

Summary
Objectives
COVID-19 pandemic is at the fourth stage of boundless local transmission in Bangladesh. The objective of this study was to assess the psychosocial impact of COVID-19 on adult Bangladeshi population.
Design
Online-based cross-sectional study.
Settings
Data were collected from different parts of the Bangladesh.
Participants
Information was collected from 213 young adults who were aged 18-34 years old using convenient sampling technique.
Results
More than 90% of participants were responded to possess a good awareness of COVID-19. However, the behavioral characteristics of young individuals in Bangladesh were not impressive. In this cohort, 24.4% of participants showed moderate change and 5.2%-little changes in their behavior due to COVID-19. Approximately 58.2% of participants had some symptoms of mental distress while 59.7% of participants were somewhat worried about COVID-19.
Conclusion
In order to control the spread of Covid-19, existing unconsciousness in young adult could turn this situation into a disaster throughout the nation which therefore must be understood by the government and policymakers to incorporate successful measures.
Keywords: Coronavirus, COVID-19, Knowledge, Perception, Behavior
Introduction
World Health Organization (WHO) had declared the outbreak of COVID-19 as a major public health concern after largely expanding across the China and worldwide on 30 January 2020 [1]. On 8 March 2020, Bangladesh found the first coronavirus cases in Dhaka, the capital of Bangladesh [2]. After that, the number of people with positive COVID-19 cases began to spread in this city. Then people get scared and a nationwide lockdown of all educational centers as well as private and government offices had taken place to avoid human transmission from 26 March till 30 May 2020.However, shortly after the lockdown declaration, more than 11 million people started leaving their work place from Dhaka to go into their home districts which further accelerates the risk of COVID-19 in other districts throughout Bangladesh. Observing population density, environmental factors, cultural norms, social structure, and healthcare capacity, it is undoubtedly challenging to install lockdown in Bangladesh [3]. During this novel coronavirus pandemic, humanitarian crises have arisen already into the country, and in most incidents, it will be the combined effects of a variety of shortages that will very likely to culminate in the worst outcomes it’s about USA, not relevant with this paper [4, 5]. The recent scenario of the pandemic in Bangladesh is given in Figure 1 [6].
Fig. 1.
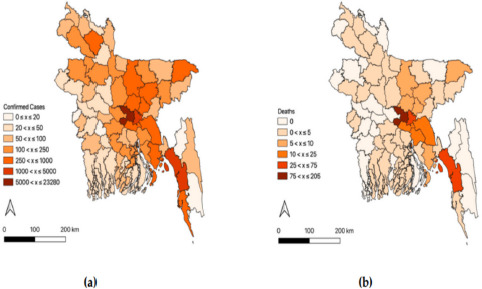
District wise Map of the present situation of COVID-19 pandemic in Bangladesh (May 25, 2020) [6].
Within four months of its outbreak, that is, by June 15, 2020, 11,474,717 people had been infected worldwide, of whom 6,491,306 had recovered and 535,097 had died. Two hundred and thirteen countries and territories have already been affected, while Bangladesh ranked 17th with 102,292 COVID-19 cases based on June 18, 2020 report and thus become one of the most infected countries in the world [7].
In Bangladesh almost 98% of people know about the pandemic, COVID-19 but the knowledge about its transmission and prevention and perception towards COVID-19 is not sufficient and is also correlated with people’s age and profession [8]. In our neighbor country India, it is stated that 43% of people described COVID-19 as a highly contagious disease while only 18.2% regarded fever as a common symptoms of COVID-19. The attitude and anxiety regarding coronavirus among people are much observed [9]. Because of the widespread availability, large genetic variation, and regular recombination, in association with the increased time humans spend in the appearance of animals, coronaviruses may often mutate to infect human hosts. Coronavirus is usually transmitted by airborne droplets into the nasal mucosa and through close touch between individuals, unwashed hands, and infrequently as a result of touching infected surfaces in closed environments [10]. Coronaviruses typically cause enteric and central nervous system (CNS), acute and chronic respiratory diseases in many species of animals including humans. There has also been considerable evidence that human coronaviruses are linked with more severe human diseases, such as multiple sclerosis [11], enteric disease, or hepatitis [12] in infants. In 2004, Ding et al. reported that, the disease may have a death rate of around 10%, but it reached nearly 50% in older people, which is a very high incidence compared to other viral diseases [13]. Governments of all countries in the world are working already to put in place countermeasures to stem potential devastating effects. The present study aimed to assess awareness about coronavirus, behavioral changes, and psychological distress caused by coronavirus in Bangladeshi young adults (18-34 years).
