

Abstract
Reading disability (dyslexia) refers to an unexpected difficulty with reading for an individual who has the intelligence to be a much better reader. Dyslexia is most commonly caused by a difficulty in phonological processing (the appreciation of the individual sounds of spoken language), which affects the ability of an individual to speak, read, and spell. In this paper, I describe reading disabilities by focusing on their underlying neurobiological mechanisms. Neurobiological studies using functional brain imaging have uncovered the reading pathways, brain regions involved in reading, and neurobiological abnormalities of dyslexia. The reading pathway is in the order of visual analysis, letter recognition, word recognition, meaning (semantics), phonological processing, and speech production. According to functional neuroimaging studies, the important areas of the brain related to reading include the inferior frontal cortex (Broca’s area), the midtemporal lobe region, the inferior parieto-temporal area, and the left occipitotemporal region (visual word form area). Interventions for dyslexia can affect reading ability by causing changes in brain function and structure. An accurate diagnosis and timely specialized intervention are important in children with dyslexia. In cases in which national infant development screening tests have been conducted, as in Korea, if language developmental delay and early predictors of dyslexia are detected, careful observation of the progression to dyslexia and early intervention should be made.
Keywords: Learning disability, Neurobiology, Reading disability (dyslexia)
Introduction
According to the American Individuals with Disabilities Education Act (IDEA) [1], a specific learning disability, which includes a reading disability, refers to a disorder in one or more of the basic psychological processes involved in understanding or using spoken or written language. It may manifest as an impaired ability to listen, think, speak, read, write, spell, or perform mathematical calculations. This includes conditions such as perceptual disabilities, brain injury, minimal brain dysfunction, dyslexia, and developmental aphasia. Specific learning disabilities exclude learning problems that are primarily the result of the visual, hearing, or motor disabilities, intellectual disability, emotional disturbance, or environmental, cultural, or economic disadvantages. In the Diagnostic and Statistical Manual of Mental Disorders-5 [2], learning disabilities are classified as impairments in reading, written expression, and mathematics, and 80% of learning disabilities are related to reading disabilities.
In this paper, I describe reading disability by focusing on the underlying neurobiological mechanisms and the importance of early diagnosis in children. In 1877, Adolph Kussmaul reported that, while some patients had no problems with sight, intelligence, or speaking ability, they were unable to read the text [3]. In 1887, German physician Rudolf Berlin first used the term dyslexia in his research [4]. The most current definition of dyslexia is codified by U.S. Federal law as follows: “The term dyslexia means an unexpected difficulty in reading for an individual who has the intelligence to be a much better reader, most commonly caused by a difficulty in the phonological processing (the appreciation of the individual sounds of spoken language), which affects the ability of an individual to speak, read, and spell.” [5]
The etiology of dyslexia is familial, occurring in 50% of children who have a parent with dyslexia and in 50% of the siblings of dyslexic persons [5]. Dyslexia is best explained by the differences in multiple genes, each contributing a small amount to its expression.
According to LaBuda and DeFries [6], the reading limitations of twins with reading disabilities are attributed to the following factors: 40% genetics, 35% shared environmental factors (socioeconomic status, parents’ reading ability, education method), and 25% to unique environmental factors. The genes that are reportedly most related to dyslexia are DCDC2 (doublecortin domain-containing protein 2) and KIAA0319. The DYX1-9 (dyslexia susceptibility 1–9) and ROBO1 (roundabout 1) genes are also known to be related [7].
Neurobiology
1. Reading pathway
To understand a written word, it is necessary to look at and interpret it (i.e., the process of extracting meaning from meaning memory) and be able to look at it and read it aloud (i.e., the process of converting it into words, phonological mediation). The process of converting text into words is a model of an independent but interactive dual-pathway system (Fig. 1).
Fig. 1.

Reading pathway of dual-route model and subsequent classification of dyslexia.
Individuals with dyslexia have difficulty converting spoken words into segmented, smaller elemental units of sound (phonemes). This process is essential for reading because it requires the ability to link the lexicon (visual word) or printed symbols to sounds.
