortality Rates in the United States, 1959–2017, 322 JAMA 1996, 2009–11 (2019).
See, e.g., Nat’l Research Council, Explaining Divergent Levels of Longevity in High-Income Countries (Eileen M. Crimmins et al. eds., 2011) (ebook); Nat’l Research Council & Inst. of Med. of the Nat’l Acads., U.S. Health in International Perspective: Shorter Lives, Poorer Health (Steven H. Woolf & Laudan Aron eds., 2013) (ebook); International Differences in Mortality at Older Ages (Eileen M. Crimmins et al. eds., 2010) (ebook).
See, e.g., Jen Christensen, US Life Expectancy Is Still on the Decline. Here’s Why, CNN (Nov. 26, 2019, 1:44 PM), http://www.cnn.com/2019/11/26/health/us-life-expectancy-decline-study/index.html [https://perma.cc/2NEX-N8G4]; Maggie Fox, What’s Killing Us? It’s Mostly Our Own Bad Habits, NBC News (Sept. 10, 2015, 6:33 PM), http://www.nbcnews.com/health/health-news/what-s-killing-us-it-s-mostly-our-own-bad-n425321 [https://perma.cc/3GK2-QK9R]; Uptin Saiidi, US Life Expectancy Has Been Declining. Here’s Why, CNBC (July 9, 2019, 12:12 AM), http://www.cnbc.com/2019/07/09/us-life-expectancy-has-been-declining-heres-why.html [https://perma.cc/ER5Z-KYUA]. The media focused only on increases in deaths from drug overdose, liver disease, and suicide when, in reality, the risk of dying from seven of the ten leading causes of death had increased. Sherry L. Murphy et al., Ctrs. For Disease Control and Prevention, Mortality in the United States, 2017, at 4 (2018), http://www.cdc.gov/nchs/data/databriefs/db328-h.pdf [https://perma.cc/F5U8-SV6C].
Christensen, supra note 11.
See, e.g., Stephanie A. Robert & Bridget C. Booske, US Opinions on Health Determinants and Social Policy as Health Policy, 101 Am. J. Pub. Health 1655, 1661 (2011).
E.g., John B. McKinlay, A Case for Refocusing Upstream: The Political Economy of Illness, Applying Behavioral Science to Cardiovascular Risk (1975), reprinted in The Sociology of Health & Illness 583, 583 (Peter Conrad & Valerie Leiter eds., 9th ed. 2013) (coining the phrase “manufacturers of illness”).
See id.; Nicholas Freudenberg, Legal but Lethal: Corporations, Consumption, and Protecting Public Health 3 (2014).
See, e.g., Clare Bambra et al., Scaling Up: The Politics of Health and Place, 232 Soc. Sci. & Med. 36 (2019); Jason Beckfield & Clare Bambra, Shorter Lives in Stingier States: Social Policy Shortcomings Help Explain the US Mortality Disadvantage, 171 Soc. Sci. & Med. 30 (2016); Jennifer Karas Montez, Deregulation, Devolution, and State Preemption Laws’ Impact on US Mortality Trends, 107 Am. J. Pub. Health 1749 (2017) [hereinafter Montez, Deregulation]; Jennifer Karas Montez et al., Educational Disparities in Adult Health: U.S. States as Institutional Actors on the Association, 5 Socius 1 (2019) [hereinafter Montez et al., Disparities in Adult Health]; Montez et al., Disparities in Adult Mortality, supra note 4.
See infra Part I.A.
The term “low-educated” is defined differently across studies, but generally refers to individuals with either zero to eleven years of education; zero to twelve years of education; the bottom 20% of the education distribution; or the bottom 25% of the education distribution.
See infra Part I.D.
Cf. Steven L. Gortmaker & Paul H. Wise, The First Injustice: Socioeconomic Disparities, Health Services Technology, and Infant Mortality, 23 Ann. Rev. Soc. 147, 148 (1997).
David Cutler et al., The Determinants of Mortality, 20 J. Econ. Persp. 97, 99–106 (2006).
U.S. Dep’t of Health & Human Servs., DHHS Pub. No. 2011–1232, Health, United States, 2010: With Special Feature on Death and Dying 134 tbl.22 (2011).
Elizabeth Arias et al., United States Life Tables, 2014, Nat’l Vital Stat. Rep., Aug. 14, 2017, at 1.
Dora L. Costa, Health and the Economy in the United States from 1750 to the Present, 53 J. Econ. Lit. 503, 526 tbl.3, 528 tbl.5 (2015).
Life Expectancy at Birth, Total (Years), supra note 3.
Id.
Id.
See Arias et al., supra note 24, at 45 tbl.19.
