

Abstract
Military personnel rely on caffeinated products such as coffee or energy drinks (ED) to maintain a maximal level of vigilance and performance under sleep-deprived and combat situations. While chronic caffeine intake is associated with decreased sleep duration and non-restful sleep in the general population, these relationships are understudied in the military. We conducted a focused review of the effects of caffeinated products on sleep and the functioning of military personnel. We used a pre-specified search algorithm and identified 28 peer-reviewed articles published between January 1967 and July 2019 involving military personnel. We classified the findings from these studies into three categories. These categories included descriptive studies of caffeine use, studies evaluating the association between caffeinated products and sleep or functioning measures, and clinical trials assessing the effects of caffeinated products on functioning in sleep-deprived conditions. Most of the studies showed that military personnel used at least one caffeine-containing product per day during active duty and coffee was their primary source of caffeine. Their mean caffeine consumption varied from 212-285 mg/day, depending on the type of personnel and their deployment status. Those who were younger than 30 years of age preferred ED use. Caffeine use in increasing amounts was associated with decreased sleep duration and increased psychiatric symptoms. The consumption of caffeinated products during sleep deprivation improved their cognitive and behavioral outcomes and physical performance. Caffeine and energy drink consumption may maintain some aspects of performance stemming from insufficient sleep in deployed personnel, but excessive use may have adverse consequences.
Keywords: Caffeine, Energy Drinks, Sleep Disturbances, Insomnia, Military
Introduction:
Stressors in the military are often both physical and neuropsychological in nature. These inconveniences may contribute to high rates of insufficient sleep duration and insomnia-related symptoms. For instance, in a military sleep disorders center, 8.9% of the respondents met the criteria for behaviorally induced insufficient sleep syndrome, and 41.8% reported a habitual sleep duration of ≤ 5hours per night (Mysliwiec et al., 2013). Surveys have demonstrated a mean sleep duration of 5.6 hours per day in personnel deployed in support of Operation Iraqi Freedom (United States Headquarters, 2013), and 5.8 hours in redeployed personnel (Luxton et al., 2011), in contrast to the recommended 7 hours of sleep (Watson et al., 2015). A study in U.S Navy Sailors found that 80.4% of the population were poor sleepers on subjective assessment and with a mean duration of 3.3h to 6 hrs of sleep on actigraphy (Matsangas and Shattuck, 2020). Around 87% of those sailors split their sleep over 1.5 episodes per day. Though such a rest-activity pattern is a recommended strategy for optimizing sleep in a 24/7 functioning environment, achieving 8hr of sleep per day may not be feasible as observed on an objective assessment of cadets in a training environment (Bernhardt et al., 2019). Insufficient sleep duration and insomnia in such situations may lead to neurocognitive and psychomotor impairment in overall functioning of military personnel, especially during their deployments.
Stimulant use is a countermeasure for fatigue in specific operational environments, and it’s use has been prevalent among military populations across the world. A historical example is the use of amphetamine and methamphetamine as performance enhancers during World War II by the allied and axis armies (Defalque and Wright, 2011; Rasmussen, 2011; Snyder, 1973). These agents are used less frequently nowadays because of possible adverse effects such as psychosis (Ellinwood et al., 1973; Snyder, 1973) and poor judgment (Caldwell et al., 2000; Somogyi, 2010). A more common psychostimulant drug used by military personnel these days is caffeine, which is comparable to the widespread caffeine use in society (Somogyi, 2010) . Caffeine is a natural product obtained from coffee, tea, cocoa, and guarana, and is indigenously grown in South America (Somogyi, 2010). It is commonly consumed in a beverage form, e.g., coffee, energy drinks (EDs) or energy shots, caffeine gum, or a concentrated pill form. Its use in the military is prevalent because of its widespread availability and acceptability. Caffeine is served with meals in the form of coffee, whereas caffeinated EDs are also part of their meals, supplied with rations, or available for purchase. Military rations may also include caffeine gum.
In addition to the traditional means of caffeine consumption through coffee use, there are newer trends involving the use of Energy Drinks (EDs). Manufacturers are aggressively marketing EDs for young adults, the largest demographic of military personnel, as a source of instant energy (Lieberman et al., 2012) with purported active ingredients including a varying combination of caffeine, vitamins, taurine, guarana, tyrosine, kola nut, Yerba mate, and other herbal supplements (Somogyi, 2010). Producers may provide these beverages in more substantial serving portions of 16-20 oz., in contrast to the 12 oz. serving size for soft drinks and coffee. Thus, it is not surprising that, after multi-vitamins, EDs are the next most common source of dietary supplements in adolescents and young adults in the U.S (Campbell et al., 2013; Simon, 2007).
There is a recent comprehensive institutional report addressing the management of sleep health in the specialized population of U.S service members (Troxel et al., 2015). However, this report highlighted the effect of caffeine use on sleep to a very limited extent. The current review aims to provide a comprehensive view of caffeine and ED use among military personnel in the context of their sleep and functioning. Understanding the epidemiology of higher caffeine consumption in the context of sleep among military personnel is an essential next step to improve the health of our military personnel. Our primary aim was to evaluate whether caffeinated products are associated with sleep-related complaints of insomnia and sleep duration abnormalities. Our secondary aim was to determine whether caffeine supplementation improved cognitive, psychomotor, and physical functioning under sleep deprivation that mimics operational deployment. The review will educate the military community on the impact of excess caffeine use on sleep health and related consequences and the utility of caffeine use in sleep-deprived operational conditions.
Methods:
We conducted this review based on the methodological framework for scoping reviews as specified by Arksey and O’Malley (Arksey and O’Malley, 2005), and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines for scoping reviews (Tricco et al., 2018). We used two databases, PUBMED and SCOPUS, and utilized the search algorithm specified in Figure 1. PUBMED was considered the primary database and SCOPUS the secondary database for the manuscript search process. The primary inclusion criteria included the following: 1) peer-reviewed studies based on military population; 2) self-reported use of caffeine or energy drinks primarily at the time of military service; 3) subjective or objective assessments of sleep disturbances; and 4) articles published in the English language. We also conducted a retrospective bibliographic review of selected manuscripts to identify any study missed by the initial search process. We limited the search to peer-reviewed manuscripts published between January 1967 and July 2019, Figure 1. The initial search yielded 123 articles. We then excluded review articles, institutional reports, case reports, commentaries, opinions, animal-based studies, and manuscripts in a language other than English. We also excluded studies involving caffeine and energy drinks that did not evaluate sleep measures as an outcome since we focused explicitly on the ramifications of caffeine on sleep disorders and related daytime dysfunction symptoms in the military population. We excluded a study conducted at a military center despite meeting the selection criteria due to the lack of clear demographic information on the personnel’s military enlistment status.
