

Abstract
目的
探讨分体式 3D 打印个性化导板(patient-specific instrumentation,PSI)应用于内侧开放楔形胫骨高位截骨术(medial open-wedge high tibial osteotomy,MOWHTO)的准确性及其治疗膝关节内侧骨关节炎的临床疗效。
方法
回顾分析 2019 年 8 月—2020 年 8 月采用分体式 3D 打印 PSI 辅助 MOWHTO 治疗的 14 例膝关节内侧骨关节炎患者临床资料。男 5 例,女 9 例;年龄 43~68 岁,平均 61 岁。病程 1~16 年,平均 4.7 年。术前膝骨关节炎 Kellgren-Lawrence 分级:Ⅰ级 2 例、Ⅱ级 6 例、Ⅲ级 6 例。术前美国特种外科医院(HSS)评分为(59.1±4.9)分。根据术后影像学资料测量下肢负重线比率(weight bearing line ratio,WBL)、髋-膝-踝角(hip-knee-ankle angle,HKA)、胫骨近端内侧角(medial proximal tibial angle,MPTA)、胫骨平台后倾角(posterior tibial slope angle,PTSA)及实际矫正角度,并与术前测量值及设计目标值进行比较,评价该导板辅助手术的精确度;分别于术后 3、6 个月及末次随访时采用 HSS 评分评估患者膝关节功能。
结果
1 例患者术后 2 周出现切口渗液,经对症治疗后好转;其余患者切口均Ⅰ期愈合。14 例患者均获随访,随访时间 7~19 个月,平均 14.8 个月,未出现神经损伤、合页骨折、钢板螺钉断裂及松动等并发症,随访期间 X 线片示 WBL 基本维持在术后水平。患者术后测量 WBL、HKA、MPTA、PTSA 均在满意范围内,术后 WBL、HKA、MPTA 均较术前显著改善(P<0.05),PTSA 与术前比较差异无统计学意义(P>0.05);术后 WBL、HKA、MPTA、矫正角度与术前设计目标值比较差异均无统计学意义(P>0.05)。术后 3、6 个月及末次随访时 HSS 评分分别为(69.2±4.7)、(77.7±4.3)、(88.1±5.4)分,均较术前提高,手术前后各时间点间比较差异均有统计学意义(P<0.05)。
结论
对于膝关节内侧骨关节炎患者,在 MOWHTO 中应用分体式 3D 打印 PSI 可辅助术者精准截骨矫形,获得良好临床效果。
Keywords: 胫骨高位截骨术, 3D 打印, 分体式导板, 准确性, 膝骨关节炎
Abstract
Objective
To investigate the accuracy of split three-dimensional (3D) printing patient-specific instrumentation (PSI) in medial open-wedge high tibial osteotomy (MOWHTO) and its effectiveness in treating medial knee osteoarthritis.
Methods
Clinical data of 14 patients with medial knee osteoarthritis and treated with split 3D printing PSI-assisted MOWHTO between August 2019 and August 2020 were retrospectively analyzed. There were 5 males and 9 females with an average age of 61 years (range, 43-68 years). The disease duration ranged from 1 to 16 years, with an average of 4.7 years. Preoperative Kellgren-Lawrence grading of knee osteoarthritis included grade Ⅰ in 2 cases, grade Ⅱ in 6 cases, and grade Ⅲ in 6 cases. The Hospital for Special Surgery (HSS) score was 59.1±4.9. The weight bearing line ratio (WBL), hip-knee-ankle angle (HKA), medial proximal tibial angle (MPTA), posterior tibial slope angle (PTSA), and actual correction angle of the lower limbs were measured on postoperative imaging data, and compared with the preoperative measurements and the designed target values to evaluate the accuracy of the PSI-assisted surgery. The patients’ knee function were evaluated with the HSS score at 3 and 6 months postoperatively, and at last follow-up.
