

Abstract
There have been various developments in intraoral 3D scanning technology. This study is aimed at investigating the accuracy of 10 scanners developed from 2015 to 2020. A maxillary dental model with reference points was printed from Form 2 (FormLabs, Somerville, MA, USA). The model was scanned 5 times with each intraoral scanner (IOS); Trios 3 (normal and high-resolution mode); Trios 4 (normal and high-resolution mode) (3Shape Trios A/S, Copenhagen, Denmark); iTero Element, iTero 2, and iTero 5D Element (Align Technologies, San Jose, California, USA); Dental Wings (Dental Wings, Montreal QC, Canada); Panda 2 (Pengtum Technologies, Shanghai, China); Medit i500 (Medit Corp. Seoul, South Korea); Planmeca Emerald™ (Planmeca, Helsinki, Finland); and Aoralscan (Shining 3D Tech. Co., Ltd., Hangzhou, China). After the scan, the 3D scanned stereolithography files were created. The various distances were measured five times in X, Y, Z, and XY axes of various scans and with a vernier caliper (control) and from the Rhinoceros software. The data were analyzed using SPSS 18. Test for the normality of the various measurement data were done using Kolmogorov-Smirnov test. The trueness and precision of the measurements were compared among the various scans using the Kruskal-Wallis test. The significance was considered at P < 0.05. The trueness of the intraoral scans was analyzed by comparing the measurements from the control. Precision was tested through the measurements of repeated scans. It showed that more the distance is less the accuracy for all scanners. In all studied scanners, the trueness varied but precision was favorably similar. Diagonal scanning showed less accuracy for all the scanners. Hence, when scanning the full arch, the dentist needs to take more caution and good scan pattern. Trios series showed the best scan results compared to other scanners.
1. Introduction
In recent decades, there has continuous advancement in digital technologies in dentistry, such as computer-aided design/computer-aided manufacturing (CAD/CAM) systems, milling systems, three-dimensional (3D) scanning, and printing of various dental biomaterials [1–3]. Digital dentistry helps in the diagnosis, treatment planning, and fabrication of prostheses. An accurate dental impression is required to fabricate a good dental prosthesis or restoration [4, 5]. To fabricate a prosthesis or restoration digitally, dentists send the digital impression obtained from an intraoral scanner (IOS) from the clinic to the dental laboratory. Then, after receiving the digital scan, the dental technician creates a digital model, then designs, and finally manufactures the prosthesis.
There are different IOSs that are available in the market [6]. Intraoral scanners generally have a scan area of 1-2 teeth [7, 8]. At present, there are advanced scanning technologies, such as triangulation technique (used by Cerec, Dentsply Sirona), active wavefront sampling (used by True Definition, 3 M ESPE), and confocal scanning technique (used by iTero, Align Technology, and Trios, 3Shape) [9–11]. The confocal scanning technology is a faster scanning technology that captures images by focusing on an optical light beam with high-resolution visual images with improved accuracy and fewer distortions [9, 12].
Hence, with the various developments in intraoral 3D scanning technology, it is important to access the scanning accuracy of various IOS in the market. Hence, this in vitro study is aimed at investigating the accuracy of 10 scanners developed from 2015 to 2020.
2. Materials and Methods
2.1. Study Model
Maxillary dental models with reference point model were drawn by CAD software using Meshmixer and were printed from Form 2 (Figure 1) (FormLabs, Somerville, MA, USA) [13, 14].
Figure 1.

3D model. (a) The model was drawn by CAD software using Meshmixer, (b) 3D printed model, and (c) scanned file from an intraoral scanner exported to Rhinoceros 3D modeling software for the measurements.
