

Abstract
目的
探讨自体血纤维蛋白凝块对前交叉韧带(anterior cruciate ligament,ACL)重建术后腱-骨愈合的作用及意义。
方法
以 2014 年 10 月—2016 年 1 月收治并符合选择标准的 34 例(34 膝)ACL 损伤患者作为研究对象,随机分为两组(n=17);ACL 重建术中试验组采用自体血纤维蛋白凝块,对照组不作该处理。两组患者术前前抽屉试验、Lachman 试验及轴移试验均为阳性。两组患者性别、年龄、致伤原因、损伤侧别、受伤至手术时间以及术前膝关节活动度、Lysholm 评分、美国特种外科医院(HSS)评分等一般资料比较,差异均无统计学意义(P<0.05),具有可比性。记录并比较两组患者术后前抽屉试验、Lachman 试验及轴移试验检查结果;术后 6、24、48 周,检查患膝关节活动度、Lysholm 评分、HSS 评分,评定膝关节功能恢复情况;行 MRI 检查,测量移植物信号强度、信噪比以及骨隧道扩大程度及移植物腱-骨结点 T2 值。
结果
两组患者术后均获随访 48 周。术后切口均Ⅰ期愈合,无 1 例出现关节内感染及关节粘连。术后两组患者前抽屉试验、Lachman 试验及轴移试验均为阴性。术后 6、24、48 周,试验组 Lysholm 评分均明显高于对照组(P<0.05);而两组膝关节活动度比较差异无统计学意义(P>0.05)。术后 6 周,两组 HSS 评分比较差异无统计学意义(P>0.05);24、48 周时试验组 HSS 评分明显高于对照组(P<0.05)。MRI 复查显示,术后 6、24、48 周两组移植物信号强度、骨隧道扩大程度、移植物信噪比比较,差异均有统计学意义(P<0.05)。术后 6、24 周两组移植物腱-骨结点 T2 值比较,差异有统计学意义(P<0.05);48 周时比较差异无统计学意义(P>0.05)。
结论
ACL 重建术中采用自体血纤维蛋白凝块,能够有效促进移植物再血管化、加快腱-骨愈合进程。
Keywords: 前交叉韧带, 韧带重建术, 自体血纤维蛋白凝块, 腱-骨愈合
Abstract
Objective
To observe the effect and significance of autologous fibrin clot on tendon-bone healing after anterior cruciate ligament (ACL) reconstruction.
Methods
Between October 2014 and January 2016, 34 patients (34 knees) with ACL injury were enrolled in the study. During ACL reconstruction, autologous fibrin clot was used in 17 cases (trial group) and was not used in 17 cases (control group). The anterior drawer test, Lachman test, and axial displa-cement test were positive in 2 groups before operation. There was no significant difference in gender, age, causes of injury, injury side, disease cause, and preoperative knee joint activity, Lysholm score, and American Hospital for Special Surgery (HSS) score between 2 groups (P>0.05), with comparable. The results of anterior drawer test, Lachman test, and axial displacement test were recorded and compared between 2 groups after operation. The knee joint activity, Lysholm score, and HSS score were used to evaluate the knee function recovery at 6, 24, and 48 weeks after operation; the graft signal intensity, graft signal to noise ratio, bone tunnel expansion, and graft tendon-bone node T2 value were measured.
Results
All patients were followed up 48 weeks. Surgical incision healed at stage I. No joint infection and joint adhesion occurred. The drawer test, Lachman test, and axial shift test were negative in 2 groups. At 6, 24, and 48 weeks after operation, the Lysholm score of trial group was significantly higher than that of control group (P<0.05); there was no significant difference in knee joint activity between 2 groups (P>0.05). The HSS score of trial group was significantly higher than that of control group at 24 and 48 weeks (P<0.05), but no significant difference was found at 6 weeks (P>0.05). MRI measu-rement showed that there was significant difference in graft signal intensity, bone tunnel expansion, and graft signal to noise ratio between 2 groups at 6, 24, and 48 weeks after operation (P<0.05). There was no significant difference in graft tendon-bone node T2 value between 2 groups (P>0.05) at 48 weeks after operation, but difference was significant at 6 and 24 weeks (P<0.05).
