

Abstract
A significant proportion of African American (AA) fathers live in households apart from their young children. This living arrangement can have detrimental effects for children, families, and fathers. One hundred seventy-eight (n = 178) AA fathers, not residing with their 2–6-year-old children, were enrolled in a randomized trial to test the Building Bridges to Fatherhood (BBTF) program against a financial literacy comparison condition. BBTF is an intervention that was developed collaboratively with a fathers’ advisory council of AA fathers who oversaw all aspects of program development. Based upon advisory council feedback, short video scenes captured fathers interacting with their children, their children’s mothers, and other fathers. These video scenes were used to jump start the discussion around fatherhood, parenting, communication, and problem solving during the intervention group meetings. The actors in the video scenes were recruited from the community. Two trained group leaders, using a standardized group leader manual, delivered the intervention. The Money Smart Financial Literacy Program (MSFLP), which served as the comparator, was also delivered by AA men. Program satisfaction was high in both conditions. Even so recruitment and retention challenges influenced the ability to detect father and child outcomes. This study informs the participation of vulnerable urban AA fathers in community-based fatherhood intervention research and provides insight into bolstering engagement in studies focused on this population.
Supplementary Information
The online version contains supplementary material available at 10.1007/s11524-021-00549-8.
Keywords: Fatherhood, Interventions, African American, Recruitment, Retention
Introduction
Although 2.3 million African American (AA) fathers live with their children, there are 1.7 million who do not [1]. AA families have the greatest percentage of children who live apart from their fathers [2], and these non-resident fathers are an understudied and vulnerable population [3]. Father non-residency can exert a negative influence on men’s health and contribute to lower father involvement [4, 5]. Beyond residency status, there are a number of additional factors that influence father involvement, such as fathers’ age, education, employment status, social support, mental health, marital status, and relationship with the child’s mother [4, 6–10]. Thus, the phenomenon of father involvement for non-resident fathers is complex and multi-faceted.
Most attention to the impact of father involvement is focused on child outcomes, possibly because of the plethora of literature demonstrating that positively involved fathers, even when they are nonresident, play key beneficial roles in the lives of their children [11, 12]. For example, the positive involvement of non-resident fathers contributes to children’s academic achievement, behavioral, emotional, psychological, and social well-being; and the quality of involvement has been found to matter more than the quantity of involvement [13].
Fatherhood Interventions
In light of these positive findings, policymakers have advocated for fatherhood initiatives that strengthen father involvement [14]. More researchers have turned their attention towards developing and testing interventions to support positive and enduring involvement among non-resident fathers [15–17]. Additionally, the evaluation of randomized clinical trial interventions designed to support father involvement among diverse non-resident fatherhood populations is slowly emerging as a field of inquiry [15].
Recruitment and Retention
Preventive fatherhood interventions, designed to promote positive family interactions, have been impacted by recruitment, engagement, and retention challenges [18, 19]. Evidence suggests that recruiting, engaging, and retaining African American fathers in preventive interventions can be even more complex than engaging less diverse fathers [19]. This complexity is likely due to the multiple logistical factors that may influence fathers’ ability to participate in interventions such as location, timing, and intentional focus on fathers [20]. The degree of participation in the intervention impacts study outcomes because of the importance of dosage in determining intervention efficacy. There are gaps in knowledge related to fathers’ engagement (level of participation [21–23]; and retention (adherence to study protocol and maintenance in the study [24–26]; in fatherhood interventions.
Fatherhood intervention participation may be particularly desirable in vulnerable families because of the need to marshal all available parenting support for the benefit of children. Yet, in families with challenging societal contexts, optimal participation may be less likely. Therefore fatherhood interventions must align with the cultural perspectives of participants while also considering potential challenges to recruitment, engagement, and retention. The findings from this study provide valuable insights into understanding the engagement of AA non-resident fathers in preventive fatherhood interventions. The two-fold purpose of this paper is to report the outcomes of the Dedicated African American Dad (DAAD) study and lessons learned related to engaging AA non-resident fathers in a fatherhood intervention.
