

Abstract
Two hundred ninety-four children from low-income families (58% White, 17% Latinx, 25% Black; 54% girls; Mage = 4.49 years old at study entry) were recruited from Head Start classrooms to participate in a randomized-controlled trial of the project REDI preschool intervention and then followed longitudinally for 10 years through ninth grade. At study entry, parents reported on their children’s exposure to adverse experiences (ACEs). Youth reported on their feelings of social-emotional distress and school bonding after making the transition into middle school (seventh grade) and high school (ninth grade). Multilevel latent profile analyses revealed three profiles of adolescent distress and school bonding. Increased rates of ACEs in early childhood predicted membership in adolescent profiles characterized by heightened social-emotional distress and reduced levels of school bonding. The REDI intervention that focused on promoting early social-emotional and language skills in preschool moderated the impact of early ACEs on adolescent adjustment and promoted youth resilience, significantly buffering children from the negative impact of early ACEs on their levels of social-emotional distress and school bonding.
Keywords: preschool intervention, social-emotional learning, adverse childhood experiences, adolescent adjustment, resilience
Children growing up in poverty are especially likely to experience adversity during the first five years of life, including parent-child separations, family violence, unstable housing, and parental dysfunction that reduces early parenting support (Evans & Kim, 2013). This early adversity may leave children vulnerable to feelings of distress and insecurity in later life, particularly during high-stress events such as the transitions into middle and high school that most students undergo in early adolescence. Interventions implemented in the preschool context may foster later resilience to school stressors by helping children develop skills that support successful adaptation and coping, including the capacity to regulate their emotions and form supportive relationships with teachers and peers. This study evaluated associations between exposure to adverse childhood experiences (ACEs) in early childhood and later adolescent adjustment. In addition, it evaluated the degree to which the REDI preschool intervention promoted resilience and buffered children against the negative effects of ACEs on levels of social-emotional distress and school bonding experienced in adolescence.
Family Adversity and Youth Development
Adverse childhood experiences (ACEs) are traumatic or otherwise stressful experiences that expose children to inconsistent and unpredictable threat and/or harm and reduce access to safe and secure sources of social and emotional support. Prior research has identified a broad set of ACEs that negatively affect development, including exposure to abuse (physical, sexual, and emotional) or neglect, domestic violence, parent-child separation, various forms of parental dysfunction (psychopathology, antisocial activity, cognitive impairment, substance use), and community violence (Anda et al., 2006; Felitti et al., 1998). Children who grow up in poverty are disproportionately exposed to ACEs (Crouch, Probst, Radcliff, Bennett, & McKinney, 2019; Evans & Kim, 2013). ACEs have been linked with a host of negative outcomes for children, including poor health outcomes (Anda et al., 2006; Hughes et al., 2017), impaired social functioning (McEwen & McEwen, 2017), increased emotional distress and poor mental health (Patten et al., 2015; Petruccelli, Davis, & Berman, 2019), and school adjustment difficulties (Hair, Hanson, Wolfe, & Pollak, 2015).
Conceptually, exposure to ACEs in early childhood may increase later vulnerability to social-emotional distress and school adjustment difficulties by disrupting the development of the physiological systems that regulate adaptive stress responding (Evans & Kim, 2013). Frequent exposure to unpredictable, inconsistent, and threatening events along with reduced access to sensitive and responsive caregiving may impede the development of the prefrontal cortex and delay the development of the self-regulatory structures that help children manage their emotions and control their attention and behavior (Blair & Raver, 2012). Exposure to ACEs in early childhood may also affect later functioning via more indirect pathways, primarily by their impact on parenting and parent-child relationships. For example, attachment theory posits that positive, consistent bonds with caregivers in early childhood help children predict, make sense of, and interact with their environment, especially in times of difficulty (Sroufe & Waters, 1977). Children internalize representations of these early caregiving experiences as they develop, and these internal working models affect the degree to which they experience feelings of inner security and efficacy versus feelings of insecurity and distress when faced with stressors (McCarthy & Maughan, 2010). Secure parent-child attachments may be impaired by ACEs, particularly those that impede effective parenting, such as parent-child separation, parent depression, substance use, or cognitive impairment (Cyr, Euser, Bakermans-Kranenburg, & Van Ijzendoorn, 2010; Steele et al., 2016). Children who experience high levels of ACEs in early childhood may remain emotionally and behaviorally reactive to stress as they get older (e.g., Lee & Hankin, 2009), creating an increased likelihood of social and emotional distress, reduced engagement with school members and peers, and feelings of vulnerability. Feelings of distress and disengagement may be amplified in early adolescence by developmental changes that include disruptions in social support associated with changes in school contexts.
Transition to Adolescence
Adolescence is a developmental period characterized by transformations in key areas of social-emotional functioning that, in the U.S. school system, typically co-occur with major transitions in school context. Most American students move from smaller, self-contained elementary classrooms to larger middle or junior high schools during preadolescence (11–12 years old). A similar shift takes place three years later for most students, as they transition from middle schools to larger high schools. At each of these school transitions, students experience increased expectations for autonomous functioning in social and academic domains, along with decreases in the familiarity and predictability of relationships with peers and teachers (Simmons & Blythe, 2017). Given the growth in size and importance of the peer group, young adolescents often experience increased concerns about acceptance and fitting in (Aikins, Bierman, & Parker, 2005). The concurrent physical and emotional changes that accompany puberty may amplify already-increased levels of stress (Simmons & Blythe, 2017).
The effects of early ACEs exposure may be particularly impactful and problematic during this early adolescent period of school transitions because early adversity may increase stress reactivity (Gunnar, Wewerka, Frenn, Long, & Griggs, 2009), predisposing youth to view the world as unsafe and unpredictable and compromising their ability to adaptively handle stressors (Breslau et al. 2014; McElroy & Hevey, 2014). School transitions may reduce the predictability and consistency in their everyday life and decrease the availability of both peer and adult sources of social-emotional support.
Childhood ACEs serve as a risk factor associated with adolescent social-emotional distress and interpersonal problems, including mental health problems (Schalinski et al., 2016; Sheffler, Stanley, & Sachs-Ericsson, 2020) and poor school engagement (Bellis et al., 2018; Bethell, Newacheck, Hawes, & Halfon, 2014). Social-emotional distress in adolescence is associated with concurrent and future anxiety and depression (Lee & Hankin, 2009) and with elevated levels of risky adolescent behaviors, including substance use, sexual promiscuity, and poor behavioral adjustment (Hessler & Katz, 2010).
Because they often predispose children to view relationships and environments as unsafe or unpredictable, early ACEs can also affect children’s perceptions of and experiences in the school setting. ACEs may especially undermine school bonding, reflecting a student’s sense of connectedness to and belonging at school. Feeling insecure in their relationships with teachers and peers can increase feelings of vulnerability at school, contributing to less positive attitudes toward school and a diminished willingness to invest or engage in school-related activities (Bethell et al., 2014). Low levels of school bonding in adolescence are associated with elevated rates of truancy and school dropout (Maynard et al., 2017; Van Eck, Johnson, Bettencourt, & Johnson, 2017), poor academic achievement (Dotterer & Lowe, 2011), and problems with depression and substance use (Wang & Peck, 2013). The failure to establish strong school bonds also deprives vulnerable youth of an important source of protective support demonstrated to buffer them against the negative effects of ACEs later in life (e.g., Clements-Nolle & Waddington, 2019; Forster, Gower, Borowsky, & McMorris, 2017). The current study sought to examine the impact of early ACEs on children’s perceptions of their own social-emotional distress and their experiences of school bonding in adolescence.
Previous research suggests that the social-emotional skills and attitudes and expectations that children have prior to their middle school transition predict post-transition distress and school adjustment (Aikins, Bierman, & Parker, 2005; Kingery, Erdley, & Marshall, 2011). It is possible that early intervention focused on strengthening social-emotional skills and social relationships might buffer children during stressful school transitions and be of particular benefit to children who are vulnerable to feelings of distress associated with early ACEs exposure (Von Cheong, Sinnott, Dahly, & Kearney, 2017).
