

Abstract
Background
For years, paediatric critical care practitioners used the adult American European Consensus Conference (AECC) and revised Berlin Definition (BD) for acute respiratory distress syndrome (ARDS) to study the epidemiology of paediatric ARDS (PARDS). In 2015, the paediatric specific definition, Paediatric Acute Lung Injury Consensus Conference (PALICC) was developed. The use of non-invasive metrics of oxygenation to stratify disease severity were introduced in this definition, although this potentially may lead to a confounding effect of disease severity since it is more common to place indwelling arterial lines in sicker patients. We tested the hypothesis that PALICC outperforms AECC/BD in our high acuity PICU, which employs a liberal use of indwelling arterial lines and high-frequency oscillatory ventilation (HFOV).
Methods
We retrospectively collected data from children < 18 years mechanically ventilated for at least 24 h in our tertiary care, university-affiliated paediatric intensive care unit. The primary endpoint was the difference in the number of PARDS cases between AECC/BD and PALICC. Secondary endpoints included mortality and ventilator free days. Performance was assessed by the area under the receiver operating characteristics curve (AUC-ROC).
Results
Data from 909 out of 2433 patients was eligible for analysis. AECC/BD identified 35 (1.4%) patients (mortality 25.7%), whereas PALICC identified 135 (5.5%) patients (mortality 14.1%). All but two patients meeting AECC/Berlin criteria were also identified by PALICC. Almost half of the cohort (45.2%) had mild, 33.3% moderate and 21.5% severe PALICC PARDS at onset. Highest mortality rates were seen in patients with AECC acute lung injury (ALI)/mild Berlin and severe PALICC PARDS. The AUC-ROC for Berlin was the highest 24 h (0.392 [0.124–0.659]) after onset. PALICC showed the highest AUC-ROC at the same moment however higher than Berlin (0.531 [0.345–0.716]). Mortality rates were significantly increased in patients with bilateral consolidations (9.3% unilateral vs 26.3% bilateral, p = 0.025).
Conclusions
PALICC identified more new cases PARDS than the AECC/Berlin definition. However, both PALICC and Berlin performed poorly in terms of mortality risk stratification. The presence of bilateral consolidations was associated with a higher mortality rate. Our findings may be considered in future modifications of the PALICC criteria.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12931-021-01848-z.
Keywords: Acute respiratory distress syndrome, Paediatric acute lung injury consensus conference, American–European consensus conference, Berlin definition, PICU, Mortality, Predictive value, Mechanical ventilation, Paediatric
Background
For long, paediatric critical care practitioners have adopted the American European Consensus Conference (AECC) definition of acute respiratory distress syndrome (ARDS) established in 1994 and its 2012 revised definition, the Berlin definition, to describe and study the epidemiology of ARDS in children [1–3]. Using this adult-based definition, the incidence of paediatric ARDS (PARDS) varies between 2 and 10 cases per 100,000 per year [4–11]. Despite this apparent low incidence, PARDS is associated with significant but at the same time variable mortality rates. Different observational and epidemiological studies of children with PARDS indicate mortality rates of 15–75% [12]. Although PARDS may differ from ARDS in adults in terms of epidemiology and triggering factors, the major limitation of both the AECC and Berlin definition is the use of invasive metrics of oxygenation (i.e., the PaO2/FiO2 ratio). Use of indwelling arterial lines is not common in children, especially in less severe disease, increasing the likelihood of underestimating the true prevalence of PARDS [5, 13].
In 2015, the Paediatric Acute Lung Injury Consensus Conference (PALICC) definition of PARDS was published, addressing the issues related to the differences between children and adults [14]. PALICC definition mirrors the Berlin definition except for two criteria. First, instead of the PaO2/FiO2 (PF) ratio, PALICC makes use of the oxygenation index (OI) or the oxygenation saturation index (OSI) when indwelling arterial lines are absent as oxygenation metrics for severity stratification in intubated patients. Second, PALICC does not require the presence of bilateral consolidations on chest radiograph. The AECC definition differs also in severity stratification and only distinguishes two severity levels, where the Berlin definition and PALICC distinguish three severities.
Better performance of PALICC over the adult-based definitions was demonstrated in a prospective, observational cross-sectional study in 145 international paediatric intensive care units (PICU) [15]. In this study, applying the PALICC definition identified more patients with high mortality risk than the Berlin definition and appeared to adequately stratify mortality risk when applied 6 h after PARDS diagnosis. However, less than half of the study population had invasive metrics of oxygenation upon PARDS diagnosis making it difficult to understand the confounding effect of disease severity as it is probably more common to put indwelling arterial lines in sicker patients. Therefore, we sought to explore the performance of PALICC compared with the Berlin definition in our high acuity PICU with a liberal use of indwelling arterial lines in invasively ventilated patients and use of high-frequency oscillatory ventilation (HFOV) by comparing the number of PARDS cases identified by both definitions. Secondary objectives included the difference between PALICC, Berlin and AECC definition in terms of mortality discrimination and PARDS severity trajectory during the first 48 h.
Methods
We retrospectively collected data from all children > 7 days (for cardiac patients, they can be admitted from birth) to < 18 years admitted to the PICU of the Beatrix Children’s Hospital between January 2014 and December 2016 who required invasive mechanical ventilation (MV) > 24 h. Patients with chronic lung disease were included if they met standard diagnostic criteria and had an acute deterioration in oxygenation from their baseline. Patients with uncorrected cyanotic heart disease, home ventilation and those on extra-corporeal life support (ECLS) were not studied. The Institutional Review Board waived the need for informed consent.