Method
Sample Recruitment
We conducted a randomized controlled trial (RCT) of two fatherhood interventions. Data were collected from fathers via in-person interviews at their location of choice at three time points (baseline, post-intervention, and 6-month post-baseline). Mothers were recruited into the study as data informants who provided data via telephone interview on father involvement and child outcomes according to the same schedule. Father and mother reports of relationship quality were collected in order to test whether father-mother relationship quality and father outcomes mediated intervention effects on paternal involvement.
The study was approved by the University Institutional Review Board. A Certificate of Confidentiality was obtained in order to protect the privacy of participants’ sensitive information. Fathers were eligible to participate if they were the AA biological father of a child 2–6 years of age; the child stayed in the father’s home no more than 48 h per week (i.e., weekends), and the father could spend time with the child who lived with the biological mother or other custodial relative. Additional inclusion criteria included the child’s mother being amenable to father-child interaction so the father could practice skills learned in the program and the father’s willingness to travel to the intervention site to attend the group meetings. Fathers were excluded if there were current safety concerns reported by the father or mother including having a history of child abuse, neglect, or violence perpetuated against the child or child’s mother (based on mother or father report).
Intervention/Comparison Condition
The intervention, Building Bridges To Fatherhood (BBTF), is a 9-session intervention + booster session, designed to be implemented with groups of 10–15 fathers. The intervention, delivered by two trained group leaders, was scheduled in 3-week intervals, with a 1 week break in between. Just prior to the break week, participating fathers were given activity vouchers to spend fun time with the target child in lieu of group attendance (e.g., museums, the zoo, movie theater). BBTF was developed in collaboration with a father’s advisory council of AA fathers [27]. Program content includes the importance of fathers to the family, parenting strategies for fathers, and communication and problem solving [27]. Short video scenes, discussion questions, and a group leader manual are used by two trained group leaders to generate discussion, problem solving, and sharing among fathers in the group.
The comparison condition was the Money Smart Financial Literacy Program (MSFLP), which was developed by the Federal Insurance Deposit Corporation (FDIC). The MSFLP, which is freely available and without copyright restrictions, is designed to improve participants’ financial skills and banking practices [28]. The comparator was delivered parallel to the BBTF intervention and facilitated by a trained AA male group leader who is also a father.
Subjects/Study Recruitment and Retention
African American non-resident fathers were recruited by AA male and female research assistants who were comfortable navigating urban communities of color. Recruitment sites included community settings frequented by AA men such as barber shops, gyms, and restaurants. Flyers were distributed in the community that included a dedicated recruitment study telephone line and a quick response (QR) code so that interested fathers could connect directly to the online interest form using their “smart” devices. Once participants were screened, and consented, an interview was scheduled, and fathers were incentivized with a $50 gift card for completing study research measures at baseline, post-intervention, and 6 month post-baseline. They were then randomized into either the BBTF or MSFLP condition. An activity voucher, valued at $30, was provided just prior to each of the three scheduled break weeks to support fathers’ participation in fun activities with their children. Fathers also received dinner and reimbursement in the amount of $10 for transportation costs at each group meeting. Mothers were incentivized with a $40 gift card for completing research measures at each of three data collection time points.
Fidelity
The five components of treatment fidelity as outlined in the Behavior Change Consortium’s model of treatment fidelity were followed [29]. These components include design, staff and training, intervention delivery, intervention receipt, and enactment. To monitor delivery of BBTF, all groups were audio recorded, and a random selection of 25% of audio recorded sessions were rated for adherence to the BBTF protocol and the quality of group leader facilitation skills using an adaptation of the Fidelity Checklist [30]. Detailed feedback on the BBTF Fidelity Checklist was provided to the group leaders to provide ongoing training and coaching, prevent intervention drift, and assure fidelity to the delivery model.
The comparator (MSFLP), group leader training was conducted through the instructor-led Money Smart training CD, which includes a helpful guide to presenting the Money Smart Curriculum. Train-the-trainer videos provide instructors with an overview of the curriculum components and highlight effective teaching strategies. Videos also provide content designed to familiarize group leaders with the student materials and stress the importance of advanced preparation. Group leaders were trained in the use of the curriculum and completed weekly checklists to monitor attendance, adherence to the protocol and enactment of skills.
