

Key Points
Question
What are post hoc treatment outcomes of lifitegrast by severity of dry eye disease (DED)?
Findings
In this post hoc analysis of 2 randomized clinical trials including 1429 patients, treatment with lifitegrast in the subgroup with an inferior corneal staining score of greater than 1.5 and eye dryness score of at least 60 at baseline (ie, moderate to severe DED) showed lifitegrast-treated participants had higher odds of achieving simultaneous improvement in clinical signs and symptoms than placebo-treated participants.
Meaning
The results of this post hoc analysis suggest that lifitegrast treatment may be associated with a response in the signs and symptoms of moderate to severe DED.
This post hoc analysis of 2 randomized clinical trials assesses the heterogeneity in treatment response with lifitegrast in different subsets of participants with dry eye disease, stratified by the severity of the signs and symptoms presented at baseline.
Abstract
Importance
An investigation of the treatment effect of lifitegrast ophthalmic solution, 5.0%, in different subgroups by severity of dry eye disease (DED) seems warranted.
Objective
To explore the heterogeneity across different subgroups of DED and identify which participants were most likely to achieve clinically meaningful benefit with lifitegrast treatment.
Design, Setting, and Participants
This post hoc responder analysis was performed using the data from the phase 3 OPUS-2 and OPUS-3 studies, which were 12-week, prospective, double-masked, multicenter, placebo-controlled, randomized, parallel-arm clinical trials that previously demonstrated the efficacy of lifitegrast in DED. Pooled data were stratified into 4 subgroups based on severity of inferior corneal staining score (ICSS; ≤1.5 vs >1.5) and eye dryness score (EDS; <60 or ≥60) at baseline. Data were collected from December 7, 2012, to October 5, 2015, and post hoc analysis was performed from April 14, 2020, to July 30, 2021.
Interventions
Lifitegrast or placebo twice daily for 84 days.
Main Outcomes and Measures
Proportion of participants with (1) a clinically meaningful improvement in signs (ICSS or total corneal staining score [TCSS]) and symptoms (EDS or global visual analog scale [VAS]) and (2) a composite response for a given sign and symptom end point pair at day 84 were measured. Clinically meaningful improvement was defined as at least 30% improvement in symptoms (EDS or global VAS) and either at least a 1-point improvement in ICSS or at least a 3-point improvement in TCSS. For the composite responder analysis, the end point pairs were defined as at least a 30% reduction in EDS and at least a 1-point improvement in ICSS; at least a 30% reduction in EDS and at least a 3-point improvement in TCSS; at least a 30% improvement in global VAS and at least a 1-point improvement in ICSS; and at least a 30% improvement in global VAS and at least a 3-point improvement in TCSS.
Results
In total, 1429 participants (716 in the placebo group and 713 in the lifitegrast group) were analyzed (1087 women [76.1%]; mean [SD] age, 58.7 [14.3] years). For the overall pooled population, responder and composite responder rates favored lifitegrast vs placebo (odds ratio range, 1.29 [95% CI, 1.05-1.59] to 2.10 [95% CI, 1.68-2.61]; P ≤ .02). In the composite analysis, the subgroup with ICSS of greater than 1.5 and EDS of at least 60 at baseline (ie, moderate to severe DED) demonstrated a 1.70- to 2.11-fold higher odds of achieving clinically meaningful improvement with lifitegrast across all sign and symptom end point pairs (P ≤ .001).
Conclusions and Relevance
These post hoc findings suggest that lifitegrast ophthalmic solution, 5.0%, treatment may be associated with a response in participants with moderate to severe signs and symptoms of DED.
Trial Registration
ClinicalTrials.gov Identifier: NCT02284516
Introduction
Dry eye disease (DED) is a chronic, multifactorial condition affecting the ocular surface that manifests as symptoms of foreign body sensation, grittiness, burning, stinging, ocular fatigue, photophobia, blurred vision, and even pain in the eye in severe cases.1 Dry eye disease has a negative effect on quality of life due to impaired productivity and has a substantial global economic burden in terms of health care costs.2 Ocular surface inflammation triggered by tear film instability and hyperosmolarity plays a key role in the pathogenesis of DED.1,3 Infiltration of proinflammatory cytokines followed by the activation of adaptive T-cell response results in ocular surface damage.1,3,4 Lifitegrast is a small anti-inflammatory molecule that inhibits T-cell–mediated inflammation and immune activation.5,6 Based on a clinical development program consisting of 4 efficacy and safety trials (a phase 2 trial7 and phase 3 trials OPUS-1,8 OPUS-2,9 and OPUS-310), lifitegrast ophthalmic solution, 5.0%, administered twice daily was approved in the US in 2016 for the treatment of both signs and symptoms of DED.11
OPUS-29 and OPUS-310 were pivotal randomized phase 3 studies that evaluated the efficacy and safety of lifitegrast in patients with DED. In both studies, lifitegrast-treated patients achieved a significant reduction in eye dryness score (EDS). Further, in the phase 2,7 OPUS-1,8 and OPUS-310 studies, lifitegrast-treated patients also showed a greater improvement in signs (inferior corneal staining score [ICSS]) of DED than the placebo group, although this end point was not met in OPUS-2.9
The poor correlation often observed between the signs and symptoms of DED makes it challenging to diagnose as well as to monitor treatment response and disease progression.12 Dichotomous responder analysis is a useful approach to quantify and compare the treatment effect between 2 groups based on a defined threshold for the change from baseline.13,14 This type of analysis can help identify patients who can achieve a clinically meaningful benefit from treatment.
The OPUS-2 and OPUS-3 trials enrolled a participant population with a range of DED severity. Accordingly, randomization was stratified by severity of signs and symptoms at baseline in these trials (ICSS ≤1.5 or >1.5 and EDS <60 or ≥60).9,10 We conducted a post hoc responder analysis of the pooled participant data from the OPUS-2 and OPUS-3 trials to understand the heterogeneity in treatment response with lifitegrast in different subsets of participants with DED, stratified by the severity of the signs (ICSS) and symptoms (EDS) presented at baseline.