Increasing evidence indicates that disruption of attention mechanisms may also play an important role in reading difficulties [5]. For this reason, many patients with attention-deficit hyperactivity disorder (ADHD) who visited the pediatric neurodevelopmental clinic were also diagnosed with dyslexia.
2. Classification
Dyslexia can be classified according to the location of each problem along the reading path (Fig. 1). First, it can be categorized into peripheral dyslexia and central dyslexia. Peripheral dyslexia refers to a reading disorder that presents as an impaired visual analysis of the word form, and central dyslexia refers to a deficit in the process following visual analysis such as semantic access or phonological mediation. Peripheral dyslexia may present as an inability to distinguish the direction of a sign, such as an arrow pointing left or right.
Central dyslexia can be classified into superficial dyslexia, phonological dyslexia, and deep dyslexia. Superficial dyslexia refers to reading by phoneme-grapheme conversion due to damage to the semantic or visual vocabulary pathway within the reading pathway. During the reading process, nonwords, regular words, or high-frequency words can be read accurately, whereas low-frequency irregular words are prone to errors. Phonological dyslexia uses the semantic pathway because of a faulty phonological pathway. In phonological dyslexia, real words can be read better than nonwords, and nonwords are read as similar real words. Deep dyslexia is characterized by a problematic semantic system and phonological pathway. In this case, real words are read better than nonwords, and reading actual words can also show semantic errors, for example, reading “cat” as “dog.”
3. Functional neuroimaging research and major brain areas related to reading
Functional brain imaging in both children and adults with dyslexia demonstrates inefficient functioning of the posterior brain systems of the left hemisphere, a pattern referred to as the neural signature of dyslexia [8]. Shaywitz et al. [8] used functional magnetic resonance imaging (fMRI) to study this effect by conducting a tapping task phonological analysis. They found significantly greater activation in posterior reading systems in typical readers than in readers with dyslexia. Readers with dyslexia compensate by developing anterior systems bilaterally, and the right homolog of the left visual word form area (VWFA) enables accurate reading, but it does not support fluent or rapid reading [9].
According to functional neuroimaging studies, the important areas of the brain related to reading include the left occipital-temporal region (VWFA), the inferior frontal cortex (Broca’s area), the midtemporal lobe region, and the inferior parietotemporal area (Fig. 2) [8].
Fig. 2.
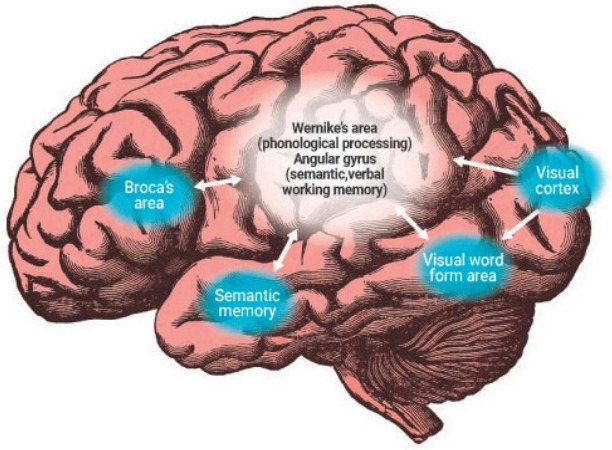
The major brain regions and interconnectivity involved in reading.
1) Inferior frontal lobe (Broca’s area)
When reading irregular low-frequency words, Broca’s area displays more activation on fMRI, which plays an important role in grapheme-phoneme conversion [10,11]. It is also thought that blood oxygen level-dependent activation reflects increased meaning processing [12]. Heim et al. suggested that both functions for reading are interrelated and that the Brodmann area 45 is related to meaning retrieval, while BA44 is related to graphemephoneme conversion [11,13].
2) Inferior parietotemporal lobe
The inferior parietotemporal lobe consists of 2 anatomical regions: the supramarginal gyrus adjacent to the superior temporal lobe and the angular gyrus. The supramarginal gyrus is related to Wernicke’s area (phonological processing), while the angular gyrus is related to the process of combining verbal working memory and semantic concepts or meaning [14,15]. In particular, it has been suggested that the left supramarginal gyrus is related to grapheme-phoneme conversion. When excitatory transcranial magnetic stimulation (TMS) was applied to this area, nonword reading was promoted, and inhibitory TMS interfered with the phonological process for visually presented words [16,17].