Research Measures
Measures
Proximal dependent variables included paternal involvement (material and in-kind (non-monetary) support and direct father/child interaction), father parenting competence (self-efficacy, satisfaction, parenting skills, and knowledge), father psychological well-being (self-esteem, general and racial stress), and father communication and problem solving. Distal outcomes included father and maternal reports of child behavior and development (cognitive, emotional, and social). Covariates included father demographics (age, marital status, highest grade completed, employment status, monthly income, conviction of a felony (yes/no), indicators of economic disadvantage, target child age/gender, and number of children) and satisfaction with social support. The Social Support Questionnaire (SSQ) [31] is a self-report measure of the availability (number of individuals) and satisfaction of a person’s social support. Cronbach’s alpha reliability for the number scale (number of support individuals) and satisfaction scale (fathers satisfaction with support; 1 = very dissatisfied to 6 = very satisfied) were .88 and .84, respectively. See Table 1 for a description of the father and child outcome measures. All outcome measures are self-reported by fathers, and data were collected at baseline, 12-week post-baseline, and 24-week post-baseline.
Table 1.
Description of father and child measures
| Variable/measure | Description | Scale | Subscale (# of items) | Scale rangea | Cronbach alphab |
|---|---|---|---|---|---|
| Physiological well-being (father) | |||||
| Center for Epidemiological Studies-Depression (CES-D) (Radloff, [32]) | Depression symptoms experienced in the past week |
0 = rarely or none of the time 3 = most or all of the time |
Total scale (20) | 0–60 (S) | .82 |
| Perceived Stress Scale (PSS) (Cohen et al., [33]) | Degree in which situations are experienced as stressful |
0 = never 4 = very often |
Total scale (10) | 0–40 (S) | .77 |
| Taylor Inventory of Self-Esteem (Taylor & Tomasic, [34]) | Measures of self-esteem and rewards and costs to self |
0 = never 8 = always |
Negative self-esteem (8) | 0–8 (M) | .65 |
| Positive self-esteem (8) | 0–8 (M) | .83 | |||
| Communication and problem solving (father) | |||||
| Tolerance For Disagreement (TFD) (Teven et al., [35]) | The degree of tolerance of interpersonal disagreement |
1 = strongly disagree 5 = strongly agree |
Total scale (15) | 15–75 (S) | .68 |
| Personal Problem Solving Inventory (PSI) (Maydeu-Olivares & D'Zurilla, [36]) | Subscales of problem solving self-efficacy and problem solving skills |
1 = strongly agree 6 = strongly disagree |
Efficacy(7) | 1–6 (M) | .70 |
| Skills (9) | 1–6 (M) | .65 | |||
| Father-mother relationship quality | |||||
|
Quality of Relationship Inventory (QRI) (Pierce et al., [37]) |
Measure of support, conflict, and depth of father-mother relationship |
1 = not at all 4 = very much |
Conflict (12) | 1–4 (M) | .83 |
| Support (7) | 1–4 (M) | .87 | |||
| Depth (6) | 1–4 (M) | .85 | |||
| Parenting (father) | |||||
| Parent Behavior Checklist (PBC) (Fox, [38]) | Measure of parenting skills and knowledge |
1 = almost never/never 4 = almost always/always |
Discipline (10) | 1–4 (M) | .76 |
| Nurturing (10) | 1–4 (M) | .75 | |||
| Expectations (12) | 1–4 (M) | .85 | |||
| Parenting Sense of Competence Scale (PSOC) (Johnston & Mash, [39]) | Parent satisfaction and self-efficacy in their role |
1 = strongly disagree 6 = strongly agree |
Satisfaction (9) | (S) | .59 |
| Self-efficacy (7) | (S) | .70 | |||
| Paternal involvement (father) | |||||
| Julion Index of Paternal Involvement (JIPI; Julion, [40]) | Direct father-child interaction (caregiving, teaching, and nurturing) |
1 = never 4 = almost always |
Total scale (19) | 1–4 (M) | .94 |
| Fragile Families Survey (FFS; Reichman et al, [41]) | Material and in-kind support fathers provide for their children |
1 = never 4 = always |
Total scale (13) | 13–52 (S) | .84 |
| Child behavior (child) | |||||
| Behavior Assessment System for Children 3rd Ed (BASC-3) (Reynolds & Kamphaus, [42]) | Adaptive and problem behaviors in community and home setting |
0 = never 3 = almost always |
Aggression (11) | T-scoresd | .45 |
| Attention (6) | .58 | ||||
| Depression (11–14) | .69 | ||||
| Hyperactivity (10, 11) | .70 | ||||
aLetter in parentheses indicates whether mean (M) or sum (S) scored
bCronbach alpha reliability coefficient in study sample at baseline assessment (N =178)
cIndividual items used for analysis
dPreschool and school age version of the BASC-3 was used and scores were converted to T-scores using norms based on age and gender
Attendance and weekly parent satisfaction data were collected from fathers in both conditions. BBTF intervention treatment fidelity was assessed using an adaptation of The Fidelity Checklist [30]. The fidelity of the weekly comparator sessions was assessed with an investigator developed weekly group leader checklist.
