

Abstract
To date, treatment of atrophic acne scars remains a therapeutic challenge for dermatologists, yet there is no standard option on the most effective treatment. Microneedling (MN) is a minimally invasive technology that involves repetitive skin puncture using sterile microneedles to disrupt dermal collagen that connects the scar tissue. Recent studies have demonstrated the potency of MN, such as dermaroller and fractionated microneedle radiofrequency, in the treatment of atrophic scars. The objective of this review is to evaluate systematically the current literature on MN for atrophic acne scars. A systematic search of literature was performed from PubMed, Medline, Cochrane Central, and Google Scholar databases for articles published during the last 20 years. Only randomised controlled trials (RCTs) with full‐text version of the manuscript available were included in our study. Nine RCTs were included in this review. All treatment modalities demonstrated consistent results that MN was efficacious in treating atrophic acne scars as a monotherapy or in combination with other treatments. Moreover, no serious adverse effects were reported in all studies after MN treatment. MN is a well‐tolerated and effective therapeutic modality in treating atrophic acne scars. Further research is required to validate the efficacy of MN with a larger sample size and lengthy follow‐up.
Keywords: atrophic acne scar, microneedling
1. INTRODUCTION
Every year there are more than 100 million patients who develop scar formation caused by various factors, such as post‐inflammatory acne and trauma. Patients with scar tissues often have physical, aesthetic, psychological, and social barriers.1 Scar tissue is naturally a protective mechanism as a consequence of tissue damage.2 Repair in skin tissue produces a spectrum of scar tissue types such as atrophic, hypertrophic, and keloid scars.1, 3 Atrophic scars are dermal depressions, which are commonly caused by the destruction of collagen following inflammatory acne.4 This permanent disfiguring sequelae correlates with the duration of acne, severity of lesion, and delay in therapy.5
To date, treatment of atrophic acne scars remains a therapeutic challenge for dermatologist, yet there is no standard option on the most effective treatment.6, 7 A range of possible options has been investigated including surgical techniques (subcision, punch graft), non‐ablative laser treatment, resurfacing techniques (ablative laser treatment, dermabrasion), and injection or dermal fillers.8, 9, 10
In recent years, microneedling (MN) therapy has been widely used as a treatment for various dermatological conditions, including scar tissue.11 Microneedling, also known as percutaneous collagen induction (PCI) or collagen induction therapy, is a minimally invasive technology used for several dermatological conditions. This technique involves repetitive skin puncture using sterile microneedles to disrupt dermal collagen that connects the scar tissue. The needle will penetrate the stratum corneum and generate small holes known as micro‐conduits with minimal damage to the epidermis. This process will provoke the regeneration of growth factors to stimulate collagen and elastin production in the lining of dermal blood vessels.12, 13 MN can be applied using a range of devices such as manual MN, motorised MN, and radiofrequency coupled.14 The use of MN has been used in the treatment of acne vulgaris, scar tissue, facial rejuvenation, abnormal pigmentation, alopecia, and transdermal drug delivery (TDD).15, 16, 17 The benefits of MN as acne scarring treatment was first described by Camirand and Doucet that used a tattoo gun to abrade atrophic scars.18 Since then, many studies have investigated the efficacy and safety of MN as monotherapy or in combination with other treatments in treating atrophic scars. Therefore, this article will evaluate systematically the current literature on MN for atrophic acne scars.
2. METHODS
Our methodology and reporting were performed following the Preferred Reporting Items for Systematic Reviews and Meta‐analyses (PRISMA). A systematic search of literature was performed on 8 October 2020 from PubMed, Medline, Cochrane Central, and Google Scholar databases for articles published during the last 20 years, since 1 January 2000 until 8 October 2020. Only articles written in English were included. The MeSH search included (“Microneedling” OR “Micro Needle” OR “Skin Needling” OR “Percutaneous Collagen Induction” OR “PCI” OR “Dermaroller” OR “Dermal Needling” OR “Dermal Rolling” OR “Collagen Induction Therapy”) AND (“Acne Scar” OR “ Atrophic Acne Scar” OR “Atrophic Scar”).