Eileen M. Crimmins, Lifespan and Healthspan: Past, Present, and Promise, 55 Gerontologist 901, 906 (2015).
S. Jay Olshansky et al., A Potential Decline in Life Expectancy in the United States in the 21st Century, 352 New Eng. J. Med. 1138, 1142 (2005). They estimated that the rising prevalence of obesity and its life-shortening consequences would reduce life expectancy and also pointed to other life-shortening factors such as a rise in hospital-acquired infections and pollution. See id. at 1142–43.
See Ellen R. Meara et al., The Gap Gets Bigger: Changes in Mortality and Life Expectancy, by Education, 1981–2000, 27 Health Aff. 350, 354 (2008). The authors defined “high education” as “at least thirteen years of schooling.” Id. at 352. They showed that between 1990 and 2000 life expectancy at age twenty-five among adults with zero to twelve years of schooling (“low education”) declined by 0.9 years for white women and 0.2 years for Black women, but increased by 0.2 years for white men and 2.0 years for Black men. Id.
See, e.g., Anne Case & Angus Deaton, Rising Morbidity and Mortality in Midlife Among White Non-Hispanic Americans in the 21st Century, 112 PNAS 15078, 15080 & tbl.1 (2015); Ryan K. Masters et al., Educational Differences in U.S. Adult Mortality: A Cohort Perspective, 77 Am. Soc. Rev. 548, 562 (2012); Jennifer Karas Montez & Anna Zajacova, Trends in Mortality Risk by Education Level and Cause of Death Among US White Women from 1986 to 2006, 103 Am. J. Pub. Health 473, 476–77 (2013); Jennifer Karas Montez et al., Trends in the Educational Gradient of U.S. Adult Mortality from 1986 Through 2006 by Race, Gender, and Age Group, 33 Res. on Aging 145, 163–65 (2011); Isaac Sasson, Trends in Life Expectancy and Lifespan Variation by Educational Attainment: United States, 1990–2010, 53 Demography 269, 286–87 (2016).
But see Sabrina Tavernise, Life Spans Shrink for Least-Educated Whites in the U.S., N.Y. Times (Sept. 20, 2012), http://www.nytimes.com/2012/09/21/us/life-expectancy-for-less-educated-whites-in-us-is-shrinking.html [https://perma.cc/E28G-34CC] (discussing Olshanky’s 2012 study).
S. Jay Olshansky et al., Differences in Life Expectancy Due to Race and Educational Differences Are Widening, and Many May Not Catch Up, 31 Health Aff. 1803, 1806 (2012), http://www.healthaffairs.org/doi/10.1377/hlthaff.2011.0746 [https://perma.cc/EA7H-X7QN]; Tavernise, supra note 34.
Olshansky et al., supra note 35, app. at 6. The appendix is available separate from the article at S. Jay Olshansky et al., Differences in Life Expectancy Due to Race and Educational Differences Are Widening, and Many May Not Catch Up: Supplemental Material, Health Aff. (Aug. 2012), http://www.healthaffairs.org/doi/suppl/10.1377/hlthaff.2011.0746 [https://perma.cc/UH3G-2J7W].
See, e.g., John Bound et al., Measuring Recent Apparent Declines in Longevity: The Role of Increasing Educational Attainment, 34 Health Aff. 2167, 2168 (2015); Jennifer B. Dowd & Amar Hamoudi, Is Life Expectancy Really Falling for Groups of Low Socio-Economic Status? Lagged Selection Bias and Artefactual Trends in Mortality, 43 Int’l J. Epidemiology 983, 983 (2014); Arun S. Hendi, Trends in U.S. Life Expectancy Gradients: The Role of Changing Educational Composition, 44 Int’l J. Epidemiology 946, 947 (2015).
See Bound et al., supra note 37, at 2168; Dowd & Hamoudi, supra note 37, at 983–84; Hendi, supra note 37, at 947.
See Dowd & Hamoudi, supra note 37, at 984.
See id. at 984–85.
See, e.g., id.
See id.
As a hypothetical example, to use this method one could take people born in 1900, rank them according to the years of schooling they attained, and define the bottom 25% as low-educated. The researchers would then repeat this process for people born in 1901, 1902, and so on. Researchers would then examine trends in mortality for the bottom 25%, or bottom quartile.
See, e.g., Hendi, supra note 37, at 948–50.
See Bound et al., supra note 37, at 2169.
Id.
See, e.g., Sasson, supra note 33, at 287 (reporting “estimates … dramatically smaller than those reported by Olshansky”).
See, e.g., Bound et al., supra note 37, at 2169–71.
Sasson, supra note 33, at 287.
