

Abstract
Introduction
Fractures of the clavicle are common injuries, accounting 2.6–4% of all fractures in adults. Of these fractures, 21–28% are lateral clavicle fractures and 2–3% are medial clavicle fractures. Bipolar clavicle fractures are defined as a lateral and medial fracture and are uncommon. There is no consensus on the treatment of these fractures. The aim of this study is to provide a treatment on bipolar clavicle fractures based on the current literature.
Methods
The electronic databases PubMed, the Cochrane library and EMBASE were searched up on September 25th, 2017. Two reviewers (KR and TG) independently screened titles and abstracts for their relevance. Studies designed to evaluate the outcomes of conservative and/or operative treatment of segmental bipolar clavicle fractures in adults (> 16 years) were included. Editorials and commentaries were excluded, as well as synthetic, cadaveric and animal studies. Primary outcomes considered were pain reduction and shoulder function. Secondary outcomes considered are complications.
Results
Ten studies reporting results from ten patients were included for the review. In most patients, if treated operatively, surgical treatment with the use of double plating was performed. Only in elderly patients conservative treatment was adopted. All included patients were pain free and had a full range of motion after 3–6 months. Only two case reports provided a DASH score, while in eight studies no functional outcome score was measured.
Conclusion
A missed bipolar fracture can complicate the clinical progress. Surgical management of these fractures may be necessary; however, the treatment of choice depends on the age of the patient, daily activities and comorbidity.
Electronic supplementary material
The online version of this article (10.1007/s00068-019-01191-5) contains supplementary material, which is available to authorized users.
Keywords: Bipolar, Clavicle, Fracture, Review
Introduction
Fractures of the clavicle are common injuries, accounting 2.6–4% of all fractures in adults. Of these fractures, 21–28% are lateral clavicle fractures and 2–3% are medial clavicle fractures [1, 2]. Bipolar clavicle fractures are defined as a lateral and medial clavicle fracture; on the other hand, the term ‘floating clavicle’ refers to a sternoclavicular and an acromioclavicular luxation, also known as a panclavicular dislocation [3–13]. This study describes a patient with a bipolar clavicle fracture and presents an overview of the current literature.
Case description
A 23-year-old man was admitted after a high speed motor vehicle accident. A total body computed tomography was performed at the emergency department and showed the following injuries: cervical 4–6 fractures with spinal cord injury, left vertebral artery dissection, left transverse process fractures thoracic 5–8, fractures of ribs 1 and 2 on the left side, bilateral contusions of the lung and a bipolar clavicle fracture on the left side. The patient was admitted to our institution for an ASIA C type injury following local spinal injury protocol. The patient remained hemodynamically stable, but became symptomatic for pain of the left clavicle with a median NRS of 5 during the admission, measured three times a day.
Additional X-rays showed a medial clavicle fracture with 15 mm displacement and a lateral fracture with 10 mm displacement (IMAGE 1 in Supplementary material). Fracture fixation was performed by double plating after fracture reduction, utilizing a Depuy Synthes 2.7–3.5 mm Variable Angle (VA) Locking Compression Plate (LCP) placed anteriorly at the medial fracture site and a Depuy Synthes superior 2.7/3.5 LCP clavicle plate with lateral extension was placed at the lateral fracture site (IMAGE 2 in Supplementary material). Postoperative X-rays showed an anatomical reduction (IMAGE 3 in Supplementary material). Direct post-operative the patient reported significant pain relief with a NRS of 0–2 and started active range of motion of the shoulder with help of a physiotherapist. Weight bearing activities were avoided for 6 weeks. The patient was discharged to a rehabilitation centre for further treatment of his spinal cord injury and bipolar clavicle fracture. The patient visited the outpatient clinic after 6 weeks. X-Rays showed initial signs of consolidation and a maintained anatomical reduction (IMAGE4 in Supplementary material). Range of motion: abduction/adduction: 65/0/20 degrees. Pain was reduced to a NRS of 1. X-Ray in July 2019 showed complete consolidation, no implant failures (IMAGE5 in Supplementary material).
