

Abstract
Background: Restrictions on movement and lockdown are measures taken in many nations, in response to the COVID-19 pandemic. University students are additionally burdened by the transition to distance e-learning. The aims of the study were to investigate the prevalence of anxiety and depression in university students and to identify associated risk factors.
Design and Methods: An online questionnaire was administered to 2,009 students in the University of Patras, Greece, during the national lockdown. Socio-demographic, academic data, and the forced disruption of daily life were assessed along with the Greek version of the Hospital Anxiety and Depression Scale.
Results: Anxiety and depression prevalence was 35.8% and 51.2% respectively. Age, school of study, financial status, self-perceived health status, level of satisfaction with the state’s and university’s response and specific aspects in the daily routine were associated with both anxiety and depression scores. At higher odds of both depression and anxiety were students with low income, bad health status, annoyed at staying home and those who encountered difficulties with the online education system. Additional risk factors for depression were studies in humanities and social sciences, and low satisfaction with the university’s response, while for anxiety were studies in agricultural sciences and absence of information about COVID-19.
Conclusions: The proportion of Greek students showing depression and anxiety, during the restrictive measures, is alarming. Mental health in university students should be monitored. Mitigation strategies should focus on specific personal, academic and social variables that have been identified as protective factors.
Significance for public health.
In response to the COVID-19 pandemic, governments and health organizations applied strict measures and movement restrictions, that disrupt normal daily routine and may seriously affect mental health. In addition, university students were forced to follow the unplanned shift from traditional face-to-face education to distance e-learning. This cross-sectional study explores the prevalence of anxiety and depression among students at a Greek university, during the national lockdown and reveals that university students are subjected to excess psychological burden due to both the compulsory lockdown and the educational transformation. Policy responses deployed to combat COVID-19 have a serious impact on resilience and mental health. Emotional and behavior balance and mental health should be safeguarded in university students, through the implementation of evidence-based psychosocial interventions. Academic and psychosocial features, that were identified to act as risk factors for anxiety and depression, give valuable information on developing effective mitigation actions.
Key words: anxiety, COVID-19, depression, lockdown, university students
Introduction
Population confinement, social distancing, fear and uncertainty about the outcome of the pandemic, following the COVID-19 outbreak, have already been incriminated for important psychological implications in the general population1,2 and in specific groups, like health care workers3 and students.4 In the face of an epidemic, the health organizations and the governments are challenged to find the intricate balance between safeguarding the physical health of the population, through the implementation of anti-contagion measures, and salvaging mental well-being of the citizens. In Greece, coronavirus appeared on February 26, 2020. The first cases were individuals and their contacts who had travelled to Italy, Israel, and Egypt. The operation of all educational institutions was suspended on 10 March, with 89 confirmed cases and no deaths in the country. On 13 March all restaurants, bars, museums, shopping centres and sports facilities in the country were closed down, followed by retail shops and the suspension of religious services three days later. Public gatherings of 10 or more people were banned on 18 March and violators would be fined 1,000 €. On 23 March, the Greek government announced restrictions on all non-essential movements throughout the country, until 4 May. The measures taken in Greece were among the strictest in Europe. Despite the elderly population, the fragile economy and the enormous load of the refugee crisis, Greece gained international praise for containing the spread of the virus and keeping the casualty toll low. After a 42-day lockdown, Greece began to gradually lift restrictions on movement and return to “normal” business activity.5
Recent epidemiological studies have documented that university students are confronted with unique stressors and financial pressure; the transition to a new, competitive and demanding environment where they are asked to develop responsibility, to make important life choices, and form new social networks along with the separation from the core family are some of the stressors that increase the risk of mental health problems.6 Further, university students are at the age of a high risk for the onset of mental illness.7 During lockdown, university students had additional obstacles to face. Except for the restrictive measures taken for the whole population, the lives of students changed due to the switch from on-campus to online teaching. Regarding the aforementioned documented tendency of students to mental health problems, concerns arise about the additional impact of confinement and new education format on this subpopulation.
On the other hand, strict measures taken to limit the spread of the disease during a pandemic, like social distancing, quarantine and isolation, seriously affect mental health, including insomnia, low mood, stress, irritability and confusion.8 Substance and alcohol dependency are common longer-term effects of quarantine.9 A recent study conducted in a Greek population three weeks after the national lockdown, reported an exacerbation of sleep disturbances, with 37.6% of the participants suffering from insomnia, a percentage greater than the worldwide prevalence before the pandemic (3.9% to 22%).10 Increase of stress levels, worry about health, feelings of loneliness, changes in social life and uncertainty about the future, are some of the causes for cognitive arousal and sleep disturbances, according to the authors. This survey was disseminated to the students of the University of Patras, Greece, on 15th April 2020. On that day, the total number of confirmed cases in Greece was 2,192 (of which 56.4% were men) and the total number of fatalities stood at 102; 28 of these were women. Of the total, 89% of the victims had underlying health issues and/or their average age was 70 years or more.11 The aim of the study was to assess the prevalence of anxiety and depression in the students at the University of Patras after 24 days of lockdown. Further we evaluated the associations of anxiety and depression with the changes in the daily routine caused by the measures’ imposition.
