

Abstract
Background:
Relatively few studies test the interpersonal psychological theory’s monotonicity hypothesis. The monotonicity hypothesis proposes that suicide capability (i.e., fearlessness about death and pain tolerance) is stable or increases linearly with exposure to painful and provocative events. Research is conflicted, suggesting that suicide capability is static, decreases, or increases and returns to baseline. The current study thus tested this hypothesis in a sample of college students with histories of suicidal ideation. We hypothesized a stable and an increasing trajectory.
Methods:
Participants were 206 undergraduates; primarily women (73%), on average 19.05 years old, heterosexual (85%), and first-years (69%). Participants completed a baseline battery of questionnaires on suicide risk factors and daily diaries on suicide capability and suicidal ideation for 90 days (n = 7,342 surveys, 40% compliance rate). Group-based trajectory analyses were conducted with the SAS macro PROC TRAJ.
Results:
Modeling revealed a three group quadratic model. Low (27.7%), Moderate (41.3%), and High (31.1%) suicide capability groups remained static over time. Baseline suicidal ideation, but not history of suicide attempts or family history of suicidal behavior, distinguished groups; participants with suicidal ideation at baseline were less likely to be in the low suicide capability group.
Limitations:
Brief, dichotomized assessments, and a high attrition rate.
Conclusions:
These data showed temporal stability of suicide capability and suggest that the “acquired” component of capability may be overemphasized. Clarifying the stability and modifiability of suicide capability will enable empirically-based applications of the theory to suicide prevention.
Keywords: capability for suicide, interpersonal psychological theory, suicide, college students, longitudinal, mixture modeling
United States age-adjusted suicide rates rose 33% from 1999–2017 (Hedegard, Curtin, & Warner, 2018), indicating an urgent need to better understand the psychological and social mechanisms that lead to a suicide. Such an understanding is most practically guided by theory. The Interpersonal Psychological Theory of Suicide (IPTS; Joiner, 2005; Van Orden et al., 2010) is notable compared to other theories of suicide in that it distinguishes between the desire and the capability for suicide. Suicidal desire is caused by hopelessness about perceived burdensomeness and thwarted belongingness. However, of those who desire death only those who are also capable of suicide will transition from thinking about to acting on suicidal thoughts. The capability for suicide develops via exposure to painful and provocative events that contribute to increased fearlessness about death and physical pain tolerance (Joiner, 2005). Given the nature and presumed development of the capability for suicide, the monotonicity hypothesis of the IPTS states that the capability for suicide should increase following exposure to painful and provocative events and never decrease (Van Orden et al., 2010), implying a static upward trend. Although numerous studies have examined hypotheses derived from the IPTS (See Chu et al., 2017, for a review), relatively few tests of the monotonicity hypothesis exist. As a result, the nature of the capability for suicide remains unclear, thus stalling efforts to apply the theory to improve prevention and intervention practices.
Compared to the initial description of the nature and development of the capability for suicide, some authors have posited alternative viewpoints. P.N. Smith and Cukrowicz (2010), for example, suggested a diathesis stress model that included genetic and other dispositions or vulnerabilities, long-term static, and acutely varying aspects of capability. This conceptual model posited that capability over the long term would conform to the monotonicity hypothesis, while acute variations would occur with momentary increases that return to baseline. Accordingly, one’s fearlessness about death and tolerance of pain might increase during alcohol intoxication or suicide attempt rehearsal, but return to baseline afterwards.
Despite alternatives to the monotonicity hypothesis being described, the literature examining the nature and development of the capability for suicide remained largely ignored. To date, few longitudinal studies have directly examined the temporal stability of capability for suicide, the validity of the monotonicity hypothesis, or differences between long-term and acute variability (Bryan et al., 2016; George et al., 2016; Willoughby et al., 2015; Zuromski, Cero, & Witte, 2018; Velkhoff & A.R. Smith, 2019; King et al., 2018; Czyz, Berona, & King, 2016). What little research does exist examining these questions presents conflicted findings with some suggesting that capability is static (Velkhoff & A.R. Smith, 2019; Czyz et al., 2016), that it increases and decreases within brief intervals (Zuromski, Cero, & Witte, 2018), or increases and returns to baseline over time despite short-term variations (Bryan et al., 2016). Future research must therefore address these conflicted findings and clarify the nature of capability.
This conflicted picture of the temporal stability of the capability for suicide is likely due, in part, to the use of different timeframes across studies, and the resulting inability to distinguish between different types of variation. Zuromski, Cero, and Witte (2018) used latent class growth modeling of fearlessness about death over 15 days. In contrast with the monotonicity hypothesis, Zuromski et al. (2018) identified a class of people for whom fearlessness about death decreased over time. Alternatively, Bryan et al, (2016) found that the capability for suicide did not change following combat exposure in United States veterans over a two-year period. Velkhoff and A.R. Smith (2019) also found no significant weekly variation in capability for suicide over a two month time frame. This range of results, varying from unexpected decreasing trends to no variability, raises the question of whether temporal variability is moderated by timeframe or contextual factors that could influence exposure to painful and provocative events in specific populations (e.g., residential treatment centers, college students). That is, are there different classes of variability in the capability for suicide and how do these conform to predicted temporal patterns?
Given these conflicting results and the critical importance of clarifying the temporal stability of capability, the current study sought to contribute another test of the monotonicity hypothesis to the literature. This literature has largely used approaches that identify groups of individuals according to their trajectories of change in the capability for suicide. Such approaches are ideal for examining developmental processes as they allow for modeling individual differences in change. The current study utilized growth mixture modeling to examine the trajectory of capability for suicide over a 90 day period in a selected sample of college students with previous histories of suicidal ideation. The current study differs from the past growth mixture modeling studies on suicide capability in that we utilized a longer, 90-day, assessment period to assess the potential for capability to return to baseline. In keeping with the IPTS, we hypothesized both a stable class and an increasing class. Finally, we conducted exploratory analyses to examine predictors of capability class membership (e.g., demographics, prior history of suicidal ideation and attempts, and family history of suicidal behavior).