Promoting Resilience with Preschool Intervention
Intervening during early childhood to address the effects of ACEs may be strategic, with the potential to prevent or reduce the negative impact on the neurodevelopment of self-regulatory processes during the preschool years (Blair & Raver, 2012). Early interventions that improve socialization supports and that promote the social-emotional and self-regulatory skills that foster adaptive stress coping may be key strategies to help address the needs of children growing up in risky environments (Blaustein & Kinniburgh, 2018). Fostering preschool language skills, particularly the capacity to label and talk about feelings as well as the ability to use language effectively to initiate and maintain supportive interpersonal relationships may also enhance self-regulation skills and build social supports (Ramsook, Welsh, & Bierman, 2020). Resilience in human development refers to good outcomes and positive adaptation in spite of threats to adaptation or development within a context of adversity (Luthar, Cicchetti, & Becker, 2000; Masten, 2016). Since ACEs may be particularly damaging to children’s internal working models and emotion regulation, it follows that promoting emotion skills (e.g., emotion knowledge, emotional reasoning) along with social and self-regulation skills in early childhood may boost resilience for children exposed to early ACEs. Such early intervention might buffer the negative impact of ACEs later in life by helping children understand and cope with their emotions and manage relationships more adaptively, thus reducing the impact of negatively-skewed internal working models. Supporting this early intervention approach, a growing research base documents the efficacy of social-emotional learning (SEL) programs for promoting the social-emotional adjustment of preschool children growing up in poverty (see reviews by Bierman & Motamedi, 2015 and McClelland, Tominey, Schmitt, & Duncan, 2017).
Children in the present study were participants in the randomized-controlled efficacy trial of the REDI intervention which used an evidence-based preschool SEL program as its foundation. This SEL program, Preschool PATHS (Promoting Alternative THinking Strategies; Domitrovich, Cortes, & Greenberg, 2007), included teacher-led lessons on prosocial skills for friendship making, emotional understanding, self-control, and social problem-solving. Each week, teachers followed a manual with detailed lesson plans and introduced a specific social-emotional skill using stories, puppets, and discussions. During the PATHS lesson and during a weekly scheduled extension session, teachers led role plays, games, or craft activities that allowed children to practice the target skill with support and feedback. Teachers also received coaching in generalized teaching practices designed to support positive social-emotional and self-regulatory skill development in the classroom throughout the day. PATHS was enriched by a synchronized interactive reading program designed to support child language skills and narrative understanding (Wasik, Bond, & Hindman, 2006) and focused on social-emotional themes. Teachers held daily reading sessions, reading and reviewing two books per week. Teachers were provided with a manual and books for the reading program, along with props, novel vocabulary, and scripted questions they could use during discussions to encourage child comprehension and promote advanced thinking and language skills. Book themes were coordinated with the PATHS program. For example, during the week when the PATHS lesson focused on the feeling “mad,” teachers read the books “I was so mad” by Mercer Mayer and “Nosy Nora” by Rosemary Wells (see https://sites.psu.edu/redi/program-materials for more detail). Focusing the interactive reading program on PATHS themes provided teachers with daily opportunities to model, discuss, and reinforce the targeted social-emotional and self-regulation skills and support the developing language skills that provide a foundation for emotional understanding, self-control, and social problem-solving.
Prior evaluations of REDI’s impact revealed positive effects on child social-emotional and self-regulation skills (Bierman et al., 2008) that were sustained through fifth grade (Welsh et al., 2020). This study explored the degree to which the intervention may have also buffered children with high ACEs exposure against heightened feelings of social-emotional distress and compromised school bonding in their early adolescent years.
The Current Study
The present study was designed to extend existing research in two ways by testing the hypotheses: 1) that early childhood ACEs will predict heightened emotional distress and diminished school bonding in early adolescence, and 2) that the REDI preschool intervention delivered in Head Start will buffer children against the negative effects of early ACEs, reducing or ameliorating negative effects on early adolescent emotional distress and school bonding. Study participants were recruited during the prekindergarten year in Head Start, when caregivers reported on their ACEs. Head Start centers were randomly assigned to receive intervention (the REDI curricular enrichments) or serve as a control group (usual practice Head Start). Participants were then followed longitudinally from pre-kindergarten through ninth grade, as they dispersed widely into multiple school districts. When they were in seventh and ninth grades, participants completed measures of social-emotional distress and school bonding. Multilevel latent profile analyses were used to identify profiles representing different levels of adolescent social-emotional distress and school bonding, and to examine predictive links associated with preschool ACEs and preschool intervention. It was hypothesized that, without early intervention, ACEs exposure would predict more negative adolescent adjustment profiles, but that the REDI intervention would promote resilience and diminish the negative effects of early ACEs exposure on adolescent adjustment.
Method
Participants
REDI trial participants included 356 prekindergarten children (58% White, 17% Latinx, 25% Black; 54% girls; Mage = 4.49 years old at study enrollment) recruited from 44 classrooms in 24 Head Start programs in three Pennsylvania counties. All 4-year-olds in these classrooms were invited to participate in the study, and the parents of 86% of them agreed to do so. Families were low-income (median annual income of $15,000). About one-third (31%) of the parents had less than a high school education, 60% graduated from high school or received a GED, 8% completed a technical degree, and 2% completed a college degree. Participating centers were stratified on rural versus urban location, length of program (e.g., half or full-day), and student demographics (percent students of color), and then randomized to intervention or control conditions. Figure 1 describes participant flow through the study. Sample demographics and additional descriptive statistics broken down by intervention status at study entry are presented in Supplemental Table S1.
Figure 1. Participant Flow Diagram for REDI Intervention.

Note. Some participants who were missing in 7th grade returned to the study in 9th grade; likewise, some participants who completed the study in 7th grade were missing in 9th grade. Because we combined 7th and 9th grade for interpretation, participants reported as missing in this flow diagram are those whose data were missing in both 7th and 9th grade.
Sample attrition was generally low and averaged about 2% per wave of data collection due mostly to participant mobility, with a retention rate of about 80% in ninth grade providing a sample of 294 for the present adolescent analyses. Attrition was not related to family demographics or baseline measures of child academic or social-emotional skills, although there was less attrition in the control group than the intervention group. Full information maximum likelihood methods were used in the analyses to handle missing data.
All study procedures followed the standards for the ethical conduct of research specified by the American Psychological Association and were approved by the Pennsylvania State University IRB (Head Start REDI – Research-based, Developmentally Informed; PRAMS00028979). Parents and teachers provided informed consent and students provided assent for participation; participants were compensated financially for completing assessments.
Intervention
The REDI classroom program (Bierman et al., 2008) targeted social-emotional learning and language/emergent literacy skills. Teachers taught the 33 weekly lessons of the Preschool PATHS curriculum (Domitrovich, Cortes, & Greenberg, 2007), covering the topics of prosocial skills, emotional understanding, self-control, and social problem-solving. Lessons introduced skill concepts using stories, puppet shows, and role plays, and teachers reinforced skill practice during weekly hands-on extension activities and by using REDI teaching strategies (positive classroom management, emotion coaching, and problem-solving dialogue) in the classroom. To reinforce social-emotional skills and enrich support for language development, teachers led interactive reading lessons four days per week following the approach of Wasik and colleagues (Wasik, Bond, & Hindman, 2006). Books were selected to link with the PATHS lesson of the week and teachers were provided with suggested questions to help them engage children in active discussion of the story. REDI also included a set of sound games to boost children’s phonological awareness, and alphabet center activities to build print awareness. To support intervention implementation, teachers received detailed manuals, four days of workshop training, and weekly coaching with a trained REDI Consultant (see Bierman et al., 2008 for more details). Implementation fidelity was monitored by REDI Consultants. On average, teachers completed most of the planned intervention activities across the academic year (ranging from 84% of the alphabet center activities to 88% of Preschool PATHS lessons). Average consultant ratings of implementation quality ranged between 4.39 – 4.70, reflecting descriptive anchors between 4 = adequate to 5 = strong.
Measures
Childhood ACEs.
At study entry, when children were in preschool, parents reported on the following nine ACEs during a structured interview describing the child’s developmental history conducted by a REDI staff member: 1) excessive family mobility (3 or more family moves); 2) a separation that involved living apart from the parent; 3) witnessing violence; 4) any form of child abuse; 5) parent arrest; 6) parent special education; 7) parent grade retention; 8) parent depression (CES-D Questionnaire) dichotomized at the clinical cutoff score for depression; and 9) frequent corporal punishment (swatting or spanking 5 times or more in the last week) (α = 0.55). Each ACE was scored dichotomously as being present or absent for a child. Rates of exposure in this sample to each of these adverse experiences and the tetrachoric correlations among the dichotomized experiences are shown in Table 1 (see Supplemental Table S2 for more details regarding the ACEs measure used in the study).
Table 1.