Literature review
The electronic databases PubMed, the Cochrane library and EMBASE were searched up on September 25th, 2017. The search was performed with both keywords and MeSH terms. The search consisted of: bipolar OR segmental AND clavicle. Two reviewers (KR and TG) independently screened titles and abstracts for their relevance. Additionally, the reference lists of all included articles were additionally searched for other relevant references.
Studies designed to evaluate the outcomes of conservative and/or operative treatment of segmental bipolar clavicle fractures in adults (> 16 years) were included. Editorials and commentaries were excluded, as well as synthetic, cadaveric and animal studies. Inclusion was not otherwise restricted by study size, language or publication type.
Primary outcomes considered were pain reduction and shoulder function. Secondary outcomes considered are complications, such as infection, non-union and implant failure. None of the ten case reports described how pain, shoulder function and complications were scored. Only two case reports provided a DASH score.
Results
Details of the literature search are shown in Fig. 1. All ten included studies are single case reports. Characteristics of the studies are shown in Table 1. Three elderly patients were treated conservatively and seven patients were treated operatively. In most of these operatively treated patients double plate fixation was performed. In two cases clinical impairment was seen. The medial clavicle fracture was missed directly after the injury. In the first case the medial fracture was found after 4 days and before surgery, so no extra operation was needed. In the second case the medial fracture was found after 28 days. An extra operation was performed. In all cases the fractures healed and in one case the operation was complicated by a pneumothorax [8]. In three cases implant removal was performed.
Fig. 1.
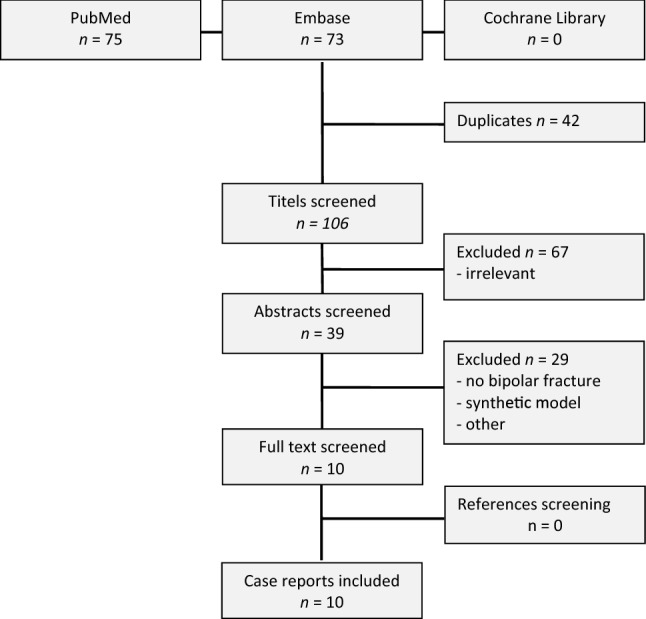
Flow chart of article inclusion
Table 1.
