

Abstract
Emergency department (ED) boarding is an indicator of less efficient hospital flow and is associated with longer inpatient length of stay, higher readmission rates and increased risk of mortality and medical errors. In addition to being associated with poor patient and staff satisfaction.
This article describes the efforts of six tertiary care governmental hospitals in the Kingdom of Saudi Arabia that have enrolled in a collaborative improvement project to reduce ED boarding time.
The hospitals implemented a multifaceted system intervention that included forming multidisciplinary flow improvement teams, implementing the National Health Service (NHS) SAFER patient flow bundle, visual management system and multidisciplinary ED bed huddles.
By the end of the project, all hospitals significantly reduced ED boarding time with a pooled mean difference of – 7.1 hours (16.6 before, 9.5 hours after, p<0.001), reaching a pooled average of 2 hours in March 2020.
Furthermore, by the end of the third learning session, all hospitals were able to achieve a boarding time below 6 hours. The enrolled hospitals also experienced an improvement in hospital flow process measures without any increase in 30-day readmission rates or bed occupancy rates.
Our project demonstrates that implementing multifaceted system-wide interventions improves hospital flow and ED boarding time. Additionally, our project demonstrates a significant correlation between improvements in ED boarding time, daily consultant-led rounds and early discharge from inpatient units and time till discharge.
Keywords: healthcare quality improvement, lean management, efficiency, organizational, hospital medicine
Problem
The purpose of this study was to evaluate the efforts of a group of hospitals that participated in a quality improvement collaborative that aimed at reducing emergency department (ED) Boarding time to less than 6 hours by the end of 2020.
The project was implemented at six tertiary care hospitals in Saudi Arabia under the General Directorate of Health Services, a governmental healthcare system that provides integrated healthcare services to the Ministry of Defence (MOD) employees and their dependents.
Hospitals included in the study were six governmental tertiary care hospitals with a cumulative bed capacity of 3736 beds across six cities, including Riyadh, Jeddah, Alhada, Khamis Mushait, Dharan and Tabuk. Table 1 describes the location and number of beds for the enrolled hospitals.
Table 1.
Details of hospitals enrolled in the project
| Hospital | City | Location | Ownership | No of beds |
| A | Riyadh | Urban | Governmental | 1341 |
| B | Jeddah | Urban | Governmental | 472 |
| C | Khamis Mushait | Urban | Governmental | 481 |
| D | Taif | Suburban | Governmental | 536 |
| E | Dhahran | Suburban | Governmental | 334 |
| F | Tabuk | Urban | Governmental | 572 |
The leadership of the General Directorate of Health Services have identified ED boarding time as a priority for measurement and improvement in early 2019, as part of the national vision realisation programme and MOD transformation programme.
An enterprise-wide improvement project was commissioned to improve hospital flow and reduce ED crowding. The improvement team designated the project as project ‘ENSIAB’ which in Arabic means ‘Flow’.
Background
ED boarding is defined as the time a patient remains in the ED after the patient has been admitted or placed into observation status at the facility but has not been transferred to an inpatient or observation unit.
ED boarding is associated with less efficient hospital flow, longer inpatient length of stay, higher readmission rates and increased risk of mortality and medical errors. In addition to being associated with poor patient and staff satisfaction.1–3
Studies looking into solutions to improve boarding time and capacity management in ED have addressed scheduling and patient throughput, but several studies considered electronic and technological solutions. All of these solutions can positively influence the quality of patient care, including satisfaction.4 A mixed-methods comparative case study that looked into the top and bottom 5% of Centers for Medicare & Medicaid Services for 2012 concluded that the presence of four organisational domains was associated with better hospital performance, which includes executive leadership involvement, hospital-wide coordinated strategies, data-driven management and performance accountability.5
One study demonstrated that implementing a discharge checklist and implementing an interdisciplinary huddle to act on the following day’s discharges significantly reduced time to discharge and ED boarding time.6 Another article reporting on patient flow changes before and after implementation of the daily huddle, as measured by paediatric ED boarding times, showed that ED boarding times were significantly shorter after huddle implementation compared with pre-huddle. These findings suggest huddles as one potential factor for improving patient flow from the ED by enhancing interprofessional and interdepartmental collaboration and communication.7
The UK National Health Service NHS improvement recommends the use of multifaceted interventions to improve hospital flow. These interventions were bundled and have been called ‘SAFER Patient Flow Bundle’. Key components of the bundle include daily senior review, documentation of clinical discharge criteria, documentation of the expected date of discharge, early admissions and discharges, and multidisciplinary team (MDT) review of patients with extended lengths of stay.8 Current evidence on the SAFER Patient Flow Bundle’s effectiveness is limited and is based on a couple of case studies.9
A study investigating the financial impact of improvement in ED boarding time concluded that reductions in ED boarding time results in significant financial cost savings from capturing left without being seen (LWBS) and diverted ambulance patients.10
Measurement
Our primary outcome measure was the average ED boarding time. This indicator measures the average duration of time in hours from admit decision to the time of the patient leaving ED to be admitted to inpatient status. Process measures included the following: daily consultant rounds, percentage of patients discharged before 12:00 hours, percentage of 7-day and 30-day outliers, early discharge planning, median time till discharge from inpatient setting (in minutes), average length of stay (ALOS) and bed turnover rate.