Conclusion
Autologous fibrin clot can effectively enhance graft revascularization, and accelerate the process of tendon-bone healing after ACL reconstruction.
Keywords: Anterior cruciate ligament, ligament reconstruction, autologous fibrin clot, tendon-bone healing
前交叉韧带(anterior cruciate ligament,ACL)损伤是临床上常见的膝关节损伤类型,应用自体腘绳肌腱解剖重建 ACL 是目前公认的最有效治疗手段[1]。但 ACL 重建术后仍存在移植物腱-骨愈合不良问题,因组织结构不同、血供较差,要实现移植物韧带化所需时间长[2],严重影响了患者膝关节功能的恢复。自体血纤维蛋白凝块含有各种有利于组织修复的因子,且取材方便、无免疫排斥反应。经河南省人民医院医学伦理委员会批准,我们进行了临床研究,在 ACL 重建术中将自体血纤维蛋白凝块嵌于腘绳肌腱移植物,以探讨自体血纤维蛋白凝块是否具有促进腱-骨愈合的作用。报告如下。
1. 临床资料
1.1. 患者选择标准
纳入标准:① 急、慢性 ACL 损伤患者,存在典型临床症状及 MRI 表现;② 无明显心脑血管疾病及肝、肾、肺功能不全者;③ 术后严格按照康复计划进行患膝关节功能锻炼。排除标准:① 合并严重膝关节脱位的多发韧带损伤及胫骨平台、股骨内外侧髁骨折患者;② 因各种因素未完成完整随访者。
2014 年 10 月—2016 年 1 月,共 34 例单膝 ACL 损伤患者符合选择标准,纳入研究。采用随机数字表法将患者随机分为 2 组,每组 17 例。其中,试验组 ACL 重建术中采用自体血纤维蛋白凝块,对照组 ACL 重建术中不采用自体血纤维蛋白凝块。患者均知情同意。
1.2. 一般资料
试验组:男 9 例,女 8 例;年龄 24~39 岁,平均 30.2 岁。左膝 8 例,右膝 9 例。受伤至手术时间 10~24 d,平均 19.9 d。对照组:男 11 例,女 6 例;年龄 22~39 岁,平均 30.9 岁。左膝 10 例,右膝 7 例。受伤至手术时间 12~27 d,平均 19.4 d。两组患者均为运动扭伤,术前前抽屉试验、Lachman 试验及轴移试验均为阳性。两组患者性别、年龄、致伤原因、损伤侧别、受伤至手术时间以及术前膝关节活动度、Lysholm 评分、美国特种外科医院(HSS)评分等一般资料比较,差异无统计学意义(P<0.05),具有可比性。见表 1~3。
表 1.
Comparison of Lysholm score between 2 groups before and after operation (n=17,
 )
)
两组手术前后 Lysholm 评分比较(n=17,
 )
)
| 组别
Group |
术前
Preoperative |
术后 6 周
Postoperative at 6 weeks |
术后 24 周
Postoperative at 24 weeks |
术后 48 周
Postoperative at 48 weeks |
| 试验组
Trial group |
35.88±3.98 | 63.83±3.84 | 83.29±2.08 | 91.65±1.73 |
| 对照组
Control group |
36.21±3.33 | 60.82±2.90 | 80.41±1.91 | 86.12±2.29 |
| 统计值
Statistic |
t=–0.187
P= 0.853 |
t=2.569
P=0.015 |
t=4.208
P=0.000 |
t=7.948
P=0.000 |
表 3.
Comparison of range of motion between 2 groups before and after operation (n=17,
 )
)
两组手术前后膝关节活动度比较(n=17,
 )
)
| 组别
Group |
术前
Preoperative |
术后 6 周
Postoperative at 6 weeks |
术后 24 周
Postoperative at 24 weeks |
术后 48 周
Postoperative at 48 weeks |
| 试验组
Trial group |
100.29±8.74 | 102.00±5.36 | 116.24±5.68 | 127.00±2.37 |
| 对照组
Control group |
101.47±7.66 | 103.76±3.35 | 119.12±4.61 | 125.65±3.30 |
| 统计值
Statistic |
t=–0.417
P= 0.679 |
t=–1.151
P= 0.260 |
t=–1.624
P= 0.114 |
t=–1.389
P= 0.174 |
表 2.