See, e.g., Alex Ho et al., Potential Gains in Life Expectancy from Reductions in Leading Causes of Death, Los Angeles County: A Quantitative Approach to Identify Candidate Diseases for Prevention and Burden Disparities Elimination, 3 J. Racial & Ethnic Health Disparities 431 (2016).
Id. at 441 tbl.4.
Id. at 442 tbl.4.
Id. at 441 tbl.4.
Id.
Case & Deaton, supra note 33.
E.g., Atul Gawande, Why Americans Are Dying from Despair, New Yorker (Mar. 16, 2020), http://www.newyorker.com/magazine/2020/03/23/why-americans-are-dying-from-despair [https://perma.cc/N327-YNWA].
Jiaquan Xu et al., Ctrs. for Disease Control and Prevention, Mortality in the United States, 2015, at 1 (2016), http://www.cdc.gov/nchs/data/databriefs/db267.pdf [https://perma.cc/63KF-7C3M]
Isaac Sasson & Mark D. Hayward, Association Between Educational Attainment and Causes of Death Among White and Black US Adults, 2010–2017, 322 JAMA 756, 761 fig.2 (2019).
See Life Expectancy at Birth, Total (Years), supra note 3.
Id.
See Ho & Hendi, supra note 1, at 1.
Irene Papanicolas et al., Health Care Spending in the United States and Other High-Income Countries, 319 JAMA 1024, 1024 (2018). These eleven countries include Australia, Canada, Denmark, France, Germany, Japan, the Netherlands, Sweden, Switzerland, the United Kingdom, and the United States. Id. at 1025.
Life Expectancy at Birth, Total (Years), supra note 3.
How Healthy Will We Be in 2040?, Inst. for Health Metrics and Evaluation (Oct. 16, 2018), http://www.healthdata.org/news-release/how-healthy-will-we-be-2040 [https://perma.cc/9744-UX9X] (citing Kyle J. Foreman et al., Forecasting Life Expectancy, Years of Life Lost, and All-Cause and Cause-Specific Mortality for 250 Causes of Death: Reference and Alternative Scenarios for 2016–40 for 195 Countries and Territories, 392 Lancet 2052 (2018)).
Data are from the Human Mortality Database housed at the University of California, Berkeley. See Hum. Mortality Database, http://www.mortality.org/ [https://perma.cc/W42U-Q5ZF] (last visited May 1, 2020). Countries in the figure (created by the author) include Australia, Austria, Belgium, Canada, Denmark, Finland, France, Iceland, Ireland, Italy, Japan, Luxembourg, the Netherlands, New Zealand, Norway, Portugal, Spain, Sweden, Switzerland, the United Kingdom, the United States, and West Germany.
See Ho & Hendi, supra note 1, at 8.
Id.
Id. (“[D]uring 2014–15 widespread declines in life expectancy occurred across high income countries.”).
Id.
Id. at 7–8, 9 tbl.1.
Id. at 9 tbl.1.
Nat’l Research Council & Inst. of Med. of the Nat’l Acads., supra note 10, at 92.
Melissa L. Martinson et al., Health Across the Life Span in the United States and England, 173 Am. J. Epidemiology 858, 864 (2011).
See Mauricio Avendano & Ichiro Kawachi, Why Do Americans Have Shorter Life Expectancy and Worse Health Than Do People in Other High-Income Countries?, 35 Ann. Rev. Pub. Health 307, 316 (2014).
Avendano & Kawachi, supra note 74, at 316; Mauricio Avendano et al., Do Americans Have Higher Mortality Than Europeans at All Levels of the Education Distribution?: A Comparison of the United States and 14 European Countries, in International Differences in Mortality at Older Ages, supra note 10, at 313, 318 tbl. 11–2, 319 tbl. 11–3; see also Martinson et al., supra note 73, at 863–64.
See, e.g., Avendano & Kawachi, supra note 74, at 311 (“The US health disadvantage is not limited to mortality but extends to many other nonfatal health outcomes beginning at birth and extending across youth, midlife, and old age.”); Martinson et al., supra note 73, at 863–64.
See Martinson et al., supra note 73, at 863.
See id.
Id. at 860 tbl.3. The percentages are 11.1% for American boys and 7.1% for English boys. Id.
See, for example, supra note 11 and accompanying text for a discussion of the media’s coverage of the discrepancy in life expectancy.
See Ho & Hendi, supra note 1, at 7. External causes of death accounted for 44% of the life expectancy decline in the United States. Id.
Avendano & Kawachi, supra note 74, at 316.
See Shannon Monnat, Our Problem Is Bigger Than Opioids, U.S. News & World Rep. (Feb. 26, 2019, 11:33 AM), http://www.usnews.com/news/healthiest-communities/articles/2019–02-26/commentary-social-and-economic-factors-are-driving-the-us-drug-crisis [https://perma.cc/FX75-CLK8].