Duplicates of articles obtained from the three databases were initially removed. Then, titles and abstracts of articles were reviewed for eligibility by JS. Any articles irrelevant to our study, based on titles and abstracts were excluded. Then, the full texts of selected articles were independently reviewed by IBSS and SAPS. Only randomised controlled trials (RCTs) with full‐text version of the manuscript available were included in our study. For participants, we included adult patients (above 18 years old), male, and female from any ethnic group with atrophic acne scars confirmed by dermatologists. Moreover, with regard to intervention, we accepted MN in any type of form including as monotherapy, combined with topical or with radiofrequency. If an article studied MN in combination with other therapy without explaining the additional benefit of MN compared with the control group, this study was not included. MN should be clearly stated as a determining variable in the study. Any overlapping data sets were described in different publications, the study with a larger population was included. Disagreements between reviewers were resolved through discussion to reach a consensus.
One reviewer (IBSS) independently extracted and synthesised methodological and outcome data and are summarised in Table 1. The extracted data were as followed: publication details, study design, intervention details, duration of treatment, number of participants lost to follow‐up, duration of follow‐up, evaluation of the treatment, and documented side effects. Meanwhile, extracted data regarding outcomes were clinical improvement reported by patient and observer. The primary outcome was repair of scar tissue assessed by physicians according to the validated scale used in the trials. Secondary data were the improvement assessed by patients themselves and adverse events associated with the intervention. The results from the table were then reviewed by another reviewer (SAPS). All RCTs were investigated for their use of randomisation, blinding, and full outcome. Since blinding of assessors and patients for procedure of MN is impossible, a performance bias is inevitable. Moreover, attrition bias was reviewed using the exclusion criteria and withdrawal.
TABLE 1.
Summary of articles
| No | Author | Year | Study design | Patients | Dropouts | Intervention | Comparison | Duration of treatment | Follow‐up | Evaluation of the treatment | Adverse events |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Alam et al | 2014 | Single centre, rater‐blinded, split‐face, placebo‐controlled, parallel group RCT | 20 | 5 | Microneedling (MN) (MTS Roller, roller depth 1‐2 mm) | Placebo | 5 weeks | 3 and 6 months after first treatment | After 3 needling treatments, there was improvement in the appearance of acne scars over time compared with the control group | No adverse events were reported, only mild transient erythema and oedema |
| 2 | Rana et al | 2017 | Single‐blinded RCT | 60 | 8 | MN with dermaroller (8‐line 1.5 mm) along with 70% GA peeling | MN with dermaroller (8‐line 1.5 mm) | 12–15 weeks | At baseline and after 22 weeks | Addition of sequential 70% glycolic acid peel to MN gives better scar improvement compared with MN alone | No report |
| 3 | Chae et al | 2014 | Single‐blinded RCT | 40 | 0 | 1550 nm Er:Glass fractional laser | Fractional microneedle radiofrequency (2 mm depth) | 12 weeks | After 4, 8, 12, and 20 weeks | Atrophic acne scars improved in both groups |
Both: pain, erythema, oedema, dryness, acne vulgaris Fractional laser: greater pain, post inflammatory hyperpigmentation (PIH) Fractional radiofrequency: fewer adverse events and shorter downtime |
| 4 | Osman et al | 2016 | Single‐blinded, split‐face RCT | 30 | 0 | Fractional ablative 2940‐nm Er:YAG laser (Fotona Xs Dynamics) | Automated MN device (Derma stamp electric pen, Auto‐Stamp Motorised Meso Machine) (2 mm depth) | 5 months | 3 months after final treatment | Both treatment modalities are effective and safe in the treatment of atrophic acne scars, with a significantly higher scar response to the fractional Er:YAG laser treatment |
