

Abstract
Adequate understanding and accurate characterization of normal and unusual root and canal morphology are essential requirements for successful root canal treatment. A new coding system for classifying root and canal morphology, accessory canals and anomalies has been introduced. In addition to technological advances related to experimental studies involving micro-computed tomography, the continuing clinical advances in magnification, illumination, imaging and intra-operative root canal treatment procedures have allowed clinicians to identify an increasingly wide range of anatomical variations in roots and canals in an attempt to achieve more predictable clinical outcomes. This review aims to provide a step-by-step explanation for the clinical application of the new coding system in dental practice, and to describe the anatomical variations in roots and canals for teeth scheduled for root canal treatment.
Keywords: Accessory canals, anatomy, anomalies, canal configuration, clinical practice, endodontics, new coding system, root, root canal morphology
HIGHLIGHTS.
This review article aims to discuss the applications of a new system for classifying root and canal morphology in clinical practice.
The application of the new coding system is a dynamic process that could vary during the various stages of root canal treatment procedures.
The systematic characterization of roots and canals using the new coding system has a significant impact on canal anatomy difficulty assessment and teaching.
INTRODUCTION
Effective root canal treatment requires a thorough knowledge and understanding of root canal anatomy (1). For decades, this topic has been the subject of numerous reports involving extracted teeth evaluated by various experimental methods from simple staining and clearing to the more advanced cone beam computed tomography (CBCT) and micro-computed tomography (microCT) techniques (2-5). This is in addition to the clinical studies involving 2D radiographic imaging as well as case reports that often describe anatomical variations and their methods of detection using various imaging techniques, magnification, and other technical intra-operative procedures (5-8).
A new classification system has been introduced that allows precise and accurate descriptions of root and canal morphology. It overcomes the inherent deficiencies of previous classification systems that do not provide an accurate categorisation of many canal systems (Fig. 1), especially those that are complex. The new system is also able to classify accessory canals and anomalies (9-12). Such complex anatomical variations become more evident with enhanced magnification and imaging facilities together with contemporary intra-operative root canal instrumentation and filling techniques (13).
Figure 1.
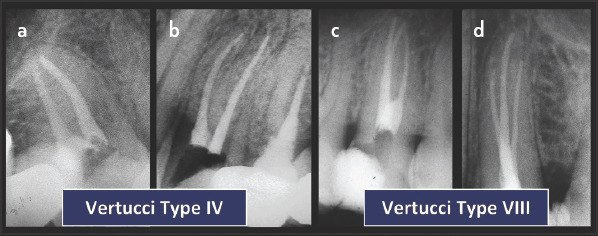
The Vertucci classification did not consider the number of roots in maxillary premolar teeth. (a, b) Single and double rooted maxillary premolar teeth with 2 separate canals are classified as Vertucci type IV. (c, d) Double and three rooted maxillary premolars with 3 separate canals are classified as Vertucci type VIII (Fig. 1c, d: reproduced from Ahmed and Cheung (15) with permission from Quintessence publishing)
A recent review has provided a detailed description for the application of the new coding system when undertaking laboratory-based microCT studies and in vivo studies using CBCT with an emphasis on the basic concepts to be followed (14). Owing to the differences in methods of identification and interpretation of the root canals in research studies compared to clinical practice, and the importance of proper identification of root canals during different phases of root canal treatment procedures in addition to record keeping and legal concerns (16-18), this review aims to provide a detailed description for the use of the new coding system during the various phases of clinical management from pre-operative radiographic interpretation to root canal filling and follow-up.
Application of the new coding system in clinical practice
The basic concepts of the new coding system have been described previously (9-12), and a recent review has explained and elaborated the application of the new system in research studies involving microCT and CBCT (14). In general, the basic principles of the new coding system can be applied in a similar manner (such as the tooth number when using any of the numbering systems), number of roots and canal configuration) regardless of the diagnostic assessment method or setting (experimental or clinical) (Fig. 2); however, it is important to highlight that the application of the new classification system in clinical practice differs from its use in microCT and CBCT observational studies in several ways:
Figure 2.
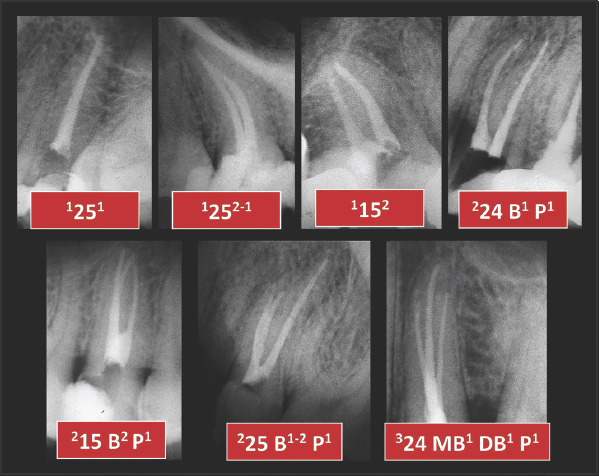
Basic concepts for the application of the new system in case reports. Tooth number with a superscript on the left for the number of roots, and superscript on the right of the tooth number for the canal configuration, or on the right of the respective root if double/multi-rooted. B: Buccal, P: Palatal, MB: Mesio-buccal, DB: Disto-buccal, P: Palatal
1) Before inclusion of teeth in microCT or CBCT studies, the collection of teeth should fulfil specific inclusion/exclusion criteria (such as teeth with complete root formation, teeth with no resorptive defects, no fractures, no root canal fillings, etc.). This is not followed in the majority of reports related to clinical practice where teeth scheduled for root canal treatment can have mature or immature roots, resorption defects or other pathological or iatrogenic changes in the root and/or canal evident on the peri-operative radiographic view(s).
