

Although racial and ethnic disparities in U.S. COVID-19 death rates are striking, focusing on COVID-19 deaths alone may underestimate the true effect of the pandemic on disparities. This study estimated excess deaths related and unrelated to COVID-19 in the United States from March to December 2020 by race/ethnicity, sex, age group, and cause.
Visual Abstract. Racial and Ethnic Disparities in Excess Deaths During the COVID-19 Pandemic.
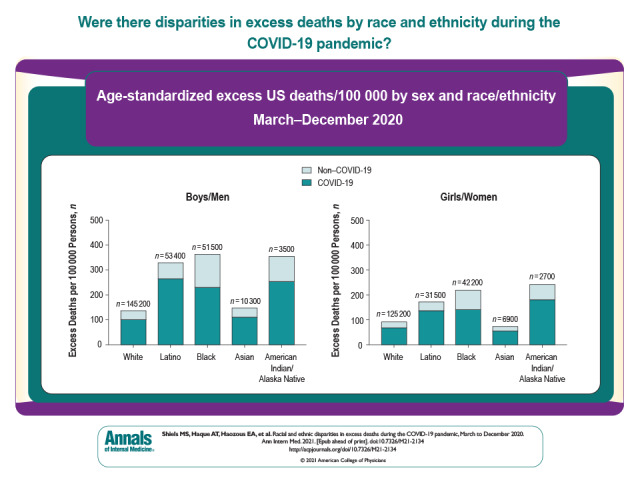
Although racial and ethnic disparities in U.S. COVID-19 death rates are striking, focusing on COVID-19 deaths alone may underestimate the true effect of the pandemic on disparities. This study estimated excess deaths related and unrelated to COVID-19 in the United States from March to December 2020 by race/ethnicity, sex, age group, and cause.
Abstract
Background:
Although racial/ethnic disparities in U.S. COVID-19 death rates are striking, focusing on COVID-19 deaths alone may underestimate the true effect of the pandemic on disparities. Excess death estimates capture deaths both directly and indirectly caused by COVID-19.
Objective:
To estimate U.S. excess deaths by racial/ethnic group.
Design:
Surveillance study.
Setting:
United States.
Participants:
All decedents.
Measurements:
Excess deaths and excess deaths per 100 000 persons from March to December 2020 were estimated by race/ethnicity, sex, age group, and cause of death, using provisional death certificate data from the Centers for Disease Control and Prevention (CDC) and U.S. Census Bureau population estimates.
Results:
An estimated 2.88 million deaths occurred between March and December 2020. Compared with the number of expected deaths based on 2019 data, 477 200 excess deaths occurred during this period, with 74% attributed to COVID-19. Age-standardized excess deaths per 100 000 persons among Black, American Indian/Alaska Native (AI/AN), and Latino males and females were more than double those in White and Asian males and females. Non–COVID-19 excess deaths also disproportionately affected Black, AI/AN, and Latino persons. Compared with White males and females, non–COVID-19 excess deaths per 100 000 persons were 2 to 4 times higher in Black, AI/AN, and Latino males and females, including deaths due to diabetes, heart disease, cerebrovascular disease, and Alzheimer disease. Excess deaths in 2020 resulted in substantial widening of racial/ethnic disparities in all-cause mortality from 2019 to 2020.
Limitations:
Completeness and availability of provisional CDC data; no estimates of precision around results.
Conclusion:
There were profound racial/ethnic disparities in excess deaths in the United States in 2020 during the COVID-19 pandemic, resulting in rapid increases in racial/ethnic disparities in all-cause mortality between 2019 and 2020.
Primary Funding Source:
National Institutes of Health Intramural Research Program.
In the United States, severe outcomes of COVID-19, including hospitalizations and deaths, have disproportionately affected American Indian/Alaska Native (AI/AN), Black, and Latino persons (1, 2). Although racial/ethnic differences in COVID-19 death rates have been profound, focusing on COVID-19 deaths alone may underestimate the extent of racial/ethnic disparities driven by the pandemic. Excess deaths due to COVID-19 have been estimated by comparing the number of deaths that occurred during 2020 with those in prior years, reflecting deaths from both diagnosed and undiagnosed COVID-19 and deaths indirectly caused by COVID-19 (3–6). During March to August 2020, 20% of excess deaths were due to non–COVID-19 causes (5). Comparisons of excess deaths across racial/ethnic groups provide a more complete assessment of racial/ethnic disparities in mortality during the pandemic.
