

Abstract
Aim
Frontline nurses’ willingness to work has significant implications for maintaining workforce stability and quality of care during the COVID‐19 pandemic; however, few studies have investigated their willingness and the corresponding reasons. This study aims to examine frontline nurses’ willingness to work, identify its predictors and explore its corresponding reasons.
Design
A mixed‐methods design was conducted.
Methods
Based on a multilevel behavioural‐diagnostic model, a questionnaire survey was used to collect quantitative and qualitative data concurrently from 13 February to 24 February 2020 to explore frontline nurses’ willingness to work and the corresponding reasons in two hospitals in Wuhan, China. One was a designated hospital which only received COVID‐19 patients, and the other was built up temporarily for COVID‐19 patients.
Results
Of the 2014 participants, most (n = 1950, 96.8%) indicated their willingness to work, and a few (n = 64, 3.2%) expressed their unwillingness. Binary logistic regression analysis identified five predictors of participants’ willingness to work, including monthly family income, average working hours per shift, belief in their colleagues’ preparedness, belief in their hospitals’ preparedness and levels of depression. These indicators explained 27% of the variance (p < .05). Frontline nurses’ willingness to work mainly arose from professional commitment, patriotism and faith, while unwillingness to do so primarily stemmed from safety concerns and family responsibility.
Conclusion
Most frontline nurses were willing to work and showed great professional commitment.
Impact
Professional commitment and patriotism were two important individual‐level factors affecting frontline nurses’ willingness to work during a pandemic. Strategies should be implemented, such as appreciating and acknowledging their contribution, rewarding their valuable work, arranging reasonable working hours, enhancing colleagues’ and hospitals’ preparedness, and providing emotional support. Moreover, adequate personal protective equipment, self‐protection training and social support should be ensured to address frontline nurses’ safety concerns and family responsibility.
Keywords: COVID‐19, frontline nurses, mixed‐methods study, pandemic, willingness
1. INTRODUCTION
The coronavirus disease 2019 (COVID‐19) pandemic is posing unprecedented challenges to health systems internationally. When the COVID‐19 broke out and spread rapidly in Wuhan, Hubei province, China, the local healthcare system was also stressed and overwhelmed (Liu et al., 2020). It is estimated that approximately 3000 local healthcare workers (HCWs) were infected with COVID‐19 and 34 died (Department of Human Resources, 2020; Wu et al., 2020). More than 42,000 HCWs across China, including 28,600 nurses, went to Hubei to support epidemic control (China Global Television Network, 2020). Frontline nurses who come into direct contact with infected and suspected cases are exceptionally vulnerable and often left stricken with mental distress, such as burnout, anxiety and depression (Hu et al., 2020).
Nurses’ willingness, the voluntary and active intention to provide nursing care (Oh et al., 2017), has significant implications for maintaining workforce stability and quality of care at a time of elevated health needs (Fernandez et al., 2020). Furthermore, nurses’ willingness could mitigate their psychological problems, including burnout, anxiety and depression (Oh et al., 2017). Although many HCWs express their willingness to work under the risk of infection and death during this pandemic, some feel that their occupational risks are too high and even consider leaving the nursing profession (Jang et al., 2020). In Qatar, 88.1% of nurses indicated their willingness to work in a frontline role (Nashwan et al., 2021). In a recent Chinese study, 90.5% of nurses were willing to work in a frontline capacity (Luo et al., 2021). However, in South Korea, 12.3% of nurses expressed their unwillingness to work and 10.6% of nurses even thought about quitting their jobs during the outbreak of COVID‐19 (Jang et al., 2020).
2. BACKGROUND
Factors affecting nurses’ willingness to continue their responsibilities during the COVID‐19 pandemic might be complicated. According to the literature, the perception of self‐efficacy, occupational risks (Luo et al., 2021), work intensity and respiratory protection training (Li et al., 2020) were found to be associated with nurses’ willingness to work. On the contrary, safety concerns, family care and childcare obligations may hamper their willingness to work (Jang et al., 2020).
According to DeJoy's behavioural‐diagnostic model, frontline nurses’ willingness to perform patient care using universal precautions (i.e., personal protective equipment) is affected by individual‐level factors and organizational‐level factors (DeJoy, 1986; DeJoy et al., 2000). This productive example suggests a multilevel diagnostic lens for exploring factors influencing nurses’ willingness to work during a pandemic. Individual‐level factors might include sociodemographic data, health‐related and work‐related variables, the intentions/history for influenza vaccination, experience/intentions of respiratory protection, risk/fear perception and pandemic‐related variables. Organizational‐level factors might include safety evaluation of the work environment, organizational trust and shared values, training for taking care of patients with infectious diseases and the employer's pandemic preparedness (DeJoy, 1986; DeJoy et al., 2000). In addition, family‐level factors (including the need for childcare and lack of family support) were also found to be associated with nurses’ willingness to work (Luo et al., 2021). Thus, three‐level factors were involved in the conceptual framework to predict frontline nurses’ willingness to work in our study (Figure 1).
FIGURE 1.
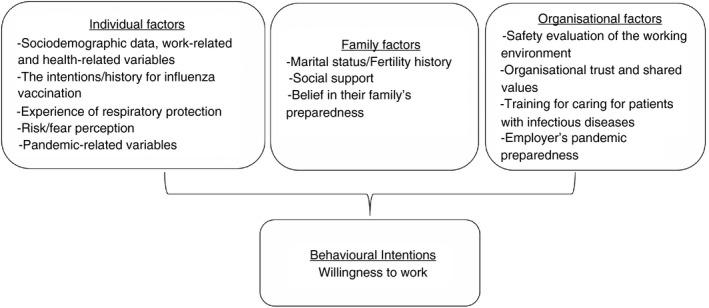
Conceptual framework of frontline nurses’ willingness to work‐adapted from DeJoy's behavioural diagnostic model (DeJoy, 1986; DeJoy et al., 2000)
Understanding multilevel factors affecting nurses’ willingness to work during the COVID‐19 pandemic may help to identify strategies to ensure that frontline nurses receive sufficient support to sustain the nursing workforce and continue to provide high‐quality patient care (Fernandez et al., 2020). To the best of our knowledge, few studies have investigated nurses’ willingness to work and its predictors during the COVID‐19 pandemic. Moreover, no prior qualitative study has been conducted to gain an in‐depth understanding of the reasons for Chinese nurses’ willingness to work. A mixed‐methods design would enable a multi‐level exploration as to whether and why frontline nurses are willing to work during the outbreak of COVID‐19 (Creswell & Creswell, 2017). Such evidence is crucial to inform future health responses; thus, this topic requires further investigation.
3. THE STUDY
3.1. Aim
The aims of this study were to examine frontline nurses’ willingness to work, compare the demographic data and health outcomes of nurses who expressed willingness or unwillingness, identify the predictors of their willingness and explore the corresponding reasons.
3.2. Design
This study used a mixed‐methods design. A questionnaire survey was used to collect quantitative and qualitative data concurrently to explore frontline nurses’ willingness to work and the corresponding reasons. An integration of both quantitative and qualitative empirical evidence would confirm and cross‐validate the findings of this study (Creswell & Creswell, 2017). A mixed‐methods approach is valuable to fully understand phenomena by capturing rich and in‐depth insights from participants (Weeks & Schaffert, 2019).