2) Apart from primary root canal treatment, teeth may be scheduled for root canal retreatment or other treatment options such as tooth hemi-section, root amputation, and root-end surgery. All these treatment procedures may have an impact on how the clinician defines root canal morphology, and they should be considered before the application of the new coding system.
3) In contrast to microCT and CBCT observational studies, teeth scheduled for root canal treatment/retreatment procedures will pass through two main phases of canal anatomy interpretation:
a) Observation phase:
In this phase, the operator combines the information gained from the initial clinical examination (such as probing of the external root surface, detection of palato-gingival grooves, etc), and interpretation of the pre-operative 2D radiographic images with various projections (if needed) in addition to the axial, sagittal and coronal sections obtained from 3D CBCT imaging (if indicated).
b) Intervention phase:
In this phase, following access cavity preparation, the operator gains more information on root canal morphology through exploration using DG16 probes and other exploratory methods such as ultrasonic troughing, in addition to canal negotiation before moving on to canal instrumentation and root canal filling. At each step, the interpretation of the canal morphology is likely to evolve as described in detail in the following sections.
1) Pre-operative radiographic interpretation:
2D radiographic imaging:
Currently, 2D radiographic imaging is the tool used most often for pre-operative diagnostic procedures. It is well known that 2D imaging has inherent limitations since it provides a 2D image of a 3D object. However, pre-operative images with more than one horizontal projection can provide additional information on the bucco-lingual dimension of the tooth to help the clinician define the root and canal anatomy more precisely (13).
At this early stage, the new coding system can be used as an initial interpretation for the number of roots in a given tooth and the complexity of the canal system, which may evolve with different horizontal projections (Fig. 3). This initial interpretation has a significant relevance in dental schools since undergraduate students usually start their clinical practice with root canal treatment in teeth with simple canal morphological features compared to postgraduate students and dentists. It is important for such cases to be evaluated carefully pre-operatively to align with the level of knowledge and experience of the operator. Figure 3 is an example of a single-rooted mandibular right second premolar with an initial code of 1451; however, when changing the horizontal angulation, the code becomes 1451-2 in which the canal is bifurcated in the apical third of the root. This complexity is most likely not suitable for an undergraduate student because of difficulties related to canal instrumentation and filling. Three rooted mandibular molars (Radix Entomolaris – RE) with a code of (RE)3ManM M2 D1 DL1 is another example of an anatomical variation that may not be suitable for undergraduate students.
Figure 3.
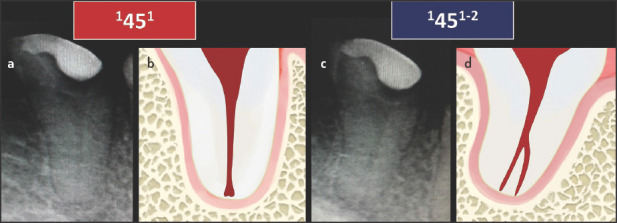
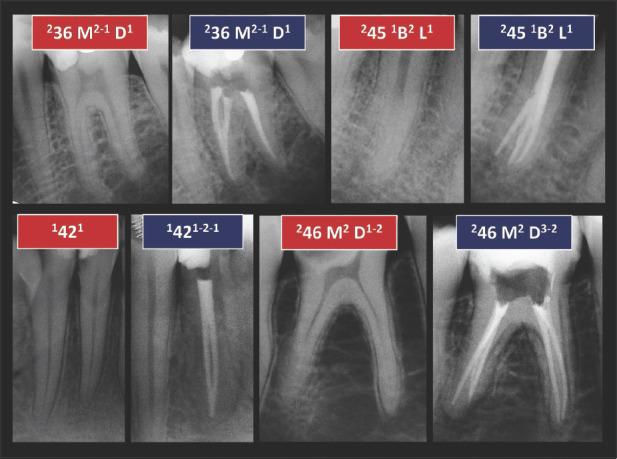
Application of the new coding system on tooth 45 with different horizontal angulation. (a, b) Striaght on periapical radiographic view showing the tooth with a code 1451, (c, d) After changing the horizontal angulation, the code becomes 1451-2
Table 1 shows examples for codes that may be suitable for undergraduate and postgraduate dental students. Indeed, such codes could vary based on the criteria and guidelines followed in a given country/dental school for preclinical and clinical endodontic teaching based on regulations from related dental associations and societies. It is also important to highlight that root canal anatomy is only one component used in the assessment of case difficulty (16, 17). Other factors such as patients with complex medical history, tooth position and inclination, canal curvatures, traumatic injuries, presence of endo-perio lesions, presence of radicular or coronal obstructions such as posts and/or crowns and accessibility, have to be evaluated alongside the root and canal anatomy to identify accurately the difficulty of a given case (16, 17).
TABLE 1.
