

Abstract
Housing instability is a thought to be a major influence on children’s healthy growth and development. However, little is known about the factors that influence housing instability, limiting the identification of effective interventions. The goals of this study were to 1) explore factors, including material hardship, satisfaction with living conditions and housing disrepair, that predict housing instability (total number of moves that a child experienced in the first seven years); and 2) examine the relationship between housing instability and child behavior at age 7, measured by the Child Behavior Checklist. We analyzed these associations among children enrolled in the Columbia Center for Children’s Environmental Health (CCCEH) Mothers and Newborns study.
In our analysis, we found that housing disrepair predicted residential change after 3 years of age, but not before. Persistent material hardship over the seven-year time period from pregnancy through age 7 was associated with increased number of moves. Children who experienced more than three moves in the first 7 years had significantly more thought- and attention-related problems compared to children who experienced less than 3 moves over the same time period. Children who experienced more than 3 moves also had higher total and internalizing problem behavior scores, although these differences were not statistically significant.
We conclude that housing instability is significantly associated with problem behavior in early childhood and that interventions to reduce socioeconomic strain may have the greatest impact in breaking the cycle of children’s environmental health disparities related to housing instability.
Keywords: Early childhood, housing instability, child behavior, material hardship
Introduction
Housing instability is a growing problem in the United States, particularly for those living in urban, low-income neighborhoods (1,2). It is challenging to studying housing instability and its effects on children’s health given its numerous and often inconsistent definitions. For example, the U.S. Department of Health and Human Services associates housing instability with high housing costs, poor housing quality, unstable neighborhoods, overcrowding, or homelessness (3). Previous studies have also used different parameters to measure housing instability, such as frequent moves and living with relatives and friends (4,5,6).
Recent research has begun to focus on the effects of housing instability, in its many forms, on child health and development (1). It is hypothesized that young children are at greater risk of being adversely affected by an unstable living environment, as this time period serves as a critical window for establishing socialization and learning habits (7,8). Additionally, the effects of housing instability may be compounded when combined with other challenges faced by low-income families (1). Previous studies have found that housing instability can alter a child’s overall academic achievement (9), emotional regulation (7,8), and verbal abilities (10). These health outcomes can have serious long-term effects as children progress through adolescence and adulthood, including decreased educational attainment (11), increased participation in risky behaviors (12,13), and a greater risk of adult-onset chronic diseases (14).
In this analysis, we explore the predictors of housing instability, including physical characteristics of housing and measures of socioeconomic strain in a low-income urban population of minority mothers and children. We also evaluate how housing instability, characterized by frequency of residential moves, affects child behavior assessed at age 7. We expect these results will inform future public health programs focused on identifying appropriate intervention points at which to break the cycle between unstable housing and child health outcomes.
Methods
Study Population
The Mothers and Newborns Study is a longitudinal birth cohort maintained by the Columbia Center for Children’s Environmental Health (CCCEH). The study enrolled 727 pregnant women living in Northern Manhattan and the South Bronx between 1998 and 2006. Study participants were African American or Dominican and were between the ages of 18 and 35 years at the time of recruitment. Subjects were excluded from the cohort if they reported smoking cigarettes or using other tobacco products during pregnancy, used illicit drugs, had their first prenatal visit after the 20th week of pregnancy, or had one of the following pre-existing conditions: diabetes, hypertension, or known HIV infection. Cohort participants were excluded from this analysis if they did not have complete information on residential history at the prenatal and ages 1, 2, 3, 5 and 7-year follow up visits or if the mother did not complete the Child Behavior Checklist (CBCL) at the 7-year visit (Figure 1). All study protocols were approved by the Institutional Review Board of Columbia University. Before each visit, mothers were informed about all study procedures and provided written informed consent to participate.
Figure 1.