Methods
Study Design
This post hoc analysis pooled data from the OPUS-2 and OPUS-3 trials, which were two 12-week, prospective, phase 3, randomized, multicenter, double-masked, placebo-controlled, parallel-arm clinical trials. OPUS-2 was conducted from December 7, 2012, to October 1, 2013, across 31 US study centers; OPUS-3, from November 6, 2014, to October 5, 2015, across 41 US study centers. Details of these trials were published previously.9,10 The trial protocols are available in Supplements 1 to 4. These trials adhered to the Health Insurance Portability and Accountability Act and the tenets of the Declaration of Helsinki.15 Study protocols were approved by the following institutional review boards (IRBs) before study initiation: OPUS-2, Alpha IRB (San Clemente, California); OPUS-3, Alpha IRB, Sterling IRB (Atlanta, Georgia), University of Houston IRB (Houston, Texas), Western Institution Review Board (Puyallup, Washington). All participants provided written informed consent to participate in the trials.9,10
The study participants were adults (≥18 years of age) who had an EDS of at least 40 (on a visual analog scale [VAS]; range, 0-100 points, with higher scores indicating increasing discomfort/symptoms), an ICSS of at least 0.5 (0- to 4-point scale with 0.5-point increments, with higher scores indicating increasing intensity of staining), regional (inferior, superior, and central) corneal staining score of at least 2 (0- to 4-point scale with 0.5-point increments, with higher scores indicating increasing intensity of staining), conjunctival redness score of at least 1 (0- to 4-point scale with 0.5-point increments, with higher scores indicating more redness), and Schirmer tear test (5 minutes, without anesthesia) ranging from 1 to 10 mm. The Schirmer tear test was performed using the following procedure: the proximal end of a sterile Schirmer test strip was bent at the notch. As the participant gazed up and in, the test strip was placed in the lower temporal lid margin of each eye. Participants were instructed to close their eyes for 5 minutes, after which time the Schirmer test strip was removed. The length of the moistened area was recorded in millimeters for each eye. The eye with worse inferior corneal staining (highest score) was assigned as the study eye.9,10
The EDS was measured with a VAS, which is an established symptom measure in DED.16,17 Corneal fluorescein staining was performed with 2% unpreserved sodium fluorescein solution. Grading of corneal fluorescein staining was based on the Expanded National Eye Institute/Industry Workshop Corneal Fluorescein Staining Scale and methods modified from Lemp (1995)18 and Shimmura et al (1995).19 A conjunctival redness scale was modified from Efron et al (2001).20
Patients were randomized 1:1 and received either the lifitegrast ophthalmic solution, 5.0%, or placebo twice daily for a period of 12 weeks.9,10 Randomization was stratified by ICSS (≤1.5 or >1.5) and EDS (<60 or ≥60) at baseline. Participants did not receive compensation or incentives to participate in the OPUS-2 and OPUS-3 clinical trials.9,10 Data analyzed for this post hoc subgroup analysis were generated from the original study populations.
Efficacy Outcome Measures
Data were pooled based on homogeneity in study design, eligibility criteria, treatment dosing, and end points. Randomization in the OPUS-2 and OPUS-3 trials was stratified by 4 subgroups based on their baseline severity of ICSS and EDS pairs (these were the randomization stratification factors in parent trials): (1) ICSS of 1.5 or less and EDS of less than 60; (2) ICSS of 1.5 or less and EDS of at least 60; (3) ICSS of greater than 1.5 and EDS of at least 60; and (4) ICSS of greater than 1.5 and EDS of less than 60. This post hoc analysis evaluated the association of treatment with lifitegrast in these subgroups based on the proportion of participants with a clinically meaningful improvement (response) in (1) signs (ICSS and total corneal staining score [TCSS]), (2) symptoms (EDS and global VAS), and (3) both signs and symptoms (composite responder analysis) of DED at day 84.
Responder Analysis
An improvement in staining of 1 point in the inferior region of the cornea represents a clinically meaningful response in ICSS (0- to 4-point scale), and an improvement of 3 points in the TCSS (0- to 12-point scale) represents a clinically meaningful improvement and reflects the healing of the corneal surface. A 30% reduction in symptoms is a relevant benchmark for DED studies and regulatory agencies and indicates a clinically meaningful improvement in patient-reported outcomes.21,22,23,24
Composite Responder Analysis
A composite responder analysis was performed by considering simultaneous sign and symptom outcomes. Composite response in the following 4 combinations was assessed: (1) at least a 30% reduction in EDS and at least a 1-point improvement in ICSS; (2) at least a 30% reduction in EDS and at least a 3-point improvement in TCSS; (3) at least a 30% improvement in global VAS and at least a 1-point improvement in ICSS; and (4) at least a 30% improvement in global VAS and at least a 3-point improvement in TCSS.
Statistical Analysis
Data for the present pooled analysis were analyzed from April 14, 2020, to July 30, 2021. All analyses were based on the intention-to-treat population (all participants who had received ≥1 dose of investigational product). Analyses were based on the treatment assigned through randomization. The efficacy analyses were performed using the last observation carried forward. Multivariate logistic regression models were used to calculate odds ratios (ORs) and 95% CIs for the overall pooled population of OPUS-2 and OPUS-3 and by randomization factors. The P values representing the interaction term between strata and treatment are provided. All P values reported are nominal and were not adjusted for multiplicity. Cumulative responder functions with ORs and 95% CIs are also provided.
Results
Baseline Demographics and Ocular Characteristics
A total of 1429 participants from OPUS-2 (360 in the placebo group and 358 in the lifitegrast group) and OPUS-3 (356 in the placebo group and 355 in the lifitegrast group) were included in this post hoc analysis consisting of 716 and 713 participants in the placebo and lifitegrast groups, respectively (Figure). Baseline characteristics were balanced between the placebo and lifitegrast groups. The mean (SD) age was 58.7 (14.3) years; 1087 participants were female (76.1%) and 342 were male (23.9%). Other baseline characteristics are presented in Table 1. The ICSS, TCSS, EDS, and global VAS values at baseline were similar between the placebo and lifitegrast groups (Table 1). At baseline, 803 participants (56.2%) had moderate to severe DED (ICSS >1.5 and EDS ≥60), whereas 85 participants (6.0%) had mild DED (ICSS ≤1.5 and EDS <60) (Table 1).