Results
One patient suffered from an incision exudation at 2 weeks postoperatively, and the incision healed after symptomatic treatment. The incisions of other patients healed by first intention. All patients were followed up 7-19 months (mean, 14.8 months). There was no neural injuries, hinge fracture, plate or screw fractures, loosening, or other complications. The WBL was maintained at the postoperative level according to the X-ray examination during the follow-up period. The WBL, HKA, MPTA, and PTSA were all within a satisfactory range after operation. The WBL, HKA, and MPTA were significantly improved when compared with the preoperative measurements (P<0.05). There was no significant difference between preoperative and postoperative PTSA (P>0.05). The differences in postoperative WBL, HKA, MPTA, and correction angle compared with the preoperative designed target values were not significant (P>0.05). The HSS scores were 69.2±4.7, 77.7±4.3, and 88.1±5.4 at 3 and 6 months postoperatively, and last follow-up, respectively. The differences between time points were significant (P<0.05).
Conclusion
For patients with medial knee osteoarthritis, the split 3D printing PSI can assist the surgeon in MOWHTO with accurate osteotomy orthopedics and achieve favorable effectiveness.
Keywords: High tibial osteotomy, three-dimensional printing, split guide, accuracy, knee osteoarthritis
自 Jackson 等[1]于 1961 年首次报道胫骨高位截骨术(high tibial osteotomy,HTO)以来,随着 HTO 手术技术和内固定材料的发展,对膝关节内侧骨关节炎伴有胫骨近端内翻畸形的患者采用 HTO 治疗已成为保膝领域的研究热点,并可获得良好的远期疗效,其中内侧开放楔形 HTO(medial open-wedge HTO,MOWHTO)应用较多[2-3]。
传统 HTO 在负重位下肢全长 X 线片上规划截骨角度,通过术中撑开的间隙大小和非负重位下反复 X 线透视评估力线和角度。这种方法缺点是术中仅评估了二维冠状面矫正情况、实时力线监测困难以及术中透视次数较多等,矫正精度存在不足[4-6]。得益于 3D 打印技术的进步,目前有多种 3D 打印个性化导板(patient-specific instrumentation,PSI)应用于 HTO,使截骨更简易、精确,缩短了手术时间和术者学习曲线,减少了术中透视[5, 7-10]。3D 打印 PSI 种类繁多,但存在 PSI 体积较大而需广泛剥离软组织,若缩小 PSI 体积将导致其与骨面的贴合部分减小,进而影响 PSI 准确性的问题,在减小创伤和提高准确性方面仍可进一步改善;其次,目前的 PSI 多为辅助截骨的导板,对矫正角度和校准力线存在不足。
本研究采用了一种自主研制的分体式 3D 打印 PSI,该 PSI 分为近端截骨和远端校准两部分,旨在缩小 PSI 体积且易于获得可靠的骨性贴面,同时减少重要软组织损伤,准确、快速辅助实施 HTO。现回顾分析 2019 年 8 月—2020 年 8 月应用该分体式 3D 打印 PSI 辅助 MOWHTO 治疗的膝关节内侧骨关节炎患者资料,探讨该 PSI 的准确性及其治疗膝关节内侧骨关节炎的早期临床疗效。报告如下。
1. 临床资料
1.1. 患者选择标准
