

Abstract
Background
Women have traditionally been underrepresented in randomized clinical trials (RCTs). We performed a systematic evaluation of the inclusion of women in cardiac surgery RCTs published in the past 2 decades.
Methods and Results
MEDLINE, EMBASE, and the Cochrane Library were searched (2000 to July 2020) for RCTs written in English, comparing ≥2 adult cardiac surgical procedures. The percentage of women enrolled and its association with year of publication, sample size, mean age, funding source, geographic location, number of sites involved, and interventions tested were analyzed using a meta‐analytic approach. Fifty‐one trials were included. Of 25 425 total patients, 5029 were women (20.8%; 95% CI, 17.6–24.4; range, 0.5%–57.9%). The proportion of women dropped significantly during the study period (29.6% in 2000 versus 13.1% in 2019, P<0.001). Women were significantly more represented in European trials (26.2%; 95% CI, 21.2–31.9), and less represented in trials of coronary bypass surgery versus other interventions (16.8%; 95% CI, 12.3–22.7 versus 33.6%; 95% CI, 27.4–40.5; P=0.0002) and in trials enrolling younger patients (P=0.009); the percentage of women was higher in industry‐sponsored versus non‐industry sponsored trials (31.7%; 95% CI, 27.2–36.6 versus 15.5%; 95% CI, 10.0–23.2; P=0.0004) and was not associated with trial sample size (P=0.52) or study design (multicenter versus monocenter: P=0.22). After exclusion of trials conducted at Veteran Affairs centers, women representation was 24.4% (95% CI, 21.1–28.0; range, 10.4%–57.9%), with no significant changes during the study period.
Conclusions
The proportion of women in cardiac surgery trials is low and likely inadequate to provide meaningful estimates of the treatment effect.
Keywords: cardiac surgery, RCT, women
Subject Categories: Cardiovascular Surgery
Nonstandard Abbreviations and Acronyms
- VA
Veteran Affairs
Clinical Perspective
What Is New?
-
‐
Women inclusion in cardiac surgery trials is low and likely inadequate to provide meaningful treatment effect estimates.
What Are the Clinical Implications?
-
‐
Substantial effort must be made by surgical trialists and funding agencies to promote the inclusion of women in cardiac surgery trials.
Women have traditionally been underrepresented in randomized clinical trials (RCTs) and, despite the efforts of funding agencies and of the academic community, this has not improved in recent years.1 While systematic analyses of the patients’ population included in clinical trials has been published for many fields of cardiology,1 no similar evaluation has been published for cardiac surgery.
An adequate women representation in cardiac surgical trials that supports evidence‐based practice is particularly important as female subjects have specific anatomic/functional characteristics and surgical outcomes2, 3, 4 and generalization of the surgical results obtained in a prevalently male population may be inappropriate and potentially harmful.
We have performed a systematic evaluation of the inclusion of women in the cardiac surgery trials published in the past 2 decades.
Methods
The data that support the findings of this study are available from the corresponding author upon reasonable request. This study follows the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses guidelines.5 As no individual patient was involved, ethical approval was not requested.
A comprehensive search to identify RCTs comparing ≥2 adult cardiac surgical procedures published from 2000 was performed in July 2020 (Ovid MEDLINE, Ovid EMBASE, and the Cochrane Library). The search strategy included the following terms: “CABG”, “off‐pump coronary surgery”, “on‐pump coronary surgery”, “arterial grafts”, “bilateral internal mammary artery”, “bilateral internal thoracic artery”, “radial artery”, “right gastroepiploic artery”, “arterial revascularization”, “saphenous vein graft”, “mitral valve repair”, “mitral valve replacement”, “tricuspid valve”, “aortic valve replacement”, “aortic valve repair”, “heart transplant”, and “ventricular assist device” (the full search strategy is reported in the Data S1). Studies performed on patients with congenital cardiac abnormalities were not included in the search.
Studies were included in the final analysis if they were RCTs written in English and compared ≥2 adult cardiac surgical procedures. In case of multiple publications from the same RCT, the report that better described the study population was selected. Two investigators (A.D.F., M.D.M.) performed data extraction independently; a third investigator (M.G.) verified data. Extracted data included publication year, sample size, mean age, number and percentage of women, funding source, geographic location, number of sites involved, interventions tested, and whether sex was tested as a potential treatment effect modifier.
Proportions were calculated using the metaprop function of meta package in R. Inverse variance method was used for data pooling. Subgroup analysis was performed using random effect. Logit‐transformation was performed to calculate CIs. DerSimonian‐Laird estimator was used to estimate between‐study variance. The Funnel plot and Egger test were used for estimation of publication bias.
As a sensitivity analysis, all comparisons were repeated after the exclusion of trials conducted at Veteran Affairs (VA) medical centers.
Results
Fifty‐one trials published between 2000 and 2020 were included (Table 1).6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55 The Preferred Reporting Items for Systematic Reviews and Meta‐Analyses flowchart is reported in Figure S1. The median sample size was 225 patients (interquartile range [IQR], 125–394); 21 trials (41.2%) were multicentric (median number of sites, 13; IQR, 7–24), 3 (5.9%) involved patients from VA medical centers, 27 (52.9%) were from Europe, 12 (23.5%) from North America, 5 (9.8%) from Asia/Australia/South America, and 7 (13.7%) involved multiple continents. The tested interventions were coronary artery bypass grafting in 37 trials (72.5%), valve surgery in 7 trials (13.7%), saphenous vein graft harvesting for bypass surgery in 2 trials (3.9%), ventricular remodeling in 2 trials (3.9%), use of mechanical assistance devices in 2 trials (3.9%), and ablation of atrial fibrillation in cardiac surgery patients in 1 trial (1.9%). Trials received institutional support in 28 cases (54.9%), private support in 6 cases (11.8%), or mixed support in 3 (5.9%) cases. Primary outcomes were clinical events in 31 trials (60.8%), patency in 12 trials (23.5%), imaging in 7 trials (13.7%), and hemodynamic data in 1 trial (1.9%).
Table 1.
Main Features of the Included Trials
| Study | Y | Total Sample Size (n) | Women (n) | Women (%) | Funding Source | Geographic Location | Multicenter/Monocenter | No. of Centers | Interventions Tested |
|---|---|---|---|---|---|---|---|---|---|
| Acker et al6 | 2014 | 251 | 96 | 38.2 | National Institutes of Health and the Canadian Institutes of Health | United States, Canada | Multicenter | 22 | MV repair vs MV replacement |
| ACORN7 | 2006 | 193 | 105 | 54.4 | The authors of this article received grant support (further details not specified) | United States, Canada | Multicenter | 29 | MV surgery+CorCap cardiac support device vs MV surgery alone |
| Al‐Ruzzeh et al8 | 2006 | 168 | 27 | 16.1 | NR | UK | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| ART9 | 2010 | 3102 | 446 | 14.3 | British Heart foundation (SP/03/001) and Medical Research Council (G0200390) | UK, Poland, Australia, Brazil, Italy, Austria, India | Multicenter | 28 | BITA vs SITA |
| BBS10 | 2010 | 339 | 121 | 35.7 | Danish Heart Foundation (08‐4‐R64‐ A2029‐B948‐22480), Danish Medical Research Council, Copenhagen Hospital Corporations Medical Research Council, Rigshospitalet Research Council, Aase and Ejnar Danielsens Foundation, Gangsted Foundation, and Danish Agency for Science, Technology, and Innovation | Denmark | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| BHACAS 1‐211 | 2002 | 401 | 72 | 17.9 | Garfield Weston Trust, Sir Siegmund Warburg’s Voluntary Settlement, and the British Heart Foundation | UK | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| CADENCE‐MIS12 | 2015 | 100 | 46 | 46 | Edwards Lifesciences LLC | Germany | Multicenter | 5 | Mini‐invasive AVR vs Full sternotomy AVR |
| Carrier et al13 | 2003 | 130 | 15 | 11.5 | NR | Canada | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| CARRPO14 | 2009 | 331 | 39 | 11.8 | Danish Heart Foundation and Lundbeck Foundation | Denmark | Monocenter | 1 | Total arterial revascularization vs SITA+SVG |