MN: Shorter duration of moderate erythema and oedema, greater pain Er:YAG: mild PIH |
| 5 | Faghihi et al. | 2017 | Single‐blinded, split‐face RCT | 25 | 0 | Fractionated microneedle radiofrequency (1.5–3.5 mm depth) | Fractionated microneedle radiofrequency (1.5–3.5 mm depth) + standard subcision by Nokor needle | 10 weeks | 3 months after final treatment | The combination of subcision and fractionated MN radiofrequency is a safe and effective modality for acne scars | Both: transient, mild side effects, such as pinpoint bleeding and immediate erythema that lasted for a few days |
| 6 | Afra et al. | 2018 | Observer‐blinded, split‐face, RCT | 36 | 2 | Tazarotene gel 0.1% once daily | MN with a standard dermaroller (192 needles, length 1.5 mm) once per month for 4 months | 3 months | After 3 and 6 months | The trial showed comparable outcomes of both treatments for the overall improvement of quantitative facial acne scar severity |
MN: pain, erythema, PIH (2 patients) Tazarotene: dryness and scaling |
| 7 | Leheta et al | 2011 | Single‐blinded RCT | 30 | 3 | MN (Dermaroller MF 8) (1.5 mm depth) | 100% TCA CROSS | 16 weeks | Every 4 weeks until 4 weeks after final treatment | Microneedling and 100% TCA CROSS were effective in the treatment of atrophic acne scars |
Microneedling: greater pain TCA: longer downtime and PIH |
| 8 | An et al | 2019 | Single‐blinded, split‐face RCT | 40 | 4 | Topical poly‐lactic acid + microneedle fractional radiofrequency (0.8–1.5 mm depth) | Microneedle fractional radiofrequency (0.8–1.5 mm depth) | 12–18 weeks | Every visit and 4–6 weeks after final treatment | Combination therapy resulted in significantly better clinical outcomes, including better scarsmoothness and smaller scar size | Both: erythema, pain, and oedema |
| 9 | Ali et al. | 2019 | RCT | 60 | 0 |
Group II: Jessner's solution (salicylic acid, 14 g; resorcinol, 14 g; lactic acid [85%], 14 g; and ethanol to 100 mL) Group III: MN + Jessner's solution |
Group I: Microneedling (Oster Dermapen Microneedle Therapy) (2,5 mm depth) | 4 months | At final treatment, and 3 months after final treatment | The combined technique (Dermapen and Jessner's solution peeling) showed the best clinical improvement with the least number of sessions |
Both: mild pain and erythema Jessner's solution: exfoliation |
3. RESULTS
Figure 1 shows a flow chart of how the studies were selected. The search results on PubMed, Medline, Google Scholar, and Cochrane Central yielded a total of 212 articles with 4 additional articles obtained from identification through references. Of those, 50 were duplicates and 122 were excluded based on screening of titles and abstracts. Then, 35 articles did not meet our exclusion and inclusion criteria and thus were excluded. Consequently, 9 studies proceeded to critical appraisal performed independently by IBSS and SAPS and yielded 9 studies eligible for review.
FIGURE 1.
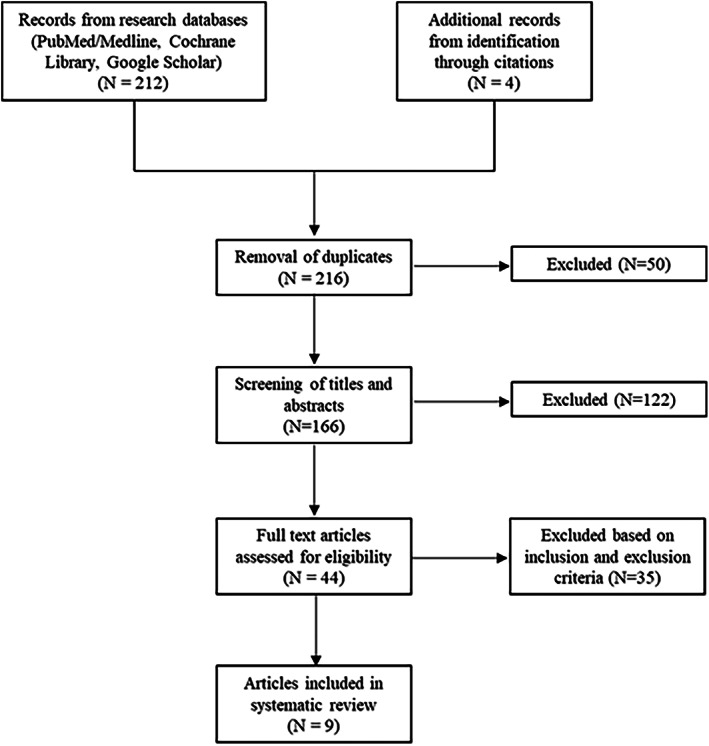
Flow diagram
3.1. Treatment protocol
Nine RCTs were included in this review. Sample sizes varied from 20 to 60 with a total of 341 participants, and 22 dropouts were reported. MN was investigated as monotherapy in six studies and in conjugation with radiofrequency in three studies. The therapeutic effects of MN were compared with those of 100% TCA CROSS, Jessner's solution peeling, 1550 nm Er:Glass fractional laser, fractional erbium‐doped yttrium aluminium garnet (Er:YAG) laser, and MN in combination with 70% glycolic acid peel and subcision. Furthermore, with regard to treatment protocol, the needle length used in the studies ranged from 0.8 mm to 3.5 mm (mean: 1.5 mm). Duration of treatment varied from 5 weeks up to 5 months while the follow‐up time after treatment ranged from 18 weeks to 8 months. All methodological data are synthesised in Table 1.