Figure. Participants From the OPUS-2 and OPUS-3 Studies Included in the Post Hoc Analysis, by Treatment Group.
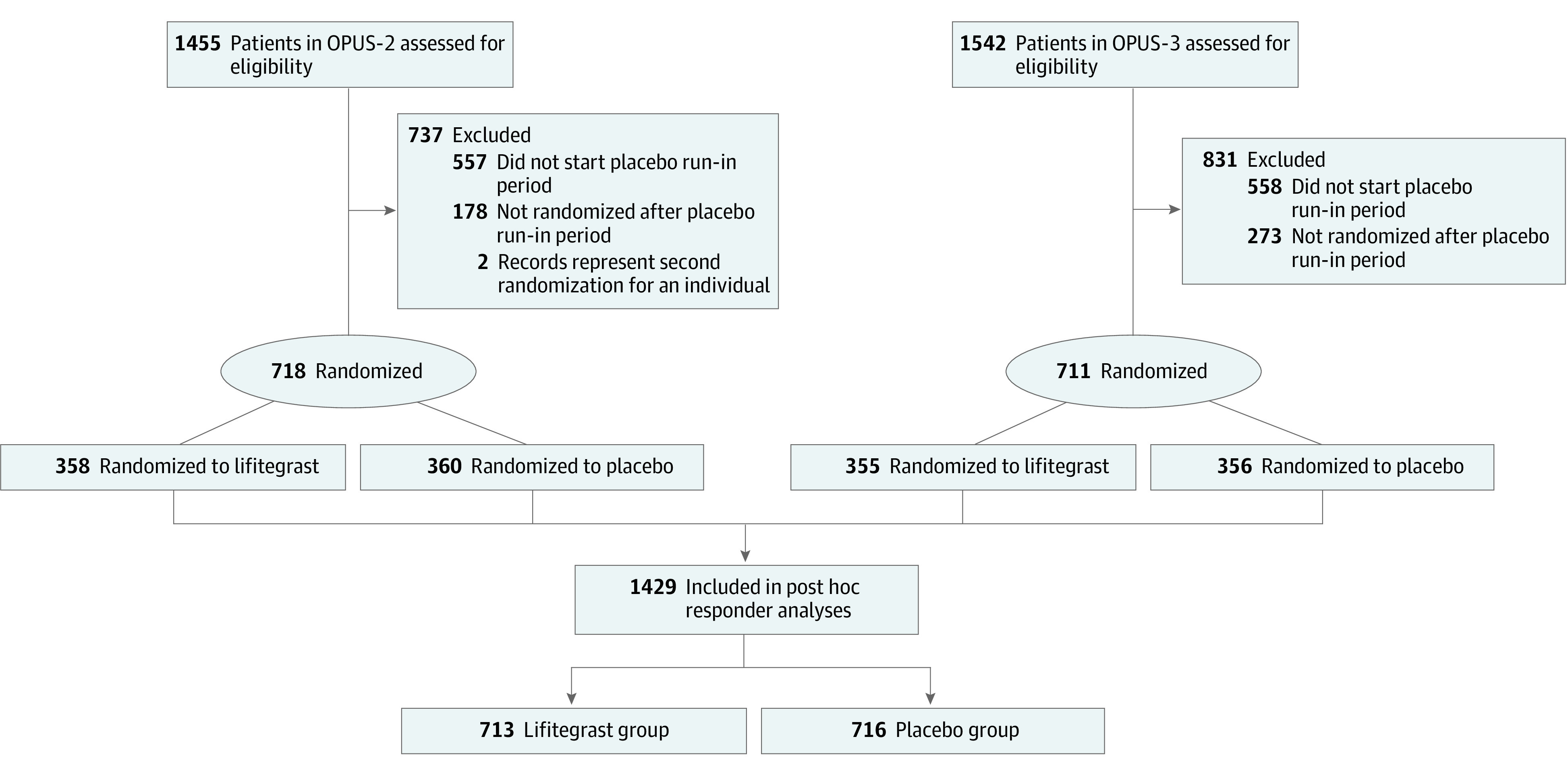
Table 1. Demographics and Baseline Ocular Characteristics (Pooled Data) of the ITT Population.
| Characteristic | Participant groupa | ||
|---|---|---|---|
| Placebo (n = 716) | Lifitegrast (n = 713) | All (N = 1429) | |
| Age, mean (SD), y | 58.7 (14.5) | 58.8 (14.0) | 58.7 (14.3) |
| Age group, y | |||
| >65 | 261 (36.5) | 242 (33.9) | 503 (35.2) |
| >75 | 78 (10.9) | 76 (10.7) | 154 (10.8) |
| Sex | |||
| Female | 534 (74.6) | 553 (77.6) | 1087 (76.1) |
| Male | 182 (25.4) | 160 (22.4) | 342 (23.9) |
| Ethnicity | |||
| Hispanic or Latino | 122 (17.0) | 139 (19.5) | 261 (18.3) |
| Other | 594 (83.0) | 574 (80.5) | 1168 (81.7) |
| Race | |||
| White | 584 (81.6) | 568 (79.7) | 1152 (80.6) |
| Otherb | 132 (18.4) | 145 (20.3) | 277 (19.4) |
| ICSS in study eye, mean (SD) [range]c | 2.43 (0.7) [0.5-4.0] | 2.43 (0.7) [0.5-4.0] | 2.43 (0.7) [0.5-4.0] |
| TCSS in study eye, mean (SD) [range]d | 5.32 (2.0) [0.5-11.5] | 5.20 (2.0) [1.0-12.0] | 5.26 (2.0) [0.5-12.0] |
| EDS, mean (SD) [range]e | 69.1 (16.9) [40-100] | 69.0 (16.9) [40-100] | 69.0 (16.9) [40-100] |
| Global VAS score, mean (SD) [range]e | 50.0 (19.7) [7-98] | 48.0 (20.1) [6-97] | 49.0 (19.9) [6-98] |
| Randomization strata | |||
| ICSS≤1.5 and EDS<60 | 43 (6.0) | 42 (5.9) | 85 (6.0) |
| ICSS≤1.5 and EDS≥60 | 62 (8.7) | 63 (8.8) | 125 (8.8) |
| ICSS>1.5 and EDS<60 | 207 (28.9) | 209 (29.3) | 416 (29.1) |
| ICSS>1.5 and EDS≥60 | 404 (56.4) | 399 (56.0) | 803 (56.2) |
Abbreviations: EDS, eye dryness score; ICSS, inferior corneal staining score; ITT, intention-to-treat; TCSS, total corneal staining score; VAS, visual analog scale.