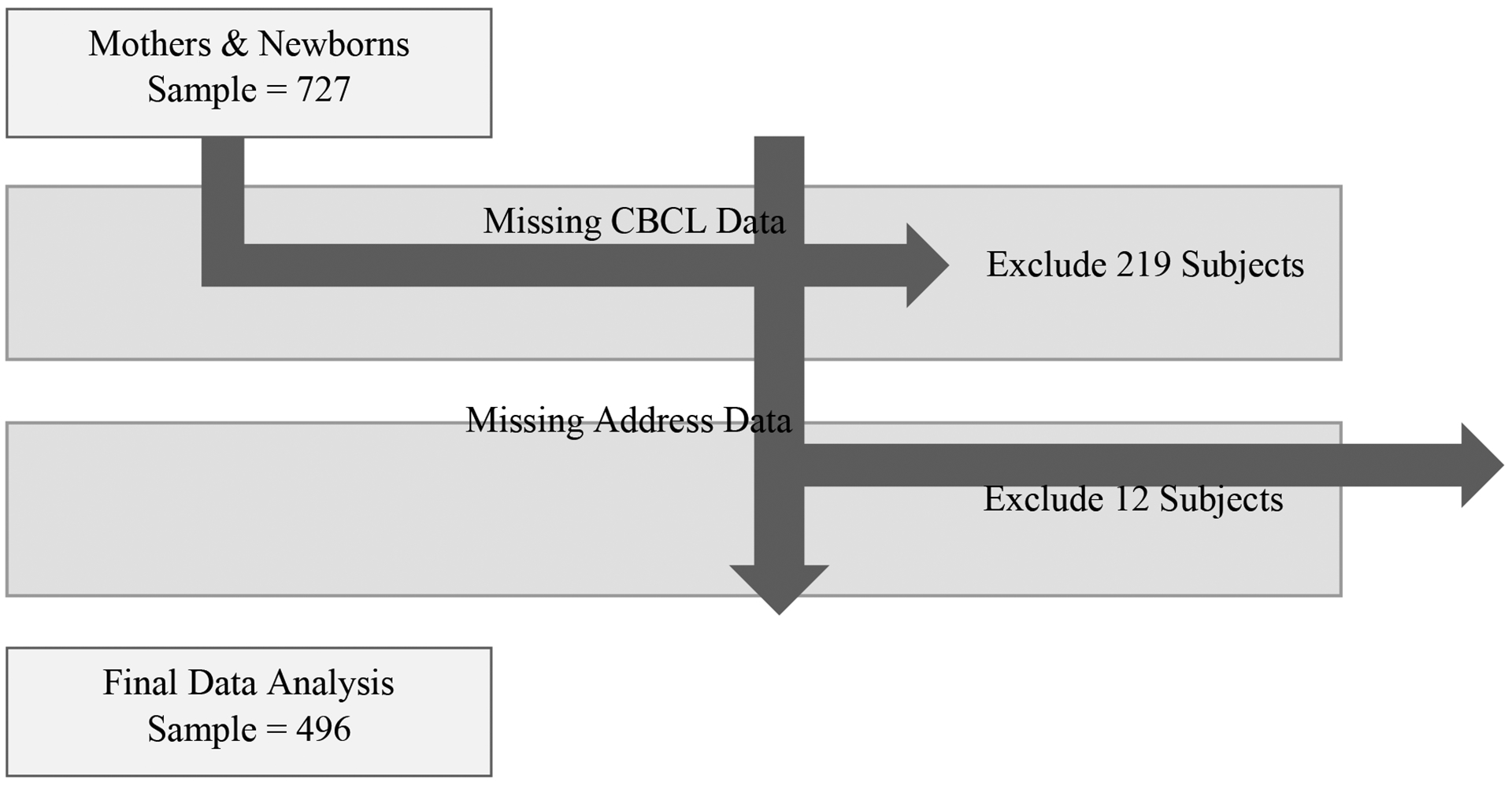
Final data analysis sample
Covariates
Mothers and their children were followed up at approximately 1, 2, 3, 5 and 7 years after birth. At each follow-up visit research workers conducted a structured interview to ascertain demographic characteristics of the mother (i.e. age, ethnicity, education, relationship status) and child (i.e. gender). Maternal demoralization, defined as the extent to which a mother experiences nonspecific psychological distress, was additionally assessed at each study visit using the Psychiatric Epidemiology Research Instrument- Demoralization (PERI-D) scale (15).