Avendano & Kawachi, supra note 74; Bambra et al., supra note 16; Beckfield & Bambra, supra note 16; Montez, Deregulation, supra note 16.
Bambra et al., supra note 16, at 38 (citation omitted).
See Avendano & Kawachi, supra note 74, at 317–21.
Id.
Bambra et al., supra note 16, at 38 (citation omitted).
See infra Part II.A.
See infra Part II.B.
See infra Part II.C.
Period Lifetables: 1959–2017, WV: West Virginia, U.S. Mortality Database (Dec. 16, 2019), https://usa.mortality.org/state.php?state=WV [https://perma.cc/R4GR-68PL].
Period Lifetables: 1959–2017, HI: Hawaii, U.S. Mortality Database (Dec. 16, 2019), https://usa.mortality.org/state.php?state=HI [https://perma.cc/HV3A-585J]. Differences in life expectancy between states cannot be written off as simply reflecting differences in the population composition (e.g., racial distribution or poverty rates) of the states. See Jennifer Karas Montez et al., Explaining Inequalities in Women’s Mortality Between U.S. States, 2 SSM – Population Health 561, 568 (2016) [hereinafter Montez et al., Explaining Inequalities]. For example, one study estimated that about one-third of the variation in mortality between states is due to differences in population composition. Id.
Compare Period Lifetables: 1959–2017, WV: West Virginia, supra note 93, with Life Expectancy at Birth, Total (Years), supra note 3 (providing data on life expectancy for the United States and other countries).
Compare Period Lifetables: 1959–2017, WV: West Virginia, supra note 93, with Life Expectancy at Birth, Total (Years), supra note 3.
Compare Period Lifetables: 1959–2017, WV: West Virginia, supra note 93, with Life Expectancy at Birth, Total (Years), supra note 3.
Compare Period Lifetables: 1959–2017, HI: Hawaii, supra note 94, with Life Expectancy at Birth, Total (Years), supra note 3.
Compare Period Lifetables: 1959–2017, HI: Hawaii, supra note 94, with Life Expectancy at Birth, Total (Years), supra note 3.
John R. Wilmoth et al., Geographic Differences in Life Expectancy at Age 50 in the United States Compared with Other High-Income Countries, in International Differences in Mortality at Older Ages: Dimensions and Sources 333, 334–35 (2011).
The data come from the U.S. Mortality Database (USMDB). See U.S. Mortality Database, https://usa.mortality.org/index.php [https://perma.cc/MK2M-99SR] (last visited May 1, 2020). The data currently span 1959–2017; however, the data in Figure 2 (created by the author) are limited to 1970–2014 to correspond to the same time frame as the state policy data shown in Section III. In Figure 2, the five highest life expectancy states in 2014 were Hawaii, California, Connecticut, Minnesota, and New York. The five lowest life expectancy states were Mississippi, West Virginia, Alabama, Oklahoma, and Louisiana
Wilmoth et al., supra note 100, at 334.
See supra note 101. The range for each year is defined as the state with the highest life expectancy state minus the state with the lowest life expectancy.
See supra note 101.
See supra note 101.
Compare Period Lifetables: 1959–2017, OK: Oklahoma, U.S. Mortality Database (Dec. 16, 2019), https://usa.mortality.org/state.php?state=OK [https://perma.cc/MF49-NX6X] (life expectancy of 71.06 in 1970), with Period Lifetables: 1959–2017, CT: Connecticut, U.S. Mortality Database (Dec. 16, 2019), http://usa.mortality.org/state.php?state=CT [https://perma.cc/2FXA-2MKR] (life expectancy of 72.57 in 1970).
Compare Period Lifetables: 1959–2017, OK: Oklahoma, supra note 106 (life expectancy of 75.74 in 2014), with Period Lifetables: 1959–2017, CT: Connecticut, supra note 106 (life expectancy of 81.12 in 2014).
The rankings can be seen at USA Human Mortality Database, U. Cal. Berkeley Dep’t of Demography, https://shiny.demog.berkeley.edu/hmd/USHMD_MapApp/ [https://perma.cc/QGT7-QW9X] (last visited May 1, 2020) (reviewing the map for life expectancy, both sexes, age zero, and 2014).
See generally Shelley A. Hearne & Katrina Forrest, Shifting from Problem Identification to Problem Solving: CityHealth as an Accountability and Solution Driving Tool for Governmental Entities, 92 Temp. L. Rev. in press (2020).
Id. at (in press, so page number is not available).
