

Abstract
Background and Purpose:
Individuals with sickle cell anemia (SCA) experience cognitive deficits, even in the absence of cerebral infarcts or strokes. This study tested the hypothesis that elevated cerebral blood flow (CBF) and oxygen extraction fraction (OEF) are associated with lower executive function in individuals with SCA.
Methods:
3-Tesla brain MRI was performed including anatomical, gray matter CBF, and global OEF imaging. Executive function was measured using the Working Memory Index from an age-appropriate Wechsler battery and tasks from the NIH Toolbox Cognition Battery. Bivariate and multivariate models were examined (significance: p<0.05).
Results:
Fifty-four participants (age range=6-31 years) with SCA were enrolled. Hematocrit was positively related to fluid cognition, CBF was inversely related to working memory and inhibitory control, and OEF was inversely related to processing speed. Associations remained significant in multivariate analyses controlling for age, income, and infarcts.
Conclusions:
Elevated CBF and OEF, markers of hemodynamic impairment, are associated with deficits in executive function in individuals with SCA.
Keywords: Hemodynamic, oxygen extraction fraction, cerebral blood flow, executive function, sickle cell anemia
Introduction
Sickle cell anemia (SCA) is a genetic hemoglobinopathy that results in hemolysis, chronic anemia, and reduced oxygen carrying capacity. Cerebral infarction is the most common cause of neurological injury in SCA,1 and infarcts are associated with significantly lower cognitive functioning.2 Nevertheless, cognitive deficits still occur in individuals without a history of infarcts.2
Cerebral hemodynamic indicators of infarct risk and cerebral metabolic stress are likely key variables in understanding the impact of SCA on cognitive function. When arterial oxygen content decreases, cerebral blood flow (CBF; ml blood/100 g tissue/min) increases to maintain adequate delivery of oxygen to tissue; if this increase is insufficient, oxygen extraction fraction (OEF), the ratio of oxygen consumed to oxygen delivered, will increase for constant cerebral metabolic rate of oxygen consumption.3 OEF is hypothesized to be a better indicator of infarct risk and metabolic stress in brain tissue compared to other compensatory changes in cerebral hemodynamics.3 Children, adolescents, and adults with SCA have been shown to have higher CBF and OEF than healthy controls,3,4 and these cerebral hemodynamic imbalances are likely critical to cognitive impairment in this population.
To extend our understanding of hemodynamic predictors of neurocognitive impairment in SCA, we tested the hypothesis that elevated CBF and OEF are associated with lower executive function, after controlling for cerebral infarcts, age, and environmental characteristics.
Methods
The data that support the study findings are available from the corresponding author upon reasonable request.
Participants
Recruitment occurred at Vanderbilt University Medical Center between January 2018 and December 2019. Children, adolescents, and young adults with SCA (hemoglobin [Hb] SS or HbSβ0 Thalassemia) were prospectively enrolled and provided informed, written consent in accordance with the Institutional Review Board.
Neuroimaging Visit
Each participant received a 3-Tesla non-contrast head MRI and MRA, and a neurologic examination by the study neurologist (See Supplemental Material). Hematocrit values were obtained from venipuncture at the time of MRI. For CBF measurement, pseudo-continuous arterial spin labeling (pCASL) MRI was performed. For OEF measurement, T2-relaxation-under-spin-tagging5 was acquired and repeated once. CBF was calculated from pCASL using the solution to the flow-modified Bloch equation after correcting for individual hematocrit. OEF was quantified using two previously characterized calibration curves generated from human blood with high levels of HbF6 and HbAA blood calibrated over an anemic hemoglobin range.7
Neurocognitive Assessment Visit
Participants and/or their caregivers completed questionnaires on demographic characteristics. Participants completed the Working Memory Index (WMI) from an age-appropriate Wechsler battery8,9 and the NIH Toolbox Cognitive Battery10 to assess domains of executive function.
Statistical analysis
Pearson correlations were used to determine bivariate associations, and the False Discovery Rate was used to correct for possible Type I error. Linear regressions determined the unique variance of cerebral hemodynamics on executive function. Each model controlled for participant age, annual household income, and history of either silent or overt infarct as each of these variables have been shown to be related to executive function in SCA.2,11 The variance inflation factor across all regressions implied no multicollinearity among variables. Supplemental regression analyses were conducted in subsamples of participants without overt stroke and without any infarcts. All analyses were performed using SPSS, version 26.
Results
Fifty-four participants with SCA were enrolled, including 29 children ages 6-17 years and 25 adults ages 18-31 years (Table 1).
Table 1.