Residential History, Building Disrepair and Housing Satisfaction
At each study visit, research assistants recorded all addresses at which the mother-child pair resided since the previous study visit. We summed the number of study visits for which an address change occurred since previous study visit to create an index of instability experienced by each child. We defined unstable housing as greater than 3 moves from the prenatal period to age 7 years. Research workers also collected information on maternal report of paint chips or dust, holes in the ceiling or walls, mold, and leaky pipes in their current residence. We coded these building disrepair variables as 1 or 0 based on whether they were present or not. Similarly, pest variables, including maternal report of roaches, rodents, and other insects were also recorded and coded as 1 or 0 based on their presence. At each time point, we summed the number of building disrepair and pest items to create a visit-specific measure of housing disrepair (range: 0 to 7), which we subsequently categorized into 3 levels: no housing disrepair, one housing disrepair item, or 2 or more housing disrepair items. Finally, mothers rated their level of satisfaction with their current living conditions on a scale of 1 to 5 (1 indicating “very satisfied” and 5 indicating “very dissatisfied”) at each interview. We created a dichotomous variable by collapsing “very satisfied,” “somewhat satisfied,” or “neither satisfied nor dissatisfied” into one level and “very dissatisfied” or “somewhat dissatisfied” responses into a second level.
Material Hardship
At each study visit mothers were asked a series of questions adapted from a survey designed to measure material hardship among urban populations (16) to determine the level of economic strain that they were experiencing. This included questions about the mother’s self-reported ability to afford housing/rent, gas and/or electricity, food, and clothing. We summed the number of ‘hardships’ at each time point to create a material hardship scale ranging from 0 to 4. As previously described (17), we used Latent Class Growth Analysis to empirically estimate trajectories of material hardship from pregnancy through age 7 years. We found that mothers belonged to one of four hardship trajectories: increasing over time, decreasing over time, consistent low, and consistent high. Given our interest in socioeconomic strain, in all analyses we compared the persistent high hardship trajectory to the other three trajectories (low or fluctuating hardship) collapsed into a single group.
Child Behavior
At the 7-year follow-up visit, mothers were administered the Child Behavior Checklist (CBCL), which is a validated tool for assessing behavior problems in children (18). Mothers rated their children’s behavior on 113 items as never present, sometimes present, or often present. Scores on these items were summed and grouped into syndrome scales, which provide information across several behavioral domains. We analyzed the scores from several scales, including: attention and rule breaking (collectively: externalizing behaviors), anxiety/depression, withdrawn, and somatic complaint (collectively: internalizing behaviors), and attention, thought, and social problems. A total behavioral problem score was obtained from the sum of all eight syndrome scores.
