

Key Points
Question
What are the risk factors associated with SARS-CoV-2 infection among farmworkers in California?
Findings
In this cross-sectional study of 1107 farmworkers, both household and workplace risk factors, including living with children aged 5 years or younger or unrelated roommates and living or working with an individual with known or suspected COVID-19, were associated with positive results on transcription-mediated amplification tests and immunoglobulin G tests for SARS-CoV-2 infection.
Meaning
These findings suggest that urgent distribution of vaccines to farmworkers and intervention on modifiable risk factors for SARS-CoV-2 infection are warranted given this population’s increased risk and the essential nature of their work.
This cross-sectional study identifies risk factors associated with SARS-CoV-2 infection among farmworkers in California.
Abstract
Importance
Essential workers in agriculture and food production have been severely affected by the ongoing COVID-19 pandemic.
Objective
To identify risk factors associated with SARS-CoV-2 infection among farmworkers in California.
Design, Setting, and Participants
This cross-sectional study invited farmworkers in California’s Salinas Valley (Monterey County) receiving transcription-mediated amplification (TMA) tests for SARS-CoV-2 infection at federally qualified community clinics and community sites to participate. Individuals were eligible if they were not pregnant, were 18 years or older, had conducted farmwork since the pandemic started, and were proficient in English or Spanish. Survey data were collected and SARS-CoV-2 tests were conducted among participants from July 16 to November 30, 2020.
Exposures
Sociodemographic, household, community, and workplace characteristics.
Main Outcomes and Measures
TMA- and immunoglobulin G (IgG)–positive SARS-CoV-2 infection.
Results
A total of 1107 farmworkers (581 [52.5%] women; mean [SD] age, 39.7 [12.6] years) were included in these analyses. Most participants were born in Mexico (922 [83.3%]), were married or living with a partner (697 [63.0%]), and worked in the fields (825 [74.5%]). Overall, 118 of 911 (13.0%) had a positive result on their TMA test for SARS-CoV-2 infection, whereas 201 of 1058 (19.0%) had antibody evidence of infection. In multivariable analyses accounting for recruitment venue and enrollment period, the incidence of TMA-positive SARS-CoV-2 infection was higher among those with lower than primary school–level education (adjusted relative risk [aRR], 1.32; 95% CI, 0.99-1.76; non–statistically significant finding), who spoke an Indigenous language at home (aRR, 1.30; 95% CI, 0.97-1.73; non–statistically significant finding), who worked in the fields (aRR, 1.60; 95% CI, 1.03-2.50), and who were exposed to a known or suspected COVID-19 case at home (aRR, 2.98; 95% CI, 2.06-4.32) or in the workplace (aRR, 1.59; 95% CI, 1.18-2.14). Positive results on IgG tests for SARS-CoV-2 infection were more common among those who lived in crowded housing (aRR, 1.23; 95% CI, 0.98-1.53; non–statistically significant finding), with children aged 5 years or younger (aRR, 1.40; 95% CI, 1.11-1.76), with unrelated roommates (aRR, 1.40; 95% CI, 1.19-1.64), and with an individual with known or suspected COVID-19 (aRR, 1.59; 95% CI, 1.13-2.24). The risk of IgG positivity was also higher among those with body mass index of 30 or greater (aRR, 1.65; 95% CI, 1.01-2.70) or diabetes (aRR, 1.31; 95% CI, 0.98-1.75; non–statistically significant finding).
Conclusions and Relevance
In this cross-sectional study of farmworkers in California, both residential and workplace exposures were associated with SARS-CoV-2 infection. Urgent distribution of COVID-19 vaccines and intervention on modifiable risk factors are warranted given this population’s increased risk of infection and the essential nature of their work.
Introduction
Essential workers in agriculture and food production have been severely affected by the ongoing COVID-19 pandemic.1 In Monterey County, California, we observed a 4-fold higher SARS-CoV-2 test positive fraction among farmworkers tested in community clinics between June and November 2020 than in the county population at large (22% vs 6%).2,3 In addition, recent studies have shown that agricultural and food workers in California experienced a 39% higher risk of all-cause death from March to October 2020 than during the same period in 2019, a greater increase than any other occupational group4; for workers with Latino backgrounds, the increase in all-cause mortality was 60%.5
Widely reported COVID-19 outbreaks among workers involved in food processing facilities have drawn attention to circumstances potentially placing agricultural and food workers at risk for SARS-CoV-2 infection, including poor hygienic conditions, medical leave policies, and residential crowding.6,7 However, specific exposures accounting for the high risk of SARS-CoV-2 infection among farmworkers remain poorly understood, and there is uncertainty about what strategies can be undertaken to reduce risk of infection in this population.8
Agricultural work is one of the lowest-paid occupations of the US economy, with 29% of full-time workers earning an annual income of less than $26 200 for a family of 4.9 Most US farmworkers are Latino (83%),10 and approximately one-third live in crowded housing,10,11,12 much of which is of substandard quality.12,13 In California, at least half of farmworkers are believed to be undocumented,10 which could further lead to labor exploitation and fewer workplace protections. In this study, we assessed sociodemographic, household, community, and workplace factors associated with SARS-CoV-2 infection in a population of more than 1000 farmworkers working in Monterey County, California.
Methods
The protocols for this cross-sectional study were approved by the Office for the Protection of Human Subjects at University of California, Berkeley. All participants provided written informed consent. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Study Setting
The Salinas Valley, located within Monterey County, California, is home to an agricultural workforce of approximately 50 000 resident farmworkers, with an additional 40 000 seasonal workers supporting the peak summer and fall seasons.12 Clinica de Salud del Valle de Salinas (CSVS), a federally qualified community health center, is the main health care system for Monterey County’s farmworkers and their families, with a network of 12 clinics throughout the valley that serve a low-income, primarily Spanish-speaking population of approximately 50 000 individuals.
SARS-CoV-2 Testing
Testing for SARS-CoV-2 infection at CSVS began June 15, 2020, and was offered to all individuals regardless of exposure, symptoms, documentation, or health insurance status. Medical personnel collected oropharyngeal specimens for detection of SARS-CoV-2 RNA via the qualitative Hologic/Aptima nucleic acid transcription-mediated amplification (TMA) assay. TMA comprises the isothermal amplification of SARS-CoV-2 ribosomal RNA by reverse transcriptase and subsequent generation of numerous transcripts by RNA polymerase.14 Testing was conducted on clinic premises or at community sites, including low-income housing, agricultural fields, and CSVS-run community health fairs.
Study Enrollment
Between July 16 and November 30, 2020, we invited farmworkers (whom we considered to include anyone employed in the agricultural sector) receiving care or getting tested for SARS-CoV-2 infection at CSVS clinics and community sites to participate in our study. We posted flyers about the study at the clinics and around town and provided study information to community groups and growers. Farmworkers were eligible for participation if they were not pregnant, were aged 18 years or older, had conducted farmwork within the 2 weeks preceding their testing date, and were sufficiently proficient in English or Spanish to give consent and complete study procedures. Beginning October 5, we enrolled any individual who had engaged in agricultural work at any time since March 2020 because the growing season was ending.
We enrolled a total of 1115 farmworkers. We excluded from analyses 8 farmworkers who did not provide blood samples or were not employed as farmworkers at the time of enrollment, leaving a total of 1107 participants.
Study Procedures
After the participant completed the SARS-CoV-2 TMA test and consented to participate in the study, the study team obtained a blood sample by venipuncture for testing of anti–SARS-CoV-2 antibody status. We then measured height and weight using a digital scale. The study team administered a 45-minute computer-guided questionnaire by telephone in Spanish or English within 2 days before (for preconsented participants) or after the enrollment visit but before SARS-CoV-2 testing results were available to avoid recall bias. The questionnaire gathered information on sociodemographic characteristics, risk factors for SARS-CoV-2 infection, and consequences of the pandemic on daily life and well-being. Participants received $50 on completion of all data collection activities.
Blood specimens were stored immediately at 4 to 7 °C and centrifuged and aliquoted within 48 hours following collection. We used an in-house enzyme-linked immunosorbent assay (ELISA) to measure immunoglobulin G (IgG) reactivity to the SARS-CoV-2 spike and receptor binding domain proteins, as described previously.2
Statistical Analysis
We examined risk factors associated with TMA-positive and IgG-positive results for SARS-CoV-2 infection separately. Analyses examining risk factors for positive results on TMA tests included participants who worked in agriculture in the 2 weeks preceding enrollment (n = 911); analyses for positive results on IgG tests included all farmworkers who provided a blood sample (n = 1058).