Our balancing measure included hospital readmission within 30 days, bed occupancy rate, ED mortality and ED patients who left ED without being seen (LWBS).
Online supplemental appendix 1 describes the operational definition of our selected measures. Table 2 details the results of our baseline measurement.
Table 2.
Results of pooled baseline results of enrolled hospitals
| Pooled data of six hospitals | Before intervention mean±SD | |
| Measure type | Measures | |
| Outcome | Boarding time* | 16.6±14.9 |
| Process | Daily consultant rounds | 69%±3% |
| Discharge before 12:00 hours | 16%±6% | |
| Time till discharge | 265±104 | |
| Early discharge planning | 66%±22% | |
| MDT review for 7 day outliers | 29%±3% | |
| Seven days outliers* | 16.3%±7.2% | |
| 30 days outliers* | 19%±10% | |
| Bed turn over* | 3.9±1.1 | |
| Average length of stay* | 6.5±2 | |
| Balancing | Readmission % within 30 days* | 5.16%±4.75% |
| Bed occupancy* | 76.9%±8.9% | |
| Percentage of ED patients that left without being seen LWBS* | 2%±1.4% | |
| No of ED deaths* | 2.4±2.1 | |
| Other | No of Admission* | 1699±584 |
| No of Discharge* | 1767±478 | |
| No of ED visits | 10589±4870 |
*Pooled ean of twelve-month period January–December 2018.
ED, emergency department; LWBS, left without being seen; MDT, multidisciplinary team.
bmjoq-2021-001505supp001.pdf (33.2KB, pdf)
Data were analysed using control charts/run charts and a before and after comparison of a calculated mean difference using t-test with a significance level of 0.05. For measures that historical data were available, a comparison was calculated for the 12 months preceding the intervention and the twelve months following the intervention. Multiple correlation analysis was conducted to investigate further the relationship between the outcome measure and other measures.
Design
Our interventions depended on the assumption that ED boarding time is interdependent on other hospital operations. Therefore, delays in the ED are a hospital-wide issue, not solely an ED operations issue.
Interventions included in the project were implementing the SAFER discharge bundle with RED 2 GREEN visual management system, implementing MDT huddles, and establishing multidisciplinary flow improvement teams. Table 3 provides a further description of the implemented interventions.
Table 3.
Details about project interventions
| Intervention | Description |
| SAFER patient flow bundle8 9 | Multifaceted interventions based on best practices that include daily senior review, documentation of clinical discharge criteria, documentation of the expected date of discharge, early admissions and discharges, and multidisciplinary team review of patients with extended lengths of stay. |
| Bed utilisation visual management and tracking system11 12 | A visual management system to that is based on the NHS RED and GREEN bed days. RED and GREEN is a visual management system to assist in the identification of wasted time in a patient’s journey and used during the board round. A patient shall be marked as RED if he receives little or no value-adding acute care. A patient shall be marked as GREEN when he receives value-adding acute care that promotes his progress towards discharge. Additionally, the system tracks the status of inpatient beds. Each unit has a board or screen that summarises the status of all patients admitted in that unit. |
| Emergency admission bed huddle7 | The emergency admission bed huddle is a planning tool for improving patient flow. A multidisciplinary team meets daily to discuss and act on admissions to the hospital from the emergency department and manage fluctuations in patient presentations by promptly allocating boarded patients to inpatient beds and authorising out of specialty admission. The huddle is led by a medical executive and includes representatives from the emergency department, critical care, inpatient units, nursing and bed management. |
| Hospital flow teams13 | A specialised team that is led by a hospital executive and includes physicians, nurses and bed managers. The team meets on a weekly basis and is responsible for maintaining patient flow and bed placement across hospital units, by monitoring hospital flow measures, elevating bottlenecks and supporting flow improvement activities. |
NHS, National Health Service.
