

Introduction
Globally, breast and cervical cancers are the two most common causes of cancer deaths in women age 15-65 years. Of the estimated 592,000 premature deaths from the two cancers in 2020, nearly 90% occurred in low- and middle-income countries.1 The recently launched WHO Global Strategy to Accelerate the Elimination of Cervical Cancer and Global Breast Cancer Initiative both promote the strengthening of comprehensive cancer control with improved access to effective interventions.2,3 Although countries expand access, it is critical that they are able to measure the impact of scale-up over time. At the population level, cancer-specific incidence, survival, and mortality are the core indicators for assessing cancer burden trends.4 Ideally, incidence and survival are provided through a population-based cancer registry and mortality through vital statistics of each country. However, these health information systems are underdeveloped in many resource-constrained countries with high cancer burden. With regard to vital statistics, the WHO shows that only 25% of countries have high-quality cause-of-death (CoD) data.5
Zambia is one of the countries facing challenges in collecting accurate CoD data. Through investigations, we noted that a substantial number of deaths occurred before their arrival at the facilities, and their CoD was not fully recorded, including those of breast and cervical cancers.
In this study, taking a case in Zambia as an example, we aimed to describe the actual challenges in counting cancer deaths that occur in communities and explore the utilization of automated verbal autopsy to improve the quality of cancer CoD data.
Challenges in Ascertaining CoD of Cases that Occurred in Communities in Zambia
In Zambia, the vital statistics system has greatly improved over the past several years; however, only one fifth of the estimated 206,224 deaths in the country were registered and certified in 2017.6 Among the certified cases, 36% of deaths were recorded with ill-defined and unknown CoD. One of the reasons is that a large proportion (approximately 55%) of deaths occur in the community.7 In a growing number of cases, when a death occurs, the deceased is taken to a health facility by the relatives to obtain a death notification form required for death registration and burial permission from the civil registration office.8 Investigations revealed that more than one third of deaths recorded at health facilities were those that occurred before their arrival (ie, brought-in-dead cases). Facility health information officers reported that the CoD of brought-in-dead cases was difficult to ascertain because of little medical information available regarding what led to death.
To examine the CoD of brought-in-dead cases, we conducted a study at the University Teaching Hospital, the largest public tertiary hospital in Zambia, between May and August, 2017. The details of this study have been described elsewhere.8 In brief, for 1,571 brought-in-dead cases more than 1 month old, trained staff interviewed the deceased's relatives and CoD was derived using SmartVA, an automated verbal autopsy computer program validated in previous studies and recommended by the WHO.9-11 The CoD written in the officially issued death notification form was also retrieved for each case. Through this study, we found erroneous descriptions (eg, recording of symptoms) and potential misclassification in nearly half of the death notification forms. Using SmartVA, the CoD of more brought-in-dead cases was determined, and the distribution of the top 10 causes of death substantially changed.
Comparison of Breast and Cervical Cancer Deaths Derived from Smartva and Death Notification Forms
In the current study, we compared cancer deaths derived from SmartVA and death notification forms. The sensitivity of verbal autopsy for cancer diagnosis is reported to be relatively high among major disease categories.12-14