Kelli A. Komro et al., The Effect of an Increased Minimum Wage on Infant Mortality and Birth Weight, 106 Am J. Pub. Health 1514, 1515 (2016); George Wehby et al., Effects of the Minimum Wage on Infant Health 16–18 (Nat’l Bureau of Economic Research, Working Paper No. 22373, 2018); see also Lindsey Rose Bullinger, The Effect of Minimum Wages on Adolescent Fertility: A Nationwide Analysis, 107 Am. J. Pub. Health 447, 449–50 (2017); David O. Meltzer & Zhuo Chen, The Impact of Minimum Wage Rates on Body Weight in the United States, in Economic Aspects of Obesity 17, 26–29 (Michael Grossman & Naci Mocan eds., 2011); Kate W. Strully et al., Effects of Prenatal Poverty on Infant Health: State Earned Income Tax Credits and Birth Weight, 75 Am. Soc. Rev. 534, 556 (2010); Mirium E. Van Dyke et al., State-Level Minimum Wage and Heart Disease Death Rates in the United States, 1980–2015: A Novel Application of Marginal Structural Modeling, 112 Preventive Med. 97, 101 (2018).
See, e.g., Julia Isaacs et al., Urban Inst., Paid Family Leave in the United States: Time for a New National Policy 5–7 (2017)
Isaacs et al., supra note 112, at 6; Maya Rossin., The Effects of Maternity Leave on Children’s Birth and Infant Health Outcomes in the United States, 30 J. Health Econ. 221, 227–31 (2011); Jenna Stearns, The Effects of Paid Maternity Leave: Evidence from Temporary Disability Insurance, 43 J. Health Econ. 85, 91–95 (2015).
Hearne & Forrest, supra note 109, at (in press, so page number is not available).
See Mike Vuolo et al., Independent and Interactive Effects of Smoking Bans and Tobacco Taxes on a Cohort of US Young Adults, 106 Am. J. Pub. Health 374, 376–77 (2016).
U.S. Dep’t of Health and Human Servs., The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General 678 (2014), http://www.ncbi.nlm.nih.gov/books/NBK179276/pdf/Bookshelf_NBK179276.pdf [https://perma.cc/5VCF-WWYB].
Steven Carlson & Brynne Keith-Jennings, Ctr. on Budget and Policy Priorities, SNAP Is Linked with Improved Nutritional Outcomes and Lower Health Care Costs 1–2 (2018), http://www.cbpp.org/sites/default/files/atoms/files/1–17-18fa.pdf [https://perma.cc/QK3A-DTQR].
Debra Umberson & Jennifer Karas Montez, Social Relationships and Health: A Flashpoint for Health Policy, 51 J. Health & Soc. Behav. S54, S58–60 (2010).
See The Turnaway Study, Ansirh, http://www.ansirh.org/sites/default/files/publications/files/turnaway_study_brief_web.pdf [https://perma.cc/HND3-RG3H] (last visited May 1, 2020).
See, e.g., Mark L. Hatzenbuehler et al., State-Level Policies and Psychiatric Morbidity in Lesbian, Gay, and Bisexual Populations, 99 Am. J. Pub. Health 2275, 2277–78 (2009); Nancy Krieger et al., The Unique Impact of Abolition of Jim Crow Laws on Reducing Inequities in Infant Death Rates and Implications for Choice of Comparision Groups in Analyzing Societal Determinants of Health, 103 Am. J. Pub Health 2234, 2237 (2013).
See Hatzenbuehler et al., supra note 120, at 2277–78.
See Bureau of Labor Statistics, Characteristics of Minimum Wage Workers, 2018, at 3 (2019), http://www.bls.gov/opub/reports/minimum-wage/2018/pdf/home.pdf [https://perma.cc/WL7E-2K9A]; Distribution of Nonelderly Adults with Medicaid by Gender, Kaiser Fam. Found., http://www.kff.org/medicaid/state-indicator/distribution-by-gender-4/ [https://perma.cc/QW39-DC2A] (last visited May 1, 2020); State Earned Income Tax Credits Help Build Opportunity for People of Color and Women, Ctr. on Budget and Pol’y Priorities, http://www.cbpp.org/sites/default/files/atoms/files/7–24-18sfp.pdf [https://perma.cc/2MQC-8MPR] (last visited May 1, 2020).
See Montez et al., Explaining Inequalities, supra note 94, at 568. The study found that characteristics of their state of residence could explain 53% of variation in women’s mortality across states compared to just 23% of the variation in men’s mortality. Id.
See Montez et al., Disparities in Adult Health, supra note 16, at 8–10; Montez et al., Disparities in Adult Mortality, supra note 4, at 636.
Jacob M. Grumbach, From Backwaters to Major Policymakers: Policy Polarization in the States, 1970–2014, 16 Persp. on Pol. 416 (2018).