ACE Item Frequencies and Tetrachoric Correlations
| ACE Items | % | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Family mobility | 43% | -- | |||||||
| 2. Separation from parent | 25% | .30** | -- | ||||||
| 3. Violence exposure | 30% | .07 | .24** | -- | |||||
| 4. Child abuse | 11% | .26** | .35** | .34** | -- | ||||
| 5. Parent arrest | 46% | .25** | .42** | .24** | .34** | -- | |||
| 6. Parent special ed | 26% | .07 | −.01 | .16** | .20** | .14** | -- | ||
| 7. Parent grade retention | 39% | .17** | .09 | .25** | .22** | .27** | .40** | -- | |
| 8. Parent depression | 49% | .04 | .07 | .24** | .02 | .30** | .14** | .26** | -- |
| 9. Corporal punishment | 14% | .08 | .11* | .39** | .28** | .38** | .04 | .28** | .27** |
Note. The “%” column shows percentage of the sample endorsing the item.
p < .05,
p < .01.
Prior research on ACEs indicates a cumulative effect of exposure to adversity (i.e., having more ACEs is associated with poorer outcomes; Herrenkohl & Herrenkohl, 2007). To create a cumulative index of ACEs in this study, the nine items listed above were submitted to an item response theory (IRT) model using the “ltm” package (Rizopoulos, 2006) in R 3.4.3 (R Core Team, 2017). Rather than simply summing the experiences, the use of IRT weights items on the basis of their extremity (e.g., the relative frequency with which children experienced each risk) and discernment (e.g., the degree to which each risk differentiates those with higher vs. lower overall risk scores). IRT statistics are shown in Table 2. In our sample, child abuse, parent special education, and frequent corporal punishment were the most extreme items (least prevalent) whereas parent depression and parent arrest were the least extreme (most prevalent). Parent arrest and child abuse were the items that best differentiated children with higher or lower overall ACE scores. After IRT scoring, this measure was dichotomized to identify the children in the sample with the highest rates of ACEs (top third).
Table 2.
Item Response Theory Weighting Details
| ACE Item | Item Extremity | Item Discernment |
|---|---|---|
| Family mobility | 0.55 | 0.58 |
| Separation from parent | 1.42 | 0.88 |
| Violence exposure | 1.05 | 0.95 |
| Child abuse | 2.12 | 1.25 |
| Parent arrest | 0.13 | 1.47 |
| Parent special ed | 2.01 | 0.55 |
| Parent grade retention | 0.56 | 0.94 |
| Parent depression | 0.08 | 0.67 |
| Corporal punishment | 1.99 | 1.13 |
Adolescent outcomes.
Youth participants completed the same set of self-report measures in seventh grade and ninth grade which reflected the two specific constructs of interest in this study: social-emotional distress and school bonding.
Social-emotional distress.
Youth completed seven measures with subscales that indicated youth feelings of social-emotional distress. Youth completed the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997), which included the Emotional Symptoms subscale (5 items describing depressed and anxious feelings; “I am often unhappy, depressed or tearful”; α = 0.71) and the Peer Problems subscale (5 items describing social difficulties; “Others pick on me or bully me”; α = 0.57). Youth also completed the Positive and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988). The Negative Affect subscale indicated the extent to which youth experienced a set of 15 negative emotions (“Sad,” “Guilty,” and “Disgusted”; α = 0.90) rated with a 5-point scale. On the Relationships with Others subscale of the School Adjustment Questionnaire (Conduct Problems Prevention Research Group [CPPRG], 1997), children rated 5 items about their peer experiences during the past year (e.g., “I am having a hard time making friends at school this year”; α = 0.79) using a 5-point scale. On the 6-item subscale assessing perceived social competence from the Perceived Competence Scale for Children (Harter, 1982), children rated their efficacy in making friends (e.g., “Some kids wish that more people their age liked them”; α = 0.75) using a 4-point scale. They also completed the short form of the Loneliness and Social Dissatisfaction Scale (Parker & Asher, 1993) with 3 items reflecting feelings of loneliness (α = 0.81) and the Fear of Negative Evaluation subscale from the Social Anxiety Scale for Children-Revised (LaGreca & Stone, 1993), with 3 items assessing social worries (“I worry that other kids don’t like me”, α = 0.78). All items were scored such that a higher score indicated more social-emotional distress. Total subscale scores were standardized at each grade level and scores at both grade levels were used in multilevel latent profile analyses as indicators of youth social-emotional distress (repeated measures within subject; αgrade7 = 0.65; αgrade9 = 0.63).
School bonding.
Youth completed three measures with subscales that indicated youth feelings of school bonding. Youth completed the People in My Life Questionnaire (Ridenour, Greenberg, & Cook, 2006), including the 4-item School Bonding subscale reflecting positive feelings about school climate (e.g., “I like my class this year”; α = 0.69) and the 7-item Affiliation with Teacher subscale, reflecting positive feelings about teachers at the school (e.g., “My teachers respect my feelings”; α = 0.87). Youth also completed the 4-item General Adjustment subscale of the School Adjustment Questionnaire (SAQ; CPPRG, 1997), rating their general attitudes toward school (e.g., “My school is a place where people treat me well”; α = 0.83) using a 5-point scale. All items were scored so that a higher score indicated more positive attitudes toward school. Total subscale scores were standardized at each grade level and scores at both grade levels were used in multilevel latent profile analyses as indicators of school bonding (αgrade7 = 0.57; αgrade9 = 0.54). Supplemental Tables S3 and S4 provide descriptive statistics for these adolescent outcomes and additional demographic information characterizing the sample when children were in seventh and ninth grades.
Plan of Analysis
The first step in the analyses was to create person-oriented profiles that described sample variation in the two outcome domains (social-emotional distress and school bonding) across the adolescent years (seventh and ninth grades). We conducted multilevel latent profile analyses (MLPA) which allowed us to characterize individual profiles based on the multiple subscales reflecting adolescent adjustment (rather than simply creating composites across measures). We included the same measures collected in seventh and ninth grades in the profile analysis in order to provide a reliable characterization of individual differences across the adolescent period. This strategy improved precision of measurement and also increased power for moderation analyses relative to a model examining only one time period alone. MLPAs were computed using Mplus statistical software version 8.1 (two-level mixture analysis, MLR estimator; Muthén & Muthén, 1998–2017). Separate analyses were conducted to characterize individual differences in the domain of social-emotional distress (seven measures, each collected in seventh and ninth grades) and school bonding (three measures, each collected in seventh and ninth grades). Models included repeated measures collected in seventh and ninth grades (level 1 variables) nested within the child across time (level 2). Our strategy for model building was informed by prior studies conducted by Henry and Muthén (2010) and Van Eck et al. (2017). Profile selection was based on several goodness-of-fit indices, including low BIC and AIC values and high entropy values. We also considered profile distinctiveness and meaningful interpretations (Beets & Foley, 2010; Roesch, Villodas, & Villodas, 2010).
As the second step in analyses, the early childhood ACEs score was added to each of the MLPAs as a predictor to assess the degree to which having high ACEs in early childhood predicted membership in adolescent profiles reflecting higher levels of social-emotional distress and lower levels of school bonding. Then, intervention status (REDI intervention vs. control group) was added to each of the MLPAs as a predictor to assess the degree to which the REDI intervention was associated with adolescent profiles in each of the outcome domains for the entire sample (an intervention main effect). Finally, the ACEs score by REDI intervention status interaction term was added to each of the MLPAs to assess whether the REDI intervention moderated the impact of early ACEs on later adolescent adjustment profiles in either outcome domain (a moderated intervention effect). In these models, intervention was dichotomous (0 = control group, 1 = intervention group), and ACEs scores were dichotomous (0 = low ACEs exposure and 1= high ACEs exposure). Thus, the interaction term allowed us to assess four orthogonal groups: control group, low ACEs; control group, high ACEs; intervention group, low ACEs; and intervention group, high ACEs. In this model, significant interaction terms indicated that the association between early ACEs and later adolescent outcomes was different for children in the intervention and control groups. For all analyses, p values of less than .05 were used to indicate statistical significance.
These models tested two hypotheses. First, without intervention (e.g., in the control group), it was anticipated that children with high ACEs exposure would exhibit adolescent profiles reflecting greater social-emotional distress and less school bonding than children with low ACEs exposure. Second, among children with high ACEs exposure, it was anticipated that those who received intervention would exhibit more positive adolescent profiles than their counterparts in the control group. For interpretation of these analyses, relative risk (RR) refers to the probability of being in a more well-adjusted profile compared to the probability of being in a more poorly-adjusted profile for each comparison; values above 1 indicate an increased probability while values below 1 indicate a decreased probability.
Results
Multilevel Latent Profile Modeling
Several latent profiles models were estimated to identify likely subgroups of social-emotional distress and school bonding in adolescence. Table 3 presents full model fitting criteria for two-, three-, four-, and five-profile solutions for social-emotional distress and school bonding, respectively.