Characteristics of included studies
| References | Year | Study design | Gender | Age (years) | Trauma | Dislocation | Treatment | Method | Postoperative treatment | Result |
|---|---|---|---|---|---|---|---|---|---|---|
| Talboys et al. [3] | 2016 | Case report | Female | 79 | Stumbled over slipper | Medial dislocation | Conservative | Sling | – | Pain free FROM after 3 months |
| Yalizis et al. [4] | 2016 | Case report | Male | 38 | Fall from push bike | Lateral and medial dislocation | Surgical | Lateral hook plate, medial plate | – | Pain free FROM after 3 months |
| Grossi [5] | 2015 | Case report | Male | 41 | Fall from roof | Lateral and medial dislocation | Surgical | Superior reconstruction plate and lateral K-wire | 7 weeks no weight-bearing + physiotherapy | Pain free FROM after 3.5 months |
| Sopu et al. [6] | 2015 | Case report | Male | 52 | Fall from push bike | Medial dislocation | Surgical | Medial plate, lateral no fixation. | 6 weeks no weight-bearing | Pain free FROM after 4 months |
| Varelas et al. [7] | 2015 | Case report | Female | 68 | Fall on ice | Lateral and medial dislocation | Surgical | Medial and lateral locking plate | Sling, no weight-bearing for 6 weeks | Pain free FROM after 3 months. DASH = 5 |
| Skedros et al. [8] | 2014 | Case report | Male | 33 | Motocross accident | Lateral and medial dislocation | Surgical | Medial and lateral reconstruction plate | 12 weeks no weight-bearing + physiotherapy | Pain free FROM after 5 months. DASH = 8 |
| Sethi et al. [9] | 2012 | Case report | Female | 70 | Fall from stairs | Medial and lateral undisplaced | Conservative | Sling | 4 weeks immobilisation in sling | Pain free FROM after 6 months |
| Miller et al. [10] | 2009 | Case report | Male | 17 | Car accident | Lateral and medial dislocation | Surgical | Medial and lateral locking plate | – | Pain free FROM after 6 months |
| Heywood et al. [11] | 2005 | Case report | Male | 54 | Molest | Lateral and medial dislocation | Surgical | Lateral hook plate, medial plate | Physiotherapy | Consolidation after 3 months |
| Pang et al. [12] | 2003 | Case report | Male | 76 | Motorcycle accident | Medial dislocation | Conservative | Sling | – | FROM after 6 months with no instability |
FROM functional range of motion
Discussion
This study describes the treatment of a patient with a bipolar clavicle fracture and presents a review of the current literature regarding bipolar clavicle fractures. Only ten single case reports could be included in the review, describing varying treatment modalities. In most patients, surgical treatment with the use of double plating was performed. Only in elderly patients conservative treatment was adopted. All included patients were pain free and had a full range of motion after 3–6 months. Furthermore only 2 of the 10 available case reports described a validated functional outcome score.
Most of the bipolar fractures are sustained by high energy trauma. Of all clavicle fractures 21–28% are lateral fractures and 2–3% are medial fractures [1]. A truly bipolar clavicle fracture is a rare entity. The term ‘’floating clavicle’’ refers to an AC- and SC-displacement without fractures [13, 14]. A bipolar fracture can easily be missed and may therefore complicate the clinical progress. It is advised to assess the whole length of the clavicle clinically and radiologically when fractured, in order not to miss a bipolar fracture. When there is any doubt, the use of a computed tomography scan is recommended.
Research has shown that a non-operative treatment of an isolated, non-displaced, medial clavicle produced limited pain and excellent functional outcomes [2]. Displaced medial fracture require operative treatment [15].
Lateral fractures require operative management if displaced [16]. Two studies in this review used a hook plate for fixation of the lateral fracture. One article has shown that locking plate fixation is superior compared to hook plate fixation in lateral clavicle fractures [17].
This study presents a complete overview of the current literature. Due to the rarity of this injury, a formal meta-analysis of the literature was not possible.
These injuries may impair clinical progress if undetected, as seen in two cases in our review. We suggest that operative treatment should be performed for displaced medial and lateral fractures in a bipolar fracture, although the treatment of choice depends on the age of the patient, daily activities and comorbidity. While displaced fractures may benefit from surgery, treating only one part of a bipolar clavicle fracture may complicate treatment should the other part become displaced at a later instance.
Conclusion
Based on the current evidence, no strong recommendation can be made on the treatment of bipolar clavicle fractures. Literature has shown that operative treatment should be performed in isolated medial an lateral clavicle fractures. We suggest that displaced bipolar clavicle fractures should be treated operatively. However the treatment of a bipolar clavicle fracture depends on the age of the patient, daily activities and comorbidity.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Funding
No funding was received.
Compliance with ethical standards
The treatments described in the manuscript were performed in accordance with the ethical standards of our institute and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Conflict of interest
The authors, their immediate family, and any research foundation with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
Ethical approval
Not applicable, experimental procedures involving human participants were not performed.