Design and Methods
Study design
A cross-sectional survey design was adopted to assess the effects on the mental health of the students at the University of Patras in Greece, during the pandemic of COVID-19, by using an anonymous online questionnaire. The University consists of 7 Schools, 35 Departments and offers 49 Postgraduate Study Programs, which altogether number 28,458 registered students, including those at the postgraduate and doctoral level. Participants were recruited from the entire student population. The online survey was disseminated to university students through the Open eClass platform, an integrated Course Management System, offered by the Greek University Network GUnet, to support asynchronous eLearning services. Students need to be registered to Open eClass in order to be able to attend a course. Open eClass, beyond its educational content, provides information, communication and collaboration tools, like an online announcement board, message exchange between students and instructors and alerts. The survey was announced first to courses’ instructors of all University Schools, through e- mails, and then, to the entire students’ population through the Open eClass platform. Relevant posts were uploaded to the social media platform of Facebook in University students’ pages. In the introduction page of the questionnaire, information about the procedure, scope and required time to answer the survey, were provided. We notified that the participation was voluntary and the confidentiality and anonymity of the participants would be retained. Moreover, the names and the emails of the investigators were given, and the participants were able to communicate with them and ask any question they wanted. Consent for participation was given by each participant digitally before initiating the survey and the research was conformed to the ethical guidelines of the Helsinki Declaration as revised in 2013. Data collection took place over 23 days, from 15 April to 7 May 2020. Within this time interval we received 2,009 responses. Considering a confidence level of 99%, we calculated that the actual margin of error was 2.8%.
Description of the questionnaire
The questionnaire comprised of 51 questions and statements about i) socio-demographic characteristics (age, gender, educational status, monthly income, place of residence during studies, having children, being a caregiver) and medical issues (current selfreported health status, chronic disease, physical or learning disability); ii) academic data (school, department and year of studies); iii) questions regarding lifestyle and changes in daily routine during the lockdown (place of residence, being informed about the virus, satisfaction level on handling and response to COVID-19 by the government and the National Public Health Organization, restraining from carnival fiestas and gatherings, changes in appetite, in physical exercise, in sleeping, in smoking and alcohol consumption, entertainment via electronic media, dissatisfaction about staying at home, not meeting family/friends, frequency of going out, belief about the time needed to return to normality); iv) questions regarding the distance e-learning of the university (satisfaction with University’s response, attendance of courses, difficulties with distance learning, preference on distance or face-to-face learning) and v) the Greek version of the Hospital Anxiety and Depression Scale (HADS).12 It is divided into an Anxiety subscale (HADS-A) and a Depression subscale (HADS-D), both containing seven items, rated from 0 to 3. The cut-off values for each subscale are: score 0-7 “non case”, score 8-10 “doubtful case” and score 11-21 “case” of either anxiety or depression. While this scale was initially developed to identify anxiety disorders and depression among patients in non- psychiatric hospital clinics, it is reported to perform equally well at screening anxiety and depression in the general population.13
Statistical analyses
Group proportions were calculated for categorical variables. Spearman’s rank correlation coefficient was estimated to assess the association between variables. Group comparisons were performed by the non-parametric Mann-Whitney U test. Associations of anxiety or depression scores with each of the independent variables described at the questionnaire were assessed by General Linear Models (GLM). The statistical significance level was set at 0.050.
Finally, subjects were classified into two groups, i.e., “no case” or “case”, by summing the doubtful and definite cases. The associations of groups of either anxiety or depression “cases” or “non cases” with independent variables, found to be related with the scores in the GLM models, were assessed via multivariate logistic regression models. Factors with p≤0.100 were kept in the models. Statistical analysis was performed by IBM SPSS v.25 statistical software (IBM Corp., Armonk, NY, USA).
Results
Study population
We received responses from 2,009 students who had completed the questionnaires (completion rate: 98.8%). Sociodemographic characteristics of the participants are presented as percentages for males, females, and total in Table 1.
The responses of students regarding the state’s attitude, the university’s handling, the distance learning system, and the changes that occurred in their daily routine due to the pandemic and the measures imposed, are presented in Supplementary Material (Table S1).
Anxiety and depression
Table 2 presents the results of the anxiety and depression scores, as extracted by the HADS scale, and the corresponding classification by gender and in total. Cronbach’s alpha coefficients of internal consistency were found to be 0.81 for anxiety and 0.79 for depression subscale. Age was positively correlated with anxiety score, in both genders (Spearman’s r = 0.171, p<0.001 for men, and r = 0.120, p<0.001 for women), while depression score showed no such correlation. Anxiety and depression scores were also correlated (Spearman’s r = 0.447, p<0.001 for men, and r = 0.461, p<0.001 for women). Depression score was not different among males and females (Mann Whitney U test, p=0.239), while anxiety score was higher in females (median value = 7.0) compared to males (median value = 4.0), as the Mann-Whitney U test revealed (p<0.001).
