

Abstract
Objective Accessory ossicles of the wrist are generally asymptomatic and detected incidentally as radiological findings. These bones are rarely symptomatic but can produce pain in cases of impingement or direct trauma. More frequently, these bones are misinterpreted as avulsion fractures in trauma patients, which may lead to unnecessary immobilization and overtreatment. The aim of this study is to determine the incidence of accessory ossicles of the wrist and also determine if the incidence is related to age, gender, or ongoing wrist pain.
Materials and Methods A total of 1146 wrist radiographs were included in the study. All radiographs were analyzed for the presence of 20 different accessory ossicles of the wrist. Patients were also divided into two groups, as with and without accessory ossicle. Two groups were compared in terms of age, gender, and side.
Results About 113 accessory ossicles were detected in 111 (9.7%) radiographs. The most common accessory ossicles were os triangulare and os ulnostyloideum, and the least common accessory ossicles were os gruberi and os praetrapezium. Patients who had accessory ossicle had a significantly higher age than those who did not have accessory ossicle. There was no significant difference between the patients with and without accessory ossicle in terms of gender and side.
Conclusions The results of this study showed that the most common accessory ossicles in the wrist were os triangulare and os ulnostyloideum, and the incidence of accessory bones increased with age.
Clinical Relevance Since accessory ossicles of the wrist can be confused with fractures in trauma patients and are frequently ignored in patients presenting with pain, it is very important to know the incidence and distribution of these ossicles. Therefore, this study is important, in that it provides potentially guiding anatomical data for clinicians in terms of diagnosis and management.
Keywords: accessory ossicles, wrist, radiography, incidence
There are more than 20 known accessory ossicles in the wrist. 1 Since most of these accessory ossicles originate from unfused secondary ossification centers, they can be considered developmental anomalies. These ossicles are generally asymptomatic and detected incidentally as radiological findings. They can rarely become symptomatic due to impingement, trauma and such causes. However, a more common problem in routine practice is that accessory ossicles can be misinterpreted as avulsion fractures in trauma patients, which may lead to overtreatment or the use of cross-sectional imaging modalities such as CT that causes further radiation exposure. Therefore, it is very important to know the localization, frequency, and distribution of accessory ossicles.
While there are numerous studies on the distribution and incidence of accessory ossicles of the foot and ankle conducted with large patient series, the number of studies about the accessory ossicles of the wrist is limited in the literature. 2 3 Most of these studies are case reports, whereas there are only two studies involving a large patient series. 4 5 6 7 Both of these studies are considerably old dated (1932, 1953) and were performed using conventional radiography. 8 9 To the best of our knowledge, there are no recent large patient series investigating the distribution and incidence of accessory ossicles of the wrist with the use of digital radiography.
The aim of this study is to determine the distribution and incidence of accessory ossicles of the wrist and whether there is a relationship between the incidence, age, gender, and side.
Materials and Methods
This retrospective study was approved by the Institutional Review Board of our hospital (IRB#672). Due to the retrospective nature of the study, informed consent was not required from the patients and providers.
Patient Inclusion
Patients who had a plain wrist radiography due to acute or chronic wrist pain between March 2019 and January 2020 were retrospectively evaluated. Patients who received conservative or surgical treatment for a fracture in the wrist, those who had a congenital anomaly in the wrist, and patients below 18 years of age were excluded from the study. A total of 1146 wrists from 1146 patients who did not satisfy the exclusion criteria were included. All patients had posteroanterior (PA) and lateral plain wrist radiographs.
Radiographic Evaluation
The 20 most common accessory bones of the wrist were detected on direct radiographs as follows ( Fig. 1 ):
Fig. 1.