Data Analysis
Handling of Missing Data
Missing data were imputed using chained equations [43] to create fifty imputed datasets. All assessments of all outcome variables and key covariates were included in the imputation model to satisfy the assumption of missing at random. Estimates from the imputed datasets were then pooled to account for within- and between-dataset variation. Analyses were performed using SAS software [44].
Statistical Analyses
Descriptive statistics were used to report program usage metrics and satisfaction. Data were analyzed using a 3 × 2 repeated measures analysis of covariance (RM-ANCOVA) with three assessment time points (baseline, 12 weeks, and 24 weeks) crossed with two between-subject treatment conditions (BBTF and MSFLP). The null hypothesis for all of these analyses was that all outcomes remained equal across the two groups over time. Planned follow-up analyses parameterized time into a set of two orthogonal Helmert contrasts (1, −½; 0, 1, −1). The first contrast tested whether critical changes occurred between times 1 and 2. The second contrast tested whether critical changes occurred between times 2 and 3. Covariates were selected based on associations with outcome variables. Five variables were included as covariates: father’s age, father’s highest level of education, number of members in father’s social network, number of adults in the household, and sex of the target child.
In addition to the primary intent-to-treat analyses, we tested attendance as a moderator of intervention effects. We created a dichotomous measure of attendance, defined as attending 5 or more of the 10 sessions. This resulted in a 3 × 2 × 2 repeated measures analysis of variance (RM-ANOVA). Planned contrasts (described above) were estimated separately for high and low attenders.
Results
The results of this study are described according to the following domains: participant descriptives, treatment fidelity, satisfaction, engagement (recruitment, attendance, retention), and study outcomes. All fathers were self-identified as African American as part of our eligibility requirement. A little under half (46%) of fathers had a high school diploma with the majority of the fathers having some college or more (54%), low income (26%), and unemployed (36%; see Table 2). The mean child age was 3.83 years, and 53% (n =93) were male and 47% (n = 84) were female.
Table 2.
Study participant demographic characteristics (N=178)
| Demographic variable | ||
|---|---|---|
| n | % | |
| Father characteristics | ||
| AgeM(SD) | 33.54 (8.96) | |
| Marital status | ||
| Married/living with partner | 6 | 3 |
| Separated | 22 | 12 |
| Divorced | 21 | 12 |
| Never married | 129 | 73 |
| Education | ||
| <High school degree | 81 | 46 |
| Some college or more | 97 | 54 |
| Employment status | ||
| Part-time | 43 | 24 |
| Full-time | 58 | 33 |
| Not currently working | 64 | 36 |
| Going to school | 5 | 3 |
| Working and going to school | 8 | 4 |
| Monthly income | ||
| <$500 | 47 | 26 |
| $501–$1000 | 37 | 21 |
| $1001 to $2000 | 46 | 26 |
| $2001 to $3000 | 16 | 9 |
| $3001 + | 31 | 18 |
| Child characteristics | ||
| Age M (SD) | 3.83 (1.24) | |
| Gender | ||
| Male | 93 | 53 |
| Female | 84 | 47 |
Treatment Fidelity and Satisfaction
A random selection of audio recorded BBTF group sessions were reviewed and coded using an adaptation of the Fidelity Checklist [30]. The overall group leader competence was 2.72 (range = 2.46–2.86), and the average adherence to the BBTF protocol was 87.6% (range = 78.6–100%). In addition, group leaders completed a weekly self-report checklist to monitor adherence to the weekly protocol. We received checklists from 56 of the 81 groups (9 groups, 9 sessions each). Of those, group leaders reported an average of 95.7% adherence to the group sessions (range = 93.6 (session 6)–98% (session 4)). Participants completed weekly and end of program satisfaction surveys. BBTF and MSFLP satisfaction were high. In the BBTF condition, 26 participants completed 154 weekly program surveys across 9 sessions (that averaged 5.9 surveys (SD=2.6) per participant). On individual survey items that focused on program content, the video scenes, group leaders, group discussion, and practice assignments, the percent of participants who found those elements helpful or very helpful were 99%, 95%, 99%, 99%, and 93%, respectively. The group leaders and program content were rated most highly, and the practice assignments were rated the lowest. Of the 143 MSFLP satisfaction forms completed by 42 participants, 85% agreed or strongly agreed that the program was useful. Fathers endorsing that the instructor and overall program were good, very good, and excellent were 100% and 99%, respectively.