Unless otherwise indicated, data are expressed as number (%) of participants in the ITT population.
Includes American Indian or Alaska Native; Asian; Black or African American; Native Hawaiian or Other Pacific Islander; and others.
Possible scores range from 0 (no staining) to 4 (severe) with 0.5-point increments.
Total score is derived from the sum of all regions (inferior, central, superior) (0-12 points).
Possible scores range from 0 (no discomfort) to 100 (maximum discomfort).
Responder Analysis
Overall, a higher proportion of participants in the lifitegrast group demonstrated a clinically meaningful improvement in the EDS (508 [71.2%] vs 388 [54.2%]), global VAS (482 [67.6%] vs 396 [55.3%]), ICSS (356 [49.9%] vs 313 [43.7%]), and TCSS (212 [29.7%] vs 172 [24.0%]) at day 84 compared with the placebo group (nominal P ≤ .02) (Table 2). eFigures 1 and 2 in Supplement 5 show the cumulative responder function of the percentage of change in EDS and global VAS, respectively, and the percentage of participants experiencing that change in each treatment group. Across a variety of responder definitions that can be identified along the cumulative distribution of the responder curve, regardless of the chosen threshold, a larger proportion of participants had a response in the lifitegrast- vs placebo-treated arms.
Table 2. Summary of Responders With Improvement in Signs (ICSS and TCSS) and Symptoms (EDS and Global VAS) at Day 84, Overall and Stratified by Baseline Severity (Pooled Data)a.
| ICSS and EDS category at randomization | Response category | Participant group, No./total No. (%) | OR (95% CI) | Nominal P value | ||
|---|---|---|---|---|---|---|
| Placebo (n = 716) | Lifitegrast (n = 713) | For OR | For interaction | |||
| Overall | ≥30% Improvement in EDS | 388/716 (54.2) | 508/713 (71.2) | 2.10 (1.68-2.61) | <.001 | .11 |
| ≥1-Point improvement in ICSS | 313/716 (43.7) | 356/713 (49.9) | 1.29 (1.05-1.59) | .02 | .99 | |
| ≥3-Point improvement in TCSS | 172/716 (24.0) | 212/713 (29.7) | 1.40 (1.10-1.78) | .01 | .66 | |
| ≥30% Improvement in global VAS | 396/716 (55.3) | 482/713 (67.6) | 1.67 (1.34-2.07) | <.001 | <.001 | |
| ICSS≤1.5 and EDS<60 | ≥30% Improvement in EDS | 27/43 (62.8) | 30/42 (71.4) | 1.55 (0.62-3.90) | .35 | NA |
| ≥1-Point improvement in ICSS | 9/43 (20.9) | 11/42 (26.2) | 1.40 (0.49-3.97) | .53 | NA | |
| ≥3-Point improvement in TCSS | 8/43 (18.6) | 7/42 (16.7) | 0.81 (0.26-2.54) | .72 | NA | |
| ≥30% Improvement in global VAS | 27/43 (62.8) | 25/42 (59.5) | 0.90 (0.37-2.20) | .81 | NA | |
| ICSS≤1.5 and EDS≥60 | ≥30% Improvement in EDS | 31/62 (50.0) | 47/63 (74.6) | 2.93 (1.38-6.25) | .01 | NA |
| ≥1-Point improvement in ICSS | 12/62 (19.4) | 17/63 (27.0) | 1.22 (0.49-3.04) | .67 | NA | |
| ≥3-Point improvement in TCSS | 8/62 (12.9) | 14/63 (22.2) | 1.83 (0.69-4.85) | .22 | NA | |
| ≥30% Improvement in global VAS | 26/62 (41.9) | 49/63 (77.8) | 4.78 (2.19-10.45) | <.001 | NA | |
| ICSS>1.5 and EDS<60 | ≥30% Improvement in EDS | 129/207 (62.3) | 147/209 (70.3) | 1.44 (0.96-2.17) | .08 | NA |
| ≥1-Point improvement in ICSS | 92/207 (44.4) | 107/209 (51.2) | 1.31 (0.89-1.93) | .17 | NA | |
| ≥3-Point improvement in TCSS | 51/207 (24.6) | 59/209 (28.2) | 1.25 (0.80-1.95) | .33 | NA | |
| ≥30% Improvement in global VAS | 134/207 (64.7) | 133/209 (63.6) | 0.96 (0.64-1.43) | .83 | NA | |
| ICSS>1.5 and EDS≥60 | ≥30% Improvement in EDS | 201/404 (49.8) | 284/399 (71.2) | 2.50 (1.87-3.34) | <.001 | NA |
| ≥1-Point improvement in ICSS | 200/404 (49.5) | 221/399 (55.4) | 1.26 (0.96-1.67) | .10 | NA | |
| ≥3-Point improvement in TCSS | 105/404 (26.0) | 132/399 (33.1) | 1.49 (1.09-2.04) | .01 | NA | |
| ≥30% Improvement in global VAS | 209/404 (51.7) | 275/399 (68.9) | 2.04 (1.53-2.73) | <.001 | NA | |
Abbreviations: EDS, eye dryness score; ICSS, inferior corneal staining score; NA, not applicable; OR, odds ratio; TCSS, total corneal staining score; VAS, visual analog scale.
For both groups, includes intention-to-treat population with last observation carried forward. Scores are described in Table 1.
Responder Analysis by Baseline Severity
As previously mentioned, most participants (803 [56.2%]) had moderate to severe DED (ICSS>1.5 and EDS≥60). Participants with moderate to severe symptoms (EDS≥60) and discordant signs (ICSS≤1.5) who were treated with lifitegrast had greater odds of improvement in symptoms as measured by the EDS (OR, 2.93; 95% CI, 1.38-6.25) and the global VAS (OR, 4.78; 95% CI, 2.19-10.45) than participants treated with placebo, but the same was not true for improvement in signs. Participants with greater signs (ICSS>1.5) but discordant symptoms (EDS<60) had slightly greater odds of improvement in signs (OR for ICSS, 1.31 [95% CI, 0.89-1.93]; OR for TCSS, 1.25 [95% CI, 0.80-1.95]), but this finding did not reach the level of nominal significance.