An example for the application of the new coding system for defining case difficulty in teaching
| Early years undergraduate students | Final year undergraduate students | Postgraduate dental students | |
|---|---|---|---|
| Maxillary Teeth suitable | 1MaxA1 | 1MaxA1 | 1MaxA1 |
| for practice using the | 1MaxP1 | 1MaxP1 | 1MaxP1 |
| new coding system | 1MaxP2 | 1MaxP2 | 1MaxP2 |
| 1MaxP2-1 | 1MaxP2-1 | 1MaxP2-1 OR 1-2 | |
| 2MaxP B1 P1 | 2MaxP B1 P1 | 2MaxP B1 P1 | |
| 3MaxM MB1 DB1 P1 | 3MaxM MB1 DB1 P1 | ||
| 3MaxM MB2-1 DB1 P1 | 3MaxM MB2-1 DB1 P1 | ||
| 3MaxM MB2 DB1 P1 | 3MaxM MB2 DB1 P1 | ||
| Mandibular Teeth suitable | 1ManA1 | 1ManA1 | 1ManA1 |
| for practice using the | 1ManP1 | 1ManP1 | 1ManP1 |
| new coding system | 1ManP2-1 | 1ManP2-1 | 1ManP2-1 OR 1-2 |
| 1ManP2 | 1ManP2 | 1ManP2 | |
| 2ManM M1 OR 1-2 OR 2 D1 OR 1-2 OR 2 | 2ManM M1 OR 1-2 OR 2D1 OR 1-2 OR 2 | ||
| Anomalies suitable for | None | None | Accessory roots such as |
| practice using the | Radix Entomolaris: | ||
| new coding system | 3ManM MO-C-F DO-C-F DLO-C-F | ||
| Three-rooted max premolar: | |||
| 3MaxP MB1 DB1 P1 |
MaxA: Maxillary Anterior, MaxP: Maxillary Premolar, MaxM: Maxillary Molars, ManA: Mandibular Anteriors, ManP: Mandibular Premolars, ManM: Mandibular Molars
The same concept can also be applied to general dental practitioners (GDPs)/dental officers, in which some cases may have complex root(s) and/or canal(s) and when it is often advisable to refer such cases to a specialist. Figure 4 is an example of a double-rooted mandibular left second premolar (tooth 45) with a complex root and canal morphology, initial code is 245 1B2 L1, in which the buccal root is suspected to have more than one canal because of the break-point appearance, which indicates the presence of canal splitting apical to the common canal in the buccal and lingual roots. Figures 5 and 6 are examples of double-rooted mandibular molars with root dilacerations in one or both roots, which may require specialist treatment.
Figure 4.
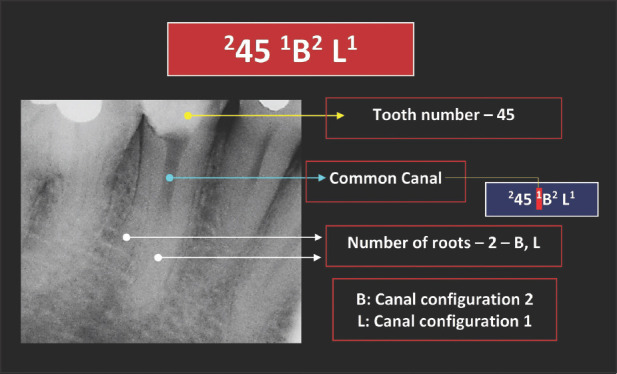
Application of the new system for complex cases indicated for primary root canal treatment
Figure 5.
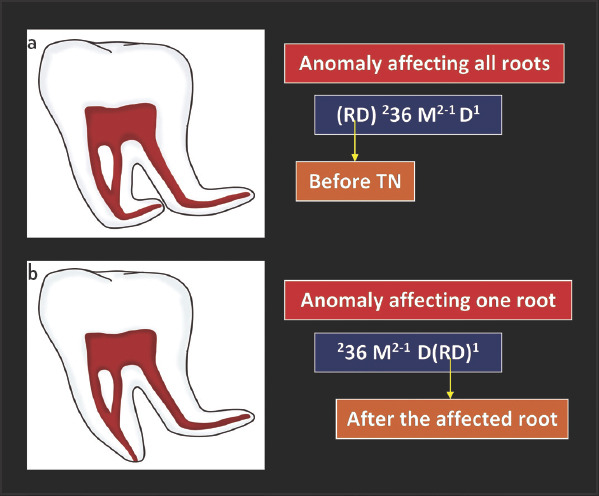
Application of the new coding system of complex root anatomy – RD: Root Dilaceration. (a) Root dilaceration affecting both roots. (b) Root dilaceration affecting one root (the distal root)
Figure 6.
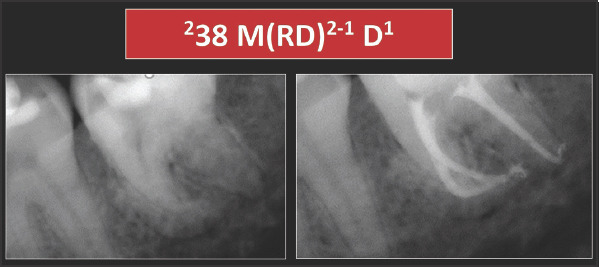
Application of the new coding system during the pre-operative assessment of complex root anatomy – RD: Root Dilaceration. 238 M(RD)2-1 D1 refers to a double rooted tooth 38 in which the mesial root is dilacerated and has configuration 2-1 and the distal root has a single root canal
Clinical cases scheduled for root canal retreatment must also be evaluated carefully. Figure 7 shows a 2D preoperative radiographic image of a previously root canal treated single-rooted maxillary left central incisor (tooth 21) with an initial code of 1211-2 in which the tooth has a missed second canal bifurcating from the main canal in the apical third of the root (canal configuration 1-2). It is obvious that such a case is more suitable for a specialist because of potential challenges in locating the missed canal after removal of the existing canal filling, negotiation and subsequent retreatment procedures. On the other hand, the neighbouring tooth coded as 1221 can be retreated by a GDP or a postgraduate student (based on the regulations followed in a given country or institution) since the canal does not have complex anatomy.
Figure 7.