Id. at 417.
Id. at 419.
Id. at 421.
Id. at 419.
See id.
Id. at 421 (footnote omitted).
See id. at 422–23. All of Grumbach’s data are available at Vol. 16(2): Replication Data for: From Backwaters to Major Policymakers: Policy Polarization in the States, 1970–2014, Harv. Dataverse, https://dataverse.harvard.edu/dataset.xhtml?persistentId=doi:10.7910/DVN/TZTW1J [https://perma.cc/RAR8-HCFS] (last visited May 1, 2020).
See id. at 422–23.
See id. at 423.
Id. at 421.
Id. at 423–24.
The author calculated the correlation coefficient using Grumbach’s data. Correlations range from negative one to one. A negative correlation means that states with more liberal policies on one domain have more conservative policies on the other domain. A positive correlation means that states with more liberal policies on one domain have more liberal policies on the other domain, and the same for those with conservative policies. A correlation near zero means that there is no relationship between the political orientation of two policy domains.
See infra Part III.A.
See infra Part III.B.
See infra Part III.C.
Thad Kousser, How America’s “Devolution Revolution” Reshaped its Federalism, 64 Revu Française De Sci. Politique 65, 66–67 (2014).
Timothy Conlan, From New Federalism to Devolution: Twenty-Five Years of Intergovernmental Reform 141–69 (1998).
Id. at 1–18; Kousser, supra note 141, at 66–67.
Conlan, supra note 142, at 141–69.
Id.
Id. at 230–56; see also Kousser, supra note 141, at 69–70.
Daniel Patrick Moynihan, Opinion, The Devolution Revolution, N.Y. Times (Aug. 6, 1995), http://www.nytimes.com/1995/08/06/opinion/the-devolution-revolution.html [https://perma.cc/9JQE-LBWD].
Id. (omission in original).
See, e.g., Nathan J. Kelly & Christopher Witko, Federalism and American Inequality, 74 J. Pol. 414, 423–25 (2012); Kousser, supra note 141, at 76–77; Sarah K. Bruch et al., Inst. for Research on Poverty, The Decentralization of the U.S. Safety Net, YouTube (Dec. 16, 2016), http://www.youtube.com/watch?v=yGHU8N0rVdo [https://perma.cc/BKV8-AD72].
Lori Riverstone-Newell, The Rise of State Preemption Laws in Response to Local Policy Innovation, 47 Publius J. Federalism 403, 404 (2017).
Id. at 407.
See, e.g., NRA & Gun Owners Win. Bloomberg / Everytown Lose., NRA-ILA (Oct. 24, 2019), http://www.nraila.org/articles/20191024/nra-and-gun-owners-win-bloombergeverytown-lose [https://perma.cc/KX7J-C4TK].
See, e.g., Sarah Milov, The Cigarette: A Political History 274 (2019) (quoting a high-profile tobacco lobbyist as saying “state laws which preempt local anti-tobacco ordinances are the most effective means to counter local challenges”); Abby Rapoport, Blue Cities Battle Red States, Am. Prospect (Aug. 22, 2016), http://prospect.org/article/blue-cities-battle-red-states [https://perma.cc/ASP6-KQ69].
See, e.g., Rapoport, supra note 153.
NRA & Gun Owners Win. Bloomberg / Everytown Lose., supra note 152.
See, e.g., Richard Briffault, The Challenge of the New Preemption, 70 Stan. L. Rev. 1995, 1997 (2018); Mary Bottari & Brendan Fischer, The ALEC-Backed War on Local Democracy, Huffington Post (Mar. 30, 2015), http://www.huffpost.com/entry/the-alec-backed-war-on-lo_b_6961142 [https://perma.cc/W9F4-HMVA]. One of the most extreme examples of corporate influence in recent years was a Kansas bill, HB 2595, enacted in 2016. See Jennifer L. Pomeranz & Mark Pertschuk, Key Drivers of State Preemption of Food, Nutrition, and Agriculture Policy: A Thematic Content Analysis of Public Testimony, 33 Am. J. Health Promotion 894, 895 (2019). It contained sweeping preemption of food, nutrition, and agricultural policies and went so far as to preempt the state’s own authority on those policies. Id.
Briffault, supra note 156, at 1997.
Id.
Lewis v. Governor of Ala., 896 F.3d 1282, 1287 (11th Cir. 2018).
Id. at 1295.
See Briffault, supra note 156, at 1997–98; Derek Carr et al., Equity-First: Conceptualizing a Normative Framework to Assess the Role of Preemption in Public Health, 98 Milbank Q. 131, 136–37 (2020).
