

Abstract
Introduction:
This trial assesses effects of a community-level alcohol prevention intervention in California on alcohol-related motor vehicle crashes.
Study Design:
The study is a group RCT with cities as the unit of assignment to condition and as the unit of analysis.
Setting/participants:
Twenty-four California cities with populations between 50,000 and 450,000 were chosen at random and roughly matched into pairs before randomly assigning 12 each to the intervention and control conditions.
Intervention:
The intervention, aimed at reducing excessive drinking among adolescents and young adults, included driving under the influence sobriety checkpoints, saturation patrols, and undercover operations to reduce service of alcohol to intoxicated patrons in bars, all including high visibility so the public would be aware of them. A measure of overall intervention intensity or “dosage” was created.
Main Outcome Measure:
The outcome was a monthly percentage of all motor vehicle crashes that were single vehicle night-time crashes for drivers aged 15–30 years.
Results:
Multilevel analyses were conducted to examine intervention effects on alcohol-related crashes among drivers aged 15–30 years. Crash data were obtained in 2018 with data preparation and analysis conducted in 2019. Intent-to-treat analyses indicated a 17% reduction in the percentage of alcohol-involved crashes among drivers aged 15–30 years relative to controls, which translates to about 310 fewer crashes. Dosage was found to have a statistically significant effect on crashes among this age group, although not in the expected direction.
Conclusions:
Enhanced alcohol enforcement operations involving both community health and law enforcement agencies can help to reduce alcohol-impaired driving and related consequences among young people. Including measures of intervention dosage raises interesting questions about the understanding of the impact of the community intervention. Future studies should continue to further develop implementation strategies that may more effectively and efficiently reduce community alcohol-related harm.
INTRODUCTION
Reducing alcohol-impaired driving and related consequences, including motor vehicle crashes, injuries, and fatalities, continues to be a public health priority.1 It is estimated that about 29 people die in an alcohol-impaired driving crash in the U.S. each day.1 The trend in alcohol-related motor vehicle fatalities has leveled off since 2010 with about 10,000 deaths occurring each year, representing about 30% of all traffic deaths.2,3 The majority of alcohol-related traffic fatalities occur among young drivers. For example, in 2017, a total 68% of drivers in alcohol-related motor vehicle fatalities were aged 16–34 years.2,3 The concern about impaired driving has led to increased attention to identifying effective interventions and the best ways to implement them.
Environmental prevention intervention programs can be effective to ameliorate the consequences of alcohol use, abuse, and addiction, including alcohol-impaired driving.4–7 In the U.S., it is at the geographic levels of neighborhoods and cities where the burden of alcohol use, misuse, and problems is most keenly felt, but also where policies at all levels (e.g., state, federal) to address them may succeed or fail.8,9 Environmental efforts at the neighborhood and city level may include enforcement activities to reduce the ability of youths to purchase alcohol,10 efforts to target risks related to sales or service of alcohol (e.g., responsible beverage service programs),11 and efforts to ameliorate problem hot spots.12 Environmental approaches often focus on acute rather than chronic problems related to use. Such problems include motor vehicle crashes, injuries, and violence rather than alcohol use or misuse per se.
Research and evaluation of prevention interventions have demonstrated the efficacy of environmental strategies at the community level. Using a variety of case comparison research methods, the early phase of this research included the Saving Lives Program,13 the Communities Mobilizing for Change on Alcohol project,14 and the Community Trials project.15 More recent examples of community prevention include the Operation Safe Crossing project in San Diego, California,16 the Sacramento Neighborhood Alcohol Prevention Project,17 the Stockholm Prevents Alcohol and Drug Problems,18–21 the Safer California Universities Project,22 the Reducing Youth Access to Alcohol Project in Oregon,23 and the Study to Prevent Alcohol-Related Consequences in North Carolina.24
It must be added that some efforts at replication have not met with the same success.25–27 Reviews of community prevention of harmful alcohol consumption are challenged by the variety of strategies implemented and outcome measures used across studies. Although one review cited “a number of positive outcomes,” the authors noted that most only demonstrated short-term effects with many questions about sustainability and the required “dosage” for achieving those effects.28 Another review was less sanguine, concluding that effects were generally small and limited to harmful consequences of alcohol rather than consumption per se.29
A partnership with the state of California’s Department of Alcohol and Drug Programs, with funding from the U.S. Substance Abuse and Mental Health Services Administration, allowed the researchers to design and implement a randomized community trial that had several novel features in its implementation. The overall goal of the grant was to develop a systematic approach to prevention that would expedite the adoption of evidence-based prevention strategies and their effective implementation.
The grant focused on reducing excessive drinking among young people aged 12–25 years, with priority given to the drinking that creates the greatest risk to the community. This age group represents a peak in risky drinking. In 2018, among those aged 12–17 years, 4.7% were considered binge drinkers (≥5 drinks in a row for men, ≥4 for women in the prior 30 days); the prevalence among those aged 18–25 years jumped to 34.9% and then dropped among those aged >25 years to 25.1%.30
The grant also required achieving community-level change in 1 or 2 years, and that those changes (reductions) would be documented via community-level archival records, including alcohol-related traffic crashes, injuries, and crimes (e.g., assaults). This paper reports on the multicomponent intervention’s effect on alcohol-related motor vehicle crash rates among drivers aged 15–30 years and among all drivers, and whether the level of intervention implementation (expressed as “dosage”) was related to that outcome.