Methods
SURVEY INSTRUMENT AND DISSEMINATION
An online-based cross-sectional survey was performed during the first week of May 2020 and responses were collected from Bangladeshi young adults from different parts of the country. The duration of this study was from May, 2020 to June, 2020. The survey covered the participant’s demographic characteristics, awareness about coronavirus, behavioral changes, and psychological distress caused by coronavirus.
INCLUSION AND EXCLUSION CRITERIA
The study included respondents aged between 18 to 34 years old. Prior to the start of the interview, each individual provided written informed consent through online. There was no on-going vaccination program in Bangladesh during the study period. This research focused mostly on young adults, both male and female. Respondents who had previous history of mental instability or were in rehabilitation due to drug or any other addiction at any time in their life, or respondents, who refused consent or were unable to interact properly during data collection were excluded from the study.
SAMPLING TECHNIQUE AND SAMPLE SIZE
Around 13% of Bangladeshi used the internet in a population of 162 million, where approximately 25% were young adults. A 23-item overview instrument was adopted utilizing WHO course materials on developing respiratory viruses, including COVID-19 [14]. The developed draft study instrument was made available via a link and was transferred to 10 specialists from various geographic regions to comprehensively evaluate the content domains of the questionnaire. As our sampling frame was 18-34 years old young adults who are familiar with the internet and regularly use online social media, at first, we had collected our data through convenient sampling technique for determining sample size, considering around 267 respondents from a pool of 800 to 1,000 young adults as the population size for this study [15]. A pilot online study was then also undertaken to standardize the questionnaire. A variety of data quality methods was implemented in the survey to ensure the validity of responses and to filter out those who did not fulfill the inclusion requirements. The poll was piloted by the research group as a quality control method (n = 10) before appearing online on social networking sites.
Individuals were excluded from the data if:
the participant (n = 14) browsed the online questionnaire but did not finish any of the measures;
the participant (n = 26) did not give complete informed consent;
the participant did not contain the inclusion requirements (i.e., 18-34 years old, n = 14);
the minimum completion speed was increased at 10 minutes, which was half of the sample’s median completion time;
although the data were reviewed for consistency of responses, no responses were eliminated based on this criterion;
there were 213 participants as a result of this;
VARIABLE AND SCORES
For data collection, a structured questionnaire was developed in Bangla from the original version. A pilot survey was conducted online (via Google Forms) to standardize the questionnaire. The pilot survey confirmed the content validity of our questionnaire by both the 10 experts (doctors and psychologist-dealing with patients affecting with COVID-19) and 10 lay persons (literate, aged more than 18 years, not dealing with any COVID-19 patients) [16] and following this pilot research, we modified the questionnaire based on the respondents’ responses to each question and their understanding of the questions we asked during the pilot research to ensure that our tool (questionnaire) is reliable to see the psychosocial impact of study participants. Cronbach’s alpha (α) test was used to determine the questionnaire’s reliability, which was 0.78.
We used Google Forms as a tool for online survey to distribute the survey questionnaire, and participants were given 15 minutes to read, comprehend, and answer all the questions.
