

Abstract
Following the ‘second wave’ of COVID-19 in India, there has been an upsurge of domestic travel to holiday destinations, particularly Himalayan mountain towns. Modelling suggests that such travel could enhance the peak of a third wave in these states by almost 50%. Principles of ‘responsible travel’ should be adhered to.
Keywords: SARS-CoV-2 Infection, Basic reproduction Number, Human Social Behaviour, Effective Contact, Travel
India’s recent ‘second wave’ of COVID-19 was severe, but showed varying impact in different states. Smaller states with rarefied population witnessed not only less intense spread than was apparent at the national level, but also delayed attainment of the second peak. Amongst these ‘smaller states’ are popular tourist destinations such as Himachal Pradesh and Assam, that are currently seeing an upsurge of visitors from elsewhere in the country. For example, there was a recent increase of visitors to Manali, a town at the foothills of the Himalayas in Himachal Pradesh. Other popular destinations such as Darjeeling in West Bengal and Assam in the North Eastern states of India, have also seen similar surges. These observations indicate increasing opportunities for transmission in areas where population-level immunity has not yet accumulated to the same levels as elsewhere in the country. Against a backdrop of increasing anticipation of a third wave of COVID-19 in India, it is important to recognize the potential risks associated with such an escalation in travel.
Mathematical modelling offers a helpful tool for understanding these risks. Building on previous work,1 Figure 1 illustrates some possible scenarios in a hypothetical state of India (see Supplementary Appendix for details), constructed to resemble Himachal Pradesh in the dynamics of its first and second waves, including the much lower seroprevalence of SARS-CoV-2 compared to the rest of the country (https://www.covid19india.org/state/HP). As illustrated by earlier work,1 it is possible that relaxation of state-level restrictions could give rise to a third wave on its own (blue trajectory).
Figure 1 .
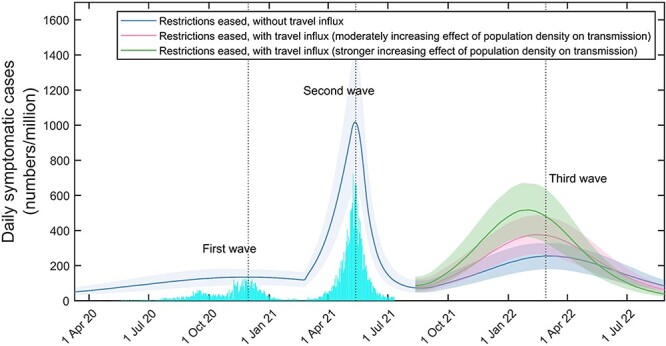
Illustration of a third wave of COVID-19 in a hypothetical State in India due to lifting of restrictive measures, and influx of visitors. Solid lines show central (median) estimates, whereas shaded areas show 95% uncertainty intervals. Turqouise bars represent the reported cases per million population in the State of Himachal Pradesh, India during the first two-waves of COVID-19. For third-wave projections, three scenarios are shown: (i) complete easing of restrictions by (31 May 2021), without any influx of holiday travel (blue curve); (ii) easing of restrictions with influx of holiday travel, assuming that transmission increases with population density in the same way as estimated in the USA4 in (red curve); (iii) as for the second scenario, but assuming that transmission increases with population density at twice the rate as estimated in the USA (green curve). These dynamics are not intended to be predictive, but serve to illustrate some plausible outcomes for the third wave in this modelled State.