We performed bivariate analyses for a wide range of sociodemographic, household, community, and work-related characteristics known or suspected to be associated with SARS-CoV-2 infection (Table 1, Table 2, Table 3, and Table 4; eTables 1-4 in Supplement 1) and assessed correlations between these characteristics (eFigure in Supplement 1). We included covariates in multivariable models if there were more than 5 TMA positive or IgG positive cases in each category, respectively, and a χ2 or t test with P < .20 in bivariate analyses. Categorical risk factors were modeled as shown in Table 1, Table 2, Table 3, and Table 4, except for language spoken at home (modeled as Indigenous language spoken at home, yes or no) and working in the fields (yes or no). Age, years in the US, and household size were modeled as continuous variables. We did not consider specific agricultural crops in multivariable analyses because farmworkers reported working in a variety of them. We used backward stepwise elimination (with a threshold of P < .10) to select covariates for inclusion in final models.
Table 1. Sociodemographic and Health-Related Risk Factors for TMA and IgG Positivity Among Farmworkers, Monterey County, 2020.
| Attribute | Individuals, No. (%)a | ||||
|---|---|---|---|---|---|
| All enrolled (N = 1107) | SARS-CoV-2 infection | ||||
| TMA positive (n = 911) | IgG positive (n = 1058) | ||||
| Yes (n = 118) | No (n = 793) | Yes (n = 201) | No (n = 857) | ||
| Recruitment site | |||||
| Clinics | 561 (50.7) | 95 (18.4)b | 420 (81.6) | 97 (18.4) | 429 (81.6) |
| Community outreach | 546 (49.3) | 23 (5.8) | 373 (94.2) | 104 (19.5) | 428 (80.5) |
| Agricultural work in the preceding 2 weeks | |||||
| No | 193 (17.4) | NA | NA | 45 (23.3)c | 148 (76.7) |
| Yes | 914 (82.6) | 118 (13.0) | 793 (87.0) | 156 (18.0) | 709 (82.0) |
| Sex | |||||
| Female | 581 (52.5) | 60 (13.0) | 400 (87.0) | 99 (18.1) | 448 (81.9) |
| Male | 526 (47.5) | 58 (12.9) | 393 (87.1) | 102 (20.0) | 409 (80.0) |
| Age, y | |||||
| Mean (SD) | 39.7 (12.6) | 39.6 (11.0) | 39.6 (12.4) | 39.6 (12.3) | 39.6 (12.6) |
| 18-29 | 275 (24.8) | 27 (12.0) | 198 (88.0) | 43 (16.3)c | 220 (83.7) |
| 30-39 | 271 (24.5) | 29 (12.9) | 195 (87.1) | 59 (22.5) | 203 (77.5) |
| 40-49 | 297 (26.8) | 42 (16.4) | 214 (83.6) | 59 (20.8) | 225 (79.2) |
| 50-59 | 198 (17.9) | 16 (10.2) | 141 (89.8) | 27 (14.5) | 159 (85.5) |
| ≥60 | 66 (6.0) | 4 (8.2) | 45 (91.8) | 13 (20.6) | 50 (79.4) |
| Education | |||||
| ≤Primary school | 488 (44.1) | 63 (15.4)b | 346 (84.6) | 100 (21.2)d | 372 (78.8) |
| >More than primary school | 618 (55.8) | 55 (11.0) | 446 (89.0) | 101 (17.3) | 484 (82.7) |
| No answer | 1 (0.1) | 0 | 1 (100.0) | 0 | 1 (100.0) |
| Marital status | |||||
| Not married or living as married | 409 (36.9) | 50 (15.3)d | 277 (84.7) | 69 (17.8) | 319 (82.2) |
| Married or living as married | 697 (63.0) | 67 (11.5) | 516 (88.5) | 132 (19.7) | 537 (80.3) |
| No answer | 1 (0.1) | 1 (100.0) | 0 | 0 | 1 (100.0) |
| Annual household income, $ | |||||
| <25 000 | 557 (50.3) | 66 (14.5) | 390 (85.5) | 101 (18.8) | 435 (81.2) |
| ≥25 000 | 494 (44.6) | 48 (11.6) | 367 (88.4) | 86 (18.5) | 380 (81.5) |
| No answer | 56 (5.1) | 4 (10.0) | 36 (90.0) | 14 (25.0) | 42 (75.0) |
| Language spoken at home | |||||
| English | 57 (5.1) | 0 (0.0) | 42 (100.0) | 12 (21.8) | 43 (78.2) |
| Indigenous | 110 (9.9) | 22 (22.7) | 75 (77.3) | 23 (21.5) | 84 (78.5) |
| Spanish | 940 (84.9) | 96 (12.4)b | 676 (87.6) | 166 (18.5) | 730 (81.5) |
| No answer | 0 | 0 | 0 | 0 | 0 |
| Country of birth | |||||
| Mexico | 922 (83.3) | 104 (13.5)d | 669 (86.5) | 163 (18.4) | 721 (81.6) |
| United States | 141 (12.7) | 7 (7.0) | 93 (93.0) | 31 (23.0) | 104 (77.0) |
| Other | 44 (4.0) | 7 (18.4) | 31 (81.6) | 7 (18.0) | 32 (82.1) |
| Time in United States, y | |||||
| Mean (SD) | 21.3 (11.1) | 20.2 (10.9) | 21.0 (11.2) | 21.3 (10.6) | 21.2 (11.3) |
| <15 | 262 (23.7) | 38 (16.5)d | 193 (83.5) | 46 (18.0)d | 209 (82.0) |
| 15-19 | 191 (17.3) | 17 (10.4) | 147 (89.6) | 44 (24.0) | 139 (76.0) |
| 20-29 | 296 (26.7) | 34 (13.5) | 218 (86.5) | 49 (17.4) | 232 (82.6) |
| ≥30 | 216 (19.5) | 22 (13.4) | 142 (86.6) | 31 (15.3) | 172 (84.7) |
| Entire life | 141 (12.7) | 7 (7.0) | 93 (93.0) | 31 (23.0) | 104 (77.0) |
| No answer | 1 (0.1) | 0 | 0 | 0 | 1 (100.0) |
| Community of residence | |||||
| Salinas | 486 (43.9) | 40 (10.4)b | 343 (89.6) | 99 (21.2)b | 369 (78.8) |
| Greenfield | 315 (28.5) | 56 (19.8) | 227 (80.2) | 63 (21.2) | 234 (78.8) |
| Other town | 306 (27.6) | 22 (9.0) | 223 (91.0) | 39 (13.3) | 254 (86.7) |
| Smoking | |||||
| Never | 899 (81.2) | 99 (13.6) | 630 (86.4) | 157 (18.4) | 698 (81.6) |
| Former | 158 (14.3) | 16 (11.4) | 124 (88.6) | 36 (23.4) | 118 (76.6) |
| Current | 49 (4.4) | 3 (7.3) | 38 (92.7) | 8 (16.7) | 40 (83.3) |
| No answer | 1 (0.1) | 0 | 1 (100.0) | 0 | 1 (100.0) |
| BMI | |||||
| Mean (SD) | 29.7 (5.5) | 29.2 (4.7) | 29.7 (5.6) | 30.4 (5.4)b | 29.4 (5.5 |
| Underweight or normal, <25 | 197 (17.8) | 18 (10.8) | 149 (89.2) | 24 (12.5)b | 168 (87.5) |
| Overweight, 25.0-29.9 | 421 (38.0) | 45 (13.0) | 302 (87.0) | 75 (18.6) | 329 (81.4) |
| Obesity, ≥30 | 461 (41.6) | 49 (13.1) | 326 (86.9) | 95 (21.7) | 342 (78.3) |
| Not collected | 28 (2.5) | 6 (27.3) | 16 (72.7) | 7 (28.0) | 18 (72.0) |
| Self-reported hypertension | |||||
| No | 954 (86.2) | 106 (13.5) | 680 (86.5) | 171 (18.7) | 744 (81.3) |
| Yes | 149 (13.5) | 12 (9.8) | 110 (90.2) | 29 (20.9) | 110 (79.1) |
| No answer | 4 (0.4) | 0 | 3 (100.0) | 1 (25.0) | 3 (75.0) |
| Self-reported diabetes | |||||
| No | 977 (88.3) | 109 (13.6)d | 694 (86.4) | 172 (18.4)d | 762 (81.6) |
| Yes | 126 (11.4) | 9 (8.6) | 96 (91.4) | 28 (23.3) | 92 (76.7) |
| No answer | 4 (0.4) | 0 | 3 (100.0) | 1 (25.0) | 3 (75.0) |
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); IgG, immunoglobulin G; NA, not applicable; TMA, transcription-mediated amplification.