3) Anterior, middle temporal lobe
This area is mainly associated with semantic memory. In reading, these areas are related to the semantic pathway (converting letters to phonemes through meaning) [18]. In fMRI studies, they show more activation in semantics relative to phonological processing of written words [18]. Patients with semantic memory loss-type dementia and superficial dyslexia show damage to this area [19].
4) Left occipitotemporal sulcus
The VWFA is a functional area of the left fusiform gyrus and surrounding cortex that is involved in identifying words and letters [20]. This area is essential to a rapid reading ability because it enhances the perception of words by becoming specifically tuned to recognizing the recurring properties of a writing system [20]. VWFA impairment causes pure alexia, a selective deficit in word recognition [21].
These 4 brain regions are systematically connected to perform reading. Phonological processing, a key matter in dyslexia, is related to the inferior parietotemporal area. The anterior, middle temporal lobe, and inferior frontal lobe are responsible for understanding reading meaning, while the left occipitotemporal area (VWFA) is involved in fast reading.
Clinical features
The epidemiology of dyslexia reveals that it is perhaps the most common neurobehavioral disorder affecting children, with a prevalence of 3%–17.5% (Table 1) [22-30]. Dyslexia is a dimensionally diagnosed disease that belongs to the lower part of the total population on a continuous line. Dyslexia refers to difficulty in reading appropriately according to an individual’s cognitive function and age. While genetic and neurobiological causes have been identified, there are no specific markers or imaging tests for diagnosis. The diagnosis considers medical history, observation, psychological evaluation, and reading test results.
Table 1.
Prevalence of dyslexia by region and language
| Study | Year | Region | Language | Prevalence |
|---|---|---|---|---|
| Lindgren et al. [23] | 1985 | Italy | Italian | 8.5% (Gross-national comparisons of prevalence in Italy and the United States) |
| Shaywitz et al. [22,24] | 1997 | US | English | 5%–17.5% |
| Hulme and Snowling [25] | 2011 | UK | English | 10.3% (1,324 UK primary school children) |
| Wilcke et al. [26] | 2016 | Germany | German | About 5% |
| Kim et al. [27] | 2018 | Korea | Korean | 3.2%–8.5% |
| Verpalen et al. [28] | 2018 | Netherlands | Dutch | About 5% |
| Kita et al. [29] | 2019 | Japan | Japanese | 3.0%–11.2% |
| Lin et al. [30] | 2020 | China | Chinese | 3.0%–12.6% |
Children with dyslexia can read, although their reading speed is slower than that of nonreading impaired children of the same age, and more effort is required [31,32]. Children with dyslexia have more difficulty with vocabulary and syntax compared to controls at approximately 36 and 42 months [33,34]. Children diagnosed with dyslexia at 3–4 years of age have a poor sense of prosody (sound stress, fluctuations, pitches, or repetition of homonyms). When singing nursery rhymes, they have difficulty recognizing rhyming words. Children with dyslexia have less knowledge of letters, phonology, and vocabulary at the age of 5 compared to non–reading-impaired children [33].
In kindergarten, children have difficulty recognizing the names and pronunciations of letters (phonemes) [31]. Most of the words are not spoken in order, and the first sound of the word may be omitted or the sounds of the word group be inverted. Additionally, the order of the syllables may change, and there may be problems with articulation.
It is important for pediatricians to know the clinical features of preschool children that can predict dyslexia because of early diagnosis and intervention before school age (Table 2).
Table 2.