Method
The current study was derived from a larger, repeated measures, daily-diary study on college students with histories of suicidal ideation and alcohol use which was designed to examine the proximal relation of alcohol use with suicide-related thoughts and behaviors. Participants reported on numerous constructs related to suicidal thoughts and behaviors during a baseline session and then each day for 90 days.
Participants
We screened 1,338 undergraduate students enrolled in introduction to psychology courses at a large Southeastern university. Thirty-three percent (n = 440) of these students met inclusion criteria for study participation and completed the baseline phase of the study. Inclusion criteria included: 18 years of age or older, consumed alcohol within the past month, and history of suicidal ideation or attempt. At least three daily surveys were required to include participants in the planned data analyses, which resulted in 206 participants (73.2% women, 25.9% men, 1% “other”). Participants were, on average, 19.05 years old (SD = 2.39; range: 18–46). The majority of the sample identified a heterosexual orientation (85%), relationship status as single (89.5%), and resided with roommates/friends (65%) or family (15%). The academic status of most participants was freshman-level (69.3%). The majority of the sample had the following yearly household income distribution: less than $50,000 (38.8%) and $50,000-$100,000 (27.7%).
Procedures
We recruited participants from introduction to psychology courses at a mid-sized Southeastern university. Individuals completed the brief screening questionnaire online via the university subject pool. Eligible individuals proceeded to view an informed consent document via Qualtrics.com, and after consenting, completed an anonymous baseline survey. Participants created a 7-letter unique identifier, which linked their baseline data to their daily data (Yurek et al., 2008). Following completion of the baseline survey, participants were directed to a separate survey where they provided their email address for the second, daily survey phase of the study. This e-mail address was not linked to their data and was kept confidential.
Beginning the day after completing the baseline survey, participants received an email at 6AM and at 12PM with an anonymous link to their daily survey for 90 days. Each survey instructed participants to recall behavior on the previous day, defined as the time they awoke until the time they went to sleep. We paid participants 75 cents to one dollar per survey, depending on when they enrolled in the study (we increased compensation later in the study to improve compliance rates). Participants were incentivized with an additional $10 for completing at least 75% of their surveys. Participants could earn up to $77.50 to $100 in compensation for study participation. See Wolford-Clevenger et al., (2019) for a more detailed account of study procedures.
Measures
Baseline Measures.
Demographics.
A measure created for the parent study collected information on demographic variables of interest (e.g., gender, age, race/ethnicity, religious identification, relationship status, academic level).
Capability for Suicide.
To assess capability for suicide, two items were included in the daily surveys from the 20-item Acquired Capability for Suicide Scale (Van Orden et al., 2008). The ACSS assesses pain tolerance and fearlessness about death on a 5-point Likert scale: 1 (“not at all like me”) to 5 (“very much like me”). Although the 20-item scale was completed by participants at baseline, only two items were used in the daily surveys were: items 4 “I can tolerate a lot more pain than most people,” and 19 “I am not at all afraid to die”). The current study assesses capability using these two items.
Suicidal Ideation and Attempts.
Presence of suicidal ideation over the week prior to the baseline session was assessed using the 4-item Hopelessness Depression Symptom Questionnaire-Suicidality Subscale (Metalsky & Joiner, 1997). The total score was the sum of the items with total possible scores ranging from 0 to 12. We dichotomized this total score such that 0 = no suicidal ideation and 1 = any score greater than 1. The scale has demonstrated validity and excellent internal consistency in college students (Metalsky & Joiner, 1997) and the present sample (α = .91). We also added one question to assess whether participants had never attempted suicide, attempted suicide once, or attempted suicide more than once over their lifetime.
Family History of Suicidal Behavior.
Participants answered two brief, yes-no questions about family history of suicide attempts and deaths: “Have any of your blood relatives ever committed suicide?” and “Have any of your blood relatives ever attempted suicide?”.
Daily Measures.
Capability for Suicide.
Participants rated their overall daily fearlessness about death and perceived pain tolerance from the previous day. We used the two items from the 20-item ACSS with highest factor loadings on the pain tolerance and fearlessness about death subscales in one of the first studies to validate the ACSS: “I could tolerate a lot more pain than most people,” and “I was not at all afraid to die” (P.N. Smith, Wolford-Clevenger, Mandracchia, & Jahn, 2013). Participants rated these perceptions on a 5-point Likert scale (1 = “not at all like me” to 5 = “very much like me”). We summed these items such that the total possible daily score ranged from 2 to 10 (with possible weekly scores ranging from 14–70).
In the current sample, the correlation between the sum of the 2 daily items at baseline (ACSS 4 and 19) and the total ACSS at baseline (with those two items removed) was .72 (p < .0001). Further, the correlation between the sum of the 2 daily items at baseline (ACSS 4 and 19) and the Fearlessness About Death scale (FAD; Ribeiro et al., 2014; with item 19 removed) was .59 (p <.0001). These construct validity scores indicate that the two daily items adequately capture the same construct as the ACSS and FAD total scores. The lower correlation for the FAD total score is likely reflective of the fact that both pain tolerance and fearlessness about death are assessed by the two daily items.
Data Analysis
Preliminary Analyses
Calculation of Intraclass Coefficient.