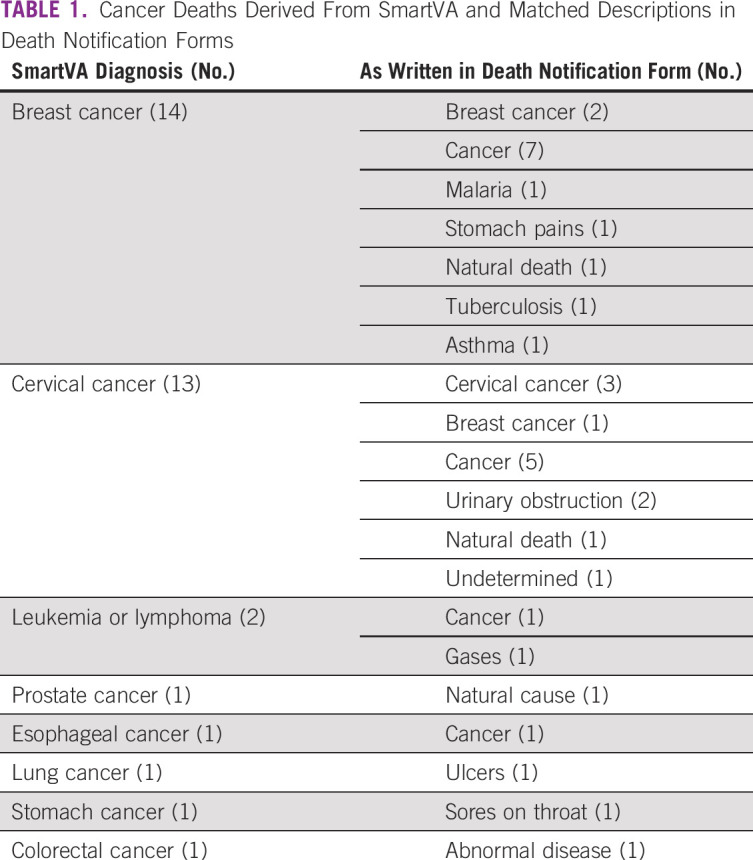
Of the 512 adult female brought-in-dead cases, 34 (6.6%) were diagnosed with cancer as CoD by SmartVA. Their mean age at death was 52.7 ± 16.3 years. Table 1 shows the cancer cases derived from SmartVA and the matched descriptions in the death notification forms. Although 14 cases were diagnosed with breast cancer by SmartVA, only two cases were in the death notification forms. Similarly, 13 cases were diagnosed with cervical cancer using SmartVA, but only three cases were in the death notification forms. This suggests that there may be about five times as many breast and cervical cancer deaths among brought-in-dead cases, as reported in death certificates and reflected in the vital statistics system. A large number of cases were recorded as cancer in the death notification forms, which should have been properly assigned to a specific cancer type to be certified as such.
TABLE 1.
Cancer Deaths Derived From SmartVA and Matched Descriptions in Death Notification Forms
Ethical approval was obtained from the University of Zambia's Biomedical Research Ethics Committee (018-12–16) and the Ethics Committee of the National Center for Global Health and Medicine in Japan (NCGM-G-002167-00). Written informed consent was obtained from the closest relatives of the deceased.
Need for Accurate Cancer Death Data and Utilization of Automated Verbal Autopsy
GLOBOCAN 2020 shows that breast and cervical cancers are the leading causes of cancer deaths in Zambia, with an estimated 400 and 1,900 deaths, respectively.1 In countries without a complete vital statistics system, these mortality estimates provide valuable information to understand the disease burden and set priorities at the national level. Indeed, Zambia is a leader among countries in strengthening cancer control under the National Cancer Control Strategic Plan 2016-2021, which prioritizes breast and cervical cancers, along with prostate and retinoblastoma.15 Through expanded access to awareness, prevention, early detection, treatment, and care, the plan aims to reduce mortality of each cancer type by 25% by 2025. For monitoring progress, however, it is essential that the number of cancer deaths be correctly counted and recorded.
To improve CoD data, there is a need to systematically certify the deaths that occur in the community in a better way. The application of physician-certified verbal autopsy, in which trained physicians identify CoD using interview data, is an option. However, this requires significant human and financial resources for training and implementation, and its nationwide expansion may be difficult in resource-constrained settings. The utilization of automated verbal autopsy, which allows operation by nonmedical staff, may be a more practical approach for routine implementation.16 Since a growing number of death cases are carried to health facilities, recording better CoD for brought-in-dead cases can be an entry point for improvement, and the health sector can play a key role.17
In conclusion, our analysis suggests that breast and cervical cancer deaths occurring in the community may be substantially underreported in Zambia. Although many resource-limited countries are trying hard to expand access to cancer interventions, collecting accurate CoD data remains a major challenge. Utilization of automated verbal autopsies could help capture more accurate CoD data. No women should die from breast and cervical cancer without being counted.
ACKNOWLEDGMENT
The authors thank Dr Charles Mutemba, Dr Kennedy Malama, Dr Consity Mwale, Dr John Musuku, Dr Alex Makupe, Ms Alice Zimba, Ms Gift Izukanji, Mr Ernest Matafwali, and Mr Justine Katukula for their support in accessing medical records needed for the study, data collection, and data recording.
Sharon Kapambwe
Honoraria: MSD
No other potential conflicts of interest were reported.