Predictors of dyslexia in preschool children
| Clinical features | Family history of dyslexia (one of the most strongest risk factor) |
| Delayed language development | |
| delayed onset of talking | |
| short mean length of utterances | |
| low complexity of syllables produced | |
| poor receptive or expressive vocabulary | |
| Poor home literacy environment | |
| Poor processing of rhythm, prosody and beat synchronization | |
| Poor ability to pronounce spoken nonsense words (pseudoword) | |
| Difficulty in report the sound that a letter make | |
| 20% to 40% of ADHD have dyslexia, and children with autism spectrum disorder, other behavioral disorders are also at increased risk of having dyslexia | |
| Findings of dyslexia-related test | Rapid automatized naming: poor ability to automatically retrieve the names of objects, letters, colors |
| Poor phonological awareness for spoken word (blending sounds together to make a word or segmenting words into parts) | |
| Lower working memory | |
| Lower level auditory or visual processing | |
| Poor performance of preschool early literacy indicators assessment |
ADHD, attention-deficit hyperactivity disorder.
In children with dyslexia, characters are often recognized backward, especially before the age of 7 years [35]. Preschool-aged children with vocabulary and syntax difficulties and a family history of dyslexia are at risk of being diagnosed with dyslexia later on, but it is difficult to differentiate between dyslexia and normal reading during development [33,36]. Therefore, it is necessary to check for a family history of dyslexia in children with language delays and monitor possible progression to dyslexia during school age [31].
In the first grade, children may present with difficulties reading sight words, experience slow progress with reading, or have illegible handwriting. Children with dyslexia are poorly fluent at grade level and frequently experience pronunciation errors when reading unfamiliar words. When learning letters, children with dyslexia memorize them differently in the logographic stage. The character memorization method entails recognizing characters as pictures using visual cues without using the phonics of the letters. In elementary school, first, second, and third graders learn to read to prepare for learning, after which they learn through reading [36,37].
Even after reading interventions and learning decoding skills, children may continue to be slow and more laborious readers [33]. In elementary school, children with dyslexia have poor academic performance, accompanied by various behavioral problems such as refusal to attend school, low self-esteem, and somatic complaints [31].
Since reading is a skill in the opposite direction of the writing process, it is highly associated with dyslexia. It is more difficult for children with dyslexia to learn a second language than the general population because it is more difficult to process phonology in a second language as well as in their first language [38]. Dyslexia symptoms continue into adulthood. Brain imaging studies have revealed that the automated reading pathway, which his essential to reading fluency, fails to activate in the mind of a dyslexic person. A common misconception is that children can “outgrow” dyslexia. Dyslexia persists through adulthood, and while reading accuracy can be achieved, fluency is still lacking [31].
Evaluation and diagnosis
Dyslexia should be considered for differential diagnosis if there are concerns about academic achievement and/or reading [37]. The assessment of children with learning disabilities routinely requires multidisciplinary collaboration between professionals, including psychologists, educators, audiologists, and occupational and speech therapists. Pediatricians should remain vigilant for symptoms of dyslexia when conducting developmental screening tests such as the Korean Developmental Screening Test in patients up to the age of 6 years.
Because early intervention before entering school is effective and can prevent learning deterioration due to dyslexia, it is necessary to provide the appropriate test for early diagnosis.
Dyslexia should be considered among patients who seek treatment due to learning difficulties or ADHD symptoms. It is important to review reading milestones based on age to understand comparisons with same-age peers [37]. Pediatricians should enquire about the child’s ability to recognize letters in kindergarten, read words in the first grade, and read and understand short picture books in the second grade [37]. Because dyslexia has a large genetic predisposition, and reports indicate that 65% of children have parents with dyslexia, it is important to obtain a comprehensive family history [39].
The direct observation of a child’s writing and spelling capabilities can be useful in clinical assessments. The practitioner may require the child to write his or her name or simple words using paper and pencils using provided examples. The child should identify the relevant letter, make the corresponding letter sound, and read the word aloud [31]. A definitive diagnosis of dyslexia is made by pediatricians after evaluating assessments are made by speech pathologists, psychologists, reading experts, and educational experts.
In the United States, the IDEA law allows children with dyslexia to be evaluated in the public school system and receive appropriate education and intervention [40]. The evaluation might include testing language and reading abilities, cognitive or IQ testing, speech and language evaluation, and/or social-emotional evaluations.
Because dyslexia is an underlying deficit in phonological processing, neuropsychological testing should focus on assessing phonological processing. Apart from phonological processing, word decoding, comprehension, and fluency are all assessed by these tools to varying degrees.