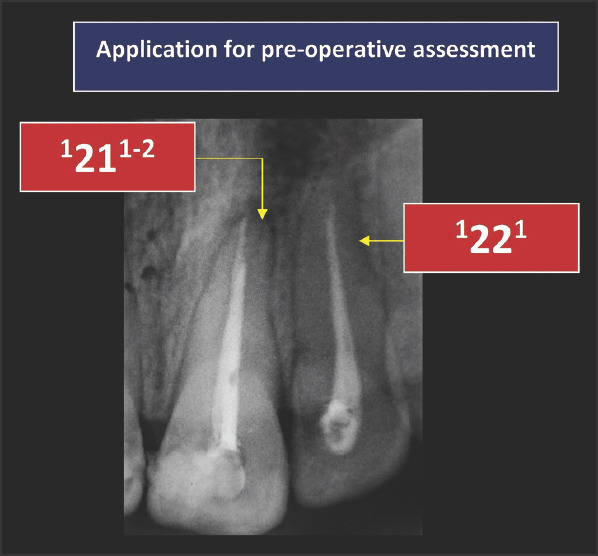
An example for two different codes for maxillary incisors that may indicate the suitability of retreatment by a GDP/postgraduate student (1221) or a specialist (1211-2)
Accessory canals (small canals leaving the main root canal that usually communicate with the external surface of the root or furcation) can rarely be seen on pre-operative 2D radiographic images; however, the presence of a lateral radiolucency is usually a landmark for its presence (Fig. 8). A new coding to classify accessory canals has been introduced (10), and further explained when applied in studies involving microCT and CBCT (14). In clinical practice (pre-operative stage), the operator can consider the possibility of the presence of this minor anatomy in the initial codes as shown in Figure 8.
Figure 8.
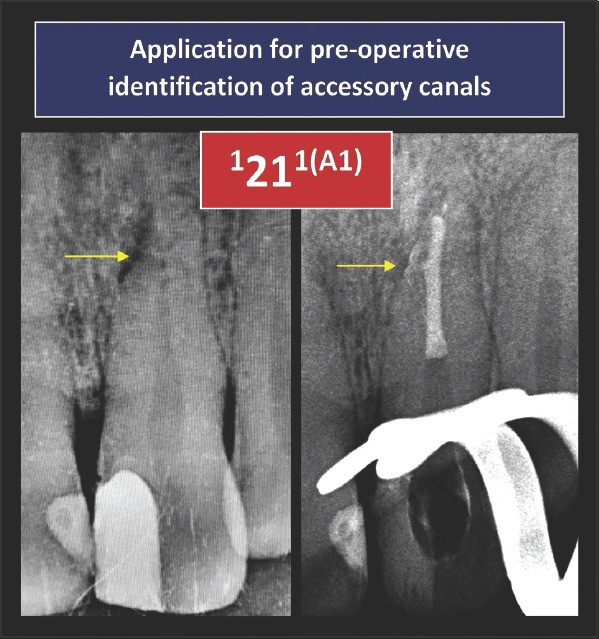
The presence of a lateral radiolucency in preoperative 2D radiographic images is a landmark for the presence of accessory canals. Code 1211(A1) refers to a single rooted tooth 21 having one root canal and one patent accessory canal in the apical third “A” of the root
Similar to microCT and CBCT studies, the operator can add information related to root and canal anomalies in the initial codes if the anatomy can be identified during clinical examination and pre-operative radiographic images (Fig. 9). Notably, on some occasions, the operator will not be able to identify the abnormality/anomaly (such as C-shaped canals) on 2D radiographic images until treatment has commenced. The type of the anomaly can be added later along the course of treatment (if identified). Indeed, a pre-operative CBCT image will provide more information when such a view is indicated.
Figure 9.
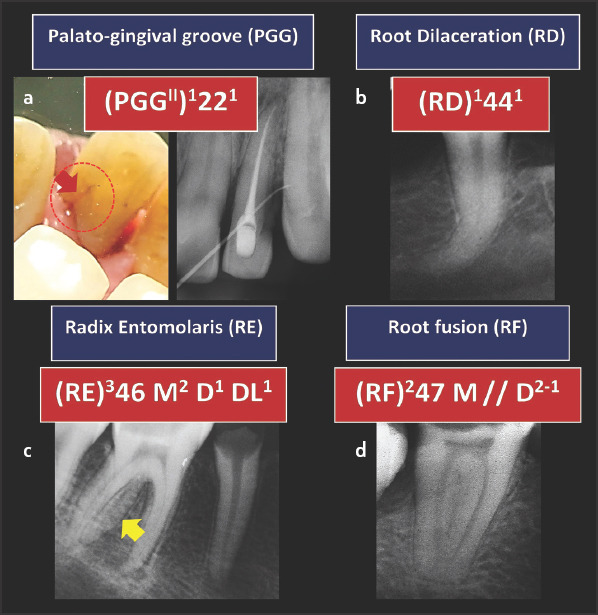
Application of the new system to address anomalies (clinical examination and preoperative radiographic views). (a) (PGGII)1221 refers to a single rooted tooth 22 with a palato-gingival groove (PGG) type II and a single root canal. (b) (RD)1441 refers to a single rooted dilacerated tooth 44 with and a single root canal. (c) (RE)346 M2 D1 DL1 refers to a three rooted tooth 46 with a radix entomolaris (RE – the exact type cannot be identified since it is a 2D image) – the mesial root (M) has 2 canals while each of the distal (D) and distolingual (DL) has one canal. (d) (RF)247 M//D2-1 refers to a double rooted tooth 47 with fused mesial and distal roots with merged canals (//) at the apical terminus – configuration 2-1
Apart from its ability to classify root numbers and configuration, canal configurations, accessory canals and anomalies, the new coding system can also be used to identify the stage of root formation, which have clinical implications in treatment planning and management (Fig. 10). It can also classify pathological changes affecting the root and/or canal such as internal and external root resorption defects, perforation (either iatrogenic or pathological), canal obliteration and other variations (Fig. 10).
Figure 10.