General linear models of anxiety and depression scores
Univariate analysis of variance was conducted to examine whether the anxiety and depression scores differ between the groups generated by the examined factors. In all models, age and gender were included as covariates. The main outcomes are presented in Figure 1, while all models are presented in the Supplementary Material (Figure S1).
Table 1.
Socio-demographic characteristics of the students’ population.
| Characteristics | Males | Females | Total | |
|---|---|---|---|---|
| (n=657) | (n=1352) | (n=2009) | ||
| Age, mean (SD) | 22.1 (3.5) | 22.0 (3.4) | 22.0 (3.4) | |
| Educational level (%) | Undergraduate | 92.1 | 90.7 | 91.1 |
| Post-graduate | 5.6 | 7.8 | 7.1 | |
| Ph.D. candidate | 2.3 | 1.5 | 1.7 | |
| School of study (%) | Humanities and Social Sciences | 3.5 | 14.6 | 11.0 |
| Health Rehabilitation Sciences | 1.2 | 5.3 | 4.0 | |
| Health Sciences | 20.2 | 23.7 | 22.6 | |
| Natural Sciences | 20.4 | 24.4 | 23.1 | |
| Economics & Business | 7.9 | 6.9 | 7.2 | |
| Engineering | 45.2 | 23.7 | 30.7 | |
| Agricultural Sciences | 1.5 | 1.4 | 1.4 | |
| Year of study (%) | 1 | 21.5 | 22.9 | 22.4 |
| 2 | 15.8 | 20.1 | 18.7 | |
| 3 | 16.3 | 17.2 | 16.9 | |
| 4 | 16.9 | 15.2 | 15.8 | |
| 5 | 11.0 | 9.7 | 10.1 | |
| 6 | 7.3 | 4.3 | 5.3 | |
| Awaiting graduation | 11.3 | 10.6 | 10.8 | |
| Place of residence | With family | 21.6 | 22.6 | 22.3 |
| (during studies) (%) | Alone on rent | 59.2 | 55.0 | 56.3 |
| Alone in own apartment | 5.0 | 5.0 | 5.0 | |
| Sharing apartment | 8.5 | 10.5 | 9.9 | |
| Dorm | 3.7 | 3.4 | 3.5 | |
| Other | 2.0 | 3.6 | 3.0 | |
| Monthly income available | <100€ | 19.2 | 24.6 | 22.8 |
| for personal needs (%) | 100-200€ | 33.3 | 37.3 | 36.0 |
| 200-300€ | 27.9 | 27.2 | 27.4 | |
| >300€ | 19.6 | 10.9 | 13.7 | |
| Current self-reported | Very bad | 1.4 | 0.7 | 0.9 |
| health status (%) | Bad | 2.1 | 1.1 | 1.4 |
| Moderate | 12.0 | 12.7 | 12.5 | |
| Good | 39.4 | 45.9 | 43.8 | |
| Very good | 45.1 | 39.6 | 41.4 | |
| Are you a caregiver? | Yes | 5.2 | 5.8 | 5.6 |
| (e.g., for a family member) (%) | No | 94.1 | 93.4 | 93.6 |
| Prefer not to answer | 0.8 | 0.8 | 0.8 | |
| Do you suffer from a chronic | Yes | 5.8 | 8.7 | 7.7 |
| disease? (%) | No | 91.8 | 89.2 | 90.0 |
| Prefer not to answer | 2.4 | 2.1 | 2.2 | |
| Do you believe you suffer from | Yes | 1.5 | 1.0 | 1.1 |
| a physical disability? (%) | No | 97.6 | 98.7 | 98.3 |
| Prefer not to answer | 0.9 | 0.4 | 0.5 | |
| Do you believe you suffer from | Yes | 7.8 | 7.3 | 7.5 |
| a learning disability? (%) | No | 90.9 | 91.7 | 91.4 |
| Prefer not to answer | 1.4 | 1.0 | 1.1 |
Students in the Schools of Health and Health Rehabilitation Sciences showed significantly lower anxiety scores than the rest of the students. The highest anxiety scores were observed in the School of Agricultural Sciences. Students in Health Sciences also exhibited the lowest depression scores, while students in the other schools did not differ with each other (Figure 1). Anxiety and depression scores were progressively reduced, as the available monthly amount to be spent for personal needs increased (Figure 1). Students feeling satisfied with the response of the University concerning distance learning had lower anxiety and depression scores. On the other hand, those who encountered problems and difficulties with the distance learning system showed higher anxiety and depression scores (Figure 1). Noteworthy is the negative correlation between the difficulties with distance learning and the satisfaction with the university’s response (Spearman’s r = -0.456, p<0.001). Students who were “very bothered” for being forced to stay at home had the highest mean depression and anxiety scores (10.59 and 7.38 respectively) (Figure 1).
