

Abstract
BACKGROUND
Primary omental tumors are uncommon, and omental fibromas account for 2% of these tumors. Due to the low incidence of omental fibromas and the limited relevant literature, it is challenging for clinicians to make an accurate diagnosis of this condition, especially before surgery.
CASE SUMMARY
A 30-year-old man was admitted to the hospital because of a left epididymal mass with vague discomfort for more than 1 mo. A physical examination was performed, and the findings showed that the epididymal mass may have entered the abdominal cavity. Pelvic computed tomography was performed in our hospital and revealed a left inguinal hernia with a mass in the hernial contents, and no masses were found in the left epididymis. A traditional inguinal hernia incision was made. Intraoperative hernia contents were found to be of the greater omentum, and a 2.5 cm-diameter mass was found at the distal end of the greater omentum. The scrotum and epididymis did not exhibit other masses. Then, the mass of the greater omentum was excised. Intraoperative frozen pathological examination suggested a spindle cell tumor. The postoperative pathological examination suggested that the mass was an omental angiofibroma. Postoperatively, the patient recovered well and was discharged. Outpatient re-examinations were performed at 1 mo and half a year after the operation and showed no obvious abnormalities.
CONCLUSION
Due to the low morbidity rate associated with and latent nature of omental tumors, these tumors are difficult to diagnose preoperatively; thorough medical history taking, detailed physical examinations, and necessary imaging auxiliary examinations can help clinicians diagnose and treat these cases.
Keywords: Diagnosis, Epididymal mass, Omental mass, Inguinal hernia, Angiofibroma, Case report
Core Tip: Primary omental tumors are not common, and omental fibromas account for 2% of these tumors. No previous studies have reported an omental fibroma combined with indirect hernia showing an epididymal mass. This case reminds us of the importance of detailed medical history, strict physical examination, and necessary imaging examinations when clinicians dealing with similar cases.
INTRODUCTION
Primary omental tumors are not common, and omental fibromas account for 2% of these tumors[1-4]. Due to the low incidence of omental fibromas and the limited relevant literature, it is challenging for clinicians to make an accurate diagnosis of this condition[1,2,5]. No previous studies have reported an omental fibroma combined with indirect hernia showing an epididymal mass. Herein, we report a case of omental angiofibroma combined with an indirect inguinal hernia, as well as important information regarding the diagnosis and treatment of omental masses.
CASE PRESENTATION
Chief complaints
A 30-year-old man was admitted to the Urological Department of Tianjin First Central Hospital because of a left epididymal mass with vague discomfort for more than 1 mo.
History of present illness
One month before the patient visited the hospital, he underwent a scrotal ultrasonographic (US) examination at another hospital for scrotal vague discomfort, which illustrated that there was a mass within the left epididymis.
History of past illness
The patient did not have any previous history of chronic disease, surgery, blood transfusion, or trauma.
Personal and family history
The patient was not a smoker and drank little liquor occasionally. No family history of malignancy was identified.
Physical examination
A physical examination was performed, and the findings showed that the epididymal mass may have entered the abdominal cavity after the patient was admitted to the hospital. Small movement of the mass was felt when the patient coughed or performed a Valsalva maneuver.
Laboratory examinations
Routine blood tests, biochemical examinations, and alpha-fetoprotein, carcinoembryonic antigen, carbohydrate antigen-19-9, carbohydrate antigen-72-4, and neuron-specific enolase tests were performed, and all of the resulting values were within the normal ranges. The patient denied experiencing weight loss, decreased appetite, fatigue, or malaise.
Imaging examinations
The scrotal US examination performed at another hospital illustrated that there was a mass within the left epididymis. Pelvic computed tomography (CT) was performed in Tianjin First Central Hospital and showed intraperitoneal fat herniation in the left scrotum through the widened left inguinal canal, and the mass appeared as dense soft tissue within a hernia with a size of approximately 2.5 cm × 1.3 cm × 3.0 cm. The CT value was approximately 24 Hu (Figure 1). CT revealed a left inguinal hernia with a mass in the hernial contents, and no masses were found in the left epididymis.