3.2. Measurement of efficacy
The clinical improvement after intervention was investigated by both observer and patient. All subjective evaluations by the investigators were objectified into categorical quantification through the use of scales. Most of the studies used the Goodman and Baron Qualitative and Quantitative grading system, followed by the échelle d'évaluation clinique des cicatrices d'acné (ECCA) scale, and the physician quartile grading scale. The Goodman and Baron qualitative system classifies lesions into four stages based on their morphology and visibility.19 Meanwhile, the Goodman and Baron quantitative scale evaluates scars by using a specific point score based on the types and frequencies of the lesion observed.20 Moreover, patient satisfaction was mostly assessed using the visual analogue scale (VAS).
3.3. Scar reduction
All treatment modalities demonstrated consistent results that MN was efficacious in treating atrophic acne scars. Monotherapy with MN showed improvement in the appearance of acne scars as early as three treatment sessions.21 A randomised clinical trial comparing tazarotene 0.1% vs MN alone found comparable results based on The Goodman and Baron quantitative and qualitative scale.22 Another clinical trial investigating MN alone compared with TCA CROSS 100% and Jessner's solution also showed improvement in atrophic scars but no statistical significance between groups.23 However, a prospective split‐face study using the 4‐point scale reported that Er:YAG laser performed higher scar response than MN, although MN was found to be effective as well.24 Compared to another laser therapy, as a fractionated microneedle radiofrequency, a study showed that both 1550 nm Er: Glass fractional laser and fractionated microneedle were comparable based on the ECCA grading scale.25 Moreover, MN in combination with 70% glycolic acid peel showed better improvement than MN therapy alone.26 A prospective study also found MN and Jessner's solution dual therapy was superior compared to monotherapy.27 As a fractionated microneedle radiofrequency, additional topical lactic acid resulted in better efficacy for scar smoothness and smaller scar size than monotherapy.28
3.4. Patients satisfaction
All studies found that patient satisfaction was good for MN regardless of the methods used, which include dermarollers and MN fractionated radiofrequency. Compared with tazarotene 0.1%, MN showed slightly better patients satisfaction.22 In addition, one study demonstrated that the percentage of patients who reported improvement was greater in the fractional radiofrequency group compared with 1550 nm Er:Glass fractional laser group.25 Two studies also found that patient satisfaction was higher when MN was performed as dual therapy, such as the combination of fractionated MN radiofrequency as well as when combined with polylactic acid.28, 29 Other combination therapies with better patient satisfaction than MN therapy alone were Jessner's solution and 70% glycolic acid.26, 27
3.5. Adverse events
No serious adverse effects were reported in all studies after MN treatment. However, mild adverse events such as pain, erythema, and oedema might occur after MN treatment. MN had fewer adverse events and shorter downtime compared with 1550 nm Er:Glass fractional laser, Er:YAG laser, and 100% TCA CROSS.23, 24, 25 By contrast, pain was reported greater in MN group compared with most other modalities.