To aid in the interpretation of the trajectory analysis, we estimated how much of the variance in repeated capability for suicide ratings were due to variance between individuals or within individuals. Using hierarchical linear modeling with the daily capability for suicide items averaged into 14 weekly ratings, we estimated a null model to calculate the intraclass coefficient: capabilityforsuicideti= π0i+ eti (Hox, Moerbeek, & Van de Schoot, 2010).
The ICC revealed the between-person variance to be .817 (81.7% of variance in capability for suicide was due to between person differences); therefore, 18.3% of the variance was due to within person differences. Although small, this variability does not preclude the use of trajectory analyses.
Compliance and Non-Compliance at Baseline and Daily Surveys.
To further characterize the sample, we report differences between the 206 participants who went on to complete at least three daily surveys (i.e., compliant) and the participants who did not (i.e., non-compliant, n = 234). As reported previously by Wolford-Clevenger et al., (2019), the proportion of women (53%) to complete the daily portion of the study was greater than the proportion of men (31%); χ2 (1) = 20.03, p < .001. Compliant participants were more likely to experience suicidal ideation at baseline (28%) than non-compliant participants who withdrew after the baseline assessment (19%); χ2 (1) = 6.86, p = .006. Compliant participants (26%) did not differ from non-compliant participants (21%) in suicide attempt history; χ2 (1) = 1.11, p = .29. Thus, the final sample who completed daily surveys comprised a greater percentage of women and individuals with suicidal ideation than the baseline sample.
We also describe the compliance rates across time in the daily portion of the study. As previously reported in Wolford-Clevenger et al., (2019), 39.6% (n = 7,342) of the 18,540 surveys sent were completed. For the total sample that completed any daily surveys, we had the following daily survey compliance rates: 30 days (57.6%), 60 days (33.8%), and 90 days (39.6%). For the final sample used in the present study (participants who completed at least three daily surveys), we had the following daily survey compliance rates: 30 days (57.7%), 60 days (45.8%), and 90 days (39.6%). Thus, on average, participants completed 17.30, 27.45, and 35.64 daily surveys out of the 30, 60, and 90 surveys, respectively. Out of the 90 daily surveys sent out, 105 participants (51%) completed less than 30 surveys, 50 participants (24.27%) completed between 30 and 60 surveys, and 51 participants (24.8%) completed 61 or more surveys. We had at least 1 month of data from 49% of the sample. Eighty participants (38.8% of the final sample) completed the final, 90th survey (but not necessarily all 90 surveys), and 48.5% of the sample completed at least one survey in the final week of the daily phase. Thus, although our daily compliance rates were low, we had a reasonable number of participants provide data to test temporal stability across the 90 days (~13 weeks).
Group Selection
Group-based trajectory analyses were calculated on participant self-reported capability for suicide using the SAS macro PROC TRAJ. PROC TRAJ is a macro for group-based modeling of longitudinal data based on mixture models for estimating trajectories (Jones et al., 2001). The purpose of using latent growth mixture modeling is to examine the possibility of different growth trajectories within a sample. By isolating groups with similar trajectories, one can better understand how predictors differently influence rates of change for each group. Latent growth models are ideal for examining developmental processes for this reason. Model selection entailed a two-step process: first determining the appropriate number of different trajectories that exist, then defining the ideal order of polynomials to best describe the trajectory of each identified group. Once the capability for suicide trajectory groups were finalized, trajectory group differences were examined. More specifically, chi-squared tests were utilized to determine if there were significant group differences between demographic characteristics, including gender, ethnicity, religion, income, relationship status, and academic status. Additional chi-square tests were used to determine if there were differences between groups on suicide specific variables including personal lifetime history of suicide attempt, presence of suicidal ideation at baseline, and family history of suicide attempts and deaths. Finally, a one-way analysis of variance (ANOVA) was utilized to determine if there were significant group differences in the age of participants.
Results
Hypothesis Testing
Group-based trajectory modeling indicated that a three group quadratic model was the best fit for self-reported capability for suicide from the initiation of the study over the course of three months of assessment (see Figure 1). In determining model selection, the Bayesian Information Criterion (BIC) was utilized, as it is a common statistic used in model selection (Jones et al., 2001). Table 1 provides the BIC values for the trajectory groups and statistics for model comparison. As suggested by the literature (Andruff et al., 2009), model selection began applying a quadratic trajectory to a single group, adding one group at a time. The decision to use the three group model was derived from a combination of the BIC and significance values. Although BIC values suggest the inclusion of a fourth group, the parameters of the fourth group are not significant. Furthermore, the three group model is consistent with the previous study utilizing latent growth curve modeling in this population (Zuromski et al., 2018) and also provided for clinical interpretability with the groups as follows: Low (participants whose reported capability for suicide remained low through the duration of the study), Moderate (participants whose reported capability for suicide remained at a moderate level through the duration of the study), and High (participants whose reported capability for suicide remained high for the duration of the study). The group proportions estimated by the group-based trajectory model determined that 27.7% were assigned to the Low group, 41.3% to Moderate, and 31.1% to the High group. The quadratic slopes (see Table 2) were as follows: .00097 (Low), .00020 (Moderate), and −.00064 (High). These results suggest minimal, albeit significant change over the course of assessment (see Figure 1). As evidenced by the significant quadratic slopes, there was significant short-term variability within the assessment window. However, no group changed classification (i.e. low capability to moderate capability) over the course of the assessment window. As evidenced by the quadratic model fit, all groups returned to baseline.
Figure 1.