Engagement
We define engagement as the recruitment of participants into the study, participant attendance, and retention of participants across assessments [45, 46]. We recruited 192 fathers, and 178 were randomized; 124 mothers were recruited into the study. The initial intent of the study was to recruit mothers to provide multi-informant perspectives on father involvement, mother-father relationships, and child outcome measures. However, we successfully recruited only 65% of mothers in the study, making it difficult to perform these multi-informant analyses (see Fig. 1). Session attendance did not differ by study condition. Of 10 sessions, average attendance was 2.52 (SD = 3.43) sessions for BBTF and 2.35 (SD = 3.16); t(176) = −0.35, p = .73. A majority of participants attended zero sessions for both BBTF (n=53, 57.6%) and MSFLP (n=44, 51.2%). The rate of non-attendance was not different between conditions; X2(1, n=178) = 0.75, p=.39. Attendance at five or more sessions did not differ between BBTF (n=28, 30.4%) and MSFLP (n=22, 25.6%), X2(1, n=178) = 0.52, p=.47. There were 87 (49%) fathers who completed the post-intervention assessment and 104 (58%) fathers who completed the 3-month follow-up assessment.
Fig. 1.
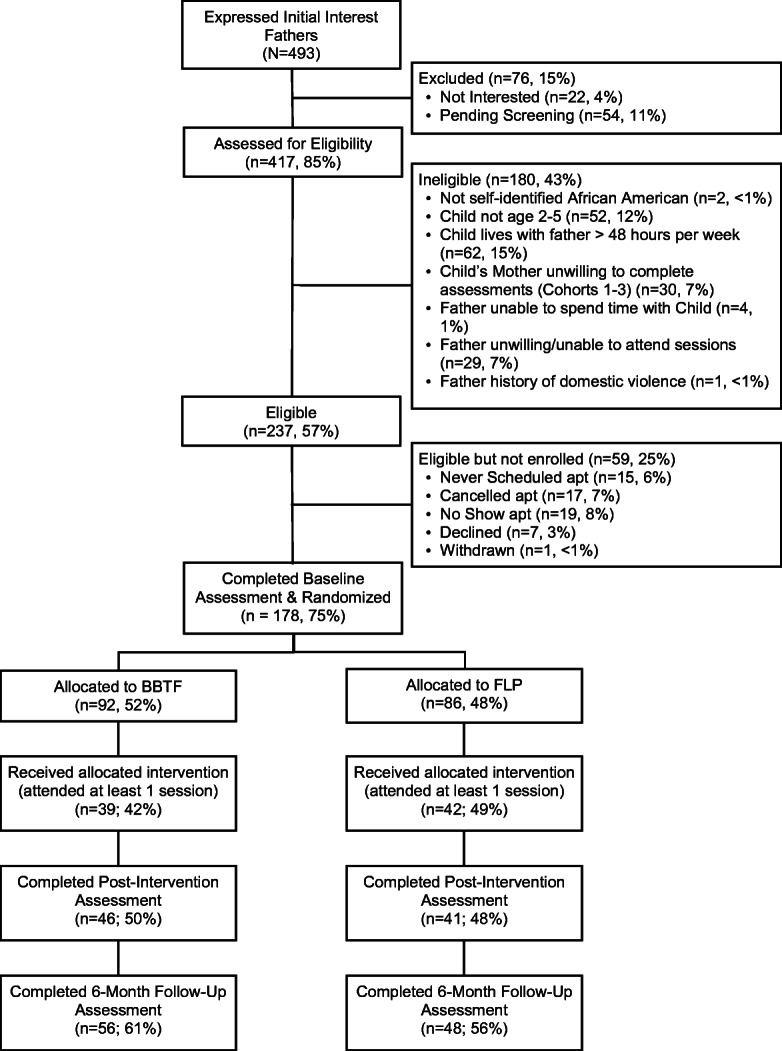
Consort diagram
DAAD Study Effects on Father-Child Outcomes
Intent to Treat Analyses
Treatment effects (i.e., treatment condition × assessment interactions) were non-significant for measures of father involvement (primary outcome measure) and other intervention targets (i.e., psychological well-being, parenting competence, communication, problem-solving ability, father-mother relationship quality (see Table 3). Table S4 in the Supplemental Material presents findings on planned contrasts for the main analyses. Treatment effects were also non-significant for child behavior outcomes.