In the subgroup of participants with moderate to severe DED (ICSS>1.5 and EDS≥60), the odds of achieving a clinically relevant improvement in EDS (OR, 2.50; 95% CI, 1.87-3.34), global VAS (OR, 2.04; 95% CI, 1.53-2.73), and TCSS (OR, 1.49; 95% CI, 1.09-2.04) were higher among lifitegrast-treated participants vs placebo-treated participants. The only statistically significant interaction term between strata and treatment group was for the global VAS (P < .001), indicating that the treatment effect varied significantly across disease severity strata.
Composite Responder Analysis
In the pooled study cohort across all end point pairs of an assessed sign and symptom outcome, a higher proportion of participants in the lifitegrast group had a clinically meaningful improvement at day 84 than in the placebo group (OR range, 1.29 [95% CI, 1.05-1.59] to 2.10 [95% CI, 1.68-2.61]; P ≤ .02) (Table 2). The highest improvement was seen in participants with an ICSS of greater than 1.5 and EDS of at least 60 at baseline, with a higher response in favor of lifitegrast than placebo for all end point pairs (OR range, 1.70 [95% CI, 1.26-2.29] to 2.11 [95% CI, 1.46-3.06]; P ≤ .001) (Table 3). Similarly, higher odds of achieving a composite improvement in both signs and symptoms of DED with lifitegrast as compared with placebo were demonstrated in participants with an ICSS of 1.5 or less and an EDS of at least 60 at baseline (OR range, 1.78 [95% CI, 0.62-5.10] to 2.06 [95% CI, 0.70-6.06]) and those with an ICSS of greater than 1.5 and an EDS of less than 60 at baseline (OR range, 1.13 [95% CI, 0.75-1.70] to 1.38 [95% CI, 0.83-2.29]), although the difference between the treatment groups was not meaningful (P > .05) (Table 3). There were no statistically significant interactions between strata and treatment group.
Table 3. Summary of Composite Responders With Improvement in Sign and Symptom End Point Pairs From Baseline to Day 84, Overall and Stratified by Baseline Severity (Pooled Data)a.
| ICSS and EDS category at randomization | Response category | Participant group, No./total No. (%) | OR (95% CI) | Nominal P value | ||
|---|---|---|---|---|---|---|
| Placebo (n = 716) | Lifitegrast (n = 713) | For OR | For interaction | |||
| Overall | ≥30% Improvement in EDS and ≥1-point improvement in ICSS | 189/716 (26.4) | 262/713 (36.7) | 1.62 (1.30-2.03) | <.001 | .22 |
| ≥30% Improvement in EDS and ≥3-point improvement in TCSS | 100/716 (14.0) | 156/713 (21.9) | 1.78 (1.34-2.35) | <.001 | .23 | |
| ≥30% Improvement in global VAS and ≥1-point improvement in ICSS | 193/716 (27.0) | 253/713 (35.5) | 1.48 (1.18-1.86) | <.001 | .20 | |
| ≥30% Improvement in global VAS and ≥3-point improvement in TCSS | 108/716 (15.1) | 150/713 (21.0) | 1.54 (1.17-2.02) | .002 | .22 | |
| ICSS≤1.5 and EDS<60 | ≥30% Improvement in EDS and ≥1-point improvement in ICSS | 8/43 (18.6) | 6/42 (14.3) | 0.60 (0.17-2.09) | .42 | NA |
| ≥30% Improvement in EDS and ≥3-point improvement in TCSS | 6/43 (14.0) | 4/42 (9.5) | 0.54 (0.13-2.21) | .39 | NA | |
| ≥30% Improvement in global VAS and ≥1-point improvement in ICSS | 8/43 (18.6) | 7/42 (16.7) | 0.96 (0.29-3.16) | .95 | NA | |
| ≥30% Improvement in global VAS and ≥3-point improvement in TCSS | 6/43 (14.0) | 4/42 (9.5) | 0.57 (0.14-2.34) | .43 | NA | |
| ICSS≤1.5 and EDS≥60 | ≥30% Improvement in EDS and ≥1-point improvement in ICSS | 7/62 (11.3) | 14/63 (22.2) | 1.78 (0.62-5.10) | .29 | NA |
| ≥30% Improvement in EDS and ≥3-point improvement in TCSS | 6/62 (9.7) | 12/63 (19.0) | 2.04 (0.69-6.02) | .20 | NA | |
| ≥30% Improvement in global VAS and ≥1-point improvement in ICSS | 7/62 (11.3) | 15/63 (23.8) | 1.99 (0.71-5.62) | .19 | NA | |
| ≥30% Improvement in global VAS and ≥3-point improvement in TCSS | 6/62 (9.7) | 12/63 (19.0) | 2.06 (0.70-6.06) | .19 | NA | |
| ICSS>1.5 and EDS<60 | ≥30% Improvement in EDS and ≥1-point improvement in ICSS | 63/207 (30.4) | 76/209 (36.4) | 1.31 (0.87-1.97) | .20 | NA |
| ≥30% Improvement in EDS and ≥3-point improvement in TCSS | 33/207 (15.9) | 43/209 (20.6) | 1.38 (0.83-2.29) | .21 | NA | |
| ≥30% Improvement in global VAS and ≥1-point improvement in ICSS | 66/207 (31.9) | 72/209 (34.4) | 1.13 (0.75-1.70) | .57 | NA | |
| ≥30% Improvement in global VAS and ≥3-point improvement in TCSS | 37/207 (17.9) | 41/209 (19.6) | 1.15 (0.70-1.89) | .59 | NA | |
| ICSS>1.5 and EDS≥60 | ≥30% Improvement in EDS and ≥1-point improvement in ICSS | 111/404 (27.5) | 166/399 (41.6) | 1.87 (1.39-2.51) | <.001 | NA |
| ≥30% Improvement in EDS and ≥3-point improvement in TCSS | 55/404 (13.6) | 97/399 (24.3) | 2.11 (1.46-3.06) | <.001 | NA | |
| ≥30% Improvement in global VAS and ≥1-point improvement in ICSS | 112/404 (27.7) | 159/399 (39.8) | 1.70 (1.26-2.29) | <.001 | NA | |
| ≥30% Improvement in global VAS and ≥3-point improvement in TCSS | 59/404 (14.6) | 93/399 (23.3) | 1.82 (1.26-2.62) | .001 | NA | |
Abbreviations: EDS, eye dryness score; ICSS, inferior corneal staining score; NA, not applicable; OR, odds ratio; TCSS, total corneal staining score; VAS, visual analog scale.