The evaluations for dyslexia used in Korea include basic academic skills assessment (BASA)-reading, comprehensive learning test-reading (CLT-R), test of reading achievement and reading cognitive processes ability (RARCP), and Korean language base reading assessment (KOLRA). Test methods mainly comprise detailed evaluation items such as word recognition, reading fluency/reading comprehension, letter knowledge, rapid automatic naming test, and phonological memory.
Some conditions that frequently occur with dyslexia include ADHD, which can have a 20%–40% co-occurrence, certain learning disabilities with math disorders (40% co-occurrence), and autism spectrum disorder (~30% co-occurrence) [41]. It is key to conduct an audiological evaluation and a vision assessment to understand whether impairments in hearing or vision compound or exacerbate the child’s difficulties.
Dyslexia requires a differential diagnosis, such as intellectual disability, hearing, visual impairment, and history or diagnosis of ADHD.
Management
The early diagnosis of dyslexia in children is pertinent to achieving successful early interventions in the reading process, which can improve reading results [37]. The management of dyslexia often requires a lifespan approach because it is a chronic condition [37,42,43]. There is no effective medicinal or nutritional method for treating dyslexia [44]. The effects of visual training, music education, and chiropractic interventions on dyslexia are doubtful [45]. In the case of dyslexia presenting alongside ADHD, treatment of comorbid ADHD is important for improving dyslexia, and atomoxetine is effective in this regard [46]. If children respond well to interventional reading trials, then they may not require any additional reading instruction, which may indicate that they have a developmental lag in reading skills and not dyslexia.
Evidence-based interventions focus on building phonemic awareness (e.g., speech is manipulated into syllables and then into words). Interventions should be performed by a teacher/reading expert, preferably in small groups with other children of a similar level [47]. Interventions should systematically target education on 1 or 2 phonemes at a time, build skills sequentially, and include a multisensory approach [42,43]. Reading skills improve meaningfully when these interventions are implemented [42].
Phoneme recognition training is followed by phonics training to recognize the correspondence between letters and sounds [48]. After mastering phonics, the focus should be to read rapidly and accurately, and then practice automatic comprehension while reading [49,50]. Using audiobooks, reading storybooks, and repeated exposure to words outside of school provides opportunities for increasing vocabulary complexity and vocabulary enrichment [31,37].
During the senior education phase, such as in high schools and universities, it is necessary to provide accommodations for students with dyslexia, such as granting additional test time, using audiobooks instead of written texts, or taking oral tests [51].
Conclusions
Reading is a complex cognitive skill that involves various areas of the brain. Dyslexia is related to problems such as poor word recognition, limited decoding ability, and impaired automatic word recognition. Clinical symptoms of dyslexia vary by age, and the main diagnostic factor is that the patient’s reading ability is insufficient compared to their cognitive ability and chronological age. Furthermore, there is a central problem in phonological processing.
Interventions for dyslexia can affect reading ability by causing changes in brain function and structure [52]. An accurate diagnosis and timely specialized intervention are important in children with dyslexia. Successful management includes early childhood intervention and the provision of suitable accommodations after adolescence.
Key message
· Neurobiological studies using functional brain imaging have uncovered the reading pathways, brain regions involved in reading, and neurobiological abnormalities of dyslexia.
· An accurate diagnosis and timely specialized intervention are important in children with dyslexia. When national infant development screening tests have been conducted as in Korea, if a language developmental delay and early predictors of dyslexia are detected, the progression to dyslexia should be carefully observed and early intervention provided.