METHODS
Study Sample
Investigators conducted an RCT from 2013 to 2016 with 24 medium-sized cities (50,000–450,000 population) in California to evaluate high-visibility alcohol enforcement operations aimed at reducing excessive drinking, drinking and driving, and alcohol-related motor vehicle crashes. The research protocol was reviewed and approved by the IRB of the Pacific Institute of Research and Evaluation.
The selection of medium-sized cities was practical in that the researchers felt that very large or smaller cities would pose difficulties for the evaluation. Senior decision makers in very large cities might be difficult to reach, whereas very small cities may not have the resources to implement the intervention components and might have too few adverse outcomes to have measures sufficiently sensitive to the interventions. There were 138 cities of medium size in the 2000 Census. Among those, more than half are in the 4 largest counties (Los Angeles [36]), Orange [18], San Bernardino [11], and San Diego [11]). In order to form a short list of manageable size, and to reduce the dominance of the largest counties, researchers then created a subset of 50 cities through a process of random selection, modified to avoid selecting 2 adjoining cities. The resulting 50 communities were thus more widely distributed throughout the state than had a simple random sample been drawn. Demographic, survey, and archival records were consolidated for the 50 communities in order to determine which may be candidates for selection based on need; that is, with the prevalence of alcohol-related problems (high consumption, alcohol-related crashes, underage drinking) in the upper half of the sample. Cities were roughly matched via cluster analysis using a combination of demographic characteristics (e.g., population size, ethnic composition) and the alcohol problem indicators. Using the distances generated from the analysis, 12 such pairs were created, and the final set of intervention communities was chosen via random selection of 1 from each pair.
Alcohol enforcement operations conducted by local enforcement agencies included driving under the influence (DUI) sobriety checkpoints and saturation patrols to reduce drink driving, and undercover operations in bars or other licensed on-premises establishments to reduce alcohol service to obviously intoxicated patrons. Visibility activities included publicizing local enforcement operations through various media channels (e.g., radio, social media, mobile signs, marquees at high schools), periodic bar visits by local enforcement officers, and letters to owners/managers of licensed on-premises establishments. In most intervention cities, a community-based organization was also involved in publicizing enforcement operations in collaboration with local enforcement agencies. Enforcement agencies and community-based organizations were expected to implement at least 2 high-visibility enforcement operations per quarter. The primary outcome of interest was alcohol-related motor vehicle crashes.
Intervention
The State of California set a budget of approximately $95,000 per year for each community randomly chosen as an intervention site. It was standard practice for the state offices to allocate prevention funding to county health departments, so in this case, officers of the counties within which the intervention communities were located were given the option of collaborating on the study. Several county offices took the option and began designating internal staff or external agencies even before the research team contacted them. In cases where the county declined participation, the research team identified and recruited local agencies to take the lead (e.g., police departments, service agencies). There was thus considerable variability in the mechanisms whereby the community interventions would be implemented.
Achieving community-level reductions in alcohol-related harm would not be trivial and required the project to adopt alcohol control measures that have proven capable of effecting community-level change. In the context of the limited time to achieve community-level effects, and that the intervention communities were selected at random resulting in varying levels of interest and capacity, a key aspect of implementation was adopting implementation “drivers”31 in a prescriptive approach that made use of logic models specifying which intervention components would be used in all communities. During the orientation and early phase of implementation, the research team felt that the use of the logic models had generally succeeded in keeping communities focused on the selected interventions, avoiding (for the most part) competing strategies and activities that could have taken up the limited resources available for the project. It was more difficult to gauge the level of enthusiasm community members may have had for the prescribed interventions.
The logic models (Appendix Figures 1 and 2), the first for reducing underage alcohol consumption and the second for reducing alcohol-impaired driving (aimed at young adults), identified key targets based on research literature. The targets were to: (1) enhance enforcement of drinking and driving laws, (2) improve retail serving practices, (3) reduce social availability especially to minors, and (4) reduce retail availability to minors. Two options were given to communities for each target (e.g., minor decoy operations versus non-enforcement purchase surveys). One of the 2 options was usually the more effective but either more costly or difficult, so another option was provided. Random roadside DUI checkpoints are more effective than saturation patrols but the latter are easier to conduct. The options were provided to allow for local conditions that may have prohibited the preferred option. The targets (e.g., reducing retail availability) were retained and served to constrain attractive but irrelevant alternatives (Appendix Table 1 provides a list of the options for each main target).
It is obvious that the interventions required cooperation from local police departments and, in some cases, local offices of the state department of alcoholic beverage control. Local resources to conduct the enforcement operations varied across the cities and over time, but participation was generally good.
During the planning phase and thereafter, community partners were told that the enforcement operations by themselves were not effective unless accompanied by high visibility publicity about the fact that those operations were taking place. The point was not to catch violators, but rather to maximize deterrence. Visibility was achieved in a variety of ways, including public service announcements on radio, announcements at high school sporting events, and portable marquees (on trailers) to warn of local DUI enforcement. In most cities, there was a division of labor in which law enforcement agencies carried out the operations, while a local prevention agency took responsibility for obtaining the visibility.