Comparison of HSS score between 2 groups before and after operation (n=17,
 )
)
两组手术前后 HSS 评分比较(n=17,
 )
)
| 组别
Group |
术前
Preoperative |
术后 6 周
Postoperative at 6 weeks |
术后 24 周
Postoperative at 24 weeks |
术后 48 周
Postoperative at 48 weeks |
| 试验组
Trial group |
35.59±4.12 | 58.29±1.93 | 79.06±2.25 | 89.76±2.51 |
| 对照组
Control group |
36.18±3.43 | 57.59±2.35 | 72.06±2.82 | 84.53±3.16 |
| 统计值
Statistic |
t=–0.452
P= 0.654 |
t=0.958
P=0.345 |
t=8.007
P=0.000 |
t=5.341
P=0.000 |
1.3. 手术方法
两组患者均按照常规自体腘绳肌腱重建 ACL 手术步骤进行。试验组:全麻下,患者取仰卧位。首先,麻醉下行前抽屉试验及 Lachman 试验,明确均为阳性。然后常规消毒铺巾,取膝关节前内侧、前外侧入路,置入关节镜,依次探查膝关节情况,清理残余韧带纤维,清理关节腔。自胫骨结节下 4 cm 处作切口,取出半腱肌及股薄肌肌腱,对折后用 15 mm Endobutton 带袢钛板固定对折处,牵引备用。术中由护士取患者静脉血 50 mL,于无菌烧杯中沿同一方向低速搅拌约 10 min,玻璃棒上逐渐黏附自体血纤维蛋白凝块;采用可吸收缝合线将血凝块缝于制备的腘绳肌腱移植物股骨端。关节镜下于 ACL 股骨及胫骨附着点,钻取股骨及胫骨骨隧道。膝关节极度屈曲位,用带线克氏针牵引肌腱通过胫骨骨道及股骨骨道,以 15 mm Endobutton 带袢钛板悬吊固定,胫骨骨道口用可吸收挤压钉固定后剪去多余肌腱移植物。移植物进入股骨隧道时,大于隧道直径的自体血纤维蛋白凝块会受到挤压而涂抹在肌腱上并封堵骨道口(图 1、2)。生理盐水冲洗关节腔,常规置引流管 1 根后,关闭切口并加压包扎。对照组:除术中不采用自体血纤维蛋白凝块外,其余操作与试验组一致。
图 1.

Autologous fibrin clots prepared during surgery were stitched to hamstring tendon grafts
术中制备自体血纤维蛋白凝块并缝至腘绳肌腱移植物
图 2.