Data Analysis
To better understand the predictors of housing instability, we examined the relationship between housing disrepair, maternal satisfaction with housing, and housing instability (Figure 2). We analyzed the relationship between housing disrepair and maternal satisfaction with living conditions at each time point using logistic regression. Satisfaction with living conditions and housing disrepair at each time point was analyzed as a predictor of having moved by the time of the next interview.
Figure 2.
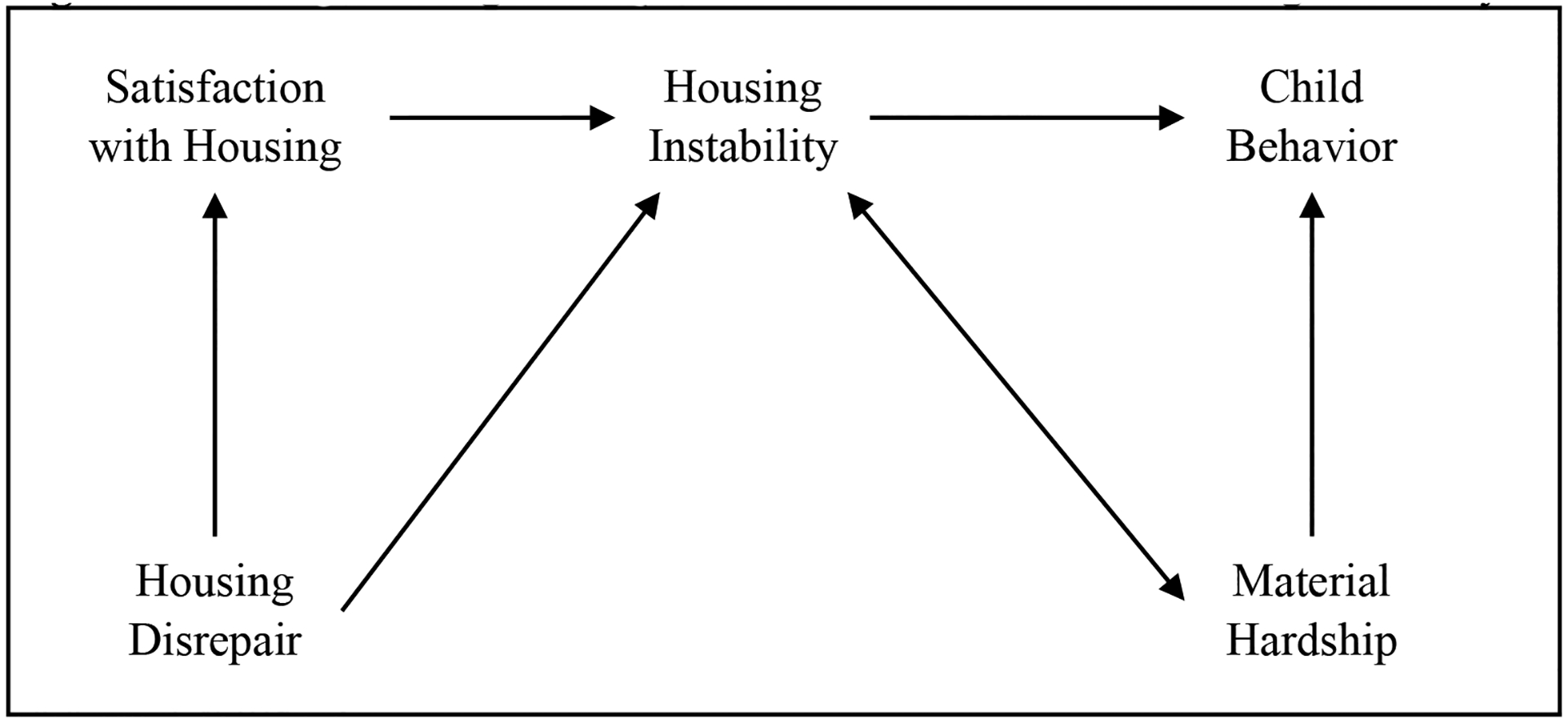
Conceptual diagram of predictors and outcomes of housing instability
We assessed CBCL outcomes using the raw scores from the checklist in a negative binomial regression model, which is well-suited for this type of count data and has been used in previous studies with the CBCL (19). The number of moves over 7 years was treated as a categorical predictor of CBCL scores using the following groups: 0–1 moves, 2–3 moves, and more than 3 moves. Since the CBCL is a maternally-reported questionnaire, and responses may be affected by the mother’s psychosocial well-being, we included maternal demoralization score, or the extent to which a mother experiences nonspecific psychological distress, in our final model (15). Additional covariates included in the model were maternal education, child age, child gender, and child ethnicity, based on their prior association with child behavior (19).
We also examined the role of material hardship in the main analysis, since material hardship has previously been shown to predict behavior problems in childhood (Figure 2) (11). In order to understand how long-term hardship was related to housing instability, total material hardship over the 7 years was analyzed using a latent variable model, which categorized each participant into 1 of 4 categories: increasing hardship over time, decreasing hardship over time, consistently low hardship, and consistently high hardship (17). We then analyzed the total number of moves over the 7-year time period as a mediator in the relationship between material hardship and housing instability.
Results
Characteristics of the Study Population
As illustrated by Table 1, the study population included individuals of Dominican or African American ethnicity. The average age of the mother at the prenatal visit was about 25 years old and approximately three-quarters of the mothers were single. Almost one quarter of the study population experienced persistent high material hardship throughout the study period. These demographic characteristics were not significantly different between the participants included (N=496) and those excluded (N=231) due to missing residential history or CBCL scores.