4. DISCUSSION
Scar is a common dermatological problem related to considerable psychological distress.30 Atrophic acne scar is the most common scar among others which usually occurs subsequently after resolution of deep inflammatory facial acne.31 It is a permanent disfigurement that sometimes requires therapy from different modalities. It arises from disorganised production and deposition of collagen in the dermis resulting in visibly depressed scars. The major types of atrophic scars are boxcar, ice pick, and rolling scars.25, 32, 33 To date, with various patterns and profiles, there is no uniform treatment for acne scar.3, 31, 34 Before selecting the appropriate treatment, several variables such as type of scar, duration of scar, skin type, age, and cost should be taken into account. MN, which is a non‐ablative and simple technique, has been the subject of many clinical studies to investigate its potency in treating atrophic scar.26 MN creates micropuncture which produces a controlled skin injury without interfering epidermis. These microinjuries will trigger a wound healing cascade, thus releasing various growth factors. The end product of this modality results in increased dermal elastin and collagen, collagen remodelling, and thickening of epidermis and dermis.35
All reviewed articles suggest that MN improves the appearance of scars. However, a noticeable difference in treatment regimen was observed in all of our selected articles. MN was performed between 3 and 8 times with intervals ranging from 2 to 4 weeks. Although there is no standard protocol available, but Singh et al in his review article found that a minimum of 4–6 sessions are required for a significant improvement.35 Moreover, diversity in needle lengths used is also a crucial component that will impact the results. In this review, we observed 0.8–3.55 mm (mostly 1.5 mm) depth was used in the studies. Majid et al stated that for treating acne scars, a needle length of 1.5–2 mm is usually used. However, it also depends on the thickness of the epidermis and dermis layers.36 Another striking difference observed in this literature review was in terms of duration of follow‐up, which varied from 5 weeks to 5 months. By contrast, Fabbrocini et al reported that the most optimal result may take 8–12 months following treatment since the deposition of new collagen progresses slowly.20 Therefore, studies with longer follow‐up time will reflect more accurate effects of MN.
Based on our literature findings, MN was investigated in many different settings. Compared with 100% TCA CROSS, tazarotene 0.1%, and 1550 nm Er:Glass fractional laser, MN performed comparable results to these therapies.22, 23, 25 However, Er:YAG laser was reported to have greater clinical improvement of acne scar appearance as assessed by 4‐point scale.24 This ablative fractional laser creates multiple columns of thermally injured skin, leading to increased expression of heat shock protein that triggers upregulation of growth factor thus promoting collagen synthesis.37 It exhibits the degree of vaporisation and coagulated tissue of the surrounding zone. The difference in the heat‐producing energy was suggested to be the advantage of Er:YAG laser over MN monotherapy.38 Nevertheless, MN has a shorter duration of total downtime compared with Er:YAG laser. Furthermore, our review also consistently found that MN in combination with other treatments including 70% glycolic acid, Jessner's solution, polylactic acid, and subcision were superior compared with MN alone. Additional peeling agents seem to induce neocollagenesis in synergistic effect with MN, as well as improve any post‐acne hyperpigmentation and post‐inflammatory hyperpigmentation.39, 40 Additional topical agents such as polylactic acid receive benefits from MN as it enhances delivery of drugs across the skin barrier. MN assists drugs bypassing the stratum corneum and delivering drugs directly to the vascular dermis.35 Serano et al also reported the significant widening of follicular infundibulum that may explain the increased drug penetration across the barrier.41 Dual therapy of fractionated microneedle radiofrequency with subcision also leads to additional benefits. Subcision releases scars from the underlying adhesions while MN induces dermal collagen remodelling.42
As atrophic acne scars can be classified into several types, evidence on the effectiveness of MN towards the various types of atrophic scars is inconclusive. Results from the study of MN and glycolic acid showed that maximum improvement was seen in patients with rolling scars, followed by mixed scars, box scars, and the least was in ice pick scars.26 Likewise, studies comparing MN vs 100% TCA CROSS showed greater improvement in the rolling scars group. On the other hand, Woong et al found that reduction of ECCA grading scales was most significant in the box scars group, and likewise, ice pick scars achieved the least reduction result.25 This was also in agreement with findings from Basma et al that box scars showed the best clinical improvement in the MN monotherapy group as well as in combination with peeling agent group.27
Most of the reports indicated MN to be safe and well‐tolerable to all patients.21, 43 Frequently reported adverse effects were erythema, pain, and oedema. Nevertheless, these side effects usually subsided after a few days. Evidence suggests that pain was more dominant in treatment with MN compared with peeling agents and laser treatment. Only Woong et al that reported a contradictory result when comparing fractionated radiofrequency microneedle with 1550 nm Er:Glass fractional laser.25 However, MN was favourable in terms of shorter downtime compared with peeling agents and laser treatment.24, 25 Most of our literatures reported no case of postinflammatory hyperpigmentation (PIH) following MN treatment, in which only two patients had PIH in the study by Afra et al.22 This result was also in agreement with previous reports regarding the absence of PIH in fractionated radiofrequency microneedle group.44, 45, 46 In recent studies, patients with skin phototypes IV and V can have an increased likelihood of PIH, which usually appears after laser treatment.47, 48 However, treatment with MN may reduce the risk of hyperpigmentation through downregulation of melanocyte‐stimulating hormone during the postinflammatory response.49, 50 Overall, patients were satisfied with MN due to its shorter downtime and fewer adverse effects.