Footnotes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
References
- 1.Yell ML, Shriner JG, Katsiyannis A. Individuals with disabilities education improvement act of 2004 and IDEA regulations of 2006: implications for educators, administrators, and teacher trainers. Focus Except Child. 2006;39:1–24. [Google Scholar]
- 2.American Psychiatric Association . Neurodevelopmental disorders: DSM-5® selections. Washington, DC: American Psychiatric Pub; 2015. [Google Scholar]
- 3.Rehnberg V, Walters E. The life and work of Adolph Kussmaul 1822–1902: ‘Sword swallowers in modern medicine’. J Intensive Care Soc. 2017;18:71–2. doi: 10.1177/1751143716676822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wagner RF. 5. Rudolf Berlin: originator of the term dyslexia. Bull Orton Soc. 1973;23:57–63. [Google Scholar]
- 5.Kliegman RM, Stanton BF, St. Geme JW III, Schor NF, Behrman RE, editors. Nelson textbook of pediatrics. 21st ed. Philadelphia (PA): Elsevier; 2020. [Google Scholar]
- 6.LaBuda MC, DeFries JC. Cognitive abilities in children with reading disabilities and controls: a follow-up study. J Learn Disabil. 1988;21:562–6. doi: 10.1177/002221948802100908. [DOI] [PubMed] [Google Scholar]
- 7.Schumacher J, Hoffmann P, Schmäl C, Schulte-Körne G, Nöthen MM. Genetics of dyslexia: the evolving landscape. J Med Genet. 2007;44:289–97. doi: 10.1136/jmg.2006.046516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shaywitz BA, Shaywitz SE, Pugh KR, Mencl WE, Fulbright RK, Skudlarski P, et al. Disruption of posterior brain systems for reading in children with developmental dyslexia. Biol Psychiatry. 2002;52:101–10. doi: 10.1016/s0006-3223(02)01365-3. [DOI] [PubMed] [Google Scholar]
- 9.Shaywitz SE. Overcoming dyslexia: a new and complete science-based program for reading problems at any level. New York: Alfred A. Knopf; 2003. [Google Scholar]
- 10.Fiez JA, Tranel D, Seager-Frerichs D, Damasio H. Specific reading and phonological processing deficits are associated with damage to the left frontal operculum. Cortex. 2006;42:624–43. doi: 10.1016/s0010-9452(08)70399-x. [DOI] [PubMed] [Google Scholar]
- 11.Fiebach CJ, Friederici AD, Müller K, von Cramon DY. fMRI evidence for dual routes to the mental lexicon in visual word recognition. J Cogn Neurosci. 2002;14:11–23. doi: 10.1162/089892902317205285. [DOI] [PubMed] [Google Scholar]
- 12.Jobard G, Crivello F, Tzourio-Mazoyer N. Evaluation of the dual route theory of reading: a metanalysis of 35 neuroimaging studies. NeuroImage. 2003;20:693–712. doi: 10.1016/S1053-8119(03)00343-4. [DOI] [PubMed] [Google Scholar]
- 13.Heim S, Eickhoff SB, Amunts K. Different roles of cytoarchitectonic BA 44 and BA 45 in phonological and semantic verbal fluency as revealed by dynamic causal modelling. NeuroImage. 2009;48:616–24. doi: 10.1016/j.neuroimage.2009.06.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Paulesu E, Frith CD, Frackowiak RS. The neural correlates of the verbal component of working memory. Nature. 1993;362:342–5. doi: 10.1038/362342a0. [DOI] [PubMed] [Google Scholar]
- 15.Binder JR, Desai RH. The neurobiology of semantic memory. Trends Cogn Sci. 2011;15:527–36. doi: 10.1016/j.tics.2011.10.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Costanzo F, Menghini D, Caltagirone C, Oliveri M, Vicari S. High frequency rTMS over the left parietal lobule increases non-word reading accuracy. Neuropsychologia. 2012;50:2645–51. doi: 10.1016/j.neuropsychologia.2012.07.017. [DOI] [PubMed] [Google Scholar]