| CORONARY15 | 2012 | 4752 | 909 | 19.1 | Canadian Institutes of Health Research | Argentina, Australia, Brazil, Canada, Chile, China, Colombia, Czech Republic, Estonia, France, India, Italy, The Netherlands, Sweden, Turkey, Ukraine, UK, Uruguay, United States | Multicenter | 79 | OFF‐PUMP vs ON‐PUMP CABG |
| COTRIP16 | 2019 | 100 | 36 | 36 | Before starting this study, the protocol was given to both manufacturers. The study was then supported by an unrestricted grant from St. Jude Medical, Eschborn, Germany | Germany | Monocenter | 1 | Trifecta valve vs Perimount Magna Ease valve |
| CRISP17 | 2014 | 106 | 25 | 23.6 | Medical Research Council/NIHR Efficacy and Mechanism Evaluation programme | UK, India | Multicenter | 9 | OFF‐PUM vs ON‐PUMP |
| Czerny et al18 | 2001 | 80 | 13 | 16.2 | NR | Austria | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| DOORS19 | 2012 | 900 | 207 | 23.0 | Danish Heart Foundation, Danish Centre for Health Technology Assessment, Danish Research Council for Health Sciences, Tove and John Girott’s Foundation, Medtronic, Guidant, and Getinge | Denmark | Multicenter | 4 | OFF‐PUMP vs ON‐PUMP CABG |
| Falk et al20 | 2008 | 129 | 39 | 30.2 | NR | Germany | Multicenter | 2 | MV Surgery (Loop technique) vs MV Surgery (Resection) |
| Fattouch et al21 | 2009 | 128 | 40 | 31.2 | NR | Italy | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| Gillinov et al22 | 2016 | 260 | 120 | 46.1 | National Institutes of Health and the Canadian Institutes of Health Research | United States, Canada | Multicenter | 20 | MV Surgery+AF ablation vs MV Surgery alone |
| Glineur et al23 | 2016 | 304 | 40 | 13.1 | Grant no. 3.4600.04 from the Fonds de la recherché scientifique médicale, Brussels, Belgium | Belgium | Monocenter | 1 | BITA Y vs BITA IN SITU |
| Goldman et al24 | 2011 | 733 | 6 | 0.8 | The Veteran Affairs Cooperative Studies Program | United States | Multicenter | 11 | RA vs SVG |
| GOPCABE25 | 2013 | 2394 | 755 | 31.5 | Unrestricted grant from Maquet | Germany | Multicenter | 12 | OFF‐PUMP vs ON‐PUMP CABG |
| Halfwerk et al26 | 2019 | 125 | 33 | 26.4 | Maquet Netherlands (travel grant to present part of this work at the 2017 Society for Cardiothoracic Surgery Annual Meeting in Belfast) | The Netherlands | Monocenter | 1 | Minimal invasive extra corporeal circulation vs Advanced extra corporeal circulation in Aortic valve surgery |
| JOCRI27 | 2005 | 167 | 22 | 13.2 | Health and Labor Science Research Grant 14‐013 from the Japanese Ministry of Health, Labor, and Welfare | Japan | Multicenter | 5 | OFF‐PUMP vs ON‐PUMP CABG |
| Karolak et al28 | 2007 | 299 | 58 | 19.4 | Funding Sources Division of Cardiac Surgery and the Maritime Heart Centre at Dalhousie University (Halifax, Nova Scotia) | Canada | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| Khan et al29 | 2004 | 103 | 13 | 12.6 | The British Heart Foundation (PG/ 9912) and the Royal Brompton and Harefield National Health Service Trust Clinical Research Committee. Medtronic Inc. supplied the Octopus II equipment for the study free of cost | UK | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| Légaré et al30 | 2004 | 300 | 59 | 19.7 | Maritime Heart Center | Canada | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| Lemma et al31 | 2012 | 411 | 126 | 30.7 | Medtronic, Italy | Italy, Switzerland | Multicenter | 8 | OFF‐PUMP vs ON‐PUMP CABG |
| Lingaas et al32 | 2004 | 120 | 26 | 21.6 | NR | Norway | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| MASS III33 | 2010 | 308 | 65 | 21.1 | This work was supported partially by a research grant from the Zerbini Foundation, Sao Paulo, Brazil, and Medical School University of Sao Paulo | Brazil | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| Michaux et al34 | 2011 | 50 | 8 | 16 | Supported in part by the Swiss Society of Anesthesiology and Reanimation | Switzerland | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| Michler et al35 | 2016 | 301 | 96 | 31.9 | Funded by the National Institutes of Health and the Canadian Institutes of Health Research | United States , Canada | Multicenter | 26 | CABG+MV Repair vs CABG alone |
| Muneretto et al36 | 2003 | 176 | 69 | 39.2 | NR | Italy | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| Myers et al37 | 2000 | 162 | 48 | 29.6 | Supported in part by Marshfield Clinic Physician Research Specific Restricted Funds, and the Gwen D. Sebold Award | United States | Monocenter | 1 | Total arterial revascularization vs SITA+SVG |
| OCTOPUS38 | 2001 | 281 | 137 | 48.7 | Funded entirely by the Netherlands National Health Insurance Council | The Netherlands | Multicenter | 3 | OFF‐PUMP vs ON‐PUMP CABG |
| Pegg et al39 | 2008 | 60 | 8 | 13.3 | The British Heart Foundation, the Medical Research Council, and the Wellcome Trust | UK | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| PRAGUE‐440 | 2004 | 388 | 225 | 57.9 | Grant NA 6569–3 of the Internal Grant Agency of the Ministry of Health of the Czech Republic | Czech Republic | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| PRAGUE‐641 | 2016 | 206 | 86 | 41.7 | Supported by "P35 ‐ PRVOU" ‐ the Scientific Plan of Charles, University in Prague, the Czech Republic, granted by the Ministry of Health of the Czech Republic | Czech Republic | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| PROMISS42 | 2010 | 150 | 24 | 16 | Merck Foundation and Sociedade de Gestao Hospitalar Cruz Vermelha Portuguesa SA | Portugal | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| RAPCO RITA43 | 2010 | 394 | 41 | 10.4 | NR | Australia | Monocenter | 1 | RA vs RITA |
| RAPCO SVG43 | 2010 | 225 | 43 | 19.1 | NR | Australia | Monocenter | 1 | RA vs SVG |
| RAPS44 | 2004 | 541 | 75 | 13.9 | Grant (MT‐13883) from the Canadian Institutes of Health Research | Canada, New Zealand | Multicenter | 13 | RA vs SVG |
| REGROUP45 | 2019 | 1150 | 6 | 0.5 | Funded by the Cooperative Studies Program, Office of Research and Development, Department of Veterans Affairs | United States | Multicenter | 16 | Endoscopic SVG harvesting vs Open SVG harvesting |
| RESTOR‐MV46 | 2010 | 147 | 35 | 23.8 | The study was terminated when the sponsor failed to secure ongoing funding; Myocor, Inc., Maple Grove, Minnesota | United States , India | Multicenter | 21 | Coapsys ventricular reshaping vs standard surgery in patients submitted to CABG+MV Repair or CABG alone |
| ROOBY47 | 2009 | 2203 | 14 | 0.6 | The Department of Veterans Affairs Cooperative Studies Program | United States | Multicenter | 18 | OFF‐PUMP vs ON‐PUMP CABG |
| RSVP48 | 2008 | 103 | 5 | 4.8 | The Kate Weeke’s Fellowship, Royal College of Surgeon of England (Dr Chong), the Clinical Research Committee, Royal Brompton and Harefield NHS Trust (Dr Webb), the Victor Phillip Dahdaleh Charitable Foundation (Dr Webb) | UK | Monocenter | 1 | RA vs SVG |
| Shahin et al49 | 2005 | 96 | 38 | 39.6 | NR | The Netherlands | Monocenter | 1 | PYSHIO Ring vs Classic Ring |
| SMART50 | 2004 | 197 | 45 | 22.8 | Grants from Medtronic Inc and the Carlyle Fraser Heart Center Foundation (Atlanta, GA) | United States | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
| STAND‐In‐Y51 | 2009 | 409 | 236 | 57.7 | NR | Italy | Monocenter | 1 | RA vs SVG |
| STICH52 | 2009 | 1000 | 147 | 14.7 | Grants (5U01‐HL‐69015, 5U01‐HL‐69013, and 5U01‐HL‐69010) from the National Heart, Lung, and Blood Institute | Poland, Russia, Canada, United States, Italy, Czech Republic, Australia, Austria, Germany, Serbia, Lithuania, Singapore, Sweden, Thailand, Brazil, New Zealand, Uruguay, Norway, Hungary, Turkey, Malaysia, Greece, Belgium | Multicenter | 127 | CABG+Surgical ventricular reconstruction vs CABG alone |
| SUPERIOR SVG53 | 2019 | 250 | 31 | 12.4 | Heart and Stroke Foundation of Canada (Grant# 7092) and the Canadian Institutes of Health Research‐funded Canadian Network and Centre for Trials Internationally (CANNeCTIN) | Canada, Sweden, Israel | Multicenter | 12 | No touch SVG vs conventional SVG |
| Vukovic et al54 | 2019 | 100 | 28 | 28 | NR | Serbia | Monocenter | 1 | Ministernotomy vs conventional sternotomy in aortic valve surgery |
| Yu et al55 | 2014 | 102 | 25 | 24.5 | NR | China | Monocenter | 1 | OFF‐PUMP vs ON‐PUMP CABG |
AF indicates atrial fibrillation; AVR, aortic valve replacement; BITA, bilateral internal thoracic artery; CABG, coronary artery bypass grafting; MV, mitral valve; NIHR, National Institute for Health Research; NR, not reported; RA, radial artery; SITA, single internal thoracic artery; and SVG, saphenous vein graft.
