

There are profound sex-based differences in both humoral and cellular immune responses to vaccination [1]. In general, adult females demonstrate higher antibody responses to bacterial and viral vaccines than men [2]. For instance, adult females vaccinated with half the dose of the trivalent inactivated influenza vaccine (TIV) produce similar humoral immune responses than adult males vaccinated with a full dose of the TIV [3]. Given that the 23-valent pneumococcal polysaccharide vaccine (PPSV23) is an important tool in our evaluation of the humoral immune response [4], we sought to determine if men and women have a significantly different immunoglobulin G (IgG) antibodyresponse to PPSV23.
The present study was performed at the Mayo Clinic (Rochester, Minnesota) in compliance with an IRB-approved protocol [5]. The study recruited healthy individuals ages ≥18 years who had no previous pneumococcal vaccination or significant pneumococcal infection. The PPSV23 vaccine was administered to all study participants after collecting blood samples to measure pre-PPSV23 pneumococcal serotype-specific IgG antibody levels (baseline). Four to six weeks after administering the PPSV23, blood samples were again collected to measure post-PPSV23 pneumococcal serotype-specific IgG antibody levels.
Participant demographics were summarized with frequencies and percentages or means and standard deviations (SD), as appropriate, and were compared by sex with chi-square or Wilcoxon rank-sum tests, as appropriate. In addition, the fold change increase in the individual serotype-specific IgG antibody levels and the sum of all twenty-three of these were compared by sex with Wilcoxon rank-sum tests and were summarized with the median and interquartile range (IQR). Multivariable analysis was performed to compare the fold change of the serotype sum with quantile regression, estimating the difference in the median by sex, adjusted for BMI, age, and days between the pre- and post-vaccine blood draws. P-values less than 0.05 were considered statistically significant. All analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC).
One hundred healthy adults were recruited to the study and received the PPSV23 between 2006 and 2007. Of these, fifty-three were female and forty-seven were male. The mean age of participants was 43.8 years (SD 13.6, range 20–66). The majority of the participants were Caucasian (81%), non-Hispanic (61%), and had a body mass index (BMI) of equal or greater than 25 (71.1%). There were no statistically significant differences in age, race, ethnicity, or BMI amongst the male and female groups.
Our results show that female healthy adults had a significantly greater fold change of the sum of all twenty-three serotype-specific IgG antibody levels after PPSV23 than their male counterparts (median 4.26 versus 3.01; P = 0.049) [Figure 1A]. When adjusted for BMI, age, and days between the pre- and post-vaccine blood draws, although the adjusted median fold change in the serotype sum was still slightly lower among males (median difference 1.06), it was not statistically significant (P = 0.10). When comparing the median fold change increase in the individual serotype-specific IgG antibody levels, all but 4 of them were higher in female subjects; but these sex differences reached statistical significance only in 2 of the serotypes: P22 (P = 0.002) and P34 (P = 0.04). Interestingly, when including only those individuals age 50 or older (17 males and 23 females) in the analysis, there was a greater sex difference in the fold change of the sum of all twenty-three serotype-specific IgG antibody levels after PPSV23 (median 5.78 versus 2.97 for females versus males, respectively; P = 0.014) [Figure 1B]. Furthermore, when adjusted for BMI and days between the pre- and post-vaccine blood draws, this sex difference remained statistically significant [P = 0.048]. Finally, there were no statistically significant sex differences in the pre-PPSV23 (p = 0.51) or the post-PPSV23 (p = 0.67) sum of twenty-three serotype-specific IgG antibody levels.
Figure 1.