纳入标准:① 年龄女性≤65 岁、男性≤68 岁;② 膝关节内侧骨关节炎,临床表现为膝关节内侧疼痛,经保守治疗无效;③ 影像学主要表现为膝关节内侧间隙变窄,内翻畸形源于胫骨近端;④ 胫骨内翻畸形>5°,胫骨近端内侧角(medial proximal tibial angle,MPTA)<85°,膝关节屈伸活动范围>90°,膝关节屈曲挛缩畸形<20°。排除标准:① 痛风性关节炎、类风湿性关节炎及血友病性关节炎等非骨关节炎患者;② 膝关节稳定性较差,下肢肌力差,骨质疏松患者;③ 伴有其他合并症且不能耐受手术者。2019 年 8 月—2020 年 8 月共 14 例患者符合选择标准纳入研究。
1.2. 一般资料
本组男 5 例,女 9 例;年龄 43~68 岁,平均 61 岁。身体质量指数 18.3~29.8 kg/m2,平均 24.0 kg/m2。左膝 4 例,右膝 10 例。患者术前膝关节以内侧疼痛为主,内翻畸形源于胫骨近端,不伴有其他膝关节明显病变。病程 1~16 年,平均 4.7 年。术前膝骨关节炎 Kellgren-Lawrence 分级[11]:Ⅰ级 2 例、Ⅱ级 6 例、Ⅲ级 6 例。术前美国特种外科医院(HSS)评分为(59.1±4.9)分。术前摄双膝关节正侧位和双下肢全长负重正位 X 线片、双下肢全长 CT,测量下肢负重线比率(weight bearing line ratio,WBL)、髋-膝-踝角(hip-knee-ankle angle,HKA)、胫骨近端内侧角(medial proximal tibial angle,MPTA)、胫骨平台后倾角(posterior tibial slope angle,PTSA)。
1.3. 术前设计
1.3.1. 数据采集与截骨规划
将患者 CT(层厚 1 mm)资料以 DICOM 格式导入 Mimics25.0 软件进行三维重建。在重建的三维模型中标记患者下肢力线和目标力线,以胫骨近端合页点(腓骨小头上 1/3,外侧平台下约 1.5 cm,距外侧皮质约 1 cm)为圆心,以合页点至踝关节中心连线为半径向外侧旋转,直至患者术前的下肢力线和目标力线重合时的旋转角度即为矫正角度。然后在重建的三维模型中设计双平面截骨,第一截骨平面开口位于鹅足上方距胫骨内侧平台约 4 cm,外侧达合页点;第二截骨平面位于胫骨结节后方,与胫骨前缘皮质大致平行。最后模拟矫正效果,在计算机上按术前设计进行截骨矫正,检验矫正后的力线位置。见图 1。记录设计的目标数据,包括 WBL、MPTA、HKA 和矫正角度。
图 1.
Planning and simulation of osteotomy
截骨规划与模拟
a. 术前设计 AC:术前下肢力线 AB:目标力线(此病例设计 WBL 为 62.5%) D:外侧合页点∠BDC:矫正角度;b. 模拟矫正效果 EF:矫正后下肢力线
a. Preoperative design AC: Preoperative lower limb force line AB: The target force line (the designed WBL for this case was 62.5%) D: Lateral hinge ∠BDC: The correction angle; b. Simulation of correctionEF: Lower limb force line after correction

1.3.2. 分体式 3D 打印 PSI 的结构
分体式 PSI 主要包括近端截骨导板、远端校准导板、固定连接杆、校准连接杆及限位垫块。近端截骨导板及远端校准导板分别位于固定连接杆两端并通过克氏针固定于胫骨,用于辅助确定截骨位置、角度、深度;完成截骨并撑开后采用校准连接杆连接近端截骨导板及远端校准导板,用于检验矫正角度;撑开至预设角度后将限位垫块插入开放楔内,辅助检验矫正角度,支撑间隙并辅助钢板安装。见图 2。
图 2.
Structure of split 3D printing PSI
分体式 3D 打印 PSI 的结构
a. 近端截骨导板和远端校准导板;b. 固定连接杆;c. 校准连接杆;d. 限位垫块
a. Proximal osteotomy guide and distal calibration guide; b. Connecting rod; c. Calibration rod; d. Positioning wedge block

1.3.3. 分体式 3D 打印 PSI 的设计及制作
在截骨规划设计完成及模拟矫正效果后,预设钢板的安装位置。首先设计近端截骨导板,近侧固定针孔对应钢板近端钉孔(D 孔),远侧平行截骨面设计 2 个平行固定针孔;再设计远端校准导板,取钢板远端第 3 孔的位置,设计固定针孔;最后设计固定连接杆、校准连接杆及限位垫块。在计算机中模拟 PSI 术中应用过程,首先安装近端截骨导板于预设位置,再安装固定连接杆及远端校准导板并临时固定;取下固定连接杆后按近端截骨导板导向进行双平面截骨及撑开;撑开后采用校准连接杆实施校验;然后采用限位垫块辅助校验及固定撑开间隙,辅助安装钢板。见图 3。将设计好的 PSI 以 STL 格式输入至 3D 打印机(Flight 403P 尼龙 3D 打印机,湖南华曙高科技有限责任公司),采用耐高温高压的高分子尼龙材料打印导板,消毒备用。
图 3.