A sudden increase in population density due to incoming tourists2 or mass congregation due to social, political or religious reasons can worsen the third-wave scenario.3 A recent study in the USA suggests that an increase in one unit of log population density increased  by 0.16 (95% CI: 0.13–0.09).4 Moreover, data from Himachal Pradesh suggests that in a typical holiday season, tourism can increase the population (and thus population density) by 40%.5 Taking this into consideration, Figure 1 shows that the third-wave peak could increase by up to 47% during the holiday season (red curve), and could occur 2 weeks earlier, compared to a scenario of easing restrictions in the absence of holiday travel. Figure 1 further illustrates a scenario where population density in India has a stronger effect on transmission than in the USA (green curve): here, the holiday period could amplify the third-wave peak by up to 103% and cumulative incidence in that wave by 43%, and hasten the timing of the epidemic peak by 4 weeks, compared to a scenario of easing restrictions in the absence of holiday travel. In India, the role of domestic travel in the spread of COVID-19 was recognized as early as in the ‘first wave’ of the pandemic in 2020.6,7
by 0.16 (95% CI: 0.13–0.09).4 Moreover, data from Himachal Pradesh suggests that in a typical holiday season, tourism can increase the population (and thus population density) by 40%.5 Taking this into consideration, Figure 1 shows that the third-wave peak could increase by up to 47% during the holiday season (red curve), and could occur 2 weeks earlier, compared to a scenario of easing restrictions in the absence of holiday travel. Figure 1 further illustrates a scenario where population density in India has a stronger effect on transmission than in the USA (green curve): here, the holiday period could amplify the third-wave peak by up to 103% and cumulative incidence in that wave by 43%, and hasten the timing of the epidemic peak by 4 weeks, compared to a scenario of easing restrictions in the absence of holiday travel. In India, the role of domestic travel in the spread of COVID-19 was recognized as early as in the ‘first wave’ of the pandemic in 2020.6,7
Now, in the wake of the overwhelming second wave throughout India, ‘revenge travel’—or an urge to travel after being under restrictions for an extended period of time—is a term increasingly being used by the media to describe what has been observed in Manali, Darjeeling and other popular tourist destinations. Such travel is particularly worrying when it involves destinations such as Himalayan mountain towns, which not only are less population-dense but also have previously imposed restrictions effectively controlling transmission, and would now see substantial increase in population density with the influx of tourists. In light of the possible resurgence shown in Figure 1, we believe that ‘responsible travel’ rather than ‘revenge travel’ will be a more prudent call in the present time.
We propose that ‘responsible travel’ would have several important elements. Amongst visitors at least, responsible mask use and observing social distancing norms could have important effects in mitigating the risk of transmission. Beyond their protective effect, mandating these precautions will also serve as an important, continuing reminder of the risk of COVID-19. Conditions on travel could also play a key role, for example with potential visitors only being eligible to travel if they can show evidence of a recent COVID-negative test. Vaccine status could also play an important role in eligibility to travel, with some caveats. First, ‘vaccine passports’ have limitations, arising from uncertainties about how the nature and strength of vaccine-induced immunity would change over time.8 Second, despite being the world’s largest producer of COVID-19 vaccines, India also faces the challenge of having the world’s second-largest population to vaccinate; at the time of writing, it is estimated that roughly 20% of India’s eligible population has been fully vaccinated. Nonetheless, as vaccination coverage scales up in the coming months, vaccine status could play an increasingly important role in eligibility to travel. Future immunization planning may also benefit from prioritizing the local population in holiday destinations.
It will also be important to maintain surveillance in at-risk settings, ensuring that virological testing is maintained even in periods of apparent low infection activity. In addition, information on genomic surveillance in other countries9 and vigil at international airports will be valuable for early identification of hitherto unrecognized variants that could later gain a foothold across the country. Although no national guideline exists on restrictions regarding domestic travel, it may be helpful for holiday-destination states to receive guidance on how they could best mitigate travel related risks. Box 1 lists some proposed considerations for this state-level guidance. Indeed, although we discuss these considerations in the context of holiday travel, in practice they would be relevant to any circumstance that involves temporary but intense increases in population density within a state. For example, there are several well-known religious events and cultural festivals that draw large number of visitors from within and outside the state, including the hornbill festival in Nagaland and the Sangai festival in Manipur. Although Kerala’s continuing epidemic is likely to be due to a combination of factors, including rates of testing that are unmatched elsewhere in India, it has also followed soon after the lifting of restrictions around sociocultural and religious events in the state. Other mass congregations include spectators at sporting events and participants in political rallies. In all of these circumstances, in a country as large and complex as India, the national Government cannot always issue mandates at a federal level, and thus it may fall to states to adopt and implement these guidelines according to their own circumstances and needs.
To inform state-level decisions, there is also a need to understand drivers of transmission, and how these drivers may vary in response to, and following, restrictions. For respiratory diseases, where transmission can occur through face-to-face conversation during close proximity, such as influenza or COVID-19, measuring social contacts becomes relevant. These contacts may range from shaking hands, or a long chat at a popular café, to a brief interaction at the roadside. It is now known that people belonging to similar age brackets come in greater contact with each other.10 However, the frequency of such interactions per day vary between sociocultural settings; recent research has revealed that11,12 the residents of Hong Kong and UK on a typical day would have physical contact with around five other people, whereas in Italy this average is 10. These characterizations reflect a stable social milieu and situations during daily routine activities. However, travel during large-scale emergencies, including cross-border migration or visits to tourist destinations, not only defies such averages, but also creates new contacts and assortments. Understanding how contacts change in these circumstances can be valuable in managing the risk of future resurgence of disease.