In the current analysis, we utilized provisional-release death certificate data from the Centers for Disease Control and Prevention (CDC) and population projections from the U.S. Census Bureau for March to December 2020 to estimate the number of excess deaths and excess deaths per 100 000 persons by race/ethnicity, sex, age group, month, and cause of death. Excess deaths were estimated as the number of deaths observed in 2020 minus the number of deaths expected in 2020 if deaths divided by population size were the same as in 2019. Also, we assessed the effect of the pandemic on disparities in age-standardized mortality in 2020 versus 2019.
Methods
Data Sources
Provisional data on deaths by month, year, sex, age group, race/ethnicity, and cause of death were obtained from the CDC National Center for Health Statistics (NCHS) for 1 March 2020 (the first full month of COVID-19 deaths in the United States) to 31 December 2020. These data were compared with final mortality data for the same months in 2019 and were released on 3 August 2021 (7). Mortality data are reported to the National Vital Statistics System by the vital registration offices in all 50 states and the District of Columbia (8). Although data from more recent months were available, the analysis was lagged to account for delays in vital statistics reporting to the CDC (9).
Population estimates were obtained from U.S. Census Bureau projections for 2019 and 2020 by month, year, age group, sex, and race/ethnicity (10). Race/ethnicity was classified in both data sources into the following mutually exclusive categories: non-Latino White (White), non-Latino African American or Black (Black), non-Latino American Indian and Alaska Native (AI/AN), non-Latino Asian (Asian), Hispanic/Latino (Latino), and other (includes persons of 2 or more races, Native Hawaiians, Pacific Islanders, and those with unknown Hispanic origin). Unknown race is reassigned by the NCHS to one of the major racial groups. Data for 2019 were used for comparison due to changes in the categorization of race/ethnicity starting in 2018. Briefly, although prior mortality data bridged persons with more than 1 race to a single racial category, starting in 2018, decedents could be designated as having more than 1 race. In addition, Asians and Native Hawaiians/Pacific Islanders are now distinct categories (11). These changes precluded comparison with regularly released data from previous years. It has been estimated that AI/AN race is misclassified on 40% of death certificates; therefore, deaths presented here for AI/AN persons are likely to be greatly underestimated (12).
Data from the NCHS included information on underlying cause of death ascertained from death certificates and classified according to International Classification of Diseases, 10th Revision codes (COVID-19 [U071], cancer [C00 to C97], heart disease [I00 to I09, I11, I13, and I20 to I51], stroke [I60 to I69], diabetes [E10 to E14], Alzheimer disease [G30], and unclassified deaths [R00 to R99]). Deaths are coded by the NCHS as being related to COVID-19 when it is reported as a contributing cause on the death certificate; these include both laboratory-confirmed cases and cases without laboratory confirmation (13). Because this analysis only considered underlying cause, causes of death were mutually exclusive. Specific non–COVID-19 causes included in the analysis were previously shown to have resulted in excess deaths or death deficits in 2020 (5).
Data Analysis
Excess deaths from March through December 2020 were estimated as the number of deaths observed in 2020 minus the number expected in 2020 by cause, race/ethnicity, sex, age group, and month. The expected number of deaths in 2020 was estimated by applying the cause-specific, race/ethnicity–specific, sex-specific, age group–specific, and month-specific deaths divided by population size in 2019 to population counts in 2020 (5). Expected deaths are the number of deaths that would have occurred in 2020 if age-specific deaths divided by the population size had been the same as in 2019. To account for population decreases caused by excess deaths in preceding months, the sum of excess deaths from all prior months was subtracted from the population estimates in each month of interest (14). This approach adjusted for population growth and aging as well as population decreases due to excess deaths in 2020.
In a sensitivity analysis, data from the average of 2018 and 2019 were used to estimate expected deaths in 2020. Non–COVID-19 deaths were estimated by subtracting COVID-19 deaths from total excess death estimates. Because COVID-19 deaths started in 2020, all of them are considered to be excess deaths. Excess deaths per 100 000 persons were estimated by dividing excess death estimates by mid-year population estimates (June 2020) and were age-standardized in 10-year categories to the 2019 U.S. population. Death estimates were rounded to the nearest 100 deaths.
Role of the Funding Source
This study was funded by the Intramural Research Programs of the National Cancer Institute and the National Institute on Minority Health and Health Disparities. The funding sources approved the final version of this manuscript but played no role in the design, conduct, or analysis of the study or the decision to submit the manuscript for publication.