Awareness was assessed by questions focusing on COVID-19 transmission, signs, and symptoms, and risk prevention while behavioral characteristics towards COVID-19 were assessed using 9 items. Each response on awareness and behavioral characteristics towards coronavirus (COVID-19) was collected with scores ranging from 0-1 (Tab. I). According to Likert scale, correct responses were scored “1” and incorrect responses were scored “0”. The scoring was categorized based on author’s discretion where, sum of scores below 50th percentile was considered as having poor awareness and behavioral changes and above 75th percentile as good awareness and behavior changes among participants. If the sum of scores ranges from 50 to 75%, moderate level of awareness and behavior changes due to sudden arrival of COVID-19.
Tab. I.
Scoring categories.
| Scores | Category |
|---|---|
| 50% or less | Poor awareness/Poor behavioral characteristics |
| 50-75% | Moderate awareness/Moderate behavioral characteristics |
| 75% or above | Good awareness/Good behavioral characteristics |
STATISTICAL ANALYSIS
The data obtained were coded and analyzed using IBM SPSS version 26.0 (IBM SPSS Statistics Inc, Chicago, IL, USA). The data were analyzed for percentages, mean for continuous variables, standard deviation and, frequency measured for the categorical variables. Chi-square test was employed to assess the degree of correlation between dependent (good, moderate, poor knowledge, respondent’s characteristics (sex, living area) and independent variables (awareness changes, behavioral changes). A chi-square test was performed to determine the strength of correlation of the independent variables with the outcome variable. The level of significance for all statistical tests was set at 0.05.
ETHICAL CONSIDERATION
This work was carried out in compliance with the ethical guidelines of the Declaration of Helsinki. Prior to the survey, the respondents’ permission was taken, and they remained anonymous. Until continuing to fill out the questionnaire, all the participants were told about the specific objective of this study. Participants were only able to complete the survey once and could terminate the survey whenever they wished. Anonymity and confidentiality of the data were ensured. Formal ethical permission of this study was obtained from the respective authority (i.e., Noakhali Science & Technology University, Sonapur, Noakhali, Bangladesh).
Results
OVERVIEW
Table II shows the socio-demographic characteristics of the participants. From a total of 213 young adults, comprising 72% (n = 154) male and 28% (n = 59) female. All participants were between18-34 years of age. The majority of the participants were living in urban settings (n = 130, 61%) and the rest of others were from the rural area (n = 83, 39%). Approximately 74% (n = 158) of the participants in this study were single. Among the respondents, 142 respondents (67%) have undergraduate degree, and most of the participants 94% (n = 201) were Muslims in terms of religion.
Tab. II.
Socio-demographic characteristics of young age populations (n = 213).
| Characteristics | Frequency (%) |
|---|---|
|
Gender Female Male |
59 (28%) 154 (72%) |
|
Living area Urban Rural |
130 (61%) 83 (39%) |
|
Age group (years) 18-24 years 25-29 years 30-34 years |
20 (10%) 158 (74%) 35 (16%) |
|
Education level High school diploma or equivalent Undergraduate Graduate |
35 (16%) 142 (67%) 36 (17%) |
|
Religion Muslim Hindu Christian |
201 (94%) 10 (5%) 2 (1%) |
|
Marital status Single Married |
158 (74%) 55 (26%) |
The data (Tab. III) showed that 91.5% of young adults had good, 8.0% had moderate, while only 0.5% of young adults had poor awareness about COVID-19. Merely 70.4% of young adults had good, 24.4% had moderate, and only 5.2% showed poor behavioral characteristics on COVID-19. Statistically significant differences were observed (P < 0.05) between awareness and behavior characteristics scores among the participants.
Tab. III.
Distribution of frequencies on awareness about Coronavirus and behavioral characteristics changes caused by Coronavirus in Bangladeshi young adults (n = 213).
| Scoring category | Awareness, n (%) | Behavior change, n (%) |
|---|---|---|
| a Good | 195 (91.5%) | 150 (70.4%) |
| a Moderate | 17 (8.0%) | 52 (24.4%) |
| a Poor | 1 (0.5%) | 11 (5.2%) |
N = number of participants. A P-value < 0.05 was considered statistically significant. Scores sharing a common superscript indicates significant differences between awareness and behavior changes.