This study is not without limitation. Lack of methodological unity of our investigated literature was our main drawback, thus a meta‐analysis could not be carried out. Limited sample size of trials (with the largest study included only a maximum of 60 patients), total sessions of treatments, and duration of follow‐up were another concern in this review. The effects of MN on hypertrophic scars and keloid have not been investigated and thus needs further research. Future investigation is important to validate current evidence by conducting well‐designed RCT with standardised measurement scales and lengthy follow‐up duration.
5. CONCLUSION
MN is a well‐tolerated and effective therapeutic modality in treating atrophic acne scars. Further research is required to validate the efficacy of MN with a larger sample size and lengthy follow‐up in comparison with other modalities and to provide cost‐effective treatment strategies for acne scar management.
CONFLICT OF INTEREST
All authors declare no conflict of interest.
ACKNOWLEDGEMENT
This work was financial supported by the Ministry of Research and Technology of the Republic of Indonesia.
Sitohang IBS, Sirait SAP, Suryanegara J. Microneedling in the treatment of atrophic scars: A systematic review of randomised controlled trials. Int Wound J. 2021;18:577–585. 10.1111/iwj.13559
DATA AVAILABILITY STATEMENT
The data supporting this review are available from the corresponding author.
REFERENCES
- 1.Bayat A, McGrouther DA, Ferguson MW. Skin scarring. BMJ. 2003;326(7380):88‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.El Ayadi A, Jay JW, Prasai A. Current approaches targeting the wound healing phases to attenuate fibrosis and scarring. Int J Mol Sci. 2020;21(3):1‐28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Connolly D, Vu HL, Mariwalla K, Saedi N. Acne scarring‐pathogenesis, evaluation, and treatment options. J Clin Aesthet Dermatol. 2017;10(9):12‐23. [PMC free article] [PubMed] [Google Scholar]
- 4.Holland DB, Jeremy AH. The role of inflammation in the pathogenesis of acne and acne scarring. Semin Cutan Med Surg. 2005;24(2):79‐83. [DOI] [PubMed] [Google Scholar]
- 5.Layton AM, Henderson CA, Cunliffe WJ. A clinical evaluation of acne scarring and its incidence. Clin Exp Dermatol. 1994;19(4):303‐308. [DOI] [PubMed] [Google Scholar]
- 6.Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol. 2001;45(1):109‐117. [DOI] [PubMed] [Google Scholar]
- 7.Goodman GJ. Management of post‐acne scarring. What are the options for treatment? Am J Clin Dermatol. 2000;1(1):3‐17. [DOI] [PubMed] [Google Scholar]
- 8.Alam M, Dover JS, Arndt KA. To ablate or not: a proposal regarding nomenclature. J Am Acad Dermatol. 2011;64(6):1170‐1174. [DOI] [PubMed] [Google Scholar]
- 9.Kim HJ, Kim TG, Kwon YS, Park JM, Lee JH. Comparison of a 1,550 nm erbium: glass fractional laser and a chemical reconstruction of skin scars (CROSS) method in the treatment of acne scars: a simultaneous split‐face trial. Lasers Surg Med. 2009;41(8):545‐549. [DOI] [PubMed] [Google Scholar]
- 10.Monstrey S, Middelkoop E, Vranckx JJ, et al. Updated scar management practical guidelines: non‐invasive and invasive measures. J Plast Reconstr Aesthet Surg. 2014;67(8):1017‐1025. [DOI] [PubMed] [Google Scholar]
- 11.Alster TS, Li MKY. Microneedling of scars: a large prospective study with long‐term follow‐up. Plast Reconstr Surg. 2020;145(2):358‐364. [DOI] [PubMed] [Google Scholar]
- 12.Lee KC, Bamford A, Gardiner F, et al. Investigating the intra‐ and inter‐rater reliability of a panel of subjective and objective burn scar measurement tools. Burns. 2019;45(6):1311‐1324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kuehlmann B, Stern‐Buchbinder Z, Wan DC, Friedstat JS, Gurtner GC. Beneath the surface: a review of laser remodeling of hypertrophic scars and burns. Adv Wound Care (New Rochelle). 2019;8(4):168‐176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Alster TS, Graham PM. Microneedling: a review and practical guide. Dermatol Surg. 2018;44(3):397‐404. [DOI] [PubMed] [Google Scholar]