Demographic characteristics and descriptive statistics of study subjects and variables
| Total Sample | p Valuea | |
|---|---|---|
| Age at assessment, M (SD) | 17.2 (8.12) | |
| Sex, n (%) | ||
| Female | 30 (55.6) | |
| Annual household income, n (%) | ||
| $10,000 or under | 14 (25.9) | |
| $10,001—$20,000 | 6 (11.1) | |
| $20,001—$30,000 | 8 (14.8) | |
| $30,001—$40,000 | 7 (13.0) | |
| $40,001—$50,000 | 3 (5.6) | |
| $50,001—$60,000 | 3 (5.6) | |
| $60,001—$70,000 | 0 (0.0) | |
| $70,001—$80,000 | 1 (1.9) | |
| $80,001 or more | 6 (11.1) | |
| Medical characteristics | ||
| SCA phenotype, n (%) | ||
| HbSS | 49 (90.7) | |
| HbSB0 | 5 (9.3) | |
| Hydroxyurea, n (%) | 42 (77.8) | |
| Transfusions, n (%) | 17 (31.5) | |
| No treatment, n (%) | 2 (3.7) | |
| Hemoglobin level | 8.98 (1.26) | |
| Hematocrit % | 25.83 (3.77) | |
| CaO2, M (SD) | 11.48 (1.71) | |
| CBF, M (SD) | 80.49 (18.10) | |
| OEF (HbF), M (SD) | 39.86 (6.94) | |
| OEF (HbAA), M (SD) | 34.52 (5.91) | |
| Silent infarct, n (%) | 20 (37.0) | |
| Stroke, n (%) | 5 (9.3) | |
| Months between MRI and assessment, M (SD) | 19.02 (10.87) | |
| Executive Function, M (SD)b | ||
| Wechsler WMI | 94.06 (15.68) | .007 |
| NIHTB-CB | ||
| Dimensional Change | 89.57 (18.16) | <.001 |
| Inhibitory Control | 79.53 (13.84) | <.001 |
| Working Memory | 92.81 (13.45) | .001 |
| Processing Speed | 86.22 (18.07) | <.001 |
| Episodic Memory | 97.06 (15.45) | .189 |
| Fluid Cognition | 83.06 (17.20) | <.001 |
CaO2 = oxygen content; CBF = cerebral blood flow; OEF = oxygen extraction fraction; WMI = working memory index; NIHTB-CB = National Institutes of Health Toolbox Cognition Battery.
p value of one-sample t test comparing scores on cognitive assessments with normative mean (M=100, SD=15).
Age-corrected standard score.
Correlations showed that hematocrit was positively related to fluid cognition (p=.020), and CBF was inversely correlated with working memory (p=.009) and inhibitory control (p=.026). Figure 1 shows FLAIR images, CBF images, and scatterplots of CBF and executive function. OEF HbF calibration was inversely related to processing speed (p=.044). These associations, however, were not significant after controlling for Type I error.
Figure 1.

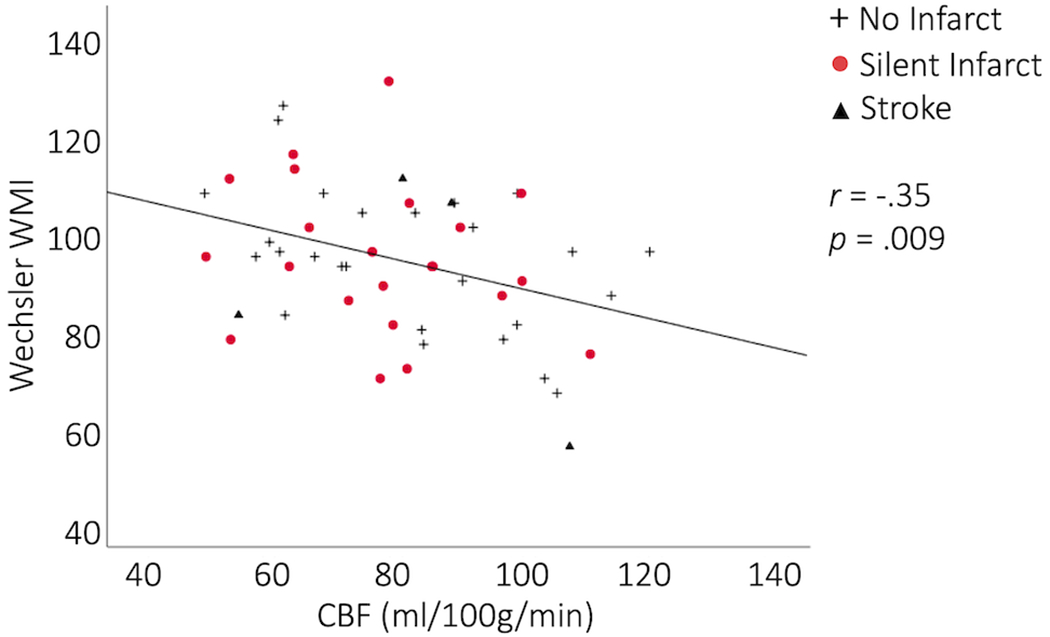

FLAIR images, CBF images, and scatterplots of CBF and executive function
(A) A 16-year-old female with sickle cell anemia (SCA) and no infarcts, and a 34-year-old male with SCA and large and small infarcts on FLAIR images. Color bar is cerebral blood flow (CBF) in units of ml blood / 100g tissue / minute. CBF is elevated in the participant with SCA and no infarcts and further elevated in the participant with SCA and large infarct. (B) Scatter plot of CBF and working memory. (C) Scatter plot of CBF and inhibitory control.