Box plots (Fig. 2) of the awareness scores (90.61 ± 13.25) showed that youngest adults had a good awareness of COVID-19 while the behavioral characteristics scores (81.32 ± 17.90) had lower than the awareness scores.
Fig. 2.

Box plots showing distribution of scores by awareness, behavioral practices towards COVID-19.
SOURCE OF INFORMATION
When we asked about the reliable sources of information towards COVID-19, the primary sources listed as social media and official websites of the Bangladesh government. Approximately 30.0 percent (n = 63) of participants reported using social media (Facebook, WhatsApp, Twitter, YouTube, Snapchat, Instagram) and news media (TV, newspapers, magazines, and radio) to access information about COVID-19. In addition, approximately 70.4% (n = 150) of the participants often discussed with their family and friends about COVID-19-related topics.
AWARENESS ABOUT COVID-19
More than 91.5% (n = 195) of young adults showed good awareness of COVID-19. The majority of young adults expressed that COVID-19 is transmitted via fecal-oral routes, contact, air (n = 199, 93%).194 individuals (91%) expressed that fever, cough, headache, sore throat, and flu are symptoms of COVID-19 while 198 individuals (93.0%) also expressed that COVID-19 leads to respiratory failure, pneumonia, and death. Additionally, 82% (n = 175) did feel that supportive care is now being used for treating COVID-19, and 93% (n = 199) agreed on covering the nose and mouth while coughing& sneezing, frequent practice of hand hygiene, and avoiding sick contacts can help prevent COVID-19 transmission (Tab. IV).
Tab. IV.
Young adult participants’ knowledge of COVID-19 (n = 213).
| Statement | Yes, n (%) |
No, n (%) |
|---|---|---|
| a COVID-19 is transmitted through air, contact, fecal-oral routes | 199 (93%) | 14 (7%) |
| a Headache, fever, cough, sore throat, and flu are symptoms of aCOVID-19 | 194 (91%) | 19 (9%) |
| COVID-19 leads to pneumonia, respiratory failure, and death | 198 (93%) | 15 (7%) |
| a Supportive care is the current treatment for COVID-19 | 175 (82%) | 38 (18%) |
|
a Hand hygiene, covering nose and mouth while coughing, and avoiding sick contacts can help in the prevention of COVID-19 transmission |
199 (93%) | 14 (7%) |
N = number of participants. A P-value < 0.05 was considered statistically significant. Scores sharing a common superscript indicates significant differences between two responses: Yes and No.
BEHAVIORAL CHARACTERISTICS OF COVID-19
Items related to behavioral characteristics among young adults were assessed using a chi-square test to examine their correlation with sex (Tab. V) and living areas (Tab. VI). Nearly 34.6% (n = 45) of participants from urban settings and 31.2% (n = 48) of the males had gone outside their home for job purposes; the differences among groups were statistically significant (P < 0.05). In addition, 73 participants (56.2%) from urban settings had gone to supermarkets, grocery stores, or pharmacies. 36.2% (n = 47) of participants from urban settings and 32.5% (n = 50) males were found spending leisure times with outsiders and these findings were statistically significant (P < 0.05).
Tab. V.
Correlation between respondents’ characteristics and behavioral changes of coronavirus disease 2019 (COVID-19) (based on gender).