Figure 1:
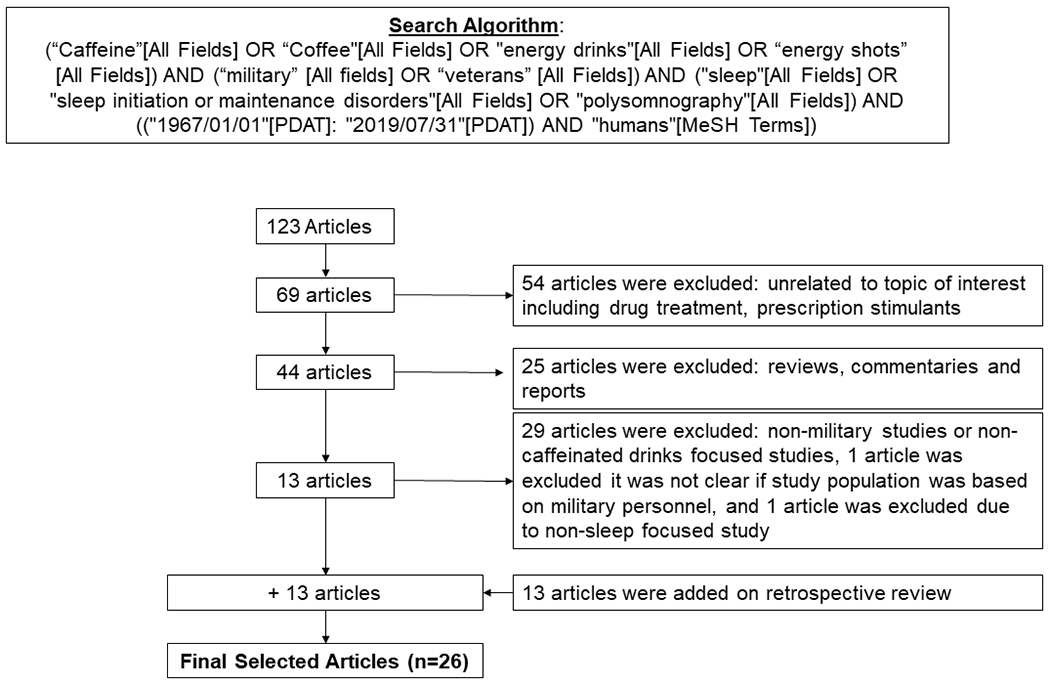
Illustration of Manuscript Selection Process for the review
We classified the identified studies into three groups based on the investigations’ nature, and they included the following: descriptive studies, association studies, and clinical trials. Furthermore, we assessed these studies for bias using the “Quality Assessment Tool for Quantitative Studies” developed by the Effective Public Health Practice Project (EPHPP), Supplementary Table 1. Our descriptive studies elaborated on the studies that reported the prevalence and pattern of caffeine use and gathered data on socio-demographic characteristics, sleep, and other pertinent clinical information. Our association studies included investigations that evaluated the relationship between caffeine use and sleep as one of the primary outcomes of interest. The clinical trials included randomized, placebo-controlled studies with a parallel assignment or a crossover trial involving different caffeine doses and placebo. These clinical trials investigated the effect of caffeine-based interventions on cognition and performance in military personnel under sleep-deprived conditions.
Results:
A total of 26 studies evaluated caffeine use in the US military population, Figure 1. The bias assessment score for these studies is provided in Supplemental Table 1 (Effective Public Health Practice Project, 1998). Overall, most of the studies were biased and had weak to moderate scores. One study from the association studies group and two studies from the experimental studies group had a low bias and were rated as the strong studies on the scale. Studies that primarily investigated caffeine use included all their available sources (such as coffee, ED, and nutritional supplements), whereas studies that examined ED use as their source of caffeine focused on energy drinks and soda. The caffeine consumption (coffee and other caffeine supplements or ED use), was self-reported within the observational studies in Table 1 and Table 2 whereas the clinical trials administered prespecified caffeine doses to the participants in Table 3.
Table 1:
Cross-sectional Descriptive Studies evaluating the use of caffeinated products in the military population
| First Author (Year) | Data Source/Study population | Goals | Measurement/Scales | Findings |
|---|---|---|---|---|
| Schmidt et al(2008) | A random sample of active-duty members (N=377) | To determine the prevalence of energy – drink and Supplement Usage | Online Survey | *About 61% used ED usage with *30% or more had ≥1 drink per week,5% reported daily consumption *ED users were more likely to endorse increased mental alertness (77.3%), and better physical endurance (35.2%). *ED users were more likely to complain of difficulty falling asleep (30.9%), and difficulty staying asleep (10.9%) |
| Boos et al (2011) | Voluntary British military personnel attending a health promotion fair while in Afghanistan (n=87) | To assess whether previous studies done on use of dietary supplements such as caffeine were still applicable | Questionnaire on dietary and exercise supplements, as well as duration of use and sources of these supplements. | *46% of the respondents consumed caffeinated drinks per day *37.9% of participants drank 6 or more caffeinated drinks a day |
| Stephens et al(2013) (Stephens et al., 2014) |
A random sample of US military personnel (N=586) | To assess the prevalence and effects of ED and energy shot use | 30-item electronic questionnaire on ED and caffeine intake use | *≥53% consumed an ED in the past month *≥19% had ≥1 energy shot in the past month *19% consumed a beverage where ED mixed was mixed with alcohol in the past month *Younger respondents (18-29 years) were more likely to use ≥1 ED drinking per week *The most common reasons for use were to improve mental alertness (61%), mental (29%) and physical (20%) endurance. *The common side effects to use were an increased pulse rate or palpitations, restlessness, and difficulty sleeping. |
| Knapnik et al (2016) | A random Sample of Navy and Marine Corps Personnel (N=1,708) | To examine the characteristics associated with caffeine consumption | Self-reported questionnaire | *87% reported using caffeinated products ≥1 time/week, *their mean ± SE daily caffeine use was 226 ± 5 mg *men consumed more caffeine than women (242 ± 7 mg/day versus 183 ± 8 mg/day) *Reported sleep duration was inversely associated with caffeine consumption. |
| Knapnik et al (2016) | Active-duty Air Force personnel from 10 US and 2 overseas installations (2010-2011, N=1,787) | To examine prevalence, daily consumption, and related characteristics of caffeine use in Air Force personnel. | Self-reported survey | *84% consumed caffeinated products ≥1 time/week. *Mean± SE of caffeine consumption was 212 ± 9 mg/day (224 ± 11 mg/day for men, 180 ± 12 mg/day for women). *Caffeine use was associated with older age, non-Blacks, and lower sleep duration. *ED use was associated with male gender, younger age, and decreased sleep duration. |
| Attipoe et al (2018) | A convenience sample of US military members (N=1,706) | To describe the prevalence of ED or Energy Shot (ES) use, and their related side-effects | An online as well as paper based self-reported survey | *50% reported ED/ES use ≥ once a month *33% used ED/ES in combination with alcohol *Young, male, enlisted service personnel were more likely to use ED/ES than others *Army personnel were more likely to use ED or ED with alcohol, than other branches. * Their reasons for ED or ES for reasons for use were to, “boost energy” (77%), and “enhance mental alertness” (52% and 57%). *13% reported adverse effects from their use. *Reasons for cessation of use were price (8%), bad taste (3% and 6%), upset stomach (2% and 3%), and inability to boost energy (2% and 4%). |
| Kullen et al (2019) | A convenience sample of Australian Army personnel (n=667) | To examine prevalence and type of dietary supplements (DS) used, including caffeine | Questionnaire on dietary supplements and reasons for use | * Caffeine was the most commonly used DS used daily (48.4%). *The most common reasons for use were “to provide energy” and “performance” |
Legend: ED = Energy Drinks; ES= Energy Shorts; US = United States; DS = Dietary Supplements; SE = Standard Error; All studies are cross-sectional.