Logistic regression models for anxiety and depression
As it is deduced from Table 2, the prevalence of anxiety, either doubtful or definite cases, was 35.8% and the corresponding depression prevalence was 51.2%. Anxiety and depression classifications were transformed to a binary variable, in which the doubtful and definite cases were summated, and were tested, via multivariate logistic models, against the factors having found to associate with anxiety and depression scores in the univariate analysis (Table 3). The models were constructed through two blocks. In the first block the “status” variables were included, i.e., school of study, chronic disease, self-reported health status, etc., and in the second, the factors connected to COVID-19 and the consequential restrictive measures were examined, in order to evaluate the effect of the pandemic measures on anxiety and depression, after controlling for the effects of status variables.
The status variables accounted for the 17.7% of the “variation” of anxiety, and for the 12.2% of the “variation” of depression, as calculated by the Nagelkerke R2 of the respective models. Interestingly, when the epidemic-related factors were included in the models, the proportion of “variation” in anxiety associated with the factors, increased to 26.9% and that in the depression reached 34.7%.
Comparison of anxiety and depression prevalence with the pre-COVID-19 era
The prevalence of anxiety and depression observed in this study was compared to the one measured in the same University three years ago, using the same HADS Scale.14 The results are presented in Figure 2. Anxiety declined in 2020, giving an overall prevalence of 35.8%, compared to the 56.7% occurring in 2017. The highest decrease is observed in the Schools of Engineering and Health Sciences. Depression has increased to 51.2% versus 36.0% in 2017.14 The highest increase (30.8%) is observed in the School of Humanities and Social Sciences.
Discussion
Over than half of our students (51.2%) are experiencing depression and 35.8% display abnormal levels of anxiety. Three years ago, students in our university were more anxious but less depressed. In another Greek university, anxiety and depressive feelings increased in >65% and 30% of the students respectively, during the lockdown.15 Moderate to extremely severe anxiety and depression symptoms were observed in the 21.34% and the 34.19% of Spanish students.4 Among 8,004 French students, 43.0% suffered from depression and 39.1% from anxiety.16 Similar results were obtained from the 2,031 US college students, with 71.26% of the participants stating that their stress/anxiety levels had increased during the pandemic.17
The decreased anxiety during the pandemic compared to the one found three years ago among our students is a rather unexpected finding. Most studies4,15,17 have reported increase in students’ levels of stress/anxiety during the pandemic and the confinement period. Living with parents is referred as a protective factor against students’ anxiety.18 However, even though 63% of our students stated they have returned to their family home during the lockdown (Table S1), the general linear models revealed no difference in anxiety scores between those who remained in student residence and those who returned to their parents (Figure S1). Consequently, the observed decrease in anxiety cannot be attributed to the return of students to their family home. Other factors known for augmenting students’ anxiety are the demanding academic tasks and the social relationships that students are requested to deal with, during studies.7 Our survey took place during the Greek Easter, so students were on vacation regarding their academic tasks. Similarly, in a Chinese study conducted during the Chinese New Year, the authors observed significantly lower anxiety in students compared to relevant studies.19 In a US survey, students that felt decreased stress and anxiety during the pandemic attributed it to saving time due to reduced schoolwork, to pursuing hobbies or to not be obliged to interact with others.17 It may be due to the compulsory confinement, combined with the cessation of academic work and the minimization of social interactions, that our students felt less anxiety but more depression compared to three years ago.
Gender and depression were not associated in our study, in contrast with previous findings;20,21 however, women had 2.07 higher possibilities of experiencing anxiety. Despite our results not concurring with the higher prevalence of depression in women found in previous studies, it has been reported that during the past two decades, social standing and income of women has improved,22 which may explain the similar depression rates in men and women, observed in our study population.
Table 2.
Anxiety and depression scores and students' classification.
| Males | Females | Total | ||
|---|---|---|---|---|
| Anxiety score | mean (SD) | 5.4 (4.3) | 7.1 (4.3) | 6.6 (4.4) |
| Depression score | mean (SD) | 8.3 (4.3) | 8.5 (4.2) | 8.5 (4.2) |
| Anxiety categories* (%) | Non cases | 73.7 | 59.6 | 64.2 |
| Doubtful cases | 13.4 | 20.1 | 17.9 | |
| Cases | 12.9 | 20.3 | 17.9 | |
| Depression categories* (%) | Non cases | 49.9 | 48.2 | 48.8 |
| Doubtful cases | 15.8 | 15.2 | 15.4 | |
| Cases | 34.2 | 36.5 | 35.8 |
*Classification: Non cases: score 0-7, doubtful cases: score 8-10, cases: score 11-21.
Figure 1.