3.3. Setting and participants
The research population included frontline nurses working in Wuhan, China. A convenience sample was recruited for this study. Nurses were eligible if they participated in frontline work and were able to complete the online survey via a mobile phone. Nurses were excluded if they were infected with COVID‐19.
Nurses were recruited from two hospitals in Wuhan, China. One was a tertiary hospital with approximately 2000 nurses caring for COVID‐19 patients; the other was built up temporarily for COVID‐19 patients, and nearly 600 frontline nurses worked there.
3.4. Sample size
An online calculator named RaoSoft (http://www.raosoft.com/samplesize.html) assisted in the sample size calculation. The population size of 83,000 is set by the estimated total nurses originally working in Wuhan (n = 54,400) and those coming from other provinces (n = 28,600) to support Wuhan (Wuhan Municipal Health Commission, 2020). With a margin error of 5%, a confidence level of 95%, and a response rate of 50%, a total of 383 participants are needed in this survey.
3.5. Outcomes and measurements
The online questionnaire was administered in Chinese. Nurses’ willingness to work in the frontline was assessed using a choice question with a ‘yes’ or ‘no’ response frame, followed by an open‐ended question to elaborate the corresponding reasons.
Sociodemographic data were collected, including general data such as gender, age, marital status, fertility history, education, professional title, clinical experience (years), average working hours per shift and previous experience in taking care of patients with infectious diseases. Data on nurses’ confidence in taking care of COVID‐19 patients and self‐protection, safety evaluation of the working environment, and belief in their family, colleagues and hospitals’ preparedness to cope with COVID‐19 were also assessed using a five‐point Likert scale. The higher the score, the more confidence the nurses had.
The Chinese version of the Maslach Burnout Inventory: Human Services Survey (MBI‐HSS) for medical personnel (MP) was used to assess frontline nurses’ level of burnout (Maslach & Jackson, 1981). This scale consists of 22 items from three dimensions. They are emotional exhaustion (EE), depersonalisation (DP) and personal accomplishment (PA; Maslach & Jackson, 1981). All items are measured with a Likert‐scale from 0 (never) to 6 (every day). Higher scores in EE, higher scores in DP and lower scores in PA imply more severe burnout. Cronbach's α coefficient for the MBI‐HSS in this study was 0.86.
Frontline nurses’ anxiety and level of depression were assessed by the Chinese version of Zung's Self‐Rating Anxiety Scale (SAS; Zung, 1971) and Zung's Self‐Rating Depression Scale (SDS; Zung, 1965). The SAS and SDS all contain 20 items, which are measured using a Likert‐scale from 1 (never) to 4 (most of the time). In this study, Cronbach's α coefficients for SAS and SDS were 0.87 and 0.88, respectively.
Frontline nurses’ fear was assessed using the self‐developed Fear Scale for Healthcare Professionals (FS‐HPs; Hu et al., 2020). FS‐HPs consists of eight items, each of which is measured using a Likert scale from 1 (entirely disagree) to 5 (entirely agree). A group of ten experts evaluated the content validity, resulting in a total content validity index (CVI) of 1.0. In this study, Cronbach's α coefficient for FS‐HPs was 0.80.
Skin Lesion Scale (SLS) was a self‐developed scale and used to measure nurses’ skin lesions. This scale examines 11 common skin lesions caused by personal protective equipment (PPE; Sichuan Academy of Medical Sciences, 2020). If the respondents reported one type of skin lesion, a score of 1 is given to each ‘yes’ answer, resulting a total possible score range from 0 to11. A group of ten experts evaluated the content validity, resulting in a total CVI of 1.0. In this study, Cronbach's α coefficient for SLS was 0.73.
The Chinese version of the General Self‐efficacy Scale (GSS) was used to assess nurses’ self‐efficacy (Schwarzer & Jerusalem, 1995). GSS consists of 10 items, and each item is measured using a five‐point Likert scale. The total score ranges from 10 to 40. In this study, Cronbach's α coefficient for the GSS was 0.93.
The Chinese version of the Connor‐Davidson Resilience Scale‐10 (CD‐RISC‐10) was used to measure nurses’ resilience (Connor & Davidson, 2003). CD‐RISC‐10 consists of 10 items, and each item is measured using a five‐point Likert scale. The total score ranges from 0 to 40. In this study, Cronbach's α coefficient for the CD‐RISC‐10 was 0.96.
The Chinese version of the Multidimensional Scale of Perceived Social Support (MSPSS) was adopted to assess nurses’ social support (Zimet et al., 1988). MSPSS consists of 12 items, and each item is measured using a seven‐point Likert scale. The total score ranges from 0 to 40. In this study, Cronbach's α coefficient for the MSPSS was 0.96.
3.6. Data collection
A popular online survey platform in China named ‘Questionnaire Star’ was used. The survey link was distributed by head nurses to eligible nurses in the two study hospitals through the popular chat platform WeChat. Upon completion and submission of the online survey, each participant was recompensated with 50 Chinese Yuan ($8 USD) as an appreciation. Data were collected from 13 February to 24 February 2020. The COVID‐19 infection rate reached its peak in Wuhan on 13 February (World Health Organisation, 2021).
3.7. Ethical considerations
Ethics approval was obtained from the Institutional Review Board of the two participating hospitals and the last author's institution (Xiamen University). Participants’ anonymity and confidentiality were guaranteed. Frontline nurses needed to tick the ‘yes’ box to indicate their consent for participation before answering the survey. This study was registered in the Chinese Clinical Trial Registry (ChiCTR 2000030290).
3.8. Data analysis
3.8.1. Quantitative analysis
IBM SPSS (25.0) for Windows was used for quantitative data analysis (IBM Corp, 2017). An independent two‐sample t test, or Fisher's exact test, or chi‐square test was used to examine the differences in sociodemographic data, nurses’ confidence and beliefs, and health outcomes between the willing and unwilling groups. All variables were conditional backward entered into the binary logistic regression model to examine the predictors of participants’ willingness. Statistical significance was set at p < 0.05.
3.8.2. Qualitative analysis
Content analysis was adopted for the qualitative data gathered from the open‐ended question, which explored the main reasons for nurses’ willingness or unwillingness to work. Manifest content analysis was conducted in Chinese following Graneheim and Lundman’s (2004) steps to achieve trustworthiness. The first and last authors independently conducted initial coding. The transcripts were read repeatedly to gain a comprehensive understanding of the data. The differences and similarities of codes were compared and sorted into subcategories, the underlying meanings of which were grouped into categories. Coding discrepancies were discussed among the research team to reach a consensus. One expert in qualitative research examined the data analysis process. Finally, participants’ quotes were translated into English for reporting purposes, and the English translations were double‐checked by two bilingual authors (Chinese and English). Summative content analysis was also performed to evaluate the frequency of statements in each identified category.