Figure 1.
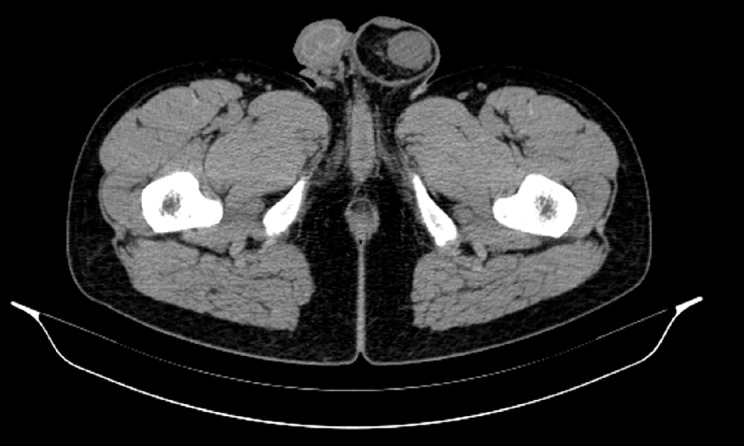
Pelvic computed tomography findings. Pelvic computed tomography showed that intraperitoneal fat herniate in the left scrotum through widened left inguinal canal, and there is a mass appearing as soft tissue density in hernia contents with a size of approximately 2.5 cm × 1.3 cm × 3.0 cm.
FINAL DIAGNOSIS
Intraoperative frozen pathological examination suggested a spindle cell tumor. Subsequently, inguinal hernia repair was performed. Postoperative pathological examination suggested that the mass was an omental angiofibroma (Figure 2), and the immunohistochemical examination showed Vimentin (+), CK (-), CD43 (+), SMA (-), S100 (-), CD31 (+), F8 (-), and Ki-67 sporadic positivity.
Figure 2.
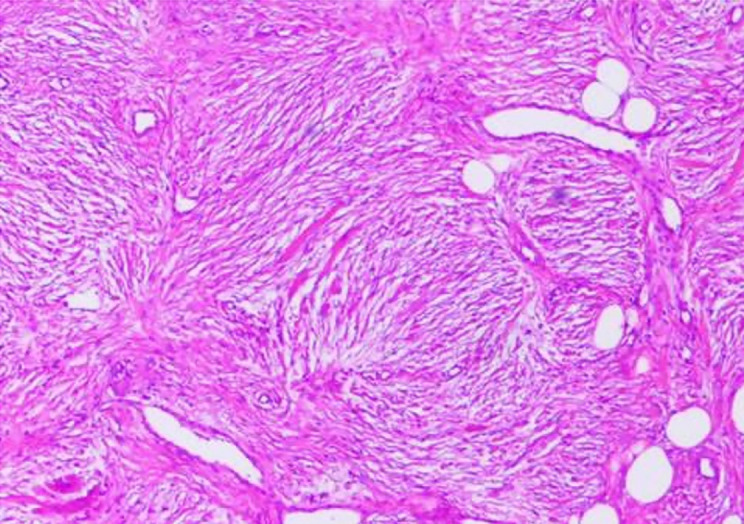
Histological findings revealed by hematoxylin and eosin staining of paraffin-embedded sections from the surgical specimen. Postoperative pathological examination suggested that the mass is omental angiofibroma (magnification × 100).
TREATMENT
A traditional inguinal hernia incision was made and served as the projection point from the outer upper part of the pubic tubercle to the internal ring orifice. Intraoperative hernia contents were found to be of the greater omentum, and a 2.5 cm-diameter mass was found at the distal end of the greater omentum. The scrotum and epididymis did not exhibit other masses. Then, a surgical mesh was placed in the inguinal canal and the mass at the distal end of the greater omentum was excised.
OUTCOME AND FOLLOW-UP
Postoperatively, the patient recovered well and was discharged. Outpatient re-examinations were performed at 1 mo and half a year after the operation and showed no obvious abnormalities.