Each hospital established flow improvement teams that included physicians, nurses, bed managers, clerks and quality coordinators. The improvement teams were led by the hospital’s chief quality officer and sponsored by the chief executive officer of the hospital. The improvement teams met weekly to review the interventions’ results and track progress on their action plans. Collaboration and learning between different hospitals were facilitated through collaborative learning sessions using the IHI’s Collaborative Model for Achieving Breakthrough Improvement.
The improvement team conducted stakeholder analysis to identify different stakeholders and manage their engagement in the project. Resistance to change was anticipated from two groups, physicians and admission office staff. This was mitigated by implementing a communication plan developed at an earlier phase to align medical staff and hospital executives regarding aim, long-term added value and the evidence beyond each intervention.
A unified system of measures was created and used throughout the hospitals, including all units and clinical services. This helped create an environment in which teams had a direct line of sight to the organisation’s overall efforts to improve flow.
Strategy
Each hospital established an improvement team that included physicians, nurses, bed managers and quality experts. In addition to establishing improvement teams, clinical leadership and hospital executives were aligned by establishing executive project oversight teams and a project steering team at the governance level to support and monitor team progress.
Improvement teams used the IHI’s model for improvement as a tool for testing and implementing changes. Collaboration and learning between different hospitals were facilitated by conducting collaborative learning sessions using the IHI’s Collaborative Model for Achieving Breakthrough Improvement. In between these learning sessions, teams were required to provide progress reports every 6 weeks. During learning sessions, team members learn from one another as they report on successes, barriers and lessons learnt in general sessions, workshops, storyboard presentations and informal dialogue and exchange.
The improvement teams underwent four learning sessions and an additional four action periods. Each hospital implemented and presented at least three improvement cycles. Table 4 summarises strategies for change in each cycle and lessons learnt.
Table 4.
Summary of strategies for change and lessons learnt during the learning sessions
| Cycle no | Strategy for change | Key learning from the cycle |
| First learning session |
|
|
| Second learning session |
|
|
| Third learning session |
|
|
ED, emergency department.
Results
The number of admissions and discharges increased in all hospitals during the study period by an average increase of 16% admissions and 19% discharges and decreased admission/discharge ratio by 0.03 (0.96 before, 0.93 after). Additionally, ED visits showed a significant increase by 14.6% after the intervention p=0.02.
Outcome measure
All hospitals significantly reduced ED boarding time with a pooled mean difference of – 7.1 hours (16.6 before, 9 hours after p<0.001)), reaching a pooled average of 2 hours in march 2020.
Control charts for all enrolled hospitals showed new performance levels after implementation with significant variability reduction (figure 1). furthermore, by the end of the third learning session, all hospitals were able to achieve a boarding time below 6 hours.
Figure 1.

Control charts for ED boarding time for each enrolled hospital. ED, emergency department; LS, learning session.
Regression analysis showed a statistically significant negative correlation between ED boarding time and the following interventions: time till discharge, daily consultant rounds, and discharge before 12:00 hours. On the other hand, there was a positive correlation between ED boarding and 30-day outliers, 7 day outliers and bed occupancy rate (figure 2).
Figure 2.