List of trials’ acronyms: ACORN indicates Acorn Clinical Trial; ART, Arterial Revascularization Trial; BBS, Best Bypass Surgery Trial; BHACAS, Beating Heart Against Cardioplegic Arrest Studies; CADENCE‐MIS, EDWARDS INTUITY Valve System CADENCE‐MIS Study; CARRPO, Copenhagen Arterial Revascularization Randomized Patency and Outcome trial; CORONARY, CABG Off or On Pump Revascularization Study; COTRIP, Randomized Comparison of Trifecta and Perimount Magna Ease Supraannular Aortic Xenografts study; CRISP, Coronary Artery Bypass Grafting in High‐Risk Patients Randomised to Off‐ or On‐Pump Surgery; DOORS, Danish On‐Pump Versus Off‐Pump Randomization Study; GOPCABE, German Off‐Pump Coronary Artery Bypass Grafting in Elderly Patients; JOCRI, Japanese Off‐Pump Coronary Revascularization Investigation; MASS III, The Medicine, Angioplasty, or Surgery Study III; OCTOPUS, Early Outcome After Off‐Pump Versus On‐Pump Coronary Bypass Surgery; PRAGUE‐4; A randomized comparison between off‐pump and on‐pump surgery; PRAGUE‐6, Off‐pump versus on‐pump coronary artery bypass graft surgery in patients with EuroSCORE ≥6; PROMISS, Prospective Randomized Comparison of Off‐Pump and On‐Pump Multi‐Vessel Coronary Artery Bypass Surgery; RAPCO, Radial Artery Patency and Clinical Outcomes; RAPS, Radial Artery Patency Study; REGROUP, Randomized Endovein Graft Prospective Trial; RESTOR‐MV, Randomized Evaluation of a Surgical Treatment for Off‐Pump Repair of the Mitral Valve; ROOBY, Veteran Affairs Randomized On/Off Bypass Study; RSVP, Radial Artery Versus Saphenous Vein Patency Trial; SMART, Surgical Management of Arterial Revascularization Therapies Trial; STAND‐In‐Y, Arterial revascularization in primary coronary artery bypass grafting: direct comparison of 4 strategies; STICH, Surgical Treatment for Ischemic Heart Failure Trial; and SUPERIOR SVG, Surgical and Pharmacological Novel Interventions to Improve Overall Results of Saphenous Vein Graft Patency in Coronary Artery Bypass Grafting Surgery Trial.
Among the 25 425 patients included, there were 5029 women (20.8%, 95% CI, 17.6–24.4, range 0.5%–57.9%) (Figure 1).6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55
Figure 1. Proportions of women in cardiac surgery trials.
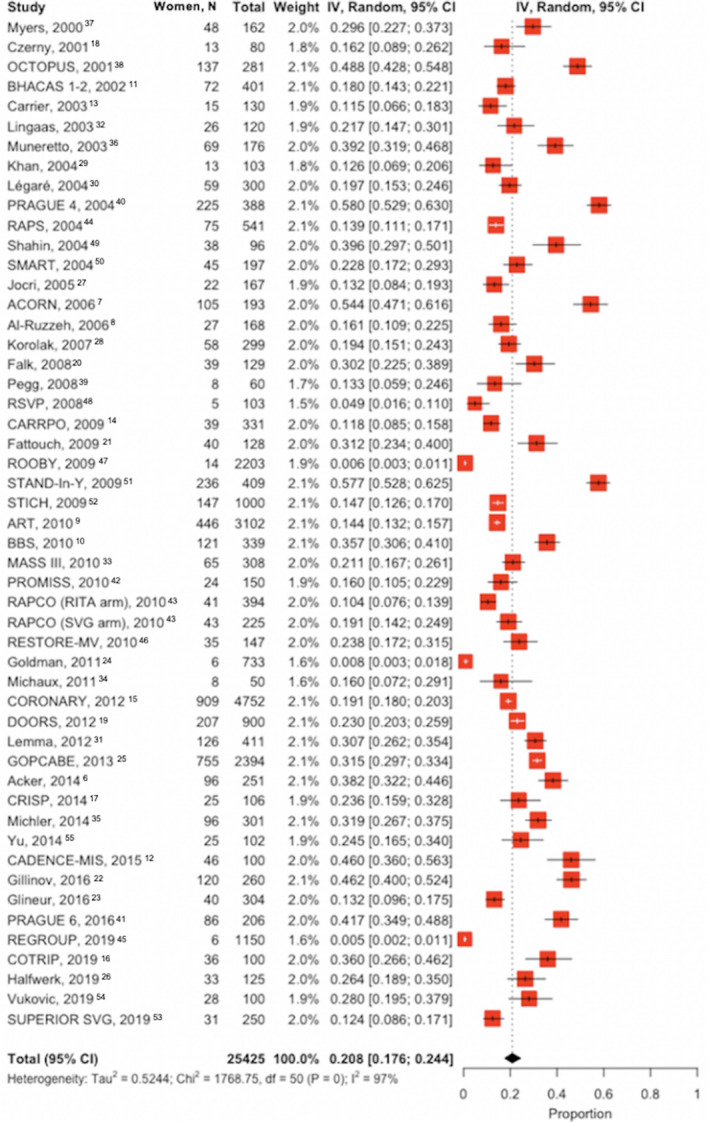
Squares represent the study weight; diamonds represent the pooled proportion of each subgroup with CIs; dots in the squares represent the study proportion and bars are the CIs (white when the CI is fully within the square (ie, very small CI, otherwise black [ie, large CI]). The dotted line represents the cumulative proportion. ACORN indicates Acorn Clinical Trial; ART, Arterial Revascularization Trial; BBS, Best Bypass Surgery Trial; BHACAS, Beating Heart Against Cardioplegic Arrest Studies; CADENCE‐MIS, EDWARDS INTUITY Valve System CADENCE‐MIS Study; CARRPO, Copenhagen Arterial Revascularization Randomized Patency and Outcome trial; CORONARY, CABG Off or On Pump Revascularization Study; COTRIP, Randomized Comparison of Trifecta and Perimount Magna Ease Supraannular Aortic Xenografts study; CRISP, Coronary Artery Bypass Grafting in High‐Risk Patients Randomised to Off‐ or On‐Pump Surgery; DOORS, Danish On‐Pump Versus Off‐Pump Randomization Study; GOPCABE, German Off‐Pump Coronary Artery Bypass Grafting in Elderly Patients; IV, inverse variance; JOCRI, Japanese Off‐Pump Coronary Revascularization Investigation; MASS III, The Medicine, Angioplasty, or Surgery Study III; OCTOPUS, Early Outcome After Off‐Pump Versus On‐Pump Coronary Bypass Surgery; PRAGUE‐4; A randomized comparison between off‐pump and on‐pump surgery; PRAGUE‐6, Off‐pump versus on‐pump coronary artery bypass graft surgery in patients with EuroSCORE ≥6; PROMISS, Prospective Randomized Comparison of Off‐Pump and On‐Pump Multi‐Vessel Coronary Artery Bypass Surgery; RAPCO, Radial Artery Patency and Clinical Outcomes; RAPS, Radial Artery Patency Study; REGROUP, Randomized Endovein Graft Prospective Trial; RESTOR‐MV, Randomized Evaluation of a Surgical Treatment for Off‐Pump Repair of the Mitral Valve; ROOBY, Veteran Affairs Randomized On/Off Bypass Study; RSVP, Radial Artery Versus Saphenous Vein Patency Trial; SMART, Surgical Management of Arterial Revascularization Therapies Trial; STAND‐In‐Y, Arterial revascularization in primary coronary artery bypass grafting: direct comparison of 4 strategies; STICH, Surgical Treatment for Ischemic Heart Failure Trial; and SUPERIOR SVG, Surgical and Pharmacological Novel Interventions to Improve Overall Results of Saphenous Vein Graft Patency in Coronary Artery Bypass Grafting Surgery Trial.
Women proportion dropped significantly between the first and the past year of the study period (29.6% in 2000 versus 13.1% in 2019, P<0.001) (Figure 2).6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55
Figure 2. Proportions of women in cardiac surgery trials by study period.