| Question and response | Female, n (%) | Male, n (%) |
|---|---|---|
|
aGone outside home for job purposes Yes No |
4 (7%) 55 (93%) |
48 (31%) 106 (69%) |
|
aGone to supermarkets, grocery stores, or pharmacies Yes No |
11 (19%) 48 (81%) |
73 (47%) 81 (53%) |
|
Gone to restaurants, cafes or shopping centers Yes No |
0 (0.0%) 59 (100%) |
6 (4%) 148 (96%) |
|
aSpent leisure times with outsiders Yes No |
6 (10%) 53 (90%) |
50 (33%) 104 (68%) |
|
Attend public events Yes No |
4 (7%) 55(93) |
21 (14%) 133 (86%) |
|
aUsed public transportation for travel mode use Yes No |
1 (2%) 58 (98%) |
15 (10%) 139 (90%) |
|
Avoid social distancing Yes No |
13 (22%) 46 (78%) |
39 (25%) 115 (75%) |
|
Wash hands with soaps after public gatherings Yes No |
53 (90%) 6 (10%) |
133 (86%) 21 (14%) |
|
Used face masks in outdoor gatherings A little of the time All of the time Most of the time None of the time Some of the time |
2 (3%) 36 (61%) 14 (24%) 4 (7%) 3 (5%) |
6 (4%) 90 (58%) 33 (21%) 9 (6%) 16 (11%) |
Data were collected from 154 male and 59 female adults aged 18 to 34 years throughout Bangladesh. N = number of participants. A P-value < 0.05 was considered statistically significant. Scores sharing a common superscript indicates significant differences between gender.
Tab. VI.
Correlation between respondents’ characteristics and behavioral changes of coronavirus disease 2019 (COVID-19) (based on living area).
| Question and response | Living area | |
|---|---|---|
| Urban, n (%) | Rural, n (%) | |
|
aGone outside home for job purposes Yes No |
45 (35%) 85 (65%) |
7 (8%) 76 (92%) |
|
aGone to supermarkets, grocery stores, or pharmacies Yes No |
73 (56%) 57 (44%) |
11 (13%) 72 (87%) |
|
aGone to restaurants, cafes or shopping centers Yes No |
6 (5%) 124 (95%) |
0 (0.0%) 83 (100%) |
|
aSpent leisure times with outsiders Yes No |
47 (36%) 83 (64%) |
9 (11%) 74 (89%) |
|
aAttendpublic events Yes No |
23 (18%) 107 (82%) |
2 (2%) 81 (98%) |
|
aUsed public transportation for travel mode use Yes No |
14 (11%) 116 (89%) |
2 (2%) 81 (98%) |
|
aAvoided social distancing Yes No |
46 (35%) 84 (65%) |
6 (7%) 77 (93%) |
|
Wash hands with soaps after public gatherings Yes No |
111 (85%) 19 (15%) |
75 (90%) 8 (10%) |
|
Used face masks in outdoor gatherings A little of the time All of the time Most of the time None of the time Some of the time |
5 (4%) 82 (63%) 27 (21%) 3 (2%) 13 (10%) |
3 (4%) 44 (53%) 20 (24%) 10 (12%) 6 (7%) |
Data were collected from 130 urban and 84 rural adults aged 18 to 34 years throughout Bangladesh. N = number of participants. A P-value < 0.05 was considered statistically significant. Scores sharing a common superscript indicates significant differences between living area (urban and rural).
Even 17.7% (n = 23) of participants from urban settings were significantly found to attend public events (p < 0.001). 9.7% (n = 15) of males used public transportation for travel mode use (n = 14, 10.8%), and 25.3% (n = 39) males avoid social distancing where this nature is also common in urban participants (n = 46, 35.4%) (p < 0.05). A large number of participants from urban settings used face masks in outdoor gatherings (n = 82, 63.1%) although the result was not significant (p > 0.05) and 111 individuals (85.4%) have the nature of washing hands with soaps after public gatherings.
CLINICAL SYMPTOMS OF COVID-19 AMONG YOUNG AGE PARTICIPANTS
In our study, 16.9% of participants suffered from headaches, aches and 13.6% had neck pain, and 8.9% had a stuffy or runny nose. Only 2.8, 5.2, and 5.6% of participants respectively suffered from fever, sore throat, and fatigue.