Missing entries were excluded from bivariate analyses.
P < .05.
P < .10.
P < .20.
Table 2. Household and Community Risk Factors for TMA and IgG Positivity Among Farmworkers, Monterey County, 2020.
| Attribute | Individuals, No. (%)a | ||||
|---|---|---|---|---|---|
| All enrolled (N = 1107) | SARS-CoV-2 infection | ||||
| TMA positive (n = 911) | IgG positive (n = 1058) | ||||
| Yes (n = 118) | No (n = 793) | Yes (n = 201) | No (n = 857) | ||
| Type of housing | |||||
| House | 522 (47.2) | 60 (13.5) | 383 (86.5) | 101 (20.6) | 389 (79.4) |
| Apartment | 481 (43.5) | 48 (12.9) | 324 (87.1) | 85 (18.2) | 383 (81.8) |
| Hotel or motel | 37 (3.3) | 6 (16.7) | 30 (83.3) | 5 (13.5) | 32 (86.5) |
| Trailer or mobile home | 43 (3.9) | 3 (7.7) | 36 (92.3) | 8 (19.5) | 33 (80.5) |
| Other | 24 (2.2) | 1 (4.8) | 20 (95.2) | 2 (9.1) | 20 (90.9) |
| Household size | |||||
| Mean (SD) | 5.5 (2.5) | 5.5 (2.4) | 5.4 (2.3) | 5.9 (2.6)b | 5.4 (2.6) |
| 0 others | 12 (1.1) | 2 (18.2) | 9 (81.8) | 3 (25.0)b | 9 (75.0) |
| 1-3 others | 397 (35.9) | 41 (12.4) | 290 (87.6) | 58 (15.3) | 321 (84.7) |
| 4-6 others | 512 (46.3) | 51 (12.3) | 363 (87.7) | 93 (19.1) | 393 (80.9) |
| ≥7 others | 186 (16.8) | 24 (15.5) | 131 (84.5) | 47 (26.0) | 134 (74.0) |
| Children <18 y living in the home | |||||
| No | 277 (25.0) | 28 (11.9) | 207 (88.1) | 43 (16.0)c | 225 (84.0) |
| Yes | 829 (74.9) | 90 (13.3) | 585 (86.7) | 157 (19.9) | 632 (80.1) |
| No answer | 1 (0.1) | 0 | 1 (100.0) | 1 (100.0) | 0 |
| Children ≤5 y living in the home | |||||
| No | 699 (63.1) | 79 (13.7) | 498 (86.3) | 110 (16.4)b | 559 (83.6) |
| Yes | 408 (36.9) | 39 (11.7) | 295 (88.3) | 91 (23.4) | 298 (76.6) |
| Children attending school or daycare | |||||
| No | 1018 (92.0) | 105 (12.6) | 726 (87.4) | 184 (18.9) | 792 (81.1) |
| Yes | 85 (7.7) | 12 (15.8) | 64 (84.2) | 16 (20.5) | 62 (79.5) |
| No answer | 4 (0.4) | 1 (25.0) | 3 (75.0) | 1 (25.0) | 3 (75.0) |
| Living with unrelated roommates | |||||
| No | 901 (81.4) | 93 (12.7) | 639 (87.3) | 156 (18.1)c | 704 (81.9) |
| Yes | 206 (18.6) | 25 (14.0) | 154 (86.0) | 45 (22.7) | 153 (77.3) |
| Living with other farmworkers | |||||
| No | 281 (25.4) | 26 (11.6) | 198 (88.4) | 49 (18.4) | 218 (81.6) |
| Yes | 823 (74.3) | 92 (13.5) | 592 (86.5) | 151 (19.2) | 637 (80.8) |
| No answer | 3 (0.3) | 0 | 3 (100.0) | 1 (33.3) | 2 (66.7) |
| Persons per bedroom | |||||
| ≤2 | 703 (63.5) | 71 (12.3) | 505 (87.7) | 113 (17.0)b | 553 (83.0) |
| >2 | 404 (36.5) | 47 (14.0) | 288 (86.0) | 88 (22.4) | 304 (77.6) |
| Access to washing machine at home | |||||
| No | 411 (37.1) | 49 (14.2) | 296 (85.8) | 77 (19.5) | 318 (80.5) |
| Yes | 696 (62.9) | 69 (12.2) | 497 (87.8) | 124 (18.7) | 539 (81.3) |
| Left home for nonessential reasons during past 2 wk | |||||
| No | 957 (86.5) | 104 (13.0) | 693 (87.0) | 169 (18.5) | 745 (81.5) |
| Yes | 144 (13.0) | 12 (11.0) | 97 (89.0) | 29 (21.0) | 109 (79.0) |
| No answer | 6 (0.5) | 2 (40.0) | 3 (60.0) | 3 (50.0) | 3 (50.0) |
| Used public transportation or ride share services in past 2 wk | |||||
| No | 1039 (93.9) | 113 (13.2)c | 745 (86.8) | 189 (19.1) | 801 (80.9) |
| Yes | 62 (5.6) | 3 (6.3) | 45 (93.8) | 8 (14.5) | 53 (85.5) |
| No answer | 6 (0.5) | 2 (40.0) | 3 (60.0) | 3 (50.0) | 3 (50.0) |
| Attended social gatherings with nonhousehold members in past 2 wk | |||||
| No | 993 (89.7) | 105 (12.8) | 714 (87.2) | 181 (19.1) | 768 (80.9) |
| Yes | 112 (10.1) | 13 (14.4) | 77 (85.6) | 20 (18.5) | 88 (81.5) |
| No answer | 2 (0.2) | 0 | 2 (100.0) | 0 | 1 (100.0) |
| Attended indoor gatherings with nonhousehold members in past 2 wk | |||||
| No | 1046 (94.5) | 109 (12.6)c | 753 (87.4) | 192 (19.2) | 807 (80.8) |
| Yes | 59 (5.3) | 9 (19.1) | 38 (80.9) | 9 (15.5) | 49 (84.5) |
| No answer | 2 (0.2) | 0 | 2 (100.0) | 0 | 1 (100.0) |
| Face covering use while <6 ft away from others all of the time | |||||
| No | 85 (7.7) | 4 (5.4)b | 70 (94.6) | 13 (16.0) | 68 (84.0) |
| Yes | 1022 (92.3) | 114 (12.6) | 723 (86.4) | 188 (19.2) | 789 (80.8) |
| Hand washing when returning home or after touching something all or most of the time | |||||
| No | 33 (3.0) | 3 (11.1) | 24 (88.9) | 5 (16.1) | 26 (83.9) |
| Yes | 1074 (97.0) | 115 (13.0) | 769 (87.0) | 196 (19.1) | 831 (80.9) |
| Possible exposure to someone with COVID-19 at home in the past 2 wkd | |||||
| No | 986 (89.1) | 79 (9.8)b | 725 (90.2) | 178 (18.8) | 767 (81.2) |
| Yes | 121 (10.9) | 39 (36.4) | 68 (63.6) | 23 (20.4) | 90 (79.6) |
| Possible exposure to someone with COVID-19 at home since the start of the pandemice | |||||
| No | 909 (82.1) | 68 (9.2)b | 675 (90.9) | 152 (17.4)b | 723 (82.6) |
| Yes | 198 (17.9) | 50 (29.8) | 118 (70.2) | 49 (26.8) | 134 (73.2) |
Abbreviations: IgG, immunoglobulin G; TMA, transcription-mediated amplification.
Missing entries were excluded from bivariate analyses.
P < .05.
P < .20.
Lived with someone who had COVID-19 symptoms or positive in the past 2 weeks.
Lived with someone who had COVID-19 symptoms or positive since the start of the pandemic.