Computer simulation of PSI in intraoperative applications
计算机模拟术中应用 PSI
a. 截骨前安装导板;b. 截骨导板辅助下行双平面截骨;c. 截骨后撑开校验;d. 限位垫块检验和辅助安装钢板
a. Installation of the PSI before osteotomy; b. Biplanar osteotomy with the aid of the osteotomy guide; c. Calibration after osteotomy; d. Calibration and installation of the plate under the guidance of the positioning wedge block

1.4. 手术方法
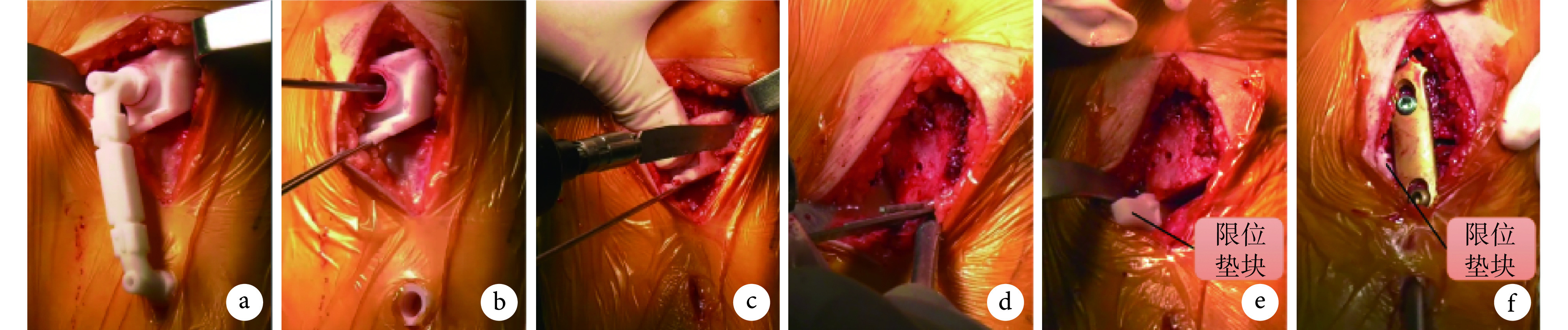
所有手术均由同一位高年资医生完成。患者取仰卧位,神经阻滞麻醉满意后消毒、铺无菌巾等。开启止血带后于胫骨近端内侧作一分段式纵切口(近侧 5~7 cm,远侧约 1 cm),依次分离皮肤及皮下组织,安装近端截骨导板(以导板与骨面贴合度、X 线透视导针方向确认其位置良好),再通过固定连接杆确认远端校准导板位置并固定。根据术前设计的目标数据,沿近端截骨导板方向进行双平面截骨。然后依次打入叠型骨刀,预计撑开至术前设计角度时安装校准连接杆,待校准连接杆刚好连接近端截骨导板和远端校准导板时停止撑开,以限位垫块辅助校验,行第二次 X 线透视辅助评估力线是否良好。矫正满意后植入钢板并用螺钉固定。见图 4。术中如果内侧撑开距离超过 1 cm 则进行植骨,术中出血较多时留置切口引流管。冲洗切口并逐层缝合,无菌敷料包扎。
图 4.