Results
Between March and December 2020, 2.88 million deaths were registered in the United States according to provisional CDC data. All-cause mortality per 100 000 persons increased for all racial/ethnic groups in both males and females between 2019 and 2020, and disparities in age-standardized deaths per 100 000 persons increased for Black and AI/AN males and females compared with White males and females (Figure 1, A and B). For example, deaths per 100 000 persons were 26% higher in 2019 and 45% higher in 2020 among Black males compared with White males and were 15% higher in 2019 and 32% higher in 2020 among Black females compared with White females.
Figure 1. Age-standardized all-cause deaths per 100 000 persons in the United States in March to December of 2019 and 2020 among males (A) and females (B) and age-standardized COVID-19 and non–COVID-19 excess deaths per 100 000 persons among males (C) and females (D), by race/ethnicity.
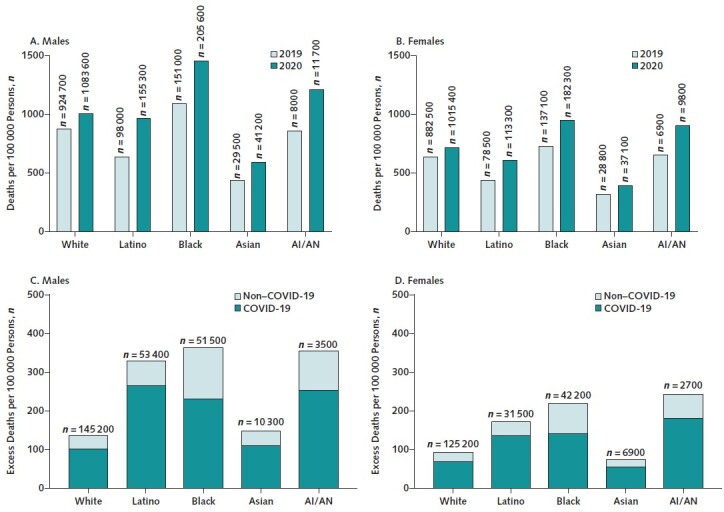
The total numbers of deaths (A and B) and excess deaths (C and D) are listed above the bars. Death rates for AI/AN persons are known to be underestimated due to racial misclassification on death certificates. AI/AN = American Indian/Alaska Native.
An estimated 477 200 excess deaths occurred between March and December 2020 compared with what would have been expected based on 2019 data. Age-standardized excess deaths per 100 000 persons in 2020 among Black, AI/AN, and Latino males and females were 2 to 3 times higher than among White and Asian males and females (Figure 1, C and D). Although excess deaths per 100 000 persons were higher among males than females within each racial/ethnic group, they were higher among AI/AN, Black, and Latino females than among White and Asian males. Results were similar when data from 2018 and 2019 were used to estimate expected deaths in 2020 (Appendix Figure 1). Figure 2 presents overall and excess deaths per 100 000 persons in 2020 by age and racial/ethnic group for males and females. Excess deaths per 100 000 persons were notably higher among AI/AN, Black, and Latino males and females compared with White and Asian males and females across age groups (Figure 2, A and B).
Appendix Figure 1. Comparison of excess deaths per 100 000 persons, by race/ethnicity.
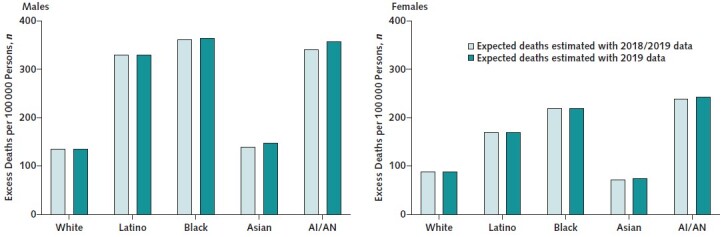
Estimates used expected deaths based on 2018/2019 data (light green) and 2019 data (dark green). AI/AN = American Indian/Alaska Native.
Figure 2. Age-specific all-cause deaths per 100 000 persons in the United States in March to December 2020 among males (A) and females (B) and age-specific COVID-19 (solid bars) and non–COVID-19 (striped bars) excess deaths per 100 000 persons among males (C) and females (D), by race/ethnicity.