DISCUSSION
The primary diagnosis for the patient was an epididymal mass. Clinically, diseases for which epididymal masses are the main manifestations include epididymal tuberculosis, seminal cysts, epididymal cysts, epididymal benign tumors, epididymal malignant tumors, etc. It is difficult to diagnose epididymal masses solely based on the patient’s medical history and clinical manifestations, and misdiagnoses easily occur. Epididymal masses are mainly identified on the basis of clinical manifestations such as the location, texture, and tenderness of the mass, combined with imaging modalities such as US, plain CT, and magnetic resonance imaging (MRI)[5-9].
The results of the physical examination and CT led us to diagnose the patient with left inguinal hernia. Inguinal hernias most commonly involve the small intestine, followed by the greater omentum. Preoperative imaging examinations alone, such as US and CT examinations, to determine hernia contents are prone to misdiagnosis. Michele et al[10] reported a patient who was diagnosed with an inguinal hernia and whose preoperative CT examination findings showed that the hernia content was of the small intestine, but the postoperative pathological examination demonstrated that the hernia content included Hodgkin's lymphoma. Tajti et al[11] also reported a patient who was diagnosed with an inguinal hernia and whose preoperative US examination findings showed that the hernia content was of an edematous intestinal loop with no circulation detected, but the hernia content was found to be of the gallbladder that was incarcerated during the operation. Taskovska and Janez[12] reported a patient who was diagnosed with an inguinal hernia and whose preoperative US examination findings showed that the hernia contents were of aperistaltic small intestine loops without dilatation, but the hernia content was found to be of the urinary bladder. In our study, the preoperative CT examination demonstrated that the hernia contents contained a mass that could not be diagnosed by imaging tests alone.
The vast majority of omental tumors are metastatic tumors. In contrast, tumors originating from the greater omentum are extremely rare, and the pathogenesis is still not clear. The most common clinical symptoms of omental tumors include abdominal pain, abdominal masses, and bloating. In most patients, abdominal pain is aggravated in the supine position and relieved in the upright position. Some patients also experience nausea and weight loss. In addition, the local symptoms of benign and malignant omental lesions are the same. In the initial stage when the tumor is small, as in the patient in this study, omental tumors are usually asymptomatic. Although imaging examinations are becoming increasingly popular and Chinese people are paying increasing attention to physical examination findings, primary omental tumors are still extremely rare[2,4].
The most common primary malignant omental tumors include leiomyosarcoma, hemangiopericytoma, and fibrosarcoma, and liposarcoma has also been reported[13-20]. The most common benign omental tumors include gastrointestinal stromal tumors, leiomyomas, lipomas, and fibroids. Only a few studies have reported cases of omental angiofibroma, and all of these cases were considered to be intra-abdominal[2,4]. No previous studies have reported an omental mass combined with indirect inguinal hernia showing an epididymal mass. In this study, a primary omental tumor herniated into the scrotum and formed an indirect inguinal hernia. The tumor was located near the epididymis. Therefore, US at another hospital showed an epididymal tumor.
In addition to regular preoperative examinations, US, CT, MRI, positron emission tomography (PET), and angiography can be used to detect omental tumors[2]. Abdominal US examinations are considered the first-line screening imaging examinations for most patients, as US can detect abdominal masses and distinguish cystic tumors from solid tumors. However, US usually cannot provide additional information about the tumor. For this reason, abdominal CT is the primary choice for the diagnosis of omental tumors. CT can provide more anatomical details, which can assist in determining the location of the primary tumor and indicate whether adjacent organs and tissues are significantly dislocated or compressed. MRI is another imaging modality that can help distinguish cystic tumors from solid tumors. MRI findings are not affected by the examiner, and contrast agents do not need to be prepared. However, MRI is time-consuming and expensive compared to other imaging methods. PET scans can also be used to help distinguish between benign and malignant tissues, necrotic scars, and active tumors when omental gastrointestinal stromal tumors are suspected. Angiography may also be helpful for patients suspected of having omental tumors. If angiography shows a tumor with rich blood supply in the greater omentum accompanied by neovascularization, it is likely to be malignant. At this time, angiography can also determine the distribution of supplying arteries and peripheral blood vessels of the tumor. At present, there is still considerable controversy about whether fine-needle aspiration biopsy should be performed for omental tumors. Although needle biopsy helps determine the pathological diagnosis preoperatively, it also increases the risk of tumor intra-abdominal implantation. However, these imaging examinations cannot help clinicians make an accurate preoperative diagnosis[2]. Usually, the definitive diagnosis still depends on postoperative pathological examination findings.