Table 3. Work-Related Risk Factors for TMA and IgG Positivity Among Farmworkers, Monterey County, 2020.
| Attribute | Individuals, No. (%)a | ||||
|---|---|---|---|---|---|
| All enrolled (N = 1107) | SARS-CoV-2 infection | ||||
| TMA positive (n = 911) | IgG positive (n = 1058) | ||||
| Yes (n = 118) | No (n = 793) | Yes (n = 201) | No (n = 857) | ||
| H2A visa holder | |||||
| No | 1029 (93.0) | 107 (12.7) | 733 (87.3) | 188 (19.2) | 792 (80.8) |
| Yes | 65 (5.9) | 9 (15.0) | 51 (85.0) | 11 (16.9) | 54 (83.1) |
| No answer | 13 (1.2) | 2 (18.2) | 9 (81.8) | 2 (15.4) | 11 (84.6) |
| Supervisor or mayordomo | |||||
| No | 1015 (91.7) | 111 (12.8) | 756 (87.2) | 183 (18.9) | 784 (81.1) |
| Yes | 50 (4.5) | 7 (15.9) | 37 (84.1) | 9 (18.4) | 40 (81.6) |
| No answer | 42 (3.8) | 0 | 0 | 9 (21.4) | 33 (78.6) |
| Type of agricultural work ever or in the past 2 wkb | |||||
| Worked in the fields | 825 (74.5) | 100 (14.7)c | 580 (85.3) | 162 (20.4)c | 633 (79.6) |
| Packing shed | 133 (12.0) | 11 (10.5) | 94 (89.5) | 21 (16.4) | 107 (83.6) |
| Processing facility | 63 (5.7) | 4 (7.0)d | 53 (93.0) | 7 (12.1)d | 51 (87.9) |
| Nursery | 38 (3.4) | 4 (12.1) | 29 (87.9) | 4 (11.4) | 31 (88.6) |
| Truck driver | 38 (3.4) | 4 (12.1) | 29 (87.9) | 3 (9.1)d | 30 (90.9) |
| Packing truck | 22 (2.0) | 1 (4.8) | 20 (95.2) | 2 (9.5) | 19 (90.5) |
| Other | 21 (1.9) | 1 (5.3) | 18 (94.7) | 2 (10.5) | 17 (89.5) |
| No answer | 10 (0.9) | 0 | 1 (100.0) | 2 (20.0) | 8 (80.0) |
| Worked indoors | |||||
| No | 844 (76.2) | 98 (14.3)c | 589 (85.7) | 166 (20.4)c | 646 (79.6) |
| Yes | 262 (23.7) | 20 (9.0) | 203 (91.0) | 35 (14.3) | 210 (85.7) |
| No answer | 1 (0.1) | 0 | 1 (100.0) | 0 | 1 (100.0) |
| Crops worked ever or in the past 2 wkb | |||||
| Berries | 236 (28.6) | 14 (7.2)c | 181 (92.8) | 39 (16.7)d | 194 (83.3) |
| Leafy greens | 218 (26.4) | 31 (17.9)d | 142 (82.1) | 50 (24.2)d | 157 (75.8) |
| Broccoli | 155 (18.8) | 28 (18.9)d | 120 (81.1) | 24 (16.3)d | 123 (83.7) |
| Grapes | 59 (7.2) | 10 (21.3)d | 37 (78.7) | 15 (26.3) | 42 (73.7) |
| Peas | 52 (6.3) | 16 (30.8)c | 36 (69.2) | 5 (10.0)e | 45 (90.0) |
| Cauliflower | 42 (5.1) | 5 (13.5) | 32 (86.5) | 11 (30.6)d | 25 (69.4) |
| Celery | 19 (2.3) | 2 (11.8) | 15 (88.2) | 3 (18.8) | 13 (81.3) |
| Artichokes | 6 (0.7) | 0 | 5 (100.0) | 1 (16.7) | 5 (83.3) |
| Other | 158 (19.2) | 9 (8.4)c | 98 (91.6) | 35 (22.6) | 120 (77.4) |
| Commuted to work with nonhousehold members | |||||
| No | 707 (63.9) | 65 (10.9)c | 530 (89.1) | 124 (18.5) | 548 (81.5) |
| Yes | 380 (34.3) | 53 (16.8) | 263 (83.2) | 72 (19.7) | 294 (80.3) |
| No answer | 20 (1.8) | 0 | 0 | 5 (25.0) | 15 (75.0) |
| Used face covering at work all the time | |||||
| No | 112 (10.1) | 11 (11.7) | 83 (88.3) | 19 (18.1) | 86 (81.9) |
| Yes | 992 (89.6) | 107 (13.1) | 709 (86.9) | 182 (19.2) | 768 (80.8) |
| No answer | 3 (0.3) | 0 | 1 (100.0) | 0 | 3 (100.0) |
| Came within 6 ft from others while working | |||||
| No | 501 (45.3) | 52 (12.6) | 361 (87.4) | 95 (19.7) | 388 (80.3) |
| Yes | 568 (51.3) | 64 (13.4) | 413 (86.6) | 97 (18.0) | 441 (82.0) |
| No answer | 38 (3.4) | 2 (9.5) | 19 (90.5) | 9 (24.3) | 28 (75.7) |
| Possible exposure to someone with COVID-19 at work in past 2 wkf | |||||
| No | 958 (86.5) | 83 (10.9)c | 680 (89.1) | 178 (19.3) | 744 (80.7) |
| Yes | 149 (13.5) | 35 (23.6) | 113 (76.4) | 23 (16.9) | 113 (83.1) |
| No answer | 0 | 0 | 0 | 0 | 0 |
| Possible exposure to someone with COVID-19 at work since the start of the pandemicg | |||||
| No | 665 (60.1) | 52 (9.9)c | 471 (90.1) | 117 (18.3) | 524 (81.7) |
| Yes | 442 (39.9) | 66 (17.0) | 322 (83.0) | 84 (20.1) | 333 (79.9) |
| No answer | 0 | 0 | 0 | 0 | 0 |
Abbreviations: IgG, immunoglobulin G; TMA, transcription-mediated amplification.
Missing entries were excluded from bivariate analyses.
Bivariate analyses compared each agricultural job with all other jobs and working in each crop with working in all other crops. Some participants worked in a variety of jobs and crops.
P < .05.
P < .20.
P < .10.
Worked with someone who had COVID-19 symptoms, tested positive for SARS-CoV-2, or who quarantined in the past 2 weeks.
Worked with someone who had COVID-19 symptoms, tested positive for SARS-CoV-2, or who quarantined since the start of the pandemic.
Table 4. Employer-Provided Preventive Measures and Their Association With TMA and IgG Positivity Among Farmworkers, Monterey County, 2020.
| Attribute | Individuals, No. (%)a | ||||
|---|---|---|---|---|---|
| All enrolled (N = 1107) | SARS-CoV-2 infection | ||||
| TMA positive (n = 911) | IgG positive (n = 1058) | ||||
| Yes (n = 118) | No (n = 793) | Yes (n = 201) | No (n = 857) | ||
| Fever and symptoms screening upon arrival at workplace | |||||
| Neither | 495 (44.7) | 54 (16.6)b | 272 (83.4) | 92 (19.2) | 388 (80.8) |
| Either or both | 611 (55.2) | 64 (10.9) | 521 (89.1) | 109 (18.9) | 468 (81.1) |
| No answer | 1 (0.1) | 0 | 0 | 0 | 1 (100.0) |
| Employer provided face coverings | |||||
| No | 168 (15.2) | 15 (12.1) | 109 (87.9) | 26 (16.0) | 136 (84.0) |
| Yes | 932 (84.2) | 102 (13.0) | 681 (87.0) | 174 (19.6) | 715 (80.4) |
| No answer | 7 (0.6) | 1 (25.0) | 3 (75.0) | 1 (14.3) | 6 (85.7) |
| Employer provided gloves | |||||
| No | 161 (14.5) | 12 (9.0)c | 121 (91.0) | 26 (17.1) | 126 (82.9) |
| Yes | 945 (85.4) | 106 (13.6) | 671 (86.4) | 175 (19.3) | 730 (80.7) |
| No answer | 1 (0.1) | 0 | 1 (100.0) | 0 | 1 (100.0) |
| Employer provided eye shields | |||||
| No | 542 (49.0) | 52 (11.7) | 392 (88.3) | 94 (18.1) | 424 (81.9) |
| Yes | 564 (50.9) | 66 (14.2) | 400 (85.8) | 107 (19.9) | 432 (80.1) |
| No answer | 1 (0.1) | 0 | 1 (100.0) | 0 | 1 (100.0) |
| Employer provided hand washing stations | |||||
| No | 6 (0.5) | 1 (20.0) | 4 (80.0) | 2 (33.3) | 4 (66.7) |
| Yes | 1100 (99.4) | 117 (12.9) | 788 (87.1) | 199 (18.9) | 852 (81.1) |
| No answer | 1 (0.1) | 0 | 1 (100.0) | 0 | 1 (100.0) |
| Employer provided liquid soap and paper towels | |||||
| No | 15 (1.4) | 2 (16.7) | 10 (83.3) | 4 (26.7) | 11 (73.3) |
| Yes | 1090 (98.5) | 116 (12.9) | 781 (87.1) | 196 (18.8) | 845 (81.2) |
| No answer | 2 (0.2) | 0 | 2 (100.0) | 1 (50.0) | 1 (50.0) |
| Employer provided hand sanitizer | |||||
| No | 95 (8.6) | 8 (11.4) | 62 (88.6) | 20 (22.5) | 69 (77.5) |
| Yes | 1011 (91.3) | 110 (13.1) | 730 (86.9) | 181 (18.7) | 787 (81.3) |
| No answer | 1 (0.1) | 0 | 1 (100.0) | 0 | 1 (100.0) |
| Workplace surfaces and tools regularly disinfected and kept clean | |||||
| No | 122 (11.0) | 12 (12.8) | 82 (87.2) | 17 (14.8) | 98 (85.2) |
| Yes | 946 (85.5) | 98 (12.5) | 687 (87.5) | 175 (19.3) | 730 (80.7) |
| No answer | 39 (3.5) | 8 (25.0) | 24 (75.0) | 9 (23.7) | 29 (76.3) |
| Employer staggered breaks to reduce exposure | |||||
| No | 608 (54.9) | 66 (13.4) | 428 (86.6) | 112 (19.2) | 471 (80.8) |
| Yes | 492 (44.4) | 51 (12.3) | 362 (87.7) | 89 (19.0) | 380 (81.0) |
| No answer | 7 (0.6) | 1 (25.0) | 3 (75.0) | 0 | 6 (100.0) |
| Employer provided information on COVID-19 symptoms | |||||
| No | 64 (5.8) | 6 (15.0) | 34 (85.0) | 17 (27.4)d | 45 (72.6) |