Table 2:
Observational Studies measuring associations between caffeinated products and sleep and related characteristics
| First Author (Year) | Data Source/Study population | Goals | Measurement/Scales | Findings |
|---|---|---|---|---|
| CDC (2012) | A random cluster sample of US Service Members on a combat deployment to Afghanistan (N=1,249) | To determine the association between ED consumption and sleep measures | Questions on sleep and ED use embedded within the Deployment Well-Being Survey of the Joint Mental Health Advisory Team (JMHAT) 7. | *About 45% drank ≥1, and 13.9% drank ≥3 ED per day. *Among those who slept 3-4 hrs./ night: - 38.2% drank ≥3 drinks/day, - 18.4% drank 1-2 drinks/day, and - 23.9% abstained from caffeine. * Disrupted sleep > 50% of the nights was related to higher ED use and psychological stress or illness |
| Jacobson et al (2012) | Millennium Cohort Longitudinal Study (2007-2008, N=106,698) | To determine association between deployment experience, physical activity, and use of body building, energy or weight loss supplements | Self-reported data from the Millennium Cohort Study, collected between 2007-2008. | *About 46.7% of the participants had used ≥1 type of supplements. * 22.0% used multiple supplements. *Deployed males preferred bodybuilding supplements, whereas females preferred weight-loss supplements. *Physically active and younger subjects reported all types of supplement use. *Sleep duration ≤5 hours a night was linked to the use of energy supplements. |
| Waits et al(2014) | A random sample of service members deployed in Afghanistan 2010-2011 | To quantify the sleep habits and energy products use among deployed service personnel. | A survey questionnaire created by the authors and incorporating the Combat Exposure Scale, and the Insomnia Symptom Questionnaire. | *Insomnia was prevalent in 83% of them; *28% were using prescription or over-the-counter sleep aids *81% consumed ≥1 energy product daily. *Use of energy products increased during deployment *There was no relationship between insomnia and the quantity of energy products used. |
| Matsangas et al (2018) | A sample of US Navy personnel on an aircraft carrier (N=767) | To assess fatigue and sleepiness as a result of working at sea. | A retrospective survey involving data from their semi-annual physical fitness assessment measures, Epworth Sleepiness Scale, and Fatigue Severity Scale. | *The mean±SD sleep duration was 6.12 ± 1.10 hours, and 70% slept <7 hours/day. *Those who were fatigued and sleepy consumed more caffeine than those who were non-fatigued/non-sleepy, and fatigued/non-sleepy. |
| McLean et al (2017) | A sample of active duty military personnel seeking treatment for PTSD after deployment to Iraq or Afghanistan (N=366) | To examine the relationship between caffeine consumption, sleep disturbances, and PTSD symptoms. | A general health Interview, Insomnia Severity Index, Self-Assessment of Sleep, Epworth Sleepiness Scale, and PTSD Symptom-Scale Interview. | *A higher caffeine use was associated with lower insomnia symptom severity, although insomnia severity was elevated in those who reported no caffeine use. *Caffeine use was not associated with any other sleep disturbance measures or PTSD symptoms. |
| Shattuck et al (2017) | A sample of US Navy crew members stationed on an aircraft carrier (n=82) | To evaluate the association between actigraphic sleep duration and caffeinated beverage consumption and other variable. | Daily log including activity, caffeine consumption, and exposure to sunlight, Epworth Sleepiness Scale score, and actigraphy, over a 12-day period. | *Their mean actigraphic sleep duration was 6.64±0.95 hours *About 96% of crewmembers reported daily use of a caffeinated beverage *Sleep duration was inversely associated with the number of caffeinated drinks consumed in a bivariate, as well as a multivariable model. |
| McLellan et al (2018) | Data from two independent surveys administered in Afghanistan. Survey # 1 involved U.S. Army combat soldiers (JMHAT-8, N=518). Survey # 2 involved soldiers deployed with different military assignments (USARIEM, N=260). | To estimate the caffeine consumption, and to examine the relationship between caffeine consumption and sleep quality, combat activities and measures of operational stress, in the combat theater. | The MHAT-8 survey questions included in this study included their demographic data, caffeine consumption, required sleep duration, and reported sleep duration. The USAREIM Deployment Survey also collected demographic data, caffeine consumption, and sleep duration. | *The mean daily caffeine intake in the J-MHAT 8 survey was 404 ± 18 mg, and 80% consumed caffeinated products. *In the JMHAT-8 survey, higher caffeine use was linked to disruptions in their sleep environment, operation tempo, and trouble falling or staying asleep during the day after night operations. *A higher caffeine intake was not associated with DFA, DSA, EMA, trouble waking up, or with being sleep deprived.. *In the USARIEM Deployment survey, intake was 303 ± 29 mg *Caffeine use was significantly higher among combat arms soldiers, than in the combat service support personnel. *Soldiers who slept ≤4 hrs used more caffeine than those who slept >6 hrs. |
| Toblin et al (2018) | A random sample of active duty U.S Army Soldiers who returned from a 12-month combat deployment to Afghanistan (N=627) | To quantify the prevalence of ED use. The study also examined the association between ED use and post-deployment insomnia, and other mental health problems. | Self-reported survey that collected data on ED use, insomnia (ISI), PCL, PHQ-9, GAD-7, and AUDIT-C scales | *The prevalence of ED use was 75.7%, with 29.2% reporting daily use, and 16.7% consuming high levels of ED (≥2/day) *When compared to low frequency of use, high frequency of ED users were more likely to complain of insomnia and alcohol misuse. |
Legend: ED = Energy Drinks; JMHAT = Joint Mental Health Advisory Team; DFSA = Difficulty Falling Asleep; DSA = Difficulty Staying Asleep; EMA = Early Morning Awakening; hrs = hours; PCL = PTSD check list; PHQ-9 = 9-item Patient Health Questionnaire; GAD-7 = 7-item Generalized Anxiety Disorder Scale; UDIT-C = 3-item version of the Alcohol Use Disorder Identification Test;
Only study with longitudinal study design. All other studies are cross-sectional.