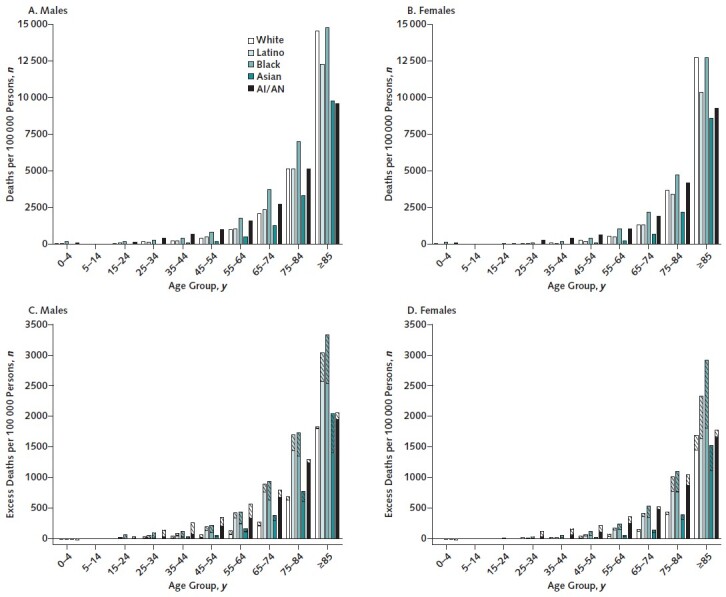
AI/AN = American Indian/Alaska Native.
Between March and December 2020, 351 400 (74%) excess deaths had COVID-19 as the underlying cause. Compared with White males and females, age-standardized COVID-19 deaths per 100 000 persons were at least 2 times higher among Black, Latino, and AI/AN males and females (Figure 1, C and D). Non–COVID-19 causes contributed 61 200 excess deaths (22.6% of total excess deaths) among White persons, 37 200 (29.7%) among Black persons, 19 300 (22.8%) among Latino persons, 4400 (25.8%) among Asian persons, and 1900 (30.9%) among AI/AN persons. Compared with White persons, excess deaths per 100 000 persons due to non–COVID-19 causes were 3 to 4 times higher among Black and AI/AN males and females and nearly 2 times higher in Latino males and females (Figure 1, C and D). Non–COVID-19 causes contributed 76% of excess deaths among persons younger than 45 years and only 22% among those aged 45 years or older. Racial/ethnic disparities were particularly pronounced among those aged 75 years or older, in whom non–COVID-19 excess deaths per 100 000 persons were 9 times higher among Black males compared with White males (Figure 2, C and D).
Figure 3 presents age-standardized overall and excess deaths due to non–COVID-19 causes per 100 000 persons in 2020 by cause of death for males and females in each racial/ethnic subgroup. Excess deaths were observed among all racial/ethnic groups for heart disease, diabetes, cerebrovascular disease, and Alzheimer disease (Figure 3, C and D) and were higher among Black, AI/AN, and Latino males and females than their respective White and Asian counterparts. Cancer deaths were lower than expected in each group, resulting in 9700 fewer cancer deaths during the period of interest. There were 27 200 deaths that had not yet been classified as of the date of the data release.
Figure 3. Age-standardized non–COVID-19 cause-specific deaths per 100 000 persons in the United States in March to December 2020 among males (A) and females (B) and age-standardized non–COVID-19 excess cause-specific deaths per 100 000 persons among males (C) and females (D), by race/ethnicity.
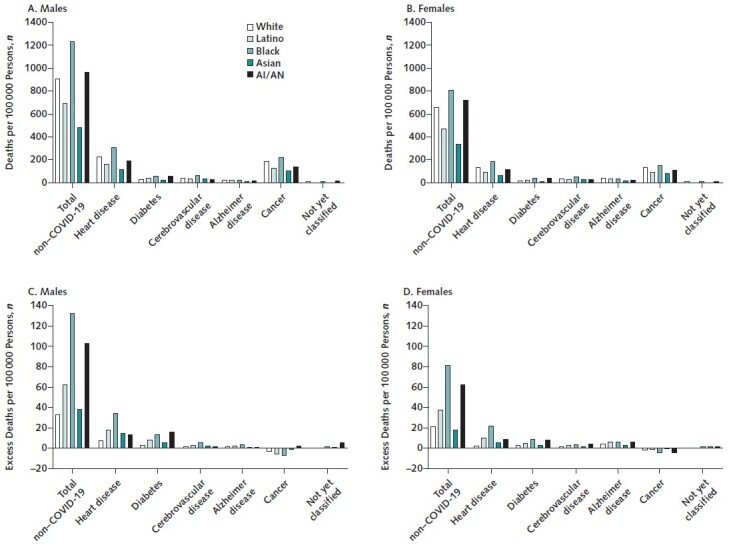
AI/AN = American Indian/Alaska Native.
