

The two main types of cardiac amyloidosis (CA), light chain (AL) and transthyretin (ATTR), typically cause restrictive cardiomyopathy (RCM) that may progress to advanced heart failure prompting consideration for orthotopic heart transplantation (OHT) or left ventricular assist device (LVAD). 1 Limited data exist on continuous‐flow LVAD (CF‐LVAD) use in CA patients, as this is not traditionally considered feasible due to the non‐dilated and restrictive nature of the cardiac chambers. 2 Herein, we describe the outcomes of CA patients on CF‐LVAD therapy at our institution.
Our single‐centre case series retrospectively identified seven CA patients (mean age 68 ± 9 years, 86% male, 71% African‐American, 57% Intermacs 1–2) all supported by CF‐LVAD (five centrifugal and two axial) from 2009 to 2021 (Table 1 and Supporting Information, Tables S1 – S3 ). Five patients had ATTR amyloidosis (three hereditary due to p.Val142Ile and two wild type), and two had AL amyloidosis. This study complies with the Declaration of Helsinki and was approved by the institutional ethics committee with waiver for informed consent. Two CA patients with pulsatile pumps were excluded.
Table 1.
Survival and surgical considerations in cardiac amyloidosis patients with left ventricular assist device implant
| Parameter | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 |
|---|---|---|---|---|---|---|---|
| Age (years) | 72 | 68 | 62 | 53 | 74 | 76 | 55 |
| Sex | Male | Male | Male | Male | Male | Male | Female |
| Race | AA | AA | AA | AA | AA | Caucasian | Caucasian |
| Amyloid type | ATTRwt | ATTRwt | ATTRv p.V142I | ATTRv p.V142I | ATTRv p.V142I | AL light chain | AL light chain |
| Intermacs level | 4 | 3 | 1 | 2 | 3 | 2 | 1 |
| Device strategy | DT | BTT | BTT | DT to BTT | DT | DT | DT |
| Device type | HMII | HVAD | HM3 | HVAD | HM3 | HVAD | HMII |
| LVAD support (months) | 43.1 | 8.4 | 13.4 | 24.1 | 18.0 | 66.9 | 48.3 |
| Survival post‐OHT (months) | NA | 48.1 | 24.9 | 6.9 | NA | NA | NA |
| Death | Yes, post‐LVAD | No, OHT | Yes, post‐OHT | No, OHT | No | No | Yes, post‐LVAD |
| RHF | Yes, early inotrope | No | Yes, early RVAD | Yes, late RVAD | No | No | No |
| LVEF (%) | 33 | 45 | 34 | 10 | 23 | 30 | 21 |
| LVEDD (cm) | 5.4 | 4.5 | 5.8 | 6.0 | 5.6 | 4.4 | 4.5 |
| RV function | Mild | Mild | Severe | Severe | Normal | Normal | Normal |
| PAPI | 1.5 | 1.6 | 0.5 | 1.3 | 8.8 | 3.0 | 16 |
| Surgical LV debulking | Several LV core resections | LV core resection only | LV core resection only | LV core resection only | LV myectomy | LV core and extensive myectomy | Circular LV apex resection |
AA, African‐American; ATTRv p.V142I, transthyretin hereditary variant p.Val142Ile mutation; ATTRwt, transthyretin wild type; BTT, bridge to transplant; DT, destination therapy; HM, Heartmate; LV, left ventricular; LVAD, LV assist device; LVEDD, LV end‐diastolic diameter; LVEF, LV ejection fraction; OHT, orthotopic heart transplant; PAPI, pulmonary artery pulsatility index; RHF, right heart failure defined by need for RVAD or inotropes ≥14 days (early = first event within 12 months, late = first event after 12 months); RVAD, right ventricular assist device.
The CF‐LVAD served as bridge to transplant (BTT) in three patients and as destination therapy (DT) in four patients. The entire cohort was alive at 12 months post‐LVAD and had a median survival of 2.01 years on LVAD support only and 3.6 years overall. The two AL amyloidosis patients with DT‐LVAD survived the longest; one died after 48.3 months, and one remains alive at 66.9 months. Both achieved complete hematologic remission after anti‐plasma cell therapy. Three patients (43%) died: one post‐OHT from acute severe cellular rejection for non‐compliance with immunosuppression; and two others whilst on device support, one from a fatal cerebral bleed after 43.1 months and the other from complications secondary to a device‐related infection after 48.3 months.