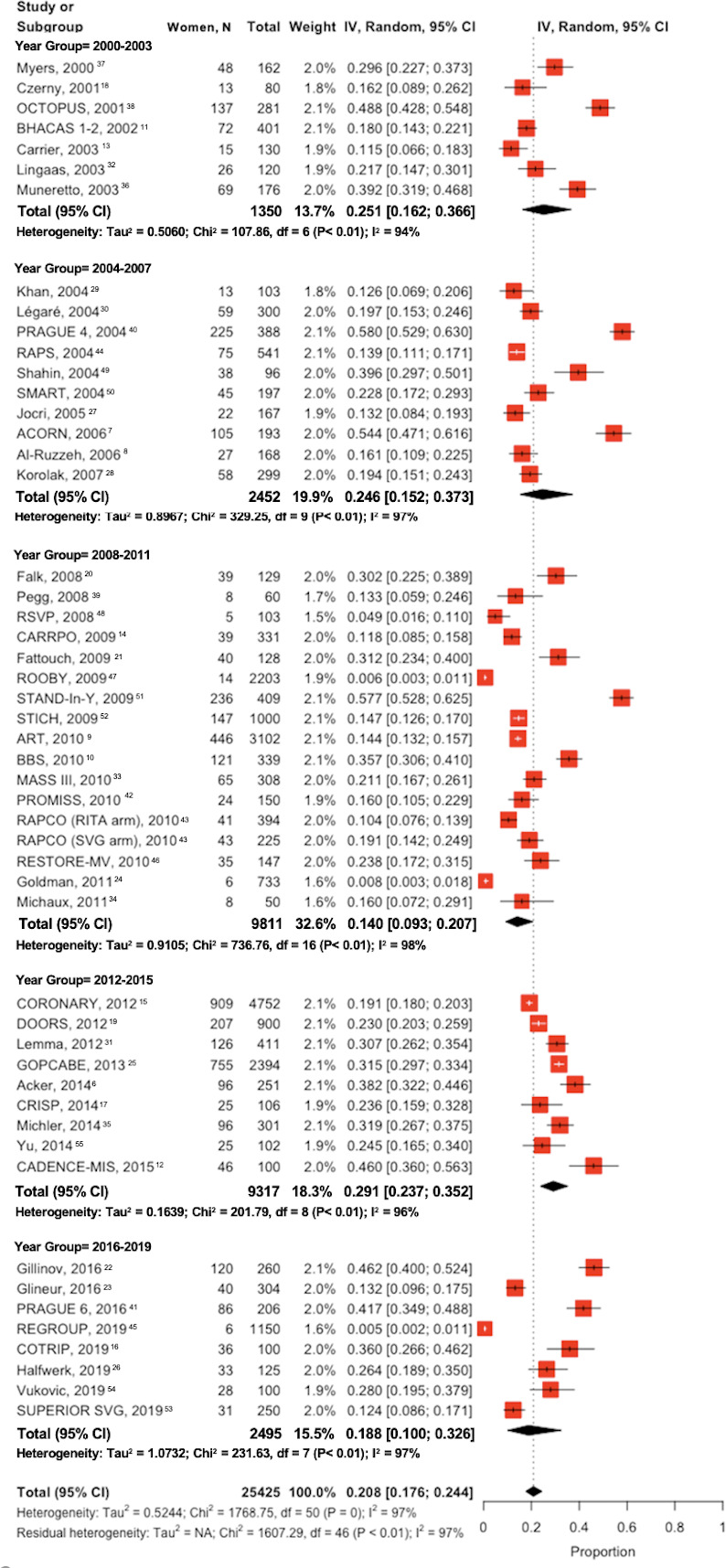
ACORN indicates Acorn Clinical Trial; ART, Arterial Revascularization Trial; BBS, Best Bypass Surgery Trial; BHACAS, Beating Heart Against Cardioplegic Arrest Studies; CADENCE‐MIS, EDWARDS INTUITY Valve System CADENCE‐MIS Study; CARRPO, Copenhagen Arterial Revascularization Randomized Patency and Outcome trial; CORONARY, CABG Off or On Pump Revascularization Study; COTRIP, Randomized Comparison of Trifecta and Perimount Magna Ease Supraannular Aortic Xenografts study; CRISP, Coronary Artery Bypass Grafting in High‐Risk Patients Randomised to Off‐ or On‐Pump Surgery; DOORS, Danish On‐Pump Versus Off‐Pump Randomization Study; GOPCABE, German Off‐Pump Coronary Artery Bypass Grafting in Elderly Patients; JOCRI, Japanese Off‐Pump Coronary Revascularization Investigation; MASS III, The Medicine, Angioplasty, or Surgery Study III; OCTOPUS, Early Outcome After Off‐Pump Versus On‐Pump Coronary Bypass Surgery; PRAGUE‐4; A randomized comparison between off‐pump and on‐pump surgery; PRAGUE‐6, Off‐pump versus on‐pump coronary artery bypass graft surgery in patients with EuroSCORE ≥6; PROMISS, Prospective Randomized Comparison of Off‐Pump and On‐Pump Multi‐Vessel Coronary Artery Bypass Surgery; RAPCO, Radial Artery Patency and Clinical Outcomes; RAPS, Radial Artery Patency Study; REGROUP, Randomized Endovein Graft Prospective Trial; RESTOR‐MV, Randomized Evaluation of a Surgical Treatment for Off‐Pump Repair of the Mitral Valve; ROOBY, Veteran Affairs Randomized On/Off Bypass Study; RSVP, Radial Artery Versus Saphenous Vein Patency Trial; SMART, Surgical Management of Arterial Revascularization Therapies Trial; STAND‐In‐Y, Arterial revascularization in primary coronary artery bypass grafting: direct comparison of 4 strategies; STICH, Surgical Treatment for Ischemic Heart Failure Trial; and SUPERIOR SVG, Surgical and Pharmacological Novel Interventions to Improve Overall Results of Saphenous Vein Graft Patency in Coronary Artery Bypass Grafting Surgery Trial.
Only 3 trials (5.9%) formally tested sex as treatment effect modifier.
Women were significantly more represented in trials based in Europe (26.2%; 95% CI, 21.2–31.9) versus North America (11.9%; 95% CI, 4.1–29.9), Asia/Australia/South America (16.8%; 95% CI, 12.7–21.9), and those involving multiple continents (16.4%; 95% CI, 14.1–19.9) (P=0.003). Women were less represented in trials of coronary bypass surgery versus other interventions (16.8%; 95% CI, 12.3–22.7 versus 33.6%; 95% CI, 27.4–40.5; P=0.0002) and in trials enrolling younger patients (P=0.009; Figure 3)6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55; the percentage of female patients was higher in industry‐sponsored versus non‐industry sponsored trials (31.7%; 95% CI, 27.2–36.6 versus 15.5%; 95% CI, 10.0–23.2; P=0.0004) and was not significantly associated with the trial sample size (P=0.52) or study design (multicenter versus monocenter: P=0.22). No publication bias was found (Figure S2; Egger test P value=0.55).
Figure 3. Proportions of women in cardiac surgery trials by age groups.