Table 3:
Experimental Studies measuring the relationship between caffeine use and cognitive, behavioral and sleep measures
| First Author (Year) | Study Design | Study population | Goals | Measurement/Scales | Findings |
|---|---|---|---|---|---|
| Lieberman et al (2002) | A randomized placebo-controlled trial of caffeine. | Navy SEAL volunteers (N=68) randomly assigned to 100, 200, or 300 mg caffeine or placebo capsules | To examine whether moderate doses of caffeine reduce adverse effects of 72-hour sleep deprivation | *Neurocognitive battery to assess visual vigilance, reaction time, memory task, and self -reported fatigue and mood | * Higher doses of caffeine (200 or 300 mg doses) reduced sleepiness, fatigue, visual vigilance and reaction time. |
| Tharion et al (2003) | A randomized trial comparing caffeine, or placebo | Male Navy SEAL trainee volunteers (N=62) who used caffeine 100, 200, or 300 mg of caffeine or placebo | To evaluate the effect of caffeine at different doses to minimize performance deficits after sleep deprivation | *Marksmanship measures of sighting time, and accuracy | * When compared to placebo or 100 mg dose of caffeine, caffeine 200 and 300 mg improved their sighting time * Caffeine at any dose did not improve accuracy between these groups. |
| McLellan et al (2004) | A double-blind trial comparing caffeine and placebo | * Volunteer soldiers(N=16) * 400mg of caffeine at 21:30 followed by 2 doses of 100mg doses at 03:00 and 05:00. |
To investigate the effect of caffeine use on overnight military activity after a period of sleep loss | *Sandbag piling task * Time to exhaustion |
* Caffeine use reduced the time to complete the sandbag piling task in session 1 only, and not session 2 *Caffeine use improved the time to exhaustion by 25%, Vs placebo. |
| Tikuisis et al (2004) | A double-blind trial of caffeine and placebo | Volunteer soldiers (N=20), ingested 400, 300 and 100 mg of drug, 7.5, 3, or 0 hours before shooting | To appraise the efficacy of caffeine on improving performance after 22 hours of wakefulness | *Target engagement time *Number of shots fired *Accuracy *Precision |
*Caffeine restored the target engagement time, as compared to placebo; *Caffeine relatively improved the number of shots fired; * Caffeine did not improve any other measure. |
| McLellan et al (2005) (McLellan et al., 2005a) |
A randomized, placebo-controlled, double-blind trial of caffeine for performance during an urban warfare situation | Volunteer Soldiers (N=30), randomized to caffeine 600mg (N=15), or placebo (N=15). On night 1 they slept for 3 hours and stayed awake overnight in Night 2, till 11:00 on Day 3. Caffeine/placebo dose was given at 21:45 (100mg), 23:45 (200mg), 1:45 (100mg), and 3:45 (200mg). | To study the effect of caffeine on physical and cognitive performance during a 55-hour period of training operation that involved insufficient sleep | *PVT (Reaction time, major lapses) *5-km run *Marksmanship task *Urban Operation Vigilance Task |
*Reaction time was maintained with caffeine use on Day 3 * Minor lapses increased in the placebo group on Day 3 compared to the caffeine group that remained steady all through out *Marksmanship scores during sleep deprivation showed no marked change with caffeine use but decreased in the placebo group *Caffeine retained the Urban Operation Vigilance Task performance in the second session at 6:00, but not at 02:00. *5-km run did not show any between-group difference |
| McLellan et al (2005) (McLellan et al., 2005b) |
A randomized, placebo-controlled trial of caffeine | Special Forces Personnel (N=31), randomized to 200 mg of caffeine (N=16) or placebo (N=15). Day 1 had a 6.3-km run; on Day 2 they did an ORVT task in the field; on Day 3, after overnight sleep deprivation, ORVT done twice between 02:00 and 06:00. | To explore the effect of caffeine on vigilance, marksmanship, and run performance during 27 hours of sustained wakefulness | *PVT (Reaction time, major lapses) *Observation and Reconnaissance Vigilance Task (ORVT) *Marksmanship task |
*Caffeine use improved the Reaction Time on Day 3 starting 3:40 *Caffeine group had significantly fewer lapses * No difference in the run-time between groups, after sleep deprivation * No difference between groups on accuracy, target engagement time or response time scores (marksmanship) |
| Lohi et al (2007) | A double blind, placebo controlled trial of caffeine on flight performance in a simulator | Volunteer Finnish military pilot students on 200 mg of caffeine (N=7) or placebo (N=6) administered before 4 flight sessions (average of 24-33 minutes), performed between days 1-2 at 09:00-12:00, 18:30-21:30, 02:00-05:00, and 09:00-12:00. | To examine the effect of caffeine consumption on simulated flight performance during 37 hours of sleep deprivation | *Instructor score for overall flight performance on a scale from 1 to 5 *Instructor evaluation on a visual analog scale (VAS) *Self-evaluation of flight performance |
*The scores given by the instructor did not differ between either treatment group *No difference in self-reported scores recorded by the pilots in either group *After about 20 hours of sleep deprivation, a non-significant trend was seen for those treated with caffeine to rate their overall flight performance to be better than their first and second flight sessions. |
|
McLellan et al (2007) (McLellan et al., 2005b) |
A randomized study comparing caffeine to placebo | Male Special Forces Personnel given 200mg of caffeine (N=10) or placebo (N=10), between 0100, 0345, 0700, and 21:45. They slept for 4 hours on nights 3 and 4. | To investigate whether caffeine given during multiple nights of wakefulness could maintain physical functioning despite partial sleep deprivation | *Vigilance task *Obstacle tasks |
*Caffeine use improved vigilance scores, when compared to placebo, on days 3-5 *The total run time on caffeine during day 3 was faster on caffeine than on placebo. The run time decreased on days 4 and 5 for both groups. |
| Kilpelainen et al (2010) | A double-blind randomized trial of 200 mg caffeine or placebo | A sample of young Finnish male, military pilot students (n=15), randomized to 200 mg pf caffeine (N=7), or placebo (N=8), four times before each simulator session | Does a moderate caffeine dose prevent decrements in mood, motivation and task performance after 37-hour sleep deprivation | *Sustained Attention Task (Clock Test) * Learning Task (learning Japanese) * POMS (mood) * Motivation (VAS) |
*Sustained attention did not differ between the caffeine or placebo groups *No between-group difference in the Learning Task * Relative to placebo, caffeine prevented a deterioration of their mood symptoms |
| Newman et al (2013) | A double blind placebo-controlled cross-over study, involving 100 mg of caffeine or placebo. | Healthy, active-duty military personnel (N=15). Lights were switched off at 00:00, and woken at 01:00 to complete PVT, and then awakened again at 06:00 to do the PVT. | To explore the effect of caffeine during sleep inertia on PVT done at 0, 6, 12, and 18 min. post--awakening after sleeping for 1 and 6 hrs. | * speed of responses on PVT *number of lapses on PVT |
*At 1:00, the caffeine group maintained better speed increased at 12 and 18 min and lower lapses at 18 min. *At 6:00, the caffeine group showed improved speed at 18 min decreased lapses at 12 and 18 minutes |
| Kamimori et al (2015) | A randomized, double-blind, placebo-controlled trial of caffeine | Healthy male volunteers from special forces (N=20). Subjects were given placebo or caffeine 100 mg every 4 hours (total ≤800 mg). | To examine the efficacy of repeated 200mg caffeine doses on functioning after being awake for 3 nights and 4-h afternoon naps. | *PVT *Logical Reasoning test (LRT) *Field Vigilance Task (FVT) *Marksmanship test *Vigilance monitor (VM) |
*Caffeine use improved their: *reaction time (PVT), *improved event detection (FVT), *improved # of correct responses (VM), *speed of response (LRT). |
Legend: PVT = Psychomotor Vigilance Task, POMS = Profile of Mood States; VAS = Visual Analog Scale;
Demographic characteristics.
Most active-duty personnel (84%) used at least one caffeinated product each day (Knapik et al., 2016), Table 1. Two studies that described the consumption patterns across different military branches found that the mean consumption varied from 212 mg/day among Air Force Personnel to 285mg/day in active-duty US Army Soldiers (Knapik et al., 2017; Knapik et al., 2016). A self-administered survey during deployment in Afghanistan found that deployed personnel reported higher caffeine consumption, while soldiers in the combat zone had the highest consumption (McLellan et al., 2018). In these observational studies, the primary sources of caffeine varied by type and age of military personnel. The primary sources of caffeine were coffee (45 to 56%), caffeinated sodas (43 to 56%), cola-type beverages (54%), energy beverages (27-39%), and energy drinks (27 to 38%) (Knapik et al., 2017). Those who were 40 years or older reported a higher prevalence of coffee use as a primary source. In comparison, younger active-duty members of both military and Air Force personnel reported higher ED consumption within the age group categories of 18-25 and 25-29 years (Attipoe et al., 2018; Centers for Disease Control Prevention, 2012; Knapik et al., 2017). Other demographic characteristics that were associated with higher caffeine consumption included male gender, Non-Hispanic White race, and a high school education level or less. One study that compared soldiers deployed with different military assignments found that service members deployed in combat had a higher daily caffeine intake than deployed service-support personnel (McLellan et al., 2018). There was no difference by service rank or special operations status in any of these cross-sectional studies (Knapik et al., 2017; Knapik et al., 2016; McLellan et al., 2018), Tables 1 and 2.
