

Abstract
Background
Pathology and imaging tests are frequently requested in the outpatient setting despite historically poor completion rates. The impact of COVID‐19 telehealth on test completion rates is unknown.
Aims
To examine the impact of the COVID‐19 pandemic and telehealth transition on pathology and imaging test request and completion rates in Australian outpatient clinics.
Methods
We performed a prospective cohort study with historical controls between March–May 2019 and March–May 2020. Pathology and imaging request and completion rates were collected in review consultation patients attending gastroenterology and rheumatology outpatient clinics at a tertiary healthcare system prior and during the early phases of the COVID‐19 pandemic in Melbourne.
Results
A total of 1376 patients was included in the study. Pathology tests were requested more frequently in the COVID‐19 group (n = 582/684, 85.2%) than the control group (n = 492/692, 71.1%, P < 0.001), but completion rates were lower in the COVID‐19 group (n = 443/582, 76.1%) than the control group (n = 426/492 (86.6%), P < 0.001). Imaging tests were requested more frequently in the COVID‐19 group (n = 345/682, 50.6%) than the control group (n = 295/692, 42.6%, P = 0.003), with lower rates of completion in the COVID‐19 group (n = 229/345, 66.4%) than the control group (n = 247/295, 83.7%, P < 0.001).
Conclusions
The COVID‐19 pandemic and telehealth transition have resulted in more frequent pathology and imaging requests but fewer test completion in the outpatients setting. This study has identified new clinical risks associated with the abrupt transition to telehealth during COVID‐19 that should be explored in future studies and appropriately mitigated.
Keywords: COVID‐19, outpatient, pathology, radiology, testing, completion
Introduction
In Australia, over 32 million episodes of specialist outpatient care were delivered between 2019 and 2020 with more than 175 million tests completed under the Medicare Benefit Scheme. 1 , 2 Tertiary hospitals provide an essential service in caring for the most vulnerable and complex members of our community. These patients tend to be older, socially disadvantaged, demonstrate lower health literacy and are culturally and linguistically diverse. 3 , 4 Pathology and radiology testing are frequently requested within the tertiary outpatient care context and are essential in the diagnosis, monitoring and management of complex conditions. There are currently no data available on outpatient hospital test patterns and completion rates. Studies conducted in primary care demonstrated that pathology and radiology tests were ordered in 47.6% and 11.0% of encounters respectively. 5 The rate of test adherence in primary care is suboptimal. Diabetic patients managed in primary care demonstrated 31% non‐adherence to pathology testing. 6 Similarly, a study in the hospital outpatient setting revealed 37.6% of non‐adherence to radiology follow‐up testing. 7 Low testing completion rates have been attributed to patient forgetfulness, poor health literacy and language barriers which further compounds the difficulty when delivering care for a complicated chronic disease cohort within an ambulatory hospital setting. 6
In response to the COVID‐19 pandemic, hospitals have pivoted towards a predominantly telehealth model of specialist outpatient management to prevent nosocomial transmission. The immediate and downstream impact of such a significant disruption to the delivery of specialist outpatient services has yet to be delineated. In Australia, 86.8% of consultations were previously delivered in‐person compared to 11.8% and 0.5% through telehealth and videoconference respectively. 3 In‐person consultations provided an avenue for clinicians to perform physical examinations, entrust patients with paper‐based prescriptions and test referrals, perform point‐of‐care investigations, and establish and reinforce the therapeutic relationship. The impact of virtual consultations on such aspects of care may be indirectly estimated from a study of telehealth in rural Australia, which highlighted the financial, cultural and technological barriers to successful telehealth implementation. 8 These barriers include insufficient funding to establish telehealth infrastructure, poor patient and clinician uptake, and lack of interoperability with existing legacy systems such as diagnostic referral systems. 8
The impact of the COVID‐19 pandemic on patient adherence to outpatient test completion prior to their telehealth appointment is currently unknown. A small survey in primary care reported 32% appointment non‐attendance and 21% non‐adherence to pathology test completion during the COVID‐19 pandemic. 9 Our study investigates the impact of telehealth transition on outpatient clinic attendance and test completion in the early phases of COVID‐19 pandemic.