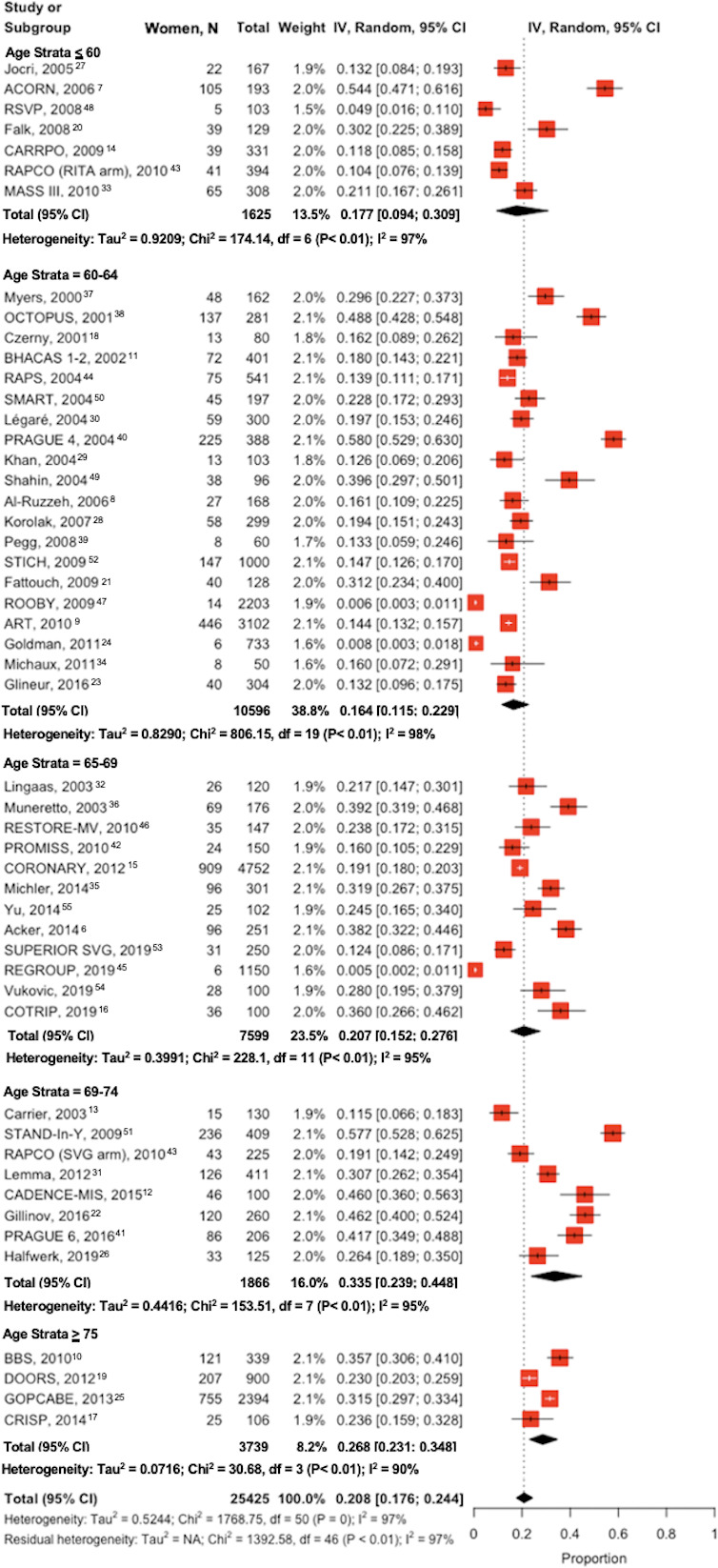
ACORN indicates Acorn Clinical Trial; ART, Arterial Revascularization Trial; BBS, Best Bypass Surgery Trial; BHACAS, Beating Heart Against Cardioplegic Arrest Studies; CADENCE‐MIS, EDWARDS INTUITY Valve System CADENCE‐MIS Study; CARRPO, Copenhagen Arterial Revascularization Randomized Patency and Outcome trial; CORONARY, CABG Off or On Pump Revascularization Study; COTRIP, Randomized Comparison of Trifecta and Perimount Magna Ease Supraannular Aortic Xenografts study; CRISP, Coronary Artery Bypass Grafting in High‐Risk Patients Randomised to Off‐ or On‐Pump Surgery; DOORS, Danish On‐Pump Versus Off‐Pump Randomization Study; GOPCABE, German Off‐Pump Coronary Artery Bypass Grafting in Elderly Patients; JOCRI, Japanese Off‐Pump Coronary Revascularization Investigation; MASS III, The Medicine, Angioplasty, or Surgery Study III; OCTOPUS, Early Outcome After Off‐Pump Versus On‐Pump Coronary Bypass Surgery; PRAGUE‐4; A randomized comparison between off‐pump and on‐pump surgery; PRAGUE‐6, Off‐pump versus on‐pump coronary artery bypass graft surgery in patients with EuroSCORE ≥6; PROMISS, Prospective Randomized Comparison of Off‐Pump and On‐Pump Multi‐Vessel Coronary Artery Bypass Surgery; RAPCO, Radial Artery Patency and Clinical Outcomes; RAPS, Radial Artery Patency Study; REGROUP, Randomized Endovein Graft Prospective Trial; RESTOR‐MV, Randomized Evaluation of a Surgical Treatment for Off‐Pump Repair of the Mitral Valve; ROOBY, Veteran Affairs Randomized On/Off Bypass Study; RSVP, Radial Artery Versus Saphenous Vein Patency Trial; SMART, Surgical Management of Arterial Revascularization Therapies Trial; STAND‐In‐Y, Arterial revascularization in primary coronary artery bypass grafting: direct comparison of 4 strategies; STICH, Surgical Treatment for Ischemic Heart Failure Trial; and SUPERIOR SVG, Surgical and Pharmacological Novel Interventions to Improve Overall Results of Saphenous Vein Graft Patency in Coronary Artery Bypass Grafting Surgery Trial.
Sensitivity Analysis Excluding the VA Trials
After the exclusion of the 3 trials conducted at VA centers (Goldman et al., REGROUP [Randomized Trial of Endoscopic or Open Vein‐Graft Harvesting for Coronary‐Artery Bypass], ROOBY [Randomized On/Off Bypass Study]),24, 45, 47 women were 5003 out of 21339 total patients (24.4%; 95% CI, 21.1–28.0; range, 10.4%–57.9%). No significant difference in the proportion of women was found comparing the beginning versus the end of the study period (29.6% in 2000 versus 24.4% in 2019, P=0.45) (Figure S3).
Women were significantly more represented in trials based in North America (29.8%; 95% CI, 21.0–40.3) and Europe (26.2%; 95% CI, 21.2–31.9) versus Asia/Australia/South America (16.8%; 95% CI, 12.7–21.9) and those involving multiple continents (16.4%; 95% CI, 14.1–19.9) (P=0.003).
Women were less represented in trials of coronary bypass surgery versus other interventions (21.4%; 95% CI, 17.8–25.5 versus 33.6%; 95% CI, 27.4–40.5; P=0.001), but not in trials enrolling younger patients (P=0.17); the percentage of female patients was higher in industry‐sponsored versus non‐industry sponsored trials (31.7%; 95% CI, 27.2–36.6 versus 21.7%; 95% CI, 17.1–27.0; P=0.002) and was not significantly associated with the trial sample size (P=0.42) or study design (multicenter versus monocenter: P=0.26). No publication bias was found (Figure S4; Egger test P value=0.66).
Discussion
Generalizability of RCT results to both sexes depends on having a sufficient number of men and women. However, underrepresentation of women in RCTs in general, and in cardiac surgery trials in particular, remains an unsolved issue.
For example, the available observational evidence on the use of multiple arterial grafting in women is conflicting, with some studies suggesting and others refuting a clinical benefit for female patients who receive >1 arterial graft for coronary artery bypass graft (CABG).56, 57, 58, 59, 60 In the only large RCT that has tested the multiple arterial grafts hypothesis (the Arterial Revascularization Trial)61 women represented only 15% of the study population and sex was not formally tested as a treatment effect modifier in the main analysis.
Similarly, the effect of off‐pump surgery for CABG in women has been associated with contradictory results.62, 63, 64 However, the percentage of women enrolled in the largest off‐pump trials was low (0.5%, 19.2%, and 31.5% in ROOBY,47 CORONARY [CABG Off or On Pump Revascularization Study],15 and GOPCABE [German Off‐Pump Coronary Artery Bypass Grafting in Elderly Patients Study],25 respectively). It is noteworthy that of the 3 mentioned trials only 1 (ie, CORONARY)15 formally tested sex as a treatment effect modifier.
In the valve literature, the COTRIP (Randomized Comparison of Trifecta and Perimount Magna Ease Supraannular Aortic Xenografts study) trial16 tested the use of 2 different prosthetic aortic valves in patients with aortic stenosis undergoing aortic valve replacement. Again, the majority of included patients were men (64%) and sex was not formally tested as a treatment effect modifier.
Our data showed a significant drop in women proportion during the study period (2000–2020) when all trials were included in the analysis.
It is interesting to note that when trials conducted at VA medical centers were excluded from the analysis the temporal drop in women representation disappeared and North American RCTs were found to be those enrolling the highest proportion of women (29.8%). The fact that trials funded by one of the most active US agencies in cardiac surgery prevalently enroll male subjects (the mean prevalence of men in the 3 VA studies included was 99.4%) explains this result.
The lower representation of women in CABG RCTs was confirmed even after the exclusion of trials conducted at VA centers. While one might speculate that these disparities could be in part because of inherent biases within the cardiovascular care system leading to lower referral for interventions for female patients with coronary artery disease,65 it should be noted that such proportions are similar to those reported in large national registries like the Society of Thoracic Surgeons adult cardiac surgical database,66 where women represent ≈25% of the overall CABG population.
Nonetheless, as such percentages are likely inadequate to provide meaningful estimates of treatment effect, overrepresentation of female patients should be taken into consideration in the design of future cardiac surgical trials.
A lower proportion of women was also found in non‐industry sponsored trials (irrespective of the exclusion of trials conducted at VA centers).
Limitations
The present analysis shares the limitations of meta‐analyses and of pooled estimates, including the potential for methodological and clinical heterogeneity among included studies and the possibility of collinearity between tested variables. Moreover, RCTs generally capture only biologic sex and gender could not be addressed in our analysis.
Conclusions
Our study shows that the proportion of women included in cardiac surgery RCTs is low and likely inadequate to provide meaningful estimates of treatment effect. It is particularly concerning that this proportion significantly decreased over the past 2 decades, although this temporal trend was not seen when trials conducted at VA medical centers were excluded from the analysis. As important sex‐related differences in cardiac surgical outcomes exist,2, 67 surgical results obtained in a prevalently male population may not apply to women and might potentially misinform surgical decision making in women. Substantial effort must be made by surgical trialists and funding agencies to promote the inclusion of women in cardiac surgery trials.
Sources of Funding
None.