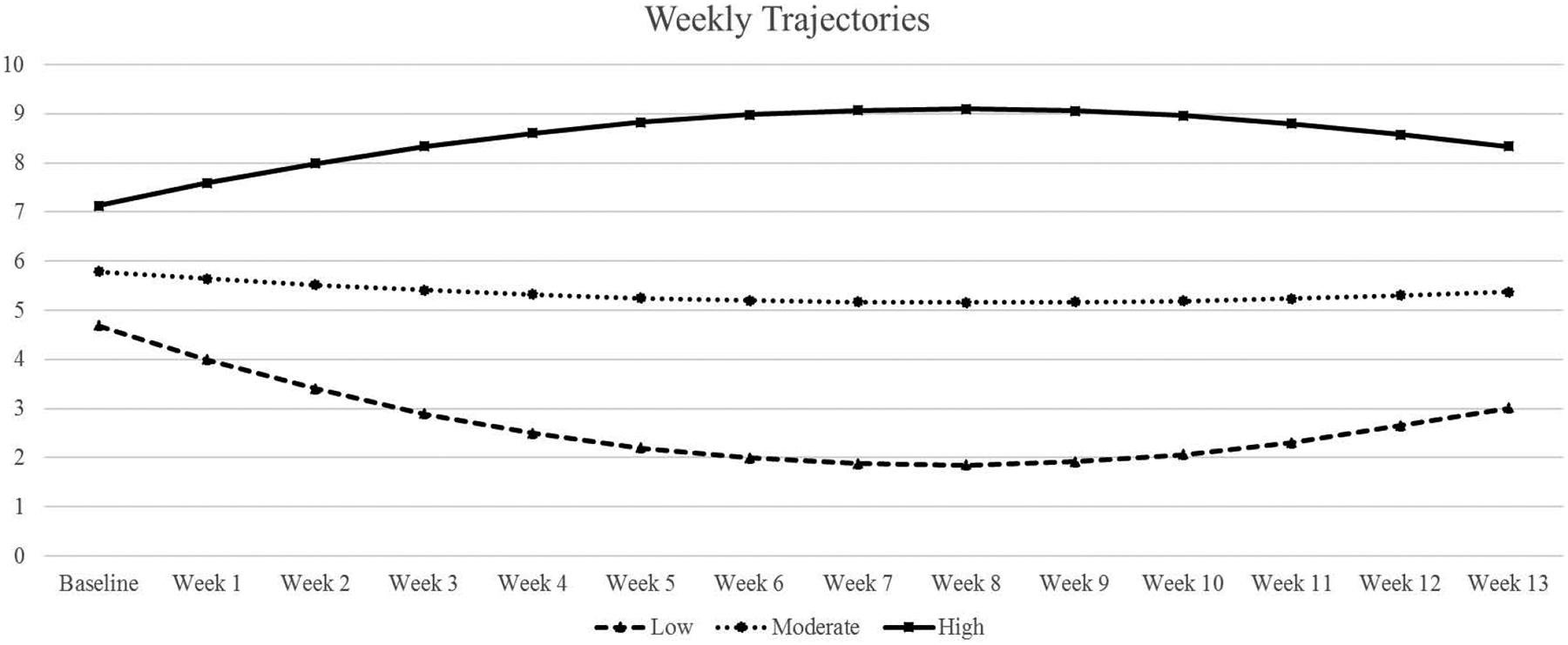
Weekly capability for suicide group trajectories.
Table 1.
Bayesian Information Criterion (BIC) and Model Comparison Statistics for Determining Capability for Suicide Trajectory Groups
| # of Groups | BIC | Null Model | 2(Δ BIC) |
|---|---|---|---|
| 1 | −3600.34 | ||
| 2 | −3044.74 | 1 | 1111.20 |
| 3 | −2838.91 | 2 | 411.66 |
| 4 | −2746.23 | 3 | 185.36 |
Table 2.
Model Fit of Group-Based Trajectory Modeling Analyses
| Intercept B(SE) | Linear B(SE) | Quadratic B(SE) | Predicted Capability for Suicide (Baseline) | Predicted Capability for Suicide (4 Weeks) | Predicted Capability for Suicide (8 Weeks) | Predicted Capability for Suicide (12 Weeks) | |
|---|---|---|---|---|---|---|---|
| Group 1 | 4.69 (.15)*** | −0.11 (.01)*** | .00097 (.00)*** | 4.69 | 2.50 | 1.85 | 2.65 |
| Group 2 | 5.79 (.13)*** | −0.02 (.01)** | .00020 (.00)* | 5.58 | 5.32 | 5.16 | 5.30 |
| Group 3 | 7.13 (.14)*** | 0.07 (.01)*** | −.00064 (.00)*** | 7.71 | 8.61 | 9.09 | 8.57 |
Note. Linear and Quadratic equations reflect change in capability for suicide per two weeks of treatment.
= p < .05,
= p < .01,
= p < .001.
Group Comparisons
Results of an ANOVA revealed there were no significant age differences between groups [F(2, 205) = 1.28, p = .28]. Furthermore, chi-square tests revealed there was no association between capability for suicide trajectory group and demographics including gender [χ2(2) = 3.79; p = .15], race and ethnicity [χ2(12) = 8.76; p= .72], religion [χ2(10) = 7.65; p = .66], socioeconomic status [χ2(8) = 5.91; p = .66], relationship status [χ2(4) = 4.48; p = .35], and academic status [χ2(8) = 13.35; p= .10] (see Table 3 for n’s and percentages). Additional chi-square tests showed there was no association between capability for suicide trajectory group and a previous suicide attempt [χ2(2) = 1.57; p = .45], a blood relative with a previous attempt [χ2(2) = .99; p = .61], and a blood relative who died by suicide [χ2(2) = 3.00; p = .22]. See Table 3 for the demographic characteristics of each group.
Table 3.