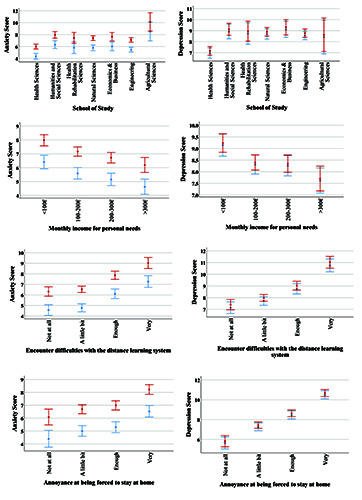
Estimated marginal means of anxiety (left panel) and depression (right panel) scores in relation to groups according to school of study, monthly income, difficulties with the distance learning system and annoyance at being forced to stay at home. Blue bars with triangles represent males and red bars with circles represent females. Error bars present the 95% confidence intervals of the means.
Figure 2.
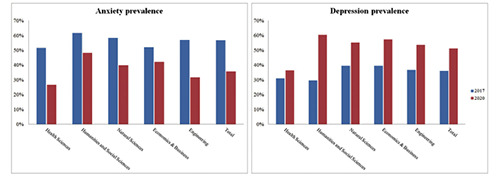
Students' prevalence of anxiety and depression (sum of doubtful and definite cases) in 2017 (blue bars) and in 2020 (red bars), per school of studies.
Table 3.
Logistic regression models of anxiety and depression.
| Anxiety | Depression | |||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Status variables | ||||
| Age | 1.09 | 1.05-1.13 | 1.05 | 1.01-1.09 |
| Gender | ||||
| Male | 1 | |||
| Female | 2.07 | 1.62-2.65 | ||
| School of Study | ||||
| Health Sciences | 1 | 1 | ||
| Humanities and Social Sciences | 1.83 | 1.25-2.68 | 1.96 | 1.33-2.90 |
| Health Rehabilitation Sciences | 1.32 | 0.76-2.28 | 1.76 | 1.00-3.12 |
| Natural Sciences | 1.53 | 1.11-2.10 | 1.77 | 1.30-2.41 |
| Economics & Business | 1.44 | 0.92-2.26 | 1.67 | 1.05-2.67 |
| Engineering | 1.16 | 0.85-1.59 | 1.55 | 1.16-2.08 |
| Agricultural Sciences | 3.20 | 1.22-8.36 | 1.17 | 0.46-3.01 |
| Monthly income for personal needs | ||||
| <100€ | 1.50 | 1.02-2.20 | 1.52 | 1.04-2.22 |
| 100-200€ | 1.55 | 1.08-2.22 | 1.22 | 0.87-1.72 |
| 200-300€ | 1.26 | 0.87-1.83 | 1.39 | 0.97-1.97 |
| >300 € | 1 | 1 | ||
| Current self-reported health status | ||||
| Very bad | 0.79 | 0.21-2.96 | 0.74 | 0.21-2.63 |
| Bad | 7.77 | 2.99-20.16 | 8.58 | 2.60-28.34 |
| Moderate | 3.36 | 2.39-4.71 | 3.71 | 2.52-5.45 |
| Good | 1.87 | 1.48-2.37 | 1.53 | 1.22-1.91 |
| Very good | 1 | 1 | ||
| Do you suffer from a chronic disease | ||||
| No | 1 | 1 | ||
| Yes | 1.09 | 0.73-1.63 | 0.64 | 0.42-0.96 |
| Prefer not to answer | 2.84 | 1.32-6.13 | 1.12 | 0.52-2.41 |
| Physical disability | ||||
| No | 1 | |||
| Yes | 2.87 | 0.92-9.00 | ||
| Prefer not to answer | 4.11 | 0.77-21.96 | ||
| Do you have children? | ||||
| No | 1 | |||
| Yes | 0.23 | 0.09-0.61 | ||
| Prefer not to answer | 0.12 | 0.00-609.85 | ||
| Are you a caregiver | ||||
| No | 1 | |||
| Yes | 1.43 | 0.87-2.34 | ||
| Prefer not to answer | 2.96 | 0.89-9.80 | ||
| COVID-19 related variables | ||||
| Informed about COVID-19 | ||||
| Not at all | 33.99 | 2.88-401.37 | ||
| Not very much | 0.85 | 0.44-1.64 | ||
| Quite a lot | 1.02 | 0.82-1.27 | ||
| Very much | 1 | |||
| Annoyance at being forced to stay at home | ||||
| Not at all | 1 | 1 | ||
| A little bit | 1.16 | 0.76-1.76 | 1.74 | 1.16-2.61 |
| Enough | 1.21 | 0.78-1.89 | 2.82 | 1.86-4.25 |
| Very | 1.73 | 1.08-2.76 | 5.66 | 3.66-8.74 |
| Increase of food appetite | ||||
| Not at all | 1 | 1 | ||
| A little bit | 1.27 | 0.92-1.73 | 0.88 | 0.65-1.19 |
| Enough | 1.11 | 0.80-1.54 | 1.18 | 0.86-1.62 |
| Very | 1.23 | 0.85-1.77 | 1.38 | 0.95-2.01 |
| It has decreased | 1.93 | 1.28-2.90 | 1.50 | 0.98-2.29 |
| Annoyance at not meeting friends/family | ||||
| Not at all | 1 | |||
| A little bit | 2.62 | 1.19-5.76 | ||
| Enough | 2.49 | 1.15-5.37 | ||
| Very | 3.12 | 1.44-6.76 | ||
| Do you exercise more often | ||||
| Yes | 1.08 | 0.82-1.43 | 0.98 | 0.74-1.29 |
| No | 1.42 | 1.09-1.84 | 1.64 | 1.26-2.13 |
| The same | 1 | 1 | ||
| Do you sleep more | ||||
| Yes | 1.09 | 0.85-1.39 | 1.37 | 1.07-1.74 |
| No | 2.28 | 1.64-3.16 | 1.68 | 1.20-2.37 |
| The same | 1 | 1 | ||
| Has your involvement with electronic media increased | ||||