PSYCHOLOGICAL DISTRESS DURING COVID-19
In our study, 42.8% (n = 91) of participants had no feelings of distress about COVID 19. However, 58.2% (n = 122) of participants had some symptoms of mental distress regarding COVID-19. On the other side, 41.3% (n = 88) of participants were not worried about COVID-19 while 59.7% of participants (n = 125) were somewhat worried about COVID-19.
Discussions
Globally, COVID-19 is a subject of debate among the public and in the media, particularly among young age groups. With the mounting transmission of coronavirus disease, an important question arises as to how we are implementing positive health messages in times of pandemic to assist in reducing the spread. In searching for the answer, we were investigating the awareness about Coronavirus, behavioral changes, and psychological distress caused by coronavirus in Bangladeshi young adults (18-34 years). Awareness and behavioral characteristics towards COVID-19 vary across various categories of young age participants. Our study reported that young age participants have satisfactory awareness about COVID-19 but the behavioral changes are not satisfactory as it may fuel spread.
Most participants were living in urban areas. An age-based study based on coronavirus patients found that 20% of the infected cases were found between 21-30 years, followed by 23% between 31-40 years, and 19% between 41-50 years of age [17]. Mainly young age population is at risk group because the median age of Bangladeshis is 27.1 years [18].The outbreak of the COVID-19 disease in the country is rising with days as lack of behavioral characteristics is commonly practiced by its population which in future will surely bring a disaster if the intergenerational households do not take preventive steps right now. This form of transmission of disease probably contributed to the overall illness burden in Bangladesh.
Preventing the transmission of COVID-19 depends mostly on proper health knowledge, hand hygiene practices, adequate staff training, and in particular, appropriate personal behavior. It is recommended that social and physical distancing interventions prevent transmission of coronavirus [6, 7, 13, 14, 19, 20]. Many preventive measures and actions have been taken by canceling or postponing major events such as sports events, festivals, ceremonies, conferences, and other types of public events. Such measures, of course, have the potential to reduce cases and, if successful, will require fewer people to seek health care, thus reducing the burden on the healthcare system [21]. Many measures to incorporate social and physical distance include working from home, online home-based learning for students at school and university, teleconferencing instead of face-to-face meetings have already been taken [22].
Current findings showed that psychological distresses caused by coronavirus in Bangladeshi young adults (18-34 years) were more common. Furthermore, pandemic-related measures such as isolation, social distancing, quarantine, and economic distress can also trigger psychological mediators such as worry, depression, dissatisfaction, anger, anxiety, frustration, nervousness, and loneliness. These are the characteristic features of typical mental health distress that many individuals endured during and after the crisis [23-26]. Finally, as indicated by researches, the role of a psychiatrist during a pandemic like COVID-19 should include: (i) informing people about common adverse psychological effects, (ii) encouraging health-promoting behaviors among individuals, (iii) incorporating available health-care services [22], (iv) promoting problem-solving, (v) inspiring patients, their families, and health-care [24].
The use of proper statistical analysis techniques has strengthened this article with high response rate. Additionally, using well-designed questionnaire controls inter-rated biases. However, this study is not without limitations. Firstly, the study was online-based which may have introduced respondent bias. Secondly, the study was conducted with low sample size and finally, cross-sectional study may limit the use findings for causal inference.
Conclusions
The findings suggest that most of the Bangladeshi youth populations possess good awareness, but their behavioral characteristics towards COVID-19 were not impressive. In addition, awareness and behavioral characteristics are related to demographic features. Mass awareness programs and proper educational strategies would help boost to adopt preferable behavioral characteristics to control disease spread. Effective preventive steps, guidelines, and healthy practices must be enforced by different government agencies while the assistance of professional organizations and academic institutions is also necessary. Additionally, citizens must need to comply with the WHO guidelines. The results of this research would be very useful to public health decision-makers and health professionals. Hoping that with the joint efforts of people and the Bangladesh Government, the country will win the fight against the COVID-19 pandemic unquestionably.