See Worker Rights Preemption in the U.S., Econ. Pol’y Inst., http://www.epi.org/preemption-map/ [https://perma.cc/UG7X-UR9Z] (last visited May 1, 2020).
See id.
Jennifer L. Pomeranz & Mark Pertschuk, State Preemption: A Significant and Quiet Threat to Public Health in the United States, 107 Am. J. Pub. Health 900, 900 (2017).
Jennifer Karas Montez, How State Preemption Laws Prevent Cities from Taking Steps To Improve Health and Life Expectancy, Scholars (Mar. 6, 2018), www.scholars.org/brief/how-state-preemption-laws-prevent-cities-taking-steps-improve-health-and-life-expectancy [https://perma.cc/F8Y3–3JT5].
Alexander Hertel-Fernandez, State Capture (2019).
Id. at 5.
See id.
Id. at 14.
See id. at 14–15; Molly Jackman, ALEC’s Influence over Lawmaking in State Legislatures, Brookings (Dec. 6, 2013), www.brookings.edu/articles/alecs-influence-over-lawmaking-in-state-legislatures/ [https://perma.cc/P3B8–2C83].
See Hertel-Fernandez, supra note 166, at 11.
See id. at xii.
See id.
See id. at 40. The close ties between ALEC and Reagan can be heard in Reagan’s acceptance speech for ALEC’s 1990 Thomas Jefferson Award, where he claimed that he and ALEC were “soldiers in common cause.” American Legislative Exchange Council (ALEC), Ronald Reagan Tribute, at 4:44, YouTube (Feb. 28, 2008), http://www.youtube.com/watch?v=sVKErDZ8deM [https://perma.cc/TTG2–4PCJ].
See Hertel-Fernandez, supra note 166, at 61–62.
See id. at 25, 34.
See Right To Work Act, Am. Legis. Exchange Council (Jan. 28, 2013), www.alec.org/model-policy/right-to-work-act/ [https://perma.cc/H6E4-YHQK].
See Hertel-Fernandez, supra note 166, at 48; Adam Weinstein, How the NRA and its Allies Helped Spread a Radical Gun Law Nationwide, Mother Jones (June 7, 2012), http://www.motherjones.com/politics/2012/06/nra-alec-stand-your-ground/ [https://perma.cc/P8DD-DWBM]; ALEC Castle Doctrine, Ctr. for Media & Democracy, http://www.alecexposed.org/wiki/ALEC_Castle_Doctrine [https://perma.cc/MME6-GHYK] (last updated Oct. 13, 2017).
See Hertel-Fernandez, supra note 166, at 2.
See id. at 10.
See Martin Gilens & Benjamin I. Page, Testing Theories of American Politics: Elites, Interest Groups, and Average Citizens, 12 Persp. on Pol. 564 (2014).
Id. at 575.
Grumbach, supra note 125, at 424; Jennifer Karas Montez et al., US State Policies, Politics, and Life Expectancy, 98 Milbank Q. (forthcoming 2020).
For examples of quasi-experimental studies finding strong evidence of policy effects, see Peter A. Muennig et al., Cost Effectiveness of the Earned Income Tax Credit as a Health Policy Investment, 51 Am. J. Preventative Med. 874, 878 (2016) (finding that state-level EITC implementation was consistently followed by an improvement in the health of the state’s population); John A. Tauras, Public Policy and Smoking Cessation Among Young Adults in the United States, 68 Health Pol’y 321, 331 (2004) (concluding that “a significant increase in cigarette excises taxes along with more stringent smoke free air laws may be an extremely effective means to reduce the death and disease caused by tobacco use in the United States”); Van Dyke et al., supra note 111, at 99 (finding that a $1 increase in state minimum wage above the federal level was associated with a 3.5% reduction in heart disease mortality among working-age adults).
Pete Walley, Raising the Minimum Wage in Mississippi: An Econometric Analysis 2 tbl.1 (2014) (unpublished manuscript), http://www.mississippi.edu/urc/downloads/pwalley_140321.pdf [https://perma.cc/3SJG-ZKRH].
History of the General Hourly Minimum Wage in New York, N.Y. St., http://www.labor.ny.gov/stats/minimum_wage.shtm [https://perma.cc/BDY9–6872] (last visited May 1, 2020).
The Tax Burden on Tobacco, 1970–2018, Ctrs. for Disease Control and Prevention, http://chronicdata.cdc.gov/Policy/The-Tax-Burden-on-Tobacco-1970–2018/7nwe-3aj9 [https://perma.cc/7V78-LNKQ] (last updated June 13, 2019).
See State Tax Credits, Tax Credits for Working Fam., http://www.taxcreditsforworkersandfamilies.org/state-tax-credits/ [https://perma.cc/E7HG-UWWM] (last visited May 1, 2020).