Methods
Study design
We performed a prospective cohort study with a historical control as the comparator. Data were collected between 3 March 2020 and 8 May 2020 for the prospective cohort (COVID‐19) and between 5 March 2019 and 10 May 2019 for the historical control (pre‐COVID‐19) at Monash Health, a 1536 bed tertiary health network in metropolitan Melbourne, Australia. From 7 July 2020, Metropolitan Melbourne entered state‐wide lockdown with restrictions eased from 8 November 2020. Patients were identified from clinic schedules and information was obtained from the hospital's scanned medical records. The five clinics included were general gastroenterology, chronic liver disease, general rheumatology, vasculitis and rheumatoid arthritis. Clinic attendance and appointment type (new vs review), were assessed for all patients. Patients who were new to the clinic or did not attend the clinic appointment in the observed time frame were excluded from further analysis of pathology and radiology test ordering and completion rates.
Data extraction
Four investigators (TLL, AR, TWL, GP) extracted clinic and patient data using a standardised template. Baseline patient demographic data including age, gender, distance from home to clinic, primary language and interpreter requirements were collected. Information regarding the number of outpatient clinic appointments and failure to attend (FTA) rates for the 12 months prior to selected clinic appointment was obtained. Attendance at this clinic, either in‐person or through telephone, was assessed for all patients. For review patients who attended the clinic, requests for pathology and imaging testing for completion prior to review were determined from the previous clinic documentation. Test completion was ascertained through the outpatient clinical documentation and cross‐referenced with available results. The location for test completion was collected from internal pathology and radiology databases and scanned medical records if completed at external services.
Statistical analysis
All analyses were conducted using Stata version 15.1 (StataCorp, College Station, TX, USA). Patient and clinic characteristics were summarised as mean ± standard deviation, proportions or median (interquartile range). Student's t‐tests and Mann–Whitney U‐tests were used to examine continuous variables with normal and skewed distributions respectively. Categorical variables were analysed using Chi‐squared or Fisher's exact test. P‐values were two‐sided with a significance level of <0.05. Subgroup analysis for rheumatology and gastroenterology clinics was specified a priori.
Ethics approval
The study was approved by the Monash Health Human Research Ethics Committee as a quality assurance initiative.
Results
Data were collected on a total of 1882 patients (pre‐COVID‐19 = 940; COVID‐19 = 942) from the respective periods in 2019 and 2020. A total of 506 patients was excluded (320 patients for non‐attendance and 186 new patients), leaving 1376 patients eligible for the final analysis. The baseline patient clinical characteristics are summarised in Table 1. The mean age was 55.1 ± 15.6 years and 720 of 1376 (52.3%) patients were female. Of 1376 patients, 801 (58.2%) attended gastroenterology clinics and 575 of 1376 (41.8%) attended rheumatology clinics. The COVID‐19 group had a larger proportion of patients from the gastroenterology clinics compared to pre‐COVID‐19 group (454/690 (66.2%) vs 349/693 (50.4%), P < 0.0001). Of 1376 patients, 562 (40.8%) owned a landline, 1346 of 1376 (97.8%) patients owned a mobile phone and 533 of 1376 (38.7%) owning both. The mean distance from the home suburb to the medical centre was 22.0 ± 33.3 km. English was the primary language in 1022 of 1376 (74.2%) patients and 273 of 1376 (19.9%) patients required an interpreter.
Table 1.
Characteristics of review patients who attended clinic pre‐COVID‐19 and during COVID‐19
| Characteristics of review patients who attended clinic (n) | Overall (1376) | Pre‐COVID‐19 (692) | COVID‐19 (684) | P value † |
|---|---|---|---|---|
| Age (years) | 55.06 ± 15.64 | 55.63 ± 15.59 | 54.47 ± 15.69 | 0.17 |
| Gender | ||||
| Female, n (%) | 720 (52.33) | 371 (53.61) | 349 (51.02) | 0.34 |
| Clinic department, n (%) | ||||
| Gastroenterology | 801 (58.21) | 349 (50.43) | 452 (66.08) | |
| Rheumatology | 575 (41.79) | 343 (49.57) | 232 (33.92) | <0.001 |
| Home phone, n (%) | 562 (40.84) | 306 (44.22) | 256 (37.43) | 0.01 |
| Mobile, n (%) | 1346 (97.82) | 673 (97.25) | 673 (98.39) | 0.15 |
| Distance from home to tertiary centre (km) (n = 634) | 21.97 ± 33.29 | 21.36 ± 35.11 | 22.72 ± 30.97 | 0.59 |
| English as a first language, n (%) | 1022 (74.27) | 526 (76.01) | 496 (72.51) | 0.14 |
| Interpreter, n (%) | 273 (19.84) | 127 (18.35) | 146 (21.35) | 0.06 |
| Total number of appointments made in past 12 months (median, interquartile range) | 3.0 (2–6) | 3.0 (2–6) | 3.0 (2–5) | 0.20 |
†Student's t‐test and Chi‐squared for parametric values; Mann–Whitney and Fisher's exact for nonparametric.