- 15.Lee KC, Dretzke J, Grover L, Logan A, Moiemen N. A systematic review of objective burn scar measurements. Burns Trauma. 2016;4:14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hou A, Cohen B, Haimovic A, Elbuluk N. Microneedling: a comprehensive review. Dermatol Surg. 2017;43(3):321‐339. [DOI] [PubMed] [Google Scholar]
- 17.Iosifidis C, Goutos I. Percutaneous collagen induction (microneedling) for the management of non‐atrophic scars: literature review. Scars Burn Heal. 2019;5:2059513119880301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Camirand A, Doucet J. Needle dermabrasion. Aesthetic Plast Surg. 1997;21(1):48‐51. [DOI] [PubMed] [Google Scholar]
- 19.Goodman GJ, Baron JA. Postacne scarring: a qualitative global scarring grading system. Dermatol Surg. 2006;32(12):1458‐1466. [DOI] [PubMed] [Google Scholar]
- 20.Fabbrocini G, Annunziata MC, D'Arco V, et al. Acne scars: pathogenesis, classification and treatment. Dermatol Res Pract. 2010;2010:893080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Alam M, Han S, Pongprutthipan M, et al. Efficacy of a needling device for the treatment of acne scars: a randomized clinical trial. JAMA Dermatol. 2014;150(8):844‐849. [DOI] [PubMed] [Google Scholar]
- 22.Afra TP, Razmi TM, Narang T, Dogra S, Kumar A. Topical Tazarotene gel, 0.1%, as a novel treatment approach for atrophic postacne scars: a randomized active‐controlled clinical trial. JAMA Facial Plast Surg. 2019;21(2):125‐132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Leheta T, El Tawdy A, Abdel Hay R, Farid S. Percutaneous collagen induction versus full‐concentration trichloroacetic acid in the treatment of atrophic acne scars. Dermatol Surg. 2011;37(2):207‐216. [DOI] [PubMed] [Google Scholar]
- 24.Osman MA, Shokeir HA, Fawzy MM. Fractional erbium‐doped yttrium aluminum garnet laser versus microneedling in treatment of atrophic acne scars: a randomized split‐face clinical study. Dermatol Surg. 2017;43(Suppl 1):S47‐s56. [DOI] [PubMed] [Google Scholar]
- 25.Chae WS, Seong JY, Jung HN, et al. Comparative study on efficacy and safety of 1550 nm Er:glass fractional laser and fractional radiofrequency microneedle device for facial atrophic acne scar. J Cosmet Dermatol. 2015;14(2):100‐106. [DOI] [PubMed] [Google Scholar]
- 26.Rana S, Mendiratta V, Chander R. Efficacy of microneedling with 70% glycolic acid peel vs microneedling alone in treatment of atrophic acne scars: a randomized controlled trial. J Cosmet Dermatol. 2017;16(4):454‐459. [DOI] [PubMed] [Google Scholar]
- 27.Ali B, ElMahdy N, Elfar NN. Microneedling (Dermapen) and Jessner's solution peeling in treatment of atrophic acne scars: a comparative randomized clinical study. J Cosmet Laser Ther. 2019;21(6):357‐363. [DOI] [PubMed] [Google Scholar]
- 28.An MK, Hong EH, Suh SB, Park EJ, Kim KH. Combination therapy of microneedle fractional radiofrequency and topical poly‐lactic acid for acne scars: a randomized controlled Split‐face study. Dermatol Surg. 2020;46(6):796‐802. [DOI] [PubMed] [Google Scholar]
- 29.Faghihi G, Poostiyan N, Asilian A, et al. Efficacy of fractionated microneedle radiofrequency with and without adding subcision for the treatment of atrophic facial acne scars: a randomized split‐face clinical study. J Cosmet Dermatol. 2017;16(2):223‐229. [DOI] [PubMed] [Google Scholar]