Informed consent
Informed consent was obtained.
References
- 1.Khan LAK, Bradnock TJ, Scott C, Robinson CM. Fractures of the clavicle. J Bone Joint Surg. 2009;91(2):447–460. doi: 10.2106/JBJS.H.00034. [DOI] [PubMed] [Google Scholar]
- 2.Salipas A, Kimmel LA, Edwards ER, Rakhra S, Moaveni AK. Natural history of medial clavicle fractures. Injury. 2016;47(10):2235–2239. doi: 10.1016/j.injury.2016.06.011. [DOI] [PubMed] [Google Scholar]
- 3.Talboys RJ, Mak M, Modi N, Garg S, Deo H. A unique bipolar clavicle fracture sustained with minimal trauma. Int J Shoulder Surg. 2016;10(1):49–51. doi: 10.4103/0973-6042.174524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Yalizis MA, Hoy GA, Ek ETH. A rare case of bipolar clavicle fracture. Case Rep Orthop. 2016;2016:4309828. doi: 10.1155/2016/4309828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Grossi EA. Segmental clavicle fracture. Revista Brasileira de Ortopedia. 2011;46(6):733–735. doi: 10.1590/S0102-36162011000600018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sopu A, Green C, Molony D. Traumatic floating clavicle—a case report. Case Rep J Orthop Case Rep. 2015;5(2):12–14. doi: 10.13107/jocr.2250-0685.287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Varelas N, Joosse P, Zermatten P. Operative treatment of an atypical segmental bipolar fracture of the clavicle. Arch Trauma Res. 2015;4(4):e29923. doi: 10.5812/atr.29923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Skedros JG, Knight AN, Mears CS, Langston TD. Temporary sternoclavicular plating for an unusual double clavicle fracture (medial nonunion, lateral acute) complicated by an intraoperative pneumothorax. Case Rep Orthop. 2014;2014:206125. doi: 10.1155/2014/206125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sethi K, Newman SDS, Bhattacharya R. An unusual case of bipolar segmental clavicle fracture. Orthop Rev. 2012;4(3):26. doi: 10.4081/or.2012.e26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Miller D, Smith KD, McClelland D. Bipolar segmental clavicle fracture. Eur J Orthop Surg Traumatol. 2009;19(5):337–339. doi: 10.1007/s00590-009-0425-y. [DOI] [Google Scholar]
- 11.Heywood R, Clasper J. An unusual case of segmental clavicle fracture. J R Army Med Corps. 2005;151(2):93–94. doi: 10.1136/jramc-151-02-06. [DOI] [PubMed] [Google Scholar]
- 12.Pang KP, Yung SW, Lee TS, Pang CE. Bipolar clavicular injury. Med J Malaysia. 2003;58(4):621–624. [PubMed] [Google Scholar]
- 13.Bucholz RW Rockwood and green’s fractures in adults. 7th Revised edition. 2009; 1576.
- 14.Jain AS. Traumatic floating clavicle. A case report. J Bone Joint Surg B. 1984;66(4):560–561. doi: 10.1302/0301-620X.66B4.6746693. [DOI] [PubMed] [Google Scholar]
- 15.Frima H, van Heijl M, Michelitsch C, van der Meijden O, Beeres FJP, Houwert RM, Sommer C. Clavicle fractures in adults; current concepts. Eur J Trauma Emerg Surg. 2019 doi: 10.1007/s00068-019-01122-4. [DOI] [PubMed] [Google Scholar]
- 16.Vaishya R, Vijay V, Khanna V. Outcome of distal end clavicle fractures treated with locking plates. Chin J Traumatol. 2017;20(1):45–48. doi: 10.1016/j.cjtee.2016.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zhang C, Huang J, Luo Y, Sun H. Comparison of the efficacy of a distal clavicular locking plate versus a clavicular hook plate in the treatment of unstable distal clavicle fractures and a systematic literature review. Int Orthop. 2014;38:1461. doi: 10.1007/s00264-014-2340-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.