The two studies that specifically assessed the use of EDs or energy supplements (ESs) found that EDs were the preferred means of caffeine consumption in about two-thirds of military personnel younger than 30 (Attipoe et al., 2018; Toblin et al., 2018), Tables 1 and 2. Attipoe and colleagues found that up to 50% of service members reported using ED at least once a month using a convenience sample of 1,706 military (Attipoe et al., 2018). In a random cluster of 1,249 Operation Enduring Freedom personnel deployed to Afghanistan, 45% of the respondents reported consuming more than 1 ED daily, whereas 14% drank three or more EDs per day (Centers for Disease Control Prevention, 2012). This estimate contrasted with the data collected online from 377 active duty Air Force personnel stationed within the United States, where 30.5% reported consuming one or more energy drinks a week, and 5.57% of them reported daily consumption (Schmidt, 2008). The easy access to EDs in vending machines, dedicated vending machines, and immediate access in work-related areas facilitated their ED consumption (Schmidt, 2008). Three studies reported that the main reasons for ED use were to increase mental alertness and mental endurance (Attipoe et al., 2018; Schmidt, 2008; Stephens et al., 2014). However, none of the studies found an association between ED use and aerobic or strength training (Knapik et al., 2017).
Sleep characteristics in ED users:
Data from the Millennium Cohort Study has shown that energy supplement users were more likely to report difficulty sleeping and sleep ≤ 6 hours per day (Jacobson et al., 2012). In a survey of active duty Air Force personnel, 30.8% reported difficulty falling asleep, and 10.8% reported trouble staying asleep as common adverse effects linked to the consumption of EDs (Schmidt, 2008). Compared to those with a lower energy drink consumption, personnel with higher energy drink consumption were more likely to fall asleep in briefings and on guard duty on a deployment in Afghanistan (Centers for Disease Control Prevention, 2012). The use of EDs use among troops who returned from a 12-month combat deployment has also been associated with mental health problems, aggression, and fatigue in a study on a random sample of active-duty U.S Army Soldiers (Toblin et al., 2018). In a recent survey among personnel deployed in combat, those who drank more than 3 EDs per day represented 38.2% of the respondents who slept for about 4 hours each day, and they complained of disrupted sleep on more than half the nights over the last month (Centers for Disease Control Prevention, 2012).
Sleep and functioning characteristics with caffeine use in clinical trials
Prior studies in the military population have mainly investigated caffeine’s impact on functioning after sleep deprivation and on their subsequent recovery sleep (Kamimori et al., 2015; Kilpelainen AA, 2010; Tikuisis et al., 2004), Table 3. We have summarized these findings in the below-mentioned categories:
a) Sleep deprivation & Sleepiness:
A few clinical trials listed in Table 3 showed that caffeine intake in the dose range of 100-800 mg improved cognitive functioning, such as vigilance learning, mood, and memory (Kamimori et al., 2015; Lieberman et al., 2002), improved target detection (Tikuisis et al., 2004), maintained alertness (McLellan et al., 2004), and conserved sustained vigilance after overnight sleep deprivation (McLellan et al., 2005a; McLellan et al., 2007). Caffeine use also prevented compromises in sighting and accuracy involving male Navy SEAL trainees in a randomized trial comparing caffeine and placebo (Tharion et al., 2003). However, one study failed to demonstrate a difference between caffeine and placebo on the vigilance test after 37 hours of sleep deprivation (Kilpelainen AA, 2010).
In addition to improved cognitive functioning, these randomized trials also found that caffeine use improved the military personnels’ behavioral outcomes and physical performance during sleep deprivation. These behavioral improvements included vigilance task (Kamimori et al., 2015) and sustained psychomotor performance in male special forces (McLellan et al., 2005b), and also maintained their physical performance after sleep deprivation (McLellan et al., 2004; McLellan et al., 2005a; McLellan et al., 2007). Furthermore, caffeine consumption decreased the sleep inertia after 1 or 6 hours of sleep in a double-blind, placebo-controlled crossover study of healthy, active-duty military personnel (Newman et al., 2013). However, two studies failed to demonstrate the beneficial effects of caffeine on sleep deprivation, such as the lack of an improvement in marksmanship performance (Tikuisis et al., 2004) or their ability to fly after 37 hours of sleep deprivation (Lohi et al., 2007). Thus, caffeine use may improve or sustain cognitive and behavioral outcomes during acute and subacute sleep deprivation. Two studies also demonstrated that caffeine-treated subjects underestimated their flight performance deficits after sleep deprivation(Kilpelainen AA, 2010; Lohi et al., 2007).
b) Insomnia:
High caffeine use was associated with lower insomnia severity and was not linked with other measures of sleep disturbance or with PTSD symptoms in a study on active duty members seeking treatment for PTSD after their deployments (McLean et al., 2017), Table 2. One study found that only the degree of combat (and not the consumption of energy products) predicted their degree of insomnia (Waits et al., 2014), Table 2. Conversely, another study involving active-duty members found that ED users were also more likely to complain about insomnia and alcohol misuse (Toblin et al., 2018).
Discussion:
The current report reviewed the caffeine and energy drink (ED) use in the military population and its relationship with sleep characteristics. We found that the service personnel had caffeine consumption within a range of 212-285 mg/day. The predominant means of caffeine consumption was coffee in older military personnel, whereas ED use was more common among the younger military personnel (Knapik et al., 2017; Knapik et al., 2016). Observational studies showed that caffeine consumption was associated with insomnia symptoms and decreased sleep duration. Moreover, ED use was also associated with fatigue, aggression, and suicidal ideation. The placebo-controlled clinical trials showed that caffeine use improved the military personnel’s cognitive and behavioral outcomes and improved their physical performance during sleep deprivation.
The mean daily caffeine consumption reported herein was higher in military personnel than in the civilian populations (Chaudhary et al., 2016; Knapik et al., 2017; Knapik et al., 2016), but the demographic characteristics linked to caffeine or ED use in this population were similar to those seen in the general population. Recent estimates have shown that 58% of young adults between the ages of 18-25 who presented to the Emergency Department reported the use of EDs in the past month, similar to estimates observed in active duty members (Cotter et al., 2013). Men consistently had higher ED consumption rates than women in the military and civilian populations (Reissig et al., 2009; West et al., 2006). ED use varied by racial group and was more common in blacks and hispanic subjects (Wells et al., 2013). In parallel to the military community, police officers showed a higher caffeine intake to stay awake, and this use was independently associated with increased odds of errors, stress, and burnout (Ogeil et al., 2018). These similarities suggest that the community-level interventions designed in the general population need to be evaluated within the military population.
The association between higher consumption of caffeine or ED use and low sleep duration was consistent across all the observational studies. However, the association between caffeine or ED use and sleep disturbances was inconsistent. Waits et al. found that the lack of an association between ED use and insomnia was accounted for by the severity of insomnia (Waits et al., 2014). The severity of insomnia among non-caffeine users was higher than caffeine users, leading to a non-significant relationship between ED use and insomnia. McLean et al. accordingly suggested that a non-significant association between caffeine use and sleep measures in their study among personnel seeking treatment for PTSD may have been secondary to a lower caffeine use in those with PTSD symptoms to avoid anxiety attacks (McLean et al., 2017). Moreover, most of the data on caffeine consumption and sleep measured collected in the studies is self-reported and cross-sectional and does not consider daily variability in both measures. Since many military personnel work in environments involving higher psychosocial stress levels, future studies should also use objective methods to characterize the variations in caffeine consumption and sleep patterns to help us improve our understanding of these relationships.