Disclosures
None.
Supporting information
Data S1
Figures S1–S4
For Sources of Funding and Disclosures, see page 11.
References
- 1.Feldman S, Ammar W, Lo K, Trepman E, van Zuylen M, Etzioni O. Quantifying sex bias in clinical studies at scale with automated data extraction. JAMA Netw Open. 2019;2:e196700. 10.1001/jamanetworkopen.2019.6700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Alam M, Bandeali SJ, Kayani WT, Ahmad W, Shahzad SA, Jneid H, Birnbaum Y, Kleiman NS, Coselli JS, Ballantyne CM, et al. Comparison by meta‐analysis of mortality after isolated coronary artery bypass grafting in women versus men. Am J Cardiol. 2013;112:309–317. DOI: 10.1016/j.amjcard.2013.03.034. [DOI] [PubMed] [Google Scholar]
- 3.Chaker Z, Badhwar V, Alqahtani F, Aljohani S, Zack CJ, Holmes DR, Rihal CS, Alkhouli M. Sex differences in the utilization and outcomes of surgical aortic valve replacement for severe aortic stenosis. J Am Heart Assoc. 2017;6:e006370. DOI: 10.1161/JAHA.117.006370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Beller CJ, Farag M, Wannaku S, Seppelt P, Arif R, Ruhparwar A, Karck M, Weymann A, Kallenbach K. Gender‐specific differences in outcome of ascending aortic aneurysm surgery. PLoS One. 2015;10:e0124461. DOI: 10.1371/journal.pone.0124461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA statement. Ann Intern Med. 2009;151:264–269, W64. [DOI] [PubMed] [Google Scholar]
- 6.Acker MA, Parides MK, Perrault LP, Moskowitz AJ, Gelijns AC, Voisine P, Smith PK, Hung JW, Blackstone EH, Puskas JD, et al. Mitral‐valve repair versus replacement for severe ischemic mitral regurgitation. N Engl J Med. 2014;370:23–32. DOI: 10.1056/NEJMoa1312808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Acker MA, Bolling S, Shemin R, Kirklin J, Oh JK, Mann DL, Jessup M, Sabbah HN, Starling RC, Kubo SH, et al. Mitral valve surgery in heart failure: insights from the Acorn Clinical Trial. J Thorac Cardiovasc Surg. 2006;132:568–577, 577.e1–4. [DOI] [PubMed] [Google Scholar]
- 8.Al‐Ruzzeh S, George S, Bustami M, Wray J, Ilsley C, Athanasiou T, Amrani M. Effect of off‐pump coronary artery bypass surgery on clinical, angiographic, neurocognitive, and quality of life outcomes: randomised controlled trial. BMJ. 2006;332:1365. DOI: 10.1136/bmj.38852.479907.7C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Taggart DP, Altman DG, Gray AM, Lees B, Nugara F, Yu L‐M, Campbell H, Flather M; Investigators ART . Randomized trial to compare bilateral vs. single internal mammary coronary artery bypass grafting: 1‐year results of the Arterial Revascularisation Trial (ART). Eur Heart J. 2010;31:2470–2481. DOI: 10.1093/eurheartj/ehq318. [DOI] [PubMed] [Google Scholar]
- 10.Moller CH, Perko MJ, Lund JT, Andersen LW, Kelbaek H, Madsen JK, Winkel P, Gluud C, Steinbruchel DA. No major differences in 30‐day outcomes in high‐risk patients randomized to off‐pump versus on‐pump coronary bypass surgery: the best bypass surgery trial. Circulation. 2010;121:498–504. DOI: 10.1161/CIRCULATIONAHA.109.880443. [DOI] [PubMed] [Google Scholar]
- 11.Angelini GD, Taylor FC, Reeves BC, Ascione R. Early and midterm outcome after off‐pump and on‐pump surgery in Beating Heart Against Cardioplegic Arrest Studies (BHACAS 1 and 2): a pooled analysis of two randomised controlled trials. Lancet. 2002;359:1194–1199. DOI: 10.1016/S0140-6736(02)08216-8. [DOI] [PubMed] [Google Scholar]
- 12.Borger MA, Moustafine V, Conradi L, Knosalla C, Richter M, Merk DR, Doenst T, Hammerschmidt R, Treede H, Dohmen P, et al. A randomized multicenter trial of minimally invasive rapid deployment versus conventional full sternotomy aortic valve replacement. Ann Thorac Surg. 2015;99:17–25. DOI: 10.1016/j.athoracsur.2014.09.022. [DOI] [PubMed] [Google Scholar]
- 13.Carrier M, Perrault LP, Jeanmart H, Martineau R, Cartier R, Pagé P. Randomized trial comparing off‐pump to on‐pump coronary artery bypass grafting in high‐risk patients. Heart Surg Forum. 2003;6:E89–E92. [PubMed] [Google Scholar]
- 14.Damgaard S, Wetterslev J, Lund JT, Lilleør NB, Perko MJ, Kelbaek H, Madsen JK, Steinbrüchel DA. One‐year results of total arterial revascularization vs. conventional coronary surgery: CARRPO trial. Eur Heart J. 2009;30:1005–1011. DOI: 10.1093/eurheartj/ehp048. [DOI] [PubMed] [Google Scholar]
- 15.Lamy A, Devereaux PJ, Prabhakaran D, Taggart DP, Hu S, Paolasso E, Straka Z, Piegas LS, Akar AR, Jain AR, et al. Off‐pump or on‐pump coronary‐artery bypass grafting at 30 days. N Engl J Med. 2012;366:1489–1497. DOI: 10.1056/NEJMoa1200388. [DOI] [PubMed] [Google Scholar]
- 16.Van Linden A, Arsalan M, Körschgen T, Blumenstein J, Kempfert J, Hecker F, Walther T. Randomized (CO)mparison of (TRI)fecta and (P)erimount Magna Ease Supraannular Aortic Xenografts‐CO.TRI.P Study. Thorac Cardiovasc Surg. 2019;67:266–273. [DOI] [PubMed] [Google Scholar]
- 17.Rogers CA, Pike K, Campbell H, Reeves BC, Angelini GD, Gray A, Altman DG, Miller H, Wells S, Taggart DP, et al. Coronary artery bypass grafting in high‐RISk patients randomised to off‐ or on‐Pump surgery: a randomised controlled trial (the CRISP trial). Health Technol Assess Winch Engl. 2014;18:v–xx;1–157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Czerny M, Baumer H, Kilo J, Zuckermann A, Grubhofer G, Chevtchik O, Wolner E, Grimm M. Complete revascularization in coronary artery bypass grafting with and without cardiopulmonary bypass. Ann Thorac Surg. 2001;71:165–169. DOI: 10.1016/S0003-4975(00)02230-X. [DOI] [PubMed] [Google Scholar]
- 19.Houlind K, Kjeldsen BJ, Madsen SN, Rasmussen BS, Holme SJ, Nielsen PH, Mortensen PE; DOORS Study Group . On‐pump versus off‐pump coronary artery bypass surgery in elderly patients: results from the Danish on‐pump versus off‐pump randomization study. Circulation. 2012;125:2431–2439. DOI: 10.1161/CIRCULATIONAHA.111.052571. [DOI] [PubMed] [Google Scholar]
- 20.Falk V, Seeburger J, Czesla M, Borger MA, Willige J, Kuntze T, Doll N, Borger F, Perrier P, Mohr FW. How does the use of polytetrafluoroethylene neochordae for posterior mitral valve prolapse (loop technique) compare with leaflet resection? A prospective randomized trial. J Thorac Cardiovasc Surg. 2008;136:1200–1206; discussion 1205–1206. DOI: 10.1016/j.jtcvs.2008.07.028. [DOI] [PubMed] [Google Scholar]
- 21.Fattouch K, Guccione F, Dioguardi P, Sampognaro R, Corrado E, Caruso M, Ruvolo G. Off‐pump versus on‐pump myocardial revascularization in patients with ST‐segment elevation myocardial infarction: a randomized trial. J Thorac Cardiovasc Surg. 2009;137:650–657. DOI: 10.1016/j.jtcvs.2008.11.033. [DOI] [PubMed] [Google Scholar]
