

Abstract
Corpus callosum agenesis is a rare condition and is sometimes associated with schizophrenia. The co‐existence of these two conditions adds value to the neurodevelopmental theory of schizophrenia.
Keywords: case report, corpus callosum agenesis, neurodevelopmental, schizophrenia
Corpus callosum agenesis is a rare condition and is sometimes associated with schizophrenia. The co‐existence of these two conditions adds value to the neurodevelopmental theory of schizophrenia.
1. INTRODUCTION
The clinical evidence linking schizophrenia with corpus callosum agenesis can support the neurodevelopmental model of schizophrenia in a subset of patients. Here, we present a case of a young man with paranoid schizophrenia who had agenesis of the corpus callosum and was successfully treated with antipsychotic drugs.
The Corpus callosum is the largest white matter structure of the human brain involved in interhemispheric signal transmission.1 The incidence of corpus callosum agenesis is about 1:4000 among live births, which can be either complete or partial and can occur as an isolated anomaly or a part of other syndromic disorders.2, 3
Studies have reported heterogeneous outcomes in those with corpus callosal agenesis ranging from being asymptomatic to having neurological manifestations as seizures, cognitive impairment, neurodevelopmental disorders like Asperger's syndrome, autism, attention deficit disorders, frank psychiatric disorders such as major depression and schizophrenia, and even personality disorders.4, 5
Here, we present a case of a 24 years‐old man who was diagnosed to have paranoid schizophrenia and was found to have complete corpus callosum agenesis in magnetic resonance imaging as a coincidental finding. To our knowledge, this is the first case of early‐onset schizophrenia with complete agenesis of the corpus callosum reported from Nepal.
2. CASE REPORT
A 24 years‐old right‐handed man from rural western Nepal was brought to our clinic by his mother with the main complaint of increasing aggression for a few weeks. The history of the patient's illness dates back ten years when a gradual change in his behavior was noted. At first, he started withdrawing himself from others and rarely interacted with them. He would remain alone in his room and appear sad most of the time. She reported that her son would hear imaginary voices and respond to them for almost the same duration. Sometimes, he yelled at them and appeared scared, while at other times, he giggled like a child. He often confronted his family, saying that both his family and neighbors were planning to kill him and talked ill about him. Additionally, he started showing aggression for the past two years. It gradually increased to the point where he started expressing homicidal thoughts directed to his mother and sister. Occasionally, he would even bring weapons and threatened to kill them if they continued troubling him and had slashed his sister's forearm once. He used to claim that people of his village were talking about him and posting his thoughts openly on social media, which often made him restless and angry. His family tried convincing him regarding that, but it never worked. On further inquiry, he had an episode of generalized tonic‐clonic seizures three years back.
The patient's treatment history revealed that he was once kept on antipsychotics at the onset of symptoms, but he stopped taking the medication after one year with some improvement. Moreover, it was difficult to convince him to go for a consultation. His family history revealed intellectual disability in his first and second‐degree relatives, and his personal history revealed him to be a difficult child. However, he did not have any developmental delay, cognitive impairment, or intellectual disability. Before the onset of symptoms, he was an average student at school, but later he could not clear the examination of tenth standard even after multiple attempts and eventually dropped out of school. Additionally, there was no history of abuse of any substance.
On physical examination, the patient did not show any gross abnormality. Mental state examination revealed a well‐dressed, cooperative, average‐built male of early twenties with proper hygiene and grooming. His attitude was satisfactory; however, his speech was monotonous, affect was restricted, and he had persecutory delusions. Further assessment revealed third‐person auditory hallucinations with the content being people planning to kill him and a complete lack of insight. He was provisionally diagnosed with paranoid schizophrenia and was started on a second‐generation antipsychotic before referring to a tertiary level hospital after initial discussion with a psychiatrist.
A detailed neuropsychological evaluation revealed no significant findings, and the formal intelligence testing was within the normal range. The basic investigations reports, serology panel, and electroencephalogram did not show any abnormal findings. However, MRI revealed complete agenesis of the corpus callosum along with dilated lateral ventricles (Figure 1 and Figures [Link], [Link], [Link], [Link]).
FIGURE 1.