| Yes | 1040 (93.9) | 112 (12.9) | 758 (87.1) | 184 (18.5) | 809 (81.5) |
| No answer | 3 (0.3) | 0 | 1 (100.0) | 0 | 3 (100.0) |
| Employer provided information on how workers can protect themselves at work | |||||
| No | 37 (3.3) | 1 (4.8) | 20 (95.2) | 12 (34.3)b | 23 (65.7) |
| Yes | 1067 (96.4) | 117 (13.2) | 772 (86.8) | 189 (18.5) | 831 (81.5) |
| No answer | 3 (0.3) | 0 | 1 (100.0) | 0 | 3 (100.0) |
| Employer provided information on how workers can protect themselves at home and in the community | |||||
| No | 70 (6.3) | 3 (6.4)c | 44 (93.6) | 17 (25.4)c | 50 (74.6) |
| Yes | 1034 (93.4) | 115 (13.3) | 748 (86.7) | 184 (18.6) | 804 (81.4) |
| No answer | 3 (0.3) | 0 | 1 (100.0) | 0 | 3 (100.0) |
| Employer provided information on whom to call if workers were sick | |||||
| No | 134 (12.1) | 18 (18.2)c | 81 (81.8) | 27 (20.9) | 102 (79.1) |
| Yes | 970 (87.6) | 100 (12.3) | 711 (87.7) | 174 (18.8) | 752 (81.2) |
| No answer | 3 (0.3) | 0 | 1 (100.0) | 0 | 3 (100.0) |
| Employer provided information on workers’ ability to get free testing and treatment if they were sick | |||||
| No | 303 (27.4) | 31 (13.1) | 206 (86.9) | 62 (21.5) | 227 (78.5) |
| Yes | 800 (72.3) | 87 (12.9) | 585 (87.1) | 138 (18.0) | 627 (82.0) |
| No answer | 4 (0.4) | 0 | 2 (100.0) | 1 (25.0) | 3 (75.0) |
| Employer provided information on where workers could get housing if they needed to quarantine or isolate away from home | |||||
| No | 607 (54.8) | 70 (14.1) | 428 (85.9) | 112 (19.3) | 467 (80.7) |
| Yes | 496 (44.8) | 48 (11.7) | 363 (88.3) | 88 (18.5) | 387 (81.5) |
| No answer | 4 (0.4) | 0 | 2 (100.0) | 1 (25.0) | 3 (75.0) |
| Employer provided information on the importance of staying away from work if workers were sick | |||||
| No | 78 (7.0) | 5 (9.1) | 50 (90.9) | 15 (19.5) | 62 (80.5) |
| Yes | 1024 (92.5) | 113 (13.2) | 741 (86.8) | 185 (19.0) | 791 (81.0) |
| No answer | 5 (0.5) | 0 | 2 (100.0) | 1 (20.0) | 4 (80.0) |
| Employer provided information on workers’ benefit to get paid to stay away from work if they were sick | |||||
| No | 334 (30.2) | 36 (13.7) | 227 (86.3) | 58 (18.4) | 258 (81.6) |
| Yes | 769 (69.5) | 82 (12.7) | 564 (87.3) | 142 (19.2) | 596 (80.8) |
| No answer | 4 (0.4) | 0 | 2 (100.0) | 1 (25.0) | 3 (75.0) |
| Received education about COVID-19 from medical staff at workplace | |||||
| No | 714 (64.5) | 76 (13.0) | 508 (87.0) | 126 (18.5) | 556 (81.5) |
| Yes | 373 (33.7) | 41 (13.1) | 271 (86.9) | 73 (20.5) | 283 (79.5) |
| No answer | 20 (1.8) | 1 (6.7) | 14 (93.3) | 2 (10.0) | 18 (90.0) |
Abbreviations: IgG, immunoglobulin G; TMA, transcription-mediated amplification.
Missing entries were excluded from bivariate analyses.
P < .05.
P < .20.
P < .10.
We used multiple imputation with chained equations to account for missing values (<2.5% missing for all variables) in our multivariable analyses. To account for differences between those recruited at clinics vs community events, as well as changes in the background positivity rate in Monterey County over the course of the study period,2 we grouped participants into strata by recruitment site and period (ie, July 16 to August 31, September 1 to 30, October 1 to 31, and November 1 to 30). We used conditional fixed-effects Poisson models15 to estimate adjusted relative risks (aRRs) while accounting for differences among strata, estimating robust standard errors using the Huber-White estimator. For multivariable models, statistical significance was set at P < .05. Analyses were conducted with Stata version 15.0 (StataCorp) and R version 3.6.1 (R Project for Statistical Computing). Given the limitations of relying on thresholds of statistical significance,16 we interpret our effect estimates based on their magnitude and precision, in light of the available sample size, instead of conditioning all conclusions on binary significance testing.
Results
Of 1107 participants (581 [52.5%] women), 922 (83.3%) were born in Mexico, 488 (44.1%) had primary school or lower levels of educational attainment, 697 (63.0%) were married or living as married, and 881 (79.6%) had overweight or obesity (defined as body mass index [BMI; calculated as weight in kilograms divided by height in meters squared] ≥25.0) (Table 1). Participants had a mean (SD) age of 39.7 (12.6) and had lived in the United States for a mean (SD) of 21.3 (11.1) years. Overall, 940 (84.9%) spoke Spanish at home, and 110 (9.9%) spoke 1 of 11 Indigenous languages (eg, Mixteco, Zapoteco, and Triqui). Half of participants (557 [50.3%]) reported household earnings of less than $25 000 per year. Approximately three-quarters (829 [74.9%]) lived with children, including 408 (36.9%) who lived with children aged 5 years or younger, and 206 (18.6%) lived with unrelated roommates (Table 2). Farmworkers lived with a mean (SD) of 5.5 (2.5) household members, and 404 (36.5%) lived in crowded conditions (ie, >2 persons/bedroom). Overall, 198 (17.9%) reported living with someone who had symptoms of COVID-19 or were known to be infected with SARS-CoV-2 since the pandemic started, and 121 (10.9%) reported such exposures at home in the 2 weeks preceding their test.
A total of 825 participants (74.5%) worked in the fields and farmed a variety of crops; the most common were berries (236 [28.6%]), leafy greens (218 [26.4%]), and broccoli (155 [18.8%]) (Table 3). Overall, 992 farmworkers (89.6%) reported using a face covering at work, and 380 (34.3%) commuted to work with members of other households. Nearly 40% (442 [39.9%]) worked with someone who had symptoms of COVID-19 or who was known to be infected with SARS-CoV-2 during the pandemic, and 149 (13.5%) reported such workplace exposure during the 2 weeks preceding their testing date. Almost all farmworkers reported that their employers provided them with hand sanitizer, gloves, face coverings, and handwashing stations; disinfected surfaces and tools regularly; and provided them with information on how to prevent SARS-CoV-2 transmission at work (Table 4). However, 495 (44.7%) reported that their employer did not screen for fever and symptoms on arrival at the workplace, which was recommended as part of a countywide agricultural advisory.17
Risk Factors for Positive SARS-CoV-2 Infection Results on TMA Tests
A total of 118 of the 911 participants (13.0%) who worked in agriculture in the 2 weeks preceding enrollment had positive results for SARS-CoV-2 infection on their TMA test, including 95 (18.4%) recruited at the clinics and 23 (5.8%) recruited via outreach (Table 1).2 Notably, we found that having a lower educational level, speaking Indigenous languages at home, living in the community of Greenfield, working in the fields, not working indoors, commuting to work with nonhousehold members, living or working with someone who had symptoms of COVID-19 or with known infection in the preceding 2 weeks, and not being screened for either fever or COVID-19 symptoms on arrival at work were factors associated with a higher prevalence of TMA-positive SARS-CoV-2 infection. We also observed correlations between some of these characteristics (eFigure in Supplement 1).