Screening of patients
Data was extracted from the patient’s paper and electronic health records. First, two reviewers (MR and JvD) evaluated chest radiographs for the presence of unilateral or bilateral consolidations in the period 24 h before admission to the PICU and the first 8 days of admission (see Additional file 1). If deemed present, an independent senior paediatric critical care physician (RB or MK) confirmed or refuted the presence of consolidations. When patients met the radiographic criteria for ARDS, we screened for hypoxaemia (i.e. PF < 300 or OI ≥ 4 (or OSI > 5 when OI was unavailable)) within 24 h of the chest radiograph [5]. Echocardiograms were not routinely performed in our unit, hence we assumed that left ventricular (LV) dysfunction was not present unless clinically documented and confirmed by echocardiography.
Definitions for PARDS
We applied published AECC and Berlin definitions [2, 3]. Briefly, criteria for meeting the AECC definition included (a) identification of known trigger, (b) bilateral consolidations on the chest radiograph, (c) absence of LV dysfunction and (d) PF < 300. For the Berlin definition, patients had to meet the same criteria at a minimal PEEP of 5 cm H2O and mild LV dysfunction were included. For both definitions, initial PARDS severity was classified by the PF ratio closest to the confirmatory chest radiograph. The closest PF ratio 24 and 48 h ± 6 h after the initial ratio was used to classify the 24 and 48 h PARDS severity. Using the Berlin definition, PARDS severity was defined as mild (200 < PF ≤ 300 mmHg), moderate (100 < PF ≤ 200 mmHg) and severe (PF ≤ 100 mmHg). The AECC definition discriminated acute lung injury (ALI) (200 < PF ≤ 300 mmHg) and ARDS (PF ≤ 200 mmHg).
Patients met PALICC criteria when (a) a trigger was identified, (b) there were ≥ 1 consolidations on chest radiograph, (c) LV dysfunction was ruled out and (d) OI ≥ 4 or OSI ≥ 5 when no PaO2 was available. Initial PARDS severity was classified by OI ≥ 4 or OSI ≥ 5 closest to the confirmatory chest radiograph. The closest OI or OSI 24 and 48 h ± 6 h after the initial ratio was used to classify the 24 and 48-h PARDS severity. PARDS severity was stratified as mild (4 ≤ OI < 8 or 5 ≤ OSI < 7.5), moderate (8 ≤ OI < 16 or 7.5 ≤ OSI < 12.3) and severe (OI ≥ 16 or OSI ≥ 12.3).
Additional data collection
For each patient, we collected demographical and clinical data including age, gender, admission diagnosis, duration of MV, MV mode, length of PICU stay and survival status. Ventilator free days (VFD) was calculated by subtracting MV duration of 28 and deceased patients were assigned with 0 VFD [16]. MV mode was stratified in three categories; HFOV for 48 h, combination of HFOV and conventional mechanical ventilation (CMV) during the first 48 h, CMV for 48 h. Disease severity was assessed using the 24-h Paediatric Risk of Mortality (PRISM) III score as proxy [17]. Although there was no clinical algorithm dictating its use, indwelling catheters are routinely inserted and arterial blood gasses (ABGs) are done at least 4 times a day early in the disease trajectory. The continuous distending pressure (CDP) was used instead of the mean airway pressure (mPaw) when patients were on the oscillator.
Study endpoints
The primary endpoint was the difference in the number of PARDS cases between AECC, Berlin and PALICC. Secondary endpoints were the difference in mortality rates, MV duration, PICU length of stay and ventilator free days (VFD).
Statistical analysis
For continuous patient characteristics and outcome data, descriptive statistics were used where mean (± SD) was used for normally distributed data, which was assessed by the Kolmogorov–Smirnov test, and median (IQR) were used for non-normal distributed data. Mortality rates as a function of PARDS severity, MV mode and chest consolidations were tested using the χ2 or Fisher’s Exact test. Receiver operating characteristics curves (ROC) were constructed to evaluate the mortality discrimination by calculating the area under the curve (AUC) with 95% confidence intervals (CI). Kruskal Wallis tests were used to test differences in length of MV, VFD and PICU stay between PARDS severity strata and MV mode. Mann–Whitney U tests were used to test the differences in length of MV, VFD and PICU stay between unilateral and bilateral consolidations. p values < 0.05 were accepted as statistically significant. All statistical analyses were performed with SPSS 24 (IBM, Chicago, Ill, USA).
Results
A total of 2.433 patients (mortality 3.7%) were admitted to the PICU during the study period, of whom N = 1.068 (43.9%) were ventilated > 24 h (Fig. 1). Of those, N = 154 patients met the exclusion criteria and five had missing data, yielding data from N = 909 patients available for analysis. There were no cases with mild LV dysfunction which made the identification by the Berlin definition equal to the AECC definition which identified N = 35 patients (1.4% of all PICU admissions and 3.3% of those ventilated > 24 h) with a mortality of 25.7% (Fig. 2). All but two patients meeting AECC/Berlin criteria were also identified by PALICC. One-hundred-and-thirty-five patients (5.5% of all PICU admissions and 12.6% of those ventilated > 24 h) met PALICC criteria, of whom N = 102 were not identified by AECC/Berlin. Ninety-five percent of those had invasive metrics for oxygenation available. The mortality rate was 14.1%. Patient characteristics, admission diagnosis and outcomes were well-balanced between the AECC/Berlin and PALICC PARDS definition (Table 1).
Fig. 1.

Flow diagram of the study population
Fig. 2.