Thirty-two percent of excess deaths occurred between March and June, 25.9% between July and September, and 42.1% between October and December. Monthly patterns in excess deaths varied across racial/ethnic groups but generally peaked in April, July and August, and December (Appendix Figures 2 and 3).
Appendix Figure 2. Total number of excess deaths among males, by month and race/ethnicity.
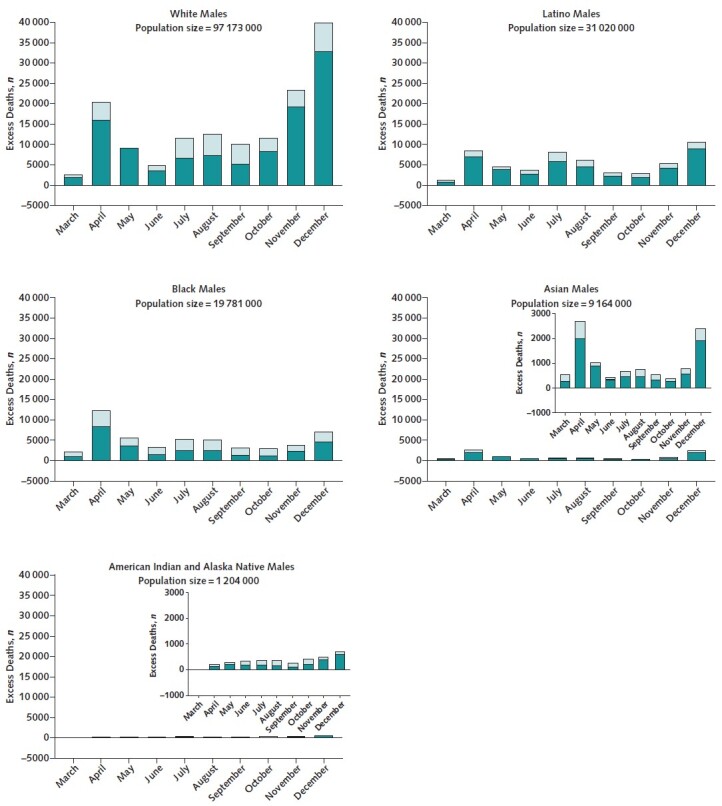
The dark green portion of each bar indicates deaths due to COVID-19, and the light green portion of each bar indicates non–COVID-19 causes. Population sizes are for June 2020. Note that the scale differs across plots.
Appendix Figure 3. Total number of excess deaths among females, by month and race/ethnicity.
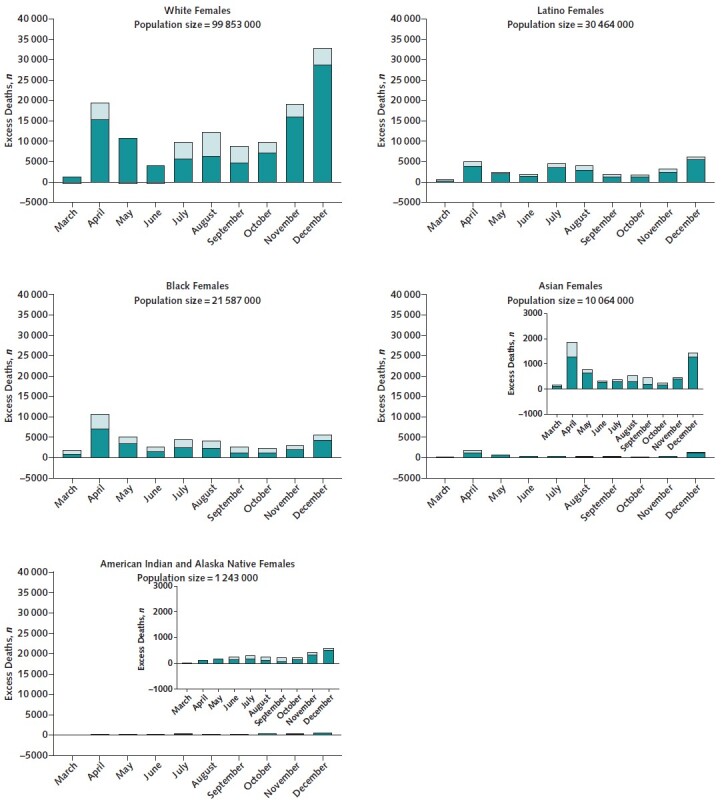
The dark green portion of each bar indicates deaths due to COVID-19, and the light green portion of each bar indicates non–COVID-19 causes. Population sizes are for June 2020. Note that the scale differs across plots.