Attendance
Clinic attendance rates were assessed for all patients. Prior to the COVID‐19 pandemic, 772 of 940 (82.1%) patients attended scheduled clinic appointments compared with 790 of 942 (83.9%) patients during the early phase of the pandemic prior to the state‐wide lockdown in metropolitan Melbourne (P = 0.32). In the 12 months prior to the first COVID clinic, the median (IQR) number of clinic appointments per patient was 3.0 (2–6) (pre‐COVID‐19 = 3.0 (2–6) vs COVID‐19 = 3.0 (2–5), P = 0.20).
Pathology tests
Pathology tests were requested in a higher proportion of consultations during the COVID‐19 pandemic (582/683; 85.2%), than pre‐COVID‐19 (492/692; 71.1%; P < 0.001) (Fig. 1). In contrast, test completion was lower during the COVID‐19 pandemic (443/582 (76.1%)) compared to pre‐COVID‐19 (426/492; 86.6%; P < 0.001) (Fig. 1). The majority of patients completed their pathology tests using the Monash Health pathology service and this was similar during the COVID‐19 pandemic (332/444; 74.8%) compared to pre‐COVID‐19 (326/426; 76.5%; P = 0.55).
Figure 1.
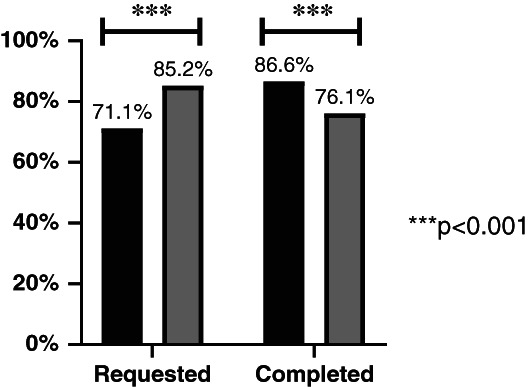
Rates of pathology test requests and completion prior to (n = 692) and during the COVID‐19 pandemic (n = 684). ( ), Pre‐COVID‐19; (
), Pre‐COVID‐19; ( ), COVID‐19.
), COVID‐19.
Imaging tests
Trends for imaging tests were similar to those of pathology. Imaging testing request rates increased during the COVID‐19 pandemic (345/682; 50.6%) compared with pre‐COVID‐19 (295/692; 42.6%; P = 0.003) (Fig. 2). However, imaging test completion was lower during the COVID‐19 pandemic (229/345; 66.4%) than pre‐COVID‐19 (247/295; 83.7%; P < 0.001) (Fig. 2). The majority of patients completed the radiology test internally at Monash Health and this did not differ during the COVID‐19 pandemic (191/227; 84.1%) compared with prior (205/248; 82.7%; P = 0.75).
Figure 2.
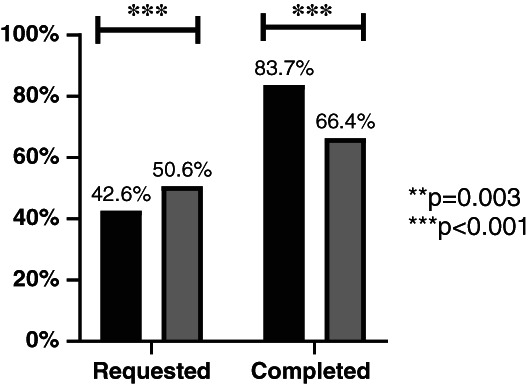
Rates of radiology test requests and completion prior to (n = 692) and during the COVID‐19 pandemic (n = 684). ( ), Pre‐COVID‐19; (
), Pre‐COVID‐19; ( ), COVID‐19.
), COVID‐19.