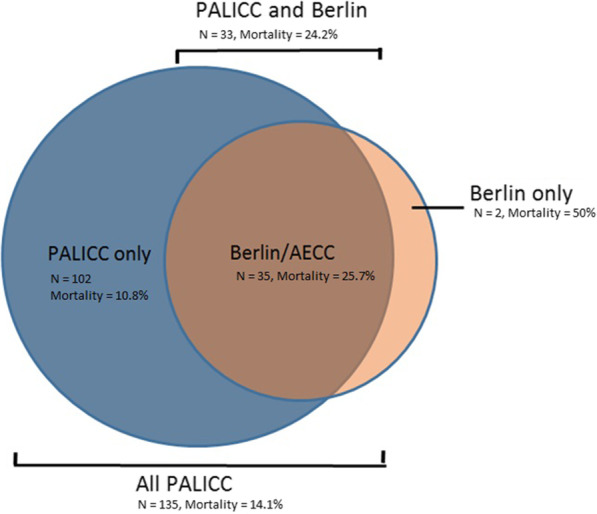
Distribution of subjects meeting ARDS criteria stratified by ARDS definition. The blue area represents 102 subjects only meeting PALICC criteria, the dark orange area represents 33 subjects meeting PALICC and Berlin/AECC criteria. The orange area represents the two subjects only meeting Berlin/AECC criteria
Table 1.
Patient characteristics of cohorts meeting ARDS criteria
| PALICC | Berlin/AECC | p value | |
|---|---|---|---|
| N | 135 | 35 | |
| Male gender, % | 59.3 | 60 | 0.937 |
| Age, median in days (IQR) | 380 (61;1917) | 770 (137;2310) | 0.179 |
| PRISM-II, median (IQR) | 14 (10;19) | 14 (12;23) | 0.378 |
| PRISM-III, median (IQR) | 4 (1;8) | 5 (1;8) | 0.811 |
| PIM, median (IQR) | − 2.505 (− 3.249;− 1.940) | − 2.380 (− 2.660;− 1.530) | 0.064 |
| PIM-II, median (IQR) | − 3.537 (− 4.382;− 2.487) | − 2.879 (− 4.210;− 1.587) | 0.052 |
| Mortality, % | 14.1 | 25.7 | 0.098 |
| Receiving HFOV at onset, n (%) | 18 (13.3) | 4 (11.4) | 0.765 |
| Timing | |||
| Between chest radiographs and meeting criteria, median in minutes (IQR) | 47 (28.5;143) | 39.5 (20.5;111.75) | 0.366 |
| Intubation cause | |||
| Pneumonia, n (%) | 78 (58) | 18 (51) | 0.409 |
| Sepsis, n (%) | 14 (10) | 6 (17) | |
| Post resuscitation, n (%) | 11 (8) | 5 (14) | |
| Post cardiac surgery, n (%) | 9 (7) | 0 (0) | |
| High energetic trauma, n (%) | 4 (3) | 0 (0) | |
| Status epilepticus, n (%) | 2 (1) | 1 (3) | |
| Liver failure/transplantation, n (%) | 1 (< 1) | 1 (3) | |
| Others, n (%) | 16 (12) | 4 (11) | |
No significant differences were found between the cohort meeting PALICC criteria and the cohort meeting Berlin/AECC criteria
Figure 3A graphically summarizes PARDS severity at onset. Almost half of the cohort (45.2%) had mild, 33.3% moderate and 21.5% severe PALICC PARDS at onset. AECC/Berlin identified 19.7% of patients with PALICC mild PARDS (Fig. 3A). For patients with moderate PALICC PARDS this was 22.2% and for severe PALICC PARDS 37.9%. Reasons for not identifying patients with PARDS included absence of bilateral consolidations (83.6% mild, 97.1% moderate, 94.4% severe) or invasive metrics of oxygenation (2% mild, 2.9% moderate, 0% severe) (Fig. 3B).
Fig. 3.

A Differences in severity stratification between PALICC and Berlin definition. Most of the 61 subjects meeting PALICC criteria for mild PARDS did not meet Berlin/AECC criteria, 6 also met criteria of mild ARDS by Berlin and ALI byAECC and 6 met criteria of moderate ARDS by Berlin and ARDS by AECC. Of the 45 subjects meeting PALICC criteria for moderate PARDS by PALICC only 6 subject met criteria for moderate ARDS by Berlin and 4 subjects met criteria for severe ARDS by the Berlin definition. Of the 29 subjects meeting PALICC criteria for severe PARDS 8 also met criteria for severe ARDS by the Berlin definition and 3 met Berlin criteria for moderate ARDS. B Reasons PALICC PARDS subjects are not identified as ARDS by Berlin/AECC. 49 subjects with mild PARDS by PALICC were not identified by Berlin/AECC, mainly due to lack of bilateral consolidations (dark blue). For the 35 subjects that were not identified by Berlin/AECC with moderate PARDS and the 18 subjects with severe PARDS a same pattern was seen
Table 2 summarizes Berlin and PALICC PARDS severity strata assessed at onset, 24 and 48 h later. There was no direct relationship with mortality for both definitions. Highest mortality rates were seen in patients with mild AECC/Berlin and severe PALICC PARDS. The AUC-ROC for AECC/Berlin was the highest at onset (0.391 [0.176–0.606] and 24 h (0.392 [0.124–0.659]). PALICC showed a higher AUC-ROC and was also the highest 24 h after onset (0.531(0.345–0.716)). There was no difference in duration of MV or length of PICU stay among patients meeting only Berlin criteria (Table 3). Similar observations were made for PALICC PARDS at onset. However, 24 h after onset MV duration, PICU length of stay and VFD differed significantly and 48 h after onset a similar difference was seen for the MV duration and VFD.
Table 2.