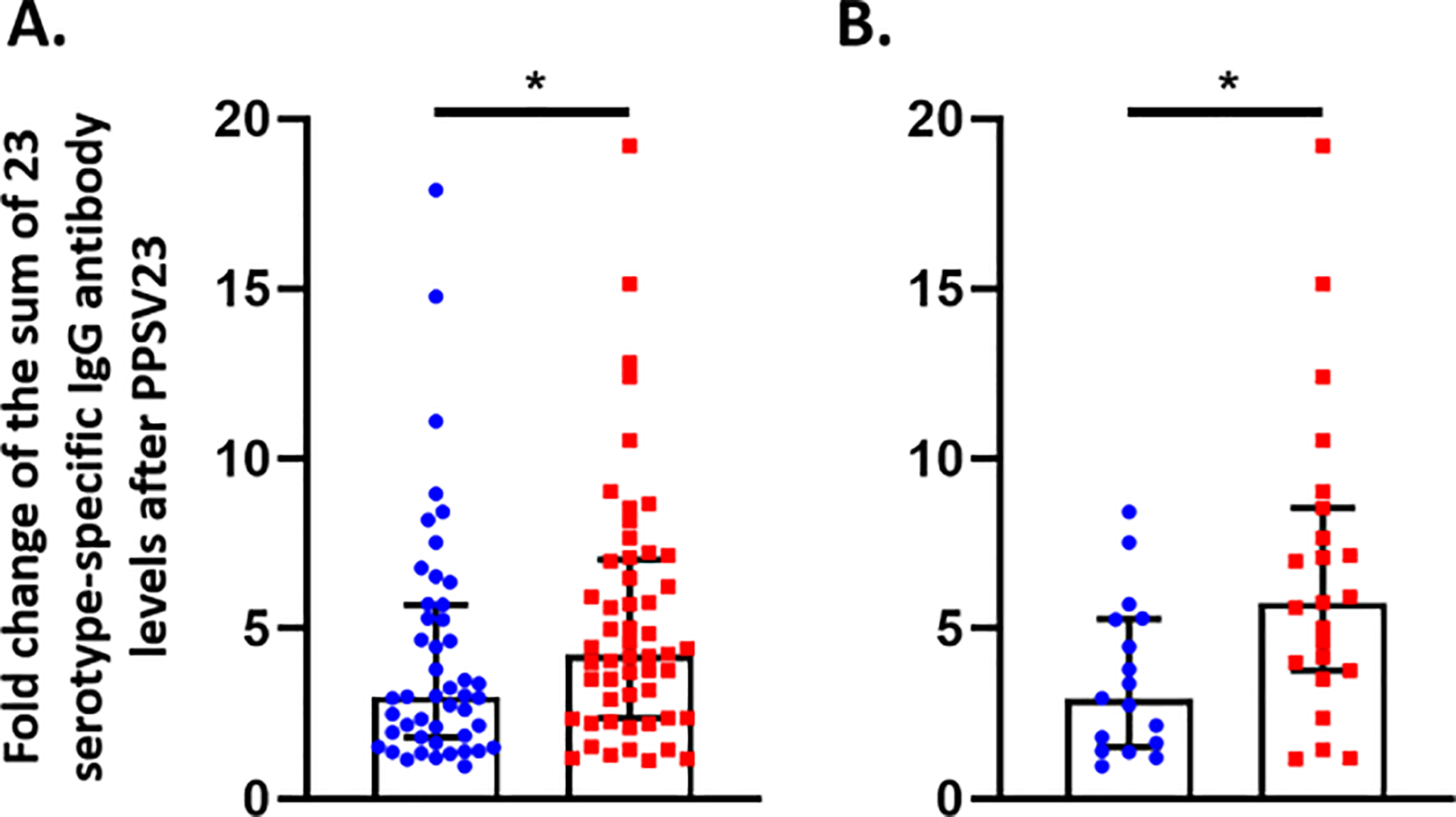
The fold changes of the sum of 23 serotype-specific IgG antibody levels after receiving the 23-valent pneumococcal polysaccharide vaccine (y-axis) measured in healthy, pneumococcal vaccine-naïve individuals. A. All males (N = 47; blue circles) versus all females (N = 53; red squares) [P = 0.049]. When adjusted for BMI, age, and days between the pre- and post-vaccine blood draws, the difference was not statistically significant [P = 0.10]. B. Males who are age 50 or older (N = 17; blue circles) versus female who are age 50 or older (N = 23; red squares) [P = 0.014]. When adjusted for BMI and days between the pre- and post-vaccine blood draws, this sex difference remained statistically significant [P = 0.048]. *P < 0.05 by Wilcoxon rank-sum test.