Discussion
The United States has seen profound racial/ethnic disparities in COVID-19 cases, hospitalizations, and deaths since the beginning of the pandemic (15). Age-standardized excess deaths per 100 000 persons from March to December 2020 among Black, AI/AN, and Latino males and females were more than double those among White males and females, reflecting disproportionate increases in mortality from both COVID-19 and other causes.
Disparities in pandemic-related total excess deaths per 100 000 persons are even more pronounced than those for COVID-19 deaths alone in Black, AI/AN, and Latino persons. Given different time periods and methodologies, it is challenging to compare our findings with those of prior research. One study reported that excess death rates were 1.5 times higher in Black persons and lower in Latino persons than in White persons (3); however, we found notably higher excess death rates in Latino persons. Consistent with our findings, another study reported that excess death rates were highest among Black and AI/AN persons younger than 65 years and Black and Latino persons aged 65 years or older. As a result of the COVID-19 pandemic, racial/ethnic disparities in overall mortality rates widened between 2019 and 2020 among Black and AI/AN persons compared with White persons. In 2019, Latino persons had notably lower mortality rates than White persons; however, this mortality advantage was substantially diminished in 2020. These findings are consistent with a recent report that estimated that the life expectancy gap between Black persons and others has widened and the life expectancy advantage among Latino persons has shrunk (16). The steady progress over the past 20 years in decreasing the mortality gap between Black and White persons has been rapidly eliminated by the COVID-19 pandemic and is likely to worsen as the full effect of the pandemic becomes apparent.
Racial/ethnic disparities in COVID-19 risk, hospitalization, and death have been attributed to structural and social determinants of health with established and deep roots in racism (17). Black and Latino persons are more likely to have occupational exposures to COVID-19 than White persons (17, 18); they also are more likely to live in multigenerational households and more densely populated neighborhoods and have less access to health care and private transportation (17, 19, 20). American Indian/Alaska Native reservation–based communities are at further risk for infection due to a lack of infrastructure and chronically underfunded health care facilities (21, 22). Equitable vaccine distribution is needed to prevent further exacerbation of racial/ethnic disparities in COVID-19 risk and mortality (23, 24). Communications that focus on the safety and benefits of vaccination and are tailored to high-risk communities and coordinated community-mobilized vaccination promotion programs from trusted sources are needed to overcome vaccine hesitancy (25), as has been shown by high vaccination rates across AI/AN communities (26).
Non–COVID-19 excess deaths have also disproportionately affected Black, AI/AN, and Latino persons and contribute the majority of excess deaths among persons younger than 45 years. These excess deaths may have been driven by fear of seeking health care during the pandemic or by misattribution of deaths from COVID-19 to other causes, particularly at the beginning of the pandemic. Conversely, it is possible that some deaths due to other causes were classified as COVID-19 deaths. Some causes of death have not yet been released by the CDC, including accidental deaths, which is the leading cause in younger populations. This is of particular concern given reported increases in drug overdose and motor vehicle deaths in 2020 (27, 28). Cancer deaths were notably lower than expected over the period of interest across racial/ethnic groups, perhaps reflecting large decreases in cancer death rates in recent years (29) or COVID-19 as a competing cause of death. Uncertainty about a person's true underlying cause of death further emphasizes the importance of all-cause excess death estimates, which are agnostic to underlying causes.
The main strength of this study is the use of excess deaths to assess racial/ethnic disparities in the effect of COVID-19 on mortality in the United States. Although prior studies have reported on excess deaths by race/ethnicity, most have not accounted for the effect of the disproportionate annual growth of the U.S. population by age and race/ethnicity even over short periods and have not focused on disparities (3, 4).
This study was limited by the completeness and availability of data provisionally released by the CDC (30). Vital statistics data remain incomplete for months after the date of death because of reporting delays (9). To overcome this, a lag of 8 months was imposed. Data were not released separately for Native Hawaiians and Pacific Islanders, groups with known health disparities (31), and we were unable to examine potential health disparities within subpopulations of any racial/ethnic group. For example, COVID-19–related health inequalities among Asians by national heritage have been noted (32). Reporting of AI/AN race on death certificates is known to be markedly underestimated, which likely resulted in substantial underestimation of death rates in this group (12). These results should be interpreted with caution until better data become available. Furthermore, although 2020 Census data were released in August 2021, updated estimates for 2019 have not been released; thus, we utilized estimates projected from the 2010 Census that might have resulted in an underestimation or overestimation of excess deaths. Finally, our analysis assumed that deaths divided by population size in 2020 would be the same as in 2019 and may not have captured ongoing temporal trends. This approach was used because of the change in classification of race/ethnicity in death certificate data that precludes the use of data from before 2018 (11). Of note, using data from 2018 and 2019 combined did not notably alter the results. In addition, because of a lack of data from previous years, we were unable to model measures of uncertainty around estimates of excess deaths. However, given that the analysis included all U.S. deaths in 2019 and 2020 and the racial/ethnic differences were substantial, uncertainty estimates are unlikely to have affected our inferences.