Performance of the Berlin and PALICC definition on predicting mortality
| Berlin | PALICC | |||||
|---|---|---|---|---|---|---|
| Mild | Moderate | Severe | Mild | Moderate | Severe | |
| Onset | ||||||
| Number of patients | 8 | 15 | 12 | 61 | 45 | 29 |
| PICU mortality | 37.5 | 26.7 | 16.7 | 14.8 | 8.9 | 20.7 |
| AUC-ROC | 0.391 (0.176–0.606) | 0.522 (0.371–0.673) | ||||
| p-value | 0.336 | 0.757 | ||||
| At 24 h | ||||||
| Number of patients | 5 | 20 | 1 | 45 | 34 | 26 |
| PICU mortality | 40.0 | 20.0 | 0 | 13.3 | 5.9 | 19.2 |
| AUC-ROC | 0.392 (0.124–0.659) | 0.531 (0.345–0.716) | ||||
| p-value | 0.429 | 0.723 | ||||
| At 48 h | ||||||
| Number of patients | 13 | 9 | 4 | 36 | 34 | 20 |
| PICU mortality | 38.5 | 11.1 | 0 | 8.3 | 11.8 | 10.0 |
| AUC-ROC | 0.267 (0.060–0.473) | 0.529 (0.336–0.722) | ||||
| p-value | 0.088 | 0.778 | ||||
At onset the Berlin stratification had an AUC-ROC of 0.391 (0.176–0.606), 24 h after onset it was 0.392 (0.124–0.659) and 48 h after onset it was 0.267 (0.060–0.473). On the right the PALICC definition is represented and shows an AUC-ROC of 0.522 (0.371–0.673) for mortality at onset, 0.531 (0.345–0.716) 24 h after onset and 0.529 (0.336–0.722) 48 h after onset
Table 3.
Performance of the Berlin and PALICC definition on predicting MV duration, PICU length of stay and VFD
| Berlin | PALICC | |||||||
|---|---|---|---|---|---|---|---|---|
| Mild | Moderate | Severe | p value | Mild | Moderate | Severe | p value | |
| Onset | ||||||||
| Number of patients | 8 | 15 | 12 | 61 | 45 | 29 | ||
| Duration of MV | 7.5 (3.75;12) | 9 (5;13) | 10.5 (7.25;14.75) | 0.454 | 8 (4.5;13) | 8 (5;12) | 10 (5.5;13) | 0.663 |
| PICU length of stay | 8.5 (3;16.25) | 10 (5;13) | 11.5 (8.25;19.75) | 0.289 | 8 (4;17.5) | 8 (7;14) | 10 (5.5;14) | 0.696 |
| VFD | 17 (0;21.25) | 19 (0;21) | 15.5 (2.5;20.75) | 0.906 | 19 (7;23) | 20 (15.5;22.5) | 17 (9;20) | 0.102 |
| At 24 h | ||||||||
| Number of patients | 5 | 20 | 1 | 45 | 34 | 26 | ||
| Duration of MV | 6 (3.5;10) | 10 (8;17.25) | 14 | 0.060 | 7 (5;10) | 9.5 (6.75;15) | 11 (8;14.25) | 0.000* |
| PICU length of stay | 10 (3.5;11.5) | 10.5 (9;21.5) | 14 | 0.320 | 7 (5;11) | 10.5 (7.75;19.25) | 11.5 (8.75;16.5) | 0.002* |
| VFD | 21 (0;24.5) | 17.5 (0;20) | 14 | 0.650 | 20 (16;23) | 18.5 (12.75;21.25) | 16 (3;19.25) | 0.006* |
| At 48 h | ||||||||
| Number of patients | 13 | 9 | 4 | 36 | 34 | 20 | ||
| Duration of MV | 9 (6;20) | 12 (7.5;16.5) | 9.5 (9;10.75) | 0.751 | 8 (5.25;10.75) | 10.5 (7;15) | 11 (8.25;15.75) | 0.008* |
| PICU length of stay | 10 (8;22) | 15 (9;21) | 10 (9.25;10.75) | 0.492 | 8.5 (7;14) | 10.5 (7.75;19.25) | 11.5 (9.25;20.25) | 0.118 |
| VFD | 15 (0;21.5) | 14 (5;20.5) | 18.5 (17.25;19) | 0.897 | 20 (16.25;22.75) | 8 (17;21) | 17 (12.25;19.75) | 0.027* |
On the left the Berlin/AECC definition is presented, on the right the PALICC criteria. Significant differences were found in MV duration and VFD when stratified by PALICC 24 h and 48 h after onset and in admission duration when stratified by PALICC 24 h after onset. Kruskal–Wallis test was used, α = 0.05
*Indicates significant differences
Ninety-seven patients (71.9%) with PALICC PARDS had unilateral chest radiograph consolidations. Unilateral consolidations was associated with a lower mortality compared to bilateral consolidations (9.3% vs. 26.3%. p = 0.025) (Table 4). A similar difference was found for the VFD (20 [IQR 14.5–23] vs 16.5 [IQR 0–21], p = 0.019) and PICU length of stay stay (8 days ([QR 5–13] vs 10 days [IQR: 7.75–19.25], p = 0.03). Duration of MV (8 days [IQR 5–11.5] vs 9 days [IQR: 6.75–14.25]) did not differ significantly (p = 0.054).
Table 4.