Table 3.
Model Fit Statistics for Social-Emotional Distress and School Bonding Latent Profile Models
| Number of level-1 profiles | df | LL | BIC | AIC | Entropy | Smallest profile n (%) |
|---|---|---|---|---|---|---|
| Social-Emotional Distress Latent Profiles | ||||||
| 2 | 22 | −5011.66 | 10162.80 | 10067.31 | 0.93 | 85 (29%) |
| 3 | 30 | −4822.68 | 9835.57 | 9705.36 | 0.90 | 31 (11%) |
| 4 | 38 | −4770.45 | 9781.84 | 9616.90 | 0.83 | 23 (8%) |
| 5 | 46 | −4716.11 | 9723.88 | 9524.22 | 0.84 | 25 (8%) |
| School Bonding Latent Profiles | ||||||
| 2 | 10 | −2231.46 | 4526.32 | 4482.91 | 0.73 | 135 (45%) |
| 3 | 14 | −2171.15 | 4431.07 | 4370.31 | 0.80 | 24 (8%) |
| 4 | 18 | −2158.77 | 4431.66 | 4353.54 | 0.71 | 20 (7%) |
| 5 | 22 | −2156.82 | 4453.12 | 4357.64 | 0.73 | 3 (1%) |
Note. The three-profile solution was selected for both Social-Emotional Distress and School Bonding.
In the domain of social-emotional distress, the three-profile model was chosen as best-fitting because entropy declined sharply past the three-profile solution and BIC indicated a substantial increase in model fit, which did not continue past the three-profile solution. Three profiles most succinctly described the data and were distinct and interpretable (see Figure 2). The “Low Distress” profile contained the most cases (n = 179; 61% of the sample) and had the lowest means on a majority of the distress indicators (i.e., youth in this profile endorsed fewer negative emotions and more social support than youth in the other profiles). The “High Distress” profile contained the fewest cases (n = 31, 11%) and had the highest means on all of the distress indicators. The remainder of the sample fell into a “Medium Distress” profile (n = 84, 29%). Full descriptive statistics for the social-emotional distress profiles are provided in Supplemental Table S5.
Figure 2. Latent Profiles for Social-Emotional Distress.

Note. Youth demographic characteristics by profile were as follows: low distress (61% of the sample; 48% female; 28% Black, 16% Latinx, 56% White), medium distress (29% of the sample; 63% female; 19% Black, 14% Latinx, 67% White), high distress (11% of the sample; 74% female; 10% Black, 10% Latinx, 80% White).
In the domain of school bonding, the three-profile model was also chosen as best-fitting because BIC reduced to its lowest point and entropy peaked at the three-profile solution. Three profiles most succinctly described the data and were distinct and interpretable (see Figure 3). The “Strong School Bond” profile (n = 109; 37% of the sample) had the highest means for all three indicators of a positive school bond (i.e., youth in this profile endorsed liking their classes more, feeling more respect from teachers, and experiencing more positive peer treatment than youth in the other profiles). The “Average School Bond” profile had the most cases (n = 161, 55%) and characterized the average level of adjustment in our sample. The “Weak School Bond” profile had the fewest cases (n = 24, 8%) and had the lowest means for all three indicators of school bond. Full descriptive statistics for the school bonding profiles are provided in Supplemental Table S6.
Figure 3. Latent Profiles for School Bonding.

Note. Youth demographic characteristics by profile were as follows: strong bond (37% of the sample; 55% female; 21% Black, 13% Latinx, 66% White), average bond (55% of the sample; 53% female; 27% Black, 16% Latinx, 57% White), weak bond (8% of the sample; 63% female; 8% Black, 17% Latinx, 75% White).
The profiles showed a moderate level of inter-correlation (r = .41), and 50% of the sample fell into a profile reflecting the same adjustment level (e.g., low, medium, or high) in both domains of social-emotional distress and school bonding. This degree of overlap is consistent with prior research that suggests that adjustment in the domains of social-emotional distress and school bonding may affect each other, but they are also distinct domains of functioning (e.g., Pate, Maras, Whitney, & Bradshaw, 2017).
Hypothesis-testing Models
Social-emotional distress.
Model results predicting the placement of adolescents in profiles of social-emotional distress are shown in Table 4. The first three rows illustrate associations between ACEs and adjustment profile placement in the control group. Consistent with the first hypothesis, without intervention, children with high ACEs were less likely than those with low ACEs to exhibit profiles of low distress than profiles of high distress (RR = 0.26, 95% CI [0.13, 0.51], p < .05) or medium distress (RR = 0.40, 95% CI [0.25, 0.64], p < .05). The next three rows in Table 4 illustrate the effect of intervention predicting adjustment profile placement for children with high ACEs exposure. Confirming hypothesis 2, children with high ACEs in early childhood who subsequently received the REDI preschool intervention were significantly more likely to exhibit profiles of low distress relative to high distress (RR = 8.10, 95% CI [3.16, 20.80], p < .05), such that children in the REDI intervention were about eight times more likely to be placed in the low distress profile relative to the high distress profile (see Figure 4). In contrast, intervention had no significant effect on the profiles of adolescent distress exhibited by children with low ACEs.
Table 4.
Relative Risk of Social-Emotional Distress Latent Profile Membership Among Children with High ACEs in the Intervention and Control Groups
| Children with High ACEs (n = 92) | Comparison | Relative Risk | Lower Bound | Upper Bound |
|---|---|---|---|---|
| Control Group (n = 41) | Medium vs. High Distress | 0.63 | 0.31 | 1.29 |
| Low vs. High Distress | 0.26* | 0.13 | 0.51 | |
| Low vs. Medium Distress | 0.40* | 0.25 | 0.64 | |
| Intervention Group (n = 51) | Medium vs. High Distress | 2.65 | 0.96 | 7.34 |
| Low vs. High Distress | 8.10* | 3.16 | 20.80 | |
| Low vs. Medium Distress | 3.06 | 1.62 | 5.78 |
p < .05
Figure 4.
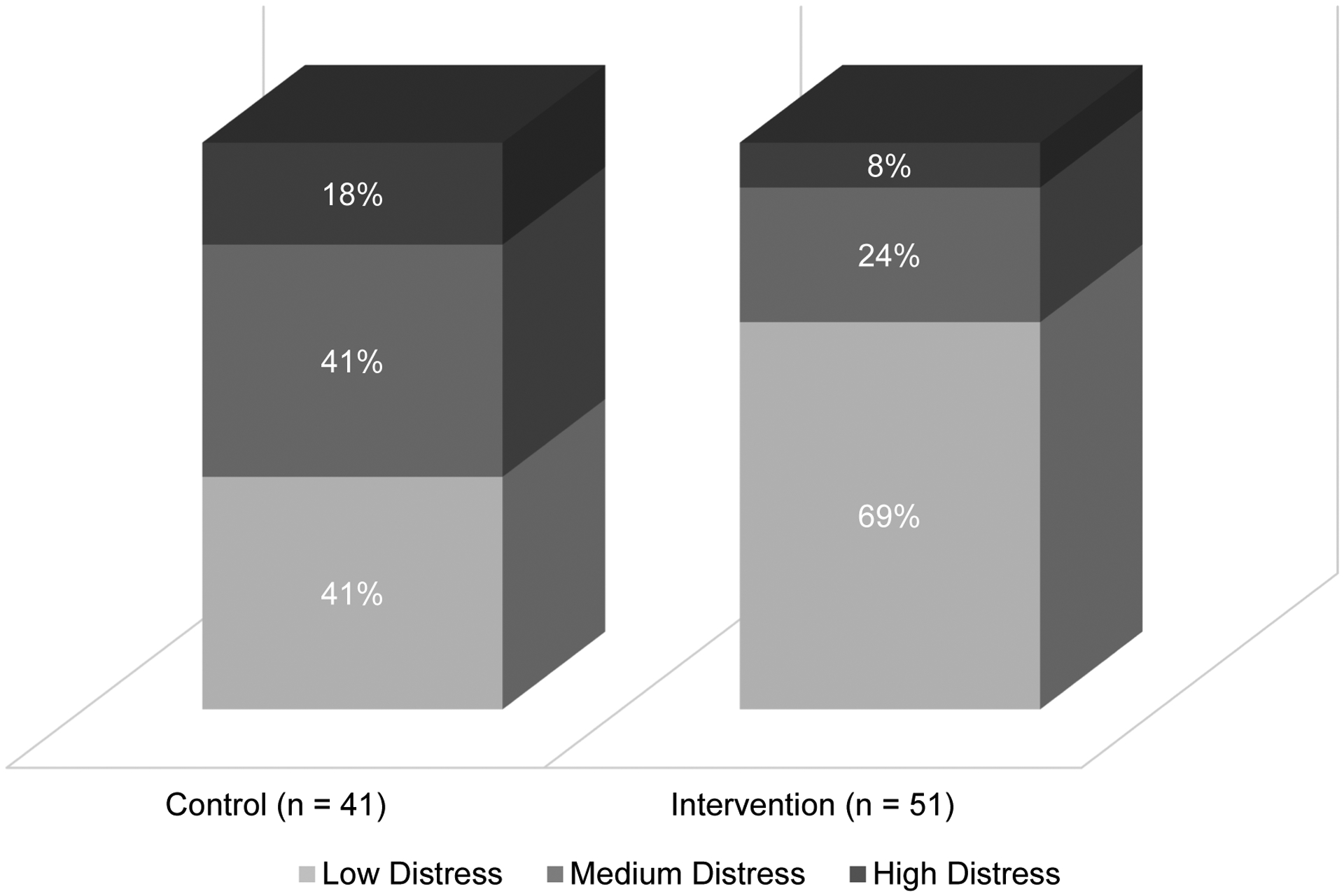
Social-Emotional Distress Latent Profile Distribution by Treatment Condition for High ACEs Group
School bonding.