In multivariable analyses, the prevalence of positive results on TMA tests was higher among individuals who had only primary school or no education (aRR, 1.32; 95% CI, 0.99-1.76; non–statistically significant finding), spoke an Indigenous language at home (aRR, 1.30; 95% CI, 0.97-1.73; non–statistically significant finding), or lived with (aRR, 2.98; 95% CI, 2.06-4.32) or worked with (aRR, 1.59; 95% CI, 1.18-2.14) someone who had symptoms of COVID-19 or was known to be infected with SARS-CoV-2 in the previous 2 weeks (Figure, A). Additionally, working in the fields (vs agricultural work in all other settings) was associated with higher risk of a positive result on TMA testing (aRR, 1.60; 95% CI, 1.03-2.50). In contrast, farmworkers screened by employers for symptoms of COVID-19 or elevated temperature had a lower prevalence of TMA positivity (aRR, 0.79; 0.61-1.01; non–statistically significant finding) (Figure, A).
Figure. Risk Factors for SARS-CoV-2 Infection.
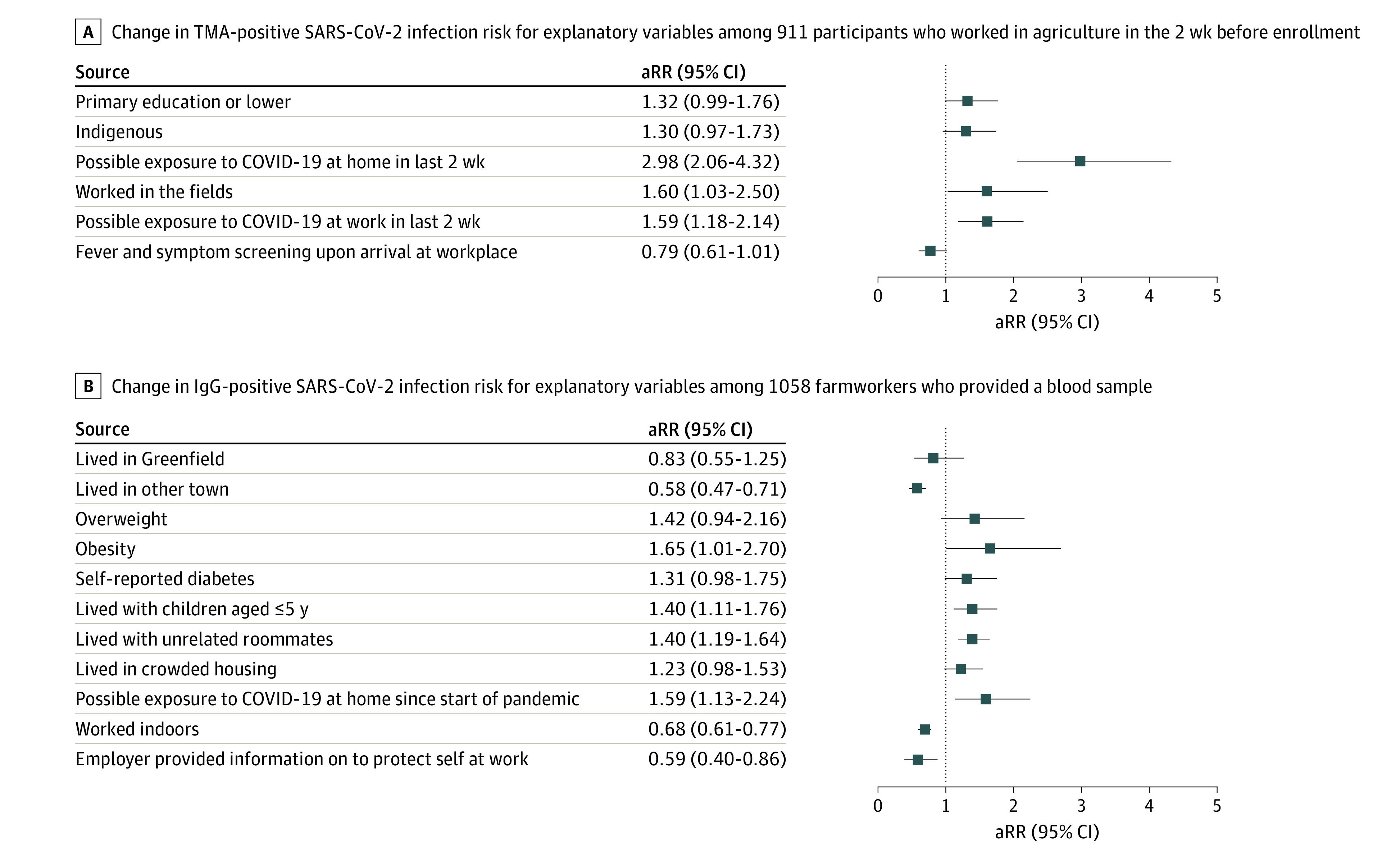
Figure shows adjusted relative risks (aRR) and 95% CIs from conditional fixed-effects Poisson models. IgG indicates immunoglobulin G; TMA, transcription-mediated amplification.
Risk Factors for Positive SARS-CoV-2 Result on IgG Test
We found that 201 of the 1058 participants (19.0%) who provided a blood sample had a positive result for SARS-CoV-2 infection on their IgG test, with similar prevalence among those tested in the clinics (97 [18.4%]) and at community sites (104 [19.5%]) (Table 1).2 Among the 118 farmworkers who had positive results on their TMA test, 22 (18.6%) also had positive results on their IgG test (9 [7.6%] missing antibody status), whereas among the 793 participants who had negative results on their TMA test, 132 (16.7%) had positive results on their IgG test (40 [5.0%] missing antibody status). In bivariate analyses, we observed that having a lower educational level, living in Salinas or Greenfield (vs other towns), having overweight or obesity, living in large households or with children 5 years or younger, living in crowded housing, having ever lived with someone who had symptoms of COVID-19 or were known to be infected with SARS-CoV-2, and working in the fields were factors associated with a higher prevalence of IgG-positive SARS-CoV-2 infection (Table 1, Table 2, Table 3). We also found that working indoors and working for an employer who provided farmworkers with information on how to protect themselves at work were conditions associated with a lower prevalence of IgG positivity (Table 3 and Table 4).
In multivariable analyses, we found that participants who had obesity (ie, BMI ≥30; aRR, 1.65; 95% CI, 1.01-2.70), overweight (ie, BMI 25.0-29.9; aRR, 1.42; 95% CI, 0.94-2.16; non–statistically significant finding), or diabetes (aRR, 1.31; 95% CI, 0.98-1.75) had a higher prevalence of positive results on their IgG tests (Figure, B). We also identified a higher prevalence of IgG positivity among those living with children 5 years or younger (aRR, 1.40; 95% CI, 1.11-1.76), with unrelated roommates (aRR, 1.40; 95% CI, 1.19-1.64), or in crowded housing (aRR, 1.23; 95% CI, 0.98-1.53; non–statistically significant finding) and those who had ever lived with someone who had symptoms of COVID-19 or were known to be infected with SARS-CoV-2 (aRR, 1.59; 95% CI, 1.13-2.24). Farmworkers who lived outside the region’s largest communities of Salinas and Greenfield (aRR, 0.58; 95% CI, 0.47-0.71), worked indoors (aRR, 0.68; 95% CI, 0.61-0.77), or whose employer provided them with information on how to protect themselves at work (aRR, 0.59; 95% CI, 0.40-0.86) had a lower risk of having a positive result for SARS-CoV-2 infection on their IgG tests (Figure, B).