Intraoperative application of PSI
PSI 的术中应用
a、b. 安装和固定截骨导板;c、d. 根据导板及导针方向行双平面截骨;e、f. 限位垫块辅助下安装钢板
a, b. Installation and fixation of the osteotomy guide; c, d. Biplanar osteotomy according to the orientation of the osteotomy guide and Kirschner wire; e, f. Installation of the plate under the guidance of the positioning wedge block
1.5. 术后处理及疗效评价指标
术后常规镇痛、冰敷、抗炎、抬高患肢等治疗,术后第 1 天开始行股四头肌收缩训练、患肢膝关节主动及被动屈伸活动,患者可扶双拐下地,患肢踩地以不引起明显疼痛为原则;术后 4 周扶单拐行走,术后 6~8 周待 X 线片显示截骨处愈合后弃拐行走,逐步恢复正常生活[12-13]。
术后 1~3 d 摄患肢膝关节正侧位和双下肢全长负重正位 X 线片,测量 WBL、HKA、MPTA、PTSA 及实际矫正角度,并与术前测量值及设计目标值进行比较,评价该导板辅助手术的精确度;术后 3、6、12 个月,摄患肢膝关节正侧位和双下肢全长负重正位 X 线片,评估截骨处愈合及膝关节情况。术后 3、6 个月及末次随访时采用 HSS 评分评价患者膝关节功能。
1.6. 统计学方法
采用 SPSS25.0 统计软件进行分析。数据以均数±标准差表示,术后各影像学数据与术前测量值及设计目标值比较采用配对 t 检验;手术前后各时间点 HSS 评分比较采用单因素重复测量方差分析,若不符合球形假设,采用 Greenhouse-Geisser 法进行校正,不同时间点间比较采用 Bonferroni 法;检验水准 α=0.05。
2. 结果
1 例患者术后 2 周出现切口渗液,经对症治疗后好转;其余患者切口均Ⅰ期愈合。14 例患者均获随访,随访时间 7~19 个月,平均 14.8 个月。未出现神经损伤、合页骨折、钢板螺钉断裂及松动等并发症,随访期间 X 线片示 WBL 基本维持在术后水平。本组患者术后测量 WBL、HKA、MPTA、PTSA 均在满意范围内[6, 8, 14]。术后 WBL、HKA、MPTA 均较术前显著改善,差异有统计学意义(P<0.05),PTSA 与术前比较差异无统计学意义(P>0.05);术后 WBL、HKA、MPTA 及矫正角度与术前设计目标值比较,差异均无统计学意义(P>0.05)。见表 1、2,图 5。术后 3、6 个月及末次随访时 HSS 评分分别为(69.2±4.7)、(77.7±4.3)、(88.1±5.4)分,较术前明显提高,手术前后各时间点间比较差异均有统计学意义(P<0.05)。
表 1.
Comparison of pre- and post-operative imaging data (n=14,
 )
)
术前及术后各影像学数据比较(n=14,
 )
)
| 时间
Time |
WBL(%) | HKA(°) | MPTA(°) | PTSA(°) |
| 术前
Preoperative |
28.7±8.4 | 174.5±2.1 | 83.3±1.5 | 10.0±2.9 |
| 术后
Postoperative |
59.5±2.5 | 182.1±1.0 | 90.3±1.7 | 10.8±3.4 |
| 统计值
Statistic |
t=13.653
P=0.000 |
t=−12.309
P=0.000 |
t=−21.906
P=0.000 |
t=−2.132
P=0.053 |
表 2.
Comparison of postoperative imaging data and preoperative designed target value (n=14,
 )
)
术后各影像学数据与术前设计目标值比较(n=14,
 )
)
| 时间
Time |
WBL(%) | HKA(°) | MPTA(°) | 矫正角度(°)
Correction angle (°) |
| 设计目标
Designed target |
60.6±2.4 | 182.6±0.6 | 90.5±0.9 | 8.6±1.5 |
| 术后
Postoperative |
59.5±2.5 | 182.1±1.0 | 90.3±1.7 | 9.2±2.0 |
| 统计值
Statistic |
t=1.521
P=0.152 |
t=1.670
P=0.119 |
t=0.315
P=0.757 |
t=−1.649
P=0.123 |
图 5.