Model results predicting adolescent profiles of school bonding are shown in Table 5. As shown in the first three rows, children from the control group with high ACEs were significantly less likely than those with low ACEs to exhibit profiles of average school bonding (RR = 0.13, 95% CI [0.06, 0.30], p < .05) or strong school bonding (RR = 0.08, 95% CI [0.03, 0.18], p < .05) than profiles of weak school bonding. Confirming hypothesis 2, children with high ACEs in early childhood who subsequently received the REDI preschool intervention were significantly more likely to exhibit profiles of average school bonding relative to weak school bonding (RR = 11.62, 95% CI [3.79, 35.66], p < .05), such that children in the REDI intervention were about 12 times more likely to be placed in the average school bond profile relative to the weak school bond profile. Additionally, these children were significantly more likely to exhibit profiles of strong school bonding relative to weak school bonding (RR = 17.81, 95% CI [5.62, 56.49], p < .05), such that children in the REDI intervention were about 18 times more likely to be placed in the strong school bond profile relative to the weak school bond profile (see Figure 5; see also Supplemental Table S7 for a tabular presentation of the data presented in Figures 4 and 5). Intervention had no significant effect on the profiles of adolescent school bonding of children with low ACEs.
Table 5.
Relative Risk of School Bonding Latent Profile Membership Among Children with High ACEs in the Intervention and Control Groups
| Children with High ACEs (n = 92) | Comparison | Relative Risk | Lower Bound | Upper Bound |
|---|---|---|---|---|
| Control Group (n = 41) | Average vs. Weak Bond | 0.13* | 0.06 | 0.30 |
| Strong vs. Weak Bond | 0.08* | 0.03 | 0.18 | |
| Strong vs. Average Bond | 0.58 | 0.35 | 0.97 | |
| Intervention Group (n = 51) | Average vs. Weak Bond | 11.62* | 3.79 | 35.66 |
| Strong vs. Weak Bond | 17.81* | 5.62 | 56.49 | |
| Strong vs. Average Bond | 1.53 | 0.79 | 2.97 |
p < .05
Figure 5.

School Bonding Latent Profile Distribution by Treatment Condition for High ACEs Group
Discussion
This study explored the associations between ACEs exposure in early childhood and aspects of social-emotional functioning in adolescence and examined the moderating impact of a preschool intervention on these associations. The central hypotheses were confirmed. High ACEs exposure in early childhood was associated with increased risk of experiencing social-emotional distress and weak school bonding in early adolescence. These findings are consistent with prior research suggesting that high ACEs during early childhood are associated with poorer adjustment in the domains of social-emotional functioning (including poor mental health; Sheffler et al., 2020) and school bonding/engagement (Bethell et al., 2014). The findings also extend prior research by documenting predictive links in a longitudinal study, with ACE exposure reported by parents when children were 4 years of age and adolescent distress and school bonding reported by adolescents at grades 7 and 9 (12–15 years of age).
In addition, this study demonstrated that receiving the REDI intervention in preschool conveyed some protection for children with high levels of early childhood ACEs exposure, reducing the prevalence of high social-emotional distress and weak school bonding experienced in adolescence. REDI is a resilience-focused, school-based intervention delivered in the classroom by Head Start teachers; thus, it has the potential to reach many young, at-risk children at relatively low cost. REDI targeted the promotion of social-emotional learning and early language skills, with the goal of helping children develop the emotional understanding, self-regulation, and social problem-solving skills that could support more positive emotion coping and social relationships as they transitioned into elementary school.
Interpreting Intervention Effects
Researchers have speculated that early interventions that promote emotional understanding, build self-regulation and coping skills, and strengthen social support systems may play a central role in enhancing the later psychosocial adjustment of children exposed to early ACEs (Blaustain & Kinniburg, 2018). This hypothesis is supported by developmental research demonstrating that vulnerable children with more well-developed social-emotional competencies and self-regulation skills show enhanced mental health and school adjustment in adolescence and later life (Eisenberg, Spinrad, & Eggum, 2010; Jones, Greenberg, & Crowley, 2015). It is also consistent with research suggesting that ACEs exposure in early childhood undermines the development of the neural systems that regulate stress reactivity and emotion regulation (Blair & Raver, 2012), and disrupt the quality of early attachment processes that provide a foundation for later internal working models and perceptions of interpersonal connectedness and self-worth (Cyr et al, 2010; Steele et al., 2016). From a conceptual standpoint, positioning interventions to support social-emotional development in the preschool years may be highly strategic because this is a time period when the foundational language and social-cognitive skills that underlie effective self-regulation and social functioning undergo rapid development and hence preschool intervention might offset the negative developmental impact of ACEs (Blair & Raver, 2012). Consistent with developmental research, a prior longitudinal study of children who received the Chicago Parent-Child Center preschool intervention (CPC; Niles, Reynolds & Roe-Sepowitz, 2008) documented improved adolescent social adjustment for the subgroup of children whose families were coded as high risk when they were preschoolers (high poverty, low parent education, single parent status), but not in those coded as low risk. Although the CPC study did not measure ACEs directly, the findings of this quasi-experimental program evaluation are consistent with the hypothesis that strategically-designed preschool interventions can have long-term benefits for the social-emotional well-being and school adjustment of young children growing up in high-risk contexts.
The REDI study findings make a unique and important contribution to this literature, as it represents the first randomized-controlled trial of a preschool enhancement intervention emphasizing enriched SEL that has followed children into adolescence to evaluate their social-emotional functioning. Children in the control group attended usual practice Head Start, reducing risks that the results reflect general aspects of educational or family support offered in the Head Start system and increase confidence that the findings can be attributed causally to the REDI intervention. At the same time, the specific mechanisms by which the REDI program reduced the social-emotional distress and promoted the school bonding of adolescents exposed to high levels of early ACEs is unclear. REDI was a multi-component intervention that included intervention activities designed to promote language and emergent literacy skills as well as social-emotional and self-regulation skills. Compared with other preschool SEL programs that have documented short-term benefits for children (Bierman & Motamedi, 2015; McClelland et al. 2017), REDI provided a “double dose” of SEL programming by integrating a daily interactive reading program with the Preschool PATHS program, so that preschool teachers focused explicitly on supporting emotion talk, self-regulation strategies, and social problem-solving skills on a daily basis. The relative roles that enhanced emotion knowledge or language skills in preschool, or improved learning engagement and interpersonal relationships during the elementary school years (Welsh et al., 2020) played in supporting the adolescent outcomes documented here remain unknown. In addition, questions about the threshold of “dose” needed to support skill levels that confer longer-term resilience remain. Future research is needed to replicate the current findings as well as to illuminate the developmental pathways that may account for the long-term intervention benefits.
Additional follow-up research is also needed to determine whether the improved social-emotional functioning documented here in adolescence will reduce the risk that ACE-exposed youth face for future mental health maladjustment or risky behaviors including substance use, school drop-out, or antisocial activities (Hessler & Katz, 2010; Maynard et al., 2017; Wang & Peck, 2013).
Conceptualizing and Assessing ACEs
This study utilized an expanded ACEs scale that incorporated indices of the early adversities often experienced by children in low-income families (Finkelhor, 2018) along with indices of abuse and violence exposure (see also Mersky, Janczewski & Topitzes, 2017). ACEs were measured by parent-report at preschool entry, likely providing a more accurate assessment than the retrospective accounts made by adults which are used in many studies (Hardt & Rutter, 2004). Additionally, our analytic strategy took into account the relative severity of different experiences by using the IRT weighting approach.