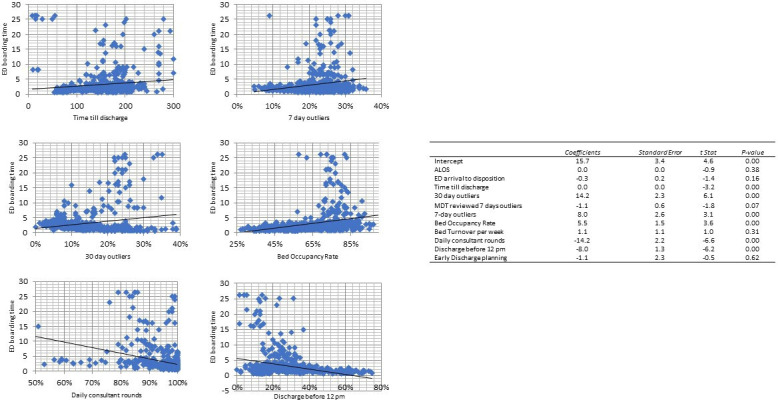
Regression analysis between ED boarding and project interventions. ALOS, average length of stay; ED, emergency department; MDT, multidisciplinary team.
Process measures
Daily consultant rounds improved from 69% at baseline to 98% after the intervention with a mean difference of 29% (95% CI −5% to 60%), p=0.053. The percentage of patients discharged before 12:00 hours improved from 16% at baseline to 36% after intervention with a mean difference of 20% (95% CI 6% to 35%). p=0.01. Time till discharge in minutes improved from 265 min at baseline to 117 min after the intervention, mean difference −147 min (95% CI −250 to −44), p=0.009. The percentage of admitted patients with a documented early discharge plan improved from 66% at baseline to 95% after the intervention with a mean difference of 29% (95% CI 8% to 50%), p=0.01. (figure 3 shows run charts for compliance to SAFER patient flow bundle).
Figure 3.

Run charts for compliance to SAFER patient flow bundle.
The percentage of 7-day outliers showed a non-significant increase after the intervention by a mean difference of 0.9% (before 16.3%, after 17.2% p value 0.5). 30-day outliers also demonstrated a non-significant decreased by −3% (before 19%, 16% after p=0.15).
A subgroup analysis of hospitals with a higher percentage of 30-day outliers at baseline (>10%) had statistically significant improvement in the percent of 30-day outliers by a mean difference of −4.2%, p=value 0.005.
Pooled ALOS was 6.5 days at baseline and showed a non-statistically significant increase with a mean difference of 0.32 (−0.32, 0.96), p=0.325. Subgroup analysis showed that three hospitals (B, C, F) demonstrated significant reductions in ALSO by an average of 0.4 days, while having lower percentage of 30-day outliers when compared with hospitals that did not have reduction in length of stay (16%, 20% mean difference 6%, p=0.002). Furthermore, regression analysis showed that ALOS is significantly associated with 30-day outlier, daily consultant rounds and bed occupancy rates (figure 4).
Figure 4.
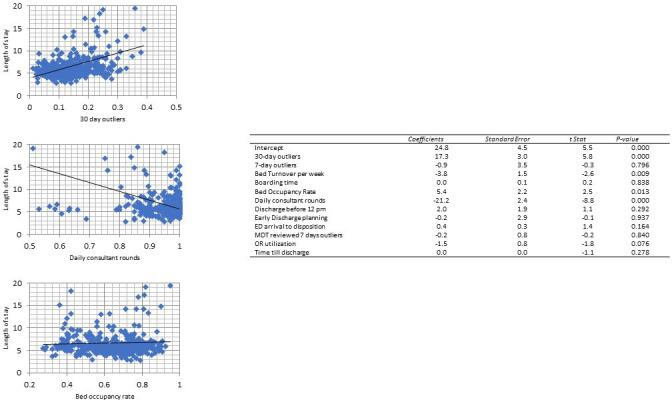
Regression analysis for average length of stay. ED, emergency department; MDT, multidisciplinary team.
Bed turnover rate showed a statistically insignificant increase after the intervention by an average of 0.32 (95% CI −0.1 to 0.7), p=0.13, with hospitals B and D showing a significant increase in bed turnover rates.
Balancing measures
Hospital readmission within 30 days did not change after the intervention (5.2% before and 5.6% after) with a mean difference of 0.5% (−1.07 2.02), p=0.5.
Bed occupancy rates did not change before and after the intervention with a 1% mean difference (77% before, 76% after), p=0.5.
ED mortality was not affected across all hospitals with a mean difference of −0.1 (before 2.39, after 2.3), p=0.8.
The percentage of ED patients LWBS did not change after the intervention, with a mean difference of −0.3 (95% CI −0.8% to 0.28%), p=0.28.