Discussion
We investigated the impact of large‐scale adoption of telehealth during the COVID‐19 pandemic on specialist ambulatory care clinic attendance, pathology and imaging request and completion rates. One of the major strengths of our study was the large sample size and diverse patient population, which helped us identify real world challenges to the ongoing expansion of telehealth in the post‐COVID world. How will telehealth change the way we request and act on diagnostic data? How can we best scale telehealth to a diverse real‐world population? Our study challenges the assumption that telehealth can improve healthcare efficiency and produce substantial cost reductions. We demonstrated a 14.1% increase in pathology and 8.0% increase in imaging orders by clinicians during the COVID‐19 pandemic. This observed change may reflect increased dependency on diagnostic testing for evaluation of disease status, driven by the inability physically to examine and assess patients in person. While the demand for telehealth enabling technology (software and hardware) has increased due to the widespread adoption of outpatient telehealth in outpatient care, there is a market gap for technology that can substitute or enable the physical examination, such as abdominal or joint examination. 10 The potential for increased healthcare cost and patient harm due to increased diagnostic test requests warrants further investigation and strategies to mitigate these unintended consequences once telehealth is scaled post‐COVID‐19.
Despite an increase in test ordering, there was a reduction in test completion. Pathology test completion was reduced by 10.5% and imaging tests by 17.4%. The beginning of the COVID‐19 pandemic brought about panic and uncertainty with fear of infection identified as a reason for avoidance of health services during the COVID‐19 pandemic, including pathology and imaging providers. 11 The Australian population was advised to avoid all non‐essential services to help stem the spread of COVID‐19. This combined with the loss of an immediate physical item in the form of a paper request could be contributing factors to less test completion that occurred during the beginning of the pandemic. Furthermore, a vital part of communication is nonverbal cues which is difficult over virtual platforms. Clinic appointments often convey a lot of information and the removal of a face‐to‐face consultation could have an impact on patients’ understanding of further management. This is particularly the case for phone consultations that lack even a visual platform in which to communicate through. In addition, the availability of services may be reduced due to social distancing measures and more stringent cleaning processes, particularly in imaging centres that have reported an anticipated 50–70% decrease in imaging volume. 12 Pathology collection centres within our network were closed during the initial phase of lockdown which also impacted on the ability of patients to complete their requested test within our health network, although we did record down external pathology results as well. The hospital system in which this study was undertaken still largely utilises paper requests for ordering outpatient investigations. With telehealth, these paper requests are now mailed to patients resulting in potential delayed or lost paperwork. This challenge is further amplified during the COVID‐19 pandemic as a result of disrupted logistic services. 13
Contrary to the literature, our clinic attendance rates were not affected by the COVID‐19 pandemic. Fear of COVID‐19 transmission in hospital settings and the need to isolate have been proposed as some of the reasons for delayed or nonattendance for medical services. 14 Our tertiary centre made a pivot to telehealth consultations early on in the pandemic (16 March 2020), allowing ongoing contact with patients without the need or fear of face‐to‐face consultations. Despite this, attendance rates for public hospital outpatient clinics have been historically poor, with 5–16% of all clinic bookings missed. 15 , 16 , 17 Our FTA rate was 17%, which is consistent with the literature, but we did not contact the patients to ascertain the reason. Common reported reasons for non‐attendance include forgetfulness, clerical errors, and inpatient admission at another hospital. 18 Past studies have identified factors that predict non‐attendance, including age 16–30 or >90 years, and low socioeconomic status. 19 Long home‐to‐clinic distances have also been reported as a predictor for non‐attendance, 20 a factor eliminated by the introduction of telehealth, similar to a previous study in Australia. 21
A study limitation is the difference in sample of specialty clinics between the pre‐COVID‐19 and COVID‐19 group. While this may be a confounding factor for the difference in test orders observed in this study, a subgroup analysis found no difference in test ordering patterns prior and during the COVID‐19 pandemic between the clinical services. As data were only obtained from two medical specialties, it may be difficult to generalise the findings of our study to other services, especially surgical clinics. This was conducted in the early days of the COVID‐19 pandemic and the consequential rapid transition to telehealth occurred nearly simultaneously, so it is difficult to attribute our findings to one or the other. It is also unclear from this study the impact of incomplete test completion on patient outcome.
Conclusion
We have highlighted a significant increase in pathology and imaging test orders, and decreased rates of test completion, after the widespread adoption of telehealth during the COVID‐19 pandemic. Future studies should investigate the underlying reasons for poor test adherence. The health and economic impacts of increased test request and test non‐adherence are yet to be elucidated, and understanding this will allow strategic allocation of funding to improve health outcomes in the setting of expanded use of telehealth during, and after, the COVID‐19 pandemic.
Funding: None.
Conflict of interest: None.