Discussion
In this primarily Mexican-born and very low-income farmworker population in California, individuals with less than primary school–level education, who spoke an Indigenous language at home, who worked in the fields rather than elsewhere in agriculture, and were exposed to a known or suspected COVID-19 case at home or in the workplace had a higher prevalence of TMA-positive SARS-CoV-2 infection. We also found that IgG-positive SARS-CoV-2 infection was associated with outdoor work and with residential exposures (living with children, unrelated roommates, or an individual with known or suspected COVID-19). Those living in the more urban areas of the county were particularly at risk for IgG positivity, as were those who had obesity or diabetes. As evidence of the importance of health education, farmworkers who reported that their employer provided them with information on COVID-19 protection had a lower risk of IgG positivity for SARS-CoV-2 infection.
Our study suggests several routes of SARS-CoV-2 exposure that may be of importance to the farmworker population. Unsurprisingly, individuals living in crowded housing or with unrelated roommates had a higher prevalence of IgG positivity for SARS-CoV-2 infection. Independent of these findings, we also observed a higher IgG positivity prevalence among individuals living with children 5 years or younger. While the role of children in SARS-CoV-2 transmission has been uncertain in many populations, in part due to lower risk of symptoms and lower frequency of testing at younger ages,18,19,20 recent investigations have demonstrated equivalent viral load across ages21 and higher risk of transmission from infected children than from adults, given similar household exposures.22 While schools and formal daycare establishments were closed during our study, informal or home-based childcare arrangements with relatives or friends may have led to additional exposure to infection. Taken together, our findings suggest substantial risk of infection associated with residential exposures in this low-income population of essential workers.
Several workplace factors were also associated with infection risk. Farmworkers whose employers provided informational resources on preventing COVID-19 at work had 41% lower risk of IgG positivity for SARS-CoV-2 infection, whereas farmworkers whose employers screened them for symptoms or fever had a 21% lower risk of TMA positivity. This reduction could owe to benefits of health education, as well as more stringent efforts by employers to reduce risk by providing education and screenings. Individuals working outside and in the fields were more likely to have both TMA and IgG positivity. Whereas indoor exposures are thought to be associated with the greatest risk of transmission,23 a lower perceived sense of risk during outdoor work or socioeconomic differences between outdoor and indoor workers may contribute to the observed association in our study. While the estimated risk ratio for infection associated with workplace exposure was lower than that for household exposure, this difference could in part reflect misclassification if individuals are more likely to know about the health of household members. Previously, we have reported higher SARS-CoV-2 test positivity among farmworkers than among age- and sex-matched adults from the same communities who also received testing at CSVS,2 further supporting the hypothesis that workplace exposures specific to agriculture may be of importance to SARS-CoV-2 transmission.
Finally, we observed that farmworkers who spoke an Indigenous language at home and those with less than primary school–level education had a higher prevalence of positive results on their TMA tests at the time of enrollment. Those who spoke Indigenous languages also had a lower educational level and had more recently arrived in the United States. They lived in more crowded conditions and were more likely to live in Greenfield, work in the fields, and commute to work with non–household members (eFigure in Supplement 1). Only limited COVID-19 health messages have been provided in Indigenous languages, which are primarily not written languages.
We found associations of IgG positivity for SARS-CoV-2 infection with comorbid conditions. While it is known that obesity increases the risk of severe COVID-19 illness,24 we observed an increased risk of IgG positivity among individuals with obesity. This finding is consistent with a recent meta-analysis of 20 studies,24 which found 46% greater odds of SARS-CoV-2 infection among individuals with obesity, possibly related to alterations in systemic metabolism, including altered adipokines25,26,27 and chronic low-grade inflammation.28,29 Similarly, diabetes can attenuate the synthesis of proinflammatory cytokines and their downstream acute phase reactants,30 but also impair macrophage and lymphocyte functions.31 As obesity and diabetes are prevalent among farmworkers as well as other low-income Latino populations, our findings that these conditions are associated with higher risk of infection add to previous concerns based on the knowledge that these conditions may also exacerbate risk of adverse clinical outcomes.
Strengths and Limitations
Our work represents one of the first epidemiological studies to address risk factors for SARS-CoV-2 infection among US farmworkers and substantiates earlier concerns32,33,34,35 that living and working conditions in this population may contribute to risk of infection. However, several limitations should be considered. We cannot determine how well our sample represents the farmworker population, many of whom are hidden due to their informal workforce participation and undocumented status.36 In addition, under the busy conditions of study recruitment in this clinical setting, we could not document participation rates systematically. As we excluded individuals who did not speak Spanish or English sufficiently well to participate, our study likely underrepresents Indigenous populations. We observed differences in prevalence of TMA positivity but not IgG positivity for SARS-CoV-2 infection between study participants recruited at clinics and those recruited via community outreach events,2 as individuals seeking testing at clinics were more likely to be symptomatic or to report recent known exposure; to mitigate confounding, we defined strata by recruitment site. Furthermore, waning antibodies, particularly for individuals experiencing mild or asymptomatic infection,37 may have contributed to misclassification for individuals infected early in the pandemic. Misclassification of active infections may have also occurred given that TMA tests can remain positive after a person has recovered from a SARS-CoV-2 infection due to detection of nonviable viral RNA.38 Additionally, many identified risk factors were highly correlated, making it difficult to separate their unique associations. Larger studies of farmworkers that allow for fine-grained analysis of living and working conditions with SARS-CoV-2 transmission are warranted.
Conclusions
Our findings underscore the urgent need to intervene on modifiable risk factors associated with SARS-CoV-2 infection among farmworkers in California, such as increasing availability of isolation facilities to reduce exposure to COVID-19 cases at home and access to paid medical leave to avoid transmission in the workplace. Individuals who spoke Indigenous languages at home, had lower levels of formal education, and lived in rural communities had a higher prevalence of infection in our study, which demonstrate disparities even within this very low-income population. Efficacious vaccines should be distributed to farmworkers with urgency owing to the high risk of infection in this population and the essential nature of their work.
eTable 1. Sociodemographic and Health-Related Risk Factors for TMA and IgG Positivity Among Farmworkers, Monterey County, 2020
eTable 2. Household and Community Risk Factors for TMA and IgG Positivity Among Farmworkers, Monterey County, 2020
eTable 3. Work-Related Risk Factors for TMA and IgG Positivity Among Farmworkers, Monterey County, 2020
eTable 4. Employer-Provided Preventive Measures and Their Association With TMA and IgG Positivity Among Farmworkers, Monterey County, 2020
eFigure. Correlation Heat Map of Risk Factors Associated With TMA and IgG Positivity Among Farmworkers, Monterey County, 2020
Nonauthor Collaborators
References
- 1.Kissam E.The impact of the COVID-19 pandemic on California farmworkers: better local data collection and reporting will improve strategic response. Stat J IAOS. 2020;36(4):867-898. doi: 10.3233/SJI-200763 [DOI] [Google Scholar]
- 2.Lewnard JA, Mora AM, Nkwocha O, et al. ; CHAMACOS-Project-19 Study Team . Prevalence and clinical profile of severe acute respiratory syndrome coronavirus 2 infection among farmworkers, California, USA, June-November 2020. Emerg Infect Dis. 2021;27(5):1330-1342. doi: 10.3201/eid2705.204949 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Moreno E. COVID-19 data, metrics and updates. November 17, 2020. Accessed August 4, 2021. https://www.co.monterey.ca.us/home/showdocument?id=96259
- 4.Chen Y-H, Glymour M, Riley A, et al. Excess mortality associated with the COVID-19 pandemic among Californians 18–65 years of age, by occupational sector and occupation: March through October 2020. medRxiv. Preprint published online January 22, 2021. doi: 10.1101/2021.01.21.21250266 [DOI] [PMC free article] [PubMed]