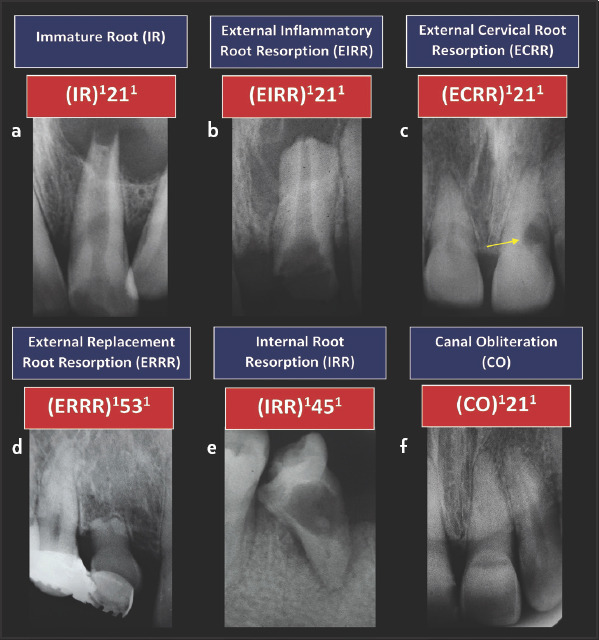
Applications of the new coding system to address other morphological and pathological changes in the root and canal
Cone beam computed tomography:
In some clinical situations, conventional 2D radiographic images provide limited information, and further details need to be identified (13). CBCT is an accurate and reliable diagnostic tool for the assessment of root and canal anatomy as well as a range of pathological changes in the root and canal such as resorption defects and cases scheduled for root canal retreatment procedures because of missed canals or iatrogenic errors (19).
The basic concepts and guidelines for using the new coding system in CBCT clinical studies have been described recently (14), which can also be applied for case reports. In order to provide a consistent interpretation of the root canal configuration, the observer will have to determine the most apical position of the CEJ (cervical line) and level of the pulp floor in single and multi-rooted teeth, respectively, in order to determine the location of the canal orifice before writing the code of the tooth of interest (Figs. 11 and 12).
Figure 11.
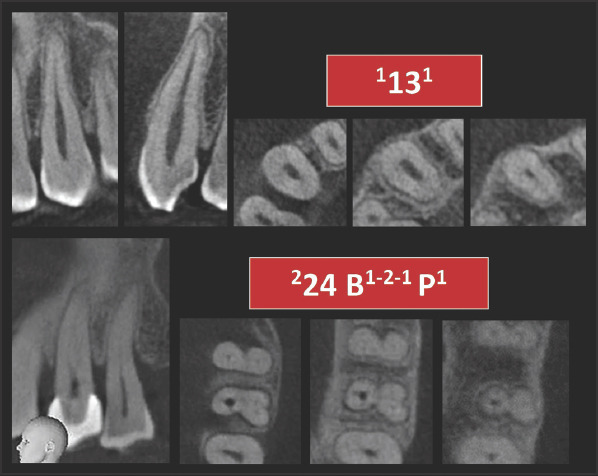
Application of the new coding system in CBCT reports (root and canal morphology). Code 1131 refers to a single rooted tooth 13 having one root canal. Code 224 B1-2-1 P1 refers to a double rooted tooth 24 in which the buccal (B) root has canal configuration 1-2-1 and the palatal root (P) has one root canal
Figure 12.
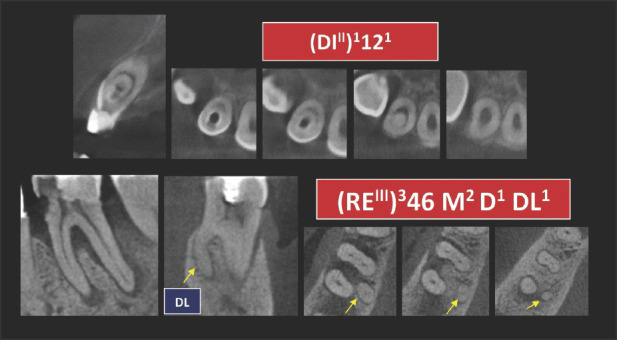
Application of the new coding system in CBCT reports (anomalies). Code (DIII)1121 refers to a single rooted tooth 12 having one root canal and a dens invaginatus (DI) type II (it is an enamel-lined form that invades the root but remains confined as a blind sac. Communication with the dental pulp may or may not occur in this type). (REIII)346 M2 D1 DL1 refers to a three rooted tooth 36 with radix entomolaris type III (Type III – curvature in the coronal third and additional buccal curvature from the middle third to the apical third of the root) in which the mesial root has two separate root canals and each of the distal (D) and distolingual (DL) roots has a single canal
In cases scheduled for root canal retreatment, the new coding system can be written in a way that highlights any missed roots and canals in the tooth scheduled for retreatment if present (Fig. 13), in addition to other iatrogenic procedural errors such as root perforations (Fig. 14). Accessory canals are not usually observed in CBCT studies; however, some accessory canals can be large enough to be identified on CBCT images (14), especially when the 2D radiographic image has a lateral radiolucency indicating the possibility of its presence; this may become evident after root canal filling.
Figure 13.
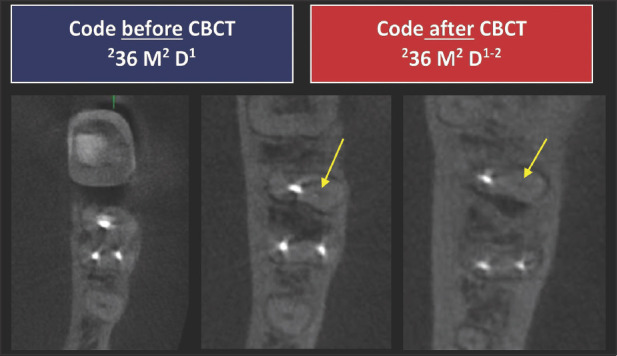
Use of the new coding system to describe cases scheduled for retreatment before and after CBCT diagnostic imaging. Before CBCT, the tooth was coded as 236 M2 D1; however, after CBCT scan, it is obvious that there is a missed second distal canal bifurcating from the main canal. Therefore, the code becomes 236 M2 D1-2
Figure 14.