References
- 1. Australian Institute of Health and Welfare (AIHW). Australia's Health 2018. Canberra: AIHW; 2018. [cited 2020 Aug 18]. Available from https://www.aihw.gov.au/reports/australias-health/australias-health-2018
- 2. Australian Government Department of Health . Medicare Statistics: Rolling 12‐Month Time Series. 2020. [cited 2020 Aug 18]. Available from https://www1.health.gov.au/internet/main/publishing.nsf/Content/Medicare+Statistics-1
- 3. Australian Institute of Health and Welfare (AIHW) . Non‐Admitted Patient Care 2018‐2019: Australian Hospital Statistics. Canberra: AIHW; 2020. [cited 2020 Aug 18]. Available from https://www.aihw.gov.au/reports-data/myhospitals/sectors/non-admitted-patients
- 4. Jessup RL, Osborne RH, Beauchamp A, Bourne A, Buchbinder R. Differences in health literacy profiles of patients admitted to a public and a private hospital in Melbourne, Australia. BMC Health Serv Res 2018; 18: 134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Britt H, Miller GC, Henderson J, Bayram C, Harrison C, Valenti L et al. General Practice Activity in Australia 2015–16. Sydney, Australia: Sydney University Press; 2016. [Google Scholar]
- 6. Ramsay N, Johnson T, Badrick T. Diabetic patient adherence to pathology request completion in primary care. Aust Health Rev 2017; 41: 277–82. [DOI] [PubMed] [Google Scholar]
- 7. You JJ, Laupacis A, Newman A, Bell CM. Non‐adherence to recommendations for further testing after outpatient CT and MRI. Am J Med 2010; 123: 557.e1–8. [DOI] [PubMed] [Google Scholar]
- 8. Jang‐Jaccard J, Nepal S, Alem L, Li J. Barriers for delivering telehealth in rural Australia: a review based on Australian trials and studies. Telemed J E Health 2014; 20: 496–504. [DOI] [PubMed] [Google Scholar]
- 9. London Agency . Consumer Survey: Access to Healthcare During COVID‐19. Continuity of Care Collaboration; 2020. [Google Scholar]
- 10. Weinstein RS, Krupinski EA, Doarn CR. Clinical examination component of telemedicine, telehealth, mHealth, and connected health medical practices. Med Clin North Am 2018; 102: 533–44. [DOI] [PubMed] [Google Scholar]
- 11. Lazzerini M, Barbi E, Apicella A, Marchetti F, Cardinale F, Trobia G. Delayed access or provision of care in Italy resulting from fear of COVID‐19. Lancet Child Adolesc Health 2020; 4: e10–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Cavallo JJ, Forman HP. The economic impact of the COVID‐19 pandemic on radiology practices. Radiology 2020; 296: E141–E4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Universal Postal Union . The COVID‐19 Crisis and the Postal Sector. Switzerland: Internation Buereau, Research and Strategy Programme; 2020. [Google Scholar]
- 14. Ornell F, Schuch JB, Sordi AO, Kessler FHP. Pandemic fear and COVID‐19: mental health burden and strategies. Braz J Psychiatry 2020; 42: 232–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Sharp DJ, Hamilton W. Non‐attendance at general practices and outpatient clinics. BMJ 2001; 323: 1081–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Pillai R, Bhangu N, Narayanan M, Yoong W. A demographic study to profile non‐attenders at a gynaecology outpatient clinic. J Obstet Gynaecol 2012; 32: 156–8. [DOI] [PubMed] [Google Scholar]
- 17. Wolff DL, Waldorff FB, von Plessen C, Mogensen CB, Sørensen TL, Houlind KC et al. Rate and predictors for non‐attendance of patients undergoing hospital outpatient treatment for chronic diseases: a register‐based cohort study. BMC Health Serv Res 2019; 19: 386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Murdock A, Rodgers C, Lindsay H, Tham TCK. Why do patients not keep their appointments? Prospective study in a gastroenterology outpatient clinic. J R Soc Med 2002; 95: 284–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Ellis DA, McQueenie R, McConnachie A, Wilson P, Williamson AE. Demographic and practice factors predicting repeated non‐attendance in primary care: a national retrospective cohort analysis. Lancet Public Health 2017; 2: e551–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Dantas LF, Fleck JL, Cyrino Oliveira FL, Hamacher S. No‐shows in appointment scheduling – a systematic literature review. Health Policy 2018; 122: 412–21. [DOI] [PubMed] [Google Scholar]
- 21. Greenup EP, Best D, Page M, Potts B. No observed reduction of non‐attendance rate in telehealth models of care. Aust Health Rev 2020; 44: 657–60. [DOI] [PubMed] [Google Scholar]