4. RESULTS/FINDINGS
4.1. Quantitative results
4.1.1. Sociodemographic data between participants who expressed willingness or unwillingness to work
Eligible nurses (n = 2600) were approached, and 2101 completed the survey. The response rate was 80.8% (82.2% and 76.0% for the two hospitals, respectively). A preliminary review of the survey was undertaken by assessing how long the nurses had been working in a frontline role during the COVID‐19 pandemic and the variation in answers. The 68 nurses who had not begun their frontline duties by reporting zero days working in the frontline and the 19 who ticked the same answers on all items were excluded. Finally, 2014 participants were included in the analysis. The mean age of participants was 30.99 (SD = 6.17) years, and the majority were female (n = 1754, 87.1%) and had children (n = 1100, 54.6%).
Of the total number of nurses, 1950 (96.8%) expressed their willingness to work, while 64 (3.2%) indicated their unwillingness. The sociodemographic data of the two groups are summarised in Table 1. Participants with a lower monthly family income, whose original workplace was outside Wuhan, and who had had previous training in taking care of patients with infectious diseases were more willing to care for COVID‐19 patients (p < .05).
TABLE 1.
Sociodemographic data of participants who expressed willingness or unwillingness to work (n = 2014)
| Sociodemographic characteristics | Willingness to work (n = 1950, 96.8%) | Unwillingness to work (n = 64, 3.2%) | Willingness proportione | t/χ2 | p | ||
|---|---|---|---|---|---|---|---|
| n (%) | M (SD) | n (%) | M (SD) | (%) | |||
| Gendera | |||||||
| Male | 250 (12.4%) | 10 (0.5%) | 96.2% | 0.433 | 0.510 | ||
| Female | 1700 (84.4%) | 54 (2.7%) | 96.9% | ||||
| Age (years)b | 30.99 (6.15) | 31.05 (6.73) | −0.071 | 0.943 | |||
| Marital statusa | |||||||
| Married | 1187 (58.9%) | 43 (2.1%) | 96.5% | 1.040 | 0.308 | ||
| Other marital statusd | 763 (37.9%) | 21 (1.0%) | 97.3% | ||||
| Fertility historya | |||||||
| At least one child | 1061 (52.7%) | 39 (1.9%) | 96.5% | 1.065 | 0.302 | ||
| No children | 889 (44.1%) | 25 (1.2%) | 97.3% | ||||
| Monthly family income (USD/month)a | |||||||
| ≤1440 | 1082 (53.7%) | 27 (1.3%) | 97.6% | 4.430 | 0.035* | ||
| >1440 | 868 (43.1%) | 37 (1.8%) | 95.9% | ||||
| Educationa | |||||||
| Diploma or lower | 427 (21.2%) | 14 (0.7%) | 96.8% | 0.000 | 0.997 | ||
| Bachelor's degree or higher | 1523 (75.6%) | 50 (2.5%) | 96.8% | ||||
| Professional titlea | |||||||
| Junior | 1445 (71.7%) | 50 (2.5%) | 96.7% | 0.524 | 0.469 | ||
| Intermediate and senior | 505 (25.1%) | 14 (0.7%) | 97.3% | ||||
| Clinical experience after graduation (years)b | 8.99 (6.52) | 8.55 (5.98) | 0.533 | 0.594 | |||
| Frontline working duration during the COVID‐19 outbreak (days)b | 20.76 (12.98) | 19.80 (11.84) | 0.585 | 0.558 | |||
| Average working hours per shiftb | 6.55 (1.90) | 7.00 (1.69) | −1.855 | 0.064 | |||
| Originally worked in Wuhana | |||||||
| Yes | 1268 (63.0%) | 56 (2.9%) | 95.8% | 13.897 | <0.001** | ||
| No | 682 (33.8%) | 8 (0.4%) | 98.8% | ||||
| Position in the original hospitalc | |||||||
| Bedside nurse | 1757 (87.2%) | 61 (3.0%) | 96.6% | 0.201 | |||
| Nurse manager | 193 (9.6%) | 3 (0.1%) | 98.5% | ||||
| Position in the Wuhan hospitalc | |||||||
| Bedside nurse | 1833 (91%) | 61 (3.0%) | 96.8% | 0.866 | |||
| Nurse manager | 117 (5.8%) | 3 (0.1%) | 97.5% | ||||
| Care specialization changeda | |||||||
| Yes | 725 (36.0%) | 22 (1.1%) | 97.1% | 0.209 | 0.648 | ||
| No | 1225 (60.8%) | 42 (2.1%) | 96.7% | ||||
| Previous training in taking care of people with infectious diseasesa | |||||||
| Yes | 1608 (79.8%) | 46 (2.3%) | 97.2% | 4.731 | 0.030* | ||
| No | 342 (17.0%) | 18 (0.9%) | 95.0% | ||||
| Previous experience in taking care of patients with infectious diseasesa | |||||||
| Yes | 767 (38.1%) | 18 (0.9%) | 97.7% | 3.273 | 0.070 | ||
| No | 1183 (58.7%) | 46 (2.3%) | 96.3% | ||||
Chi‐square test with χ 2 value presented.
Independent two‐sample t test with p values presented.
Fisher's exact test.
Other marital status: including single, divorced and separated.
Willingness proportion = the number willing/(number of willing + unwilling).
p < 0.05
p < 0.01.
4.1.2. Comparison of confidence and belief levels between participants who expressed willingness or unwillingness to work
Table 2 shows the differences in confidence and belief levels between the two groups. Compared with unwilling nurses, nurses who were willing to work reported a higher level of confidence in taking care of COVID‐19 patients (p < 0.001) and self‐protection (p < 0.001), as well as a better safety evaluation of the work environment (p < 0.001). Moreover, nurses who were willing to work indicated a significantly higher belief in their families’, colleagues’ and hospitals’ preparedness to cope with COVID‐19 (p < 0.001).
TABLE 2.
Comparison of confidence and belief levels between participants who expressed willingness or unwillingness to work (n = 2014)
| Willingness to work M (SD) (n = 1950, 96.8%) | Unwillingness to work M (SD) (n = 64, 3.2%) | t | p | |||
|---|---|---|---|---|---|---|
| M (SD) | Actual range | M (SD) | Actual range | |||
| Confidence in taking care of COVID‐19 patientsa | 3.78 (0.97) | 1–5 | 2.98 (1.09) | 1–5 | 6.461 | <0.001 |
| Confidence in self‐protectiona | 3.67 (0.93) | 1–5 | 2.80 (1.00) | 1–5 | 7.389 | <0.001 |
| Safety evaluation of the working environmentb | 3.52 (0.97) | 1–5 | 2.70 (1.02) | 1–5 | 6.625 | <0.001 |
| Belief in their families’ preparedness to cope with COVID‐19c | 3.80 (0.87) | 1–5 | 3.08 (1.04) | 1–5 | 5.487 | <0.001 |
| Belief in their colleagues’ preparedness to cope with COVID‐19c | 4.01 (0.75) | 1–5 | 3.02 (1.11) | 1–5 | 7.115 | <0.001 |
| Belief in their hospitals’ preparedness to cope with COVID‐19c | 4.09 (0.77) | 1–5 | 3.02 (1.05) | 1–5 | 8.136 | <0.001 |
Independent two‐sample t tests with t values presented. Statistical significance was set at p < 0.05.