In conclusion, there are undoubtedly important benefits as society gradually returns to normal, in India and elsewhere; domestic travel to holiday destinations provides benefits not just for visitors, but also for local economies that have been under considerable stress for over a year. Nonetheless, with the possibility of a severe third wave in India still looming, it remains critical to recognize and mitigate the risks involved. A shared sense of responsibility, amongst visitors, residents and local authorities, will go a long way towards protecting the welfare of the country as a whole.
Box 1. Summary of proposed principles for ‘responsible travel’
Suggested considerations for states in India, to inform their policies on travel.
Individuals should be advised not to travel if they have COVID-like symptoms, including a prolonged dry cough, or loss of taste and smell.
States may consider requiring proof of completed vaccination status, or a recent COVID-negative test result, in order to stay at accommodations in destinations within the state.
The aforementioned restrictions could be applied at the point of arrival in holiday accommodation, where current rules require the collection of traveller details.
All travellers should also register their contact details upon arrival, to facilitate contact tracing in the event of any upsurge in infection.
While visiting, travellers should be advised to observe COVID-appropriate behaviour, including mask use and social distancing.
Rather than coercive measures, all of the above should be seen as collaborative efforts between the local population, visitors and local government.
Authors’ contributions
SP and BB conceptualized the study; SM and NA developed the modelling approach and SM performed the modelling. All authors analysed and interpreted the results; SM and SP wrote a first draft of the manuscript, and all authors contributed to the final draft and approved the version for submission to the journal.
Conflicts of interest
None declared.
Supplementary Material
Acknowledgement
Authors (SM, BB and SP) acknowledge funding from the Indian Council of Medical Research, and NA acknowledges funding from the UK Medical Research council. No additional funding or grant support was utilized for execution of this study by the authors who remained supported by their respective institutes of affiliation as indicated while independently carrying out the present study.
Contributor Information
Sandip Mandal, Indian Council of Medical Research, New Delhi 110029, India.
Nimalan Arinaminpathy, MRC Centre for Global Infectious Disease Analysis, School of Public Health, Imperial College London, London W2 1PG, UK.
Balram Bhargava, Indian Council of Medical Research, New Delhi 110029, India.
Samiran Panda, Indian Council of Medical Research, New Delhi 110029, India.
References
- 1. Mandal S, Arinaminpathy N, Bhargava B, Panda S. Plausibility of a third wave of COVID-19 in India: a mathematical modelling based analysis. Indian J Med Res 2021. 10.4103/ijmr.ijmr_1627_21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Statistics IT. Ministry of Tourism. Gov India 2019; 2019. https://tourism.gov.in. [Google Scholar]
- 3. Panda S, Kaur H, Dandona L, Bhargava B. Face mask - an essential armour in the fight of India against COVID-19. Indian J Med Res 2021; 153:233–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Sy KTL, White LF, Nichols BE. Population density and basic reproductive number of COVID-19 across United States counties. PLoS One 2021; 16:e0249271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. ORG-MARG Acn. Tourism survey for the state of Himachal Pradesh (April 2011 – March 2012). Gov of India: Ministry of Tourism, 2012. https://tourism.gov.in/statistical-surveys. [Google Scholar]
- 6. Ebrahim SH, Ali A, Koya SF et al. Focus on international and domestic travellers are equally important for successful SARS-COV-2 mitigation: ecological comparison of emigrant and migrant travel patterns and COVID-19 trends in Kerala State, India. J Travel Med 2021; 28:taab003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Azad S, Devi S. Tracking the spread of COVID-19 in India via social networks in the early phase of the pandemic. J Travel Med 2020; 27:taaa130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Chen LH, Freedman DO, Visser LG. COVID-19 immunity passport to ease travel restrictions? J Travel Med 2020; 27:taaa085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Scheepers C, Everatt J, Amoako DG et al. The continuous evolution of SARS-CoV-2 in South Africa: a new lineage with rapid accumulation of mutations of concern and global detection. medRxiv 2021. 10.1101/2021.08.20.21262342 August 24, 2021, preprint: not peer reviewed. [DOI] [Google Scholar]
- 10. Hoang T, Coletti P, Melegaro A et al. A systematic review of social contact surveys to inform transmission models of close-contact Infections. Epidemiology 2019; 30:723–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Mossong J, Hens N, Jit M et al. Social contacts and mixing patterns relevant to the spread of infectious diseases. PLoS Med 2008; 5:e74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Kucharski AJ, Kwok KO, Wei VWI et al. The contribution of social behaviour to the transmission of influenza A in a human population. PLoS Pathog 2014; 10:e1004206. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.