Research to guide the number of operations required to achieve an impact was sparse or nonexistent. The research team requested communities to implement at least 2 operations per quarter with accompanying relevant publicity.
Measures
Researchers used data from the California Statewide Integrated Traffic Records System to create a monthly measure of alcohol-related motor vehicle crashes for each city from January 2010 through April 2016, just after intervention activities ended (1,824 observations). Specifically, they computed the percentage of all motor vehicle crashes that were single vehicle night-time crashes for drivers aged 15–30 years (and also for all drivers). Though the top of the target age was 25 years, researchers raised the age to increase the number of crashes for analysis and reduce possible noise and floor effects. It is also the case that those who were aged 25 years at the start of the project aged over the years it was in effect. Single vehicle night-time (SVN) crashes are a commonly used and valid proxy for alcohol-related motor vehicle crashes when blood alcohol concentration data for drivers are not available and assessment of driver impairment is only based on the judgment of law enforcement officers for non-injury and non-fatal crashes.32
A continuous time variable representing 76 months was created for analyses. Additionally, based on seasonal variation in SVN crashes, this study included a dummy variable for early fall months (September/October) as SVN crash rates were consistently lowest in these months from 2010 to 2016.
An intent-to-treat intervention condition variable was coded 0 for all 76 months for the 12 control cities and only for pre-intervention months for the 12 intervention cities. The intervention condition variable was coded 1 for post-intervention months for the 12 intervention cities.
Monthly intervention activities were reported by local enforcement agencies and community-based organizations from April 2013 through March 2016. The average number of monthly intervention activities specifically related to drink driving was calculated for each city. Cities were then classified as meeting a minimum average threshold of 2 high-visibility DUI enforcement operations per quarter or not meeting this threshold over the 3-year period. Of the 12 intervention cities, 5 implemented <2 high-visibility DUI enforcement operations per quarter and 7 implemented ≥2 high-visibility DUI operations per quarter. Two dummy variables were created for intervention cities to represent ≥2 high-visibility DUI operations per quarter or <2 high-visibility DUI operations per quarter.
City demographic characteristics included population size, percentage ethnic minority, and a standardized SES factor score based on percentage of residents living above poverty, percentage employed, percentage with a college degree, and median household income. These characteristics were based on 2011 Census data.
Statistical Analysis
Descriptive statistics for the 24 cities were first examined, including a comparison of cities in intervention and control conditions. Multilevel Poisson regression analyses were conducted to examine whether the intervention had an effect on alcohol-related motor vehicle crashes among drivers aged 15–30 years. The initial intent-to-treat model included intervention condition with time and the seasonal dummy variable at the observation level and city-level characteristics included as covariates. The second model included intervention dosage level at the observation level along with the same covariates included in the initial model. Analyses were conducted in HLM version, 8.0 software, allowing for random effects to account for variance attributable to correlation of repeated observations nested within cities and random variation in outcome slopes between cities. Robust SEs were used to account for the non-normal distribution of dependent variables. Crash data were obtained in 2018 with data preparation and analysis conducted in 2019.
RESULTS
Descriptive statistics for city characteristics are provided in Table 1. There were no statistically significant differences in demographic characteristics between cities in intervention and control conditions, though the SES factor score was somewhat higher for intervention cities. The unadjusted pre-intervention percentages of SVN/total crashes for drivers aged 15–30 years were also not significantly different for intervention and control cities. Drivers aged 15–30 years were involved in 57.6% of all motor vehicle crashes and 44% of SVN crashes in intervention cities during the study period; these figures were 61.3% and 46.9%, respectively, in control cities.
Table 1.
City Characteristics by Intervention Condition, Mean (SD) or Percent
| Variable | Total sample (N=24) |
Intervention (n=12) |
Control (n=12) |
|---|---|---|---|
| Population size | 103,132 (45,555) | 104,512 (44,484) | 101,751 (48,540) |
| Percent ethnic minority | 27.32 (11.69) | 26.88 (10.62) | 27.76 (13.15) |
| SES factor scorea | 0.0 (1.0) | 0.17 (0.81) | −0.17 (1.17) |
| SVN/total crashes (%)b 15–30 year olds | |||
| Pre-intervention (2010–2012) | 7.15 | 6.70 | 7.62 |
| Post-intervention (2013–2016) | 7.16 | 6.32 | 8.00 |
Standardized factor score based on percent of residents living above poverty, percent employed, percent with a college degree, and median household income.
SVN/total crashes is the percentage of all motor vehicle crashes that were single vehicle night-time crashes.
SVN, single vehicle night-time.
Results of multilevel Poisson regression analyses are provided in Table 2. The initial intent-to-treat regression model for drivers aged 15–30 years indicated a significant reduction in the percentage of SVN crashes in intervention cities relative to controls when controlling for the time trend and seasonal effect at the observation level, and city characteristics. The event rate ratio indicated a 17% lower percentage of SVN crashes among drivers aged 15–30 years in intervention cities from 2013 to 2016 relative to controls. The relative change in the percentage of SVN crashes is illustrated in Figure 2A.