In conclusion, we observed profound racial/ethnic disparities in U.S. excess death rates in 2020 during the COVID-19 pandemic. These findings portend severe widening of racial/ethnic disparities in all-cause mortality as longer-term data are released. Although vaccination rates accelerated rapidly during the spring of 2021, racial/ethnic inequities continue and will further drive mortality disparities if not addressed with urgency and cultural competence, as has been done by tribal communities. The disproportionate effect of the pandemic on Black, AI/AN, and Latino communities has been devastating and highlights the urgent need to address long-standing structural inequities.
Footnotes
This article was published at Annals.org on 5 October 2021.
References
- 1.National Center for Immunization and Respiratory Diseases. Risk for COVID-19 Infection, Hospitalization, and Death By Race/Ethnicity (footnote 3). Updated 16 July 2021. Accessed at www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html#footnote03 on 29 March 2021.
- 2.Romano SD , Blackstock AJ , Taylor EV , et al. Trends in racial and ethnic disparities in COVID-19 hospitalizations, by region — United States, March–December 2020. MMWR Morb Mortal Wkly Rep. 2021;70:560-5. [PMID: ] doi: 10.15585/mmwr.mm7015e2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Woolf SH , Chapman DA , Sabo RT , et al. Excess deaths from COVID-19 and other causes in the US, March 1, 2020, to January 2, 2021. JAMA. 2021. [PMID: ] doi: 10.1001/jama.2021.5199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rossen LM , Branum AM , Ahmad FB , et al. Excess deaths associated with COVID-19, by age and race and ethnicity — United States, January 26–October 3, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1522-7. [PMID: ] doi: 10.15585/mmwr.mm6942e2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Shiels MS , Almeida JS , García-Closas M , et al. Impact of population growth and aging on estimates of excess U.S. deaths during the COVID-19 pandemic, March to August 2020. Ann Intern Med. 2021;174:437-43. [PMID: ] doi: 10.7326/M20-7385 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rossen LM , Ahmad FB , Anderson RN , et al. Disparities in excess mortality associated with COVID-19 — United States, 2020. MMWR Morb Mortal Wkly Rep. 2021;70:1114-9. [PMID: ] doi: 10.15585/mmwr.mm7033a2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Centers for Disease Control and Prevention. AH Monthly Provisional Counts of Deaths for Select Causes of Death by Sex, Age, and Race and Hispanic Origin. Updated 3 August 2021. Accessed at https://data.cdc.gov/NCHS/AH-Monthly-Provisional-Counts-of-Deaths-for-Select/65mz-jvh5 on 3 August 2021.
- 8.U.S. Census Bureau. National Population by Characteristics: 2010–2019. Accessed at www.census.gov/data/tables/time-series/demo/popest/2010s-national-detail.html on 13 October 2020.
- 9.Ahmad FB, Dokpesi P, Escobedo L, et al. Timeliness of Death Certificate Data by Sex, Age, and Geography. Vital Statistics Rapid Release. Report no. 009. June 2020.
- 10.U.S. Census Bureau. Methodology. Accessed at www.census.gov/programs-surveys/popest/technical-documentation/methodology.html on 24 November 2020.
- 11.Heron M . Comparability of race-specific mortality data based on 1977 versus 1997 reporting standards. Natl Vital Stat Rep. 2021;70:1-31. [PMID: ] [PubMed] [Google Scholar]
- 12.Arias E , Heron M , Hakes J ; National Center for Health Statistics. The validity of race and Hispanic-origin reporting on death certificates in the United States: an update. Vital Health Stat 2. 2016:1-21. [PMID: ] [PubMed] [Google Scholar]
- 13.National Center for Health Statistics. Technical Notes: Provisional Death Counts for Coronavirus Disease (COVID-19). Accessed at www.cdc.gov/nchs/nvss/vsrr/covid19/tech_notes.htm on 25 August 2021.