Group membership for each capability for suicide trajectory group.
| Low Group n (% of total) | Moderate Group n (% of total) | High Group n (% of total) | |
|---|---|---|---|
| Total | 57 (27.7) | 85 (41.3) | 64 (31.1) |
| Gender | |||
| Women | 40 (19.7) | 68 (33.5) | 42 (20.7) |
| Men | 17 (8.4) | 16 (7.9) | 20 (9.9) |
| Academic Status | |||
| Freshman | 48 (23.4) | 52 (25.4) | 42 (20.5) |
| Sophomore | 3 (1.5) | 20 (9.8) | 14 (6.8) |
| Junior | 3 (1.5) | 6 (2.9) | 3 (1.5) |
| Senior | 3 (1.5) | 7 (8.2) | 3 (1.5) |
| Relationship Status | |||
| Single, living with partner | 8 (4.0) | 6 (3.0) | 4 (2.0) |
| Single, not living with partner | 49 (24.5) | 73 (36.5) | 57 (28.5) |
| Married, living with spouse | 0 (0.0) | 1 (0.5) | 2 (1.0) |
| Race/Ethnicity | |||
| White | 47 (22.9) | 72 (35.1) | 50 (24.4) |
| Black | 4 (2.0) | 3 (1.5) | 3 (1.5) |
| American Indian/Alaskan Native | 0 (0.0) | 0 (0.0) | 1 (0.5) |
| Asian | 0 (0.0) | 2 (1.0) | 3 (1.5) |
| Multiracial | 3 (1.5) | 4 (2.0) | 4 (2.0) |
| Other | 3 (1.5) | 2 (1.0) | 2 (1.0) |
| Religion | |||
| Catholic | 4 (2.9) | 12 (8.6) | 6 (4.3) |
| Protestant | 11 (7.9) | 20 (14.4) | 18 (12.9) |
| Buddhist | 1 (0.7) | 0 (0.0) | 2 (1.4) |
| Jewish | 0 (0.0) | 1 (0.7) | 1 (0.7) |
| Islam | 0 (0.0) | 0 (0.0) | 1 (0.7) |
| Other | 19 (13.7) | 27 (19.4) | 18 (12.9) |
| Suicidal Ideation | 9 (4.5) | 24 (11.9) | 23 (11.4) |
| Attempted Suicide | 11 (5.5) | 21 (10.6) | 18 (9.0) |
| Blood Relative Attempted Suicide | 23 (11.6) | 27 (13.6) | 23 (11.6) |
| Blood Relative Died by Suicide | 10 (5.0) | 10 (5.0) | 14 (7.0) |
However, chi-square tests revealed a significant association between capability for suicide trajectory group and presence of suicidal ideation at baseline [χ2(2) = 6.26; p = .04]. Follow up analyses utilizing a Bonferroni correction indicated a significant individual chi-square test for having suicidal ideation at baseline and the low capability for suicide group [χ2(1) = 5.24; p = .02]. Participants who endorsed suicidal ideation at baseline were less likely to be classified in the low capability for suicide group, whereas participants who did not have suicidal ideation at baseline were more likely to be classified in the low capability group.
Discussion
The primary aim of this study was to test the monotonicity hypothesis of the IPTS, which states that the capability for suicide should steadily increase or remain stable, but not decrease, over time. Using latent growth mixture modeling, the current study aimed to examine group-level differences in capability growth trajectories, and how demographic and suicide-related predictors influenced group membership. Latent growth mixture modeling was selected to more effectively probe capability over the course of time, and to examine clinical predictors of group membership. Three groups emerged: low, average, and high, and the within person variability in capability for suicide was small (18.3%). Although each group exhibited trends mirroring Zuromski and colleagues’ (2018) study (e.g. high, average, and low), all the groups remained within the same classification as their initial scores (i.e. low, moderate, high) and, therefore, remained relatively stable. Furthermore, any measured changes in capability returned to baseline by the end of the assessment period as evidenced by the quadratic model fit. While this finding is a departure from Zuromski et al. (2018), whose high, average, and low groups increased, remained stable, and decreased, respectively this may be attributed to differences in assessment measures and analyses utilized. Finally, suicidal ideation at baseline was the sole predictor of class membership with those in the low capability group less likely to endorse current suicidal ideation at study intake.
Prior research on this topic has produced seemingly mixed results, suggesting that the capability for suicide may remain stable (Velkhoff & A.R. Smith, 2019; Czyz & King, 2015; King et al., 2018), increase or decrease over brief intervals (Zuromski, Cero, & Witte, 2018) and increase in the short-term only to return to baseline (Bryan et al., 2016). Our findings support that there exist classes of varying levels of suicide capability (i.e., low, moderate, high) that may change in the short-term and return to baseline. Taken together, we interpret this literature as supporting the conceptualization of capability for suicide as a temporally stable construct, but showing some variation over short intervals that return to baseline. The one study that did detect changes over time in capability also collected data within the shortest window (15 days). We posit that the assessment window is critical in differentiating stability versus variability. That is, though capability can increase or decrease over short periods (e.g. minutes, days, weeks), it will return to baseline and remain stable when examined over longer periods (e.g., 56 days, two years; Bryan et al., 2016; Velkhoff & A.R Smith, 2019).
Another critical factor is the use of quadratic versus linear regression to examine growth trajectories. The current study interpreted both the linear and the quadratic slopes. The quadratic slopes describe change over time beyond what is described by the linear slopes, and capture trajectories that return to baseline. Prior latent growth models of capability interpreted the linear slopes (Zuromski et al., 2018; Velkhoff & A.R Smith, 2019). In contrast, Bryan and colleagues (2016) were able to capture return to baseline using a dynamical systems theory approach. Analytic approaches that can capture various types of change within an assessment window may yield more nuanced results.