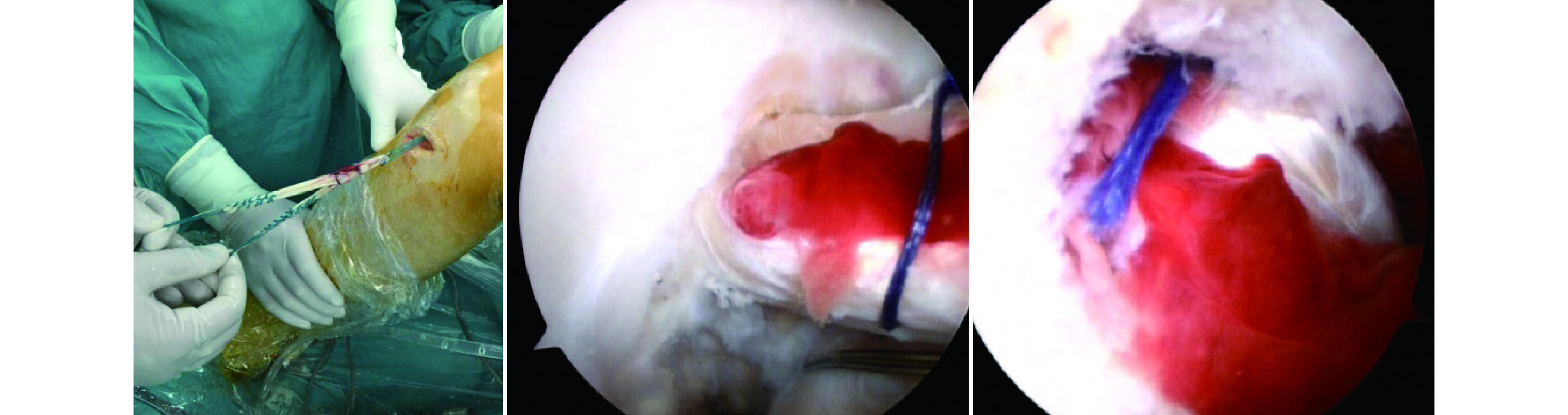
Pulling the hamstring tendon graft into the bone tunnel
术中将腘绳肌腱移植物拉入骨隧道
1.4. 术后处理
两组术后处理方法一致。术后抬高患肢 20~30°,患膝持续冰敷 24 h,24 h 后拔除引流管。术后早期主要进行股四头肌锻炼及关节活动度锻炼,防止肌肉萎缩及关节粘连;中期主要进行患膝关节周围肌肉强化锻炼、恢复部分运动,包括适度行走及慢跑,避免剧烈活动;后期可恢复游泳、慢跑等稍剧烈活动。
1.5. 疗效评价指标
两组患者手术前后行前抽屉试验、Lachman 试验及轴移试验检查,术前及术后 6、24、48 周检查患膝关节活动度、Lysholm 评分、HSS 评分,评定膝关节功能恢复情况。术后 6、24、48 周行 MRI 检查,将移植物分为上、中、下 3 个感兴趣区,测量移植物信号强度、信噪比(移植物与同侧正常韧带的比值)、骨隧道扩大程度及移植物腱-骨结点 T2 值,测量值取均值。
1.6. 统计学方法
采用 SPSS19.0 统计软件进行分析。计量资料以均数±标准差表示,组间比较采用独立样本 t 检验;计数资料组间比较采用 χ2 检验;检验水准 α=0.05。
2. 结果
两组患者术后均获随访 48 周。术后切口均Ⅰ期愈合,无 1 例出现关节内感染及关节粘连等并发症。术后两组患者前抽屉试验、Lachman 试验及轴移试验均为阴性。术后 6、24、48 周,试验组 Lysholm 评分均明显高于对照组,比较差异有统计学意义(P<0.05);但两组间膝关节活动度比较差异无统计学意义(P>0.05)。术后 6 周,两组 HSS 评分比较差异无统计学意义(P>0.05);24、48 周试验组评分明显高于对照组,比较差异有统计学意义(P<0.05)。见表 1~3。MRI 复查示,术后 6 周试验组移植物新生血管活跃,含水量较高,再血管化进程较对照组快,移植物信号高于对照组;24、48 周,试验组移植物信号已向正常韧带低信号转变,移植物信号较对照组低,移植物血管化及韧带化进程较对照组快。见图 3、4。术后 6、24、48 周两组移植物信号强度、骨隧道扩大程度、移植物信噪比比较,差异均有统计学意义(P<0.05)。术后 6、24 周两组移植物腱-骨结点 T2 值比较,差异有统计学意义(P<0.05);48 周比较差异无统计学意义(P>0.05)。见表 4。
图 3.
MRI of a 32-year-old male patient with right ACL injury in the trial group
试验组患者,男,32岁,右膝 ACL 损伤 MRI
a. 术前;b. 术后 6 周;c. 术后 24 周;d. 术后 48 周
a. Before operation; b. At 6 weeks after operation; c. At 24 weeks after operation; d. At 48 weeks after operation

图 4.