- 17.Sliwinska MW, Khadilkar M, Campbell-Ratcliffe J, Quevenco F, Devlin JT. Early and sustained supramarginal gyrus contributions to phonological processing. Front Psychol. 2012;3:161. doi: 10.3389/fpsyg.2012.00161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mechelli A, Josephs O, Lambon Ralph MA, McClelland JL, Price CJ. Dissociating stimulus-driven semantic and phonological effect during reading and naming. Hum Brain Mapp. 2007;28:205–17. doi: 10.1002/hbm.20272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wilson SM, Brambati SM, Henry RG, Handwerker DA, Agosta F, Miller BL, et al. The neural basis of surface dyslexia in semantic dementia. Brain. 2009;132:71–86. doi: 10.1093/brain/awn300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.McCandliss BD, Cohen L, Dehaene S. The visual word form area: Expertise for reading in the fusiform gyrus. Trends Cogn Sci. 2003;7:293–9. doi: 10.1016/s1364-6613(03)00134-7. [DOI] [PubMed] [Google Scholar]
- 21.Dehaene S, Cohen L. The unique role of the visual word form area in reading. Trends Cogn Sci. 2011;15:254–62. doi: 10.1016/j.tics.2011.04.003. [DOI] [PubMed] [Google Scholar]
- 22.Peterson RL, Pennington BF. Developmental dyslexia. Lancet. 2012;379:1997–2007. doi: 10.1016/S0140-6736(12)60198-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lindgren S, De Renzi E, Richman L. Cross-national comparisons of developmental dyslexia in Italy and the United States. Child Dev. 1985;56:1404–17. [PubMed] [Google Scholar]
- 24.Shaywitz SE, Shaywitz BA, Fletcher JM, Escobar MD. Prevalence of reading disability in boys and girls. Results of the Connecticut longitudinal study. JAMA. 1990;264:998–1002. [PubMed] [Google Scholar]
- 25.Hulme C, Snowling MJ. Children’s reading comprehension difficulties: nature, causes, and treatments. Curr Dir Psychol Sci. 2011;20:139–42. [Google Scholar]
- 26.Wilcke A, Müller B, Schaadt G, Kirsten H, Boltze J, Members of the Legascreen Consortium High acceptance of an early dyslexia screening test involving genetic analyses in Germany. Eur J Hum Genet. 2016;24:178–82. doi: 10.1038/ejhg.2015.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kim AH, Kim EJ, Kim JK, Jung DY. Who are the students with learning disabilities, dyslexia, poor learning (including borderline intelligence) and learning support, and is the educational support okay? Notes on the role and challenges of special education. Korean J Spec Educ. 2018;53:1–21. [Google Scholar]
- 28.Verpalen A, Van de Vijver F, Backus A. Bias in dyslexia screening in a Dutch multicultural population. Ann Dyslexia. 2018;68:43–68. doi: 10.1007/s11881-018-0155-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kita Y, Ashizawa F, Inagaki M. Prevalence estimates of neurodevelopmental disorders in Japan: A community sample questionnaire study. Psychiatry Clin Neurosci. 2020;74:118–23. doi: 10.1111/pcn.12950. [DOI] [PubMed] [Google Scholar]
- 30.Lin Y, Zhang X, Huang Q, Lv L, Huang A, Li A, et al. The prevalence of dyslexia in primary school children and their Chinese literacy assessment in Shantou, China. Int J Environ Res Public Health. 2020;17:7140. doi: 10.3390/ijerph17197140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Shaywitz SE, Shaywitz BA. Dyslexia (specific reading disability) Pediatr Rev. 2003;24:147–53. doi: 10.1542/pir.24-5-147. [DOI] [PubMed] [Google Scholar]
- 32.Lyon GR, Shaywitz SE, Shaywitz BA. A definition of dyslexia. Ann Dyslexia. 2003;53:1–14. [Google Scholar]
- 33.Scarborough HS. Early syntactic development of dyslexic children. Ann Dyslexia. 1991;41:207–20. doi: 10.1007/BF02648087. [DOI] [PubMed] [Google Scholar]
- 34.McCardle P, Scarborough HS, Catts HW. Predicting, explaining, and preventing children's reading difficulties. Learn Disabil Res Pract. 2001;16:230–9. [Google Scholar]