The current findings also suggest that people vary in their mean level or baseline. A three or four class solution is common in cross-sectional and longitudinal mixture modeling studies assessing suicidal ideation and behavior. Findings from such studies often represent some variation of low, moderate, and high risk groups (Czyz & King, 2015; Ma et al., 2017, Hamza & Willoughby, 2013). Of the two prior mixture modeling studies assessing capability for suicide, Zuromski et al., (2018) also found three groups, whereas Velkhoff and A.R. Smith, (2019) found only one group. We speculate that such differences are likely due to the nature of the samples. There was likely less variability in the capability for suicide in Velkhoff and A.R. Smith’s (2018) sample of eating disorder patients compared to Zuromski and colleagues’ (2018) college student sample with a wider range of clinical histories. In the same vein, the present study included college students with histories of suicidal ideation that may have also been subject to wider variability compared to Velkhoff and A.R. Smith’s (2018) diagnostically homogenous group.
We also interpret the current findings that differences in individual’s baseline or mean levels of capability might suggest that fearlessness about death and pain tolerance are more congruent with the three-step theory’s (Klonsky & May, 2015) description of a dispositional or trait aspect of suicide capability, versus an acquired capability. Though several studies have purportedly found that the capability for suicide develops in response to repeated exposure to painful and provocative life events, such studies are predominantly cross-sectional, correlational studies examining retrospectively recalled frequency of exposure to painful and provocative life events. This body of literature thus may overestimate the effects of painful and provocative life events on suicide capability.
The predictor of class membership demonstrated in the current study was the presence of suicidal ideation at baseline: participants who endorsed suicidal ideation at baseline were less likely to be classified in the low capability for suicide group. This is consistent with meta-analytic findings that suicidal ideation correlates, if only weakly, with capability for suicide (Chu et al., 2017). One explanation for these findings is that frequent, chronic suicidal ideation often involves increases in imagery, planning, and mental rehearsal, which are believed to be associated with capability (P.N. Smith & Cuckrowicz, 2010). Such a process is perhaps akin to the development or expression of what Rudd and colleagues (2006) would call the suicidal mode. That is, frequent, regular activation of suicidal thoughts primes suicide-related cognitive content and associated affective, physiological systems.
Gender, race and ethnicity, religion, socioeconomic status, relationship status, and academic status were not predictive of class membership and suicide capability levels. Of these sociodemographic variables, it was most surprising that men were not more likely to be in the high capability group. Prior studies found that men were more likely to be in the stable and increasing group (Zuromski et al., 2018) and capability is often posed as the mechanism explaining higher rates of suicide among men due to their adherence to masculine gender norms that facilitate increased exposure to painful and provocative events (Granato, P. N. Smith, & Selwyn, 2015; P. N. Smith et al., 2016). However, other research indicates that some stereotypically masculine traits believed to promote suicide capability operate in the same manner when displayed by women (Fadoir, Kuhlman, & P. N. Smith, 2019), suggesting that homogeneity in certain personality traits or life experiences is more critically important than sex.
Two frequently hypothesized contributors to capability for suicide are family and individual history of suicidal behavior (P. N. Smith & Cukrowicz, 2010; Joiner, 2005). However, there was no association between either suicide attempt history, exposure to kin suicidal behavior and suicide capability trajectory group. Regarding suicide exposure, several prior studies point to potential heightened suicide risk following kin suicide (e.g., Rajalin, Hirvikoski, & Jokinen, 2013; Nanayakkara, Misch, Chang, & Henry, 2013; Pitman, Osborn, King, & Erlangsen, 2014). However, pre-existing mental health conditions and life experiences (e.g., depression, interpersonal violence in childhood) may account for more variance in these associations (Nanayakkara, Misch, Chang, & Henry, 2013; Rajalin, Hirvikoski, & Jokinen, 2013). Regarding capability, some prior studies show that it differentiates ideators from attempters and those who select more versus less lethal suicide methods (Klonsky & May, 2015; Dhingra et al., 2018; P. N. Smith et al., 2012). However, other studies do not support this association (Paashaus et al., 2019; Burke et al., 2018; Bauer et al., 2020). Similarly, Chu and colleagues’ (2017) meta-analysis found only a weak significant relationship between suicide attempt history and capability for suicide. Capability for suicide may only be associated with a history of a suicide attempt in people with current ideation (P. N. Smith et al., 2016) or thwarted interpersonal needs (Chu et al., 2017). The current study’s null results suggest that personal and family history of suicidal behavior do not relate to capability for suicide as has been theorized. Complex models accounting for the effect of multiple variables may yield more theoretically consistent results.
The current findings must be interpreted in light of several limitations. Similar to other studies using daily diary and ecological momentary assessment methods, the current study relied on a very brief assessment (i.e., two self-report items of fearlessness about death and pain tolerance) for over-time measurement of the capability for suicide. Although these items were selected due their highest factor loadings in a prior validation study of the Acquired Capability for Suicide Scale, range restriction may have hindered more robust changes within groups. However, the pain tolerance item asked participants to compare their pain tolerance relative to others, which may have been difficult for participants to accurately rate on a daily basis. Indeed, one might interpret that the 18.3% of the variance in capability for suicide being due to within person differences was, in part, because of crude measurement. However, one could also interpret it as additional support for capability’s stability relative to more dynamic constructs (e.g. suicide ideation; Kleiman et al., 2017). Further, self-report measurement may not be an accurate or valid manner by which to assess this construct. Future studies should consider alternatives (e.g., implicit associations, objective pain tolerance) as they are developed and gain support in longitudinal studies. Participant attrition and compliance rates may have biased the results and/or impacted the detection of statistically significant results. Participants who went on to complete the daily surveys were more likely than those who dropped out after the baseline assessment to be women and to report experiencing suicidal ideation in the week prior to entering the study. At present, it is unknown whether gender and the presence of suicidal ideation might moderate the trajectory of the capability for suicide by an individual. Suicide characteristic variables were also dichotomized, potentially limiting our ability to understand how the spectrum of suicidal thoughts and behaviors might have predicted class membership. The current study also suffered from a low compliance rate with the daily surveys and was limited by a potentially homogenous sample with regards to sociodemographic and suicide-related variables, which may have impacted power to detect more robust differences. Finally, the current study did not include assessment of exposure to painful and provocative life events, which would enable a more rigorous test of the monotonicity hypothesis. Future empirical work should improve these methods by assessing changes in the capability for suicide in response to experiences of painful and provocative life events. Future research should also seek to replicate findings in a range of clinical and community samples to capture a diversity of demographic and clinical characteristics.