Correlation analysis revealed that hospital readmission within 30 days was positively correlating with ED boarding time, percentage of 30-day outliers and the number of ED patients who LWBS. Table 5 details results of before and after hospital results and calculated mean difference.
Table 5.
Pooled before and after results of all enrolled hospitals
| Pooled data of six hospitals | Before intervention mean±SD | After intervention mean±SD | Mean difference (95% CI) | P value | |
| Measure type | Measures | ||||
| Outcome | Boarding time | 16.6±14.9 | 9.5±12.9 | −7.1 (−2.5 to 11.7) | 0.003 |
| Process | Daily consultant rounds | 69%± 30% | 98%±3% | 29% (-0.5% to 60%) | 0.053 |
| Discharge before 12:00 pm | 16%±6% | 36%±14% | 20% (6% to 35%) | 0.01 | |
| Time till discharge | 265±104 | 117±43 | −147.8 (−250 to 44) | 0.0095 | |
| Early discharge planning | 66%±22% | 95%±5.9% | 29% (8% to 50%) | 0.011 | |
| MDT review for 7 day outliers | 29%±3% | 86%±14% | 51% (25% to 89%) | 0.002 | |
| 7 days outliers | 16.3%±7.1% | 17.2%±7.5% | 0.89% (−1.9% to 3.7%) | 0.531 | |
| 30 days outliers | 18.8%±9.9% | 15.9%±10.3% | −2.9% (−6.8% to 1.0%) | 0.149 | |
| Bed turn over | 3.9±1.1 | 4.3±1.6 | 0.32 (−0.09 to 0.73) | 0.125 | |
| Average length of stay | 6.5±2.00 | 6.8±2.00 | 0.32 (−0.32 to 0.96) | 0.325 | |
| Balancing | Readmission % within 30 days | 5.2%±4.8% | 5.6%±4.9% | 0.5% (−1.1% to 2.0%) | 0.543 |
| Bed occupancy | 76.9%±8.9% | 76.0%±7.0% | −0.9 (−3.6 to 1.7) | 0.49 | |
| Percentage of ED LWBS | 1.8%±1.5% | 1.5%±0.8% | −0.3% (−0.8% to 0.2%) | 0.208 | |
| No of ED deaths | 2.4±2.1 | 2.3±2.1 | −0.10 (−0.78 to 0.57) | 0.763 | |
| Other | Admission | 1699±584 | 1977±567 | 277 (92to 462) | 0.004 |
| Discharge | 1767±478 | 2111±444 | 343 (196 to 491) | <0.001 | |
| No of ED visits | 10 589±4870 | 12 100±3396 | 1511(222 to 2800) | 0.022 |
ED, emergency department; LWBS, left without being seen.
Lessons and limitations
The project aim was to improve hospital flow by reducing emergency boarding time to less than 6 hours by implementing a multifaceted change package.
Establishing hospital flow teams and implementing the SAFER bundle resulted in initial improvements in ED boarding time but hospital teams faced difficulties in implementing MDT reviews for 7-day outliers due to unclear roles and responsibilities. The improvement team developed standard operating procedures for MDT review, which improved and standerdized team activities. Furthermore, the ED bed huddle process was not clear to the teams conducting the huddles, which led the improvement team to develop a written guideline to clarify and standardise huddle activities. This resulted in further improvements in boarding time at the second learning session. Hospital teams faced difficulty at the start of the project in discharging long-stay patients exceeding 30 days. The main reason was reluctance from main responsible physicians to discharge such patients due to multiple factors related to the support and resources at the community level. The improvement team developed a process that used lean methodology to establish a pull system that relied on standing orders to assess long-term patients by an MDT regarding the need and feasibility of patient transition to community-based care.
When analysing the association between the project interventions and ED boarding time, we found that daily consultant rounds, discharge before 12:00 pm, and reductions in 7 and 30 days outliers seem to significantly correlate with ED boarding time.
One of the projects’ significant strengths is the implementation across multiple hospitals with a large sample size and high level of engagement from hospital teams and leadership.
In terms of limitations, fidelity to the change package was an issue half-way through the project, which required the improvement team to establish a compliance audit tool and conduct site audits and further training for the hospital teams. Additionally, the study’s design was quasi-experimental before and after, and all hospitals used a sequential implementation method of roll-out that might have diluted the effects of the interventions. The improvement team tried to adjust for this during the data analysis phase.