Differences in outcome measures for unilateral vs bilateral consolidations in PALICC population
| Unilateral | Bilateral | p-value | |
|---|---|---|---|
| PICU mortality, in % | 9.3% | 26.3% | 0.025* |
| Ventilator free days, median (IQR) in days | 20 [14.5–23] | 16.5 [0–21] | 0.019* |
| PICU length of stay, median (IQR) in days | 8 [5–13] | 10 [7.75–19.25] | 0.030* |
| MV duration, median (IQR) in days | 8 [5–11.5] | 9 [6.75–14.25] | 0.054 |
A significant lower mortality was found in the PALICC population with unilateral consolidations (9.3%) compared to bilateral consolidations (26.3%). For the cohort with unilateral consolidations also a significant difference was found in VFD (median 20 vs 16.5 days) and PICU length of stay (median 8 vs 10 days) compared to bilateral consolidations. No significant difference was found for the MV duration
*Indicates significant differences
Eighteen patients received HFOV at PARDS onset, of whom 10 (55.6%) had severe PARDS (Fig. 4). At 48 h all patients with severe PARDS (N = 20) received HFOV. Application of the Berlin definition affected severity stratification (Fig. 5). Of the 117 patients receiving CMV at onset, 29 patients received HFOV 24 h after onset and 8 were extubated/deceased. VFD and mortality did not differ between the groups (Fig. 6). When patients were stratified in three categories by MV strategy over 48 h (HFOV for 48 h, partly HFOV/partly CMV and CMV for 48 h) there was no significant difference found in mortality (p = 0.833) nor in VFD (p = 0.135).
Fig. 4.

Distribution of ventilator mode stratified by PARDS severity at three time points (onset of PARDS, and 24 and 48 h after onset). The blue area represents CMV and the orange area HFOV. At onset 135 met PALICC criteria. 98% of the subjects with mild PARDS received CMV, 84.4% of the moderate group received CMV and 65.5% of the subjects meeting PALICC criteria for severe PARDS at onset received CMV. Twenty-four hours after onset still 105 met PALICC criteria (45 mild, 34 moderate, 26 severe). Of the group with mild PARDS 95.5% received CMV, 44.4% of the moderate group received CMV 24 h after onset and only 15.4% of the subjects with severe PARDS 24 h after onset received CMV. Forty-eight hours after onset 90 subject still met PALICC criteria for PARDS (36 mild, 34 moderate, 20 severe). Of the group with mild PARDS after 48 h 86.1% received CMV at that moment, of the moderate group 41.1% received CMV, of the severe group 0% received CMV
Fig. 5.

Difference in severity by oxygenation assessment method. Eighteen subjects received HFOV at PARDS onset. When severity was stratified by OI, 1 had mild PARDS, 7 moderate and 10 severe. When the PF is used for the same subjects 3 have mild ARDS, 11 moderate ARDS, 4 severe ARDS. Forty-three subjects received HFOV 24 h after onset, when severity is stratified by the OI 2 meet criteria for mild PARDS, 19 for moderate PARDS, 22 for severe PARDS. When the PF is used 1 doesn’t meet criteria for ARDS anymore, 8 meet criteria for mild ARDS, 27 for moderate and 7 for severe ARDS. Forty-five subjects received HFOV 48 h after onset. Hereof 5 met criteria for mild PARDS, 20 for moderate and 20 for severe PARDS. When these subjects were stratified by PF 3 do not meet ARDS criteria anymore, 11 meet criteria for mild ARDS, 19 for moderate ARDS and 12 meet criteria for severe ARDS
Fig. 6.

The effect of ventilation strategy in the first 24 h on the PARDS severity distribution, mortality and VFD. On the left the group of subjects receiving CMV the first 24 h after onset, on the right the group who are switched from CMV to HFOV within the first 24 h after onset. Grey bars represent number of cases with mild, moderate and severe PARDS. Orange dots depict median (with interquartile range) VFD-28 (bottom Y-axis) and blue triangles represent mortality (%) (upper Y-axis)
Discussion
The main finding of this study is that identification of PARDS improved significantly when paediatric specific definition was applied. This was mainly due to not mandating bilateral consolidations on chest radiograph. Both existing adult definitions and the paediatric specific definition poorly stratified the risk for mortality in our cohort.
The PALICC PARDS definition was created to overcome the limitations of the adult-based definitions including epidemiological differences and the need for invasive metrics for oxygenation [18]. The international, observational Paediatric acute respiratory distress syndrome incidence and epidemiology (PARDIE) confirmed a better performance of PALICC PARDS in terms of identification of new PARDS cases and risk stratification [15]. The number of new PARDS cases in our study increased with the PALICC definition, comparable to PARDIE and numbers reported by others in retrospective single-center studies [19, 20]. However, in PARDIE less than half of the newly diagnosed PARDS cases was based on invasive metrics of oxygenation. Furthermore, there was a higher use of arterial blood gas in non-survivors, suggesting that there was a preference not to use indwelling arterial lines in lesser sick patients not being on vaso-active drugs as has been suggested previously [13]. In contrast, in our unit indwelling arterial lines are routinely inserted upon start of MV and not just for better haemodynamic monitoring, making that almost all our newly identified PARDS cases were based on arterial blood gasses. Also, our study differs from PARDIE as we did not include any patient on non-invasive ventilation (not offered in our unit). Like PARDIE, we observed the highest mortality rate among severe PARDS patients. Since our study was retrospective, it may thus be surmised that not the definition itself, but increased awareness may at least partially better identify new cases of PARDS.
We observed a prevalence of new PARDS of 5.5% which is in accordance with literature of the PALICC definition which ranges from 2.7 to 5.7% [15, 19, 20]. Our prevalence is most likely to be underestimated since patients who received NIMV, had home ventilation or cyanotic heart disease were excluded in this study although these are specially categorized in the PALICC definition.