Table 2.
Results of Multi-level Poisson Regression Analyses to Assess Intervention Effects on Alcohol-related Motor Vehicle Crashes Among 15 to 30-Year-Old Drivers
| Variable | Intent-to-treat Event rate ratio (95% CI) |
Dosage level Event rate ratio (95% CI) |
|---|---|---|
| Observation level | ||
| Time | 1.003 (1.00, 1.005) * | 1.003 (1.00, 1.005) * |
| September/October | 0.89 (0.82, 0.96) ** | 0.89 (0.82, 0.96) ** |
| Intervention perioda | 0.83 (0.70, 0.98) * | – |
| <2 DUI operations/quarterb | – | 0.73 (0.60, 0.90) ** |
| ≥2 DUI operations/quarterb | – | 0.87 (0.72, 1.06) |
| City level | ||
| SES factor scorec | 0.89 (0.82, 0.97) * | 0.89 (0.82, 0.98) * |
| Percent minority | 0.63 (0.27, 1.47) | 0.67 (0.28, 1.61) |
| Population size | 0.99 (0.97, 1.02) | 0.99 (0.97, 1.02) |
Note: Event rate ratios less than 1.0 indicate a lower incidence of alcohol-related crashes during intervention years. The difference from 1.0 represents the percent reduction in the incidence of crashes (e.g., 0.83 represents a 17% reduction in alcohol-related crashes in the 12 intervention cities). Boldface indicates statistical significance
p<0.05;
p<0.01.
From April 2013 to March 2016 when high-visibility DUI enforcement operations were taking place in 12 intervention cities compared to the 12 control cities and pre-intervention period for all 24 cities.
DUI enforcement operations included sobriety checkpoints and saturation patrols to provide visible enforcement of drink-driving laws. These were accompanied by various types of media (e.g., posters, mobile signs) to raise public awareness of enforcement operations.
Standardized factor score based on percent of residents living above poverty, percent employed, percent with a college degree, and median household income.
DUI, driving under the influence.
Figure 2.
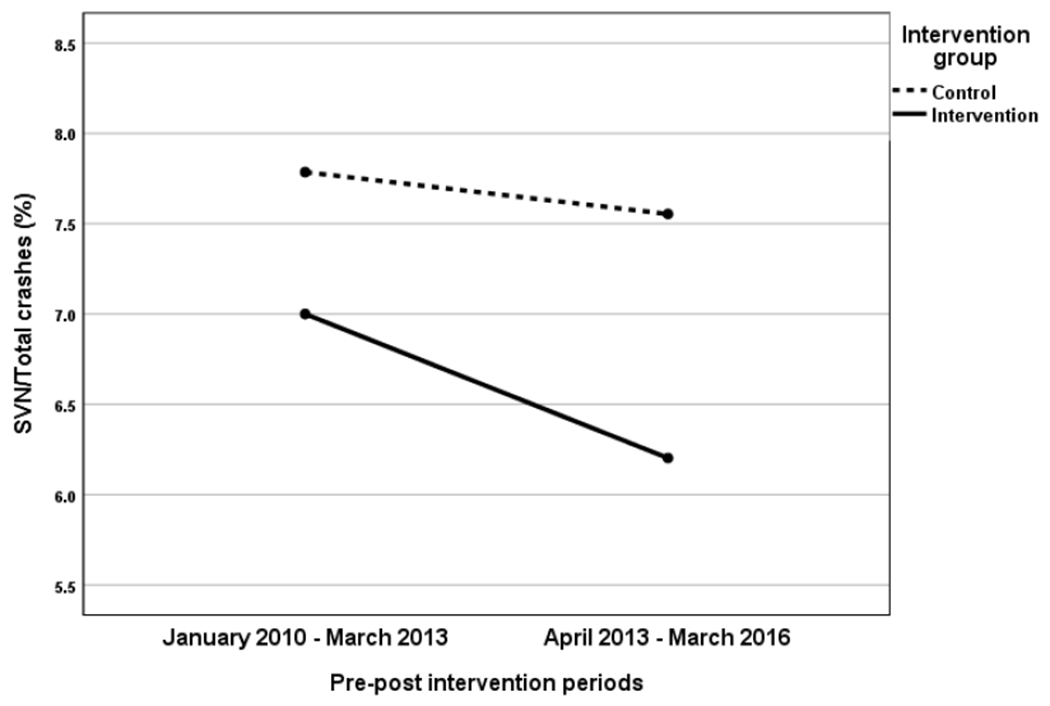
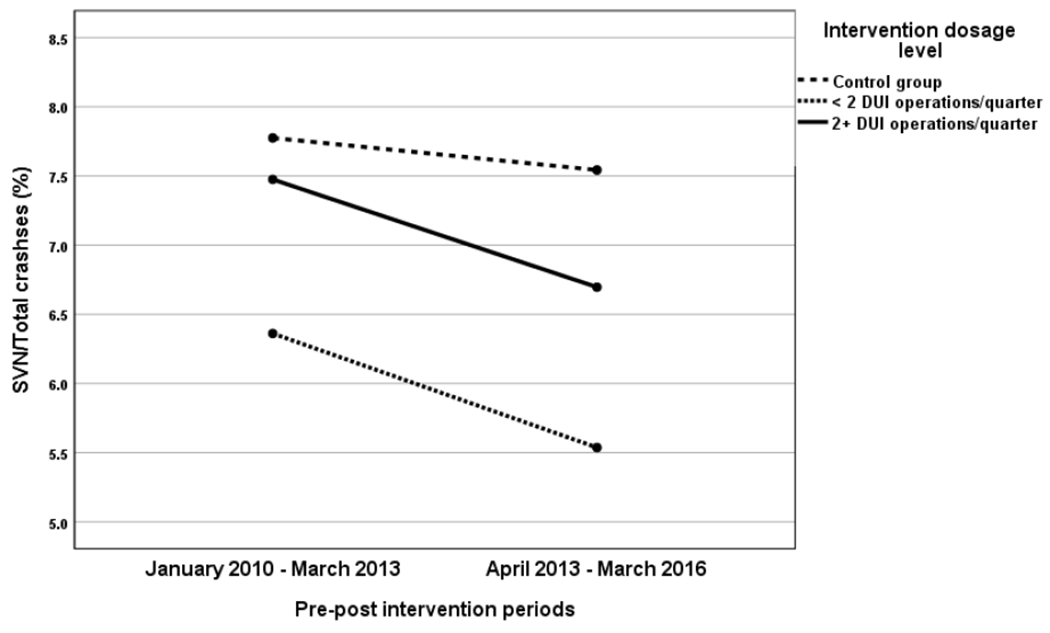
(A) Change in the percentage of motor vehicle crashes that are single vehicle nighttime (SVN) crashes among 15 to 30-year-old drivers in intervention and control cities. (B) Change in the percentage of motor vehicle crashes that are single vehicle nighttime (SVN) crashes among 15 to 30-year-old drivers by intervention dosage level. Of the 12 intervention cities, 5 implemented < 2 DUI enforcement operations per quarter and 7 implemented 2 or more DUI operations per quarter.
Notes: The SVN/total crashes percentage is adjusted for city characteristics.
DUI, driving under the influence.
The intervention dosage model for drivers aged 15–30 years also indicated a significant reduction in the percentage of SVN crashes at the low intervention dosage level for intervention cities (i.e., <2 high-visibility DUI operations per quarter), and a non-significant reduction for cities that implemented ≥2 high-visibility DUI operations per quarter. Event rate ratios indicated a 27% and 13% lower percentage of SVN crashes among intervention cities with low and high intervention dosage levels, respectively, from 2013 to 2016 relative to control cities. The relative changes in percentage of SVN crashes are illustrated in Figure 2B.
As an aside, the same analyses were conducted for all drivers, including those older than the target of the intervention. The event rate ratio was 0.90 for the intervention condition and not significant. Dosage effect was similar to young drivers, with event rate ratios of 0.91 and 0.88 for low and high dosages and again, not significant.