MRI of a 23-year-old male patient with right ACL injury in the control group
对照组患者,男,23 岁,右膝 ACL 损伤 MRI
a. 术前;b. 术后 6 周;c. 术后 24 周;d. 术后 48 周
a. Before operation; b. At 6 weeks after operation; c. At 24 weeks after operation; d. At 48 weeks after operation

表 4.
Comparison of MRI measurement indexes between 2 groups after operation (n=17,
 )
)
术后各时间点 MRI 检测指标比较(n=17,
 )
)
| 组别
Group |
移植物信号强度
Graft signal intensity |
骨隧道扩大程度(mm)
Bone tunnel expansion (mm) |
|||||
| 术后 6 周
Postoperative at 6 weeks |
术后 24 周
Postoperative at 24 weeks |
术后 48 周
Postoperative at 48 weeks |
术后 6 周
Postoperative at 6 weeks |
术后 24 周
Postoperative at 24 weeks |
术后 48 周
Postoperative at 48 weeks |
||
| 试验组
Trial group |
6.41±1.18 | 2.59±0.51 | 1.35±0.49 | 0.09±0.02 | 0.75±0.06 | 1.14±0.10 | |
| 对照组
Control group |
3.24±0.44 | 5.71±0.85 | 3.47±0.51 | 0.17±0.15 | 1.58±0.09 | 2.19±0.36 | |
| 统计值
Statistic |
t=10.441
P= 0.000 |
t=–2.999
P= 0.000 |
t=–12.258
P= 0.000 |
t=–2.029
P= 0.047 |
t=–16.790
P= 0.000 |
t=–11.687
P= 0.000 |
|
| 组别
Group |
移植物信噪比
Graft signal to noise ratio |
移植物腱-骨结点 T2 值
Graft tendon-bone node T2 value |
|||||
| 术后 6 周
Postoperative at 6 weeks |
术后 24 周
Postoperative at 24 weeks |
术后 48 周
Postoperative at 48 weeks |
术后 6 周
Postoperative at 6 weeks |
术后 24 周
Postoperative at 24 weeks |
术后 48 周
Postoperative at 48 weeks |
||
| 试验组
Trial group |
4.37±0.26 | 3.50±0.27 | 2.84±0.12 | 235.03±14.08 | 137.29± 7.52 | 45.06±3.25 | |
| 对照组
Control group |
3.13±0.10 | 4.16±0.24 | 3.18±0.12 | 179.78±10.38 | 202.68±14.12 | 45.33±2.85 | |
| 统计值
Statistic |
t=18.198
P= 0.000 |
t=–7.560
P= 0.000 |
t=–8.085
P= 0.000 |
t=13.020
P= 0.000 |
t=–16.854
P= 0.000 |
t=–0.257
P= 0.799 |
|
3. 讨论
ACL 重建术后腱-骨愈合不良是导致手术失败的主要原因之一[3]。正常的 ACL 有较丰富血供,断裂后由于断端游离导致血供中断,因此 ACL 损伤后一般不能自行愈合,但韧带残端仍有良好的血供[4]。腱-骨愈合较缓慢,术后 8 周左右移植物表面才会出现新生血管[5],因此过早恢复功能锻炼会延长移植物与骨隧道间愈合时间,甚至出现不愈合,导致腱-骨结合部位纤维强度下降或者出现骨溶解造成骨隧道扩大等[6]。ACL 重建术后影响腱-骨愈合的因素主要包括:移植物类型及固定方法、重建方法、腱-骨间隙炎性反应的影响、肌腱的机械应力[7]等。
ACL 重建术后如何加快腱-骨界面愈合,成为运动医学领域研究的热点[8]。目前,研究发现促进 ACL 重建术后腱-骨愈合的方法有很多,如给予生长因子[9]、骨膜包裹[10]、磷酸钙[11]、体外冲击波[12]、基因工程[13]、富血小板血浆[14],但这些方法大多需要复杂的实验室技术,临床可操作性不强。本研究选择的自体血纤维蛋白凝块,可以在术中完成制备,无需特殊设备,操作简便。此外,自体血纤维蛋白凝块还具有以下优势,其结构呈柔韧多孔状,可有效网聚血小板因子和白细胞等重要成分,缓慢释放其内含的各种有利于组织修复的因子[15],如 IGF、TGF、VEGF、PDGF 等。这些因子具有促进细胞增殖分化、基质改建及软组织内的血管再生等生理作用,有效调控与组织修复紧密相关的细胞增殖、分化以及凋亡,是促进软硬组织愈合的重要调节因子[16]。并且充分填充移植物与骨道之间的间隙,与骨道接触面积大,起到断端间的桥接作用,利于周围血管长入,改善局部血供,加快移植物的再血管化进程。目前已经广泛应用于骨缺损移植、牙槽骨的骨量恢复[17]、半月板移植[18]等领域。