Measured by a five‐point scale including ‘1 = Extremely unconfident’, ‘2 = Unconfident’, ‘3 = Somewhat confident’, ‘4 = Confident’, and ‘5 = Very confident’.
Measured by a five‐point scale including ‘1 = Extremely unsafe’, ‘2 = Unsafe’, ‘3 = Somewhat safe’, ‘4 = Safe’, and ‘5 = Extremely safe’.
Measured by a five‐point scale including ‘1 = Extremely disbelieve’, ‘2 = Disbelieve’, ‘3 = Somewhat believe’, ‘4 = Believe’, and ‘5 = Extremely believe’.
4.1.3. Comparison of health outcomes between participants who expressed willingness or unwillingness to work
Compared with unwilling nurses, nurses who were willing to work experienced less burnout (p < 0.001), less anxiety (p < 0.001), less depression (p < 0.001), less fear (p < 0.05) and fewer skin lesions (p < 0.05). Furthermore, nurses who were willing to work reported significantly higher levels of self‐efficacy (p < 0.001), resilience (p < 0.001) and social support (p < 0.001; Table 3).
TABLE 3.
Comparison of health outcomes between participants who expressed willingness or unwillingness to work (n = 2014)
| Health variables |
Willingness to work (n = 1950, 96.8%) |
Unwillingness to work(n = 64, 3.2%) |
t | p | ||
|---|---|---|---|---|---|---|
| M (SD) | Actual range | M (SD) | Actual range | |||
| Burnout (MBI‐HSS)a: emotional exhaustion | 23.05 (13.57) | 0–54 | 35.31 (15.43) | 0–54 | −6.279 | <0.001** |
| Burnout (MBI‐HSS)a: depersonalization | 6.62 (6.99) | 0–30 | 11.25 (7.67) | 0–30 | −5.200 | <0.001** |
| Burnout (MBI‐HSS)a: personal accomplishment | 35.01 (9.88) | 0–48 | 29.25 (10.54) | 1–48 | 4.579 | <0.001** |
| Anxiety (SAS)b | 47.43 (10.97) | 25–90 | 59.13 (12.29) | 35–83 | −8.364 | <0.001** |
| Depression (SDS)c | 50.14 (11.19) | 25–96 | 61.31 (9.44) | 35–85 | −9.256 | <0.001** |
| Fear (FS‐HPs)d | 30.31 (7.55) | 8–40 | 33.27 (8.53) | 8–40 | −3.065 | 0.002* |
| Skin lesion (SLS)e | 3.88 (2.25) | 0–11 | 5.06 (3.17) | 0–11 | −2.973 | 0.004* |
| Self‐efficacy (GSS)f | 26.96 (5.81) | 10–40 | 23.92 (6.57) | 10–40 | 4.105 | <0.001** |
| Resilience (CD‐RISC‐10)g | 26.34 (7.21) | 0–40 | 20.02 (8.32) | 0–32 | 6.873 | <0.001** |
| Social support (MSPSS)h | 5.50 (1.04) | 1–7 | 4.64 (1.13) | 1–7 | 6.496 | <0.001** |
MBI‐HSS: Maslach Burnout Inventory: Human Services Survey (possible range: 0 to 54).
SAS: Zung's Self‐Rating Anxiety Scale (possible range: 25 to 100).
SDS: Zung's Self‐Rating Depression Scale (possible range: 25 to 100).
FS‐HPs: Fear Scale for Healthcare Professionals (possible range: 8 to 40).
SLS: Skin Lesion Scale (possible range: 0 to 11).
GSS: General Self‐efficacy Scale (possible range: 10 to 40).
CD‐RISC‐10: Connor‐Davidson Resilience Scale‐10 (possible range: 0 to 40).
MSPSS: Multidimensional Scale of Perceived Social Support (possible range: 1 to 7).
Independent two‐sample t test with t values presented.
p < 0.05
p < 0.01.
4.1.4. Predictors of nurse participants’ willingness to work
Table 4 presents the predictors of participants’ willingness to work. Seven variables were included in the equation. Except for clinical experience and social support, five variables were identified that predicted 27.0% of participants’ willingness: monthly family income, average working hours per shift, belief in their colleagues’ preparedness to cope with COVID‐19, belief in their hospitals’ preparedness and levels of depression (p < 0.05).
TABLE 4.
Predictors of nurse participants’ willingness to work
| B | Std. error | Wald | p | Exp (B) | 95% Confidence interval | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Monthly family income (USD/month)a | −0.819 | 0.296 | 7.637 | .006* | 0.441 | 0.247 | 0.788 |
| Clinical experience after graduation (years) | 0.043 | 0.025 | 2.834 | .092 | 1.044 | 0.993 | 1.097 |
| Average working hours per shift | −0.166 | 0.079 | 4.462 | .035* | 0.847 | 0.726 | 0.988 |
| Belief in their colleagues’ preparedness to cope with COVID‐19b | 0.576 | 0.219 | 6.891 | .009* | 1.779 | 1.157 | 2.735 |
| Belief in their hospitals’ preparedness to cope with COVID‐19b | 0.493 | 0.208 | 5.609 | .018* | 1.637 | 1.089 | 2.461 |
| Depression (SDS)c | −0.073 | 0.016 | 20.266 | <.001** | 0.930 | 0.900 | 0.960 |
| Social support (MSPSS)d | 0.240 | 0.128 | 3.529 | .060 | 1.271 | 0.990 | 1.632 |
Overall R 2 = 0.270. B = beta coefficient.
In the binary logistic regression model, 0 = unwilling to care for COVID‐19 patients and 1 = willing to care for COVID‐19 patients.
Monthly family income (USD/month): 0 ≤ 1440, 1 > 1440.
Measured by a five‐point scale including ‘1 = Extremely disbelieve’, ‘2 = Disbelieve’, ‘3 = Somewhat believe’, ‘4 = Believe’, and ‘5 = Extremely believe’.
SDS: Zung's Self‐Rating Depression Scale.
MSPSS: Multidimensional Scale of Perceived Social Support. Statistically significant at p < 0.05.
p < 0.05.
p < 0.01.
4.2. Qualitative findings
4.2.1. Willingness to work
Five categories emerged from the content analysis of the willing group: (1) commitment to the nursing profession (n = 1465, 72.7%); (2) patriotism and faith (n = 301, 14.9%); (3) organizational commitment (59, 2.9%); (4) previous working experience in taking care of patients with infectious diseases (n = 18, 0.9%); and (5) tangible benefits (n = 17, 0.8%; Table 5). Seventy participants (3.5%) gave a variety of reasons for their willingness, and 20 participants (1.0%) did not give their reasons for being willing to work.
TABLE 5.
Reasons for nurse participants’ willingness or unwillingness to work
| Willingness to work (n = 1860) | Unwillingness to work (n = 52) |
|---|---|
|
Commitment to the nursing profession (n = 1465)
|
Safety concerns (n = 33) |
|
Patriotism and faith (n = 301)
|
Participants’ need to care for their families (n = 14) |
| Organizational commitment (59) | Participants’ own physical health (n = 5) |
| Previous working experience in taking care of patients with infectious diseases (n = 18) | |
| Tangible benefits (n = 17) |
4.2.1.1. Category 1: Commitment to the nursing profession
A total of 1465 participants expressed their willingness to work because of their commitment to the nursing profession, including the responsibility of the nursing profession (n = 1402) and self‐fulfilment (n = 63).