Anteroposterior double-limb weight bearing X-ray film of a 57-year-old female patient with medial osteoarthritis of bilateral knees (more severe pain in the left knee, bilateral Kellgren-Lawrence grade Ⅰ)
患者,女,57 岁,双膝关节内侧骨关节炎(左膝疼痛明显,双侧 Kellgren-Lawrence 分级Ⅰ级),双下肢全长负重正位 X 线片
a. 术前;b. 术后 2 个月
a. Before operation; b. At 2 months after operation

3. 讨论
HTO 治疗的核心是恢复患者下肢正常力线,减小膝关节内侧间室应力,有效缓解软骨的进一步磨损和关节退变,从而改善膝关节内侧骨关节炎的症状[14-16]。精准矫形恢复下肢力线是保证 HTO 良好远期效果的关键,也是 HTO 手术的难点[16-18]。传统 HTO 高度依赖术者经验,术中需凭借反复 X 线透视评估和调整力线及角度,力线评估受到肢体旋转、视野遮挡的影响,且难于考虑到三维矫正,因此存在矫正精度有限、医患辐射暴露多、手术时间长等不足[4-6, 19-20];而不精准的手术容易造成胫骨平台、合页骨折,胫骨平台后倾角改变等,进而影响 HTO 的疗效[21]。
随着数字医学的进步,计算机导航、3D 打印导板等技术已被应用于 HTO。有报道应用计算机导航辅助 HTO 能实现满意矫正[22-23]。最近,Cerciello 等[24]的一项荟萃分析结果表明,应用计算机导航辅助 HTO 较传统手术能减少矫正的异常值,但矫正的准确性未显著提升。另外计算机导航也存在注册失败、软件故障、学习周期长及成本高等不足[9]。应用 3D 打印导板辅助 HTO 是近年研究热点,可取得良好矫正效果[8, 19, 25]。Fucentese 等[26]的研究表明,使用 PSI 辅助 HTO 有利于获得预期的 HKA 矫正和保持胫骨后倾角基本不变;Jacquet 等[10]的一项前瞻性队列研究表明,应用 PSI 辅助 HTO 在确保矫正准确性的同时可缩短手术时间、减少术中透视次数,且学习曲线短。然而,目前报道的 PSI 结构、功能参差不齐。一方面,PSI 体积较大需要剥离较多软组织从而增加创伤,且广泛剥离不彻底会进一步影响 PSI 与骨面的贴合及矫正的准确性;另一方面,目前的 PSI 多为辅助截骨导板,对撑开角度和力线校验不足。PSI 的应用虽然取得了良好的初步临床效果,但在减小创伤、功能全面性、矫正准确性等方面尚可提升。
本研究使用的 PSI 采用了分体式结构设计,将 PSI 分为近端截骨导板和远端校验导板。首先,分体式结构设计可减小 PSI 各部分体积,不需分离鹅足等重要软组织结构,减少软组织损伤同时获得可靠的骨性贴面;其次,以近端截骨导板指示截骨的位置、角度、深度,远端校准导板进一步辅助判断矫正角度及校准后的力线,提高矫正精确度;另外,以近端截骨导板和远端校验导板固定针位置与钢板相应螺孔对应,术中限位垫块保持撑开角度的大小,可辅助钢板的安装。
目前对于 HTO 手术后应达到的理想目标力线仍存在一定争议[14, 24],本研究术前设计 WBL 为 60.6%±2.4%,术后 WBL(59.5%±2.5%)与术前设计目标差异绝对值为 2.1%±1.9%,但差异无统计学意义,与 Kim 等[19]报道的应用 PSI 辅助 HTO 所得力线与设计目标差异 2.3%±2.5% 相当,优于基于二维医学影像信息系统的 HTO 差异值 6.2%±5.1%。本组术后 HKA(182.3±1.1)° 较术前设计差异绝对值为(1.0±0.6)°,差异无统计学意义,与 Chaouche 等[25]的队列研究报道差异相当。术后实际矫正角度较术前设计差异绝对值为(0.9±0.9)°,差异无统计学意义;术后 PTSA 与术前比较差异无统计学意义,说明通过该分体式 3D 打印 PSI 辅助 MOWHTO 可以在术中同时达到良好的冠状面、矢状面矫正。从功能评分来看,本组术后 HSS 评分随时间增加均有显著提高。
综上述,分体式 3D 打印 PSI 辅助 MOWHTO 具有较高准确性,可获得满意矫正效果,且操作简便、可减少软组织损伤,避免术中反复透视调整力线和多次截骨,缩短手术时间,具备良好的实用性。但本研究样本量少,随访时间短,仍需更大样本量的随机对照研究以及更长时间随访观察,明确该导板应用的中远期疗效。
作者贡献:高发维负责研究设计及实施、数据收集整理及统计分析、论文撰写;钟达负责研究总体设计和实施、论文审阅;王成功、胡懿郃参与手术实施及对文章内容作批评性审阅;苏士龙、齐军参与手术实施,并负责随访与数据收集、分析。
利益冲突:所有作者声明,在课题研究和文章撰写过程中不存在利益冲突;基金项目经费支持没有影响文章观点和对研究数据客观结果的统计分析及其报道。
机构伦理问题:研究方案经中南大学湘雅医院医学伦理委员会批准(202008253)。
Funding Statement
国家自然科学基金资助项目(81974360)
National Natural Science Foundation of China (81974360)
References