Total omentectomy is performed to treat primary omental tumors, as it seems to significantly improve the survival time of patients postoperatively, even with peritoneal implantation metastasis. The first symptoms of omental tumors can also be rupture-related bleeding and intestinal obstruction, requiring emergency surgery. The inability to safely remove the tumor due to local invasion is an absolute contraindication for surgical resection[21,22].
Owing to the rarity of primary omental tumors, the role of other adjuvant therapies, such as chemotherapy and radiotherapy, in the treatment of omental malignant tumors is currently unclear. In this study, because the intraoperative frozen pathological test results suggested a benign spindle cell tumor, only omental tumor resection and inguinal hernia repair were performed instead of total omental resection.
The pathology of this case was considered to be angiofibroma, which is mainly composed of proliferating blood vessels and fibrous tissue[23]. It mostly takes place in the nasopharynx of male adolescents, rarely occurs outside the nasopharyngeal area, and even more rarely occurs in the genitourinary system[24,25]. Studies have suggested that angiofibroma may originate from the periosteum of the skull base, but its exact pathogenesis is still not clear[1-3].
The median survival time of patients with primary malignant tumors of the greater omentum is only 6 mo. Two years after surgery, only approximately 10%-20% of patients are alive. The reasons for this poor prognosis are still unclear, potentially due to the small sample sizes of studies and the fact that some patients have had distant metastases at the time of admission. The prognosis of benign tumors of the greater omentum is significantly better than that of malignant tumors. Studies have reported that the 5-year survival rate for benign tumors of the greater omentum is approximately 75% and that this rate varies by the specific pathological type[1,2,4]. Due to the limited number of clinical studies on patients with omental tumors, there is no consensus on the postoperative management of patients with omental tumors. Some omental tumors, such as sarcoma, may recur and metastasize 20 years after surgery. Therefore, it is recommended that patients with omental tumors undergo long-term follow-ups after surgery[26]. In this study, although the postoperative pathology of this case was benign angiofibroma, we still recommended that the patient undergo active reexamination and follow-ups.
CONCLUSION
Due to the low morbidity rate associated with and latent nature of omental tumors, these tumors are difficult to diagnose preoperatively; thorough medical history taking, detailed physical examinations, and necessary imaging auxiliary examinations can help clinicians diagnose and treat these cases.
Footnotes
Informed consent statement: Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Conflict-of-interest statement: The authors declare that they have no conflict of interest to report.
CARE Checklist (2016) statement: The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Manuscript source: Unsolicited manuscript
Peer-review started: March 30, 2021
First decision: April 28, 2021
Article in press: August 4, 2021
Specialty type: Urology and nephrology
Country/Territory of origin: China
Peer-review report’s scientific quality classification
Grade A (Excellent): 0
Grade B (Very good): B
Grade C (Good): 0
Grade D (Fair): 0
Grade E (Poor): 0
P-Reviewer: Ferreira GSA S-Editor: Liu M L-Editor: Wang TQ P-Editor: Ma YJ
Contributor Information
Jia-Yi Liu, Department of Urology, Tianjin First Central Hospital, School of Medicine, Nankai University, Tianjin 300192, China.
Shuai-Qi Li, School of Medicine, Nankai University, Tianjin 300192, China.