All patients had an LV ejection fraction (LVEF) ≤ 45%, with variable LV end‐diastolic diameter (LVEDD). Two patients with a dilated LVEDD ≥ 5.8 cm were bridged to OHT. Of five patients with LVEDD ≤ 5.6 cm, four had intra‐operative LV debulking that entailed multiple extensive core resections or myectomy, a decision made by the cardiothoracic surgeon during direct LV cavity visualization after apical core resection. All three with smaller LVEDD ≤ 4.5 cm had no clinically documented suction events that led to malignant arrhythmias, hypotension, pump thrombosis, or right heart failure (RHF). However, one of these patients with DT‐Heartmate II and LVEDD 4.5 cm had LV inflow cannula‐induced premature ventricular contractions resulting in recurrent ventricular tachycardia (VT). There were no speed ramp downs or changes in pulsatility index to suggest suction events, and there was no further VT after successful ablation. In most patients, the pump speed was kept steady and at a relatively lower target speed than in non‐CA patients (Supporting Information, Table S1 ). Heart failure, diuretic, and anti‐arrhythmic therapies were adjusted in all patients based on their mean arterial pressure, renal function, electrolytes, volume status, and arrhythmia burden; however, negative inotropes (e.g. beta‐blockers) and high‐dose diuretics were used with caution or avoided. Aspirin (81–325 mg daily) and Coumadin (INR goal 2–3) were reduced in patients with bleeding. One patient was peri‐operatively safely bridged with bivalirudin to anti‐coagulation for heparin‐induced thrombocytopenia.
Right heart failure requiring right ventricular assist device (RVAD) and/or inotropes ≥14 days occurred in three patients (43%) at ~0.5, 6, and 23 months (Table 1 and Supporting Information, Table S1 ). They all had a pre‐implant pulmonary artery pulsatility index (PAPI) of ≤1.5. The two patients who required an RVAD had severe pre‐implant echocardiographic RV dysfunction; the RVAD was implanted shortly after CF‐LVAD in the one patient bridged to heart–kidney transplantation, and the RVAD was placed almost 2 years after CF‐LVAD in the other patient also successfully bridged to heart transplantation. The third patient with RHF after DT‐Heartmate II was on long‐term inotropes and died from cerebral bleeding complications due to a mechanical fall.
This study highlights several key findings: first, in our cohort, the survival was 100% at 12 months post‐CF‐LVAD with a median survival of 2.01 years on device support and 3.6 years overall. This is the longest survival reported to date (Supporting Information, Table S3 ). In contrast, Grupper et al. reported a median survival of 1.5 years with a 6 month mortality of >50% in a 10‐patient cohort with CA on CF‐LVAD therapy. 1 Although a different mode of mechanical circulatory support, Kittleson et al. reported using total artificial heart as an effective BTT strategy in nine CA patients with biventricular dysfunction with a 12 month survival of 82%. 3 Another recent INTERMACS analysis by Michelis et al. of 46 CA patients reported a median survival of over ~2 years in ATTR CA and ~0.5–1 years in AL CA; however, a significant proportion (46%) had pulsatile devices generally associated with worse event‐free survival relative to CF‐LVAD therapy. 4 Importantly, mortality in all three cases in our study was unrelated to anatomic concerns regarding LV size, acknowledging that several patients underwent different degrees of surgical LV debulking.
Second, three patients with an LVEDD of ≤4.5 cm did not experience clinically significant suction events or thrombotic complications (Supporting Information, Tables S1 and S2 ). One of the main anatomic concerns of LVAD implantation in CA patients is a smaller LV cavity size that can lead to suction events by obstructing the inflow cannula, thereby predisposing to low flow, hypotension, and pump thrombosis, as well as arrhythmias and worsening RV function. To offset these concerns, CF‐LVAD management in our cohort included keeping RPM at a lower target speed, and caution with negative inotrope (e.g. beta‐blocker) and high‐dose diuretic use post‐CF‐LVAD. Also, the surgical decision to create more space in the apical area via debulking was individualized and proved feasible (Figure S1 ). However, we do not know what LVEDD size is too small to consider for CF‐LVAD in CA patients, and we are not advocating consideration in any LV smaller than 4.4 cm, the lowest in this cohort. There was also no correlation seen with LVEDD or LVEF and survival or post‐implant complications in our cohort, similar to other studies. 1 , 4
Third, the incidence of RHF was high (three of seven patients), independent of type of CF‐LVAD pump, but was manageable enough for two patients to get to OHT with RVAD support (Table 1 and Supporting Information, Table S1 ). The third patient had fatal post‐traumatic cerebral bleeding 36 months after initiating inotropic RV support. There is a valid physiologic concern for RHF post‐CF‐LVAD implantation in amyloid heart disease given there is universal RV involvement. Analyses of the INTERMACS registry reported a 6.4% overall incidence of RVAD use in RCM patients and a 15% incidence of early RHF in CA patients. 4 , 5 Grupper et al. described a 39% incidence of RHF, with 10% using RVADs. 1 These studies do not describe late RHF, which we noted in one patient herein. In our analysis, severe pre‐implant echocardiographic RV dysfunction and low pre‐implant PAPI ≤ 1.5 was found in the patients who had RHF. Future studies will need to explore the specific predictors of early vs. late onset RHF in CA patients.