- 1.Jackson JP, Waugh W Tibial osteotomy for osteoarthritis of the knee. J Bone Joint Surg (Br) 1961;43-B:746–751. doi: 10.1302/0301-620X.43B4.746. [DOI] [PubMed] [Google Scholar]
- 2.Hantes ME, Natsaridis P, Koutalos AA, et al Satisfactory functional and radiological outcomes can be expected in young patients under 45 years old after open wedge high tibial osteotomy in a long-term follow-up. Knee Surg Sports Traumatol Arthrosc. 2018;26(11):3199–3205. doi: 10.1007/s00167-017-4816-z. [DOI] [PubMed] [Google Scholar]
- 3.Gaasbeek RD, Nicolaas L, Rijnberg WJ, et al Correction accuracy and collateral laxity in open versus closed wedge high tibial osteotomy. A one-year randomised controlled study. Int Orthop. 2010;34(2):201–207. doi: 10.1007/s00264-009-0861-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kwun JD, Kim HJ, Park J, et al Open wedge high tibial osteotomy using three-dimensional printed models: Experimental analysis using porcine bone. Knee. 2017;24(1):16–22. doi: 10.1016/j.knee.2016.09.026. [DOI] [PubMed] [Google Scholar]
- 5.Mao Y, Xiong Y, Li Q, et al. 3D-printed patient-specific instrumentation technique vs. conventional technique in medial open wedge high tibial osteotomy: A prospective comparative atudy. Biomed Res Int, 2020, 2020: 1923172. doi: 10.1155/2020/1923172.
- 6.Iorio R, Pagnottelli M, Vadalà A, et al Open-wedge high tibial osteotomy: comparison between manual and computer-assisted techniques. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):113–119. doi: 10.1007/s00167-011-1785-5. [DOI] [PubMed] [Google Scholar]
- 7.Pérez-Mañanes R, Burró JA, Manaute JR, et al 3D surgical printing cutting guides for open-wedge high tibial osteotomy: Do it yourself. J Knee Surg. 2016;29(8):690–695. doi: 10.1055/s-0036-1572412. [DOI] [PubMed] [Google Scholar]
- 8.Munier M, Donnez M, Ollivier M, et al Can three-dimensional patient-specific cutting guides be used to achieve optimal correction for high tibial osteotomy? Pilot study. Orthop Traumatol Surg Res. 2017;103(2):245–250. doi: 10.1016/j.otsr.2016.11.020. [DOI] [PubMed] [Google Scholar]
- 9.Yang JC, Chen CF, Luo CA, et al. Clinical experience using a 3D-printed patient-specific instrument for medial opening wedge high tibial osteotomy. Biomed Res Int, 2018, 2018: 9246529. doi: 10.1155/2018/9246529.