4.2.1.1.1. Subcategory 1: Responsibilities of the nursing profession
A total of 1402 participants stated that taking care of patients was nurses’ responsibility and commitment. They believed that nurses should care for COVID‐19 patients regardless of what happened.
‘It is the nurses’ responsibility to care for patients. Although we do not know what will happen tomorrow, we need to commit ourselves to take care of COVID‐19 patients. They need us. We can use what we have learned to help patients.
4.2.1.1.2. Subcategory 2: Self‐fulfilment
Sixty‐three participants were expected to achieve self‐fulfilment when working in the frontline. They thought that taking care of COVID‐19 patients was a good opportunity for achievement.
I wish to do something meaningful in my career. I think working at the frontline is a precious experience for me. The frontline work helps me realise my value of being a nurse. Also, my nursing career will embed something memorable and meaningful.
4.2.1.2. Category 2: Patriotism and faith
There were 301 participants who expressed patriotism and faith as reasons for taking care of COVID‐19 patients, including love for the country and the people (n = 231) and belief in the ability to triumph over adversity (n = 70).
4.2.1.2.1. Subcategory 1: Love for the country and the people
A total of 231 participants expressed their love for the country and the people. When they volunteered to care for COVID‐19 patients, they prioritized national benefits.
I have deep love for my country and the people. When the country is in trouble, every person should do something for his country.
4.2.1.2.2. Subcategory 2: Belief in the ability to triumph over adversity
A total of seventy participants expressed their belief that they would finally win the battle against COVID‐19. They believed that the unity and cooperation among the government, hospitals, HCWs, and community would help conquer COVID‐19.
I still remember the outbreak of SARS in 2003. At that time, people from across the country worked together to defeat the epidemic. We should stand shoulder to shoulder to fight this outbreak of COVID‐19, we will eventually win.
4.2.1.3. Category 3: Organizational commitment
A total of 59 participants expressed loyalty to their organization and would respond to the calls from their organizations.
I responded to the call from our organisation and came to the frontline.
4.2.1.4. Category 4: Previous working experience in taking care of people with infectious diseases
A total of 18 participants indicated that previous working experience helped them take care of COVID‐19 patients. Seven of them had working experience in taking care of severe acute respiratory syndrome (SARS) patients, and two nurses worked in the frontline during the Ebola epidemic in Africa in 2015.
I took care of SARS patients in 2003. I think I can use my previous experience to help more patients.
4.2.1.5. Category 5: Tangible benefits
A total of seventeen participants were motivated by tangible benefits—extra bonus or getting a promotion.
I just bought a house, so I need to earn money and pay the mortgage every month.
4.2.2. Unwillingness to work
Three categories emerged from the qualitative data of nurses who were unwilling to work: (1) safety concerns (n = 33, 1.8%); (2) the need to care for their families (n = 14, 0.8%); and (3) their own physical health (n = 5, 0.2%). Six participants (0.3%) gave other reasons for their unwillingness, and six participants (0.3%) did not give reasons.
4.2.2.1. Category 1: Safety concerns
Thirty‐three participants expressed safety concerns. As the incidence of COVID‐19 continued to rise in February 2020, they were afraid of being infected.
The working environment in the isolation ward is insecure. The virus was so strong that I was scared of being infected. I have no confidence in self‐protection.
4.2.2.2. Category 2: Participants’ need to care for their families
Fourteen participants indicated that they needed to care for their families; thus, they could not undergo quarantine after work.
Because I work as a frontline nurse, as required, I cannot go home and should stay in a designated hotel for sleeping. My child is still young, and my parents are getting old. I cannot leave them alone.
4.2.2.3. Category 3: Participants’ own physical health
Five participants were unwilling to work in the frontline because of their own physical health. One participant had severe hormonal dermatitis on the face and upper limb, while the others had chronic diseases.
5. DISCUSSION
Our study explored frontline nurses’ willingness to work in Wuhan, China, during the COVID‐19 pandemic. The large sample size and the use of a mixed‐methods approach contributed to a deeper insight into whether and why frontline nurses would fulfil their roles and responsibilities during this crisis. A conceptual framework comprising individual, family and organizational factors was used to interpret and organize the findings.
In our study, most frontline nurses (1950, 96.8%) indicated their willingness to work. Similar to our study, another study reported that 83.4% of the nurses from three provinces expressed that they were willing to work in Hubei during the outbreak of COVID‐19 (Gan et al., 2020). The higher willingness in our study may be explained by the composition of our participants. The majority of our participants in our study (n = 1324) originally worked in Wuhan, and their relatives or colleagues might have been infected with COVID‐19. The witness of their loved ones’ suffering might trigger their motivation to fight COVID‐19. Moreover, the rest of our participants (n = 690) had already expressed their willingness before they were sent to support the epidemic control from other provinces.
5.1. Factors affecting frontline nurses’ willingness to work
This study found individual, family, and organisational factors which might influence frontline nurses’ willingness to work during the COVID‐19 pandemic. The quantitative data suggested that the individual predictors of frontline nurses’ willingness included average working hours per shift and levels of depression. The family predictor was the monthly family income. Organizational predictors involved belief in their colleagues’ and hospitals’ preparedness to cope with COVID‐19. Moreover, the qualitative data provided an in‐depth understanding of the factors which complemented the quantitative findings. There were individual factors (including commitment to the nursing profession, patriotism and faith, previous working experience, safety concerns and participants’ own physical health), family factors (participants’ need to care for their families) and organizational factors (organizational commitment).
5.1.1. Individual factors
In our study, frontline nurses’ high willingness mainly arose from their commitment to the nursing profession. Professional commitment is the consistency between personal beliefs and professional goals with greater consistency, indicating higher individual efforts (Teng et al., 2007). Our qualitative findings identified two perspectives of commitment to the nursing profession, including the responsibility of the nursing profession and self‐fulfilment. Perceived responsibility to work is the nature and meaning of nurses’ roles (Damery et al., 2010). Although frontline nurses put their lives at risk when caring for COVID‐19 patients, they remain in the nursing profession because of their sense of responsibility (Liu et al., 2020). Furthermore, appreciation from patients and the society might help them realize their professional values and achieve their self‐fulfilment (Sheng et al., 2020). To build nurses’ professional commitment, nurse educators should make a conscious effort to model and teach responsibility and loyalty to the nursing profession (Gambino, 2010). Moreover, when nurses express low professional commitment, nursing managers should convey appreciation from patients and their families to inspire nurses’ commitment and encourage them to continue their roles and responsibilities (Chang et al., 2019).