There was no consensus across clinical trials on the effect of higher doses of caffeine on improving neurocognitive performance, marksmanship, and vigilance tasks after sleep deprivation. Multiple state and trait-based reasons may explain the lack of such a consensus. The environment (training vs. simulated) under which the experiments were conducted could have affected the pattern of wakefulness and performance intent. It may have been a state-based reason for the discrepancy in the results. Moreover, studies that ascertained caffeine ingestion time or had multiple dosages of caffeine observed improvement in these measures (Lieberman et al., 2002; McLellan et al., 2007). Some of the trait-based reasons may include the differences in susceptibility to the effects of sleep deprivation and the variability in caffeine metabolism. The susceptibility to the effects of sleep deprivation is a heritable trait, with different people showing a varying level of impairment (Nunes et al., 2017). It is possible that caffeine consumption differentially improved performance in individuals who were more susceptible to the effects of sleep deprivation. It is also possible that the persistence of a higher concentration of caffeine in the system secondary to lower caffeine metabolism resulted in an improved neurocognitive performance at the time of these activities. Individuals with high CYPA2 enzyme activity may require higher doses of caffeine to achieve the same level of performance compared to those with low enzyme activity (Kilpelainen AA, 2010; Rasmussen et al., 2002). While measurements of urinary metabolites of caffeine will address this issue in future experiments, these factors need to be kept in mind while evaluating the relationships between caffeine use and sleep deprivation.
Despite these biases and improved performance, we should keep in mind caffeine’s deleterious effect on sleep. On a short-term basis, caffeine consumption may increase night-time worrying and sleep continuity-related abnormalities (Omvik et al., 2007). Some of these abnormalities include increased sleep latency, decreased stages 2 and 4 of Non-Rapid Eye Movement Sleep, brief arousals from sleep, reduced sleep duration and a decrease in sleep efficiency (which is the time in bed that spent sleeping) (Chaudhary et al., 2016; Shilo et al., 2002; Watson et al., 2016). These effects are prominent on the first day of consumption (Keenan et al., 2014). Strong associations also exist on the co-occurrence of psychological distress and disturbed affect in conjunction with disturbed sleep (Ogeil and Phillips, 2015). A study evaluating adult Americans demonstrated that when sleep duration decreased, the relationship between increased caffeine consumption and non-restorative sleep became stronger (Kozak PJ, 2011).
After an extended period of sleep restriction, the onset of acute recovery sleep may be a function of the high sleep pressure, secondary to increased homeostatic activity (Borbely et al., 2016). This recovery sleep may improve the neurocognitive performance to the baseline. Beyond the phase of acute recovery sleep, continuous caffeine use may trigger a circadian wake-promoting signal during daytime and lead to fragmented sleep affecting complete recovery (Banks et al., 2010; Carrier et al., 2009). Given that service members are a population at high risk for insufficient sleep duration and its effects on subsequent sleep recovery, these findings suggest that caffeine may play a role in impairing restorative sleep among service members.
Most of the studies in our review were designed using convenience samples from available military personnel during their active-duty or combat-related activities. These studies are not comparable to traditional population-based studies for which bias risk assessment tools are available. Accordingly, most of our studies had scores of weak to moderate on our assessments and indicates to medium to high risk of bias. Such an approach itself indicates selection bias and a non-representative military cohort but it also raises a question on the most feasible way to gather data on this important sub-population. Future studies should consider effective strategies to gather data from a representative active-duty sample. A future direction of research may involve the use of caffeinated alcoholic beverages and their effect on sleep and next-day functioning in military personnel. Despite the ban on pre-mixed caffeinated alcoholic drinks, the intake of consumer-mixed alcohol with EDs is a more disturbing trend than ED use alone. Alcohol is a commonly used substance among military personnel along with caffeinated beverages with a growing trend of use of caffeinated beverages along with alcohol in a younger military population (Manchester et al., 2017; Stephens et al., 2014). The use of caffeinated beverages with alcohol use is associated with adverse alcohol-related consequences including sleep disorders ((Drake et al., 2003; McKetin et al., 2015). We did not find any study that examined the effect of caffeinated alcoholic drinks on sleep. Only one study examined the combined role of alcohol use and energy drink use in the U.S Army (Mash et al., 2014). The study observed that soldiers who reported daily alcohol and energy drink use were three times more likely to have reported suicidal ideation or attempts. Heavy use of energy drinks alone during combat deployment has been associated with psychiatric problems, aggressive behaviors, and fatigue, despite caffeine being a countermeasure for fatigue (Toblin et al., 2018). Caffeine may promote higher levels of alcohol consumption by countering the hypnotic effect of alcohol, improving the reaction time even in an intoxicated state, and distorting subjective perceptions of impairment (Curry and Stasio, 2009; Mallett et al., 2014; McKetin et al., 2015; Peacock et al., 2012)). But, the existing studies in the general population suggest the relationship between alcohol mixed EDs and sleep is variable (McKetin et al., 2015; Peacock et al., 2014), and require additional investigations.
In summary, insufficient sleep still plagues military personnel and may have a chronic course with fluctuations in its intensity over time, despite the implementation of strategies to improve sleep. This insufficient sleep is further complicated by fatigue as a consequence of the expected higher levels of vigilance and performance. Caffeine use, and increasingly EDs are being used by military personnel to counter this sleepiness and fatigue. The chronic and excessive use of caffeine and EDs in the military may further lead to dependence on caffeine, insomnia, and non-restorative sleep. Such behavioral patterns of caffeine use in the presence of acute stressors places service members at heightened risk of psychiatric disorders, such as PTSD (Gehrman et al., 2013). Better sleep strategies may offset the performance issues in deployed service personnel with insufficient sleep and may decrease the need for higher caffeine consumption.
Supplementary Material
Highlights:
Military personnel report mean daily consumption of 212-285mg/day
Coffee was the primary caffeine source for military personnel over the age of 25 years, but Energy Drink use was common for those 25 years of age and younger
Energy Drink use was associated with sleep disturbances.
Caffeine/ED use had beneficial effects on performance after prolonged sleep deprivation.
Acknowledgement
The content of this publication do not represent the views of the Department of Veterans Affairs, University of Pennsylvania, the United States Government, or other participating institutions
Funding:
This work was supported by the following grants: VA - 1IK2CX000855 (S.C.); 1K23HL110216 & 5R21ES022931 (M.G.); R01HL112646 (W.T.).