2.2. Scanning and 3D Model
The model was scanned 5 times with each intraoral scanner (IOS); Trios 3 (normal and high-resolution mode); Trios 4 (normal and high-resolution mode) (3Shape Trios A/S 2020, Copenhagen, Denmark); iTero Element, iTero 2, and iTero 5D Element (Align Technologies, San Jose, California, USA);Dental Wings (DentalWings, Montreal QC, Canada); Panda (Pengtum Technologies, Shanghai, China); Medit i500 (Medit Corp. Seoul, South Korea), Planmeca Emerald™ (Planmeca, Helsinki, Finland); and Aoralscan (Shining 3D Tech. Co., Ltd. Hangzhou, China) (Figure 2). Then, the 3D scanned files were saved as stereolithography (.STL).
Figure 2.
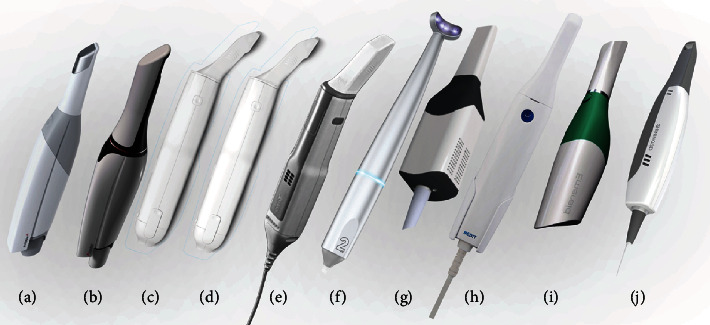
Various scanners used in this study: (a) Trios 3, (b) Trios 4, (c) iTero Element, (d) iTero 2, (e) iTero 5D Element, (f) Dental Wings, (g) Panda, (h) Medit i500, (i) Planmeca Emerald™, and (j) Aoralscan.
2.3. Measurements
The various distances were measured five times in X, Y, Z, and XY (Figure 3). The XY represented the measurement crossing the midline, and we designated it as diagonal. The measurements were measured from the Rhinoceros software (Rhino, Robert McNeel & Associates, Washington DC, USA). Measurements measured from a vernier caliper were used as the control.
Figure 3.
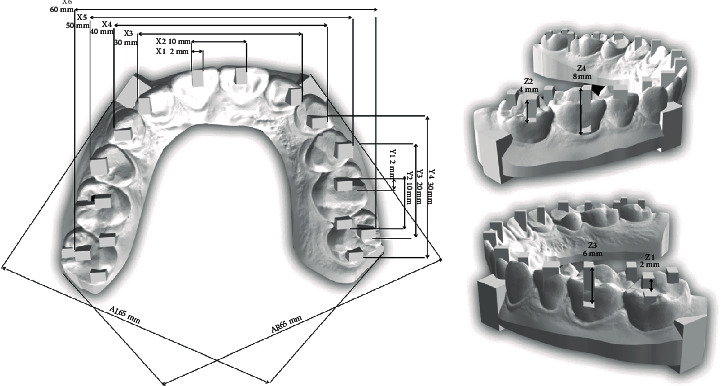
Various measurements in X, Y, and X-axis.
2.4. Statistical Analysis
The data were analyzed using SPSS 18. Test for the normality of the various measurement data were done using Kolmogorov-Smirnov test. The trueness and precision of the measurements were compared among the various scans using the Kruskal-Wallis test. The significance was considered at P < 0.05. The trueness of the intraoral scans was analyzed by comparing the measurements from the control. Precision was tested through the measurements of repeated scans.
3. Results
The results of various measurements in X, Y, XY, and diagonal measurements are shown in Tables 1–4. Table 5 shows the results of the test for the normality of data using Kolmogorov-Smirnov of various measurements. It showed that the data are not normally distributed. It showed that there was a significant difference for all the measurements among the scanners. In all studied scanners, the trueness varied but precision was favorably similar.
Table 1.