Table 3.
Main father and child outcomes of intervention effects
| Outcome | Covariate/effect | F | df | p |
|---|---|---|---|---|
| Fragile Families Scale (FFS) of Paternal Involvement | ||||
| Father’s age (log transformed) | 1.84 | 1167 | .177 | |
| Number of adults in HH | 0.36 | 1167 | .548 | |
| Father highest grade completed | 1.93 | 1167 | .166 | |
| Number of social network members (log transformed) | 3.09 | 1167 | .081 | |
| Target child’s sex is female | 0.16 | 1167 | .691 | |
| Wave | 0.06 | 2167 | .940 | |
| Treatment condition | 0.08 | 1167 | .779 | |
| Wave × treatment condition | 0.04 | 2167 | .962 | |
| Julion Index of Paternal Involvement (JIPI) | ||||
| Father’s age (log transformed) | 0.33 | 1167 | .569 | |
| Number of adults in HH | 2.34 | 1167 | .128 | |
| Father highest grade completed | 0.15 | 1167 | .697 | |
| Number of social network members (log transformed) | 0.05 | 1167 | .817 | |
| Target child's sex is female | 1.18 | 1167 | .279 | |
| Wave | 1.66 | 2167 | .193 | |
| Treatment condition | 0.01 | 1167 | .914 | |
| Wave × treatment condition | 0.02 | 2167 | .982 | |
| Taylor Inventory of Self-Esteem_positive | ||||
| Father’s age (log transformed) | 0.70 | 1167 | .405 | |
| Number of adults in HH | 0.07 | 1167 | .799 | |
| Father highest grade completed | 3.91 | 1167 | .050 | |
| Number of social network members (log transformed) | 0.11 | 1167 | .737 | |
| Target child’s sex is female | 0.26 | 1167 | .608 | |
| Wave | 0.75 | 2167 | .473 | |
| Treatment condition | 2.08 | 1167 | .152 | |
| Wave x Treatment Condition | 0.63 | 2167 | .534 | |
| Taylor Inventory of Self-Esteem_negative | ||||
| Father’s age (log transformed) | 0.99 | 1167 | .321 | |
| Number of adults in HH | 0.00 | 1167 | .952 | |
| Father highest grade completed | 3.14 | 1167 | .078 | |
| Number of social network members (log transformed) | 0.11 | 1167 | .742 | |
| Target child’s sex is female | 1.46 | 1167 | .229 | |
| Wave | 0.72 | 2167 | .489 | |
| Treatment condition | 0.14 | 1167 | .710 | |
| Wave × treatment condition | 0.32 | 2167 | .730 | |
| Perceived Stress Scale_neg | ||||
| Father’s age (log transformed) | 1.11 | 1167 | .293 | |
| Number of adults in HH | 0.06 | 1167 | .813 | |
| Father highest grade completed | 4.97 | 1167 | .027 | |
| Number of social network members (log transformed) | 0.89 | 1167 | .347 | |
| Target child’s sex is female | 3.88 | 1167 | .050 | |
| Wave | 1.44 | 2167 | .240 | |
| Treatment condition | 0.44 | 1167 | .510 | |
| Wave × treatment condition | 0.08 | 2167 | .927 | |
| Perceived Stress Scale_pos | ||||
| Father’s age (log transformed) | 0.13 | 1167 | .714 | |
| Number of adults in HH | 0.08 | 1167 | .778 | |
| Father highest grade completed | 2.42 | 1167 | .122 | |
| Number of social network members (log transformed) | 0.19 | 1167 | .664 | |
| Target child’s sex is female | 1.54 | 1167 | .216 | |
| Wave | 2.49 | 2167 | .086 | |
| Treatment condition | 0.16 | 1167 | .687 | |
| Wave × treatment condition | 0.17 | 2167 | .841 | |
| CESD | ||||
| Father’s age (log transformed) | 0.19 | 1167 | .667 | |
| Number of adults in HH | 0.25 | 1167 | .621 | |