- 22.Gillinov AM, Gelijns AC, Parides MK, DeRose JJ, Moskowitz AJ, Voisine P, Ailawadi G, Bouchard D, Smith PK, Mack MJ, et al. Surgical ablation of atrial fibrillation during mitral‐valve surgery. N Engl J Med. 2015;372:1399–1409. DOI: 10.1056/NEJMoa1500528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Glineur D, Boodhwani M, Hanet C, de Kerchove L, Navarra E, Astarci P, Noirhomme P, El Khoury G. Bilateral internal thoracic artery configuration for coronary artery bypass surgery. Circulation. 2016;9:e003518. DOI: 10.1161/CIRCINTERVENTIONS.115.003518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Goldman S, Sethi GK, Holman W, Thai H, McFalls E, Ward HB, Kelly RF, Rhenman B, Tobler GH, Bakaeen FG, et al. Radial artery grafts vs saphenous vein grafts in coronary artery bypass surgery: a randomized trial. JAMA. 2011;305:167–174. DOI: 10.1001/jama.2010.1976. [DOI] [PubMed] [Google Scholar]
- 25.Diegeler A, Börgermann J, Kappert U, Breuer M, Böning A, Ursulescu A, Rastan A, Holzhey D, Treede H, Rieß F‐C, et al. Off‐pump versus on‐pump coronary‐artery bypass grafting in elderly patients. N Engl J Med. 2013;368:1189–1198. DOI: 10.1056/NEJMoa1211666. [DOI] [PubMed] [Google Scholar]
- 26.Halfwerk FR, Knol K, Mariani S, Grandjean JG, Mecozzi G. Randomized trial of miniaturized versus standard extracorporeal circulation in aortic valve surgery. Ann Thorac Surg. 2019;108:37–44. DOI: 10.1016/j.athoracsur.2019.01.019. [DOI] [PubMed] [Google Scholar]
- 27.Kobayashi J, Tashiro T, Ochi M, Yaku H, Watanabe G, Satoh T, Tagusari O, Nakajima H, Kitamura S; Japanese Off‐Pump Coronary Revascularization Investigation (JOCRI) Study Group . Early outcome of a randomized comparison of off‐pump and on‐pump multiple arterial coronary revascularization. Circulation. 2005;112:I338–343. [DOI] [PubMed] [Google Scholar]
- 28.Karolak W, Hirsch G, Buth K, Légaré J‐F. Medium‐term outcomes of coronary artery bypass graft surgery on pump versus off pump: results from a randomized controlled trial. Am Heart J. 2007;153:689–695. DOI: 10.1016/j.ahj.2007.01.033. [DOI] [PubMed] [Google Scholar]
- 29.Khan NE, De Souza A, Mister R, Flather M, Clague J, Davies S, Collins P, Wang D, Sigwart U, Pepper J. A randomized comparison of off‐pump and on‐pump multivessel coronary‐artery bypass surgery. N Engl J Med. 2004;350:21–28. DOI: 10.1056/NEJMoa031282. [DOI] [PubMed] [Google Scholar]
- 30.Légaré J‐F, Buth KJ, King S, Wood J, Sullivan JA, Friesen CH, Lee J, Stewart K, Hirsch GM. Coronary bypass surgery performed off pump does not result in lower in‐hospital morbidity than coronary artery bypass grafting performed on pump. Circulation. 2004;109:887–892. DOI: 10.1161/01.CIR.0000115943.41814.7D. [DOI] [PubMed] [Google Scholar]
- 31.Lemma MG, Coscioni E, Tritto FP, Centofanti P, Fondacone C, Salica A, Rossi A, De Santo T, Di Benedetto G, Piazza L, et al. On‐pump versus off‐pump coronary artery bypass surgery in high‐risk patients: operative results of a prospective randomized trial (on‐off study). J Thorac Cardiovasc Surg. 2012;143:625–631. DOI: 10.1016/j.jtcvs.2011.11.011. [DOI] [PubMed] [Google Scholar]
- 32.Lingaas PS, Hol PK, Lundblad R, Rein KA, Tønnesen TI, Svennevig JL, Hauge SN, Vatne K, Fosse E. Clinical and angiographic outcome of coronary surgery with and without cardiopulmonary bypass: a prospective randomized trial. Heart Surg Forum. 2004;7:37–41. [PubMed] [Google Scholar]
- 33.Hueb W, Lopes NH, Pereira AC, Hueb AC, Soares PR, Favarato D, D'Oliveira Vieira R, Lima EG, Garzillo CL, da Silva Paulitch F, et al. Five‐year follow‐up of a randomized comparison between off‐pump and on‐pump stable multivessel coronary artery bypass grafting. The MASS III Trial. Circulation. 2010;122:S48–S52. DOI: 10.1161/CIRCULATIONAHA.109.924258. [DOI] [PubMed] [Google Scholar]
- 34.Michaux I, Filipovic M, Skarvan K, Bolliger D, Schumann R, Bernet F, Seeberger M. A randomized comparison of right ventricular function after on‐pump versus off‐pump coronary artery bypass graft surgery. J Thorac Cardiovasc Surg. 2011;141:361–367. DOI: 10.1016/j.jtcvs.2010.02.023. [DOI] [PubMed] [Google Scholar]
- 35.Michler RE, Smith PK, Parides MK, Ailawadi G, Thourani V, Moskowitz AJ, Acker MA, Hung JW, Chang HL, Perrault LP, et al. Two‐year outcomes of surgical treatment of moderate ischemic mitral regurgitation. N Engl J Med. 2016;374:1932–1941. DOI: 10.1056/NEJMoa1602003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Muneretto C, Bisleri G, Negri A, Manfredi J, Metra M, Nodari S, Dei CL. Off‐pump coronary artery bypass surgery technique for total arterial myocardial revascularization: a prospective randomized study. Ann Thorac Surg. 2003;76:778–783. DOI: 10.1016/S0003-4975(03)00564-2. [DOI] [PubMed] [Google Scholar]
- 37.Myers WO, Berg R, Ray JF, Douglas‐Jones JW, Maki HS, Ulmer RH, Chaitman BR, Reinhart RA. All‐artery multigraft coronary artery bypass grafting with only internal thoracic arteries possible and safe: a randomized trial. Surgery. 2000;128:650–659. DOI: 10.1067/msy.2000.108113. [DOI] [PubMed] [Google Scholar]
- 38.van Dijk D, Nierich AP, Jansen EWL, Nathoe HM, Suyker WJL, Diephuis JC, van Boven W‐J, Borst C, Buskens E, Grobbee DE, et al. Early outcome after off‐pump versus on‐pump coronary bypass surgery: results from a randomized study. Circulation. 2001;104:1761–1766. DOI: 10.1161/hc4001.097036. [DOI] [PubMed] [Google Scholar]
- 39.Pegg TJ, Selvanayagam JB, Karamitsos TD, Arnold RJ, Francis JM, Neubauer S, Taggart DP. Effects of off‐pump versus on‐pump coronary artery bypass grafting on early and late right ventricular function. Circulation. 2008;117:2202–2210. DOI: 10.1161/CIRCULATIONAHA.107.735621. [DOI] [PubMed] [Google Scholar]
- 40.Straka Z, Widimsky P, Jirasek K, Stros P, Votava J, Vanek T, Brucek P, Kolesar M, Spacek R. Off‐pump versus on‐pump coronary surgery: final results from a prospective randomized study PRAGUE‐4. Ann Thorac Surg. 2004;77:789–793. DOI: 10.1016/j.athoracsur.2003.08.039. [DOI] [PubMed] [Google Scholar]
- 41.Hlavicka J, Straka Z, Jelinek S, Budera P, Vanek T, Maly M, Widimsky P. Off‐pump versus on‐pump coronary artery bypass grafting surgery in high‐risk patients: PRAGUE‐6 trial at 30 days and 1 year. Biomed Pap Med Fac Univ Palacky Olomouc Czechoslov. 2016;160:263–270. DOI: 10.5507/bp.2015.059. [DOI] [PubMed] [Google Scholar]
- 42.Sousa Uva M, Cavaco S, Oliveira AG, Matias F, Silva C, Mesquita A, Aguiar P, Bau J, Pedro A, Magalhães MP. Early graft patency after off‐pump and on‐pump coronary bypass surgery: a prospective randomized study. Eur Heart J. 2010;31:2492–2499. DOI: 10.1093/eurheartj/ehq210. [DOI] [PubMed] [Google Scholar]
- 43.Hayward PAR, Gordon IR, Hare DL, Matalanis G, Horrigan ML, Rosalion A, Buxton BF. Comparable patencies of the radial artery and right internal thoracic artery or saphenous vein beyond 5 years: results from the Radial Artery Patency and Clinical Outcomes trial. J Thorac Cardiovasc Surg. 2010;139:60–67. DOI: 10.1016/j.jtcvs.2009.09.043. [DOI] [PubMed] [Google Scholar]
- 44.Desai ND, Cohen EA, Naylor CD, Fremes SE. A randomized comparison of radial‐artery and saphenous‐vein coronary bypass grafts. N Engl J Med. 2004;351:2302–2309. DOI: 10.1056/NEJMoa040982. [DOI] [PubMed] [Google Scholar]