Results of measurements in X-axis measured from various scanners.
| Control | A (N) | A (HD) | A (N) | B (HD) | C | D | E | F | G | H | I | J | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| X1 | 1.90 ± 0.03 | 1.87 ± 0.03 | 1.88 ± 0.03 | 1.93 ± 0.04 | 1.88 ± 0.01 | 1.78 ± 0.032 | 1.80 ± 0.09 | 1.82 ± 0.07 | 1.87 ± 0.05 | 1.90 ± 0.03 | 1.80 ± 0.07 | 1.95 ± 0.02 | 1.87 ± 0.06 |
| X2 | 9.92 ± 0.02 | 9.86 ± 0.03 | 9.96 ± 0.02 | 9.89 ± 0.03 | 9.87 ± 0.02 | 9.86 ± 0.02 | 9.89 ± 0.06 | 9.87 ± 0.06 | 9.86 ± 0.07 | 9.92 ± 0.02 | 9.77 ± 0.6 | 9.96 ± 0.08 | 9.92 ± 0.04 |
| X3 | 29.84 ± 0.05 | 29.73 ± 0.02 | 29.91 ± 0.03 | 29.87 ± 0.07 | 29.82 ± 0.02 | 29.77 ± 0.05 | 29.71 ± 0.14 | 29.75 ± 0.07 | 29.80 ± 0.17 | 29.84 ± 0.05 | 29.55 ± 0.11 | 29.76 ± 0.73 | 29.83 ± 0.06 |
| X4 | 39.89 ± 0.04 | 39.71 ± 0.01 | 39.69 ± 0.24 | 39.97 ± 0.06 | 39.97 ± 0.03 | 39.73 ± 0.10 | 40.74 ± 0.18 | 39.80 ± 0.06 | 39.11 ± 0.17 | 39.89 ± 0.04 | 39.58 ± 0.08 | 39.70 ± 0.28 | 39.94 ± 0.03 |
| X5 | 50.01 ± 0.02 | 49.86 ± 0.11 | 50.21 ± 0.13 | 50.15 ± 0.03 | 50.14 ± 0.04 | 50.06 ± 0.08 | 49.87 ± 0.20 | 50.09 ± 0.20 | 50.83 ± 0.42 | 50.01 ± 0.02 | 49.61 ± 0.15 | 50.04 ± 0.23 | 50.33 ± 0.06 |
| X6 | 60.53 ± 0.05 | 60.06 ± 0.27 | 60.36 ± 0.51 | 60.53 ± 0.13 | 60.64 ± 0.23 | 61.60 ± 0.08 | 61.53 ± 0.33 | 61.56 ± 0.14 | 61.95 ± 0.37 | 61.74 ± 0.24 | 61.58 ± 0.33 | 61.51 ± 0.33 | 61.51 ± 0.15 |
A (N): Trios3 (normal); A (HD): Trios3HR; B (N): T rios4; B (HD): Trios4HR; C: iTero Element; D: iTero Element2; E: iTero Element 5D; F: Dental Wings; G: Panda; H: Planmeca Medit i500; I: Emerald™; J: Aoralscan.
Table 2.
Results of measurements in Y-axis measured from various scanners.
| Control | A (N) | A (HD) | A (N) | B (HD) | C | D | E | F | G | H | I | J | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Y1 | 1.92 ± 0.15 | 1.85 ± 0.03 | 1.85 ± 0.07 | 1.91 ± 0.04 | 1.86 ± 0.02 | 1.71 ± 0.09 | 1.87 ± 0.17 | 1.81 ± 0.12 | 1.82 ± 0.01 | 1.92 ± 0.01 | 1.77 ± 0.02 | 1.87 ± .0.09 | 1.80 ± 0.03 |
| Y2 | 9.87 ± 0.02 | 9.98 ± 0.14 | 9.81 ± 0.82 | 9.91 ± 0.06 | 9.84 ± 0.33 | 9.68 ± 0.98 | 9.78 ± 0.17 | 9.72 ± 0.06 | 9.80 ± 0.07 | 9.87 ± 0.02 | 9.73 ± 0.10 | 9.72 ± 0.13 | 9.90 ± 0.04 |
| Y3 | 19.80 ± 0.37 | 19.71 ± 0.12 | 19.81 ± 0.06 | 19.83 ± 0.04 | 19.83 ± 0.08 | 19.57 ± 0.09 | 19.74 ± 0.19 | 19.50 ± 0.24 | 19.63 ± 0.51 | 19.80 ± 0.03 | 19.67 ± 0.10 | 19.50 ± 0.01 | 19.76 ± 0.12 |
| Y4 | 30.47 ± 0.16 | 29.97 ± 0.39 | 30.18 ± 0.59 | 29.69 ± 0.13 | 29.63 ± 0.07 | 29.47 ± 0.13 | 29.48 ± 0.33 | 29.49 ± 0.42 | 29.75 ± 0.42 | 29.47 ± 0.37 | 29.47 ± 0.03 | 29.41 ± 0.09 | 29.77 ± 0.29 |
A (N): Trios3 (normal); A (HD): Trios3HR; B (N): Trios4; B (HD): Trios4HR; C: iTero Element; D: iTero Element2; E: iTero Element 5D; F: Dental Wings; G: Panda; H: Planmeca Medit i500; I: Emerald™; J: Aoralscan.