PALICC PARDS poorly stratified risk of mortality in our study, contrasting the findings from the PARDIE study [15]. However, PARDIE only found higher mortality rates among patients with severe PARDS, an observation that was also made in the patient cohort coming from the Children’s Hospital of Los Angeles (CHLA) [19]. This lack of performance is not easily explained. From a methodological perspective, it might be argued that incorporating non-invasive metrics for oxygenation in the PALICC definition dilutes the cohort by including less sick PARDS patients, although in the PARDIE study the way how oxygenation was assessed (invasive vs non-invasive) did not appear to be associated with hypoxaemia severity. Alternatively, mortality may not be the right endpoint in PARDS since many patients die with and not from ARDS [21]. In fact, neurologic aetiologies of death in children with PARDS are common, confounding true mortality rates [22]. Overall mortality in our study was low, like other high-income countries but lower than low-income countries, and increased with increasing severity [23, 24]. We found that the best risk prediction for mortality, duration of MV, VFD and PICU length of stay was 24 h after onset by the PALICC definition, which is like the CHLA dataset but different from PARDIE reporting that this could be best done 6 h after PARDS diagnosis [15, 19]. Importantly, PARDS is a heterogenous syndrome with, calling for unpacking the syndrome by PARDS trigger or by clinical phenotype. For example, respiratory syncytial virus (RSV) lower respiratory tract infection may cause PARDS but is associated with low mortality [25]. Thus, future studies evaluating paediatric specific definitions for ARDS may consider stratifying by PARDS trigger, disease severity and cause of death.
Surprisingly, we found that not only PALICC but also the adult based Berlin definition performed poorly in terms of outcome stratification. De Luca and colleagues provided support for the usefulness of the Berlin definition in infants, but we could not confirm this in the present study [26]. However, we did find that the presence of bilateral consolidations on chest radiograph significantly added to mortality in contrast with the PARDIE study, making that there was higher mortality rate in severe patients when the Berlin definition was applied [27]. This warrants further study.
Our findings may also have been confounded by a liberal use of HFOV Patients receiving HFOV had more severe PARDS and all patients who met criteria for severe PARDS 48 h after onset received HFOV. In our unit, HFOV is used as an alternative mode of ventilation to prevent conventional ventilator settings becoming toxic or when there is severe hypoxaemia. Since we use an open-lung strategy characterised by high mPaw, automatically the OI will be higher and thereby influence the PARDS severity strata [28]. Interestingly, we observed lower mortality rates in patients managed with HFOV within 24 h after PARDS diagnosis, but numbers were too small to draw statistically significant conclusions.
There are various limitations to our analysis. First, our study was designed as a retrospective, single centre study. Although our unit probably is comparable to many other units based in high-income countries, our institutional practices including the times per date ABGs are done may vary confounding the main outcome parameters. Inherent with the retrospective design, clinical decision-making could not be captured, and missing data were not imputed. Second, pulse oximetry data were retrospectively making that precise alignment of mPaw, SpO2 and FiO2 could not be guaranteed; this has also been reported by others [29]. Furthermore, the number of patients with SpO2 > 97% precluded application of the PALICC criteria. Third, the presence of LV dysfunction was not evaluated in all patients and only deemed present if noted in the electronic health record. Lastly, evaluating chest radiographs is very subjective and has a proven high inter-observer variability [27, 30–32]. Our strategy was modelled after clinical practice where one observer interprets the chest-radiograph and only in case of uncertainty by a second observer. Inherently, this led to a high preselection and made it unreliable to calculate Cohen’s Kappa.
Conclusions
This single-centre study confirmed that PALICC identified more new cases PARDS than the adult-based Berlin definition. However, both PALICC and Berlin performed poorly in terms of mortality risk stratification. The presence of bilateral consolidations was associated with a higher mortality rate. Our findings may be considered in future modifications of the PALICC criteria. They also indicate that patient with severe PARDS with bilateral consolidations may be the primary target population for future randomised controlled trials.
Supplementary Information
Additional file 1. Flow chart of the experimental design. First all patients were selected who received MV over 24 h during PICU admission, then there was screened for exclusion criteria. Of the remaining cohort all chest radiographs were reviewed during day -1 up to day 8 of PICU admission by the first reviewer (MR). In case of a possible consolidation the second reviewer reviewed the chest radiographs (JvD). Hereof another selection was made and reviewed by a third reviewer (MK or RB), in case of a found consolidation the patient card was screened for the oxygenation criterium +/− 24 h of the chest radiograph.
Acknowledgements
Not applicable.
Abbreviations
- ABG
Arterial blood gas
- AECC
American–European consensus conference
- ALI
Acute lung injury
- ARDS
Acute respiratory distress syndrome
- AUC
Area under the curve
- BD
Berlin definition
- CDP
Continuous distending pressure
- CI
Confidence interval
- CMV
Conventional mechanical ventilation
- CPAP
Continuous positive airway pressure
- ECLS
Extracorporeal life support
- HFOV
High frequency oscillatory ventilation
- (I)MV
Invasive mechanical ventilation
- IQR
Interquartile range
- LV
Left ventricular
- mPaw
Mean airway pressure
- NIMV
Non-invasive mechanical ventilation
- OI
Oxygenation index, formula: [FiO2 × Paw × 100]/PaO2
- OSI
Oxygen saturation index, formula: [FiO2 × Paw × 100]/SpO2
- PALICC
Paediatric acute lung injury consensus conference
- PARDS
Paediatric acute respiratory distress syndrome
- Paw
Mean airway pressure
- PEEP
Positive end expiratory pressure
- PF
PaO2/FiO2
- PICU
Paediatric intensive care unit
- PIM
Paediatric index of mortality
- PRISM
Paediatric risk of mortality score
- ROC
Receiver operating curve
- RSV
Respiratory syncytial virus
- UMCG
University Medical Center Groningen
- VFD
Ventilator free days at 28 days
Authors’ contributions
JvD analysed first selection of chest X-rays and reviewed the manuscript. RB analysed 40% of the second selection of chest X-rays and reviewed the manuscript. MK analysed 60% of second selection chest X-rays, assisted with the statistical analyses and wrote the manuscript. MR collected all data, analysed all chest X-rays, performed the statistical analyses and wrote the manuscript. All authors read and approved the final manuscript.