| Father highest grade completed | 4.91 | 1167 | .028 | |
| Number of social network members (log transformed) | 1.19 | 1167 | .276 | |
| Target child’s sex is female | 3.46 | 1167 | .065 | |
| Wave | 0.23 | 2167 | .798 | |
| Treatment condition | 0.55 | 1167 | .460 | |
| Wave × treatment condition | 0.33 | 2167 | .722 | |
| Parenting Sense of Competence_satisfaction | ||||
| Father’s age (log transformed) | 0.10 | 1167 | .750 | |
| Number of adults in HH | 0.01 | 1167 | .917 | |
| Father highest grade completed | 4.72 | 1167 | .031 | |
| Number of social network members (log transformed) | 0.00 | 1167 | .997 | |
| Target child’s sex is female | 0.22 | 1167 | .641 | |
| Wave | 0.23 | 2167 | .792 | |
| Treatment condition | 1.68 | 1167 | .196 | |
| Wave × treatment condition | 0.34 | 2167 | .715 | |
| Parenting Sense of Competence_efficacy | ||||
| Father’s age (log transformed) | 0.03 | 1167 | .871 | |
| Number of adults in HH | 0.00 | 1167 | .998 | |
| Father highest grade completed | 0.82 | 1167 | .367 | |
| Number of social network members (log transformed) | 0.26 | 1167 | .613 | |
| Target child’s sex is female | 0.97 | 1167 | .325 | |
| Wave | 0.19 | 2167 | .828 | |
| Treatment condition | 0.01 | 1167 | .923 | |
| Wave × treatment condition | 0.11 | 2167 | .900 | |
| Parent Behavior Checklist_expectations | ||||
| Father’s age (log transformed) | 0.01 | 1167 | .904 | |
| Number of adults in HH | 0.02 | 1167 | .894 | |
| Father highest grade completed | 4.54 | 1167 | .035 | |
| Number of social network members (log transformed) | 0.20 | 1167 | .653 | |
| Target child’s sex is female | 0.02 | 1167 | .900 | |
| Wave | 1.54 | 2167 | .218 | |
| Treatment condition | 0.25 | 1167 | .618 | |
| Wave × treatment condition | 0.03 | 2167 | .967 | |
| Parent Behavior Checklist_discipline | ||||
| Father’s age (log transformed) | 0.86 | 1167 | .354 | |
| Number of adults in HH | 0.98 | 1167 | .324 | |
| Father highest grade completed | 3.63 | 1167 | .058 | |
| Number of social network members (log transformed) | 3.99 | 1167 | .047 | |
| Target child’s sex is female | 3.00 | 1167 | .085 | |
| Wave | 0.49 | 2167 | .616 | |
| Treatment condition | 0.39 | 1167 | .533 | |
| Wave × treatment condition | 1.32 | 2167 | .271 | |
| Parent Behavior Checklist_nurturing | ||||
| Father’s age (log transformed) | 0.61 | 1167 | .434 | |
| Number of adults in HH | 0.37 | 1167 | .544 | |
| Father highest grade completed | 4.59 | 1167 | .034 | |
| Number of social network members (log transformed) | 0.23 | 1167 | .632 | |
| Target child’s sex is female | 0.88 | 1167 | .350 | |
| Wave | 0.44 | 2167 | .646 | |
| Treatment condition | 0.21 | 1167 | .645 | |
| Wave × treatment condition | 0.01 | 2167 | .987 | |
| Tolerance for Disagreement Score | ||||
| Father’s age (log transformed) | 5.23 | 1167 | .023 | |
| Number of adults in HH | 1.14 | 1167 | .288 | |
| Father highest grade completed | 2.85 | 1167 | .093 | |
| Number of social network members (log transformed) | 0.01 | 1167 | .942 | |
| Target child’s sex is female | 0.21 | 1167 | .647 | |
| Wave | 0.54 | 2167 | .585 | |