何蔚等[19]采用自体腘绳肌腱保留残端解剖重建 ACL,术后效果良好。因此,本次研究选择相同术式,A 组同时应用自体血纤维蛋白凝块。经随访比较显示,A 组膝关节功能评分均优于 B 组。另外我们选择了 MRI 观测评估移植物情况。利用 MRI 技术评价 ACL 重建术后移植物状况比较准确[20],经各时间点两组移植物信号强度、信噪比、腱-骨结点 T2 值及骨隧道扩大程度对比分析,提示术后 A 组患者骨隧道溶解情况优于 B 组。综上述,本研究结果表明自体血纤维蛋白凝块能有效促进早期移植物再血管化、加快腱-骨愈合进程,有利于患者早日恢复膝关节稳定性及正常生理功能。我们认为主要有以下原因:① 将自体血纤维蛋白凝块缝在腘绳肌腱移植物股骨端,在肌腱拉入股骨骨道的过程中,血凝块能涂抹至骨道壁上并堵塞骨道口,通过自体血凝块内富含的各种促进组织修复因子及营养成分的作用,加快移植物血管化及腱-骨愈合。② 股骨钻头一般为 6.5、7.0、7.5 mm 等固定尺寸,因此存在制备的骨隧道与移植物肌腱不完全匹配可能,可能导致术后移植物在骨隧道中产生雨刷效应,不仅不利于腱-骨愈合,甚至会加重骨隧道溶解。而应用自体血纤维蛋白凝块可有效封堵骨道口,消除雨刷效应,防止关节积液大量进入骨道阻碍腱-骨愈合。
但本研究随访时间较短,其中远期疗效有待进一步随访观察。此外,能否将自体血纤维蛋白凝块用于后交叉韧带、内外侧副韧带重建以及肩袖修补术,以促进腱-骨愈合,是下一步研究方向。
Funding Statement
河南省基础与前沿技术研究计划项目(162300410093);河南省医学科技攻关项目(201602196)
Fundamental Research and Advanced Technology Program of Henan Province (162300410093); Medical Science and Technology Program of Henan Province (201602196)
References
- 1.陈康, 朱伟民, 陆伟, 等 关节镜下前交叉韧带单束和双束个体化解剖重建临床疗效对比研究. 中华骨与关节外科杂志. 2016;9(6):484–488. [Google Scholar]
- 2.Petersen W, Laprell H Insertion of autologous tendon grafts to the bone: a histological and immunohistochemical study of hamstring and patellar tendon grafts. Knee Surg Sports Traumatol Arthrosc. 2000;8(1):26–31. doi: 10.1007/s001670050006. [DOI] [PubMed] [Google Scholar]
- 3.崔巍, 吕伟, 时剑辉, 等 关节镜下自体骨膜包裹 6 股腘绳肌腱移植前交叉韧带重建的中期疗效评价. 中国现代药应用. 2016;10(17):114–116. [Google Scholar]
- 4.区永亮, 黄华扬, 李凭跃, 等 骨道内移植物更合理分布的单隧道单束前交叉韧带重建的中期疗效观察. 中国骨与关节外科. 2014;7(1):27–30. [Google Scholar]
- 5.程鹏飞, 柴益民 界面螺钉在前十字韧带修复中的应用进展. 中华骨科杂志. 2016;36(12):810–816. [Google Scholar]
- 6.周平, 赵其纯, 尚希福, 等 rhBMP-2 联合 rhVEGF165 对兔前交叉韧带重建后腱-骨愈合的影响. 安徽医科大学学报. 2013;48(5):458–462. [Google Scholar]
- 7.王辉, 王万明 前交叉韧带重建术后腱骨愈合影响因素研究进展. 实用医学杂志. 2014;30(14):2343–2345. [Google Scholar]
- 8.陈平, 曲戎梅, 韩忠宇, 等 人脂肪源干细胞促进前交叉韧带重建后腱骨界面愈合的实验研究. 中国临床解剖学杂志. 2016;34(6):643–646. [Google Scholar]
- 9.Yamazaki S, Yasuda K, Tomita F, et al The effect of transforming growth factor-betal on intraosseous healing of flexor tendon autograft replacement of anterior cruciate ligament in dogs. Arthroscopy. 2005;21(9):1034–1041. doi: 10.1016/j.arthro.2005.05.011. [DOI] [PubMed] [Google Scholar]