This study has limitations as a retrospective single‐centred analysis including a small number of select CA patients over a long time‐period.
Our experience highlights the feasibility of supporting highly selected CA patients with CF‐LVAD as BTT or DT including the HeartMate 3 pump with reasonable outcomes, principally for those with a reduced LVEF and an absence of significant pre‐implant RV dysfunction or PAPI ≤ 1.5. Significant caution should still be exercised in pursuing this strategy, and future analyses are warranted to further refine careful patient selection to improve outcomes, with particular consideration to surgical debulking around the inflow cannula for smaller LV cavities and ongoing surveillance of RV function.
Funding
Dr Hanna receives funding support from the term chair in amyloid heart disease.
Supporting information
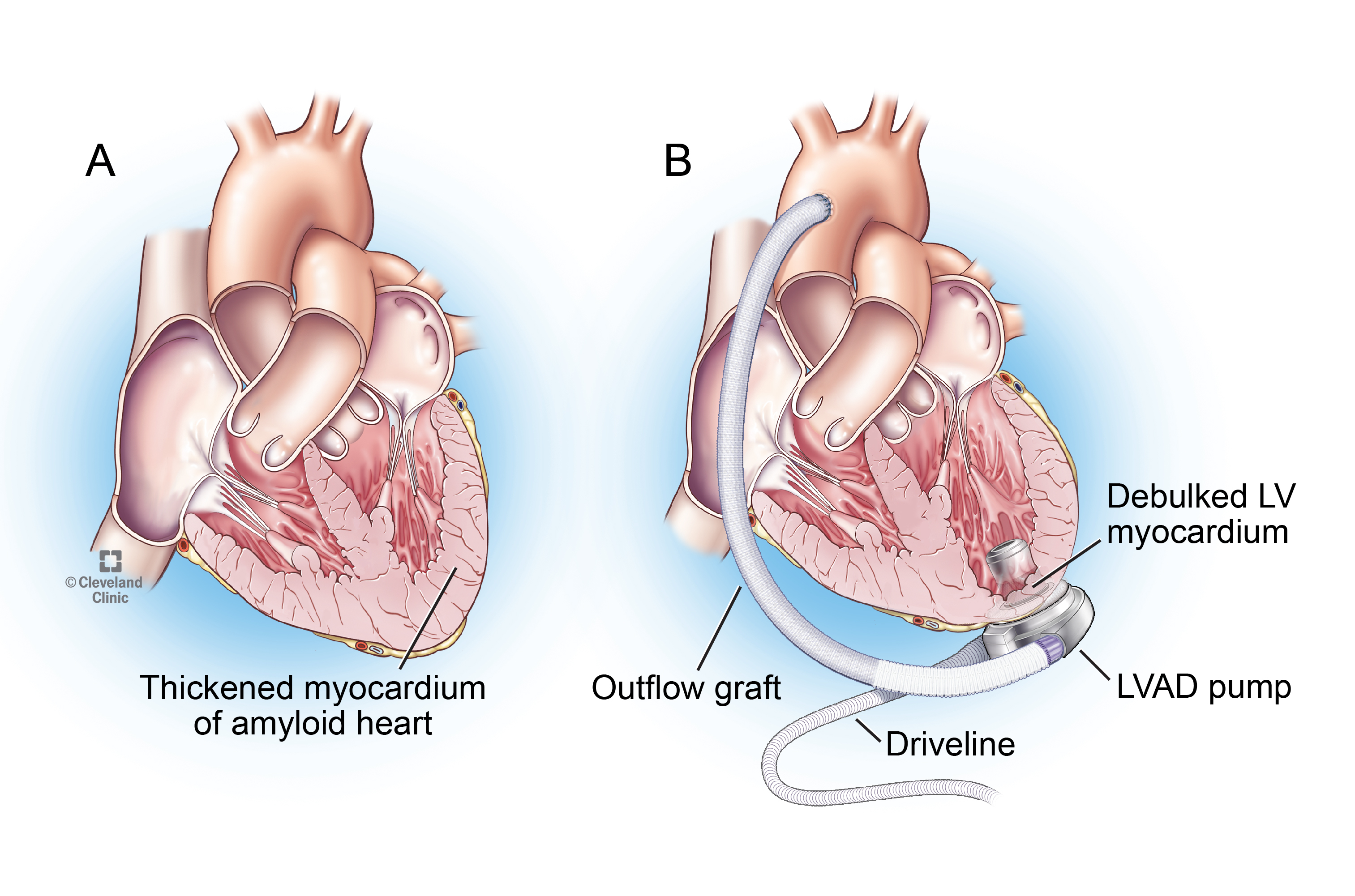
Figure S1. Pictorial of Continuous‐Flow Left Ventricular Assist Device (CF‐LVAD) Implant in Cardiac Amyloidosis. Small left ventricle (LV) with thickened myocardium without (A) or following (B) surgical LV debulking and CF‐LVAD pump in situ.