- 35.Blackburne LK, Eddy MD, Kalra P, Yee D, Sinha P, Gabrieli JD. Neural correlates of letter reversal in children and adults. PLoS One. 2014;9:e98386. doi: 10.1371/journal.pone.0098386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Vellutino FR, Fletcher JM, Snowling MJ, Scanlon DM. Specific reading disability (dyslexia): What have we learned in the past four decades? J Child Psychol Psychiatry. 2004;45:2–40. doi: 10.1046/j.0021-9630.2003.00305.x. [DOI] [PubMed] [Google Scholar]
- 37.Shaywitz SE, Gruen JR, Shaywitz BA. Management of dyslexia, its rationale, and underlying neurobiology. Pediatr Clin North Am. 2007;54:609–23. doi: 10.1016/j.pcl.2007.02.013. [DOI] [PubMed] [Google Scholar]
- 38.Shaywitz SE, Fletcher JM, Holahan JM, Shneider AE, Marchione KE, Stuebing KK, et al. Persistence of dyslexia: the Connecticut longitudinal study at adolescence. Pediatrics. 1999;104:1351–9. doi: 10.1542/peds.104.6.1351. [DOI] [PubMed] [Google Scholar]
- 39.Scarborough HS. Predicting the future achievement of second graders with reading disabilities: Contributions of phonemic awareness, verbal memory, rapid naming, and IQ. Ann Dyslexia. 1998;48:115–36. [Google Scholar]
- 40.Yell ML, Shriner JG. Katsiyannis A. Individuals with disabilities education improvement act of 2004 and IDEA regulations of 2006: Implications for educators, administrators, and teacher trainers. Focus Except Child. 2006;39:1–24. [Google Scholar]
- 41.Hendren RL, Haft SL, Black JM, White NC, Hoeft F. Recognizing psychiatric comorbidity with reading disorders. Front Psychiatry. 2018;9:101. doi: 10.3389/fpsyt.2018.00101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Torgesen JK, Wagner RK, Rashotte CA, Rose E, Lindamood P, Conway T, et al. Preventing reading failure in young children with phonological processing disabilities: Group and individual responses to instruction. J Educ Psychol. 1999;91:579–93. [Google Scholar]
- 43.Torgesen JK, Alexander AW, Wagner RK, Rashotte CA, Voeller KK, Conway T. Intensive remedial instruction for children with severe reading disabilities: immediate and long-term outcomes from two instructional approaches. J Learn Disabil. 2001;34:33–58. doi: 10.1177/002221940103400104. [DOI] [PubMed] [Google Scholar]
- 44.Siegel LS. Perspectives on dyslexia. Paediatr Child Health. 2006;11:581–7. doi: 10.1093/pch/11.9.581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.American Academy of Pediatrics Learning disabilities, dyslexia, and vision. Pediatrics. 2009;124:837–44. doi: 10.1542/peds.2009-1445. [DOI] [PubMed] [Google Scholar]
- 46.Germanò E, Gagliano A, Curatolo P. Comorbidity of ADHD and dyslexia. Dev Neuropsychol. 2010;35:475–93. doi: 10.1080/87565641.2010.494748. [DOI] [PubMed] [Google Scholar]
- 47.Breaux KC, Lichtenberger EO. Essentials of KTEA-3 and WIAT-III Assessment. Hoboken (NJ): John Wiley & Sons; 2016. [Google Scholar]
- 48.Galuschka K, Ise E, Krick K, Schulte-Körne G. Effectiveness of treatment approaches for children and adolescents with reading disabilities: A meta-analysis of randomized controlled trials. PLoS One. 2014;9:e89900. doi: 10.1371/journal.pone.0089900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Chard DJ, Vaughn S, Tyler BJ. A synthesis of research on effective interventions for building reading fluency with elementary students with learning disabilities. J Learn Disabil. 2002;35:386–406. doi: 10.1177/00222194020350050101. [DOI] [PubMed] [Google Scholar]
- 50.Wolf M. Katzir-Cohen T. Reading fluency and its intervention. Sci Stud Read. 2001;5:211–39. [Google Scholar]
- 51.Tressoldi PE, Lorusso ML, Brenbati F, Donini R. Fluency remediation in dyslexic children: Does age make a difference? Dyslexia. 2008;14:142–52. doi: 10.1002/dys.359. [DOI] [PubMed] [Google Scholar]
- 52.Munzer T, Hussain K, Soares N. Dyslexia: neurobiology, clinical features, evaluation and management. Transl Pediatr. 2020;9:S36. doi: 10.21037/tp.2019.09.07. [DOI] [PMC free article] [PubMed] [Google Scholar]