Funding
Not applicable.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
The Institutional Review Board of the University Medical Center Groningen approved the study and waived the need for informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests in this section.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Michelle Rudolph, Email: m.w.rudolph@umcg.nl.
Jefta van Dijk, Email: j.van.dijk01@umcg.nl.
Pauline de Jager, Email: p.de.jager@umcg.nl.
Sandra K. Dijkstra, Email: s.k.dijkstra@umcg.nl
Johannes G. M. Burgerhof, Email: j.g.m.burgerhof@umcg.nl
Robert G. T. Blokpoel, Email: r.g.t.blokpoel@umcg.nl
Martin C. J. Kneyber, Email: m.c.j.kneyber@umcg.nl
References
- 1.Ashbaugh D, Boyd Bigelow D, Petty T, Levine B. Acute respiratory distress in adults. The Lancet. 1967;290:319–323. doi: 10.1016/S0140-6736(67)90168-7. [DOI] [PubMed] [Google Scholar]
- 2.Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, The American-European Consensus Conference on ARDS et al. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149(3 Pt 1):818–824. doi: 10.1164/ajrccm.149.3.7509706. [DOI] [PubMed] [Google Scholar]
- 3.Force ADT, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307(23):2526–2533. doi: 10.1001/jama.2012.5669. [DOI] [PubMed] [Google Scholar]
- 4.Dahlem P, van Aalderen WM, Hamaker ME, Dijkgraaf MG, Bos AP. Incidence and short-term outcome of acute lung injury in mechanically ventilated children. Eur Respir J. 2003;22(6):980–985. doi: 10.1183/09031936.03.00003303. [DOI] [PubMed] [Google Scholar]
- 5.Kneyber MC, Brouwers AG, Caris JA, Chedamni S, Plotz FB. Acute respiratory distress syndrome: is it underrecognized in the pediatric intensive care unit? Intensive Care Med. 2008;34(4):751–754. doi: 10.1007/s00134-008-1029-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zimmerman JJ, Akhtar SR, Caldwell E, Rubenfeld GD. Incidence and outcomes of pediatric acute lung injury. Pediatrics. 2009;124(1):87–95. doi: 10.1542/peds.2007-2462. [DOI] [PubMed] [Google Scholar]
- 7.Bindl L, Dresbach K, Lentze MJ. Incidence of acute respiratory distress syndrome in German children and adolescents: a population-based study. Crit Care Med. 2005;33(1):209–312. doi: 10.1097/01.CCM.0000151137.76768.08. [DOI] [PubMed] [Google Scholar]
- 8.Lopez-Fernandez Y, Azagra AM, de la Oliva P, Modesto V, Sanchez JI, Parrilla J, et al. Pediatric Acute Lung Injury Epidemiology And Natural History Study: Incidence and outcome of the acute respiratory distress syndrome in children. Crit Care Med. 2012;40(12):3238–3245. doi: 10.1097/CCM.0b013e318260caa3. [DOI] [PubMed] [Google Scholar]
- 9.Erickson S, Schibler A, Numa A, Nuthall G, Yung M, Pascoe E, et al. Acute lung injury in pediatric intensive care in Australia and New Zealand: a prospective, multicenter, observational study. Pediatr Crit Care Med. 2007;8(4):317–323. doi: 10.1097/01.PCC.0000269408.64179.FF. [DOI] [PubMed] [Google Scholar]
- 10.Hu X, Qian S, Xu F, Huang B, Zhou D, Wang Y, et al. Incidence, management and mortality of acute hypoxemic respiratory failure and acute respiratory distress syndrome from a prospective study of Chinese paediatric intensive care network. Acta Paediatr. 2010;99(5):715–721. doi: 10.1111/j.1651-2227.2010.01685.x. [DOI] [PubMed] [Google Scholar]
- 11.Yu WL, Lu ZJ, Wang Y, Shi LP, Kuang FW, Qian SY, et al. The epidemiology of acute respiratory distress syndrome in pediatric intensive care units in China. Intensive Care Med. 2009;35(1):136–143. doi: 10.1007/s00134-008-1254-x. [DOI] [PubMed] [Google Scholar]
- 12.Schouten LR, Veltkamp F, Bos AP, van Woensel JB, Serpa Neto A, Schultz MJ, et al. Incidence and mortality of acute respiratory distress syndrome in children: a systematic review and meta-analysis. Crit Care Med. 2016;44(4):819–829. doi: 10.1097/CCM.0000000000001388. [DOI] [PubMed] [Google Scholar]
- 13.Khemani RG, Rubin S, Belani S, Leung D, Erickson S, Smith LS, et al. Pulse oximetry vs. PaO2 metrics in mechanically ventilated children: Berlin definition of ARDS and mortality risk. Intensive Care Med. 2015;41(1):94–102. doi: 10.1007/s00134-014-3486-2. [DOI] [PubMed] [Google Scholar]
- 14.Pediatric Acute Lung Injury Consensus Conference, G Pediatric acute respiratory distress syndrome: consensus recommendations from the pediatric acute lung injury consensus conference. Pediatr Crit Care Med. 2015;16(5):428–439. doi: 10.1097/PCC.0000000000000350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Khemani RG, Smith L, Lopez-Fernandez YM, Kwok J, Morzov R, Klein MJ, et al. Paediatric acute respiratory distress syndrome incidence and epidemiology (PARDIE): an international, observational study. Lancet Respir Med. 2019;7(2):115–128. doi: 10.1016/S2213-2600(18)30344-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yehya N, Harhay MO, Curley MAQ, Schoenfeld DA, Reeder RW. Reappraisal of ventilator-free days in critical care research. Am J Respir Crit Care Med. 2019;200(7):828–836. doi: 10.1164/rccm.201810-2050CP. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pollack MM, Patel KM, Ruttimann UE. PRISM III: an updated Pediatric Risk of Mortality score. Crit Care Med. 1996;24(5):743–752. doi: 10.1097/00003246-199605000-00004. [DOI] [PubMed] [Google Scholar]