Patriotism and faith were other reasons indicated by frontline nurses for their willingness to work. Our qualitative data showed that patriotism and faith involve love for the country and the people and belief in the ability to triumph over adversity. Patriotism was found to be the most motivating factor for healthcare students in Saudi Arabia to volunteer during the COVID‐19 pandemic (AlOmar et al., 2021). Another study also reported that patriotism had a positive effect on nurses’ willingness to work during a national emergency in Israel (Kagan et al., 2017). Chinese people believe in a value that ‘When the country is in trouble, every person should do something for his country’. Furthermore, being sustained by their belief in the ability to triumph over adversity, nurses were more confident and willing to engage in frontline work during the COVID‐19 pandemic. Frontline nurses’ patriotism and faith in our study may be promoted by support from the Chinese government and society. Adequate provision of medical protective supplies and medicines brought frontline nurses a sense of safety (Liu et al., 2020). The widespread acknowledgement of nurses’ contribution to epidemic control from social media might give frontline nurses a sense of pride and social recognition (Gan et al., 2020). In turn, frontline nurses demonstrated love and confidence in their country and expressed their willingness to work for their country.
This study found that the average working hours per shift predicted nurses’ willingness to work. Specifically, the average working hours per shift in the group willing to work was 6.55, while in the group unwilling to work it was 7.00. The National Health Commission (NHC) of China recommends four hours per shift for frontline nurses in intensive care units during the COVID‐19 pandemic (National Health Commission of P. R. China, 2020; Zhang et al., 2021). However, nurses had to extend their working hours due to a shortage of staff during the COVID‐19 pandemic. Furthermore, prolonged wearing of PPE causes sweating and dehydration, which can lead to severe dyspnoea and distress among nurses (Liu et al., 2020). Therefore, working hours per shift should be set reasonably to support frontline nurses (Adams & Walls, 2020).
Our results found that the levels of depression were a predictor of participants’ willingness to work. HCWs who come into direct contact with confirmed cases often feel scared, and the challenges and stress they experience can trigger depression (Bao et al., 2020). A recent study by Kang et al. (2020) reported that medical workers in China battling with COVID‐19 were additionally plagued with depression, which is in line with another study reporting a depression prevalence of 27.5% among those who worked in the SARS units (Su et al., 2007). To sustain nurses’ willingness, emotional competencies training would be beneficial for decreasing depression in such an emergency situation (Manzano García & Ayala Calvo, 2021).
Previous working experience in taking care of patients with infectious diseases influenced nurses’ willingness to work (Li et al., 2020). Previous experience may enhance nurses’ competency in self‐protection and coping strategies to deal with psychological distress (Fernandez et al., 2020). In our study, only 785 out of the 2014 nurses had such previous experience in taking care of patients with infectious diseases. Continuous medical education and COVID‐19 training plans should be offered to those who have no such experience to improve their competency (Labrague & de Los Santos, 2020).
Participants’ unwillingness to work primarily comes from safety concerns. Personal safety was the most cited concern among frontline nurses while working during a respiratory pandemic (Fernandez et al., 2020). Therefore, self‐protection training would be beneficial for enhancing nurses’ sense of safety (Raven et al., 2018). In our study, frontline nurses’ concern for their physical health safety and the adequacy of protection from infection was found to be one of the reasons for their unwillingness to work. Therefore, nursing managers should consider nurses’ physical health conditions and their workload when delegating nurses to work in the frontline.
5.1.2. Family factors
In our study, monthly family income was a predictor of participants’ willingness to work. Nurses with lower monthly family incomes were more willing to care for COVID‐19 patients. Supported by our qualitative data, we also found that tangible benefits were one of the reasons influencing frontline nurses’ willingness to work. Compensation could be beneficial for maintaining a sufficient healthcare workforce during the COVID‐19 pandemic (Jang et al., 2020).
Consistent with other studies, during the COVID‐19 pandemic, frontline nurses also indicated that the need for family care was another reason for their unwillingness to work (Gan et al., 2020). Appropriate social support would be beneficial for relieving frontline nurses’ concerns about family responsibility (Raven et al., 2018). For example, the local community may provide help to frontline nurses’ families in need to address their family responsibilities (Mo et al., 2020).
5.1.3. Organizational factors
In our study, frontline nurses’ beliefs in their colleagues’ preparedness to cope with COVID‐19 predicted their willingness to work. Colleagues’ preparedness includes core abilities and knowledge regarding an effective response to disasters to meet the needs of patients (Baack & Alfred, 2013). Disaster preparedness training would be beneficial for enhancing nurses’ specific knowledge of COVID‐19 and increasing their self‐confidence (Sultan et al., 2020). Moreover, education on safety practices is essential to promote their skill management (Shi et al., 2020).
In addition, hospital preparedness predicted nurses’ willingness to work. Hospital preparedness for a pandemic involves the ability to develop efficient patient triage strategies, accommodate the increasing number of patients, support HCWs with adequate PPE and establish protocols for the rational use of medical resources (Griffin et al., 2020). Hospital preparedness is important to protect frontline nurses and maintain their morale and well‐being (Chopra et al., 2020). With better hospital preparedness, frontline nurses will feel motivated and more willing to engage in health responses to emergency crises.
Our qualitative study showed that organizational commitment was another reason for willingness to work. Nurses’ loyalty reflects their emotional attachment and sense of belonging to their organization (Kagan et al., 2017). Higher organizational commitment indicates stronger teamwork relationships and a higher willingness to work in national emergencies (Kagan et al., 2017).
5.2. Limitations
Limitations exist in this study. Convenience sampling was adopted for data collection in Wuhan, which may limit the representativeness of other nurses in other provinces or other countries. Nurses might provide a socially desirable response due to expectations and praise from both their organization and society during the COVID‐19 pandemic. The cross‐sectional design could not provide longitudinal data. Future cohort studies could be carried out to evaluate the willingness to work trends across different time points during the pandemic. Our qualitative data were collected using an open‐ended question. Face‐to‐face semi‐structured interviews would be beneficial to gain deeper insight into nurses’ willingness to work.
6. CONCLUSION
Our study discusses frontline nurses’ willingness to work during the COVID‐19 pandemic in Wuhan and its associated predictors, as well as the corresponding reasons. In this study, we found that professional commitment and patriotism were two important individual‐level factors affecting frontline nurses’ willingness to work during a pandemic. Strategies should be implemented, such as appreciating and acknowledging their contribution, rewarding their valuable work, arranging reasonable working hours, enhancing colleagues’ and hospitals’ preparedness, and providing emotional support. Moreover, adequate PPE, self‐protection training and social support should be ensured to address frontline nurses’ safety concerns and family responsibilities.
CONFLICT OF INTEREST
No conflict of interest has been declared by the authors.
AUTHOR CONTRIBUTIONS
JZ, SC, QS and WL designed the study and obtained the grants. QK and YK collected data. QK, JF and WL analysed and interpreted data, QK, YK and QS searched literature, JZ, QK and SC interpreted the results and wrote the manuscript.
PEER REVIEW
The peer review history for this article is available at https://publons.com/publon/10.1111/jan.14989.
ACKNOWLEDGEMENT
We acknowledge the departments of nursing in the two participating hospitals and all participating nurses for their support.
Ke, Q., Chan, S. W.‐C., Kong, Y., Fu, J., Li, W., Shen, Q., & Zhu, J. (2021). Frontline nurses’ willingness to work during the COVID‐19 pandemic: A mixed‐methods study. Journal of Advanced Nursing, 77, 3880–3893. 10.1111/jan.14989
Clinical trial registration number: ChiCTR2000030290
Funding information
This study was supported by Xiamen University COVID‐19 Emergency Response Grant (20720200025) and National Natural Science Foundation of China (71974162).