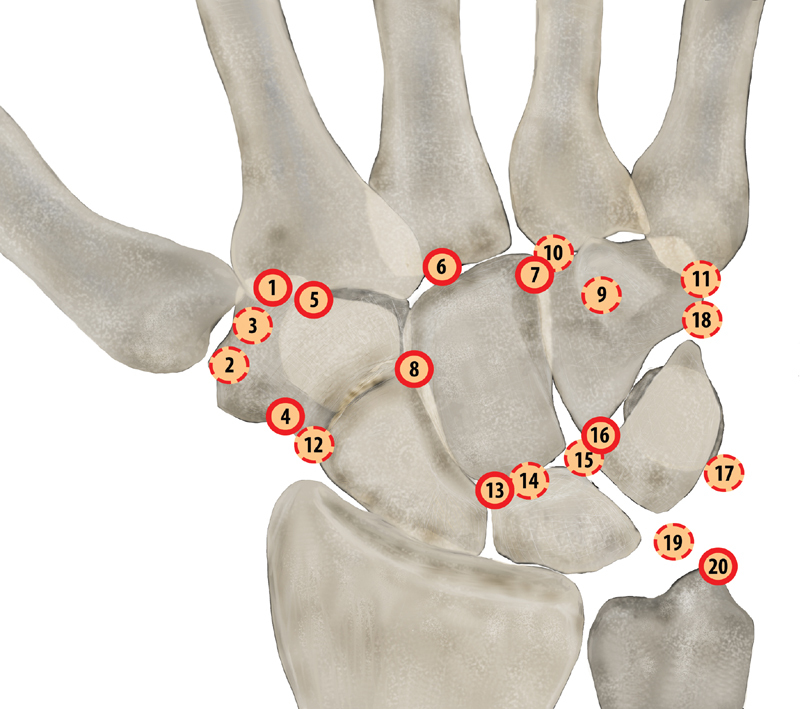
Schematic illustration of dorsal aspect of the right hand, showing the accessory ossicles of the wrist. Palmar-located accessory ossicles are shown in broken outline. (1: Os trapezium secundarium, 2: Os paratrapezium, 3: Os praetrapezium, 4: Os epitrapezium, 5: Os trapezoideum secundarium, 6: Os styloideum, 7: Os capitatum secundarium, 8: Os centrale carpi, 9: Os hamuli proprium, 10: Os gruberi, 11: Os vesalianum manus, 12: Os radiale externum, 13: Os epilunatum, 14: Os hypolunatum, 15: Os hypotriquetrum, 16: Os epitriquetrum, 17: Os pisiforme secundarium, 18: Os ulnare externum, 19: Os triangulare, 20: Os ulnostyloideum).
Os trapezium secundarium: between the bases of the first and second metacarpal bones at the superomedial aspect of the trapezium.
Os paratrapezium: between the trapezium and the radial aspect of the base of the first metacarpal bone ( Fig. 2 ).
Os praetrapezium: between the distal trapezium and the central portion of the base of the first metacarpal.
Os epitrapezium: on the dorsolateral side of the trapezium, at the distal lateral aspect of the scaphoid in close proximity to the trapezium.
Os trapezoideum secundarium: between the trapezium, trapezoid, and the bases of the first and second metacarpal bones.
Os styloideum: between capitate, trapezoid, and bases of second and third metacarpal bones ( Fig. 3 ).
Os capitatum secundarium: between the capitate and bases of the third and fourth metacarpal bones at the radiodistal margin of the hamate body.
Os centrale carpi: in the dorsal aspect of the space between scaphoid, capitate, and trapezoid.
Os hamuli proprium: secondary ossification center in the hook of the hamate that does not fuse with the hamate body and located in the palmar aspect of the midbody.
Os gruberi: between the hamate, capitate, and the base of the third and fourth metacarpals.
Os vesalianum manus: at the lateral aspect of the carpus, between the base of the fifth metacarpal and the hamate.
Os radiale externum: on the radial side, adjacent to the space between the scaphoid and trapezium ( Fig. 4 ).
Os epilunatum: between the lunate, scaphoid and capitate, along the distal border of the scaphoid and lunate.
Os hypolunatum: between the lunate and the capitate, just ulnar to the site of the os epilunatum.
Os hypotriquetrum: in the vicinity of the lunate, capitate, proximal pole of the hamate, and triquetrum.
Os epitriquetrum: between the lunate, hamate and the triquetrum, just ulnar to the site of the os hypotriquetrum.
Os pisiforme secundarium (os ulnare antebrachii): between the distal ulna and pisiform, close to the proximal edge of the pisiform.
Os ulnare externum: at the distal end of the triquetrum and adjacent to the ulnar border of the distal hamate.
Os triangulare (os intermedium antebrachii, os triquetrum secundarium): distal to the head of the ulna, between the ulnar head, lunate and triquetrum ( Fig. 5 ).
Os ulnostyloideum (persistent ulnar styloid ossicle): in the vicinity of ulnar styloid ( Fig. 6 ).
Fig. 2.

Posteroanterior radiograph of the wrist shows an os paratrapezium (arrow) between the trapezium and the radial aspect of the base of the first metacarpal bone.
Fig. 3.

Posteroanterior radiograph of the wrist shows an os styloideum (circled) located between the capitate, trapezoid, and bases of second and third metacarpal bones.