| Not at all | 1 | 1 | ||
| A little bit | 1.23 | 0.82-1.86 | 1.03 | 0.69-1.54 |
| Enough | 1.10 | 0.74-1.61 | 1.29 | 0.88-1.88 |
| Very | 1.48 | 1.00-2.20 | 2.23 | 1.51-3.30 |
| Do you smoke more | ||||
| Yes | 1.32 | 0.85-2.03 | 1.53 | 0.96-2.43 |
| I do not smoke | 0.90 | 0.67-1.20 | 1.02 | 0.76-1.38 |
| No | 1 | 1 | ||
| Going out for essential activities (times/week) | ||||
| <2 | 1 | |||
| 2-4 | 0.72 | 0.56-0.92 | ||
| 5-7 | 0.67 | 0.50-0.91 | ||
| 8-10 | 0.63 | 0.38-1.05 | ||
| >10 | 0.64 | 0.36-1.14 | ||
| Encounter difficulties with the distance learning system | ||||
| Not at all | 1 | 1 | ||
| A little bit | 1.08 | 0.80-1.46 | 1.31 | 0.98-1.75 |
| Enough | 1.61 | 1.16-2.22 | 1.36 | 0.97-1.91 |
| Very | 1.71 | 1.16-2.50 | 1.94 | 1.24-3.02 |
| Satisfaction with state's handling of COVID-19 pandemic | ||||
| Not at all | 1.33 | 0.81-2.18 | ||
| A little bit | 1.54 | 1.07-2.22 | ||
| Enough | 1.16 | 0.90-1.48 | ||
| Very | 1 | |||
| Satisfaction with University's response for distance learning | ||||
| Not at all | 1.95 | 1.08-3.51 | ||
| A little bit | 1.45 | 1.02-2.06 | ||
| Enough | 0.99 | 0.77-1.29 | ||
| Very | 1 | |||
| Encounter difficulties with daily diet/feeding | ||||
| Not at all | 1 | |||
| A little bit | 1.58 | 1.15-2.17 | ||
| Enough | 1.49 | 0.87-2.54 | ||
| Very | 2.65 | 1.17-6.01 | ||
| Residence during lockdown | ||||
| Remain in student residence | 1 | |||
| Student residence is my family home | 1.08 | 0.71-1.66 | ||
| Have returned to family home | 1.50 | 1.02-2.23 | ||
| Live in friends | 1.84 | 0.60-5.67 | ||
| Live in another place | 0.72 | 0.38-1.37 | ||
| Not participation in carnival events | ||||
| Not at all | 0.66 | 0.49-0.87 | ||
| A little bit | 0.83 | 0.62-1.11 | ||
| Enough | 1.06 | 0.79-1.43 | ||
| Very | 1 | |||
OR, odds ratio; CI, confidence interval; bold values indicate ORs with p<0.100.
Coinciding with previous studies, age, chronic diseases, selfreported health status,1 monthly income20 and school of study,4,23 were found to be the key demographics and underlying conditions to be associated with both depression and anxiety. Lower household income has been previously reported as a predictive factor for symptoms of depression.20 In line with this and other surveys,24 students in our university that have at their disposal less than 100 € to spend for their monthly personal needs were at higher risk of developing anxiety and depression, compared to their colleagues spending more than 300 €.
A surprising finding was the lower possibility (OR = 0.64) of those suffering from a chronic disease to undergo depression. This could possibly be explained by the speculation that these students are used to confronting the disease and its uncertainty, and have learnt to cope with such situations.
Variations across academic disciplines were observed in this study, in accordance to a previous one,4 that found Engineering to be the field with the lowest scores and Arts and Humanities the field with the highest scores in anxiety, depression, and stress. These differentiations may be related to different stressors, level of competition and traits developed across distinct fields of study. Ludwig23 pointed out that professions that require logical, objective, and proof-based forms of expression are more likely to attract more emotionally stable people, able to focus on objective problems outside of themselves. On the other side, professions that require more intuitive, subjective, and emotive forms, like literature, visual arts etc. attract people with temperament and particular cognitive style best suiting these requirements.