Contributor Information
Qu Shen, Email: shenqumail@163.com.
Jiemin Zhu, Email: Jieminzhu@xmu.edu.cn.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Adams, J. G., & Walls, R. M. (2020). Supporting the health care workforce during the COVID‐19 global epidemic. JAMA, 323(15), 1439–1440. 10.1001/jama.2020.3972 [DOI] [PubMed] [Google Scholar]
- AlOmar, R. S., AlShamlan, N. A., AlAmer, N. A., Aldulijan, F., AlMuhaidib, S., Almukhadhib, O., Algarni, S. A., Alshaibani, A., Darwish, M., & Al Shammari, M. (2021). What are the barriers and facilitators of volunteering among healthcare students during the COVID‐19 pandemic? A Saudi‐based cross‐sectional study. British Medical Journal Open, 11(2), e042910. 10.1136/bmjopen-2020-042910 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baack, S., & Alfred, D. (2013). Nurses’ preparedness and perceived competence in managing disasters. Journal of Nursing Scholarship, 45(3), 281–287. 10.1111/jnu.12029 [DOI] [PubMed] [Google Scholar]
- Bao, Y., Sun, Y., Meng, S., Shi, J., & Lu, L. (2020). 2019‐nCoV epidemic: Address mental health care to empower society. Lancet, 395(10224), e37–e38. 10.1016/s0140-6736(20)30309-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chang, H. Y., Lee, I. C., Chu, T. L., Liu, Y. C., Liao, Y. N., & Teng, C. I. (2019). The role of professional commitment in improving nurses’ professional capabilities and reducing their intention to leave: Two‐wave surveys. Journal of Advanced Nursing, 75(9), 1889–1901. 10.1111/jan.13969 [DOI] [PubMed] [Google Scholar]
- China Global Television Network . (2020). COVID‐19 frontline: Chinese nurses share COVID‐19 working experience. https://news.cgtn.com/news/2020‐04‐23/COVID‐19‐Frontline‐Chinese‐nurses‐share‐COVID‐19‐working‐experience–PVhwPtdANa/index.html
- Chopra, V., Toner, E., Waldhorn, R., & Washer, L. (2020). How should U.S. hospitals prepare for coronavirus disease 2019 (COVID‐19)? Annals of Internal Medicine, 172(9), 621–622. 10.7326/m20-0907 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Connor, K. M., & Davidson, J. R. (2003). Development of a new resilience scale: The Connor‐Davidson resilience scale (CD‐RISC). Depression and Anxiety, 18(2), 76–82. 10.1002/da.10113 [DOI] [PubMed] [Google Scholar]
- Creswell, J. W., & Creswell, J. D. (2017). Research design: Qualitative, quantitative, and mixed methods approaches (5th edn.). SAGE Publications. [Google Scholar]
- Damery, S., Draper, H., Wilson, S., Greenfield, S., Ives, J., Parry, J., Petts, J., & Sorell, T. (2010). Healthcare workers’ perceptions of the duty to work during an influenza pandemic. Journal of MedicalEethics, 36(1), 12–18. 10.1136/jme.2009.032821 [DOI] [PubMed] [Google Scholar]
- DeJoy, D. M. (1986). A behavioral‐diagnostic model for self‐protective behavior in the workplace. Prof Saf., 31, 26–30. [Google Scholar]
- DeJoy, D. M., Searcy, C. A., Murphy, L. R., & Gershon, R. R. (2000). Behavioral‐diagnostic analysis of compliance with universal precautions among nurses. Journal of Occupational Health Psychology, 5(1), 127–141. 10.1037//1076-8998.5.1.127 [DOI] [PubMed] [Google Scholar]
- Department of Human Resources . (2020). Decision to commend the advanced collectives and individuals in the prevention and control of new pneumonia epidemic in the national health system [N] national health commission, PRC. http://www.nhc.gov.cn/renshi/s7771/202003/28cc60d7e33b4dc7bd77af485fab1a58.shtml
- Fernandez, R., Lord, H., Halcomb, E., Moxham, L., Middleton, R., Alananzeh, I., & Ellwood, L. (2020). Implications for COVID‐19: A systematic review of nurses’ experiences of working in acute care hospital settings during a respiratory pandemic. International Journal of Nursing Studies, 111, 103637. 10.1016/j.ijnurstu.2020.103637 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gambino, K. M. (2010). Motivation for entry, occupational commitment and intent to remain: A survey regarding Registered Nurse retention. Journal of Advanced Nursing, 66(11), 2532–2541. 10.1111/j.1365-2648.2010.05426.x [DOI] [PubMed] [Google Scholar]
- Gan, X., Shi, Z., Chair, S. Y., Cao, X., & Wang, Q. (2020). Willingness of Chinese nurses to practice in Hubei combating the coronavirus disease 2019 epidemic: A cross‐sectional study. Journal of Advanced Nursing, 76(8), 2137–2150. 10.1111/jan.14434 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today, 24(2), 105–112. 10.1016/j.nedt.2003.10.001 [DOI] [PubMed] [Google Scholar]
- Griffin, K. M., Karas, M. G., Ivascu, N. S., & Lief, L. (2020). Hospital preparedness for COVID‐19: A practical guide from a critical care perspective. American Journal of Respiratory and Critical Care Medicine, 201(11), 1337–1344. 10.1164/rccm.202004-1037CP [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu, D., Kong, Y., Li, W., Han, Q., Zhang, X., Zhu, L. X., Wan, S. W., Liu, Z., Shen, Q., Yang, J., He, H. G., & Zhu, J. (2020). Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID‐19 outbreak in Wuhan, China: A large‐scale cross‐sectional study. EClinicalMedicine, 24, 100424. 10.1016/j.eclinm.2020.100424 [DOI] [PMC free article] [PubMed] [Google Scholar]
- IBM Corp . (2017). IBM SPSS statistics for windows, 25.0 ed.