However, it is worth noting that researchers have not yet reached a consensus regarding the specific experiences that should be included in the valid measurement of ACEs or the optimal assessment strategy. Initial measures of ACES tended to include a smaller set of events focused on child maltreatment and household dysfunction (Felitti et al., 1998). Subsequent researchers suggested that additional adverse life events often affect children growing up in poverty (Cronholm et al., 2015), leading to an expansion of items in ACEs scales designed to accurately capture the totality of the early adversity experience (Finkelhor, 2018; Finkelhor, Shattuck, Turner, & Hamby, 2015). For instance, a recent meta-analysis (Hughes et al., 2017) found that 31 different ACEs items appeared across 37 reviewed studies, and only 15 items appeared in three or more studies. In addition, a recent study demonstrated good psychometric properties and factor structure for a measure including both original ACEs and additional items, including bullying and food insecurity (Mersky, Janczewski & Topitzes, 2017). Similarly, our measure, obtained by parent report when children were preschoolers, included both widely accepted items such as child maltreatment and family instability (e.g., parent depression, parent-child separations, frequent moves), as well as several less common items that more closely represented the unique risk facing this low-income, Head Start sample (e.g., parent special education, parent grade retention, corporal punishment). Future research is needed to further refine measures of ACEs in ways that both identify and capture all salient features of children’s life experiences and exclude those that are less predictive of important outcomes. In addition, future research is needed to determine the optimal source of information about ACEs.
Study Strengths and Limitations
Important strengths of this study included the relatively large sample size, long-term prospective longitudinal design, and randomized-control trial that allowed for unbiased estimates of intervention impact. In addition, there are several study limitations to this study that should be considered when interpreting the results.
Although intervention was randomly assigned, ACEs were not. Hence, causal interpretations of the links between early childhood ACEs and adolescent outcomes are purely speculative. Multiple factors associated with the presence of ACEs may contribute to later outcomes, and the impact of early ACEs may continue throughout development as children are often continuously exposed to adversity.
As noted above, our assessment of ACE exposure was based on parent report collected at study entry when children were 4 years old. On the one hand, this kind of prospective data collected during early childhood is likely to avoid the significant recall biases associated with retrospective self-reports collected in adulthood (Hardt & Rutter, 2004; Reuben et al., 2016). For example, as many as 40% of individuals inconsistently remember experiences when recalling them retrospectively over multiple time points (Colman et al., 2016), making the prospective parent report of ACEs a strength of the study. At the same time, additional data sources would have bolstered the validity of these parent reports. For example, administrative data (e.g., school records, documented contact with social services or court systems, physicians’ notes) could counter potential tendencies for parent under-reporting of certain data (e.g., past abuse or incarceration). Such records are difficult to obtain, and many studies that include administrative data have incomplete or limited records (Reuben et al., 2016). However, even the availability of additional reporters (other caregivers, teachers) would have provided an assessment of reporting accuracy and the potential for a more robust ACEs assessment.
The outcome measures included in this study were limited to self-reports. Prior research suggests that adolescent self-reports of internalizing symptomatology do not typically align well with parent (Rescorla et al., 2013) or teacher ratings (De Los Reyes, Alfano, & Beidel, 2010). Hence, self-report measures may be the most valid source of data regarding adolescent’s perceptions about their feelings of distress and school bonding. In this study, findings were based on self-report data collected at two time points during adolescence to increase the robustness of the assessments of social-emotional experiences. However, these findings may not reflect other indices of adolescent maladjustment that could be measured more accurately by parent or teacher report or school records, such as school attendance and performance or behavior problems. Future studies should examine a wider array of adolescent outcomes and include measures from other raters (i.e., teacher-report, administrative data) to understand the breadth of ACEs association and early intervention impact.
Finally, it should be noted that the present study sample was drawn from Head Start programs in three counties in Pennsylvania. The degree to which the current findings may generalize more broadly to youth from low-income families in demographically and culturally dissimilar contexts is unknown.
Conclusions and Implications for Practice
The study findings carry important implications for educational policy and practice. Given that ACEs are common in the lives of young children growing up in poverty, it is important that interventions effective at mitigating their impacts be readily available in classroom settings, and that teachers receive the training and professional development required to implement them in a time- and cost-effective manner. Many of the interventions designed to reduce social-economic disparities in education focus on enriching cognitive programming in preschool; this study suggests that focused and evidence-based efforts to support social-emotional learning in preschool may be especially important for children growing up in poverty in order to address the negative impact of ACEs on their future social-emotional well-being and school engagement. It further demonstrates that classroom teachers can effectively promote the resilience of children with high ACEs exposure, when they are provided with an evidence-based SEL program and coached in teaching strategies that enhance child social-emotional and self-regulation skills. Specific implications for practice include consistently incorporating support for the teaching strategies and skills taught in REDI into preschool practice, including an emphasis on building the social-emotional and foundational language skills that support self-regulation, adaptive school engagement, and positive interpersonal relationships. Future studies are needed to replicate and expand these findings and to explore the scalability and sustainability of preschool-based interventions like REDI that may support resilience and enhance the later school adjustment and social-emotion well-being of high-risk children.
In addition, ongoing research is needed to better understand the range of social, educational, and policy-based programming that can address the existing widespread disparities that affect the educational attainment, health, and overall well-being of children growing up in poverty.
Public health models suggest that addressing economic disparities and incorporating trauma informed principles into policies and social systems affecting these at-risk children may be critical to fully instigate social change (e.g., Shaefer et al, 2018; Weiland & Yoshikawa, 2012). Documenting the kind of early educational programming that can promote adolescent adjustment for children at early risk is an important first step. A broad perspective and high-quality research are needed to further identify the strategies that can help create greater equity in educational, mental health, and health outcomes.
Supplementary Material
Impact and Implications Statement:
This study illustrates the value of providing preschool social-emotional learning interventions to socioeconomically-disadvantaged children who have experienced multiple forms of adversity. Exposure to early trauma, family instability, and compromised parenting increases risk for later emotional distress, insecure social relationships, and school disengagement in adolescence. This study shows that children from low income families who experienced high levels of early adversity were protected from these negative adolescent outcomes when they received the REDI intervention: on average, these children showed similar levels of social-emotional distress and school bonding as children who did not experience extreme early adversity. By promoting early social-emotional interventions such as REDI, researchers and policy makers can positively impact the lives of many children.
Acknowledgments
This project was supported by the National Institute of Child Health and Human Development grant HD046064 and the Institute of Education Sciences grant R305B090007. The views expressed in this article are ours and do not necessarily represent the granting agencies. Appreciation is expressed to the teachers, students, parents, and program personnel who served as partners in this project in the Huntingdon, Blair, and York County Head Start Programs of Pennsylvania and the school districts supporting the longitudinal data collection.