Fig. 4.

Posteroanterior ( A ) and lateral ( B ) radiographs of the wrist show an os radiale externum (arrow) between the scaphoid and trapezium on the radial side.
Fig. 5.

Posteroanterior radiograph of the wrist shows an os triangulare distal to the ulnar head (arrow).
Fig. 6.

Posteroanterior radiograph of the wrist shows an os ulnostyloideum distal to the ulnar styloid.
All radiographs were analyzed by a radiologist and anatomist for the presence of accessory ossicles and confirmed by a radiologist who had 20 years of experience in musculoskeletal radiology. Incidences were determined for the detected accessory ossicles. Patients were also divided into two groups, as with and without accessory ossicle. Two groups were compared in terms of age, gender, and side.
Statistical Analysis
The data were analyzed using Statistical Package for Social Sciences (SPSS), version 24.0, software (IBM, Armonk, NY). The Mann–Whitney U test was used to determine if there was a statistically significant difference between the patients with and without accessory ossicles in terms of mean age. Chi-square test was used to determine if there was a difference between genders and sides in terms of the incidence of accessory ossicles. A probability of the null of p ≤ 0.05 was considered statistically significant.
Results
The study group consisted of 1146 patients (600 women [52.4%], 546 men [47.6%]; mean age = 42.6 years; age range = 18–90 years) with 1146 wrist radiographs. Of the 1146 wrist radiographs, 652 belonged to the right side (56.9%) and 494 to the left side (43.1%). 1035 (90.3%) of the 1146 wrist radiographs did not have any accessory ossicles, whereas 113 accessory ossicles were detected in 111 (9.7%) radiographs. Only two patients had more than one accessory ossicle in the same wrist. Of these two patients, one had os triangulare and os paratrapezium, and the other had os ulnare externum and os vesalianum manus. None of the patients had three or more accessory ossicles. The most common accessory ossicles were os triangulare (28/1146, 2.4%) and os ulnostyloideum (17/1146, 1.5%), whereas the least common accessory ossicles were os gruberi (1/1146, 0.1%) and os praetrapezium (1/1146, 0.1%). The quantitative distribution of accessory ossicles is shown in Table 1 .
Table 1. Incidence of accessory ossicles of the wrist.
| Accessory ossicles | Incidence | Gender ( n ) | Side ( n ) | ||
|---|---|---|---|---|---|
| F | M | R | L | ||
| Os triangulare | 28 (2.4%) | 17 | 11 | 16 | 12 |
| Os ulnostyloideum | 17 (1.5%) | 7 | 10 | 7 | 10 |
| Os radiale externum | 9 (0.8%) | 5 | 4 | 4 | 5 |
| Os pisiforme secundarium | 9 (0.8%) | 6 | 3 | 5 | 4 |
| Os paratrapezium | 8 (0.7%) | 6 | 2 | 4 | 4 |
| Os styloideum | 8 (0.7%) | 2 | 6 | 4 | 4 |
| Os centrale carpi | 7 (0.6%) | 4 | 3 | 2 | 5 |
| Os capitatum secundarium | 6 (0.5%) | 4 | 2 | 4 | 2 |
| Os ulnare externum | 4 (0.3%) | 2 | 2 | 3 | 1 |
| Os vesalianum manus | 4 (0.3%) | 2 | 2 | 3 | 1 |
| Os trapezium secundarium | 3 (0.3%) | 2 | 1 | 2 | 1 |
| Os hypotriquetrum | 2 (0.2%) | 1 | 1 | 2 | − |
| Os hypolunatum | 2 (0.2%) | 1 | 1 | 1 | 1 |
| Os epilunatum | 2 (0.2%) | 2 | – | 1 | 1 |
| Os epitrapezium | 2 (0.2%) | 2 | – | 1 | 1 |
| Os gruberi | 1 (0.1%) | 1 | – | – | 1 |
| Os praetrapezium | 1 (0.1%) | 1 | – | – | 1 |
| Os hamuli proprium | – | – | – | – | – |
| Os trapezoideum secundarium | – | – | – | – | – |
| Os epitriquetrum | – | – | – | – | – |
Abbreviations: F, female; L, left; M, Male; n , number of patients; R, right.
Considering all accessory ossicles, there was no statistically significant difference between the patients with and without accessory ossicle in terms of gender and side ( p = 0.187, p = 0.976, respectively). With respect to the mean age of the patients with and without accessory ossicles, patients who had accessory ossicles had a significantly higher age than those who did not have accessory ossicles ( p = 0.009) ( Table 2 ).