- 10.Chen CH, Chen WJ, Shih CH, et al Enveloping the tendon graft with periosteum to enhance tendon-bone healing in a bone tunnel: A biomechanical and histologic study in rabbits. Arthroscopy. 2003;19(3):290–296. doi: 10.1053/jars.2003.50014. [DOI] [PubMed] [Google Scholar]
- 11.Huangfu X, Zhao J Tendon-bone healing enhancement using injectable tricalcium phosphate in a dog anterior cruciate ligament reconstruction model. Arthroscopy. 2007;23(5):455–462. doi: 10.1016/j.arthro.2006.12.031. [DOI] [PubMed] [Google Scholar]
- 12.石斌, 刘玉杰, 李志超, 等 体外冲击波促进兔 ACL 重建后腱骨愈合的实验研究. 中国矫形外科杂志. 2008;16(4):292–295. [Google Scholar]
- 13.Martinek V, Latterman C, Usas A, et al Enhancement of tendon-bone integration of anterior cruciate ligament grafts with bone morphogenetic protein-2 gene transfer: a histological and biomechanical study. J Bone Joint Surg (Am) 2002;84-A(7):1123–1131. doi: 10.2106/00004623-200207000-00005. [DOI] [PubMed] [Google Scholar]
- 14.MishraAK, Skrepnik NV, Edwards SG, et al Efficacy of platelet-rich plasma for chronic tennis elbow: a double-blind, prospective, multicenter, randomized controlled trial of 230 patients. Am J Sports Med. 2014;42(2):463–471. doi: 10.1177/0363546513494359. [DOI] [PubMed] [Google Scholar]
- 15.季锋, 许华 富血小板血浆用于软组织炎症及损伤治疗的研究进展. 中国疼痛医学杂志. 2017;23(2):135–138. [Google Scholar]
- 16.Opera WE, Karp JM, Hosseini MM, et al Effect of platelet releasate on bone cell migration and recruitment in vitro . J Craniofac Surg. 2003;14(3):292–300. doi: 10.1097/00001665-200305000-00006. [DOI] [PubMed] [Google Scholar]
- 17.Hotz G Alevolar ridge augmentation with hydroxylapatite using fibrin sealant for fixation. Part I: An experimental study. Int J Oral Maxillofac Surg. 1991;20(4):204–207. doi: 10.1016/s0901-5027(05)80175-4. [DOI] [PubMed] [Google Scholar]
- 18.van Trommel MF, Simonian PT, Potter HG, et al Arthroscopic meniscal repairwith fibrin clot of complete radial tears of the lateral meniscus in the avascular zone. Arthroscopy. 1998;14(4):360–365. doi: 10.1016/s0749-8063(98)70002-7. [DOI] [PubMed] [Google Scholar]
- 19.何蔚, 刘玉杰 交叉韧带重建术后腱骨愈合相关研究进展. 军医进修学院学报. 2010;31(10):978–980. [Google Scholar]
- 20.Gao F, Zhang ZJ, Tang W, et al A preliminary research of T2 and T2 star relaxtion times mapping for assessment of articular cartilage in the knee. J Clin Radiology. 2013;32(9):1305–1309. [Google Scholar]