References
- Aikins JW, Bierman KL, & Parker JG (2005). Navigating the transition to junior high school: The influence of pre-transition friendship and self-system characteristics. Social Development, 14(1), 42–60. 10.1111/j.1467-9507.2005.00290.x [DOI] [Google Scholar]
- Anda RF, Felitti VJ, Bremner JD, Walker JD, Whitfield CH, Perry BD, Dube SR, & Giles WH (2006). The enduring effects of abuse and related adverse experiences in childhood. European Archives of Psychiatry and Clinical Neuroscience, 256(3), 174–186. 10.1007/s00406-005-0624-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beets MW, & Foley JT (2010). Comparison of 3 different analytic approaches for determining risk-related active and sedentary behavioral patterns in adolescents. Journal of Physical Activity and Health, 7(3), 381–392. 10.1123/jpah.7.3.381 [DOI] [PubMed] [Google Scholar]
- Bellis MA, Hughes K, Ford K, Hardcastle KA, Sharp CA, Wood S, Homolova L, & Davies A (2018). Adverse childhood experiences and sources of childhood resilience: A retrospective study of their combined relationships with child health and educational attendance. BMC Public Health, 18, 1–12. 10.1186/s12889-018-5699-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bethell CD, Newacheck P, Hawes E, & Halfon N (2014). Adverse childhood experiences: Assessing the impact on health and school engagement and the mitigating role of resilience. Health Affairs, 33(12), 2106–2115. 10.1377/hlthaff.2014.0914 [DOI] [PubMed] [Google Scholar]
- Bierman KL, Domitrovich CE, Nix RL, Gest SD, Welsh JA, Greenberg MT, Blair C, Nelson KE, & Gill S (2008). Promoting academic and social-emotional school readiness: The Head Start REDI program. Child Development, 79(6), 1802–1817. 10.1111/j.1467-8624.2008.01227.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bierman KL, & Motamedi M (2015). Social-emotional learning programs for preschool children. In Durlak JA, Domitrovich CE, Weissberg RP, & Gullotta TP (Eds.), Handbook of social and emotional learning: Research and practice (pp. 223–250). Guilford Press. [Google Scholar]
- Blair C, & Raver CC (2012). Child development in the context of adversity: Experiential canalization of brain and behavior. American Psychologist, 67(4), 309–318. 10.1037/a0027493 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blaustein ME, & Kinniburgh KM (2018). Treating traumatic stress in children and adolescents: How to foster resilience through attachment, self-regulation, and competency (2nd ed.). Guilford Press. [Google Scholar]
- Breslau N, Koenen KC, Luo Z, Agnew-Blais J, Swanson S, Houts RM, Poulton R, & Moffitt TE (2014). Childhood maltreatment, juvenile disorders and adult post-traumatic stress disorder: A prospective investigation. Psychological Medicine, 44(9), 1937–1945. 10.1017/S0033291713002651 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clements-Nolle K, & Waddington R (2019). Adverse childhood experiences and psychological distress in juvenile offenders: the protective influence of resilience and youth assets. Journal of Adolescent Health, 64(1), 49–55. 10.1016/j.jadohealth.2018.09.025 [DOI] [PubMed] [Google Scholar]
- Colman I, Kingsbury M, Garad Y, Zeng Y, Naicker K, Patten S, Jones PB, Wild TC, & Thompson AH (2016). Consistency in adult reporting of adverse childhood experiences. Psychological Medicine, 46(3), 543–549. 10.1017/S0033291715002032 [DOI] [PubMed] [Google Scholar]
- Conduct Problems Prevention Research Group (CPPRG). (1997). School Adjustment. Available from the Fast Track Project Web site, http://www.fasttrackproject.org
- Crouch E, Probst JC, Radcliff E, Bennett KJ, & McKinney SH (2019). Prevalence of adverse childhood experiences (ACEs) among US children. Child Abuse & Neglect, 92, 209–218. 10.1016/j.chiabu.2019.04.010 [DOI] [PubMed] [Google Scholar]
- Cronholm PF, Forke CM, Wade R, Bair-Merritt MH, Davis M, Harkins-Schwarz M, Pachter LM, & Fein JA (2015). Adverse childhood experiences: expanding the concept of adversity. American Journal of Preventive Medicine, 49(3), 354–361. 10.1016/j.amepre.2015.02.001 [DOI] [PubMed] [Google Scholar]
- Cyr C, Euser EM, Bakermans-Kranenburg MJ, & Van Ijzendoorn MH (2010). Attachment security and disorganization in maltreating and high-risk families: A series of meta-analyses. Development and Psychopathology, 22(1), 87–108. 10.1017/S0954579409990289 [DOI] [PubMed] [Google Scholar]
- De Los Reyes A, Alfano CA, & Beidel DC (2010). The relations among measurements of informant discrepancies within a multisite trial of treatments for childhood social phobia. Journal of Abnormal Child Psychology, 38(3), 395–404. 10.1007/s10802-009-9373-6 [DOI] [PubMed] [Google Scholar]
- Domitrovich CE, Cortes RC, & Greenberg MT (2007). Improving young children’s social and emotional competence: A randomized trial of the preschool “PATHS” curriculum. The Journal of Primary Prevention, 28(2), 67–91. 10.1007/s10935-007-0081-0 [DOI] [PubMed] [Google Scholar]
- Dotterer AM, & Lowe K (2011). Classroom context, school engagement, and academic achievement in early adolescence. Journal of Youth and Adolescence, 40, 1649–1660. 10.1007/s10964-011-9647-5 [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Spinrad TL, & Eggum ND (2010). Emotion-related self-regulation and its relation to children’s maladjustment. Annual Review of Clinical Psychology, 6, 495–525. 10.1146/annurev.clinpsy.121208.131208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evans GW, & Kim P (2013). Childhood poverty, chronic stress, self-regulation, and coping. Child Development Perspectives, 7(1), 43–48. 10.1111/cdep.12013 [DOI] [Google Scholar]
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, & Marks JS (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245–258. 10.1016/S0749-3797(98)00017-8 [DOI] [PubMed] [Google Scholar]
- Finkelhor D (2018). Screening for adverse childhood experiences (ACEs): Cautions and suggestions. Child Abuse & Neglect, 85, 174–179. 10.1016/j.chiabu.2017.07.016 [DOI] [PubMed] [Google Scholar]
- Finkelhor D, Shattuck A, Turner H, & Hamby S (2015). A revised inventory of adverse childhood experiences. Child Abuse & Neglect, 48, 13–21. 10.1016/j.chiabu.2015.07.011 [DOI] [PubMed] [Google Scholar]
- Forster M, Gower AL, Borowsky IW, & McMorris BJ (2017). Associations between adverse childhood experiences, student-teacher relationships, and non-medical use of prescription medications among adolescents. Addictive Behaviors, 68, 30–34. 10.1016/j.addbeh.2017.01.004 [DOI] [PubMed] [Google Scholar]
- Goodman R (1997). The Strengths and Difficulties Questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586. 10.1111/j.1469-7610.1997.tb01545.x [DOI] [PubMed] [Google Scholar]
- Gunnar MR, Wewerka S, Frenn K, Long JD, & Griggs C (2009). Developmental changes in hypothalamus–pituitary–adrenal activity over the transition to adolescence. Development and Psychopathology, 21(1), 69–85. 10.1017/S0954579409000054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hair NL, Hanson JL, Wolfe BL, & Pollak SD (2015). Association of child poverty, brain development, and academic achievement. JAMA Pediatrics, 169(9), 822–829. 10.1001/jamapediatrics.2015.1475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hardt J, & Rutter M (2004). Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry, 45(2), 260–273. 10.1111/j.1469-7610.2004.00218.x [DOI] [PubMed] [Google Scholar]
- Harter S (1982). The perceived competence scale for children. Child Development, 53(1), 87–97. https://www.jstor.org/stable/1129640 [PubMed] [Google Scholar]
- Henry KL, & Muthén B (2010). Multilevel latent class analysis: An application of adolescent smoking typologies with individual and contextual predictors. Structural Equation Modeling, 17(2), 193–215. 10.1080/10705511003659342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hessler DM, & Katz LF (2010). Brief report: Associations between emotional competence and adolescent risky behavior. Journal of Adolescence, 33(1), 241–246. 10.1016/j.adolescence.2009.04.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herrenkohl TI, & Herrenkohl RC (2007). Examining the overlap and prediction of multiple forms of child maltreatment, stressors, and socioeconomic status: A longitudinal analysis of youth outcomes. Journal of Family Violence, 22(7), 553–562. 10.1007/s10896-007-9107-x [DOI] [Google Scholar]
- Hughes K, Bellis MA, Hardcastle KA, Sethi D, Butchart A, Mikton C, Jones L, & Dunne MP (2017). The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. The Lancet Public Health, 2(8), e356–e366. 10.1016/S2468-2667(17)30118-4 [DOI] [PubMed] [Google Scholar]
- Jones DE, Greenberg M, & Crowley M (2015). Early social-emotional functioning and public health: The relationship between kindergarten social competence and future wellness. American Journal of Public Health, 105(11), 2283–2290. 10.2105/AJPH.2015.302630 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kingery JN, Erdley CA, & Marshall KC (2011). Peer acceptance and friendship as predictors of early adolescents’ adjustment across the middle school transition. Merrill-Palmer Quarterly, 57(3), 215–243. https://www.jstor.org/stable/23098045 [Google Scholar]