Table 3.
Results of measurements in Z-axis measured from various scanners.
| Control | A (N) | A (HD) | A (N) | B (HD) | C | D | E | F | G | H | I | J | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Z1 | 2.00 ± 0.17 | 2.01 ± 0.03 | 1.99 ± 0.04 | 1.99 ± 0.04 | 1.97 ± 0.02 | 1.92 ± 0.02 | 1.99 ± 0.08 | 1.91 ± 0.07 | 1.99 ± 0.06 | 2.00 ± 0.17 | 1.89 ± 0.06 | 1.88 ± 0.11 | 1.95 ± 0.03 |
| Z2 | 3.98 ± 0.01 | 3.98 ± 0.07 | 3.95 ± 0.07 | 4.00 ± 0.04 | 3.98 ± 0.02 | 3.94 ± 0.02 | 3.82 ± 0.09 | 3.91 ± 0.15 | 3.97 ± 0.05 | 3.98 ± 0.01 | 3.94 ± 0.08 | 3.80 ± 0.14 | 4.00 ± 0.06 |
| Z3 | 6.08 ± 0.03 | 5.90 ± 0.20 | 5.97 ± 0.01 | 5.99 ± 0.04 | 5.95 ± 0.04 | 5.83 ± 0.13 | 5.85 ± 0.06 | 5.81 ± 0.16 | 6.14 ± 0.15 | 6.08 ± 0.03 | 5.87 ± 0.07 | 5.85 ± 0.04 | 5.89 ± 0.07 |
| Z4 | 8.12 ± 0.08 | 7.96 ± 0.08 | 7.97 ± 0.13 | 7.93 ± 0.05 | 7.96 ± 0.03 | 7.83 ± 0.05 | 7.83 ± 0.10 | 7.71 ± 0.34 | 7.99 ± 0.15 | 8.12 ± 0.08 | 7.92 ± 0.13 | 7.83 ± 0.06 | 7.91 ± 0.13 |
A (N): Trios3 (Normal); A (HD): Trios3HR; B (N): Trios4; B (HD): Trios4HR; C: iTero Element; D: iTero Element2; E: iTero Element 5D; F: Dental Wings; G: Panda; H: Planmeca Medit i500; I: Emerald™; J: Aoralscan.
Table 4.
Results of measurements in diagonal measured from various scanners.