For both groups, includes intention-to-treat population with last observation carried forward. Scores are described in Table 1.
Discussion
The ODISSEY European consensus group has previously proposed the use of a simple 2-step criteria: inclusion of 1 objective clinical sign and 1 subjective symptom score for assessment of DED severity.25 Using a similar approach in this post hoc analysis, participants with DED were stratified according to baseline severity of ICSS and EDS, and the efficacy of lifitegrast was assessed in these subgroups. The results of this study demonstrate that the association of treatment with lifitegrast with response is consistent in the DED subgroup with an ICSS of greater than 1.5 and an EDS of at least 60. In general, this subgroup represents participants who are clinically categorized as having moderate to severe DED with evidence of ocular surface damage and increasing discomfort. Across all 4 composite responder definitions (sign and symptom end point pairs), the treatment difference favored lifitegrast, with participants having 1.70- to 2.11-fold higher odds of achieving clinically meaningful improvement after 12 weeks of treatment compared with those in the placebo group. In a previously published survey, moderate to severe DED was associated with a substantial decline in productivity and daily activities compared with mild forms of DED.26 Another US-based survey observed that the equivalent lost workdays because of affected performance was 94.9 and 128.2 per year in individuals with moderate and severe DED, respectively.27
It is well established that DED is a heterogeneous disease involving different parts of the ocular surface unit.1 As a result, considerable variability exists depending on the underlying cause, stage of the disease, degree of tear film instability, inflammation, and neurosensory abnormalities. Thus, individual responses to treatment can vary in that some participants may achieve greater improvement in symptoms than in signs, or vice versa, underscoring the unmet need in DED management. In both OPUS-2 and OPUS-3, participants were required to have a baseline ICSS of at least 0.5.9,10 Thus, for participants with an ICSS of 0.5 at baseline, it is numerically impossible to demonstrate an improvement of 1 point. This phenomenon further contributes to the potential floor effect, observed in subgroups with an ICSS of 1.5 or less. The number of participants in the mildest DED category (ICSS≤1.5 and EDS<60) was quite small (85 [6.0%] of the total study cohort), which makes drawing conclusions from this subgroup difficult. Further studies in a larger group of patients with mild disease would allow a better understanding of the effectiveness of lifitegrast in this cohort.
It is important to emphasize that without timely and adequate treatment, DED can progress to a chronic condition characterized by a “vicious self-perpetuating circle” of inflammation.1(p279) Therefore, including anti-inflammatory treatments in the early stages of DED may be beneficial to break the inflammatory circle and prevent corneal epithelial damage and progressive worsening of symptoms. The Tear Film and Ocular Surface Society (TFOS) Dry Eye Workshop (DEWS) II committee recommends an evidence-based treatment approach for the management of DED, taking into account disease etiology and severity.28 However, no single sign or symptom can be correlated specifically with DED severity owing to the heterogeneity in clinical presentation of the condition, making the day-to-day management of DED challenging.12,29 Therefore, therapy for DED needs to be customized and tailored according to individual needs.
For this analysis, ICSS and EDS were used as objective and subjective measures, respectively, to define the degree of severity. Corneal fluorescein staining is routinely used in clinical practice for DED diagnosis and management.29 The EDS measures a common symptom in participants with DED. Although the EDS can show variability across the population with DED, eye dryness is one of the most frequent complaints in patients with DED.17,30 An EDS of at least 60 indicates a high degree of discomfort.31 Increasing EDS severity was found to be associated with worse scores on other questionnaires such as the Ocular Comfort Index, Dry Eye Questionnaire-5, Symptom Assessment in Dry Eye, Rasch-scored 28-item Visual Function Questionnaire, and Work Productivity and Activity Impairment.31
The composite responder rates in the overall study cohort support the efficacy of lifitegrast in the treatment of DED, as reported in clinical trials.7,8,9,10 Use of lifitegrast may offer some advantages over other anti-inflammatory therapies, such as topical cyclosporine A that is indicated for the chronic treatment of moderate to severe signs of DED. The improvement in signs and symptoms with lifitegrast is observed as early as day 14 and the treatment is generally well tolerated, with an acceptable long-term safety profile.8,9,10,32,33 In contrast, topical cyclosporine A has a delayed onset, and reports suggest that 16% to 29% of patients may experience pain/irritation/burning in the eye on instillation.34,35,36,37 Although corticosteroids provide immediate improvement of inflammation, they are indicated for short-term (<2 weeks) use only and, when used for longer periods, can be associated with safety concerns.35 Considering that DED often requires prolonged therapy, several factors thus need to be evaluated in the selection of the anti-inflammatory agent for the management of the condition.
Artificial tears are the first-line treatment for DED and are designed to provide temporary symptomatic relief without addressing the underlying cause of inflammation.13,16 However, artificial tear use is usually continued in all stages of DED in conjunction with other treatments.38 Although artificial tear use was required to be discontinued before enrollment in the OPUS-2 and OPUS-3 studies,9,10 Atallah et al39 reported a significant improvement in the signs and symptoms of chronic DED with lifitegrast in a 6-month retrospective study, even in patients with concurrent use of artificial tears. In that study, most patients continued concomitant use of other DED treatments (79% used artificial tears) while receiving lifitegrast.39 In the 1-year SONATA (Safety of a 5.0% Concentration of Lifitegrast Ophthalmic Solution) safety study, participants reported a decrease in the frequency of concomitant use of artificial tears during the 1-year period following treatment with lifitegrast.33 Taken together, these findings support the effectiveness of lifitegrast therapy in DED even in combination with topical artificial tears.