Table 2. Patient demographics.
| With accessory ossicle | Without accessory ossicle | p -Value | |
|---|---|---|---|
| Age, mean ± SD | 46.7 (SD 17.2) | 42.2 (SD 17.4) | 0.009 |
| Gender | |||
| Female | 64 (57.7%) | 536 (51.8%) | 0.187 |
| Male | 47 (42.3%) | 499 (48.2%) | |
| Side | |||
| Right | 63 (56.8%) | 589 (56.9%) | 0.976 |
| Left | 48 (43.2%) | 446 (43.1%) | |
Abbreviation: SD, standard deviation.
There was no statistically significant difference between the age groups, genders, and sides in terms of the presence of os triangulare and os ulnostyloideum, that is, the most common accessory ossicles ( p > 0.05).
Discussion
The incidence of accessory ossicles of the wrist varies in the literature. In a study by O'Rahilly et al conduced in 1953, 743 plain radiographs were analyzed, and the incidence of accessory ossicles of the wrist was reported to be 1.6%. 9 Moreover, the same was calculated to be 0.3% in another study by Bogart et al conducted with 1452 radiographs in 1932. 8 These studies were performed at the time of analog radiography and are, therefore, considerably old dated. In the present study, the incidence of accessory ossicles of the wrist was found to be 9.7% among 1146 radiographs. We are of the opinion that the most important reason for the significant difference between the results of this study and other previous studies is the technological advancements in radiography techniques. We also believe that better image quality in digital radiography as compared with conventional radiography has enhanced the visibility of accessory ossicles on radiographs. Therefore, this study reported a higher number of accessory ossicles with a higher incidence. The fact that the studies were conducted with populations of different ethnic origins can be another reason for the difference between the reported incidence values. The number of existing studies is not sufficient to determine if there is a difference between ethnic groups in terms of the accessory ossicles of the wrist. However, there are numerous studies on accessory ossicles of the foot or sesamoid bones of the hand conducted with different populations, reporting different incidences. 2 3 10 11 12 The present study was conducted on the Turkish population, which may have had an impact on the different incidence obtained.
In this study, the most common accessory ossicles were os triangulare and os ulnostyloideum. Both ossicles are in close vicinity of the ulnar styloid process. Since ulnar styloid process fractures, various ossifications, and dystrophic/heterotopic calcifications are also localized in this area, a clear distinction needs to be made. Especially, these ossicles may be very difficult to distinguish from a fractured ulnar styloid process. Some characteristics of accessory bones can be of higher benefit in differential diagnosis, as accessory bones have well-defined, regular contours, whereas the contours of a fracture are irregular; while accessory bones have a cortex, cortical continuation cannot be seen on at least one surface of a fracture. Bogart et al found only two os triangulare (0.1%) on 1452 plain radiographs. 8 In addition, Aydinlioglu et al analyzed 388 plain radiographs to investigate the incidence of os ulnostyloideum, which was found to be 2.5%. 13 In the present study, the incidence of os triangulare and os ulnostyloideum were 2.4% and 1.5%, respectively.
The literature does not provide the incidence for each accessory ossicle. Therefore, it was not possible to compare the incidence of all 17 accessory ossicles that were investigated in this study with the literature. One of the accessory ossicles that was relatively common in this study and discussed relatively more in the literature was os styloideum. The clinical significance of os styloideum stems from its relationship with carpal boss, which is a painful lump in the dorsum of the wrist. While os styloideum is defined as a separate ossicle (may have a fibrous connection with metacarpal bones or carpus), carpal boss is defined as a bony protuberance, fused to the base of the metacarpal bones. Lawson stated that the incidence of os styloideum in the normal wrist is in the range of 1.3 to 3%. 14 In this study, the incidence of os styloideum was found to be 0.7%. Greditzer et al conducted a study with 16 National Hockey League players and found os styloideum in 13 of the players (81%). 15 Similar to the results obtained in the present study, this incidence was markedly higher than the results of previous studies conducted with the general population. Although the etiology of os styloideum is not entirely clear, the authors explained it with adaptive and reactive bone formation, similar to the formation of cam type deformity in the hip due to increased loading and repeating microtrauma in these athletes.