- 45.Zenati MA, Bhatt DL, Bakaeen FG, Stock EM, Biswas K, Gaziano JM, Kelly RF, Tseng EE, Bitondo J, Quin JA, et al. Randomized trial of endoscopic or open vein‐graft harvesting for coronary‐artery bypass. N Engl J Med. 2019;380:132–141. DOI: 10.1056/NEJMoa1812390. [DOI] [PubMed] [Google Scholar]
- 46.Grossi EA, Patel N, Woo YJ, Goldberg JD, Schwartz CF, Subramanian V, Feldman T, Bourge R, Baumgartner N, Genco C, et al. Outcomes of the RESTOR‐MV Trial (Randomized Evaluation of a Surgical Treatment for Off‐Pump Repair of the Mitral Valve). J Am Coll Cardiol. 2010;56:1984–1993. DOI: 10.1016/j.jacc.2010.06.051. [DOI] [PubMed] [Google Scholar]
- 47.Shroyer AL, Grover FL, Hattler B, Collins JF, McDonald GO, Kozora E, Lucke JC, Baltz JH, Novitzky D; Veterans Affairs Randomized On/Off Bypass (ROOBY) Study Group . On‐pump versus off‐pump coronary‐artery bypass surgery. N Engl J Med. 2009;361:1827–1837. DOI: 10.1056/NEJMoa0902905. [DOI] [PubMed] [Google Scholar]
- 48.Collins P, Webb CM, Chong CF, Moat NE; Radial Artery Versus Saphenous Vein Patency (RSVP) Trial Investigators . Radial artery versus saphenous vein patency randomized trial: five‐year angiographic follow‐up. Circulation. 2008;117:2859–2864. DOI: 10.1161/CIRCULATIONAHA.107.736215. [DOI] [PubMed] [Google Scholar]
- 49.Shahin GMM, van der Heijden GJMG, Bots ML, Cramer M‐J, Jaarsma W, Gadellaa JCA, de la Rivière AB, van Swieten HA. The Carpentier‐Edwards Classic and Physio mitral annuloplasty rings: a randomized trial. Heart Surg Forum. 2005;8:394–395; discussion E394–E395. DOI: 10.1532/hsf.419. [DOI] [PubMed] [Google Scholar]
- 50.Puskas JD, Williams WH, Mahoney EM, Huber PR, Block PC, Duke PG, Staples JR, Glas KE, Marshall JJ, Leimbach ME, et al. Off‐pump vs conventional coronary artery bypass grafting: early and 1‐year graft patency, cost, and quality‐of‐life outcomes: a randomized trial. JAMA. 2004;291:1841–1849. DOI: 10.1001/jama.291.15.1841. [DOI] [PubMed] [Google Scholar]
- 51.Nasso G, Coppola R, Bonifazi R, Piancone F, Bozzetti G, Speziale G. Arterial revascularization in primary coronary artery bypass grafting: direct comparison of 4 strategies–results of the Stand‐in‐Y Mammary Study. J Thorac Cardiovasc Surg. 2009;137:1093–1100. DOI: 10.1016/j.jtcvs.2008.10.029. [DOI] [PubMed] [Google Scholar]
- 52.Jones RH, Velazquez EJ, Michler RE, Sopko G, Oh JK, O'Connor CM, Hill JA, Menicanti L, Sadowski Z, Desvigne‐Nickens P, et al. Coronary bypass surgery with or without surgical ventricular reconstruction. N Engl J Med. 2009;360:1705–1717. DOI: 10.1056/NEJMoa0900559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Deb S, Singh SK, de Souza D, Chu MWA, Whitlock R, Meyer SR, Verma S, Jeppsson A, Al‐Saleh A, Brady K, et al. SUPERIOR SVG: no touch saphenous harvesting to improve patency following coronary bypass grafting (a multi‐Centre randomized control trial, NCT01047449). J Cardiothorac Surg. 2019;14:85. DOI: 10.1186/s13019-019-0887-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Vukovic PM, Milojevic P, Stojanovic I, Micovic S, Zivkovic I, Peric M, Milicic M, Milacic P, Milojevic M, Bojic M. The role of ministernotomy in aortic valve surgery‐a prospective randomized study. J Card Surg. 2019;34:435–439. DOI: 10.1111/jocs.14053. [DOI] [PubMed] [Google Scholar]
- 55.Yu L, Gu T, Shi E, Wang C, Fang Q, Yu Y, Zhao X, Qian C. Off‐pump versus on‐pump coronary artery bypass surgery in patients with triple‐vessel disease and enlarged ventricles. Ann Saudi Med. 2014;34:222. DOI: 10.5144/0256-4947.2014.222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Schwann TA, Engoren M, Bonnell M, Clancy C, Habib RH. Comparison of late coronary artery bypass graft survival effects of radial artery versus saphenous vein grafting in male and female patients. Ann Thorac Surg. 2012;94:1485–1491. DOI: 10.1016/j.athoracsur.2012.05.029. [DOI] [PubMed] [Google Scholar]
- 57.Dimitrova KR, Hoffman DM, Geller CM, Ko W, Lucido DJ, Dincheva GR, Tranbaugh RF. Radial artery grafting in women improves 15‐year survival. J Thorac Cardiovasc Surg. 2013;146:1467–1473. DOI: 10.1016/j.jtcvs.2012.10.004. [DOI] [PubMed] [Google Scholar]
- 58.Kurlansky PA, Traad EA, Dorman MJ, Galbut DL, Zucker M, Ebra G. Bilateral internal mammary artery grafting reverses the negative influence of gender on outcomes of coronary artery bypass grafting surgery. Eur J Cardio‐Thorac Surg. 2013;44:54–63. DOI: 10.1093/ejcts/ezs683. [DOI] [PubMed] [Google Scholar]
- 59.Vrancic JM, Navia DO, Espinoza JC, Piccinini F, Camporrotondo M, Benzadon M, Dorsa A. Is sex a risk factor for death in patients with bilateral internal thoracic artery grafts? J Thorac Cardiovasc Surg. 2019;158:1345–1353.e1. DOI: 10.1016/j.jtcvs.2019.01.025. [DOI] [PubMed] [Google Scholar]
- 60.Kurlansky PA, Traad EA, Galbut DL, Zucker M, Ebra G. Efficacy of single versus bilateral internal mammary artery grafting in women: a long‐term study. Ann Thorac Surg. 2001;71:1949–1958; discussion 1957–1958. DOI: 10.1016/S0003-4975(01)02592-9. [DOI] [PubMed] [Google Scholar]
- 61.Taggart DP, Benedetto U, Gerry S, Altman DG, Gray AM, Lees B, Gaudino M, Zamvar V, Bochenek A, Buxton B, et al. Bilateral versus single internal‐thoracic‐artery grafts at 10 years. N Engl J Med. 2019;380:437–446. DOI: 10.1056/NEJMoa1808783. [DOI] [PubMed] [Google Scholar]
- 62.Lamy A, Devereaux PJ, Prabhakaran D, Taggart DP, Hu S, Straka Z, Piegas LS, Avezum A, Akar AR, Lanas Zanetti F, et al. Five‐year outcomes after off‐pump or on‐pump coronary‐artery bypass grafting. N Engl J Med. 2016;375:2359–2368. DOI: 10.1056/NEJMoa1601564. [DOI] [PubMed] [Google Scholar]
- 63.Kirmani BH, Holmes MV, Muir AD. Long‐term survival and freedom from reintervention after off‐pump coronary artery bypass grafting: a propensity‐matched study. Circulation. 2016;134:1209–1220. DOI: 10.1161/CIRCULATIONAHA.116.021933. [DOI] [PubMed] [Google Scholar]
- 64.Puskas JD, Kilgo PD, Kutner M, Pusca SV, Lattouf O, Guyton RA. Off‐pump techniques disproportionately benefit women and narrow the gender disparity in outcomes after coronary artery bypass surgery. Circulation. 2007;116:I192–199. DOI: 10.1161/CIRCULATIONAHA.106.678979. [DOI] [PubMed] [Google Scholar]
- 65.Jabagi H, Tran DT, Hessian R, Glineur D, Rubens FD. Impact of gender on arterial revascularization strategies for coronary artery bypass grafting. Ann Thorac Surg. 2018;105:62–68. DOI: 10.1016/j.athoracsur.2017.06.054. [DOI] [PubMed] [Google Scholar]
- 66.ElBardissi AW, Aranki SF, Sheng S, O’Brien SM, Greenberg CC, Gammie JS. Trends in isolated coronary artery bypass grafting: an analysis of the Society of Thoracic Surgeons adult cardiac surgery database. J Thorac Cardiovasc Surg. 2012;143:273–281. DOI: 10.1016/j.jtcvs.2011.10.029. [DOI] [PubMed] [Google Scholar]
- 67.Chung J, Stevens L‐M, Ouzounian M, El‐Hamamsy I, Bouhout I, Dagenais F, Cartier A, Peterson MD, Boodhwani M, Guo M, et al. Sex‐related differences in patients undergoing thoracic aortic surgery. Circulation. 2019;139:1177–1184. DOI: 10.1161/CIRCULATIONAHA.118.035805. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1
Figures S1–S4