- LaGreca A, & Stone WL, (1993). Social anxiety scale for children – revised: Factor structure and concurrent validity. Journal of Clinical Child Psychology, 22(1), 17–27. 10.1207/s15374424jccp2201_2 [DOI] [Google Scholar]
- Lee A, & Hankin BL (2009). Insecure attachment, dysfunctional attitudes, and low self-esteem predicting prospective symptoms of depression and anxiety during adolescence. Journal of Clinical Child & Adolescent Psychology, 38(2), 219–231. 10.1080/15374410802698396 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luthar SS, Cicchetti D, & Becker B (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71(3), 543–562. 10.1111/1467-8624.00164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masten AS (2016). Resilience in developing systems: The promise of integrated approaches. European Journal of Developmental Psychology, 13(3), 297–312. 10.1080/17405629.2016.1147344 [DOI] [Google Scholar]
- Maynard BR, Vaughn MG, Nelson EJ, Salas-Wright CP, Heyne DA, & Kremer KP (2017). Truancy in the United States: Examining temporal trends and correlates by race, age, and gender. Children and Youth Services Review, 81, 188–196. 10.1016/j.childyouth.2017.08.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCarthy G, & Maughan B (2010). Negative childhood experiences and adult love relationships: The role of internal working models of attachment. Attachment & Human Development, 12(5), 445–461. 10.1080/14616734.2010.501968 [DOI] [PubMed] [Google Scholar]
- McClelland MM, Tominey SL, Schmitt SA, & Duncan R (2017). SEL interventions in early childhood. Future of Children, 27(1), 33–47. https://www.jstor.org/stable/44219020 [Google Scholar]
- McElroy S, & Hevey D (2014). Relationship between adverse early experiences, stressors, psychosocial resources and wellbeing. Child Abuse & Neglect, 38, 65–75. 10.1016/j.chiabu.2013.07.017 [DOI] [PubMed] [Google Scholar]
- McEwen CA, & McEwen BS (2017). Social structure, adversity, toxic stress, and intergenerational poverty: An early childhood model. Annual Review of Sociology, 43, 445–472. 10.1146/annurev-soc-060116-053252 [DOI] [Google Scholar]
- Mersky JP, Janczewski CE, & Topitzes J (2017). Rethinking the measurement of adversity: Moving toward second-generation research on adverse childhood experiences. Child Maltreatment, 22(1), 58–68. https://doi.org/10.1177%2F1077559516679513 [DOI] [PubMed] [Google Scholar]
- Muthén LK and Muthén BO (1998–2017). Mplus User’s Guide. Eighth Edition. Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Niles MD, Reynolds AJ, & Roe-Sepowitz D (2008). Early childhood intervention and early adolescent social and emotional competence: Second-generation evaluation evidence from the Chicago Longitudinal Study. Educational Research, 50(1), 55–73. 10.1080/00131880801920395 [DOI] [Google Scholar]
- Parker JG, & Asher SR (1993). Friendship and friendship quality in middle childhood: Links with peer group acceptance and feelings of loneliness and social dissatisfaction. Developmental Psychology, 29(4), 611–621. https://psycnet.apa.org/doi/10.1037/0012-1649.29.4.611 [Google Scholar]
- Pate CM, Maras MA, Whitney SD, & Bradshaw CP (2017). Exploring psychosocial mechanisms and interactions: Links between adolescent emotional distress, school connectedness, and educational achievement. School Mental Health, 9(1), 28–43. 10.1007/s12310-016-9202-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patten SB, Wilkes TCR, Williams JVA, Lavorato DH, El-Guebaly N, Schopflocher D, Wild C, Coleman I, & Bulloch AGM (2015). Retrospective and prospectively assessed childhood adversity in association with major depression, alcohol consumption and painful conditions. Epidemiology and Psychiatric Sciences, 24(2), 158–165. 10.1017/S2045796014000018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petruccelli K, Davis J, & Berman T (2019). Adverse childhood experiences and associated health outcomes: A systematic review and meta-analysis. Child Abuse & Neglect, 97, 104127. 10.1016/j.chiabu.2019.104127 [DOI] [PubMed] [Google Scholar]
- R Core Team (2017). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/. [Google Scholar]
- Ramsook KA, Welsh JA, & Bierman KL (2020). Not just what you say, but also how you say it: Preschoolers’ growth in vocabulary and communication skills differentially predict kindergarten academic achievement and self-regulation. Social Development, 29(3), 783–800. 10.1111/sode.12425 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rescorla LA, Ginzburg S, Achenbach TM, Ivanova MY, Almqvist F, Begovac I, Bilenberg N, Bird H, Chahed M, Dobrean A, Döpfner M, Erol N, Hannesdottir H, Kanbayashi Y, Lambert MC, Leung PWL, Minaei A, Novik TS, Oh K, … Döpfner M (2013). Cross-informant agreement between parent-reported and adolescent self-reported problems in 25 societies. Journal of Clinical Child & Adolescent Psychology, 42(2), 262–273. 10.1080/15374416.2012.717870 [DOI] [PubMed] [Google Scholar]
- Reuben A, Moffitt TE, Caspi A, Belsky DW, Harrington H, Schroeder F, Hogan S, Ramrakha S, Poulton R, & Danese A (2016). Lest we forget: Comparing retrospective and prospective assessments of adverse childhood experiences in the prediction of adult health. Journal of Child Psychology and Psychiatry, 57(10), 1103–1112. 10.1111/jcpp.12621 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ridenour TA, Greenberg MT, & Cook ET (2006). Structure and validity of people in my life: A self-report measure of attachment in late childhood. Journal of Youth and Adolescence, 35(6), 1037–1053. 10.1007/s10964-006-9070-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rizopoulos D (2006). ltm: An R package for latent variable modelling and item response theory analyses. Journal of Statistical Software, 17(5), 1–25. http://www.jstatsoft.org/v17/i05/ [Google Scholar]
- Roesch SC, Villodas M, & Villodas F (2010). Latent class/profile analysis in maltreatment research: A commentary on Nooner et al., Pears et al., and looking beyond. Child Abuse & Neglect, 34(3), 155. 10.1016/j.chiabu.2010.01.003 [DOI] [PubMed] [Google Scholar]
- Schalinski I, Teicher MH, Nischk D, Hinderer E, Müller O, & Rockstroh B (2016). Type and timing of adverse childhood experiences differentially affect severity of PTSD, dissociative and depressive symptoms in adult inpatients. BMC Psychiatry, 16, 1–15. 10.1186/s12888-016-1004-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaefer HL, Collyer S, Duncan G, Edin K, Garfinkel I, Harris D, Smeeding TM, Waldfogel J, Wimer C, & Yoshikawa H (2018). A universal child allowance: A plan to reduce poverty and income instability among children in the United States. RSF: The Russell Sage Foundation Journal of the Social Sciences, 4(2), 22–42. 10.7758/RSF.2018.4.2.02 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheffler JL, Stanley I, & Sachs-Ericsson N (2020). ACEs and mental health outcomes. In Asmundson GJ & Afifi TO (Eds.), Adverse childhood experiences (pp. 47–69). Academic Press. [Google Scholar]
- Simmons RG, & Blythe DA (2017). Moving into adolescence: The impact of pubertal change and school context. Routledge. [Google Scholar]
- Sroufe LA, & Waters E (1977). Attachment as an organizational construct. Child Development, 48(4), 1184–1199. https://www.jstor.org/stable/1128475 [Google Scholar]
- Steele H, Bate J, Steele M, Dube SR, Danskin K, Knafo H, Nikitiades A, Bonuck K, Meissner P, & Murphy A (2016). Adverse childhood experiences, poverty, and parenting stress. Canadian Journal of Behavioural Science, 48(1), 32–38. 10.1037/cbs0000034 [DOI] [Google Scholar]
- Van Eck K, Johnson SR, Bettencourt A, & Johnson SL (2017). How school climate relates to chronic absence: A multi–level latent profile analysis. Journal of School Psychology, 61, 89–102. 10.1016/j.jsp.2016.10.001 [DOI] [PubMed] [Google Scholar]
- Von Cheong E, Sinnott C, Dahly D, & Kearney PM (2017). Adverse childhood experiences (ACEs) and later-life depression: Perceived social support as a potential protective factor. BMJ Open, 7(9), e013228. 10.1136/bmjopen-2016-013228 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang MT, & Peck SC (2013). Adolescent educational success and mental health vary across school engagement profiles. Developmental Psychology, 49(7), 1266. 10.1037/a0030028 [DOI] [PubMed] [Google Scholar]
- Wasik BA, Bond MA, & Hindman A (2006). The effects of a language and literacy intervention on Head Start children and teachers. Journal of Educational Psychology, 98(1), 63–74. 10.1037/0022-0663.98.1.63 [DOI] [Google Scholar]
- Watson D, Clark LA, & Tellegen A (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54(6), 1063–1070. [DOI] [PubMed] [Google Scholar]
- Weiland C, & Yoshikawa H (2012). The effects of large-scale economic change and policies on children’s developmental contexts and developmental outcomes. Child Development Perspectives, 6(4), 342–350. 10.1111/j.1750-8606.2011.00222.x [DOI] [Google Scholar]
- Welsh JA, Bierman KL, Nix RL, & Heinrichs BN (2020). Sustained effects of a school readiness intervention: 5th grade outcomes of the Head Start REDI program. Early Childhood Research Quarterly, 53, 151–160. 10.1016/j.ecresq.2020.03.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.