- 10.Jacquet C, Sharma A, Fabre M, et al Patient-specific high-tibial osteotomy’s ‘cutting-guides’ decrease operating time and the number of fluoroscopic images taken after a Brief Learning Curve. Knee Surg Sports Traumatol Arthrosc. 2020;28(9):2854–2862. doi: 10.1007/s00167-019-05637-6. [DOI] [PubMed] [Google Scholar]
- 11.Kellgren JH, Lawrence JS Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502. doi: 10.1136/ard.16.4.494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Brinkman JM, Luites JW, Wymenga AB, et al Early full weight bearing is safe in open-wedge high tibial osteotomy. Acta Orthop. 2010;81(2):193–198. doi: 10.3109/17453671003619003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Saito T, Kumagai K, Akamatsu Y, et al Five- to ten-year outcome following medial opening-wedge high tibial osteotomy with rigid plate fixation in combination with an artificial bone substitute. Bone Joint J. 2014;96-B(3):339–344. doi: 10.1302/0301-620X.96B3.32525. [DOI] [PubMed] [Google Scholar]
- 14.Martay JL, Palmer AJ, Bangerter NK, et al A preliminary modeling investigation into the safe correction zone for high tibial osteotomy. Knee. 2018;25(2):286–295. doi: 10.1016/j.knee.2017.12.006. [DOI] [PubMed] [Google Scholar]
- 15.Kumagai K, Akamatsu Y, Kobayashi H, et al Factors affecting cartilage repair after medial opening-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2017;25(3):779–784. doi: 10.1007/s00167-016-4096-z. [DOI] [PubMed] [Google Scholar]
- 16.Amendola A Unicompartmental osteoarthritis in the active patient: the role of high tibial osteotomy. Arthroscopy. 2003;19 Suppl 1:109–116. doi: 10.1016/j.arthro.2003.09.048. [DOI] [PubMed] [Google Scholar]
- 17.Hernigou P, Medevielle D, Debeyre J, et al Proximal tibial osteotomy for osteoarthritis with varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg (Am) 1987;69(3):332–354. doi: 10.2106/00004623-198769030-00005. [DOI] [PubMed] [Google Scholar]
- 18.Van den Bempt M, Van Genechten W, Claes T, et al How accurately does high tibial osteotomy correct the mechanical axis of an arthritic varus knee? A systematic review. Knee. 2016;23(6):925–935. doi: 10.1016/j.knee.2016.10.001. [DOI] [PubMed] [Google Scholar]
- 19.Kim HJ, Park J, Shin JY, et al More accurate correction can be obtained using a three-dimensional printed model in open-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2018;26(11):3452–3458. doi: 10.1007/s00167-018-4927-1. [DOI] [PubMed] [Google Scholar]
- 20.Han SB, Kim HJ, Lee DH. Effect of computer navigation on accuracy and reliability of limb alignment correction following open-wedge high tibial osteotomy: A meta-analysis. Biomed Res Int, 2017, 2017: 3803457. doi: 10.1155/2017/3803457.
- 21.Lee YS, Moon GH Comparative analysis of osteotomy accuracy between the conventional and devised technique using a protective cutting system in medial open-wedge high tibial osteotomy. J Orthop Sci. 2015;20(1):129–136. doi: 10.1007/s00776-014-0663-7. [DOI] [PubMed] [Google Scholar]
- 22.Heijens E, Kornherr P, Meister C The role of navigation in high tibial osteotomy: a study of 50 patients. Orthopedics. 2009;32(10 Suppl):40–43. doi: 10.3928/01477447-20090915-58. [DOI] [PubMed] [Google Scholar]
- 23.Kim SJ, Koh YG, Chun YM, et al Medial opening wedge high-tibial osteotomy using a kinematic navigation system versus a conventional method: a 1-year retrospective, comparative study. Knee Surg Sports Traumatol Arthrosc. 2009;17(2):128–134. doi: 10.1007/s00167-008-0630-y. [DOI] [PubMed] [Google Scholar]
- 24.Cerciello S, Ollivier M, Corona K, et al. CAS and PSI increase coronal alignment accuracy and reduce outliers when compared to traditional technique of medial open wedge high tibial osteotomy: a meta-analysis. Knee Surg Sports Traumatol Arthrosc, 2020, 10. doi: 10.1007/s00167-020-06253-5.
- 25.Chaouche S, Jacquet C, Fabre-Aubrespy M, et al Patient-specific cutting guides for open-wedge high tibial osteotomy: safety and accuracy analysis of a hundred patients continuous cohort. Int Orthop. 2019;43(12):2757–2765. doi: 10.1007/s00264-019-04372-4. [DOI] [PubMed] [Google Scholar]
- 26.Fucentese SF, Meier P, Jud L, et al. Accuracy of 3D-planned patient specific instrumentation in high tibial open wedge valgisation osteotomy. J Exp Orthop, 2020, 7(1): 7. doi: 10.1186/s40634-020-00224-y.