| Control | A (N) | A (HD) | A (N) | B (HD) | C | D | E | F | G | H | I | J | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AR | 65.06 ± 0.03 | 64.87 ± 0.11 | 65.12 ± 0.17 | 64.83 ± 0.47 | 65.08 ± 0.46 | 66.42 ± 0.38 | 66.48 ± 0.55 | 66.41 ± 0.44 | 66.44 ± 0.26 | 66.43 ± 0.33 | 66.46 ± 0.32 | 66.49 ± 0.30 | 66.52 ± 0.39 |
| AL | 65.32 ± 0.60 | 65.43 ± 0.48 | 65.40 ± 0.32 | 65.28 ± 0.13 | 65.27 ± 0.13 | 66.56 ± 0.17 | 66.55 ± 0.48 | 66.62 ± 0.25 | 66.56 ± 0.41 | 66.81 ± 0.44 | 66.63 ± 0.45 | 66.71 ± 0.48 | 66.64 ± 0.07 |
A (N): Trios3 (Normal); A (HD): Trios3HR; B (N): Trios4; B (HD): Trios4HR; C: iTero Element; D: iTero Element2; E: iTero Element 5D; F: Dental Wings; G: Panda; H: Planmeca Medit i500; I: Emerald™; J: Aoralscan.
Table 5.
The results of the test for normality of data using Kolmogorov-Smirnov of various measurements.
| Various measurements | Kolmogorov-Smirnova | ||
|---|---|---|---|
| Statistic | Degree of freedom | P value | |
| X1 | 0.120 | 65 | 0.022∗ |
| X2 | 0.104 | 65 | 0.076∗ |
| X3 | 0.097 | 65 | 0.200∗ |
| X4 | 0.127 | 65 | 0.011∗ |
| X5 | 0.125 | 65 | 0.013∗ |
| X6 | 0.147 | 65 | 0.001∗ |
| Y1 | 0.072 | 65 | 0.200∗ |
| Y2 | 0.130 | 65 | 0.008∗ |
| Y3 | 0.146 | 65 | 0.001∗ |
| Y4 | 0.152 | 65 | 0.001∗ |
| AR | 0.164 | 65 | <0.0001∗ |
| AL | 0.172 | 65 | <0.0001∗ |
| Z1 | 0.181 | 65 | <0.0001∗ |
| Z2 | 0.139 | 65 | 0.003∗ |
| Z3 | 0.056 | 65 | 0.200∗ |
| Z4 | 0.085 | 65 | 0.200∗ |
aLilliefors Significance Correction; ∗significant at P value <0.05.
It showed that the more the distance, the less is the trueness. For the precision, there was no significant difference (P > 0.05) from the Kruskal-Wallis test. For scanning in the diagonal axis, there was less accuracy for all scanners. Trios series showed better trueness and precision results compared to other scanners.
The mean difference of the various measurements of different IOS in various axes is shown in Figures 4–7.
Figure 4.
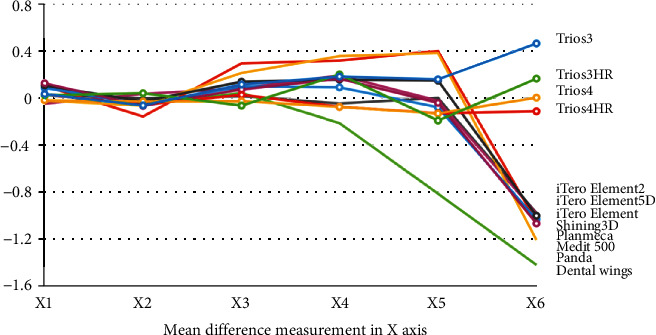
Mean difference of the various measurements of different intraoral scanners in X-axis.
Figure 5.
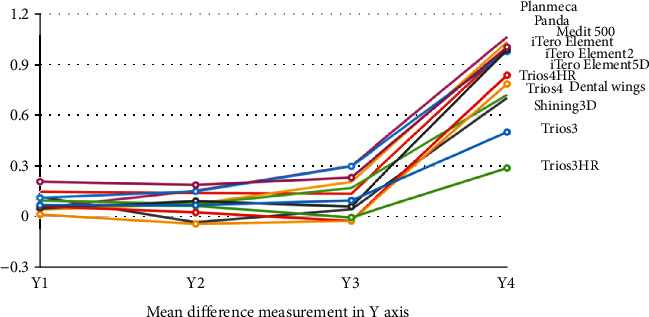
Mean difference of the various measurements of different intraoral scanners in Y-axis.