- 14.Faust JS, Du C, Li S, et al. Correcting excess mortality for pandemic-associated population decreases. medRxiv. Preprint posted online 12 February 2021. doi:10.1101/2021.02.10.21251461
- 15.Centers for Disease Control and Prevention. Risk for COVID-19 Infection, Hospitalization, and Death By Race/Ethnicity. Updated 16 July 2021. Accessed at www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html on 13 April 2021.
- 16.Arias E, Tejada-Vera B, Ahmad F, et al. Provisional Life Expectancy Estimates for 2020. Vital Statistics Rapid Release. Report no. 015. July 2021.
- 17.Zalla LC , Martin CL , Edwards JK , et al. A geography of risk: structural racism and coronavirus disease 2019 mortality in the United States. Am J Epidemiol. 2021;190:1439-46. [PMID: ] doi: 10.1093/aje/kwab059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.McClure ES , Vasudevan P , Bailey Z , et al. Racial capitalism within public health—how occupational settings drive COVID-19 disparities. Am J Epidemiol. 2020;189:1244-53. [PMID: ] doi: 10.1093/aje/kwaa126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Webb Hooper M, Nápoles AM, Pérez-Stable EJ.. COVID-19 and racial/ethnic disparities. JAMA. 2020;323:2466-7. [PMID: ] doi: 10.1001/jama.2020.8598 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lopez L 3rd, Hart LH 3rd, Katz MH.. Racial and ethnic health disparities related to COVID-19. JAMA. 2021;325:719-20. [PMID: ] doi: 10.1001/jama.2020.26443 [DOI] [PubMed] [Google Scholar]
- 21.Graves JM , Mackelprang JL , Amiri S , et al. Barriers to telemedicine implementation in Southwest tribal communities during COVID-19 [Letter]. J Rural Health. 2021;37:239-41. [PMID: ] doi: 10.1111/jrh.12479 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rodriguez-Lonebear D , Barceló NE , Akee R , et al. American Indian reservations and COVID-19: correlates of early infection rates in the pandemic. J Public Health Manag Pract. 2020;26:371-7. [PMID: ] doi: 10.1097/PHH.0000000000001206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Krieger N , Waterman PD , Chen JT , et al. Missing again: US racial and ethnic data for COVID-19 vaccination [Letter]. Lancet. 2021;397:1259-60. [PMID: ] doi: 10.1016/S0140-6736(21)00465-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Centers for Disease Control and Prevention. Demographic Characteristics of People Receiving COVID-19 Vaccinations in the United States. Accessed at https://covid.cdc.gov/covid-data-tracker/#vaccination-demographic on 4 May 2021.
- 25.Webb Hooper M, Nápoles AM, Pérez-Stable EJ.. No populations left behind: vaccine hesitancy and equitable diffusion of effective COVID-19 vaccines [Editorial]. J Gen Intern Med. 2021;36:2130-3. [PMID: ] doi: 10.1007/s11606-021-06698-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Urban Indian Health Institute. Results from a National COVID-19 Vaccination Survey: Strengthening Vaccine Efforts in Indian Country. Urban Indian Health Institute; 2021.
- 27.Faust JS , Du C , Mayes KD , et al. Mortality from drug overdoses, homicides, unintentional injuries, motor vehicle crashes, and suicides during the pandemic, March–August 2020. JAMA. 2021;326:84-6. [PMID: ] doi: 10.1001/jama.2021.8012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rossen LM, Hedegaard H, Warner M, et al. Early Provisional Estimates of Drug Overdose, Suicide, and Transportation-Related Deaths: Nowcasting Methods to Account for Reporting Lags. Vital Statistics Rapid Release. Report no. 011. February 2021.
- 29.Henley SJ , Ward EM , Scott S , et al. Annual report to the nation on the status of cancer, part I: national cancer statistics. Cancer. 2020;126:2225-49. [PMID: ] doi: 10.1002/cncr.32802 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gerberding JL . Measuring pandemic impact: vital signs from vital statistics [Editorial]. Ann Intern Med. 2020;173:1022-3. [PMID: ] doi: 10.7326/M20-6348 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Wang D , Gee GC , Bahiru E , et al. Asian-Americans and Pacific Islanders in COVID-19: emerging disparities amid discrimination [Editorial]. J Gen Intern Med. 2020;35:3685-8. [PMID: ] doi: 10.1007/s11606-020-06264-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Yee A. COVID's Outsize Impact on Asian Americans Is Being Ignored. Scientific American. 6 May 2021.