- 18.Khemani RG, Wilson DF, Esteban A, Ferguson ND. Evaluating the Berlin Definition in pediatric ARDS. Intensive Care Med. 2013;39(12):2213–2216. doi: 10.1007/s00134-013-3094-6. [DOI] [PubMed] [Google Scholar]
- 19.Parvathaneni K, Belani S, Leung D, Newth CJ, Khemani RG. Evaluating the performance of the pediatric acute lung injury consensus conference definition of acute respiratory distress syndrome. Pediatr Crit Care Med. 2017;18(1):17–25. doi: 10.1097/PCC.0000000000000945. [DOI] [PubMed] [Google Scholar]
- 20.Gupta S, Sankar J, Lodha R, Kabra SK. Comparison of prevalence and outcomes of pediatric acute respiratory distress syndrome using pediatric acute lung injury consensus conference criteria and Berlin definition. Front Pediatr. 2018;6:93. doi: 10.3389/fped.2018.00093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yehya N, Thomas NJ. Relevant outcomes in pediatric acute respiratory distress syndrome studies. Front Pediatr. 2016;4:51. doi: 10.3389/fped.2016.00051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Yehya N, Harhay MO, Klein MJ, Shein SL, Pineres-Olave BE, Izquierdo L, et al. Predicting mortality in children with pediatric acute respiratory distress syndrome: a pediatric acute respiratory distress syndrome incidence and epidemiology study. Crit Care Med. 2020;48:e514–e522. doi: 10.1097/CCM.0000000000004345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Schouten LRA, Veltkamp F, Bos AP, van Woensel JBM, Serpa Neto A, Schultz MJ, et al. Incidence and mortality of acute respiratory distress syndrome in children. Crit Care Med. 2016;44:819–829. doi: 10.1097/CCM.0000000000001388. [DOI] [PubMed] [Google Scholar]
- 24.Moynihan KM, Alexander PMA, Schlapbach LJ, Millar J, Jacobe S, Ravindranathan H, et al. Epidemiology of childhood death in Australian and New Zealand intensive care units. Intensive Care Med. 2019;45:1262–1271. doi: 10.1007/s00134-019-05675-1. [DOI] [PubMed] [Google Scholar]
- 25.Bem RA, Kneyber MC, van Woensel JB. Respiratory syncytial virus-induced paediatric ARDS: why we should unpack the syndrome. Lancet Respir Med. 2017;5(1):9–10. doi: 10.1016/S2213-2600(16)30425-8. [DOI] [PubMed] [Google Scholar]
- 26.De Luca D, Piastra M, Chidini G, Tissieres P, Calderini E, Essouri S, et al. The use of the Berlin definition for acute respiratory distress syndrome during infancy and early childhood: multicenter evaluation and expert consensus. Intensive Care Med. 2013;39(12):2083–2091. doi: 10.1007/s00134-013-3110-x. [DOI] [PubMed] [Google Scholar]
- 27.López-Fernández YM, Smith LS, Kohne JG, Weinman JP, Modesto-Alapont V, Reyes-Dominguez SB, et al. Prognostic relevance and inter-observer reliability of chest-imaging in pediatric ARDS: a pediatric acute respiratory distress incidence and epidemiology (PARDIE) study. Intensive Care Med. 2020;46(7):1382–1393. doi: 10.1007/s00134-020-06074-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.de Jager P, Kamp T, Dijkstra SK, Burgerhof JGM, Markhorst DG, Curley MAQ, et al. Feasibility of an alternative, physiologic, individualized open-lung approach to high-frequency oscillatory ventilation in children. Ann Intensive Care. 2019;9(1):9. doi: 10.1186/s13613-019-0492-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Khemani RG, Parvathaneni K, Yehya N, Bhalla AK, Thomas NJ, Newth CJL. PEEP lower than the ARDS Network Protocol is associated with higher pediatric ARDS mortality. Am J Respir Crit Care Med. 2018;198:77–89. doi: 10.1164/rccm.201707-1404OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Meade MO, Cook RJ, Guyatt GH, Groll R, Kachura JR, Bedard M, Cook DJ, Slutsky AS, Stewart TE. Interobserver variation in interpreting chest radiographs for the diagnosis of acute respiratory distress syndrome. Am J Respir Crit Care Med. 2000;161:85–90. doi: 10.1164/ajrccm.161.1.9809003. [DOI] [PubMed] [Google Scholar]
- 31.Angoulvant F, Llor J, Alberti C, Kheniche A, Zaccaria I, Garel C, et al. Inter-observer variability in chest radiograph reading for diagnosing acute lung injury in children. Pediatr Pulmonol. 2008;43(10):987–991. doi: 10.1002/ppul.20890. [DOI] [PubMed] [Google Scholar]
- 32.Rubenfeld GD, Caldwell E, Granton J, Hudson LD, Matthay MA. Interobserver variability in applying a radiographic definition for ARDS. Chest. 1999;116(5):1347–1353. doi: 10.1378/chest.116.5.1347. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1. Flow chart of the experimental design. First all patients were selected who received MV over 24 h during PICU admission, then there was screened for exclusion criteria. Of the remaining cohort all chest radiographs were reviewed during day -1 up to day 8 of PICU admission by the first reviewer (MR). In case of a possible consolidation the second reviewer reviewed the chest radiographs (JvD). Hereof another selection was made and reviewed by a third reviewer (MK or RB), in case of a found consolidation the patient card was screened for the oxygenation criterium +/− 24 h of the chest radiograph.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.