Table 1:
Characteristics of maternal-child pairs included in the analysis (N=496)
| N (%) or Mean±SD |
|
|---|---|
| Maternal age at prenatal visit | 25.2 ± 4.96 |
| African American | 188 (38.0) |
| Dominican | 307 (62.0) |
| <High school education at prenatal visit | 178 (32.2) |
| Married or stable relationship at prenatal visit | 128 (25.8) |
| Maternal demoralization at 7 year visit | 0.97 ± 0.68 |
| Male | 229 (46.2) |
| Child age at Child Behavior Checklist | 7.06 ± 0.20 |
| Persistent high material hardship | 106 (21.4) |
| Maternal dissatisfaction with living conditions: | |
| Prenatal visit | 49 (9.88) |
| 1 year visit | 57 (11.5) |
| 2 year visit | 70 (14.1) |
| 3 year visit | 62 (12.5) |
| 5 year visit | 62 (12.5) |
| 7 year visit | 64 (12.9) |
| Ever moved since previous study visit: | |
| 1 year visit | 80 (16.1) |
| 2 year visit | 84 (16.9) |
| 3 year visit | 104 (20.9) |
| 5 year visit | 146 (29.4) |
| 7 year visit | 145 (29.2) |
| Total number of study visits between which a residential move occurred: | |
| 0–1 | 301 (60.6) |
| 2–3 | 173 (34.8) |
| >3 | 22 (4.44) |
| ≥2 building disrepair items | |
| Prenatal visit | 379 (76.4) |
| 1 year visit | 324 (65.3) |
| 2 year visit | 320 (64.5) |
| 3 year visit | 302 (60.8) |
| 5 year visit | 285 (57.4) |
| 7 year visit | 272 (54.8) |
Housing Disrepair, Satisfaction with Living Conditions and Housing Instability
Higher housing disrepair scores at each time point after birth were associated with lower maternal report of satisfaction with living conditions at the same time point (range of p-values: 0.000 to 0.023) (Table 2). However, dissatisfaction with living conditions did not predict movement at the following interview. We observed a statistically significant positive association between housing disrepair at the 3-year visit (OR=1.81, p<0.05) and 5-year visit (OR=1.67, p<0.05) and at least one address change by the following visit, indicating that housing disrepair may predict housing instability as children grow older (Table 2).
Table 2.
Association between housing disrepair, satisfaction with living conditions, and residential moves
| Dissatisfied vs. satisfied with living conditions OR (p-value) |
Ever vs. never moved since previous study visit OR (p-value) |
|
|---|---|---|
| Housing disrepair: ≥2 items vs. 0 items | ||
| Prenatal | 0.812 (0.544) | N/A |
| 1 year | 2.12 (0.023) | 0.842 (0.541) |
| 2 year | 2.16 (0.009) | 1.40 (0.198) |
| 3 year | 2.42 (0.005) | 0.895 (0.629) |
| 5 year | 2.21 (0.008) | 1.81 (0.005) |
| 7 year | 3.07 (0.000) | 1.67 (0.012) |
| Dissatisfied vs. satisfied with living conditions | ||
| Prenatal | N/A | N/A |
| 1 year | N/A | 0.687 (0.416) |
| 2 year | N/A | 1.07 (0.856) |
| 3 year | N/A | 1.32 (0.372) |
| 5 year | N/A | 3.26 (0.000) |
| 7 year | N/A | 0.913 (0.767) |
Housing Instability and Child Behavior
In adjusted models, we found that children who experienced housing instability, defined as a residential move reported at more than 3 study visits (N=22), had 1.95 (p<0.05) and 1.56 (p<0.05) times the number of thought-related and attention-related problems compared to children with stable housing (defined as a residential move reported at one or fewer study visits), respectively. The total number of behavior problems and overall internalizing problems were also higher in children who experienced more than 3 moves over 7 years, but these associations were not statistically significant after adjusting for confounders (Table 3).
Table 3.
Summary of CBCL results in relation to housing instability and persistent material hardship included in the same modela.