{kind=link}
Table S1. Morbidity Outcomes in Cardiac Amyloidosis Patients with LVAD Therapy.
Table S2. Characteristics of Cardiac Amyloidosis Patients on LVAD Therapy.
Table S3. Studies Reporting on Cardiac Amyloidosis Patients with Durable Mechanical Support.
Randhawa, V. K. , Gabrovsek, A. , Soltesz, E. G. , Tong, M. Z. Y. , Unai, S. , Chen, L. , Mountis, M. M. , Tang, W. H. W. , Starling, R. C. , Estep, J. D. , and Hanna, M. (2021) A case series of cardiac amyloidosis patients supported by continuous‐flow left ventricular assist device. ESC Heart Failure, 8: 4353–4356. 10.1002/ehf2.13422.
References
- 1. Grupper A, Park SJ, Pereira NL, Schettle SD, Gerber Y, Topilsky Y, Edwards BS, Daly RC, Stulak JM, Joyce LD, Kushwaha SS. Role of ventricular assist therapy for patients with heart failure and restrictive physiology: improving outcomes for a lethal disease. J Heart Lung Transplant 2015; 34: 1042–1049. [DOI] [PubMed] [Google Scholar]
- 2. Sridharan L, Wayda B, Truby LK, Latif F, Restaino S, Takeda K, Takayama H, Naka Y, Colombo PC, Maurer M, Farr MA, Topkara VK. Mechanical circulatory support device utilization and heart transplant waitlist outcomes in patients with restrictive and hypertrophic cardiomyopathy. Circ Heart Fail 2018; 11: ee004665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Kittleson MM, Cole RM, Patel J, Ramzy D, Passano E, Chang DH, Geft DR, Czer L, Vescio R, Chung J, Kobashigawa JA, Arabia F, Esmailian F, Moriguchi JD. Mechanical circulatory support for cardiac amyloidosis. Clin Transplant 2019; 33: e13663. [DOI] [PubMed] [Google Scholar]
- 4. Michelis KC, Zhong L, Tang WHW, Young JB, Peltz M, Drazner MH, Pandey A, Griffin J, Maurer MS, Grodin JL. Durable mechanical circulatory support in patients with amyloid cardiomyopathy: insights from INTERMACS. Circ Heart Fail 2020; 13: 3007931. [DOI] [PubMed] [Google Scholar]
- 5. Patel SR, Saeed O, Naftel D, Myers S, Kirklin J, Jorde UP, Goldstein DJ. Outcomes of restrictive and hypertrophic cardiomyopathies after LVAD: an INTERMACS analysis. J Card Fail 2017; 23: 859–867. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Pictorial of Continuous‐Flow Left Ventricular Assist Device (CF‐LVAD) Implant in Cardiac Amyloidosis. Small left ventricle (LV) with thickened myocardium without (A) or following (B) surgical LV debulking and CF‐LVAD pump in situ.
Table S1. Morbidity Outcomes in Cardiac Amyloidosis Patients with LVAD Therapy.
Table S2. Characteristics of Cardiac Amyloidosis Patients on LVAD Therapy.
Table S3. Studies Reporting on Cardiac Amyloidosis Patients with Durable Mechanical Support.