Despite these limitations, this study is one of the first seeking to clarify the temporal stability and modifiability of capability, a necessary task for defining appropriate clinical applications of the theory that are currently limited due to small effect sizes across studies (Chu et al., 2017). Although the inclusion of painful and provocative events is critical to a full and rigorous test of the monotonicity hypothesis, the primary question of the current study is how capability changes over time. The discussion of painful and provocative events and their highly contested measurement (especially in the context of a daily diary study in which assessment is constrained) could have detracted from this primary purpose. Furthermore, researchers have recently considered whether capability is less influenced by life events and more likely a genetic or trait factor (P.N. Smith & Cuckrowicz, 2010), by virtue of its long-term stability (Bryan et al., 2016; Velkhoff & Smith, 2018).
Ample research suggests that the acquired component of capability is significantly overemphasized, and its role in the prevention, assessment and management of suicide risk therefore remains unclear. Along the lines of King and colleagues’ (2018) study, future work must therefore examine the modifiability and stability of the IPTS constructs over the course of treatment.
Conclusions
Despite these limitations, the current study adds to an emerging literature that informs our understanding of how the capability for suicide develops and changes (or not) over time. Indeed, the current study employed a large sample compared to other longitudinal studies of suicide capability, utilized latent growth modeling, and an intensive daily assessment schedule over a 90-day period. Although findings might be interpreted as partially supporting the IPTS monotonicity hypothesis, it also appears that the acquired component of capability may be overemphasized (P. N. Smith et al., 2012; Velkhoff & A.R. Smith, 2018; Chu et al., 2017). Rather, consistent with the majority of other longitudinal studies, it appears that the capability for suicide is temporally stable and varies across individuals.
Highlights.
Three classes emerged: low, moderate, and high capability for suicide.
There was significant short-term variability in capability for suicide
No group changed classification over the assessment period and all groups returned to baseline
Suicidal ideation at baseline was the sole predictor of class membership: those in the low capability group were less likely to endorse current suicidal ideation at study intake.
The “acquired” component of capability may be overemphasized.
Funding Information:
Please note that this work was supported, in part, by grant F31AA024685 from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) and the Thomas Fellowship awarded to the fourth author. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding sources.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Dcelaration of Competing Intereast
The authors have no conflicts of interest to disclose regarding the submitted manuscript.
Publisher's Disclaimer: Disclaimer: The opinions or assertions contained herein are the private views of the authors and do not necessarily reflect the views of the University of South Alabama, University of Houston - Downtown, Menninger Clinic, University of Tennessee Knoxville, or the University of Alabama at Birmingham.
Institutional Review Board: All study procedures were approved by the study site (University of Tennessee) IRB.
References
- Andruff H, Carraro N, Thompson A, Gaudreau P, & Louvet B (2009). Latent growth modelling: A tutorial. Tutorials in Quantitative Methods for Psychology, 5, 11–24. [Google Scholar]
- Bauer BW, Gai AR, Duffy ME, Rogers ML, Khazem LR, Martin RL, … & Capron DW (2020). Fearlessness about death does not differ by suicide attempt method. Journal of Psychiatric Research. [DOI] [PubMed] [Google Scholar]
- Bryan CJ, Sinclair S, & Heron EA (2016). Do military personnel “acquire” the capability for suicide from combat? A test of the interpersonal-psychological theory of suicide. Clinical Psychological Science, 4(3), 376–385. [Google Scholar]
- Burke TA, Ammerman BA, Knorr AC, Alloy LB, & McCloskey MS (2018). Measuring acquired capability for suicide within an ideation-to-action framework. Psychology of Violence, 8(2), 277–286. 10.1037/vio0000090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chu C, Buchman-Schmitt JM, Stanley IH, Hom MA, Tucker RP, Hagan CR, … & Michaels MS (2017). The interpersonal theory of suicide: A systematic review and meta-analysis of a decade of cross-national research. Psychological bulletin, 143(12), 1313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Czyz EK, Berona J, & King CA (2016). A prospective examination of the interpersonal-psychological theory of suicidal behavior among psychiatric adolescent inpatients. Journal of Religion and Health, 55(4), 1172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Czyz EK, & King CA (2015). Longitudinal trajectories of suicidal ideation and subsequent suicide attempts among adolescent inpatients. Journal of Clinical Child & Adolescent Psychology, 44(1), 181–193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dhingra K, Persson S, & Swogger MT (2018). Examining the relationship between suicidal behavior and psychopathic traits through the lens of the interpersonal–psychological theory of suicide. In Routledge International Handbook of Psychopathy and Crime (pp. 544–558). Routledge. [Google Scholar]