- 30.Behnam B, Taheri R, Ghorbani R, Allameh P. Psychological impairments in the patients with acne. Indian J Dermatol. 2013;58(1):26‐29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kravvas G, Al‐Niaimi F. A systematic review of treatments for acne scarring. Part 1: non‐energy‐based techniques. Scar Burn Heal. 2017;3:2059513117695312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.O'Daniel TG. Multimodal management of atrophic acne scarring in the aging face. Aesthetic Plast Surg. 2011;35(6):1143‐1150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Moon J, Yoon JY, Yang JH, Kwon HH, Min S, Suh DH. Atrophic acne scar: a process from altered metabolism of elastic fibres and collagen fibres based on transforming growth factor‐β1 signalling. Br J Dermatol. 2019;181(6):1226‐1237. [DOI] [PubMed] [Google Scholar]
- 34.Gupta A, Kaur M, Patra S, Khunger N, Gupta S. Evidence‐based surgical management of post‐acne scarring in skin of color. J Cutan Aesthet Surg. 2020;13(2):124‐141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Singh A, Yadav S. Microneedling: advances and widening horizons. Indian Dermatol Online J. 2016;7(4):244‐254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Iriarte C, Awosika O, Rengifo‐Pardo M, Ehrlich A. Review of applications of microneedling in dermatology. Clinical, Cosmetic and Investigational Dermatology. 2017;10:289‐298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Goldberg DJ. Erbium: YAG laser resurfacing: what is its role? Aesthet Surg J. 1998;18(4):255‐260. [DOI] [PubMed] [Google Scholar]
- 38.Hantash BM, Mahmood MB. Fractional photothermolysis: a novel aesthetic laser surgery modality. Dermatol Surg. 2007;33(5):525‐534. [DOI] [PubMed] [Google Scholar]
- 39.Sharad J. Combination of microneedling and glycolic acid peels for the treatment of acne scars in dark skin. J Cosmet Dermatol. 2011;10:317‐323. [DOI] [PubMed] [Google Scholar]
- 40.Saadawi AN, Esawy AM, Kandeel AH, El‐Sayed W. Microneedling by dermapen and glycolic acid peel for the treatment of acne scars: comparative study. J Cosmet Dermatol. 2019;18(1):107‐114. [DOI] [PubMed] [Google Scholar]
- 41.Serrano G, Almudéver P, Serrano JM, et al. Microneedling dilates the follicular infundibulum and increases transfollicular absorption of liposomal sepia melanin. Clin Cosmet Investig Dermatol. 2015;8:313‐318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Garg S, Baveja S. Combination therapy in the management of atrophic acne scars. J Cutan Aesthet Surg. 2014;7(1):18‐23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Safety AG. Effectiveness of an automated microneedling device in improving the signs of aging skin. J Clin Aesthet Dermatol. 2018;11(8):29‐34. [PMC free article] [PubMed] [Google Scholar]
- 44.Hruza G, Taub AF, Collier SL, Mulholland SR. Skin rejuvenation and wrinkle reduction using a fractional radiofrequency system. J Drugs Dermatol. 2009;8(3):259‐265. [PubMed] [Google Scholar]
- 45.Cho SI, Chung BY, Choi MG, et al. Evaluation of the clinical efficacy of fractional radiofrequency microneedle treatment in acne scars and large facial pores. Dermatol Surg. 2012;38(7 Pt 1):1017‐1024. [DOI] [PubMed] [Google Scholar]
- 46.Gold MH, Biron JA. Treatment of acne scars by fractional bipolar radiofrequency energy. J Cosmet Laser Ther. 2012;14(4):172‐178. [DOI] [PubMed] [Google Scholar]
- 47.Ong MW, Bashir SJ. Fractional laser resurfacing for acne scars: a review. Br J Dermatol. 2012;166(6):1160‐1169. [DOI] [PubMed] [Google Scholar]
- 48.Al Qarqaz F, Al‐Yousef A. Skin microneedling for acne scars associated with pigmentation in patients with dark skin. J Cosmet Dermatol. 2018;17(3):390‐395. [DOI] [PubMed] [Google Scholar]
- 49.Aust MC, Reimers K, Repenning C, et al. Percutaneous collagen induction: minimally invasive skin rejuvenation without risk of hyperpigmentation – fact or fiction? Plast Reconstr Surg. 2008;122(5):1553‐1563. [DOI] [PubMed] [Google Scholar]
- 50.Cohen B, Elbuluk N. Microneedling in skin of color:a review of uses and efficacy. J Am Acad Dermatol. 2015;74:348‐355. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data supporting this review are available from the corresponding author.