Figures and tables
Acknowledgements
Funding sources: this research did not receive any spe-cific grant from funding agencies in the public, commer-cial, or not-for-profit sectors.
Footnotes
Ethical approval
The ethical approval for this study was taken from Ethics board of Noakhali Science and Technology University.
Conflict of interest statement
The authors declare no conflict of interest.
Authors’ contributions
MAH has designed the study and contributed on the data collection, data analysis, interpretation and the manuscript writing. RJR has contributed on data collection. TR and AIC have contributed on data analysis, interpretation and manuscript writing as well. MAZ has critically review the manuscript and made final version of paper as well.
References
- [1].Habib MA. General overview of coronavirus disease 2019 (COVID-19): a summary of evidence. Asian J Immunol 2020:24-33. [Google Scholar]
- [2].Coronavirus COVID-19 Dashboard, 2020. http://103.247.238.81/webportal/pages/covid19.php?fbclid=IwAR0fvp1tINehCpQfHn8c6lCqwqMmjNncdLdhNqYLIsMAhaSxD2nM4Jd043Y [Google Scholar]
- [3].Bodrud-Doza M, Shammi M, Bahlman L, Islam ARM, Rahman M. Psychosocial and socio-economic crisis in Bangladesh due to COVID-19 pandemic: a perception-based assessment. Front Public Health 2020;8:341. https://doi.org/10.3389/fpubh.2020.00341 10.3389/fpubh.2020.00341 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Truog RD, Mitchell C, Daley GQ. The toughest triage - allocating ventilators in a pandemic. N Engl J Med 2020;382:1973-5. https://doi.org/10.1056/NEJMp2005689 10.1056/NEJMp2005689 [DOI] [PubMed] [Google Scholar]
- [5].Truog R, Mitchell C, Daley Q. The toughest triage - allocating ventilators in a pandemic. N Engl J Med; 2020;382:1973-5. https://doi.org/10.1056/NEJMp2005689 10.1056/NEJMp2005689 [DOI] [PubMed] [Google Scholar]
- [6].Sakamoto M, Begum S, Ahmed T. Vulnerabilities to COVID-19 in Bangladesh and a reconsideration of sustainable development goals. Sustainability 2020;12:5296. https://doi.org/10.3390/su12135296 10.3390/su12135296 [DOI] [Google Scholar]
- [7].Hridoy A-EE, Naim M, Emon NU, Tipo IH, Alam S, Al Mamun A, Islam MS. Forecasting COVID-19 dynamics and endpoint in Bangladesh: a data-driven approach. medRxiv 2020. https://doi.org/10.1101/2020.06.26.20140905 10.1101/2020.06.26.20140905 [DOI] [Google Scholar]
- [8].Mannan DKA, Mannan KA. Knowledge and perception towards Novel Coronavirus (COVID 19) in Bangladesh. Int Res J Bus soc sci 2020;6. https://doi.org/10.2139/ssrn.3576523 10.2139/ssrn.3576523 [DOI] [Google Scholar]
- [9].Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr 2020:102083. https://doi.org/10.1016/j.ajp.2020.102083 10.1016/j.ajp.2020.102083 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].ter Meulen V. Biology of Coronaviruses 1983. In: Molecular Biology and Pathogenesis of Coronaviruses. Springer 1984, pp. 227-35. [DOI] [PubMed] [Google Scholar]
- [11].Burks JS, DeVald B, Jankovsky LD, Gerdes JC. Two coronaviruses isolated from central nervous system tissue of two multiple sclerosis patients. Science 1980;209:933-4. https://doi.org/10.1126/science.7403860 10.1126/science.7403860 [DOI] [PubMed] [Google Scholar]
- [12].Resta S, Luby JP, Rosenfeld CR, Siegel JD: Isolation and propagation of a human enteric coronavirus. Science 1985;229:978-81. https://doi.org/10.1126/science.2992091 10.1126/science.2992091 [DOI] [PubMed] [Google Scholar]