SUPPORT
Supported by the Research Fund of Ministry of Health, Labour and Welfare of Japan and NCGM Intramural Research Fund, Japan (21A04).
DATA SHARING STATEMENT
The data sets generated and/or analyzed during the study are not publicly available due to ethical restriction (patient confidentiality) but are available from the corresponding author on reasonable request.
AUTHOR CONTRIBUTIONS
Conception and design: Rei Haruyama, Yuta Yokobori
Provision of study materials or patients: Yuta Yokobori
Collection and assembly of data: Rei Haruyama, Yuta Yokobori
Data analysis and interpretation: All authors
Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
The following represents disclosure information provided by the authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/go/authors/author-center.
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).
Sharon Kapambwe
Honoraria: MSD
No other potential conflicts of interest were reported.
REFERENCES
- 1.Ferlay J Laversanne M Ervik M, et al. : Global Cancer Observatory: Cancer Today. Lyon, France, International Agency for Research on Cancer, 2020. https://gco.iarc.fr/today [Google Scholar]
- 2.World Health Organization : Global strategy to accelerate the eliminate cervical cancer as a public health problem. 2020. https://www.who.int/publications/i/item/9789240014107
- 3.Anderson BO Ilbawi AM Fidarova E, et al. : The Global Breast Cancer Initiative: A strategic collaboration to strengthen health care for non-communicable diseases. Lancet Oncol:22:578-581, 2021 [DOI] [PubMed] [Google Scholar]
- 4.Pineros M Saraiya M Baussano I, et al. : The role and utility of population-based cancer registries in cervical cancer surveillance and control. Prev Med 144:106237, 2021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.World Health Organization : World health statistics 2018: Monitoring health for the SDGs, sustainable development goals. 2018. https://apps.who.int/iris/handle/10665/272596
- 6.Zambia Statistics Agency Ministry of Home Affairs : 2017 vital statistics report. 2020. https://www.zamstats.gov.zm/
- 7.Zambia Ministry of Home Affairs CSO, Ministry of Health : 2015/16 Zambia sample vital registration with verbal autopsy report. 2018. https://www.zamstats.gov.zm/
- 8.Yokobori Y Matsuura J Sugiura Y, et al. : Analysis of causes of death among brought-in-dead cases in a third-level Hospital in Lusaka, Republic of Zambia, using the tariff method 2.0 for verbal autopsy: A cross-sectional study. BMC Public Health 20:473, 2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Serina P Riley I Stewart A, et al. : Improving performance of the tariff method for assigning causes of death to verbal autopsies. BMC Med 13:291, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.James SL, Flaxman AD, Murray CJ: Performance of the tariff method: Validation of a simple additive algorithm for analysis of verbal autopsies. Popul Health Metr 9:31, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.World Health Organization : Verbal autopsy standards: Ascertaining and attributing cause of death. https://www.who.int/healthinfo/statistics/verbalautopsystandards/en/
- 12.Ganapathy SS Yi K Omar MA, et al. : Validation of verbal autopsy: Determination of cause of deaths in Malaysia 2013. BMC Public Health 17:653, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Polprasert W Rao C Adair T, et al. : Cause-of-death ascertainment for deaths that occur outside hospitals in Thailand: Application of verbal autopsy methods. Popul Health Metr 8:13, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Yang G Rao C Ma J, et al. : Validation of verbal autopsy procedures for adult deaths in China. Int J Epidemiol 35:741-748, 2006 [DOI] [PubMed] [Google Scholar]
- 15.Zambia Ministry of Health : National cancer control strategic plan 2016-2021. 2016. http://dspace.unza.zm/handle/123456789/5189
- 16.D'Ambruoso L Boerma T Byass P, et al. : The case for verbal autopsy in health systems strengthening. Lancet Glob Health 5:e20-e21, 2017 [DOI] [PubMed] [Google Scholar]
- 17.Yokobori Y Obara H Sugiura Y, et al. : Gaps in the civil registration and vital statistics systems of low- and middle-income countries and the health sector's role in improving the situation. Glob Health Med, 2021. 10.35772/ghm.2020.01103. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data sets generated and/or analyzed during the study are not publicly available due to ethical restriction (patient confidentiality) but are available from the corresponding author on reasonable request.