Strengths and Limitations
This pooled post hoc analysis has both strengths and limitations. The post hoc analysis included data from 1429 participants with DED from masked clinical trials, which adds credence to the findings. A 30% or greater reduction threshold in symptoms defined as a clinically meaningful response is in line with that used by other dry eye studies and regulatory agencies.21,22,23,24 Limitations of this study include the post hoc nature of the analyses and the lack of efficacy data beyond 3 months. It is important to note that all P values reported were not adjusted for multiplicity. Further, considering the complexity of DED, evaluating the role of other baseline factors such as type of DED (aqueous and evaporative), tear film breakup time, and tear osmolarity would be beneficial for clinical practice and should be considered in future trials.
Conclusions
The results of this post hoc analysis potentially add to the overall evidence of the benefit of lifitegrast in the treatment of signs and symptoms of DED, particularly in moderate to severe DED. More data from the clinical practice setting would be useful in understanding the long-term benefit of lifitegrast and its effectiveness in subgroups with varying degrees of DED severity that will help maximize treatment benefit for individual patients.
OPUS-2 SAP
OPUS-3 SAP
OPUS-2 Protocol
OPUS-3 Protocol
eFigure 1. Percentage of Participants With DED and Improvement in Symptoms (EDS) From Baseline to Day 84, by Treatment Group (Pooled Data)
eFigure 2. Percentage of Participants With DED and Improvement in Symptoms (Global VAS) From Baseline to Day 84, by Treatment Group (Pooled Data)
Data Sharing Statement
References
- 1.Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276-283. doi: 10.1016/j.jtos.2017.05.008 [DOI] [PubMed] [Google Scholar]
- 2.Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II epidemiology report. Ocul Surf. 2017;15(3):334-365. doi: 10.1016/j.jtos.2017.05.003 [DOI] [PubMed] [Google Scholar]
- 3.Bron AJ, de Paiva CS, Chauhan SK, et al. TFOS DEWS II pathophysiology report. Ocul Surf. 2017;15(3):438-510. doi: 10.1016/j.jtos.2017.05.011 [DOI] [PubMed] [Google Scholar]
- 4.Ganesalingam K, Ismail S, Sherwin T, Craig JP. Molecular evidence for the role of inflammation in dry eye disease. Clin Exp Optom. 2019;102(5):446-454. doi: 10.1111/cxo.12849 [DOI] [PubMed] [Google Scholar]
- 5.Abidi A, Shukla P, Ahmad A. Lifitegrast: a novel drug for treatment of dry eye disease. J Pharmacol Pharmacother. 2016;7(4):194-198. doi: 10.4103/0976-500X.195920 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Keating GM. Lifitegrast ophthalmic solution 5%: a review in dry eye disease. Drugs. 2017;77(2):201-208. doi: 10.1007/s40265-016-0681-1 [DOI] [PubMed] [Google Scholar]
- 7.Semba CP, Torkildsen GL, Lonsdale JD, et al. A phase 2 randomized, double-masked, placebo-controlled study of a novel integrin antagonist (SAR 1118) for the treatment of dry eye. Am J Ophthalmol. 2012;153(6):1050-60.e1. doi: 10.1016/j.ajo.2011.11.003 [DOI] [PubMed] [Google Scholar]
- 8.Sheppard JD, Torkildsen GL, Lonsdale JD, et al. ; OPUS-1 Study Group . Lifitegrast ophthalmic solution 5.0% for treatment of dry eye disease: results of the OPUS-1 phase 3 study. Ophthalmology. 2014;121(2):475-483. doi: 10.1016/j.ophtha.2013.09.015 [DOI] [PubMed] [Google Scholar]
- 9.Tauber J, Karpecki P, Latkany R, et al. ; OPUS-2 Investigators . Lifitegrast ophthalmic solution 5.0% versus placebo for treatment of dry eye disease: results of the randomized phase III OPUS-2 study. Ophthalmology. 2015;122(12):2423-2431. doi: 10.1016/j.ophtha.2015.08.001 [DOI] [PubMed] [Google Scholar]
- 10.Holland EJ, Luchs J, Karpecki PM, et al. Lifitegrast for the treatment of dry eye disease: results of a phase III, randomized, double-masked, placebo-controlled trial (OPUS-3). Ophthalmology. 2017;124(1):53-60. doi: 10.1016/j.ophtha.2016.09.025 [DOI] [PubMed] [Google Scholar]
- 11.Shire US. Inc. Xiidra (lifitegrast ophthalmic solution) 5%. Package insert. Shire US Inc; 2017. Accessed October 12, 2020. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/208073s002lbl.pdf
- 12.Bartlett JD, Keith MS, Sudharshan L, Snedecor SJ. Associations between signs and symptoms of dry eye disease: a systematic review. Clin Ophthalmol. 2015;9:1719-1730. doi: 10.2147/OPTH.S89700 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lin Y. Robust inference for responder analysis: innovative clinical trial design using a minimum P value approach. Contemp Clin Trials Commun. 2016;3:65-69. doi: 10.1016/j.conctc.2016.04.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Snapinn SM, Jiang Q. Responder analyses and the assessment of a clinically relevant treatment effect. Trials. 2007;8:31. doi: 10.1186/1745-6215-8-31 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.World Medical Association . World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-2194. doi: 10.1001/jama.2013.281053 [DOI] [PubMed] [Google Scholar]
- 16.Taylor M, Ousler G, Torkildsen G, et al. A phase 2 randomized, double-masked, placebo-controlled study of novel nonsystemic kinase inhibitor TOP1630 for the treatment of dry eye disease. Clin Ophthalmol. 2019;13:261-275. doi: 10.2147/OPTH.S189039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.McDonnell PJ, Pflugfelder SC, Stern ME, et al. Study design and baseline findings from the Progression of Ocular Findings (PROOF) natural history study of dry eye. BMC Ophthalmol. 2017;17(1):265. doi: 10.1186/s12886-017-0646-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lemp MA. Report of the National Eye Institute/Industry Workshop on Clinical Trials in Dry Eyes. CLAO J. 1995;21(4):221-232. [PubMed] [Google Scholar]