- 5.Riley AR, Chen Y-H, Matthay EC, et al. Excess deaths among Latino people in California during the COVID-19 pandemic. medRxiv. Preprint published online January 25, 2021. doi: 10.1101/2020.12.18.20248434 [DOI] [PMC free article] [PubMed]
- 6.Dyal JW, Grant MP, Broadwater K, et al. COVID-19 among workers in meat and poultry processing facilities—19 states, April 2020. MMWR Morb Mortal Wkly Rep. 2020;69(18):69. doi: 10.15585/mmwr.mm6918e3 [DOI] [PubMed] [Google Scholar]
- 7.Steinberg J, Kennedy ED, Basler C, et al. COVID-19 outbreak among employees at a meat processing facility—South Dakota, March–April 2020. MMWR Morb Mortal Wkly Rep. 2020;69(31):1015-1019. doi: 10.15585/mmwr.mm6931a2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.COVID-19 Farmworkers Study . Preliminary data brief. July 27, 2020. Accessed December 15, 2020. http://covid19farmworkerstudy.org/survey/wp-content/uploads/2020/08/EN-COFS-Preliminary-Data-Brief_FINAL.pdf
- 9.Stephenson J. COVID-19 outbreaks among food production workers may intensify pandemic’s disproportionate effects on people of color. JAMA Health Forum. 2020;1(6):e200783. doi: 10.1001/jamahealthforum.2020.0783 [DOI] [PubMed] [Google Scholar]
- 10.Hernandez T, Gabbard S. Findings from the National Agricultural Workers Survey (NAWS) 2015–2016: a demographic and employment profile of United States farmworkers. JBS International. January 2018. Accessed December 15, 2020. https://www.dol.gov/sites/dolgov/files/OASP/legacy/files/NAWS-Research-Report-13.pdf
- 11.Mines R, Nichols S, Runsten D. California’s indigenous farmworkers: final report of the Indigenous Farmworker Study (IFS). January 2010. Accessed April 13, 2021. http://www.indigenousfarmworkers.org/IFS%20Full%20Report%20_Jan2010.pdf
- 12.California Institute for Rural Studies . Farmworker housing study and action plan for Salinas Valley and Pajaro Valley. April 2018. Accessed August 4, 2021. https://www.co.monterey.ca.us/home/showdocument?id=63729
- 13.Bradman A, Chevrier J, Tager I, et al. Association of housing disrepair indicators with cockroach and rodent infestations in a cohort of pregnant Latina women and their children. Environ Health Perspect. 2005;113(12):1795-1801. doi: 10.1289/ehp.7588 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wernecke M, Mullen C. Molecular biology in microbiological analysis. In: Batt CA, Tortorello ML, eds. Encyclopedia of Food Microbiology. Second ed. Academic Press; 2014:808-814. doi: 10.1016/B978-0-12-384730-0.00225-1 [DOI] [Google Scholar]
- 15.Armstrong BG, Gasparrini A, Tobias A. Conditional Poisson models: a flexible alternative to conditional logistic case cross-over analysis. BMC Med Res Methodol. 2014;14(1):122. doi: 10.1186/1471-2288-14-122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Amrhein V, Greenland S, McShane B. Scientists rise up against statistical significance. Nature. Published online March 20, 2019. Accessed August 9, 2021. https://www.nature.com/articles/d41586-019-00857-9 [DOI] [PubMed]
- 17.County of Monterey; Monterey County Agricultural Commissioner; Monterey County Farm Bureau; Grower-Shipper Association of Central California; Monterey County Vintners & Growers Association; Coastal Growers Association; California Strawberry Commission . Advisory for agricultural worker protection during COVID-19 crisis on the central coast of California. Accessed January 25, 2021. https://www.co.monterey.ca.us/home/showdocument?id=88499
- 18.Kim L, Whitaker M, O’Halloran A, et al. ; COVID-NET Surveillance Team . Hospitalization rates and characteristics of children aged <18 years hospitalized with laboratory-confirmed COVID-19—COVID-NET, 14 states, March 1-July 25, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1081-1088. doi: 10.15585/mmwr.mm6932e3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Swann OV, Holden KA, Turtle L, et al. ; ISARIC4C Investigators . Clinical characteristics of children and young people admitted to hospital with COVID-19 in United Kingdom: prospective multicentre observational cohort study. BMJ. 2020;370:m3249. doi: 10.1136/bmj.m3249 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Zhen-Dong Y, Gao-Jun Z, Run-Ming J, et al. Clinical and transmission dynamics characteristics of 406 children with coronavirus disease 2019 in China: a review. J Infect. 2020;81(2):e11-e15. doi: 10.1016/j.jinf.2020.04.030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jones TC, Biele G, Mühlemann B, et al. Estimating infectiousness throughout SARS-CoV-2 infection course. Science. 2021;373(6551):eabi5273. doi: 10.1126/science.abi527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Li F, Li Y-Y, Liu M-J, et al. Household transmission of SARS-CoV-2 and risk factors for susceptibility and infectivity in Wuhan: a retrospective observational study. Lancet Infect Dis. 2021;21(5):617-628. doi: 10.1016/S1473-3099(20)30981-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bulfone TC, Malekinejad M, Rutherford GW, Razani N. Outdoor transmission of SARS-CoV-2 and other respiratory viruses: a systematic review. J Infect Dis. 2021;223(4):550-561. doi: 10.1093/infdis/jiaa742 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Popkin BM, Du S, Green WD, et al. Individuals with obesity and COVID-19: a global perspective on the epidemiology and biological relationships. Obes Rev. 2020;21(11):e13128. doi: 10.1111/obr.13128 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Rasouli N, Kern PA. Adipocytokines and the metabolic complications of obesity. J Clin Endocrinol Metab. 2008;93(11)(suppl 1):S64-S73. doi: 10.1210/jc.2008-1613 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Grossmann V, Schmitt VH, Zeller T, et al. Profile of the immune and inflammatory response in individuals with prediabetes and type 2 diabetes. Diabetes Care. 2015;38(7):1356-1364. doi: 10.2337/dc14-3008 [DOI] [PubMed] [Google Scholar]
- 27.Wada J, Makino H. Innate immunity in diabetes and diabetic nephropathy. Nat Rev Nephrol. 2016;12(1):13-26. doi: 10.1038/nrneph.2015.175 [DOI] [PubMed] [Google Scholar]
- 28.Maurizi G, Della Guardia L, Maurizi A, Poloni A. Adipocytes properties and crosstalk with immune system in obesity-related inflammation. J Cell Physiol. 2018;233(1):88-97. doi: 10.1002/jcp.25855 [DOI] [PubMed] [Google Scholar]
- 29.McLaughlin T, Ackerman SE, Shen L, Engleman E. Role of innate and adaptive immunity in obesity-associated metabolic disease. J Clin Invest. 2017;127(1):5-13. doi: 10.1172/JCI88876 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Odegaard JI, Chawla A. Connecting type 1 and type 2 diabetes through innate immunity. Cold Spring Harb Perspect Med. 2012;2(3):a007724. doi: 10.1101/cshperspect.a007724 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Dooley KE, Chaisson RE. Tuberculosis and diabetes mellitus: convergence of two epidemics. Lancet Infect Dis. 2009;9(12):737-746. doi: 10.1016/S1473-3099(09)70282-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Handal AJ, Iglesias-Ríos L, Fleming PJ, Valentín-Cortés MA, O’Neill MS. “Essential” but expendable: farmworkers during the COVID-19 pandemic—the Michigan Farmworker Project. Am J Public Health. 2020;110(12):1760-1762. doi: 10.2105/AJPH.2020.305947 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bojorquez K. CA lawmakers urge relief for farm workers amid pandemic. The Sacramento Bee. Published August 2020. Accessed January 25, 2021. https://www.sacbee.com/news/politics-government/capitol-alert/article244769262.html
- 34.Lazo A. As California struggles with COVID-19, farmworkers are among most affected. The Wall Street Journal. August 17, 2020. Accessed January 25, 2021. https://www.wsj.com/articles/as-california-struggles-with-covid-19-farmworkers-are-among-most-affected-11597665116
- 35.Knight V. Without federal protections, farm workers risk coronavirus infection to harvest crops. NPR. August 8, 2020. Accessed January 25, 2021. https://www.npr.org/sections/health-shots/2020/08/08/900220260/without-federal-protections-farm-workers-risk-coronavirus-infection-to-harvest-c
- 36.Bail KM, Foster J, Dalmida SG, et al. The impact of invisibility on the health of migrant farmworkers in the southeastern United States: a case study from Georgia. Nurs Res Pract. Published online July 1, 2012. doi: 10.1155/2012/760418 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Choe PG, Kang CK, Suh HJ, et al. Waning antibody responses in asymptomatic and symptomatic SARS-CoV-2 infection. Emerg Infect Dis. 2021;27(1):327-329. doi: 10.3201/eid2701.203515 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.US Food and Drug Administration. Aptima SARS-CoV-2 Assay (Panther System). Accessed August 5, 2021. https://www.fda.gov/media/138096/download
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Sociodemographic and Health-Related Risk Factors for TMA and IgG Positivity Among Farmworkers, Monterey County, 2020
eTable 2. Household and Community Risk Factors for TMA and IgG Positivity Among Farmworkers, Monterey County, 2020
eTable 3. Work-Related Risk Factors for TMA and IgG Positivity Among Farmworkers, Monterey County, 2020
eTable 4. Employer-Provided Preventive Measures and Their Association With TMA and IgG Positivity Among Farmworkers, Monterey County, 2020
eFigure. Correlation Heat Map of Risk Factors Associated With TMA and IgG Positivity Among Farmworkers, Monterey County, 2020
Nonauthor Collaborators