Os centrale carpi is generally associated with other congenital anomalies (Holt–Oram syndrome, hand-foot-uterus syndrome, etc.) and is rarely an isolated finding. 16 To the best of our knowledge, there is no information about the incidence thereof. Therefore, our study is the first one to report an incidence of os centrale carpi, which was found in seven patients, leading to an incidence of 0.6%. Os centrale carpi can be confused with scaphoid fractures or can cause pain due to osteonecrosis, which constitute the clinical significance thereof. 4 17 18 Linear and irregular lucent areas superposed on the scaphoid waist due to os centrale carpi may make it challenging to distinguish between this ossicle and transverse, ununited scaphoid fractures. 4 However, an acute scaphoid fracture usually shows noncorticated sharp or irregular margins. An os centrale carpi generally has better-defined cortical margins and is usually round, dense, and structureless. On the other hand, although old fractures generally exhibit demineralization and cyst formation, it is not always possible to differentiate between these fractures and os centrale carpi, particularly in patients with no history of trauma. CT can be beneficial in such cases.
Os epilunatum is another rare ossicle investigated in this study, which was detected only in two patients (0.2%). Bogart et al did not find an os epilunatum in a patient series with 1452 radiographies. 8 Mauler et al stated that accessory ossicles constituted an important differential diagnosis in chronic wrist pain and presented the first case that manifested with inflammatory changes and synovitis around the os epilunatum. 6 It was also stated that another important point to consider in patients complaining about pain due to os epilunatum was concomitant scapholunate ligament tears. 6 Therefore, it is essential to examine the adjacent anatomical structures when an accessory ossicle is identified, particularly in patients who planned to undergo surgical excision.
In this study, there was no significant difference between the patients with and without accessory ossicles in terms of gender and side. On the other hand, mean age was higher among patients who had accessory ossicles than those who did not have the same. According to a study by Sun et al, investigating the distribution patterns of sesamoid bones in metatarsophalangeal (MTP) joints, the number of sesamoid bones and number of MTP joints with sesamoids had a positive correlation with age, wherein it was reported that the number of sesamoid bones and affected joints increased parallelly to age. 19 Ossification of accessory ossicles and sesamoids typically begins before the age of 20 years and continues throughout the lifetime. These bones become visible on radiographs once ossified. Sun et al considered the positive correlation they obtained an indicator of the fact that sesamoid ossification also continues after the age of 20 years. 19 Our study also provided a similar result, which suggests that accessory bone ossification is a lifelong process.
This study had some limitations. It was retrospective in design and involved unilateral standard plain radiographic images. The incidence of bilateral accessory ossicles could not be discussed, since the radiographs employed in this study were unilateral. In addition, bilateral imaging could have provided higher incidence values. Another limitation of the study is that radiographs were obtained from patients presenting with trauma or local symptoms of the wrist. A study conducted with healthy individuals without a history of trauma or any symptoms may have a stronger design. However, the most important limitation of such a study will be that it includes additional radiation dose. The strengths of our study are that it has a large sample size and provides incidence information for many accessory ossicles that was not provided in the literature.
In conclusion, the present study represents the first detailed report on the incidence of accessory ossicles of the wrist on digital radiography, with particular emphasis on their clinical significance. Accessory ossicles of the wrist can be confounding, since they can be confused with fractures in trauma patients and are frequently ignored in patients presenting with pain. Therefore, this study is important, in that it provides potentially guiding anatomical data for clinicians in terms of diagnosis and management. The results of this study showed that the most common accessory ossicles in the wrist were os triangulare and os ulnostyloideum, and the incidence of accessory bones increased with age.
Funding Statement
Funding None.
Conflict of Interest None declared.
Note
The study was performed at the Izmir Katip Celebi University, Ataturk Training and Research Hospital.
Ethical Review Approval
This retrospective study was approved by the Institutional Review Board of Izmir Katip Celebi University (IRB#672). Due to the retrospective nature of the study, informed consent was not required from the patients and providers.