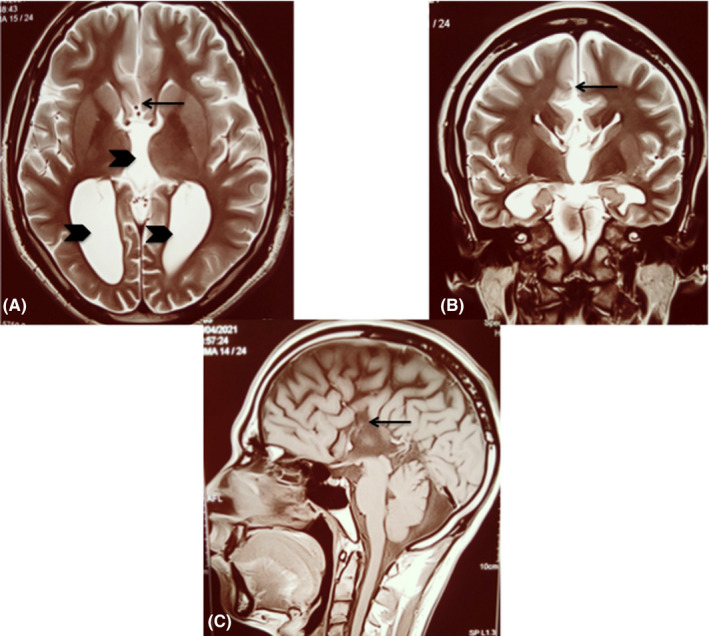
T2‐weighted MRI images of the brain, A. axial view, B. coronal view, C. sagittal view (arrow: normal location of the corpus callosum, which is absent in our patient; arrowheads: dilated ventricles)
With the final diagnosis of paranoid schizophrenia with corpus callosum agenesis, he was prescribed 20 mg aripiprazole, 500 mg sodium valproate, and 2 mg lorazepam. Finally, after significant improvement, he was discharged from the hospital after 13 days with a follow‐up management plan. He is on regular follow‐up at our clinic and is doing well.
3. DISCUSSION
Cases of isolated corpus callosal agenesis in schizophrenia with no symptoms of disconnection syndrome have been reported in various case series and reports.5 Our patient has complete agenesis of the corpus callosum with dilated lateral ventricles, and he has had paranoid symptoms since the age of fifteen. This is consistent with previous studies presenting evidence regarding the onset of symptoms either in late childhood or early adolescence in an isolated subtype with a normal level of intelligence and neuropsychological development.6 The patient did not have any physical deformity, and there was no history of significant delay in achieving developmental milestones. His symptoms gradually started from initial anhedonia to third‐person auditory hallucinations, delusions of persecution, delusions of reference, and finally aggressive behavior. The prominent and persistent paranoid symptoms present in this patient are the major concern of intractability in this disease.7 Even so, our patient showed significant improvement within weeks of the start of antipsychotics. However, a longer follow‐up is necessary to have a clear picture of the course and prognosis of this patient.
Several factors can explain the symptoms of schizophrenia in patients with agenesis of the corpus callosum.8, 9 The corpus callosum has intimate connections with other limbic structures such as the hippocampus and cingulate cortex during embryonic development, and there is ample evidence that these structures are involved in patients with schizophrenia.1, 10 Additionally, aberrant neuronal connections between the two cerebral hemispheres, which might be the cause of many neurological symptoms such as seizures, have been considered as one of the underlying mechanisms of the biological causes of schizophrenia.7, 10 The experimental neuropsychology in schizophrenics has also provided evidence that abnormal patterns of interhemispheric transfer may account for the symptoms of psychosis.8 Ultimately, this provides support for the neurodevelopmental model of schizophrenia, at least for a subset of patients. The enlargement of the lateral ventricle found in most patients with schizophrenia is a well‐known structural neuroanatomical substrate in schizophrenia and,11 unfortunately, is related to the poor outcome in schizophrenia.12
4. CONCLUSION
We report successful management of a case of paranoid schizophrenia with corpus callosum agenesis in a young male patient. The early age of onset with predominantly chronic positive symptoms in schizophrenia offers some insight into the neurodevelopmental model of schizophrenia.