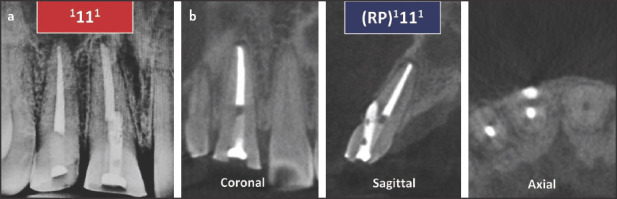
Application of the new system for describing teeth scheduled for root canal retreatment before and after CBCT imaging. RP – Root perforation. (a) In the 2D radiographic image, the tooth is coded as 1111. However, after CBCT scan (b), a root perforation was detected. Therefore, the code becomes (RP)1111
2) Intra-operative radiographic interpretation:
After access cavity preparation, the operator goes through various steps including exploration of the pulp chamber floor, orifice(s) detection, troughing (if needed), canal negotiation and exploration. Second mesio-buccal (MB) canals in maxillary molars and middle mesial (MM) canals in mandibular molars are examples of canals that are usually not identified in the pre-operative 2D radiographic images, and therefore, the initial codes given in the pre-operative phase will evolve during the intra-operative stage (Fig. 15). Indeed, this variation between pre- and intra-operative interpretation is reduced when a CBCT image is available (if indicated).
Figure 15.
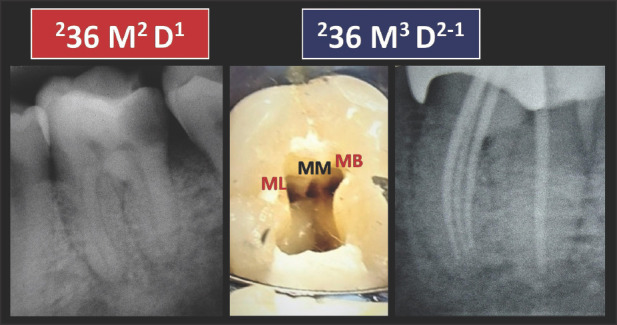
Application of the new coding system in the intra-operative stage. The code may change during intra-operative procedures. Based on the pre-operative radiographic image, this molar tooth was coded as 236 M2 D1. During intra-operative exploration, a middle mesial canal was identified, and the code changed after root canal treatment to code 236 M3 D2-1 (Reproduced from Ahmed and Luddin (20) with permission from Quintessence publishing)
After detection of canals and defining their configurations, the operator commences canal instrumentation using various manual and/or automated systems. Based on certain anatomical features and technical factors (such as presence of thin dentine septum between canals and use of greater taper files), the configuration of the prepared canals could vary from the initial interpretation made during the early exploratory intra-operative stage. For instance, after instrumentation, one canal may merge with the other canal as shown in Figure 16. Such changes in root canal configurations may also become evident in root canal retreatment procedures. On some occasions, under assisted magnification and following the use of root canal fillings using warm compaction techniques, the operator may detect intra-canal communications, which can be detected postoperatively by the movement of filling material between canals.
Figure 16.
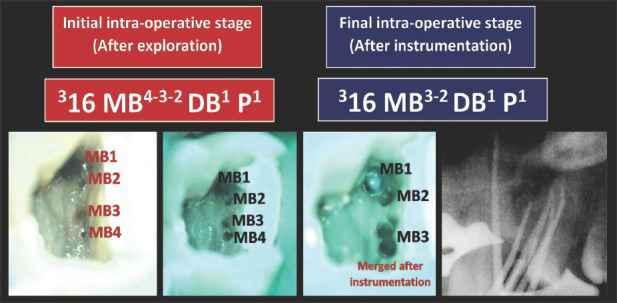
In the intra-operative, the root canal configuration is dynamic in nature – which may show changes along instrumentation. In this case, the initial intra-operative stage shows that the mesiobuccal (MB) root of the three rooted tooth 16 has 4 MB canals with a configuration 4-3-2 (tooth code 316 MB4-3-2 DB1 P1). However, after instrumentation, the MB3 and MB4 merged, and the code changed to 3-2 (tooth code 316 MB3-2 DB1 P1)
During root canal treatment, the operator may create procedural errors such as a ledge, zip or apical, mid-root, coronal or strip perforations. Such iatrogenic factors can be highlighted in the codes as explained above. Other treatment options such as root amputation, tooth hemisection and root-end surgery can also change the code of a given tooth – as explained below.
3) Post-operative radiographic interpretation
Post-operative radiographic images usually provide the definitive code of a given tooth. Figure 17 shows examples of teeth with codes during both the pre-operative assessment phase and post-operative phase.
Figure 17.
First row: Tooth having similar pre-operative and post-operative codes. Second row: Teeth showed post-operative codes different from the peri-operative assessment code
As mentioned in the intra-operative stage, a change in the root canal configuration may become evident after retreatment procedures. Figure 18 shows a CBCT image of double-rooted tooth 46 in which the mesial root has 2 separate canals and the distal root has one canal (code 246 M2 D1). After canal preparation and filling of the perforating resorption defect, the two mesial canals merged in the apical third, and the code becomes 246 M2-1 D1.
Figure 18.
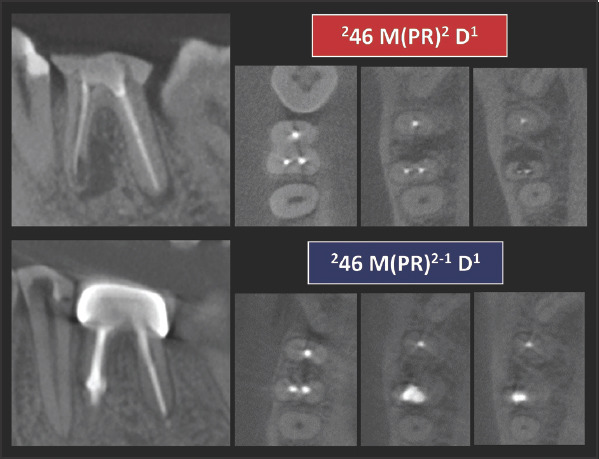
CBCT images showing changing the code before (a) and after (b) treatment of double rooted tooth 46 with extensive root resorption defect (Perforating Resorption – PR) in the mesial root
In some clinical situations, the outcome of treatment results in tooth hemisection or amputation of a root. The new system can address this change in the root and canal anatomy before and after treatment as shown in Figure 19. A “strikethrough” can be given to the code of the resected root.