As percentage reduction is difficult to appreciate in practical terms, each intervention city’s number of crashes and results of multilevel regression analyses were used to generate the estimated reduction in the number of SVN crashes. For the intent-to-treat model for drivers aged 15–30 years, the estimated reduction of SVN crashes (relative to controls) was 310 across the 12 cities for the post-intervention period of April 2013 to March 2016. For the dosage model, there were an estimated 164 fewer SVN crashes for the lower dose and 146 for the recommended dose. These numbers reflect the fact that, although effect size was nearly double for low-dosage cities, they had slightly more than half the number of crashes at baseline as cities in the recommended dosage group.
Given estimates of the cost of an alcohol-involved crash amount to $296,12733,34 (including fatal, injury, and property damage–only crashes), 310 fewer crashes translates to >$91 million. Total funds for each community came to $95,000 per year, some of which went to overhead and other indirect expenses, but using the gross allocation, total funding for 12 cities during the 3-year intervention period was approximately $3,420,000. This would mean that the benefit–cost ratio was roughly 27:1 or $27 saved for every $1 spent.
DISCUSSION
The findings of this study suggest that the community prevention effort reduced alcohol-involved crashes among youth and young adults by a significant degree. The results are perhaps especially interesting given that the communities were chosen at random without regard to any interest expressed by anyone in those cities, nor with regard to any notion of “readiness.” Additionally, the research team had very limited opportunities to select partnering agencies, and those agencies were uncertain at the start of the intervention about the role of the researchers with respect to the state funding agency, even when the state and the research team had defined their roles early on. This study may be the first to attempt investigator-initiated community prevention where communities neither self-selected nor selected for any specific characteristics likely to favor implementation.
This sample perhaps led to the counterintuitive effects of dosage for drivers aged 15–30 years; that is, a greater effect was seen in cities with lower dosage. One would expect that the cities that met the recommended dosage would have produced a greater effect than those that did not. The 2 groups had no obvious differences in terms of demographics or level of the alcohol-related problems used to roughly match the cities. The cities who met the recommended dosage were more likely to have had enforcement grants from state agencies, however. Perhaps those cities were therefore more capable of implementing the enforcement interventions, and the recommended intervention dosage level did not represent any meaningful change in the level of DUI enforcement from pre-intervention years. If communities had been purposely selected for having already been active in DUI enforcement, this unexpected result may not have been seen, but this is speculative.