Figure 6.
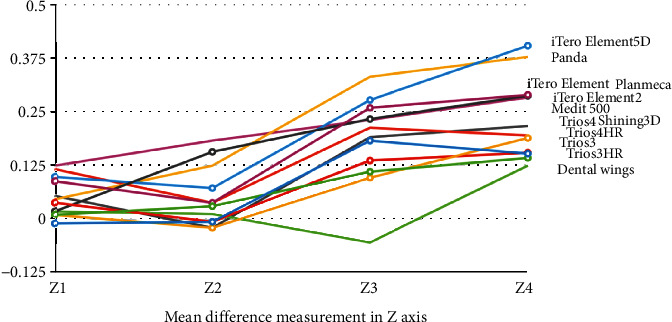
Mean difference of the various measurements of different intraoral scanners in the Z-axis.
Figure 7.
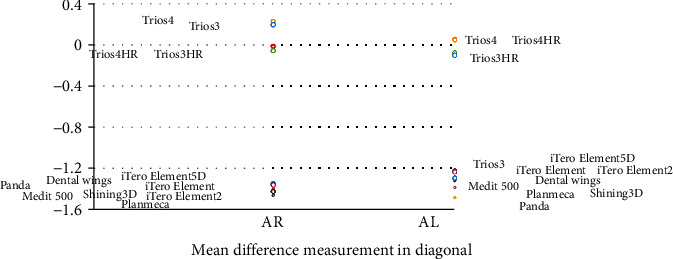
Mean difference of the various measurements of different intraoral scanners in XY axis (diagonal).
4. Discussion
The IOS has various advantages such as they make easier for the clinician and the laboratory technicians to communicate, eliminating the dental plaster models and reduce the working time. The precision and trueness of the IOS are an important factor as it influences the restorations [1, 2].
In this study, the accuracy of various scans is studied. The surface area in the X-axis and Y-axis ranged from 2 to 60 mm The accuracy of scans followed Y − axis > X − axis = Z − axis > diagonal axis. In the posterior area, the accuracy is more, whereas in the anterior area, the accuracy is less as the shape of teeth creates more error when capturing the images. The scanning depth (Z-axis) ranged from 2 to 8 mm, where special precaution is needed especially in the deep cavity.
A study by Mutwalli et al. [15] found that regarding the interarch distance measurements, Trios 3 had the lowest trueness, followed by Trios 3 mono and Itero Element, But Trios had the lowest precision, followed by iTero Element and Trios 3 Mono. But in our study, the Trios series presented higher accuracy compared to other IOS. Our study is supported by another study done by Renne et al. [8] where they found that for complete-arch scanning, the 3Shape Trios was found to have the best balance of speed and accuracy.
The result of our study is supported by the study done by Medina-Sotomayor et al. [16] where they compared the scanning strategy with the greatest accuracy, in terms of trueness and precision, of 4 IOS in the impression of a complete dental arch. They found that the trueness of the Trios and iTero system showed better results with strategy “D,” Omnicam with strategy “B,” and True Definition with strategy “C.” In terms of precision, both iTero and True Definition showed better results with strategy “D,” while Trios showed the best results with strategy “A” and Omnicam with strategy “B.” There were significant differences between the scanning strategies with the iTero scanner, but not with the other scanners. They concluded that the digital impression systems used in the experiment provided sufficient flexibility for the acquisition of 3D images without this affecting the accuracy of the scanner.
Similarly, another study [17] evaluated the trueness and precision of 2 widely used intraoral scanners (Trios 3, 3Shape, and CS 3600, Carestream), using an industrial scanner (Artec Space Spider) as a reference. Surface-based matching was implemented using the iterative closest point algorithm (ICP). Trios 3 showed slightly higher precision (approximately 10 μm) compared to CS 3600, only after superimposition on the whole dental arch (P < 0.05). Both intraoral scanners showed good performance and comparable trueness. However, in individual cases and various, not spatially defined areas, higher imprecision was evident. Thus, the IOS appropriateness for highly demanding, spatially extended clinical applications remains questionable.