CONFLICTS OF INTEREST
All authors of the manuscript acknowledge that they are not affiliated with or associated with any organization or entity that has a financial or non‐financial interest in the subject matter or materials discussed in the manuscript.
AUTHOR CONTRIBUTIONS
All three authors significantly contributed to both the clinical management of the patient and writing the case report.
CONSENT
All the authors of this manuscript have confirmed during submission that patient consent has been signed and collected in accordance with the journal's patient consent policy.
Supporting information
Fig S1
{kind=link}
Fig S2
{kind=link}
Fig S3
{kind=link}
Fig S4
{kind=link}
Neupane H, Adhikari S, Dhungana S. Complete agenesis of the corpus callosum in paranoid schizophrenia—a case report. Clin Case Rep. 2021;9:e04911. 10.1002/ccr3.4911
Funding information
There was no funding available for this article
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
REFERENCES
- 1.Bondade S, Kumar KK, Hussain D. Arnold‐Chiari malformation and agenesis of the corpus callosum in a case of brief psychotic disorder. Arch Psychiatry Psychother. 2018;20(2):42‐45. 10.12740/APP/84886 [DOI] [Google Scholar]
- 2.Lieb JM, Ahlhelm FJ. Agenesis of the corpus callosum. Radiologe. 2018;58(7):636‐645. 10.1007/s00117-018-0388-2 [DOI] [PubMed] [Google Scholar]
- 3.Dávila‐Gutiérrez G. Agenesis and dysgenesis of the corpus callosum. Semin Pediatr Neurol. 2002;9(4):292‐301. 10.1053/spen.2002.32505 [DOI] [PubMed] [Google Scholar]
- 4.D’Antonio F, Pagani G, Familiari A, et al. Outcomes associated with isolated agenesis of the corpus callosum: a meta‐analysis. Pediatrics. 2016;138(3):e20160445. 10.1542/peds.2016-0445 [DOI] [PubMed] [Google Scholar]
- 5.Popoola O, Olayinka O, Azizi H, et al. Neuropsychiatric manifestations of partial agenesis of the corpus callosum: a case report and literature review. Jönsson E, ed. Case Rep Psychiatry. 2019;2019:1‐8. 10.1155/2019/5925191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Moutard M‐L, Kieffer V, Feingold J, et al. Isolated corpus callosum agenesis: a ten‐year follow‐up after prenatal diagnosis (how are the children without corpus callosum at 10 years of age?). Prenat Diagn. 2012;32(3):277‐283. 10.1002/pd.3824 [DOI] [PubMed] [Google Scholar]
- 7.Hallak JEC, Crippa JADS, Pinto JP, et al. Total agenesis of the corpus callosum in a patient with childhood‐onset schizophrenia. Arq Neuropsiquiatr. 2007;65(4b):1216‐1219. 10.1590/S0004-282X2007000700024 [DOI] [PubMed] [Google Scholar]
- 8.David AS. Schizophrenia and the corpus callosum: developmental, structural and functional relationships. Behav Brain Res. 1994;64(1‐2):203‐211. 10.1016/0166-4328(94)90132-5 [DOI] [PubMed] [Google Scholar]
- 9.David AS, Wacharasindhu A, Lishman WA. Severe psychiatric disturbance and abnormalities of the corpus callosum: review and case series. J Neurol Neurosurg Psychiatry. 1993;56(1):85‐93. 10.1136/jnnp.56.1.85 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wojtalik JA, Smith MJ, Keshavan MS, Eack SM. A systematic and meta‐analytic review of neural correlates of functional outcome in schizophrenia. Schizophr Bull. 2017;43(6):1329‐1347. 10.1093/schbul/sbx008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sayo A, Jennings RG, Van Horn JD. Study factors influencing ventricular enlargement in schizophrenia: a 20 year follow‐up meta‐analysis. NeuroImage. 2012;59(1):154‐167. 10.1016/j.neuroimage.2011.07.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mitelman SA, Canfield EL, Brickman AM, Shihabuddin L, Hazlett EA, Buchsbaum MS. Progressive ventricular expansion in chronic poor‐outcome schizophrenia. Cogn Behav Neurol. 2010;23(2):85‐88. 10.1097/WNN.0b013e3181cfb52a [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Fig S1
Fig S2
Fig S3
Fig S4
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.