In terms of data validity, the improvement team used a multilayered approach that used data abstraction and correlation of measures with related measures reported to the governing body.
Although the change package resulted in significant ED boarding time improvements, ALOS did not demonstrate significant improvement in the 12 months after implementation. An explanation may be attributed to the fact that length of stay is known to be highly skewed and causally related to the number of bed days of discharged patients. Therefore, if patients with extended length of stay (stranded patients) are discharged more frequently, ALOS will increase in the short and intermediate term. This theory is reinforced by the observed correlation between 30-day outlier and length of stay. Additionally, hospitals that did not demonstrate reductions in ALOS had significant higher rate of 30-day outliers despite an observed increase in the number of discharges and bed turnover.
Although the percentage of 30-day outliers decreased in some hospitals, 7-day outliers did not change in almost all hospitals throughout the study period despite attempts at standardising the MDT review process. For this to be enhanced further, a future project should investigate different methods of conducting the MDT review and measure the ALOS for more extended periods.
Our project demonstrates that implementing multifaceted system-wide intervention improves hospital flow and ED boarding time. Additionally, our project demonstrates a significant correlation between daily consultant-led rounds and improvements in ED boarding time.
All the six enrolled hospitals were able to significantly reduce ED boarding time to less than 6 hours by the end of the project and demonstrate sustained improvements in ED boarding time beyond the third learning session. Compliance to process measures was acceptable, while most hospitals did not see significant reductions in 7-day outliers and ALOS. This can be explained by an increased discharge of long-term patients and increased bed turnover rate. The balancing measures did not exhibit any undesired trends.
To further ensure that the results continue to be sustainable, the improvement team has integrated the SAFER flow bundle components and the ED bed huddle as part of the organisation policy and procedure. Besides, a hospital flow unit has been established to ensure that monitoring and improving patient flow is part of the routine activities and to ensure sustainability.
Impact of COVID-19 pandemic
Due to the ongoing COVID-19 pandemic, lockdowns and surge plans have impacted the number of available hospital beds, hospital admissions and bed turnover. During the height of the lockdowns in April 2020, ED boarding time continued to decrease, reaching less than 2 hours for the majority of 2020 with no hospital reporting ED-related COVID-19 outbreaks or closures.
On the other hand, bed occupancy rates dropped significantly in March 2020, with an initial decrease in bed turnover rate. Subsequently, by the end of 2020, hospitals achieved prepandemic bed turnover rates despite having a lower number of available hospital beds.
The project has helped participating hospitals maintain efficient patient flow and enhance bed utilisation during the pandemic (figures 5 and 6).
Figure 5.
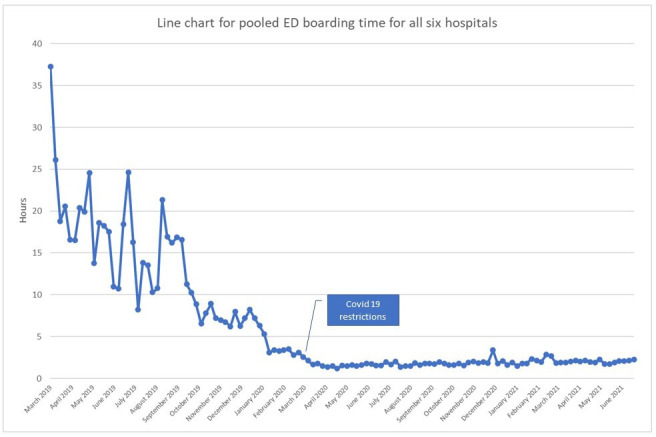
Line chart for pooled ED boarding time for all six hospitals. ED, emergency department.
Figure 6.