Multivariate regressions controlled for age, income, and history of silent or overt infarct; hematocrit was positively related to inhibitory control, processing speed, and fluid cognition (ps< .05). CBF was inversely related to working memory and inhibitory control, and OEF HbF calibration was inversely related to processing speed (p<.05). Supplemental regression analyses showed that both OEF models were significant inverse predictors of processing speed (ps<.05) in analyses excluding participants with overt stroke and analyses excluding participants with any infarcts. Further, CBF was inversely related to working memory (p=.022) when excluding participants with infarcts.
See Data Supplement for tables describing correlations and regression analyses.
Discussion
Impaired cerebral hemodynamics are related to poor executive performance in individuals with SCA. Prior research on cerebral hemodynamic risks for cognitive deficits in SCA has focused primarily on transcranial Doppler ultrasound (TCD) velocity.11 TCD is often conceptualized as a proxy for blood delivery to the brain, though elevated velocities could be related to low hematocrit and arterial stenosis. CBF, however, assesses the actual rate of blood delivery to brain tissue. Elevated CBF indicates a higher autoregulatory response required to offset reduced arterial blood oxygen content,3,4 and results suggest that higher CBF is associated with reduced working memory and inhibitory control.
Findings also provide the first evidence of the association of OEF with a measure of executive function in SCA. Findings suggest that OEF could play an additional role in cognitive function in individuals with SCA beyond the effect of cerebral infarcts and psychosocial factors. These results extend prior research on 15O positron emission tomography (PET)-measured OEF and cognitive function in adults with cardiovascular disease,12 suggesting that high baseline OEF is related to lower cognitive function. While prior research has provided evidence for cerebral hemodynamic effects on general intelligence12 and other domains of cognition,11 findings here suggest a specific impact on executive functions.
Although elevated CBF and OEF are adaptive compensatory cerebral mechanisms to accommodate for hypoxic and anemic conditions, dysregulation of these parameters likely indicates stroke risk and associated deficits in executive function. Lower CBF and OEF baseline levels could provide additional room for necessary hemodynamic change during the difficult executive tasks that require input from multiple structures throughout the brain. Reducing CBF and OEF in SCA could have direct downstream effects on executive function and indirect preservation of functioning by reducing infarct and stroke risk. Prior research suggests that elevated cerebral hemodynamics are sensitive to biological interventions for stroke prevention,13 and these interventions also improve executive function.14 Hemodynamic changes could be important mediating factors in the association between SCA treatments and changes in executive function. Further study and clinical assessment of cerebral hemodynamics may be warranted for intervention and prevention of cognitive decline in SCA.
Several limitations should be considered when interpreting findings, including the modest sample size that does not allow for detailed statistical modeling of other medical comorbidities and treatment effects. Further, although significant bivariate correlations did not withstand correction using False Discovery Rate, we proceeded with multivariate analyses due to the preliminary and novel aims of the current study. Other limitations include use of whole-brain hemodynamic measures as regional differences may be important for specific aspects of executive function, with some controversy regarding the MRI method to assess OEF which requires calibration models relating MRI-assessed T2 venous blood relaxation times (Yv) to oxygenation5,6,7,15 (see discussion in the Data Supplement), and a prospective design with wide variance in lag time across participants. The current study did not include comparisons of associations relative to healthy controls. Individuals with SCA have been shown to have consistently higher CBF and often higher OEF than healthy peers,3,4 and elevated OEF is related to lower executive function; therefore, it is possible that the association between OEF and executive function is stronger in SCA. Nevertheless, it will be important to replicate findings using a larger sample that includes healthy controls and additional relevant global and regional covariates of tissue health and white and grey matter volume.
Supplementary Material
Acknowledgments
Sources of Funding
Grants from the National Institutes of Health, F31-HD09559, R01NS096127, K24-HL147017, T32-MH18921, and the American Heart Association 14CSA20380466.