Errors can occur which scanning by the IOS. The IOS captures approx. 1200 images when scanning. Scanning errors can result from the superimposition of the images while scanning and processing [7, 8]. This is due to the deviations of images which are more seen in the anterior teeth which have steep inclines and less tooth surface. Errors also can occur while computer processing from filter algorithms and calibration [18, 19]. In addition, errors during computer processing are due to filter algorithms [7]. Errors can occur on any axis. In this study, more errors were seen while scanning the depth (Z-axis).
Other factors that can affect the accuracy of IOS are intraoral factors (temperature, relative humidity, and illumination), operator (scanning pattern and skill), scanner unit (capture box, receiver, light source), computer software speed, and scanning area (scanning area, length, and surface irregularities) [20–23]. These factors were not considered in this study. In addition, since the model in this study overlaps the tooth with a complex shape, the side of these rectangular parallelepipeds can be scanned only when the scanner is tilted more. It is thought to be different from the usual scanning strategy performed in the actual clinical setting.
5. Conclusion
Within the limitations of this study, the following conclusions can be drawn.
More the scan distance, less the accuracy for all the scanners
In all studied scanners, the trueness varied but precision was favorably similar
Diagonal scanning showed less accuracy for all the scanners. Hence, when scanning the full arch, the dentist needs to take more caution and good scan pattern
Trios series showed the best scan results compared to other scanners
Acknowledgments
This research was supported by Maxillofacial Prosthodontics and Dental Materials Research Unit, Faculty of Dentistry, Prince of Songkla University and Scholarship Award of Thai Ph.D. Student under Thailand's Education Hub for Southern Region of ASEAN countries, Prince of Songkla University.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- 1.Beuer F., Schweiger J., Edelhoff D. Digital dentistry: an overview of recent developments for CAD/CAM generated restorations. British Dental Journal. 2008;204(9):505–511. doi: 10.1038/sj.bdj.2008.350. [DOI] [PubMed] [Google Scholar]
- 2.Amornvit P., Sanohkan S. The accuracy of digital face scans obtained from 3D scanners: an in vitro study. International Journal of Environmental Research and Public Health. 2019;16(24):p. 5061. doi: 10.3390/ijerph16245061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Humagain M., Rokaya D. Integrating digital technologies in dentistry to enhance the clinical success. Kathmandu University Medical Journal (KUMJ) 2019;17(68):256–257. [PubMed] [Google Scholar]
- 4.Suese K. Progress in digital dentistry: the practical use of intraoral scanners. Dental Materials Journal. 2020;39(1):52–56. doi: 10.4012/dmj.2019-224. [DOI] [PubMed] [Google Scholar]
- 5.Alqurashi H., Khurshid Z., Syed A. U. Y., Rashid Habib S., Rokaya D., Zafar M. S. Polyetherketoneketone (PEKK): an emerging biomaterial for oral implants and dental prostheses. Journal of Advanced Research. 2021;28:87–95. doi: 10.1016/j.jare.2020.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sawase T., Kuroshima S. The current clinical relevancy of intraoral scanners in implant dentistry. Dental Materials. 2020;39(1):57–61. doi: 10.4012/dmj.2019-285. [DOI] [PubMed] [Google Scholar]
- 7.Takeuchi Y., Koizumi H., Furuchi M., Sato Y., Ohkubo C., Matsumura H. Use of digital impression systems with intraoral scanners for fabricating restorations and fixed dental prostheses. Journal of Oral Science. 2018;60(1):1–7. doi: 10.2334/josnusd.17-0444. [DOI] [PubMed] [Google Scholar]