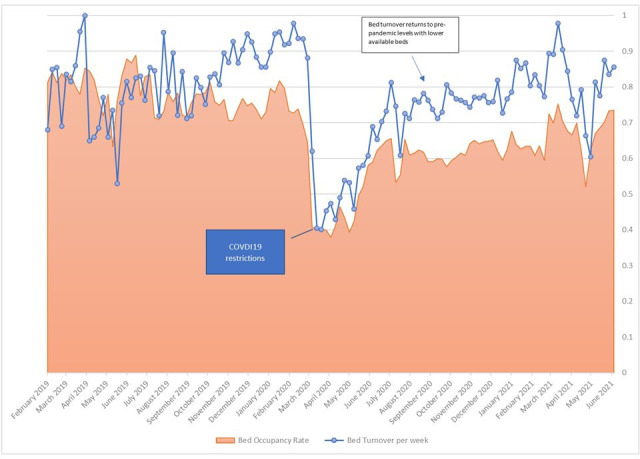
Combo chart for pooled bed occupancy rate and bed turn over rate before and after COVID-19 pandemic.
Conclusion
Due to significant improvements in our project, other hospitals within the MOD healthcare system have started to implement elements of the interventions. Further work is underway by the improvement team to build capacity in managing hospital flow by developing and conducting educational activities for healthcare workers and executive leadership. Moreover, further research is required to identify more effective strategies to reduce the percentage of 7-day outliers.
Footnotes
Correction notice: This article has been corrected since it first published. The author name 'Ahmed Alamry' has been updated.
Contributors: YA: project team leader, conducted and reported the work. NA: planning, reporting of the paper. AA: planning and review or the paper.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Ethics statements
Patient consent for publication
Not required.
References
- 1.American College of Emergency Physicians . Definition of Boarded patient. Policy statement, 2018. Available: https://www.acep.org/globalassets/new-pdfs/policy-statements/definition-of-boarded-patient.pdf
- 2.Singer AJ, Thode HC, Viccellio P, et al. The association between length of emergency department boarding and mortality. Acad Emerg Med 2011;18:1324–9. 10.1111/j.1553-2712.2011.01236.x [DOI] [PubMed] [Google Scholar]
- 3.Morley C, Unwin M, Peterson GM, et al. Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS One 2018;13:e0203316. 10.1371/journal.pone.0203316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.McCaughey D, Erwin CO, DelliFraine JL. Improving capacity management in the emergency department: a review of the literature, 2000-2012. J Healthc Manag 2015;60:63–75. 10.1097/00115514-201501000-00011 [DOI] [PubMed] [Google Scholar]
- 5.Chang AM, Cohen DJ, Lin A, et al. Hospital strategies for reducing emergency department crowding: a mixed-methods study. Ann Emerg Med 2018;71:497–505. 10.1016/j.annemergmed.2017.07.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Beck MJ, Okerblom D, Kumar A, et al. Lean intervention improves patient discharge times, improves emergency department throughput and reduces congestion. Hosp Pract 2016;44:252–9. 10.1080/21548331.2016.1254559 [DOI] [PubMed] [Google Scholar]
- 7.McBeth CL, Durbin-Johnson B, Siegel EO. Interprofessional huddle: One children’s hospital’s approach to improving patient flow. Pediatr Nurs 2017;43:71–6. [PubMed] [Google Scholar]
- 8.NHS Improvment . SAFER patient flow bundle, 2021. Available: https://improvement.nhs.uk/resources/safer-patient-flow-bundle-implement/
- 9.Irvine S, Awan M, Chharawala F, et al. Factors affecting patient flow in a neurosurgery department. Ann R Coll Surg Engl 2020;102:18–24. 10.1308/rcsann.2019.0090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pines JM, Batt RJ, Hilton JA, et al. The financial consequences of lost demand and reducing boarding in hospital emergency departments. Ann Emerg Med 2011;58:331–40. 10.1016/j.annemergmed.2011.03.004 [DOI] [PubMed] [Google Scholar]
- 11.Patel PB, Combs MA, Vinson DR. Reduction of admit wait times: the effect of a leadership-based program. Acad Emerg Med 2014. [DOI] [PubMed] [Google Scholar]
- 12.Meo N, Paul E, Wilson C, et al. Introducing an electronic tracking tool into daily multidisciplinary discharge rounds on a medicine service: a quality improvement project to reduce length of stay. BMJ Open Qual 2018;7:e000174. 10.1136/bmjoq-2017-000174 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Winasti W, Elkhuizen S, Berrevoets L, et al. Inpatient flow management: a systematic review. Int J Health Care Qual Assur 2018;31:718–34. 10.1108/IJHCQA-03-2017-0054 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjoq-2021-001505supp001.pdf (33.2KB, pdf)