Shi-Jie Yao, Department of Urology, Tianjin First Central Hospital, School of Medicine, Nankai University, Tianjin 300192, China.
Qian Liu, Department of Urology, Tianjin First Central Hospital, School of Medicine, Nankai University, Tianjin 300192, China. simonlq@163.com.
References
- 1.Ono M, Tanaka K, Ikezawa N, Kobayashi Y, Inoue Y, Yokota M, Matsumura S, Uehara I, Hattori Y, Kurahashi T, Shimada T, Nakagawa H. Fibroma of the omentum resembling an ovarian tumor in the pelvis. Keio J Med. 2009;58:234–236. doi: 10.2302/kjm.58.234. [DOI] [PubMed] [Google Scholar]
- 2.Iusco D, Donadei E, Sgobba G, Sarli L. Giant fibroma of the lesser omentum: report of a rare case. Acta Biomed. 2005;76:42–44. [PubMed] [Google Scholar]
- 3.Paksoy Y, Sahin M, Açikgözoğlu S, Odev K, Omeroğlu E. Omental fibroma: CT and US findings. Eur Radiol. 1998;8:1422–1424. doi: 10.1007/s003300050566. [DOI] [PubMed] [Google Scholar]
- 4.Ishida H, Ishida J. Primary tumours of the greater omentum. Eur Radiol. 1998;8:1598–1601. doi: 10.1007/s003300050594. [DOI] [PubMed] [Google Scholar]
- 5.Gao L, Song H, Mu K, Wang J, Guo B, Shi B, Li G. Primary epididymis malignant triton tumor: case report and review of the literature. Eur J Med Res. 2015;20:79. doi: 10.1186/s40001-015-0172-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bedir R, Şehitoğlu İ, Uzun H, Yurdakul C. Inflammatory pseudotumor of the epididymis: a case report and review of the literature. Turk J Urol. 2013;39:281–284. doi: 10.5152/tud.2013.068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Borges WM, Bechara GR, de Miranda MML, de Figueiredo GB, Venturini BA, Laghi CR. Epididymis tuberculosis: Case report and brief review of the literature. Urol Case Rep. 2019;26:100969. doi: 10.1016/j.eucr.2019.100969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Huang Y, Song J, Xu M, Zan Q. Primary Leydig cell tumour of epididymis: a rare case report with review of literature. Andrologia. 2013;45:430–433. doi: 10.1111/and.12049. [DOI] [PubMed] [Google Scholar]
- 9.Marcou M, Perst V, Cacchi C, Lehnhardt M, Vögeli TA. Epididymal leiomyoma: a benign intrascrotal tumour. Andrologia. 2017;49 doi: 10.1111/and.12689. [DOI] [PubMed] [Google Scholar]
- 10.Teodoro M, Mannino M, Vitale M, Mattone E, Palumbo V, Fraggetta F, Toro A, Di Carlo I. Small bowel lymphoma presenting as inguinal hernia: case report and literature review. World J Surg Oncol. 2018;16:91. doi: 10.1186/s12957-018-1396-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tajti J Jr, Pieler J, Ábrahám S, Simonka Z, Paszt A, Lázár G. Incarcerated gallbladder in inguinal hernia: a case report and literature review. BMC Gastroenterol . 2020;20:425. doi: 10.1186/s12876-020-01569-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Taskovska M, Janež J. Inguinal hernia containing urinary bladder-A case report. Int J Surg Case Rep. 2017;40:36–38. doi: 10.1016/j.ijscr.2017.08.046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Becker JHR, Koto MZ, Matsevych OY, Bida NM. Haemangiopericytoma/solitary fibrous tumour of the greater omentum. S Afr J Surg. 2014;52:111–113. doi: 10.7196/sajs.2274. [DOI] [PubMed] [Google Scholar]