- Fadoir NA, Kuhlman ST, & Smith PN (2019). Suicide risk and restricted emotions in women: the diverging effects of masculine gender norms and suicide capability. Archives of Suicide Research, 1–17. [DOI] [PubMed] [Google Scholar]
- George SE, Page AC, Hooke GR, & Stritzke WG (2016). Multifacet assessment of capability for suicide: Development and prospective validation of the Acquired Capability With Rehearsal for Suicide Scale. Psychological Assessment, 28(11), 1452. [DOI] [PubMed] [Google Scholar]
- Granato SL, Smith PN, & Selwyn CN (2015). Acquired capability and masculine gender norm adherence: Potential pathways to higher rates of male suicide. Psychology of Men & Masculinity, 16(3), 246. [Google Scholar]
- Hamza CA, Willoughby T (2013) Nonsuicidal Self-Injury and Suicidal Behavior: A Latent Class Analysis among Young Adults. PLoS ONE 8(3): e59955. doi: 10.1371/journal.pone.0059955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hedegaard H, Curtin SC, Warner M. Suicide mortality in the United States, 1999–2017. NCHS Data Brief, no 330. Hyattsville, MD: National Center for Health Statistics. 2018. [Google Scholar]
- Hox JJ, Moerbeek M, & Van de Schoot R (2010). Multilevel analysis: Techniques and applications. Routledge. [Google Scholar]
- Joiner TE, 2005. Why People Die by Suicide. Harvard University Press, Cambridge, MA. [Google Scholar]
- Jones JL, Nagin DS, & Roeder K (2001). A SAS procedure based on mixture models for estimating developmental trajectories. Sociological Methods, 29, 374–393. [Google Scholar]
- King JD, Horton SE, Hughes JL, Eaddy M, Kennard BD, Emslie GJ, & Stewart SM (2018). The Interpersonal–psychological Theory of Suicide in adolescents: A preliminary report of changes following treatment. Suicide and Life- Threatening Behavior, 48(3), 294–304. [DOI] [PubMed] [Google Scholar]
- Kleiman EM, Turner BJ, Fedor S, Beale EE, Huffman JC, & Nock MK (2017). Examination of real-time fluctuations in suicidal ideation and its risk factors: Results from two ecological momentary assessment studies. Journal of abnormalpsychology, 126(6), 726. [DOI] [PubMed] [Google Scholar]
- Klonsky ED, & May AM (2015). The three-step theory (3ST): A new theory of suicide rooted in the “ideation-to-action” framework. International Journal of Cognitive Therapy, 8(2), 114–129. [Google Scholar]
- Metalsky GI, & Joiner TE (1997). The hopelessness depression symptomquestionnaire. Cognitive Therapy and Research, 21(3), 359–384. [Google Scholar]
- Nanayakkara S, Misch D, Chang L, & Henry D (2013). Depression and exposure to suicide predict suicide attempt. Depression and Anxiety, 30(10), 991–996. [DOI] [PubMed] [Google Scholar]
- Paashaus L, Forkmann T, Glaesmer H, Juckel G, Rath D, Schönfelder A, Engel P, & Teismann T (2019). Do suicide attempters and suicide ideators differ in capability for suicide? Psychiatry Research, 275, 304–309. https://doi-org.libproxy.usouthal.edu/10.1016/j.psychres.2019.03.038 [DOI] [PubMed] [Google Scholar]
- Pitman A, Osborn D, King M, & Erlangsen A (2014). Effects of suicide bereavement on mental health and suicide risk. The Lancet Psychiatry, 1(1), 86–94. [DOI] [PubMed] [Google Scholar]
- Rajalin M, Hirvikoski T, & Jokinen J (2013). Family history of suicide and exposure to interpersonal violence in childhood predict suicide in male suicide attempters. Journal of Affective Disorders, 148(1), 92–97. [DOI] [PubMed] [Google Scholar]
- Smith PN, & Cukrowicz KC (2010). Capable of suicide: A functional model of the acquired capability component of the interpersonal-psychological theory of suicide. Suicide and Life-Threatening Behavior, 40(3), 266–275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith PN, Selwyn C, D’Amato D, Granato S, Kuhlman S, & Mandracchia JT (2016). Life experiences and the acquired capability for suicide in incarcerated men. Death Studies, 40(7), 432–439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Orden KA, Witte TK, Gordon KH, Bender TW, & Joiner TE Jr. (2008). Suicidal desire and the capability for suicide: Tests of the interpersonal-psychological theory of suicidal behavior among adults. Journal of Consulting and Clinical Psychology, 76, 72. [DOI] [PubMed] [Google Scholar]
- Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby EA, & Joiner TE Jr (2010). The interpersonal theory of suicide. Psychological review, 117(2), 575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Velkoff EA, & Smith AR (2019). Examining patterns of change in the acquired capability for suicide among eating disorder patients. Suicide and Life-Threatening Behavior, 49(4), 1032–1043. [DOI] [PubMed] [Google Scholar]
- Willoughby T, Heffer T, & Hamza CA (2015). The link between nonsuicidal self-injury and acquired capability for suicide: A longitudinal study. Journal of Abnormal Psychology, 124(4), 1110. [DOI] [PubMed] [Google Scholar]
- Wolford-Clevenger C, Stuart GL, Elledge LC, McNulty JK, & Spirito A (2019). Proximal Correlates of Suicidal Ideation and Behaviors: A Test of the Interpersonal-Psychological Theory of Suicide. Suicide and Life-Threatening Behavior. Advanced publication online. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yurek LA, Vasey J, & Sullivan Havens D (2008). The use of self-generated identification codes in longitudinal research. Evaluation Review, 32(5), 435–452. [DOI] [PubMed] [Google Scholar]
- Zuromski KL, Cero I, & Witte T,K (2018). Non-monotonic temporal variation in fearlessness about death: A latent class growth analysis. Psychiatric Research, 268, 45–52. [DOI] [PubMed] [Google Scholar]