- 8.Rudolph H., Salmen H., Moldan M., et al. Accuracy of intraoral and extraoral digital data acquisition for dental restorations. Journal of Applied Oral Science. 2016;24:85–94. doi: 10.1590/1678-775720150266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Logozzo S., Zanetti E. M., Franceschini G., Kilpelä A., Mäkynen A. Recent advances in dental optics - Part I: 3D intraoral scanners for restorative dentistry. Optics and Lasers in Engineering. 2014;54:203–221. doi: 10.1016/j.optlaseng.2013.07.017. [DOI] [Google Scholar]
- 10.Renne W., Ludlow M., Fryml J., et al. Evaluation of the accuracy of 7 digital scanners: an in vitro analysis based on 3-dimensional comparisons. The Journal of Prosthetic Dentistry. 2017;118(1):36–42. doi: 10.1016/j.prosdent.2016.09.024. [DOI] [PubMed] [Google Scholar]
- 11.Mangano F., Gandolfi A., Luongo G., Logozzo S. Intraoral scanners in dentistry: a review of the current literature. BMC Oral Health. 2017;17(1):p. 149. doi: 10.1186/s12903-017-0442-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Logozzo S., Franceschini G., Kilpelä A., Caponi M., Governi L., Blois L. A comparative analysis of intraoral 3d digital scanners for restorative dentistry. The Internet Journal of Medical Technology. 2009;5:1–18. doi: 10.5580/1b90. [DOI] [Google Scholar]
- 13.Amornvit P., Sanohkan S., Peampring C. Studying the optical 3D accuracy of intraoral scans: an in vitro study. Journal of Healthcare Engineering. 2020;2020:9. doi: 10.1155/2020/5739312.5739312 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Amornvit P., Rokaya D., Peampring C., Sanohkan S. Confocal 3D optical intraoral scanners and comparison of image capturing accuracy. Computers, Materials and Continua. 2020;66:303–314. [Google Scholar]
- 15.Mutwalli H., Braian M., Mahmood D., Larsson C. Trueness and precision of three-dimensional digitizing intraoral devices. International Journal of Dentistry. 2018;2018:10. doi: 10.1155/2018/5189761.5189761 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Medina-Sotomayor P., Agustín Pascual M., Isabel Camps A. Accuracy of four digital scanners according to scanning strategy in complete-arch impressions. PLoS One. 2018;13(9, article e0202916) doi: 10.1371/journal.pone.0202916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Winkler J., Gkantidis N. Trueness and precision of intraoral scanners in the maxillary dental arch: an in vivo analysis. Scientific Reports. 2020;10(1):p. 1172. doi: 10.1038/s41598-020-58075-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mehl A., Ender A., Mormann W., Attin T. Accuracy testing of a new intraoral 3D camera. International Journal of Computerized Dentistry. 2009;12(1):11–28. [PubMed] [Google Scholar]
- 19.Ender A., Mehl A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. The Journal of Prosthetic Dentistry. 2013;109(2):121–128. doi: 10.1016/S0022-3913(13)60028-1. [DOI] [PubMed] [Google Scholar]
- 20.Kudva P. K. Digital dentistry: the way ahead. Journal of Indian Society of Periodontology. 2016;20(5):482–483. doi: 10.4103/jisp.jisp_355_16. [DOI] [Google Scholar]
- 21.Park H. N., Lim Y. J., Yi W. J., Han J. S., Lee S. P. A comparison of the accuracy of intraoral scanners using an intraoral environment simulator. The Journal of Advanced Prosthodontics. 2018;10(1):58–64. doi: 10.4047/jap.2018.10.1.58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Matta R. E., Adler W., Wichmann M., Heckmann S. M. Accuracy of impression scanning compared with stone casts of implant impressions. The Journal of Prosthetic Dentistry. 2017;117(4):507–512. doi: 10.1016/j.prosdent.2016.07.026. [DOI] [PubMed] [Google Scholar]
- 23.Nedelcu R. G., Persson A. S. Scanning accuracy and precision in 4 intraoral scanners: an in vitro comparison based on 3-dimensional analysis. The Journal of Prosthetic Dentistry. 2014;112(6):1461–1471. doi: 10.1016/j.prosdent.2014.05.027. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon reasonable request.