Authors' Contributions
M.G. and I.C. researched literature and conceived the study. M.G., I.C., and T.B. were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. M.G. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
References
- 1.Freyschmidt J, Sternberg A, Brossmann J, Wiens J. 4th ed. New York, NY: Thieme Verlag; 1993. Köhler/Zimmer Borderlands of Normal and Early Pathologic Findings in Skeletal Radiography; pp. 79–93. [Google Scholar]
- 2.Coskun N, Yuksel M, Cevener M. Incidence of accessory ossicles and sesamoid bones in the feet: a radiographic study of the Turkish subjects. Surg Radiol Anat. 2009;31(01):19–24. doi: 10.1007/s00276-008-0383-9. [DOI] [PubMed] [Google Scholar]
- 3.Koo B S, Song Y, Lee S, Sung Y K, Sung I H, Jun J B. Prevalence and distribution of sesamoid bones and accessory ossicles of the foot as determined by digital tomosynthesis. Clin Anat. 2017;30(08):1072–1076. doi: 10.1002/ca.22952. [DOI] [PubMed] [Google Scholar]
- 4.Abascal F, Cerezal L, del Piñal F. Unilateral osteonecrosis in a patient with bilateral os centrale carpi: imaging findings. Skeletal Radiol. 2001;30(11):643–647. doi: 10.1007/s002560100423. [DOI] [PubMed] [Google Scholar]
- 5.Karmazyn B, Siddiqui A R. Painful os styloideum in a child. Pediatr Radiol. 2002;32(05):370–372. doi: 10.1007/s00247-001-0639-6. [DOI] [PubMed] [Google Scholar]
- 6.Mauler F, Rahm S, Schweizer A, Nagy L. Bilateral symptomatic os epilunatum: a case report. J Wrist Surg. 2015;4(01):68–70. doi: 10.1055/s-0034-1543978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nicolodi G C, Trippia C R, Caboclo M FFS, de Lima R R, Miller W P. Carpal boss syndrome: os styloideum fused to the trapezoid. Radiol Bras. 2017;50(03):200–201. doi: 10.1590/0100-3984.2015.0160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bogart F B. Variations of the bones of the wrist. AJR Am J Roentgenol. 1932;28:638–646. [Google Scholar]
- 9.O'Rahilly R. A survey of carpal and tarsal anomalies. J Bone Joint Surg Am. 1953;35-A(03):626–642. [PubMed] [Google Scholar]
- 10.Amar E, Rozenblat Y, Chechik O. Sesamoid and accessory bones of the hand--an epidemiologic survey in a Mediterranean population. Clin Anat. 2011;24(02):183–187. doi: 10.1002/ca.21077. [DOI] [PubMed] [Google Scholar]
- 11.Dharap A S, Al-Hashimi H, Kassab S, Abu-Hijleh M F. Incidence and ossification of sesamoid bones in the hands and feet: a radiographic study in an Arab population. Clin Anat. 2007;20(04):416–423. doi: 10.1002/ca.20378. [DOI] [PubMed] [Google Scholar]
- 12.Lee J H, Kyung M G, Cho Y J, Go T W, Lee D Y. Prevalence of accessory bones and tarsal coalitions based on radiographic findings in a healthy, asymptomatic population. Clin Orthop Surg. 2020;12(02):245–251. doi: 10.4055/cios19123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aydinlioglu A, Ragbetli M C, Akpinar F, Tosun N, Dogan A. The accessory ulnar styloid process. Ulus Travma Acil Cerrahi Derg. 1998;4:53–57. [Google Scholar]
- 14.Lawson J P. International Skeletal Society Lecture in honor of Howard D. Dorfman. Clinically significant radiologic anatomic variants of the skeleton. AJR Am J Roentgenol. 1994;163(02):249–255. doi: 10.2214/ajr.163.2.8037009. [DOI] [PubMed] [Google Scholar]
- 15.Greditzer H G, IV, Hutchinson I D, Geannette C S, Hotchkiss R N, Kelly B T, Potter H G. Prevalence of os styloideum in national hockey league players. Sports Health. 2017;9(05):469–473. doi: 10.1177/1941738117707914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Poznanski A K, Holt J F. The carpals in congenital malformation syndromes. Am J Roentgenol Radium Ther Nucl Med. 1971;112(03):443–459. doi: 10.2214/ajr.112.3.443. [DOI] [PubMed] [Google Scholar]
- 17.Lane L B, Gould E S, Stein P D, Coffey E. Unilateral osteonecrosis in a patient with bilateral os centrale carpi. J Hand Surg Am. 1990;15(05):751–754. doi: 10.1016/0363-5023(90)90150-p. [DOI] [PubMed] [Google Scholar]
- 18.Yang Z Y, Gilula L A, Jonsson K. Os centrale carpi simulating a scaphoid waist fracture. J Hand Surg [Br] 1994;19(06):754–756. doi: 10.1016/0266-7681(94)90252-6. [DOI] [PubMed] [Google Scholar]
- 19.Sun T, Zhao H, Wang L, Wu W, Hu W. Distribution patterns and coincidence of sesamoid bones at metatarsophalangeal joints. Surg Radiol Anat. 2017;39(04):427–432. doi: 10.1007/s00276-016-1759-x. [DOI] [PubMed] [Google Scholar]