References:
- Arksey H, O’Malley L, 2005. Scoping studies: towards a methodological framework. International journal of social research methodology 8(1), 19–32. [Google Scholar]
- Attipoe S, Delahanty L, Stephens M, Deuster PA, 2018. Energy Beverage Use Among U.S. Service Members. Mil Med. [DOI] [PubMed] [Google Scholar]
- Banks S, Van Dongen HP, Maislin G, Dinges DF, 2010. Neurobehavioral dynamics following chronic sleep restriction: dose-response effects of one night for recovery. Sleep 33(8), 1013–1026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bernhardt KA, Kelley AM, Feltman KA, Curry IP, 2019. Rest and Activity Patterns of Army Aviators in Routine and Operational Training Environments. Aerosp Med Hum Perform 90(1), 48–52. [DOI] [PubMed] [Google Scholar]
- Borbely AA, Daan S, Wirz-Justice A, Deboer T, 2016. The two-process model of sleep regulation: a reappraisal. J Sleep Res 25(2), 131–143. [DOI] [PubMed] [Google Scholar]
- Caldwell JA Jr., Caldwell JL, Smythe NK 3rd, Hall KK, 2000. A double-blind, placebo-controlled investigation of the efficacy of modafinil for sustaining the alertness and performance of aviators: a helicopter simulator study. Psychopharmacology 150(3), 272–282. [DOI] [PubMed] [Google Scholar]
- Campbell B, Wilborn C, La Bounty P, Taylor L, Nelson MT, Greenwood M, Ziegenfuss TN, Lopez HL, Hoffman JR, Stout JR, Schmitz S, Collins R, Kalman DS, Antonio J, Kreider RB, 2013. International Society of Sports Nutrition position stand: energy drinks. J Int Soc Sports Nutr 10(1), 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carrier J, Paquet J, Fernandez-Bolanos M, Girouard L, Roy J, Selmaoui B, Filipini D, 2009. Effects of caffeine on daytime recovery sleep: A double challenge to the sleep-wake cycle in aging. Sleep Med 10(9), 1016–1024. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control Prevention, 2012. Energy drink consumption and its association with sleep problems among US service members on a combat deployment-Afghanistan, 2010. MMWR Morb Mortal Wkly Rep 61(44), 895. [PubMed] [Google Scholar]
- Chaudhary NS, Grandner MA, Jackson NJ, Chakravorty S, 2016. Caffeine consumption, insomnia, and sleep duration: Results from a nationally representative sample. Nutrition 32(11–12), 1193–1199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cotter BV, Jackson DA, Merchant RC, Babu KM, Baird JR, Nirenberg T, Linakis JG, 2013. Energy drink and other substance use among adolescent and young adult emergency department patients. Pediatr Emerg Care 29(10), 1091–1097. [DOI] [PubMed] [Google Scholar]
- Curry K, Stasio MJ, 2009. The effects of energy drinks alone and with alcohol on neuropsychological functioning. Human psychopharmacology 24(6), 473–481. [DOI] [PubMed] [Google Scholar]
- Defalque RJ, Wright AJ, 2011. Methamphetamine for Hitler’s Germany: 1937 to 1945. Bull Anesth Hist 29(2), 21–24, 32. [DOI] [PubMed] [Google Scholar]
- Effective Public Health Practice Project, 1998. Quality assessment tool for quantitative studies. https://merst.ca/ephpp/. (Accessed 20 February 2021).
- Ellinwood EH Jr., Sudilovsky A, Nelson LM, 1973. Evolving behavior in the clinical and experimental amphetamine (model) psychosis. Am J Psychiatry 130(10), 1088–1093. [DOI] [PubMed] [Google Scholar]
- Gehrman P, Seelig AD, Jacobson IG, Boyko EJ, Hooper TI, Gackstetter GD, Ulmer CS, Smith TC, 2013. Predeployment Sleep Duration and Insomnia Symptoms as Risk Factors for New-Onset Mental Health Disorders Following Military Deployment. Sleep 36(7), 1009–1018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacobson IG, Horton JL, Smith B, Wells TS, Boyko EJ, Lieberman HR, Ryan MA, Smith TC, 2012. Bodybuilding, energy, and weight-loss supplements are associated with deployment and physical activity in U.S. military personnel. Ann Epidemiol 22(5), 318–330. [DOI] [PubMed] [Google Scholar]
- Kamimori GH, McLellan TM, Tate CM, Voss DM, Niro P, Lieberman HR, 2015. Caffeine improves reaction time, vigilance and logical reasoning during extended periods with restricted opportunities for sleep. Psychopharmacology 232(12), 2031–2042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Killgore WD, Rupp TL, Grugle NL, Reichardt RM, Lipizzi EL, Balkin TJ, 2008. Effects of dextroamphetamine, caffeine and modafinil on psychomotor vigilance test performance after 44 h of continuous wakefulness. J Sleep Res 17(3), 309–321. [DOI] [PubMed] [Google Scholar]
- Kilpelainen AA HK, Lohi JJ, Lyytinen H, 2010. Effect of Caffeine on Vigilance and Cognitive Performance During Extended Wakefulness. The International Journal of Aviation Psychology 20(2), 144–159. [Google Scholar]
- Knapik JJ, Austin KG, McGraw SM, Leahy GD, Lieberman HR, 2017. Caffeine consumption among active duty United States Air Force personnel. Food Chem Toxicol 105, 377–386. [DOI] [PubMed] [Google Scholar]
- Knapik JJ, Trone DW, McGraw S, Steelman RA, Austin KG, Lieberman HR, 2016. Caffeine Use among Active Duty Navy and Marine Corps Personnel. Nutrients 8(10). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kozak PJ PA, Jackson NJ, Chakravorty S, Grandner MA, 2011. Alcohol, smoking, caffeine and drug use associated with sleep duration and sleep quality, Sleep. [Google Scholar]
- Kullen C, Prvan T, O’Connor H, 2019. Dietary Supplement Use in Australian Army Personnel. Mil Med 184(5-6), e290–e297. [DOI] [PubMed] [Google Scholar]
- Lieberman HR, Stavinoha T, McGraw S, White A, Hadden L, Marriott BP, 2012. Caffeine use among active duty US Army soldiers. J Acad Nutr Diet 112(6), 902–912, 912 e901–904. [DOI] [PubMed] [Google Scholar]
- Lieberman HR, Tharion WJ, Shukitt-Hale B, Speckman KL, Tulley R, 2002. Effects of caffeine, sleep loss, and stress on cognitive performance and mood during U.S. Navy SEAL training. Sea-Air-Land. Psychopharmacology 164(3), 250–261. [DOI] [PubMed] [Google Scholar]
- Lohi JJ, Huttunen KH, Lahtinen TM, Kilpelainen AA, Muhli AA, Leino TK, 2007. Effect of caffeine on simulator flight performance in sleep-deprived military pilot students. Mil Med 172(9), 982–987. [DOI] [PubMed] [Google Scholar]
- Luxton DD, Greenburg D, Ryan J, Niven A, Wheeler G, Mysliwiec V, 2011. Prevalence and impact of short sleep duration in redeployed OIF soldiers. Sleep 34(9), 1189–1195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mallett KA, Marzell M, Scaglione N, Hultgren B, Turrisi R, 2014. Are all alcohol and energy drink users the same? Examining individual variation in relation to alcohol mixed with energy drink use, risky drinking, and consequences. Psychology of addictive behaviors : journal of the Society of Psychologists in Addictive Behaviors 28(1), 97–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mash HB, Fullerton CS, Ramsawh HJ, Ng TH, Wang L, Kessler RC, Stein MB, Ursano RJ, 2014. Risk for suicidal behaviors associated with alcohol and energy drink use in the US Army. Soc Psychiatry Psychiatr Epidemiol 49(9), 1379–1387. [DOI] [PubMed] [Google Scholar]
- Matsangas P, Shattuck NL, 2018. Discriminating Between Fatigue and Sleepiness in the Naval Operational Environment. Behav Sleep Med 16(5), 427–436. [DOI] [PubMed] [Google Scholar]