| CBCL Syndrome | Housing instabilityb, c IRR (p-value) |
Persistent hardshipd IRR (p-value) |
|---|---|---|
| Anxiety/Depression | 1.24 (0.32) | 1.27 (0.04) |
| Withdrawn | 1.46 (0.20) | 1.34 (0.05) |
| Somatic complaints | 1.10 (0.72) | 1.40 (0.01) |
| Social problems | 1.37 (0.13) | 1.13 (0.26) |
| Thought problems | 1.95 (0.02) | 1.56 (0.01) |
| Attention problems | 1.58 (0.04) | 1.27 (0.05) |
| Rule breaking behavior | 1.27 (0.29) | 1.15 (0.24) |
| Aggressive behavior | 0.00 (0.99) | 1.19 (0.14) |
| Internalizing behavior problems | 1.25 (0.25) | 1.33 (0.01) |
| Externalizing behavior problems | 1.08 (0.71) | 1.18 (0.13) |
| Total behavior problems | 1.29 (0.15) | 1.23 (0.03) |
Abbreviations: CBCL- Child Behavior Checklist
Models also adjusted for maternal demoralization, maternal education, child gender, child ethnicity, and child age at time of CBCL
Defined as more than 3 residential moves from the prenatal period to age 7 years
Reference group defined as 0–1 moves over the first 7 years
Reference group defined as to low or fluctuating hardship
The Role of Material Hardship
Compared to families with low or fluctuating material hardship, we found that families experiencing persistent high material hardship were significantly more likely to experience housing instability (Incidence Rate Ration (IRR)=1.36, p<0.05). Additionally, children in families who experienced persistent material hardship had significantly higher internalizing (IRR=1.32, p<0.05) and total (IRR=1.22, p<0.05) problem scores as well as significantly higher anxiety/depression (IRR=1.25, p<0.05), somatic complaint (IRR=1.41, p<0.05) and thought-related (IRR=1.53, p<0.05) problem scores. When we adjusted for the number of moves a child experienced, the effect of persistent material hardship on anxiety/depression, somatic complaint, thought-related, internalizing, and total problems was virtually unchanged. The results for all syndrome scores from the adjusted model are presented in Table 3.
Discussion
We examined the predictors of housing instability, as well as behavioral outcomes of housing instability among a subset of participants enrolled in the CCCEH Mothers and Newborns birth cohort. We observed significant inverse associations between housing instability and child behavior at age 7 years. Material hardship over time was a significant predictor of poor behavior outcomes, and was also associated with housing instability.
These findings demonstrate the importance of material hardship as a predictor of housing instability as well as an independent predictor of child behavior outcomes. While building disrepair had some effect on movement, it was only a significant predictor in the later years of early childhood. We found that both attention- and thought-related behavior problems were associated with housing instability, even when controlling for material hardship. Problems with attention may include concentration difficulties, impulsivity, day dreaming, difficulty sitting still, nervousness, and poor performance in school (18). Thought-related problems may include seeing or hearing things, repeating acts, and having strange ideas and behaviors (18). These are issues that can have serious consequences for children, especially in terms of their academic performance and social and emotional well-being (7,8,11). These results are consistent with those from the Fragile Families and Child Wellbeing Study, which saw increased attention problems in children who experienced both housing instability and poverty (11).
The results from this analysis indicate that economic strain may be an optimal point of intervention in order to both reduce frequent moves and decrease the effects of housing instability on child neurobehavioral development (Figure 3). Previous research shows that families who receive subsidies or energy assistance are less likely to experience frequent moves (20). However, families eligible for housing subsidies rarely receive them due to the high demand and low availability, especially in large urban areas (21). There is a clear need for greater financial support for low-income families experiencing material hardship, but recent investment has instead addressed the issue with new structural development and improvement. These efforts to improve neighborhoods and living conditions often backfire on the immediate community, leading to increased cost of living, higher property taxes, and eventual gentrification (22).
Figure 3.