The study cannot address the question of sustainability. Indeed, all the participants were aware of the timeframe of the study, which may have increased cooperation in some cases (e.g., because commitments were limited) or detracted it in others (e.g., resistant participants would know the project would end). There may well be different strategies and different phases to maintain community prevention efforts other than those to launch them. The long time needed to obtain crash data also works against using outcomes to build motivation quickly. These issues would be valuable topics for future research in this area.
There were a number of obstacles that bear comment. One significant and unexpected implementation challenge was that some partnering prevention agencies were wholly inexperienced in working with law enforcement agencies. In some cases, there were even formal barriers to shifting dollars from prevention agencies to law enforcement. This was a surprise given the example of drink driving enforcement campaigns, in which researchers expected partnering agencies and organizations would have participated.
Second, in communities with a long history of addressing alcohol-related crashes, there may have been a problem with low rates, a floor problem. The ratio of SVN to other crashes was about 10% at baseline, and with month-to-month variability that may pose a challenge statistical testing in any replication.
Related to these possible issues is having few communities in the sample (N=24). Community-level evaluations such as this are commonly faced with the challenge of compromising between the number of communities and the quantity and quality of time and resources available to ensure implementation. The logic models and other strategies used in this project made for some efficiencies in implementing intervention activities across 12 communities, but some required more effort or were hampered by logistical problems (e.g., obtaining budget approvals from city or county governments).
Limitations
Potential study limitations include inaccurate measurement of intervention dosage levels across the 12 intervention cities, which relied upon monthly reports provided by community or local law enforcement agencies. Lack of similar information on alcohol enforcement operations in control cities limited the possibility of comparing and assessing effects of intervention dosage levels across all 24 cities. Using SVN crashes as the primary indicator of alcohol-related motor vehicle crashes may have underestimated the actual occurrence of such crashes over the study period, and this in turn may have led to an underestimation or overestimation of intervention effects.
Despite these limitations, this study provides evidence that enhanced DUI and responsible beverage service enforcement operations can help to reduce alcohol-related motor vehicle crashes and related injuries and fatalities at the community level, particularly among young drivers. This study also indicates the potential for local community health and local law enforcement agencies to work together to implement effective environmental interventions, involving alcohol policy enforcement operations and a variety of media channels to increase visibility and public awareness.
CONCLUSIONS
Enhanced alcohol enforcement operations involving both community health and law enforcement agencies can help to reduce alcohol-impaired driving and related consequences among young people. Having measures of intervention dosage improves the understanding of the impact of the community intervention but raises questions regarding the sources of variation in dosage. Dosage may be related to implementation strategy, competing demands on community agencies, sampling design, or the somewhat artificial and time-limited nature of a research project. Future studies should focus on alternative implementation strategies that may more effectively and efficiently reduce community alcohol-related harm.
Supplementary Material
Figure 1.
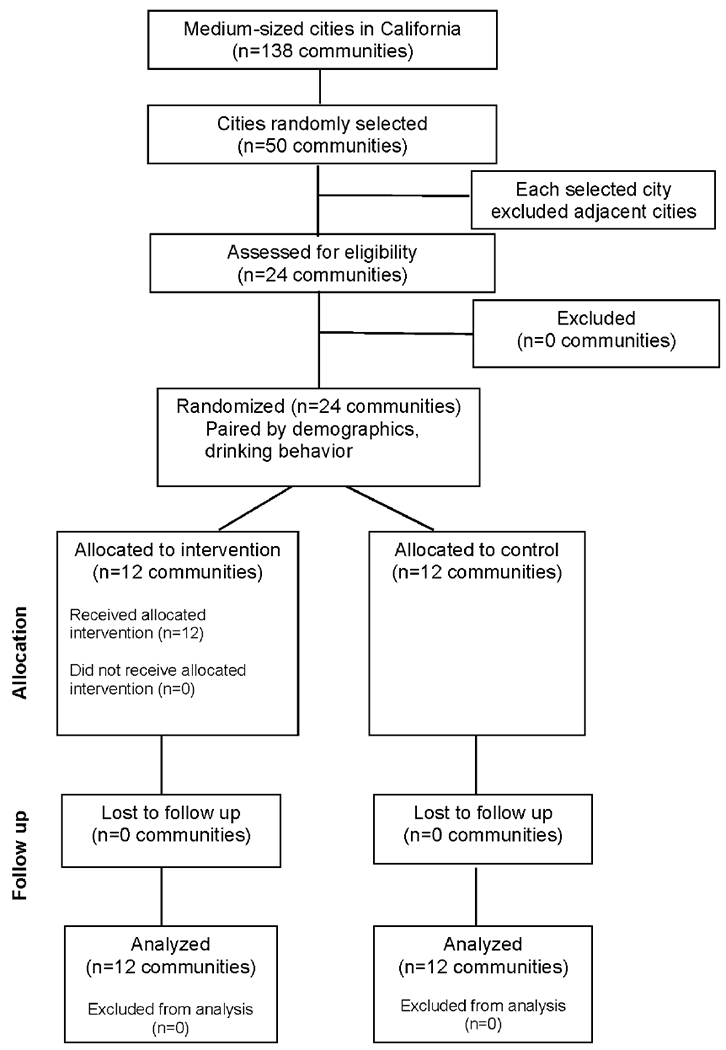
Flow of clusters (communities) through the group-randomized prevention trial.