Figure 19.

The application of the new coding system in teeth scheduled for tooth hemisection or amputation. The initial code of this tooth was 236 M2 D1. After root canal treatment of the distal root, the code becomes 236 M2 D2-1. After hemisection, the code can be written as 236 M2 D2-1
In some cases, the operator may identify “hidden” anatomy that was not detected in the pre- and/or intra-operative phase. Interpretation of the post-operative radiographic images is the common stage where accessory canals are identified after canal filling; however, the operator (up to that time) may not be able to define whether an accessory canal is patent or blind. Figure 20 shows cases with accessory canals identified after canal filling. Filling of inter-canal communications is another example of hidden anatomy that may not be identified at the intra-operative stage.
Figure 20.
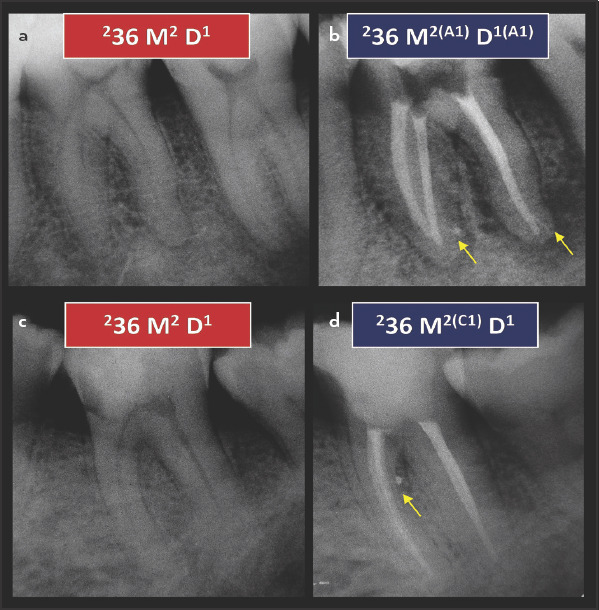
Application of the new coding system before and after treatment of molar with accessory canals. (a) Code 236 M2 D1 (Pre-operative), (b) Post-operative: Code 236 M2(A1) D1(A1) refers to double-rooted tooth 36 with 2 separate canals in the mesial root and one patent accessory canal in the apical third (A) and the distal root has one canal with one patent accessory canal in the apical third. (c) Code 236 M2 D1 (Pre-operative), (d) Post-operative: Code 236 M2 D1 refers to double-rooted tooth 36 with 2 separate canals in the mesial root and one patent accessory canal in the coronal third (C) and the distal root has one canal
Application of the new system in the primary dentition
The new coding system can also be used to describe canal morphology in the primary dentition as explained in a previous publication (21). Figure 21 shows its application before and after pulpectomy procedures in the anterior and posterior primary dentition.
Figure 21.
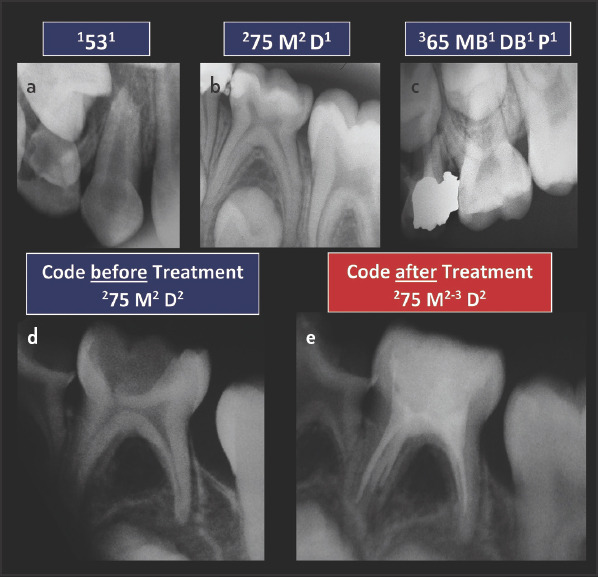
Application of the new system in the primary dentition. (a) Code 1531 refers to single-rooted tooth 53 having a single root canal, (b) Code 275 M2 D1 refers to double-rooted tooth 75 with 2 separate canals in the mesial root and the distal root has one canal. (c) Code 365 MB1 DB1 P1 refers to three-rooted tooth 65 in which each of the MB, DB and P roots has one canal configuration. (d) Pre-operative: Code 275 M2 D2 refers to double rooted-tooth 75 with 2 separate canals in each of the mesial and distal roots. (e) Post-operative: Code 275 M2-3 D2 refers to double rooted-tooth 36 with canal configuration 2-3 in the mesial root and the distal root has two separate canals
CONCLUSION
The new coding system for root and canal morphology has wide applications in clinical practice. This article explains, elaborates and provides a detailed discussion on its application in simple and complex root and canal anatomical variations identified using 2D radiographic and CBCT images as well as clinical exploration at different phases of root canal treatment. This systematic characterization of the root canal system has a significant impact on canal anatomy difficulty assessment and teaching.
Footnotes
Conflict of interest: The authors have no conflict of interest.
Ethics Committee Approval: Not applicable.
Peer-review: Externally peer-reviewed.
Financial Disclosure: Not applicable.