Students in the Health Sciences were found to experience less severe anxiety and depression than non-medical students, in consistency with previous studies on the psychological effect of COVID-19.25 A possible explanation may be that medical students privilege an advanced and deeper knowledge about viruses and epidemics compared to others.
Being informed about COVID-19 was identified as a protective factor for our students. Even though only the 0.5% of our study population stated “not at all” informed about COVID-19, they had 34.0 higher possibilities of manifesting anxiety. This finding reflects the importance of educational intervention and provision of reliable information.21 In line with this, knowledge about numbers of recovered and infected individuals was significantly associated with lower stress, anxiety, and depression in the general Austrian population.26. Knowledge plays a significant role in alleviating psychological distress in response to epidemics because it helps in understanding and accurately estimating the severity and risk of contamination.25 However, in other studies, exposure to COVID-19 related news was associated with increase in anxiety and depression.21,25 Three quarters of respondents indicated fear and worry induced by news outlets,17 and the authors attributed that to the large amount of misinformation, false and fabricated news.
Concerning the epidemic- and lockdown-related factors, annoyance at being forced to stay at home and compulsory social isolation, decreased food appetite, less physical activity, fewer hours of sleep, and more time spent on electronic media for entertainment were found as risk factors for both anxiety and depression. Preservation of social contacts, i.e., meeting family or friends every few days, has been previously reported to be significantly associated with lower anxiety and depression.26 A mental healthprotective role of physical activity was elucidated in our study, in accord with previous surveys.26,27 Students that followed a transition to a more sedentary lifestyle, i.e., those who spent less time to exercise during lock-down, had 1.4 and 1.6 times higher possibilities of manifesting anxiety and depression, respectively. Changes in eating and sleeping habits are important indicators of mental health status.2,17 In our survey, 55.6% of the respondents stated their sleep duration was increased during the lockdown, while another 15.3% were sleeping for fewer hours. Both categories were associated with higher possibilities of depression, while those with decreased sleep duration had higher possibilities of experiencing anxiety as well.
In our survey the grade of satisfaction with the University’s response for distance learning and the difficulties encountered with this delivery method were evaluated. A percentage of 67.2% gave a negative response to whether they prefer distance to face-to-face learning. In accordance, in another Greek university survey, 20% of the students found online teaching unsatisfactory and 40% believe it cannot replace face-to-face teaching.15
The psychological burden coming with the alteration in academic life and education is a major contributor affecting all students around the world, during the pandemic. Compulsory, rapid adaptation to distance learning may be a very stressful situation, especially for students who do not have access to laptops and internet facilities at home, or are obliged to share computers and IT equipment with their parents, siblings and other relatives who have to work from home.28 Increased difficulty stemming from the use of e-platforms, concerns about academic progress and delayed graduation, and fear of possible loss of scholarships are some of the worries expressed by students in previous studies.17,26 In our survey, the odds for those facing technical difficulties with the online courses were 1.9 times higher to feel depression and 1.7 times higher to exhibit anxiety than their counterparts.
This study reveals that the subpopulation of university students, which is the future core of society, are subjected to additional psychological burden due to the compulsory lockdown measures. It further identifies specific academic and daily life tasks that act as risk factors for augmenting anxiety and depression. Isolation and accompanying stressors may lead to long- term negative impact on emotional and behavioral balance and mental health.29 Among university students this balance should be safeguarded, especially during times of global crises. Specific mental health measures should be based on the identified academic and psychosocial risk or protective factors for mental health.
The study has some strengths and limitations. The large sample size, allowing for a robust analysis and solid associations, and the online survey format that allowed students to participate without violating the measures for social distancing, strengthen the study. Regarding the limitations, the cross-sectional nature of the study does not allow to draw conclusions about the cause-and-effect relationships between the variables involved. The online survey may contribute to some selection bias in the study result. Larger scale and long-term cohort studies in different universities should be conducted to verify and generalize the findings.
Conclusions
Lockdown due to the COVID-19 pandemic and the transition to distance learning were associated with increased psychological burden on the students in the University of Patras, Greece. Depression prevalence reached 51.6%, higher than the one determined three years ago (36.0%). On the contrary, anxiety was prevalent in the 35.8% of the students, compared to the 56.7% demonstrated in 2017. Epidemic-related factors seem to be highly associated with depression and anxiety, as the logistic regression models revealed. A high percentage (37.9%) of students are facing difficulties with the online distance learning system. Medical students seem to cope better than their colleagues with anxiety and depression, during the pandemic.
Acknowledgements
The authors would like to acknowledge all the students who participated in this survey.