ACKNOWLEDGMENTS
This study was funded by the California Department of Health Care Services (Contract No. U79SP015622-01) and the National Institute on Alcohol Abuse and Alcoholism (NIAAA Grant No. P60-AA006282). The content is solely the responsibility of the authors and does not necessarily represent the official views of the California Department of Health Care Services, NIAAA, or NIH. The project was greatly aided by colleagues Richard McGaffigan, MA, and Peter Nygaard, PhD. As Project Manager, Ms. Jane Williams’ support was crucial. Dr. Steve Wirtz of the California Department of Public Health provided guidance throughout the study, including this paper. Extremely valuable suggestions were provided by the anonymous reviewers.
Dr. Paschall has received funding from the AB InBev Foundation to conduct an independent evaluation of the Global Smart Drinking Goals initiative. Drs. Saltz and O’Hara declare no conflict of interest.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
No financial disclosures were reported by the authors of this paper.
REFERENCES
- 1.National Academies of Sciences, Engineering and Medicine. Getting to Zero Alcohol-Impaired Driving Fatalities: A Comprehensive Approach to a Persistent Problem. Washington, DC: The National Academies Press, 2018. 10.17226/24951. [DOI] [PubMed] [Google Scholar]
- 2.Insurance Information Institute. Facts + Statistics: Alcohol-Impaired Driving. https://www.iii.org/fact-statistic/facts-statistics-alcohol-impaired-driving. Accessed May 13, 2020.
- 3.National Highway Traffic Safety Administration. Traffic Safety Facts, 2017 Data: Alcohol-Impaired Driving. Washington, DC: NHTSA National Center for Statistics and Analysis; November2018. https://crashstats.nhtsa.dot.gov/Api/Public/ViewPublication/812630. Accessed August 13, 2020. [Google Scholar]
- 4.Holder HD, Gruenewald PJ, Ponicki WR, et al. Effect of community-based interventions on high risk drinking and alcohol-related injuries. JAMA. 2000;284(18):2341–2347. 10.1001/jama.284.18.2341. [DOI] [PubMed] [Google Scholar]
- 5.Gruenewald PJ, Treno AJ, Holder HD, FaScala EA. Community-based approaches to the prevention of substance use related problems. In: Sher KJ, ed. Oxford Handbook of Substance Use Disorders. Oxford, UK: Oxford University Press, 2016. 10.1093/oxfordhb/9780199381678.013.005. [DOI] [Google Scholar]
- 6.Pentz MA. Institutionalizing community-based prevention through policy change. J Community Psychol. 2000;28(3):257–270. 10.1002/(sici)1520-6629(200005128:3<257::aid-icop3>3.0.co:2-1. [DOI] [Google Scholar]
- 7.Wagenaar AC, Perry CL. Community strategies for the reduction of youth drinking: theory and application. J Res Adolesc. 1994;4(2):319–345. 10.1207/s15327795ira0402_8. [DOI] [Google Scholar]
- 8.Holder HD. Alcohol and the Community: A Systems Approach to Prevention. Cambridge, UK: Cambridge University Press; 1998. [Google Scholar]
- 9.Holder HD, Reynolds RI. Application of local policy to prevent alcohol problems: experiences from a community trial. Addiction. 1997;92(suppl 2):S285–S292. 10.1080/09652149737584. [DOI] [PubMed] [Google Scholar]
- 10.Grube JW. Preventing sales of alcohol to minors: results from a community trial. Addiction. 1997;92(suppl 2):S251–S260. 10.1111/j.1360-0443.1997.tb02995.x. [DOI] [PubMed] [Google Scholar]
- 11.Saltz RF, Stanghetta P. A community-wide responsible beverage service program in three communities: early findings. Addiction. 1997;92(suppl 2):S237–S249. 10.1111/j.1360-0443.1997.tb02994.x. [DOI] [PubMed] [Google Scholar]
- 12.Gruenewald PJ, Treno AJ. Local and global alcohol supply: economic and geographic models of community systems. Addiction. 2000;95(suppl 4):S537–S549. 10.1080/09652140020Q13764. [DOI] [PubMed] [Google Scholar]
- 13.Hingson R, McGovern T, Howland J, et al. Reducing alcohol impaired driving in Massachusetts: the Saving Lives program. Am J Public Health. 1996;86(6):791–797. 10.2105/ajph.86.6.791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wagenaar AC, Murray DM, Gehan JP, et al. Communities mobilizing for change on alcohol: outcomes from a randomized community trial. J Stud Alcohol. 2000;61(1):85–94. 10.15288/jsa.2000.61.85. [DOI] [PubMed] [Google Scholar]
- 15.Holder HD, Gruenewald PJ, Ponicki WR, et al. Effect of community-based interventions on high risk drinking and alcohol-related injuries. JAMA. 2000;284(18):2341–2347. 10.1001/jama.284.18.2341. [DOI] [PubMed] [Google Scholar]
- 16.Voas RB, Tippetts AS, Johnson MB, Lange JE, Baker J. Operation Safe Crossing: using science within a community intervention. Addiction. 2002;97(9):1205–1214. 10.1046/j.1360-0443.2002.00183.x. [DOI] [PubMed] [Google Scholar]