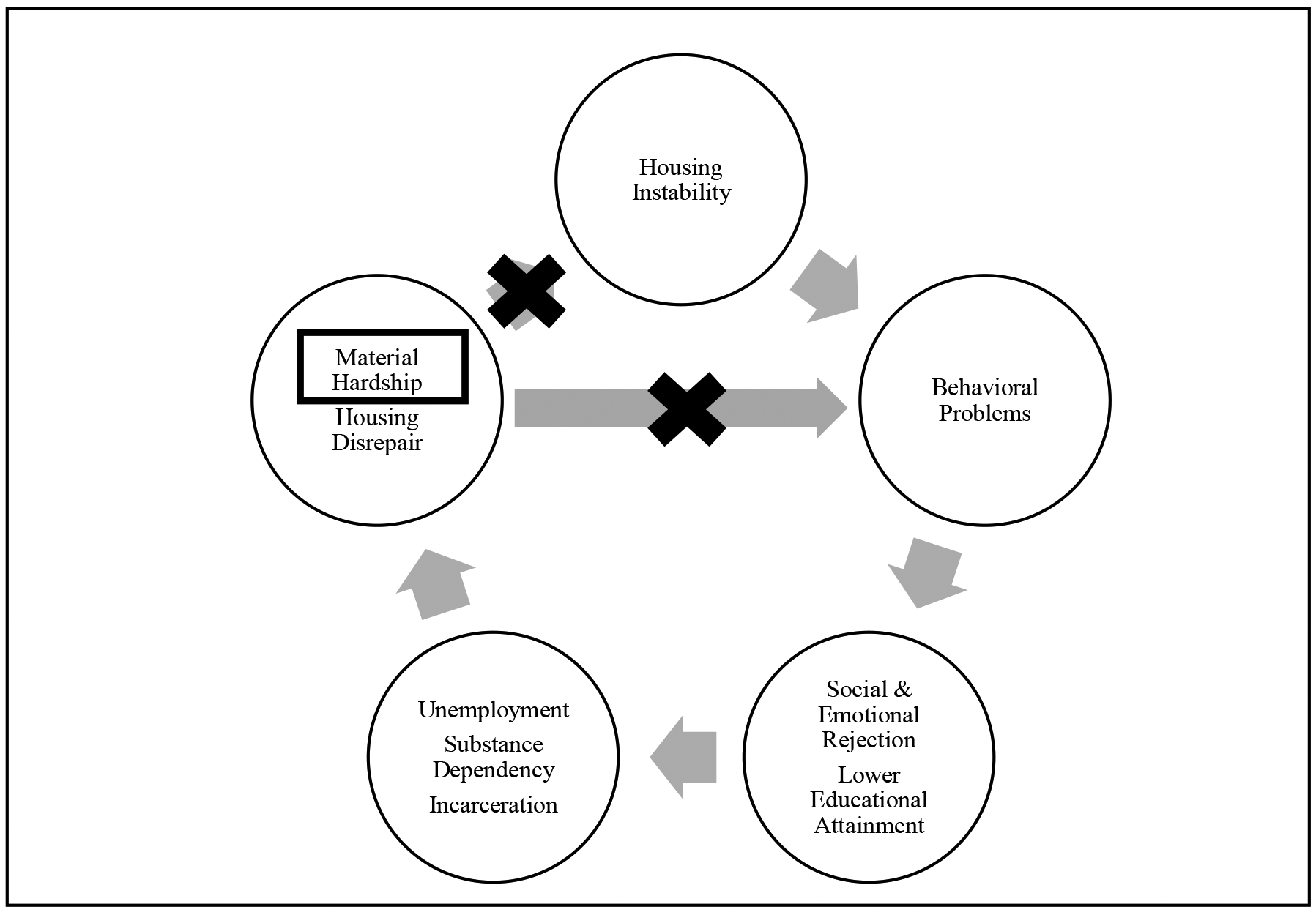
Breaking the cycle of environmental health disparities related to housing instability and child behavior
There are several limitations to our analysis. We did not have information on why the mothers in the study cohort moved, so we cannot determine if the move was forced or a choice. Additionally, it was not feasible to determine whether a move was lateral, downwards, or upwards in terms of living conditions or neighborhood indicators of poverty, based on the available measures. Our exclusion parameters prevented subjects with incomplete address data, likely due to loss to follow up or inability to locate, from being included in the analysis. These mothers may have experienced high levels of housing instability, introduced selection bias and prevented us from evaluating the full impact of housing instability in this cohort. This analysis was done in a cohort of low-income, urban, minority mothers, and the results may not be reproducible in other highly mobile families, such as migrant workers or military families. Despite these limitations, our analysis included detailed and thorough information on housing characteristics and material hardship. These parameters were collected at several time points throughout the study period, allowing us to understand the longitudinal effects of possible predictors of housing instability.
Conclusion
Material hardship is a predictor of behavior problems in childhood and is also significantly associated with housing instability. Housing instability is associated with increased behavior problems in childhood, particularly in relation to thought- and attention-related processes. These results support the idea that housing assistance in the form of subsidies may be the most effective use of spending to combat the issue of housing instability for families living in low-income neighborhoods.