- [13].Ding Y, He L, Zhang Q, Huang Z, Che X, Hou J, Wang H, Shen H, Qiu L, Li Z. Organ distribution of severe acute respiratory syndrome (SARS) associated coronavirus (SARS-CoV) in SARS patients: implications for pathogenesis and virus transmission pathways. J Patho 2004;203:622-30. https://doi.org/10.1002/path.1560 10.1002/path.1560 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].World Health Organisation. Emerging respiratory viruses, including COVID-19: methods for detection, prevention, response and control. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Taherdoost H. Sampling methods in research methodology; how to choose a sampling technique for research. IJARM 2016;5:18-27. https://doi.org/10.2139/ssrn.3205035 10.2139/ssrn.3205035 [DOI] [Google Scholar]
- [16].Lam KW, Hassan A, Sulaiman T, Kamarudin N. Evaluating the face and content validity of an instructional technology competency instrument for university lecturers in Malaysia. Int J Acad Res J Bus soc sci 2018;8:367-85. https://doi.org/10.6007/ijarbss/v8-i5/4108 10.6007/ijarbss/v8-i5/4108 [DOI] [Google Scholar]
- [17].Maswood M. Young, working-age people mostly infected with COVID-19 in Bangladesh. NEWAGE/Bangladesh 2020;13. [Google Scholar]
- [18].IndexMundi: Bangladesh Demographics Profile 2019. 2019. [Google Scholar]
- [19].Nawaz S, Hasin CT. Dietary intake and nutritional status of dialysis and non-dialysis patients in Bangladesh. J Nutr 2013;26:14. [Google Scholar]
- [20].Payahoo L, Khaje-Bishak Y, Gargari BP, Kabir-Alavi M-B, AsghariJafarabadi M. Assessment of nutritional and depression status in free-living elderly in Tabriz, Northwest Iran. Health Promot Perspect 2013;3:288. https://doi.org/10.5681/hpp.2013.033 10.5681/hpp.2013.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Rodriguez-Tadeo A, Wall-Medrano A, Gaytan-Vidaña M, Campos A, Ornelas-Contreras M, Novelo-Huerta H. Malnutrition risk factors among the elderly from the US-Mexico border: the “one thousand” study. J Nutr Health Aging. 2012, 16:426-431. https://doi.org/10.1007/s12603-011-0349-1 10.1007/s12603-011-0349-1 [DOI] [PubMed] [Google Scholar]
- [22].De Rezende CA, Coelho L, Oliveira L, Penha-Silva N. Dependence of the geriatric depression scores on age, nutritional status, and haematologic variables in elderly institutionalized patients. JNHA 2009;13:617-21. https://doi.org/10.1007/s12603-009-0172-0 10.1007/s12603-009-0172-0 [DOI] [PubMed] [Google Scholar]
- [23].Ahorsu DK, Lin C-Y, Imani V, Saffari M, Griffiths MD, Pakpour AH. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addict 2020March27:1-9. https://doi.org/10.1007/s11469-020-00270-8 10.1007/s11469-020-00270-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Banerjee D. The COVID-19 outbreak: crucial role the psychiatrists can play. Asian J Psychiatr 2020;50:102014. https://doi.org/10.1016/j.ajp.2020.102014 10.1016/j.ajp.2020.102014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Cheung Y, Chau PH, Yip PS. A revisit on older adults suicides and Severe Acute Respiratory Syndrome (SARS) epidemic in Hong Kong. Int J Geriatr Psychiatry 2008;23:1231-8. https://doi.org/doi.org/10.1002/gps.2056 10.1002/gps.2056 [DOI] [PubMed] [Google Scholar]
- [26].Xiang Y-T, Yang Y, Li W, Zhang L, Zhang Q, Cheung T, Ng CH. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020;7:228-9. https://doi.org/10.1016/S2215-0366(20)30046-8 10.1016/S2215-0366(20)30046-8 [DOI] [PMC free article] [PubMed] [Google Scholar]