- 19.Shimmura S, Ono M, Shinozaki K, et al. Sodium hyaluronate eyedrops in the treatment of dry eyes. Br J Ophthalmol. 1995;79(11):1007-1011. doi: 10.1136/bjo.79.11.1007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Efron N, Morgan PB, Katsara SS. Validation of grading scales for contact lens complications. Ophthalmic Physiol Opt. 2001;21(1):17-29. [PubMed] [Google Scholar]
- 21.European Medicines Agency . Ikervis. EMA/CHMP/473489/2014. January 22, 2015. Accessed October 12, 2020. https://www.ema.europa.eu/en/documents/assessment-report/ikervis-epar-public-assessment-report_en.pdf
- 22.Pflugfelder S. Management and therapy of dry eye disease: report of the Management and Therapy Subcommittee of the International Dry Eye Workshop (2007). Ocul Surf. 2007;5(2):163-178. doi: 10.1016/S1542-0124(12)70085-X [DOI] [PubMed] [Google Scholar]
- 23.Rao N. Dry eye. In: Yanoff M, Duker S, eds. Ophthalmology. 4th ed. Elsevier Saunders; 2014. [Google Scholar]
- 24.Younger J, McCue R, Mackey S. Pain outcomes: a brief review of instruments and techniques. Curr Pain Headache Rep. 2009;13(1):39-43. doi: 10.1007/s11916-009-0009-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Baudouin C, Aragona P, Van Setten G, et al. ; ODISSEY European Consensus Group Members . Diagnosing the severity of dry eye: a clear and practical algorithm. Br J Ophthalmol. 2014;98(9):1168-1176. doi: 10.1136/bjophthalmol-2013-304619 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Patel VD, Watanabe JH, Strauss JA, Dubey AT. Work productivity loss in patients with dry eye disease: an online survey. Curr Med Res Opin. 2011;27(5):1041-1048. doi: 10.1185/03007995.2011.566264 [DOI] [PubMed] [Google Scholar]
- 27.Yu J, Asche CV, Fairchild CJ. The economic burden of dry eye disease in the United States: a decision tree analysis. Cornea. 2011;30(4):379-387. doi: 10.1097/ICO.0b013e3181f7f363 [DOI] [PubMed] [Google Scholar]
- 28.Jones L, Downie LE, Korb D, et al. TFOS DEWS II management and therapy report. Ocul Surf. 2017;15(3):575-628. doi: 10.1016/j.jtos.2017.05.006 [DOI] [PubMed] [Google Scholar]
- 29.Baudouin C, Irkeç M, Messmer EM, et al. ; ODISSEY European Consensus Group Members . Clinical impact of inflammation in dry eye disease: proceedings of the ODISSEY group meeting. Acta Ophthalmol. 2018;96(2):111-119. doi: 10.1111/aos.13436 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Begley CG, Chalmers RL, Abetz L, et al. The relationship between habitual patient-reported symptoms and clinical signs among patients with dry eye of varying severity. Invest Ophthalmol Vis Sci. 2003;44(11):4753-4761. doi: 10.1167/iovs.03-0270 [DOI] [PubMed] [Google Scholar]
- 31.Dana R, Meunier J, Markowitz JT, Joseph C, Siffel C. Patient-reported burden of dry eye disease in the United States: results of an online cross-sectional survey. Am J Ophthalmol. 2020;216:7-17. doi: 10.1016/j.ajo.2020.03.044 [DOI] [PubMed] [Google Scholar]
- 32.Nichols KK, Donnenfeld ED, Karpecki PM, et al. Safety and tolerability of lifitegrast ophthalmic solution 5.0%: pooled analysis of five randomized controlled trials in dry eye disease. Eur J Ophthalmol. 2019;29(4):394-401. doi: 10.1177/1120672118791936 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Donnenfeld ED, Karpecki PM, Majmudar PA, et al. Safety of lifitegrast ophthalmic solution 5.0% in patients with dry eye disease: a 1-year, multicenter, randomized, placebo-controlled study. Cornea. 2016;35(6):741-748. doi: 10.1097/ICO.0000000000000803 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Boboridis KG, Konstas AGP. Evaluating the novel application of cyclosporine 0.1% in ocular surface disease. Expert Opin Pharmacother. 2018;19(9):1027-1039. doi: 10.1080/14656566.2018.1479742 [DOI] [PubMed] [Google Scholar]
- 35.Cutolo CA, Barabino S, Bonzano C, Traverso CE. The use of topical corticosteroids for treatment of dry eye syndrome. Ocul Immunol Inflamm. 2019;27(2):266-275. doi: 10.1080/09273948.2017.1341988 [DOI] [PubMed] [Google Scholar]
- 36.Leonardi A, Van Setten G, Amrane M, et al. Efficacy and safety of 0.1% cyclosporine A cationic emulsion in the treatment of severe dry eye disease: a multicenter randomized trial. Eur J Ophthalmol. 2016;26(4):287-296. doi: 10.5301/ejo.5000779 [DOI] [PubMed] [Google Scholar]
- 37.Sall K, Stevenson OD, Mundorf TK, Reis BL. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease: CsA Phase 3 Study Group. Ophthalmology. 2000;107(4):631-639. doi: 10.1016/S0161-6420(99)00176-1 [DOI] [PubMed] [Google Scholar]
- 38.Lemp MA. Management of dry eye disease. Am J Manag Care. 2008;14(3)(suppl):S88-S101. [PubMed] [Google Scholar]
- 39.Atallah RT, Castanos MV, Najac R, Donnenfeld E. Six months’ treatment with lifitegrast in patients with moderate-to-severe symptomatic dry eye: a retrospective chart review. Clin Ophthalmol. 2019;13:1033-1037. doi: 10.2147/OPTH.S191635 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
OPUS-2 SAP
OPUS-3 SAP
OPUS-2 Protocol
OPUS-3 Protocol
eFigure 1. Percentage of Participants With DED and Improvement in Symptoms (EDS) From Baseline to Day 84, by Treatment Group (Pooled Data)
eFigure 2. Percentage of Participants With DED and Improvement in Symptoms (Global VAS) From Baseline to Day 84, by Treatment Group (Pooled Data)
Data Sharing Statement