Men have a higher incidence of invasive pneumococcal disease than women [6]. In this study, we present evidence to suggest a trend towards a more robust IgG antibody response to the PPSV23 in healthy adult females compared to males. This sex difference was more pronounced in those age 50 or older. Similar to our findings, prior studies have also reported that male sex can be associated with lower responses to PSSV23 [7]. These sex differences in the PPSV23-induced IgG responses might be particularly relevant when using fold change increases in antibody levels as part of the diagnostic evaluation of functional antibody deficiencies, such as specific antibody deficiency [4, 8]. A limitation of our study is that we were underpowered to detect the difference in the fold change of the serotype sum between all females and males in adjusted analyses. Larger studies to confirm and further explore the sex differences in antibody responses to pneumococcal vaccines (both PPSV23 and the pneumococcal conjugate vaccine [PCV13]) are warranted. These studies should include an analysis of serotype-specific sex differences as immunogenicity may vary between individual serotypes [9]. Furthermore, since both sex chromosome and sex hormones can influence the immune responses to vaccination [10], we suspect these sex differences will be influenced by the reproductive stage of the groups studied (i.e. pre-menopausal versus post-menopausal). Finally, additional studies are needed to determine if this sexual dimorphism is present in non-healthy populations, such as those with primary immunodeficiency disorders or asthma.
Sources of funding:
This study was funded by NIH/NIAID K08AI141765 (Sergio E. Chiarella)
The authors thank Dr. Alexandra Graden for her contributions to this manuscript.
Footnotes
Conflicts of interest: The authors declare that they have no conflict of interest
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol. 2016;16(10):626–638. [DOI] [PubMed] [Google Scholar]
- 2.Cook IF. Sexual dimorphism of humoral immunity with human vaccines. Vaccine. 2008;26(29–30):3551–3555. [DOI] [PubMed] [Google Scholar]
- 3.Engler RJ, Nelson MR, Klote MM, VanRaden MJ, Huang C, Cox NJ, et al. Half- vs full-dose trivalent inactivated influenza vaccine (2004–2005): age, dose, and sex effects on immune responses. Arch Intern Med. 2008;168(22):2405–2414. [DOI] [PubMed] [Google Scholar]
- 4.Orange JS, Ballow M, Stiehm ER, Balias ZR, Chinen J, De La Morena M, et al. Use and interpretation of diagnostic vaccination in primary immunodeficiency: a working group report of the Basic and Clinical Immunology Interest Section of the American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol. 2012;130(3 Suppl):S1–24. [DOI] [PubMed] [Google Scholar]
- 5.Park MA, Jenkins SM, Smith CY, Pyle RC, Sacco KA, Ryu E, et al. Pneumococcal serotype-specific cut-offs based on antibody responses to pneumococcal polysaccharide vaccination in healthy adults. Vaccine. 2021;39(21):2850–2856. [DOI] [PubMed] [Google Scholar]
- 6.Wagenvoort GH, Sanders EAM, Vlaminckx BJ, De Melker HE, Van der Ende A, Knol MJ. Sex differences in invasive pneumococcal disease and the impact of pneumococcal conjugate vaccination in the Netherlands, 2004 to 2015. Euro Surveill. 2017;22(10). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Parker AR, Skold M, Harding S, Clayborn Barton J, Bertoli LF, Barton JC. Pneumococcal vaccination responses in adults with subnormal IgG subclass concentrations. BMC Immunol. 2019;20(1):29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Perez E, Bonilla FA, Orange JS, Ballow M. Specific Antibody Deficiency: Controversies in Diagnosis and Management. Front Immunol. 2017;8:586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kong Y, Zhang W, Jiang Z, Wang L, Li C, Li Y, et al. Immunogenicity and safety of a 23-valent pneumococcal polysaccharide vaccine in Chinese healthy population aged >2 years: A randomized, double-blinded, active control, phase III trial. Hum Vaccin Immunother. 2015;11(10):2425–2433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Klein SL, Marriott I, Fish EN. Sex-based differences in immune function and responses to vaccination. Trans R Soc Trop Med Hyg. 2015;109(1):9–15. [DOI] [PMC free article] [PubMed] [Google Scholar]