- 17.Treno AJ, Gruenewald PJ, Lee JP, et al. The Sacramento Neighborhood Alcohol Prevention Project: outcomes from a community prevention trial. J Stud Alcohol Drugs. 2007;68(2):197–207. 10.15288/jsad.2007.68.197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wallin E, Gripenberg J, Andréasson S. Overserving at licensed premises in Stockholm: effects of a community action program. J Stud Alcohol. 2005;66(6):806–814. 10.15288/jsa.2005.66.806. [DOI] [PubMed] [Google Scholar]
- 19.Wallin E, Norström T, Andréasson S. Alcohol prevention targeting licensed premises: a study of effects on violence. J Stud Alcohol. 2003;64(2):270–277. 10.15288/jsa.2003.64.270. [DOI] [PubMed] [Google Scholar]
- 20.Gripenberg J, Wallin E, Andréasson S. Effects of a community-based drug use prevention program targeting licensed premises. Subst Use Misuse. 2007;42(12–13):1883–1898. 10.1080/10826080701532916. [DOI] [PubMed] [Google Scholar]
- 21.Månsdotter AM, Rydberg MK, Wallin E, Lindholm LA, Andréasson S. A cost-effectiveness analysis of alcohol prevention targeting licensed premises. Eur J Public Etealth. 2007;17(6):618–623. 10.1093/eurpub/ckm017. [DOI] [PubMed] [Google Scholar]
- 22.Saltz RF, Paschall MJ, McGaffigan RM, Nygaard PM. Alcohol risk management in college settings: the Safer California Universities Randomized Trial. Am J Prev Med. 2010;39(6):491–499. 10.1016/j.amepre.2010.08.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Flewelling RL, Grube JG, Paschall MJ, et al. Reducing youth access to alcohol: findings from a community-based randomized trial. Am J Community Psychol. 2012;51(1–2):264–277. 10.1007/s10464-012-9529-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wolfson M, Champion H, McCoy TP, et al. Impact of a randomized campus/community trial to prevent high-risk drinking among college students. Alcohol Clin Exp Res. 2012;36(10):1767–1778. 10.1111/j.1530-0277.2012.01786.X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Trolldal B, Brännström L, Paschall MJ, Leifman H. Effects of a multi-component responsible beverage service programme on violent assaults in Sweden. Addiction. 2013;108(1):89–96. 10.1111/j.1360-0443.2012.04004.x. [DOI] [PubMed] [Google Scholar]
- 26.Rossow I, Baklien B. Effectiveness of responsible beverage service: the Norwegian experiences. Contemp Drug Probl. 2010;37(1):91–107. 10.1177/0091450910037001Q5. [DOI] [Google Scholar]
- 27.Shakeshaft A, Doran C, Petrie D, et al. The effectiveness of community action in reducing risky alcohol consumption and harm: a cluster randomised controlled trial. PLoS Med. 2014;11(3):e1001617. 10.1371/journal.pmed.1001617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Giesbrecht N, Bosma L, Juras J, et al. Implementing and sustaining effective alcohol-related policies at the local level: evidence, challenges, and next steps. World Med Health Policy. 2014;6(3):203–230. 10.1002/wmh3.98. [DOI] [Google Scholar]
- 29.Stockings E, Bartlem K, Hall A, et al. Whole-of-community interventions to reduce population-level harms arising from alcohol and other drug use: a systematic review and meta-analysis. Addiction. 2018;113(11):1984–2018. 10.1111/add.14277. [DOI] [PubMed] [Google Scholar]
- 30.HHS, Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. Key substance use and mental health indicators in the United States: Results from the 2018 National Survey on Drug Use and Health. HHS Publication No. SMA 18-5068, NSDUH Series H-53; 2019. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/NSDUHNationalFindingsReport2018/NSDUHNationalFindingsReport2018.pdf. Accessed August 13, 2020.
- 31.Fixen DL, Naoom SF, Blase KA, Friedman RM, Wallace F. Implementation Research: A Synthesis of the Literature. Tampa, FL: University of South Florida, Louis de la Parte Florida Mental Health Institute, The National Implementation Research Network, FMHI Publication #231; 2005. [Google Scholar]
- 32.Voas RB, Romano E, Peck R. Validity of surrogate measures of alcohol involvement when applied to nonfatal crashes. Accid Anal Prev. 2009;41(3):522–530. 10.1016/j.aap.2009.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Miller TR, Nygaard P, Gaidus A, et al. Heterogeneous costs of alcohol and drug problems across cities and counties in California.Alcohol Clin Exp Res. 2017;41(4):758–768. 10.1111/acer.13337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Zaloshnja E, Miller TR, Blincoe L. Costs of alcohol-involved crashes, United States, 2010. Ann Adv Automot Med. 2013;57:3–12. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.