Walley, supra note 185, at 2 tbl.1. Technically, Mississippi does not have a minimum wage; however, employers in the state who are subject to the Fair Labor Standards Act are required to pay the federal minimum wage, which is $7.25 per hour.
History of the General Hourly Minimum Wage in New York, supra note 186.
The Tax Burden on Tobacco, 1970–2018, supra note 187.
See State Tax Credits, supra note 188.
The data on life expectancy come from the USMDB. See U.S. Mortality Database, supra note 101. The data on policy orientation come from Grumbach. See Grumbach, supra note 125. Policy orientation scores range from zero (most conservative) to one (most liberal).
See Wilmoth et al., supra note 100, at 333–60. Life expectancy at age fifty is defined as the average number of additional years that a person aged fifty could expect to live, if they experienced the sex- and age-specific death rates prevailing in that year. Cf. Life Expectancy at Age 60 (Years), World Health Org., http://www.who.int/data/gho/indicator-metadata-registry/imr-details/2977 [https://perma.cc/MUP8-LHGN] (last visited May 1, 2020).
Wilmoth et al., supra note 100, at 359–60.
See Hertel-Fernandez, supra note 166, at 23–63 (providing a timeline of ALEC’s success). See supra Part II.A for trends in life expectancy by state.
See Ho & Hendi, supra note 1, at 8.
Compare Period Lifetables: 1959–2017, USA: United States, U.S. Mortality Database (Dec. 16, 2019), http://usa.mortality.org/national.php?national=USA [https://perma.cc/XZ3M-9SWY] (life expectancy of 70.75), with Period Lifetables: 1959–2017, OK: Oklahoma, supra note 106 (life expectancy of 71.06), and Period Lifetables: 1959–2017, CT: Connecticut, supra note 106 (life expectancy of 72.57).
Compare Period Lifetables: 1959–2017, OK: Oklahoma, supra note 106 (life expectancy of 71.06 in 1970), with Period Lifetables: 1959–2017, CT: Connecticut, supra note 106 (life expectancy of 72.57 in 1970).
Hertel-Fernandez, supra note 166, at 74.
See Period Lifetables: 1959–2017, OK: Oklahoma, supra note 106 (life expectancy of 75.74 in 2014). The rankings can be seen at USA Human Mortality Database, supra note 108.
Hertel-Fernandez, supra note 166, at 74.
See Period Lifetables: 1959–2017, CT: Connecticut, supra note 106 (life expectancy of 81.12 in 2014). The rankings can be seen at USA Human Mortality Database, supra note 108.
Gladiator (DreamWorks Pictures & Universal Pictures 2000).
National Strategy To Increase Life Expectancy Act of 2018, H.R. 7035, 115th Cong. (2018).
Abbey Interrante, Exclusive: The National Strategy To Increase Life Expectancy Bill Introduced to Congress Today, Newsweek (Oct. 5, 2018, 11:03 AM), http://www.newsweek.com/exclusive-national-strategy-life-expectancy-bill-1154948 [https://perma.cc/38RY-2FYH].
H.R. 7035 (115th): National Strategy To Increase Life Expectancy Act of 2018, GovTrack, http://www.govtrack.us/congress/bills/115/hr7035 [https://perma.cc/YYL2-ZET2] (last visited May 1, 2020).
See supra Section II for a discussion of a few studies that have made this shift to date and the impact of their findings.
See supra note 111 and accompanying text.
See McKinlay, supra note 14, at 583.
Id. (recounting a story that Irving Zola told the author to illustrate the “dilemmas of the modern practice of medicine).
See, for example, supra notes 31–40 for examples of scholars who have contributed to this research.
See, e.g., Ho & Hendi, supra note 1.
E.g., Scott Burris et al., A Transdisciplinary Approach to Public Health Law: The Emerging Practice of Legal Epidemiology, 37 Ann. Rev. Pub. Health 135, 139 (2016).
Freudenberg, supra note 15, at viii.
See, e.g., Lissy C. Friedman et al., Tobacco Industry Use of Personal Responsibility Rhetoric in Public Relations and Litigation: Disguising Freedom To Blame as Freedom of Choice, 105 Am. J. Pub. Health 250, 252–54 (2015) (documenting the tobacco industry’s strategic use of the terms “liberty” and “freedom of choice” in their advertisements and public relations statements).
See, e.g., Arlie Russell Hochschild, Strangers in Their Own Land: Anger and Mourning on the American Right (2016); MacLean, supra note 9; Jonathan M. Metzl, Dying of Whiteness: How the Politics of Racial Resentment Is Killing America’s Heartland (2019).