- Matsangas P, Shattuck NL, 2020. Sleep quality, occupational factors, and psychomotor vigilance performance in the US Navy sailors. Sleep 43(12), zsaa118. [DOI] [PubMed] [Google Scholar]
- McKetin R, Coen A, Kaye S, 2015. A comprehensive review of the effects of mixing caffeinated energy drinks with alcohol. Drug Alcohol Depend 151, 15–30. [DOI] [PubMed] [Google Scholar]
- McLean CP, Zandberg L, Roache JD, Fitzgerald H, Pruiksma KE, Taylor DJ, Dondanville KA, Litz BT, Mintz J, Young-McCaughan S, Yarvis JS, Peterson AL, Foa EB, Strong Star Consortium, 2017. Caffeine Use in Military Personnel With PTSD: Prevalence and Impact on Sleep. Behav Sleep Med, 1–11. [DOI] [PubMed] [Google Scholar]
- McLellan TM, Bell DG, Kamimori GH, 2004. Caffeine improves physical performance during 24 h of active wakefulness. Aviat Space Environ Med 75(8), 666–672. [PubMed] [Google Scholar]
- McLellan TM, Kamimori GH, Bell DG, Smith IF, Johnson D, Belenky G, 2005a. Caffeine maintains vigilance and marksmanship in simulated urban operations with sleep deprivation. Aviat Space Environ Med 76(1), 39–45. [PubMed] [Google Scholar]
- McLellan TM, Kamimori GH, Voss DM, Bell DG, Cole KG, Johnson D, 2005b. Caffeine maintains vigilance and improves run times during night operations for Special Forces. Aviat Space Environ Med 76(7), 647–654. [PubMed] [Google Scholar]
- McLellan TM, Kamimori GH, Voss DM, Tate C, Smith SJ, 2007. Caffeine effects on physical and cognitive performance during sustained operations. Aviat Space Environ Med 78(9), 871–877. [PubMed] [Google Scholar]
- McLellan TM, Riviere LA, Williams KW, McGurk D, Lieberman HR, 2018. Caffeine and energy drink use by combat arms soldiers in Afghanistan as a countermeasure for sleep loss and high operational demands. Nutr Neurosci, 1–10. [DOI] [PubMed] [Google Scholar]
- Mysliwiec V, McGraw L, Pierce R, Smith P, Trapp B, Roth BJ, 2013. Sleep disorders and associated medical comorbidities in active duty military personnel. Sleep 36(2), 167–174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newman RA, Kamimori GH, Wesensten NJ, Picchioni D, Balkin TJ, 2013. Caffeine gum minimizes sleep inertia. Percept Mot Skills 116(1), 280–293. [DOI] [PubMed] [Google Scholar]
- Nunes RA, Mazzotti DR, Hirotsu C, Andersen ML, Tufik S, Bittencourt L, 2017. The association between caffeine consumption and objective sleep variables is dependent on ADORA2A c. 1083T> C genotypes. Sleep Med 30, 210–215. [DOI] [PubMed] [Google Scholar]
- Ogeil RP, Barger LK, Lockley SW, O’Brien CS, Sullivan JP, Qadri S, Lubman DI, Czeisler CA, Rajaratnam SMW, 2018. Cross-sectional analysis of sleep-promoting and wake-promoting drug use on health, fatigue-related error, and near-crashes in police officers. BMJ Open 8(9), e022041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peacock A, Bruno R, Martin FH, 2012. The subjective physiological, psychological, and behavioral risk-taking consequences of alcohol and energy drink co-ingestion. Alcohol Clin Exp Res 36(11), 2008–2015. [DOI] [PubMed] [Google Scholar]
- Peacock A, Pennay A, Droste N, Bruno R, Lubman DI, 2014. ‘High’ risk? A systematic review of the acute outcomes of mixing alcohol with energy drinks. Addiction 109(10), 1612–1633. [DOI] [PubMed] [Google Scholar]
- Rasmussen BB, Brix TH, Kyvik KO, Brøsen K, 2002. The interindividual differences in the 3-demthylation of caffeine alias CYP1A2 is determined by both genetic and environmental factors. Pharmacogenetics and Genomics 12(6), 473–478. [DOI] [PubMed] [Google Scholar]
- Rasmussen N, 2011. Medical science and the military: the Allies’ use of amphetamine during World War II. J Interdiscip Hist 42(2), 205–233. [DOI] [PubMed] [Google Scholar]
- Reissig CJ, Strain EC, Griffiths RR, 2009. Caffeinated energy drinks--a growing problem. Drug Alcohol Depend 99(1–3), 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidt RMM, Lindsey K; Caldwell John A. ; Hallman Chris, 2008. Prevalence of Energy-Drink and Supplement Usage in a Sample of Air Force Personnel.
- Shattuck NL, Matsangas P, 2017. Sunlight Exposure, Work Hours, Caffeine Consumption, and Sleep Duration in the Naval Environment. Aerosp Med Hum Perform 88(6), 579–585. [DOI] [PubMed] [Google Scholar]
- Simon MM,J, 2007. Alcohol, Energy Drinks, and Youth: A Dangerous Mix Marin Institute, San Raefel, CA. [Google Scholar]
- Snyder SH, 1973. Amphetamine psychosis: a “model” schizophrenia mediated by catecholamines. Am J Psychiatry 130(1), 61–67. [DOI] [PubMed] [Google Scholar]
- Somogyi LP, 2010. Caffeine intake by the US population. ‘Food and Drug Administration and Oakridge National Laboratory; ’. [Google Scholar]
- Stephens MB, Attipoe S, Jones D, Ledford CJ, Deuster PA, 2014. Energy drink and energy shot use in the military. Nutr Rev 72Suppl 1, 72–77. [DOI] [PubMed] [Google Scholar]
- Tharion WJ, Shukitt-Hale B, Lieberman HR, 2003. Caffeine effects on marksmanship during high-stress military training with 72 hour sleep deprivation. Aviat Space Environ Med 74(4), 309–314. [PubMed] [Google Scholar]
- Tikuisis P, Keefe AA, McLellan TM, Kamimori G, 2004. Caffeine restores engagement speed but not shooting precision following 22 h of active wakefulness. Aviat Space Environ Med 75(9), 771–776. [PubMed] [Google Scholar]
- Toblin RL, Adrian AL, Hoge CW, Adler AB, 2018. Energy Drink Use in U.S. Service Members After Deployment: Associations With Mental Health Problems, Aggression, and Fatigue. Mil Med 183(11-12), e364–e370. [DOI] [PubMed] [Google Scholar]
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, Moher D, Peters MDJ, Horsley T, Weeks L, Hempel S, Akl EA, Chang C, McGowan J, Stewart L, Hartling L, Aldcroft A, Wilson MG, Garritty C, Lewin S, Godfrey CM, Macdonald MT, Langlois EV, Soares-Weiser K, Moriarty J, Clifford T, Tuncalp O, Straus SE, 2018. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 169(7), 467–473. [DOI] [PubMed] [Google Scholar]
- Troxel WM, Shih RA, Pedersen ER, Geyer L, Fisher MP, Griffin BA, Haas AC, Kurz J, Steinberg PS, 2015. Sleep in the military: Promoting healthy sleep among US servicemembers. Rand health quarterly 5(2). [PMC free article] [PubMed] [Google Scholar]
- United States Headquarters, 2013. Mental Health Advisory Team 9 (MHAT 9) Operation Enduring Freedom (OEF) 2013 Afghanistan.
- Waits WM, Ganz MB, Schillreff T, Dell PJ, 2014. Sleep and the use of energy products in a combat environment. US Army Med Dep J, 22–28. [PubMed] [Google Scholar]
- Watson NF, Badr MS, Belenky G, Bliwise DL, Buxton OM, Buysse D, Dinges DF, Gangwisch J,. [Google Scholar]
- Wells BE, Kelly BC, Pawson M, Leclair A, Parsons JT, Golub SA, 2013. Correlates of concurrent energy drink and alcohol use among socially active adults. The American journal of drug and alcohol abuse 39(1), 8–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- West DS, Bursac Z, Quimby D, Prewitt TE, Spatz T, Nash C, Mays G, Eddings K, 2006. Self-reported sugar-sweetened beverage intake among college students. Obesity (Silver Spring) 14(10), 1825–1831. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.