- Jang, Y., You, M., Lee, S., & Lee, W. (2020). Factors associated with the work intention of hospital workers’ in South Korea during the early stages of the COVID‐19 outbreak. Disaster Medicine and Public Health Preparedness, 1–8. 10.1017/dmp.2020.221 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kagan, I., Itzhaki, M., & Melnikov, S. (2017). Patriotism, organizational commitment and nurses’ intention to report for work in emergencies. International Nursing Review, 64(4), 468–475. 10.1111/inr.12395 [DOI] [PubMed] [Google Scholar]
- Kang, L., Li, Y., Hu, S., Chen, M., Yang, C., Yang, B. X., Wang, Y., Hu, J., Lai, J., Ma, X., Chen, J., Guan, L., Wang, G., Ma, H., & Liu, Z. (2020). The mental health of medical workers in Wuhan, China, dealing with the 2019 novel coronavirus. The Lancet Psychiatry, 7(3), e14. 10.1016/S2215-0366(20)30047-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- Labrague, L. J., & de Los Santos, J. (2020). Fear of COVID‐19, psychological distress, work satisfaction and turnover intention among frontline nurses. Journal of Nursing Management, 29(3), 395–403. 10.1111/jonm.13168 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li, J., Li, P., Chen, J., Ruan, L., Zeng, Q., & Gong, Y. (2020). Intention to response, emergency preparedness and intention to leave among nurses during COVID‐19. Nursing Open, 7(6), 1867–1875. 10.1002/nop2.576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu, Q., Luo, D., Haase, J. E., Guo, Q., Wang, X. Q., Liu, S., Xia, L., Liu, Z., Yang, J., & Yang, B. X. (2020). The experiences of health‐care providers during the COVID‐19 crisis in China: A qualitative study. Lancet Global Health, 8(6), e790–e798. 10.1016/s2214-109x(20)30204-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo, Y., Feng, X., Zheng, M., Zhang, D., Xiao, H., & Li, N. (2021). Willingness to participate in frontline work during the COVID‐19 pandemic: A cross‐sectional study of nurses from a province in South‐West China. Journal of Nursing Management. 10.1111/jonm.13309 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manzano García, G., & Ayala Calvo, J. C. (2021). The threat of COVID‐19 and its influence on nursing staff burnout. Journal of Advanced Nursing, 77(2), 832–844. 10.1111/jan.14642 [DOI] [PubMed] [Google Scholar]
- Maslach, C., & Jackson, S. E. (1981). The measurement of experienced burnout. Journal of Organisational Behavior, 2(2), 99–113. 10.1002/job.4030020205 [DOI] [Google Scholar]
- Mo, Y., Deng, L., Zhang, L., Lang, Q., Liao, C., Wang, N., Qin, M., & Huang, H. (2020). Work stress among Chinese nurses to support Wuhan in fighting against COVID‐19 epidemic. Journal of Nursing Management, 28(5), 1002–1009. 10.1111/jonm.13014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nashwan, A. J., Abujaber, A. A., Mohamed, A. S., Villar, R. C., & Al‐Jabry, M. M. (2021). Nurses’ willingness to work with COVID‐19 patients: The role of knowledge and attitude. Nursing Open, 8(2), 695–701. 10.1002/nop2.674 [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Health Commission of the People’s Republic of China . (2020). Nursing standards for patients of severe type and critical type with coronavirus disease 2019 (COVID‐19). http://www.nhc.gov.cn/xcs/zhengcwj/202003/8235a35f35574ea79cdb7c261b1e666e/files/f4269c33b5a94135a124609252595613.pdf
- Oh, N., Hong, N., Ryu, D. H., Bae, S. G., Kam, S., & Kim, K. Y. (2017). Exploring nursing intention, stress, and professionalism in response to infectious disease emergencies: The experience of local public hospital nurses during the 2015 MERS outbreak in South Korea. Asian Nursing Research, 11(3), 230–236. 10.1016/j.anr.2017.08.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raven, J., Wurie, H., & Witter, S. (2018). Health workers’ experiences of coping with the Ebola epidemic in Sierra Leone's health system: A qualitative study. BMC Health Services Research, 18(1), 251. 10.1186/s12913-018-3072-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwarzer, R., & Jerusalem, M. (1995). Generalized self‐efficacy scale. In In Weinman J., Wright S., & Johnston M. (Eds.), Measures in health psychology: A user’s portfolio. Causal and control beliefs (pp. 35–37). NFER‐NELSON. [Google Scholar]
- Sheng, Q., Zhang, X., Wang, X., & Cai, C. (2020). The influence of experiences of involvement in the COVID‐19 rescue task on the professional identity among Chinese nurses: A qualitative study. Journal of Nursing Management, 28(7), 1662–1669. 10.1111/jonm.13122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shi, Y., Wang, J., Yang, Y., Wang, Z., Wang, G., Hashimoto, K., Zhang, K., & Liu, H. (2020). Knowledge and attitudes of medical staff in Chinese psychiatric hospitals regarding COVID‐19. Brain, Behavior, & Immunity Health, 4, 100064. 10.1016/j.bbih.2020.100064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sichuan Academy of Medical Sciences . (2020). Epidemic prevention medical protective equipment related skin lesion and management (In Chinese). https://mp.weixin.qq.com/s/NqHFAN2cINbJ4fQMwpM8Dg
- Su, T. P., Lien, T. C., Yang, C. Y., Su, Y. L., Wang, J. H., Tsai, S. L., & Yin, J. C. (2007). Prevalence of psychiatric morbidity and psychological adaptation of the nurses in a structured SARS caring unit during outbreak: A prospective and periodic assessment study in Taiwan. Journal of Psychiatric Research, 41(1–2), 119–130. 10.1016/j.jpsychires.2005.12.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sultan, M., Løwe Sørensen, J., Carlström, E., Mortelmans, L., & Khorram‐Manesh, A. (2020). Emergency healthcare providers’ perceptions of preparedness and willingness to work during disasters and public health emergencies. Healthcare, 8(4), 442. 10.3390/healthcare8040442 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teng, C. I., Lotus Shyu, Y. I., & Chang, H. Y. (2007). Moderating effects of professional commitment on hospital nurses in Taiwan. Journal of Professional Nursing, 23(1), 47–54. 10.1016/j.profnurs.2006.10.002 [DOI] [PubMed] [Google Scholar]
- Weeks, K. P., & Schaffert, C. (2019). Generational differences in definitions of meaningful work: A mixed methods study. Journal of Business Ethics, 156(4), 1045–1061. 10.1007/s10551-017-3621-4 [DOI] [Google Scholar]
- World Health Organisation . (2021). WHO Coronavirus (COVID‐19) dashboard (China situation). https://covid19.who.int/region/wpro/country/cn
- Wu, B., Zhao, Y., Xu, D., Wang, Y., Niu, N., Zhang, M., Zhi, X., Zhu, P., & Meng, A. (2020). Factors associated with nurses’ willingness to participate in care of patients with COVID‐19: A survey in China. Journal of Nursing Management, 28(7), 1704–1712. 10.1111/jonm.13126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wuhan Municipal Health Commission . (2020). Updates on epidemic control by 18 February (10:23). http://wjw.wuhan.gov.cn/ztzl_28/fk/fkdt/202004/t20200430_1197241.shtml
- Zhang, X., Jiang, Z., Yuan, X., Wang, Y., Huang, D., Hu, R., Zhou, J., & Chen, F. (2021). Nurses reports of actual work hours and preferred work hours per shift among frontline nurses during coronavirus disease 2019 (COVID‐19) epidemic: A cross‐sectional survey. International Journal of Nursing Studies Advances, 3, 100026. 10.1016/j.ijnsa.2021.100026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41. 10.1207/s15327752jpa5201_2 [DOI] [PubMed] [Google Scholar]
- Zung, W. W. (1965). A self‐rating depression scale. Archives of General Psychiatry, 12(1), 63–70. 10.1001/archpsyc.1965.01720310065008 [DOI] [PubMed] [Google Scholar]
- Zung, W. W. (1971). A rating instrument for anxiety disorders. Psychosomatics: Journal of Consultation and Liaison Psychiatry, 12(6), 371–379. 10.1016/S0033-3182(71)71479-0 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.