- 14.Brañes A, Bustamante C, Valbuena J, Pimentel F, Quezada N. Primary leiomyosarcoma of the greater omentum: a case report. Int J Surg Case Rep. 2016;28:317–320. doi: 10.1016/j.ijscr.2016.10.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Okamoto K, Okada Y, Ohno K, Yagi T, Tsukamoto M, Akahane T, Shimada R, Hayama T, Tsuchiya T, Nozawa K, Matsuda K, Ishida T, Kondo F, Hashiguchi Y. A rare case of perivascular epithelioid cell tumor (PEComa) of the greater omentum. World J Surg Oncol. 2018;16:113. doi: 10.1186/s12957-018-1407-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Llenas-García J, Guerra-Vales JM, Moreno A, Ibarrola C, Castelbon FJ, Fernández-Ruiz M, Meneu JC, Ballestin C, Moreno E. Primary extragastrointestinal stromal tumors in the omentum and mesentery: a clinicopathological and immunohistochemical study. Hepatogastroenterology. 2008;55:1002–1005. [PubMed] [Google Scholar]
- 17.Schwartz RW, Reames M, McGrath PC, Letton RW, Appleby G, Kenady DE. Primary solid neoplasms of the greater omentum. Surgery. 1991;109:543–549. [PubMed] [Google Scholar]
- 18.Todoroki T, Sano T, Sakurai S, Segawa A, Saitoh T, Fujikawa K, Yamada S, Hirahara N, Tsushima Y, Motojima R, Motojima T. Primary omental gastrointestinal stromal tumor (GIST) World J Surg Oncol. 2007;5:66. doi: 10.1186/1477-7819-5-66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chauhan U, Udiya AK, Prabhu SM, Shetty GS. Malignant nerve sheath tumour of omentum and the "omental vascular pedicle sign". BJR Case Rep. 2016;2:20150037. doi: 10.1259/bjrcr.20150037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Urabe M, Yamagata Y, Aikou S, Mori K, Yamashita H, Nomura S, Shibahara J, Fukayama M, Seto Y. Solitary fibrous tumor of the greater omentum, mimicking gastrointestinal stromal tumor of the small intestine: a case report. Int Surg. 2015;100:836–840. doi: 10.9738/INTSURG-D-14-00141.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Alves M. Primary omental gastrointestinal stromal tumor- what we know based on case series and literature review. Eur J Surg Oncol. 2020;46:E135–E136. [Google Scholar]
- 22.Hashimoto S, Arai J, Nishimuta M, Matsumoto H, Fukuoka H, Muraoka M, Nakashima M, Yamaguchi H. Resection of liposarcoma of the greater omentum: A case report and literature review. Int J Surg Case Rep. 2019;61:20–25. doi: 10.1016/j.ijscr.2019.06.067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.López F, Triantafyllou A, Snyderman CH, Hunt JL, Suárez C, Lund VJ, Strojan P, Saba NF, Nixon IJ, Devaney KO, Alobid I, Bernal-Sprekelsen M, Hanna EY, Rinaldo A, Ferlito A. Nasal juvenile angiofibroma: Current perspectives with emphasis on management. Head Neck. 2017;39:1033–1045. doi: 10.1002/hed.24696. [DOI] [PubMed] [Google Scholar]
- 24.Pérez-Navarro JV, Flores-Cardoza A, Anaya-Prado R, González-Izquierdo Jde J, Ramírez-Barba EJ. Angiofibrolipoma of the greater omentum: case report and literature review. Cir Cir. 2009;77:229–232. [PubMed] [Google Scholar]
- 25.Windfuhr JP, Vent J. Extranasopharyngeal angiofibroma revisited. Clin Otolaryngol. 2018;43:199–222. doi: 10.1111/coa.12939. [DOI] [PubMed] [Google Scholar]
- 26.Vasdeki D, Bompou E, Diamantis A, Anagnostou A, Tepetes K, Efthimiou M. Haemangiopericytoma of the greater omentum: a rare tumour requiring long-term follow-up. J Surg Case Rep. 2018;2018:rjy087. doi: 10.1093/jscr/rjy087. [DOI] [PMC free article] [PubMed] [Google Scholar]