Funding Statement
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- 1.Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health 2020;17:1729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Papandreou C, Arija V, Aretouli E, et al. Comparing eating behaviours and symptoms of depression and anxiety between Spain and Greece during the COVID- 19 outbreak: Cross-sectional analysis of two different confinement strategies. Eur Eat Disorders Rev 2020;28:836-46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wu W, Zhang Y, Wang P, et al. Psychological stress of medical staffs during outbreak of COVID-19 and adjustment strategy. J Med Virol 2020;92:1962-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Odriozola-González P, Planchuelo-Gómez A, Irurtia MJ, de Luis-García R.Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res 2020;290:113108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.National Public Health Organization. Current state of Covid- 19 outbreak in Greece and timeline of key containment events. [cited. 2020, Apr 10]. Available from: https://eody.gov.gr/en/current-state-of-covid-19-outbreak-in-greece-and-timeline-ofkey-containment-events/ [Google Scholar]
- 6.King N, Pickett W, McNevin SH, et al. Mental health need of students at entry to university: Baseline findings from the UFlourish Student Well-Being and Academic Success Study. Early Interv Psychiatry 2021;15:286-95. [DOI] [PubMed] [Google Scholar]
- 7.Duffy A, Saunders KEA, Malhi GS, et al. Mental health care for university students: a way forward? Lancet Psychiatry 2019;6:885-7. [DOI] [PubMed] [Google Scholar]
- 8.Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 2020;395:912-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wu P, Liu X, Fang Y, et al. Alcohol abuse/dependence symptoms among hospital employees exposed to a SARS outbreak. Alcohol Alcohol 2008;43:706-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Voitsidis P, Gliatas I, Bairachtari V, et al. Insomnia during the COVID-19 pandemic in a Greek population. Psychiatry Res 2020;289:113076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.National Public Health Organization. Daily report of epidemiological surveillance of the new coronavirus infection (COVID-19). Data until April 15,. 2020, at 15:00 [in Greek]. Accessed on:. 2020, Sep 15. Available from: https://eody.gov.gr/wp-content/uploads/2020/04/covid-grdaily-report-20200415.pdf [Google Scholar]
- 12.Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67:361-70. [DOI] [PubMed] [Google Scholar]
- 13.Bjelland I, Dahl AA, Haug TT, Neckelmann D.The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res 2002;52:69-77. [DOI] [PubMed] [Google Scholar]
- 14.Giourou E, Giannopoulou E, Alexopoulou S, et al. Undergraduate students' anxiety and depression prevalence at the University of Patras, Greece due to academic and other stressors including gender inequality: a cross-sectional study. Eur Psychiatry 2019;56:S120. [Google Scholar]
- 15.Patsali ME, Mousa D-PV, Papadopoulou EVK, et al. University students’ changes in mental health status and determinants of behavior during the COVID-19 lockdown in Greece. Psychiatry Res 2020;292:113298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Essadek A, Rabeyron T.Mental health of French students during the Covid-19 pandemic. J Affect Disord. 2020;277:392-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wang X, Hegde S, Son C, et al. Investigating mental health of US College students during the COVID-19 pandemic: crosssectional survey study. J Med Internet Res 2020;22:e22817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Cao W, Fang Z, Hou G, et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res 2020;287:112934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wang ZH, Yang HL, Yang YQ, et al. Prevalence of anxiety and depression symptom, and the demands for psychological knowledge and interventions in college students during COVID-19 epidemic: A large cross-sectional study. J Affect Disord 2020;275:188-93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J Affect Disord 2020;277:55-64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Salari N, Hosseinian-Far A, Jalali R, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta- analysis. Glob Health 2020;16:57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lim GY, Tam WW, Lu Y, et al. Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci Rep 2018;8:2861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ludwig AM. Method and madness in the arts and sciences. Creat Res J 1998;11:93-101. [Google Scholar]
- 24.Solomou I, Constantinidou F.Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: age and sex matter. Int J Environ Res Public Health 2020;17:4924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Xie L, Luo H, Li M, et al. The immediate psychological effects of Coronavirus Disease 2019 on medical and non-medical students in China. Int J Public Health 2020;65:1445-53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Traunmüller C, Stefitz R, Gaisbachgrabner K, Schwerdtfeger A.Psychological correlates of COVID-19 pandemic in the Austrian population. BMC Public Health 2020;20:1395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhang Y, Zhang H, Ma X, Di Q.Mental health problems during the COVID-19 Pandemics and the mitigation effects of exercise: A longitudinal study of college students in China. Int J Environ Res Public Health 2020;17:3722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sahu P. Closure of Universities due to Coronavirus Disease 2019 (COVID-19): Impact on education and mental health of students and academic staff. Cureus 2020;12:e7541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sinha M, Pande B, Sinha R.Impact of COVID-19 lockdown on sleep-wake schedule and associated lifestyle related behavior: A national survey. J Public Health Res 2020;9:1826. [DOI] [PMC free article] [PubMed] [Google Scholar]