References
- 1.Leventhal T, Newman S. Housing and child development. Children and Youth Services Review 2010;32(9):1165–74. [Google Scholar]
- 2.Long L International perspectives on the residential mobility of America’s children. Journal of Marriage and Family 1992;54(8):861–9. [Google Scholar]
- 3.Johnson A, Meckstroth A. Ancillary services to support welfare to work. U.S. Department of Health and Human Services, Washington DC, 1998. [Google Scholar]
- 4.Duchon LM, Weitzman BC, Shinn M. The relationship of residential instability to medical care utilization among poor mothers in New York City. Med Care 1999;37(12):1282–93. [DOI] [PubMed] [Google Scholar]
- 5.Carrion BV, Earnshaw VA, Kershaw T, Lewis JB, Stasko EC, Tobin JN, Ickovics JR. Housing instability and birth weight among young urban mothers. Journal of Urban Health: Bulletin of the New York Academy of Medicine 2014;92(1):1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jellyman T, Spencer N. Residential mobility in childhood and health outcomes: A systematic review. Journal of Epidemiology and Community Health 2008;62(7):584–92. [DOI] [PubMed] [Google Scholar]
- 7.Pittman JF, Bowmen GL. Adolescents on the move: Adjustments to family relocation. Youth & Society 1994;26:69–91. [Google Scholar]
- 8.Wood D, Halfon N, Scarlata D, Newacheck P, Nessim S. Impact of family relocation on children’s growth, development, school function, and behavior. Journal of the American Medical Association 1993;270(11):1334–8. [PubMed] [Google Scholar]
- 9.Adam EK. Beyond quality: Parental and residential stability and children’s adjustment. Current Directions in Psychological Science 2004;13(5):210–3. [Google Scholar]
- 10.Fowler PJ, McGrath LM, Henry DB, Schoeny M, Chavira D, Taylor JJ, Day O. Housing mobility and cognitive development: Change in verbal and nonverbal abilities. Child Abuse and Neglect 2015;48:104–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ziol-Guest KM, McKenna CC. Early childhood housing instability and school readiness. Child Development 2014;85(1):103–13. [DOI] [PubMed] [Google Scholar]
- 12.Hundelby JD, Mercer GW. Family and friends as social environmental and their relationship to young adolescents’ use of alcohol, tobacco, and marijuana. Journal of Marriage and Family 1987; 49(1):151–64. [Google Scholar]
- 13.Sharkey P, Sampson RJ. Destination effects: Residential mobility and trajectories of adolescent violence in a stratified metropolis. Criminology 2010;48(3):639–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shonkoff JP, Fisher PA. Rethinking evidence-based practice and two-generation programs to create the future of early childhood policy. Development and Psychopathology 2103;25(4):1635–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Roberts RE, Vernon SW. Usefulness of the PERI Demoralization Scale to screen for psychiatric disorder in a community sample. Psychiatry Research 1981;5:183–93. [DOI] [PubMed] [Google Scholar]
- 16.Mayer S, Jencks C. Poverty and the distribution of material hardship. Journal of Human Resources 1988:88–112. [Google Scholar]
- 17.Paper under review.
- 18.Achenbach TM, Rescorla LA. Manual for the ASEBA School-Age forms & profiles. University of Vermont, Burlington, VT, Research Center for Children, Youth & Families, 2001. [Google Scholar]
- 19.Cowell WJ, Lederman SA, Sjödin A, Jones R, Wang S, Perera FP, Wang R, Rauh VA, Herbstman JB. Prenatal exposure to polybrominated diphenyl ethers and child attention problems at 3–7 years. Neurotoxicol Teratol 2015;52:143–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mills G, Gubits D, Orr L. Effects of Housing Vouchers on Welfare Families. U.S. Department of Housing and Urban Development, Office of Policy Development and Research, Washington DC, 2006. [Google Scholar]
- 21.Sard B, Rice D. Decade of neglect has weakened federal low-income housing programs: New resources required to meet growing needs. Center on Budget and Policy Priorities, Washington DC, 2009. [Google Scholar]
- 22.Lees L Super-gentrification: The case of Brooklyn Heights, New York City. Urban Studies 2003;40(12):2487–2509. [Google Scholar]