Disclosures
Manus Donahue receives research-related support from Philips Healthcare and is a paid consultant for Global Blood Therapeutics, Pfizer, Biomuse, LymphaTouch, and bluebird bio. Lori Jordan has consulted for bluebird bio. Michael DeBaun has consulted regarding clinical trials for Global Blood Therapeutics and Novartis and for Vertex/CRISPR CTX001 Therapeutics. All outside the submitted work.
Non-standard Abbreviations and Acronyms:
- CBF
cerebral blood flow
- OEF
oxygen extraction fraction
- SCA
sickle cell anemia
- TCD
transcranial Doppler ultrasound
Footnotes
References
- 1.Ohene-Frempong K, Weiner SJ, Sleeper LA, Miller ST, Embury S, Moohr JW, Wethers DL, Pegelow CH, Gill FM. Cerebrovascular accidents in sickle cell disease: rates and risk factors. Blood. 1998;91:288–294. [PubMed] [Google Scholar]
- 2.Prussien KV, Jordan LC, DeBaun MR, Compas BE. Cognitive function in sickle cell disease across domains, cerebral infarct status, and the lifespan: A meta-analysis. J Pediatr Psychol. 2019;44:948–958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fields ME, Guilliams KP, Ragan DK, Binkley MM, Eldeniz C, Chen Y, Hulbert ML, McKinstry RC, Shimony JS, Vo KD, et al. Regional oxygen extraction predicts border zone vulnerability to stroke in sickle cell disease. Neurology. 2018;90:e1134–1142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jordan LC, Gindville MC, Scott AO, Juttukonda MR, Strother MK, Kassim AA, Chen SC, Lu H, Pruthi S, Shyr Y, et al. Non-invasive imaging of oxygen extraction fraction in adults with sickle cell anaemia. Brain. 2016;139(Pt 3):738–750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lu H, Xu F, Grgac K, Liu P, Qin Q, van Zijl P. Calibration and validation of TRUST MRI for the estimation of cerebral blood oxygenation. Magn Reson Med. 2012;67:42–49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Liu P, Chalak LF, Krishnamurthy LC, Mir I, Peng SL, Huang H, Lu H. T1 and T2 Values of Human Neonatal Blood at 3 Tesla: Dependence on Hematocrit, Oxygenation, and Temperature. Magn Reson Med. 2016;75(4):1730–1735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bush A, Borzage M, Detterich J, Kato RM, Meiselman HJ, Coates T, Wood JC. Empirical model of human blood transverse relaxation at 3 T improves MRI T2 oximetry. Magn Reson Med. 2017;77:2364–2371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wechsler D Wechsler intelligence scale for children--fifth edition. San Antonio, TX: Pearson; 2014. [Google Scholar]
- 9.Wechsler D Wechsler adult intelligence scale--fourth edition. San Antonio, TX: Pearson; 2008. [Google Scholar]
- 10.Weintraub S, Dikmen SS, Heaton RK, Tulsky DS, Zelazo PD, Bauer PJ, Carlozzi NE, Slotkin J, Blitz D, Wallner-Allen K, et al. Cognition assessment using the NIH Toolbox. Neurology. 2013;80(11 Suppl 3):S54–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Prussien KV, Siciliano RE, Ciriegio AE, Anderson AS, Sathanayagam R, DeBaun MR, Jordan LC, Compas BE. Correlates of Cognitive Function in Sickle Cell Disease: A Meta-Analysis. J Pediatr Psychol. 2020;45:145–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Marshall RS, Festa JR, Cheung YK, Chen R, Pavol MA, Derdeyn CP, Clarke WR, Videen TO, Grubb RL, Adams HP, et al. Cerebral hemodynamics and cognitive impairment: baseline data from the RECON trial. Neurology. 2012;78: 250–255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Guilliams KP, Fields ME, Ragan DK, Eldeniz C, Binkley MM, Chen Y, Comiskey LS, Doctor A, Hulbert ML, Shimony JS, et al. Red cell exchange transfusions lower cerebral blood flow and oxygen extraction fraction in pediatric sickle cell anemia. Blood. 2018;131: 1012–1021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hood AM, King AA, Fields ME, Ford AL, Guilliams KP, Hulbert ML, Lee JM, White DA. Higher executive abilities following a blood transfusion in children and young adults with sickle cell disease. Pediatr Blood Cancer. 2019;66:e27899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Li W, Xu X, Liu P, Strouse JJ, Casella JF, Lu H, van Zijl PCM, Qin Q. Quantification of whole-brain oxygenation extraction fraction and cerebral metabolic rate of oxygen consumption in adults with sickle cell anemia using individual T 2 -based oxygenation calibrations. Magn Reson Med. 2020;83:1066–1080. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.