Authorship contributions: Concept – H.M.A.A.; Design – H.M.A.A.; Supervision – H.M.A.A., A.A.R.H., P.M.H.D.; Funding - None; Materials - None; Data collection &/or processing – None; Analysis and/or interpretation – H.M.A.A., A.A.R.H., P.M.H.D.; Literature search – H.M.A.A., A.A.R.H., P.M.H.D.; Writing – H.M.A.A., A.A.R.H., P.M.H.D.; Critical Review – H.M.A.A., A.A.R.H., P.M.H.D.
REFERENCES
- 1.Vertucci F. Root canal morphology and its relationship to endodontic procedures. Endod Top. 2005;10(1):3–29. [Google Scholar]
- 2.Vertucci F, Seelig A, Gillis R. Root canal morphology of the human maxillary second premolar. Oral Surg Oral Med Oral Pathol. 1974;38(3):456–64. doi: 10.1016/0030-4220(74)90374-0. [DOI] [PubMed] [Google Scholar]
- 3.Versiani MA, Ordinola-Zapata R, Keleş A, Alcin H, Bramante CM, Pécora JD, et al. Middle mesial canals in mandibular first molars:A micro-CT study in different populations. Arch Oral Biol. 2016;61:130–7. doi: 10.1016/j.archoralbio.2015.10.020. [DOI] [PubMed] [Google Scholar]
- 4.Kantilieraki E, Delantoni A, Angelopoulos C, Beltes P. Evaluation of Root and Root Canal Morphology of Mandibular First and Second Molars in a Greek Population:A CBCT Study. Eur Endod J. 2019;4(2):62–8. doi: 10.14744/eej.2019.19480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ahmed HMA, Rossi-Fedele G. Preferred Reporting Items for Root and Canal Anatomy in the Human Dentition (PROUD 2020) - A Systematic Review and a Proposal for a Standardized Protocol. Eur Endod J. 2020;5(3):159–76. doi: 10.14744/eej.2020.88942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hashem AAR, Ahmed HMA. Endodontic Management of a Mandibular First Molar with Unusual Canal Morphology. Eur Endod J. 2017;2(1):1–4. doi: 10.5152/eej.2017.17042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Azim AA, Deutsch AS, Solomon CS. Prevalence of middle mesial canals in mandibular molars after guided troughing under high magnification:an in vivo investigation. J Endod. 2015;41(2):164–8. doi: 10.1016/j.joen.2014.09.013. [DOI] [PubMed] [Google Scholar]
- 8.Ahmed HM, Hashem AA. Accessory roots and root canals in human anterior teeth:a review and clinical considerations. Int Endod J. 2016;49(8):724–36. doi: 10.1111/iej.12508. [DOI] [PubMed] [Google Scholar]
- 9.Ahmed HMA, Versiani MA, De-Deus G, Dummer PMH. A new system for classifying root and root canal morphology. Int Endod J. 2017;50(8):761–70. doi: 10.1111/iej.12685. [DOI] [PubMed] [Google Scholar]
- 10.Ahmed HMA, Neelakantan P, Dummer PMH. A new system for classifying accessory canal morphology. Int Endod J. 2018;51(2):164–76. doi: 10.1111/iej.12800. [DOI] [PubMed] [Google Scholar]
- 11.Ahmed HMA, Dummer PMH. A new system for classifying tooth, root and canal anomalies. Int Endod J. 2018;51(4):389–404. doi: 10.1111/iej.12867. [DOI] [PubMed] [Google Scholar]
- 12.Ahmed HMA, Dummer PMH. Advantages and Applications of a New System for Classifying Roots and Canal Systems in Research and Clinical Practice. Eur Endod J. 2017;3(1):9–17. doi: 10.5152/eej.2017.17064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Abella F, Morales K, Garrido I, Pascual J, Duran-Sindreu F, Roig M. Endodontic applications of cone beam computed tomography:case series and literature review. G Ital Endod. 2015;29(2):38–50. [Google Scholar]
- 14.Ahmed HMA, Ibrahim N, Mohamad NS, Nambiar P, Muhammad RF, Yusoff M, et al. Application of a new system for classifying root and canal anatomy in studies involving micro-computed tomography and cone beam computed tomography - Explanation and elaboration. Int Endod J. 2021;54(7):1056–1082. doi: 10.1111/iej.13486. [DOI] [PubMed] [Google Scholar]
- 15.Ahmed HMA, Cheung GS. Accessory roots and root canals in maxillary premolar teeth:a review of a critical endodontic challenge. ENDO - Endod Prac Today. 2012;6(1):7–18. [Google Scholar]
- 16.Shah PK, Chong BS. A web-based endodontic case difficulty assessment tool. Clin Oral Investig. 2018;22(6):2381–8. doi: 10.1007/s00784-018-2341-1. [DOI] [PubMed] [Google Scholar]
- 17.AAE Endodontic Case Difficulty Assessment Form and Guidelines. AAE. 2019. [Accessed Feb 17, 2021]. Available at: https://www.aae.org/specialty/wp-content/uploads/sites/2/2019/02/19AAE_CaseDifficultyAssessmentForm.pdf .
- 18.Ahmed HMA. Endodontics and forensic personal identification:An update. Eur J Gen Dent. 2017;6(1):5–8. [Google Scholar]
- 19.Patel S, Brown J, Pimentel T, Kelly RD, Abella F, Durack C. Cone beam computed tomography in Endodontics - a review of the literature. Int Endod J. 2019;52(8):1138–52. doi: 10.1111/iej.13115. [DOI] [PubMed] [Google Scholar]
- 20.Ahmed HMA, Luddin N. Accessory mesial roots and root canals in mandibular molar teeth:Case reports, SEM analysis and literature review. ENDO Endod Prac Today. 2012;6(3):195–205. [Google Scholar]
- 21.Ahmed HMA, Musale PK, El Shahawy OI, Dummer PMH. Application of a new system for classifying tooth, root and canal morphology in the primary dentition. Int Endod J. 2020;53(1):27–35. doi: 10.1111/iej.13199. [DOI] [PubMed] [Google Scholar]