| Treatment condition | 0.54 | 1167 | .464 | |
| Wave × treatment condition | 0.23 | 2167 | .791 | |
| Personal Problem Solving Inventory_self-efficacy | ||||
| Father's age (log transformed) | 0.05 | 1167 | .828 | |
| Number of adults in HH | 2.37 | 1167 | .126 | |
| Father highest grade completed | 9.63 | 1167 | .002 | |
| Number of social network members (log transformed) | 0.07 | 1167 | .796 | |
| Target child’s sex is female | 0.14 | 1167 | .709 | |
| Wave | 1.72 | 2167 | .183 | |
| Treatment condition | 0.02 | 1167 | .897 | |
| Wave × Treatment Condition | 0.54 | 2167 | .583 | |
| Personal Problem Solving Inventory_skills | ||||
| Father’s age (log transformed) | 0.23 | 1167 | .635 | |
| Number of adults in HH | 0.66 | 1167 | .419 | |
| Father highest grade completed | 5.27 | 1167 | .023 | |
| Number of social network members (log transformed) | 0.04 | 1167 | .848 | |
| Target child’s sex is female | 0.49 | 1167 | .487 | |
| Wave | 1.99 | 2167 | .140 | |
| Treatment condition | 0.00 | 1167 | .998 | |
| Wave × treatment condition | 0.16 | 2167 | .851 | |
| Quality of Relationship Inventory_support | ||||
| Father’s age (log transformed) | 0.08 | 1167 | .777 | |
| Number of adults in HH | 0.58 | 1167 | .447 | |
| Father highest grade completed | 1.59 | 1167 | .208 | |
| Number of social network members (log transformed) | 0.83 | 1167 | .364 | |
| Target child’s sex is female | 0.32 | 1167 | .574 | |
| Wave | 0.32 | 2167 | .729 | |
| Treatment condition | 0.29 | 1167 | .593 | |
| Wave × treatment condition | 0.37 | 2167 | .693 | |
| Quality of Relationship Inventory_conflict | ||||
| Father’s age (log transformed) | 0.01 | 1167 | .937 | |
| Number of adults in HH | 0.14 | 1167 | .708 | |
| Father highest grade completed | 0.00 | 1167 | .971 | |
| Number of social network members (log transformed) | 0.00 | 1167 | .957 | |
| Target child’s sex is female | 0.01 | 1167 | .924 | |
| Wave | 1.77 | 2167 | .173 | |
| Treatment condition | 0.00 | 1167 | .993 | |
| Wave × treatment condition | 0.59 | 2167 | .557 | |
| Quality of Relationship Inventory_depth | ||||
| Father’s age (log transformed) | 0.63 | 1167 | .427 | |
| Number of adults in HH | 0.26 | 1167 | .609 | |
| Father highest grade completed | 0.87 | 1167 | .352 | |
| Number of social network members (log transformed) | 0.00 | 1167 | .944 | |
| Target child’s sex is female | 0.39 | 1167 | .536 | |
| Wave | 0.44 | 2167 | .647 | |
| Treatment condition | 2.03 | 1167 | .156 | |
| Wave × treatment condition | 0.39 | 2167 | .681 | |
| Behavior Assessment System for Children (BASC)_aggression | ||||
| Father's age (log transformed) | 0.53 | 1167 | .466 | |
| Number of adults in HH | 0.05 | 1167 | .820 | |
| Father highest grade completed | 1.21 | 1167 | .273 | |
| Number of social network members (log transformed) | 0.40 | 1167 | .526 | |
| Target child’s sex is female | 0.07 | 1167 | .798 | |
| Wave | 0.97 | 2167 | .381 | |
| Treatment condition | 1.51 | 1167 | .221 | |
| Wave × treatment condition | 0.95 | 2167 | .389 | |
| Behavior Assessment System for Children (BASC)_attention | ||||
| Father’s age (log transformed) | 0.39 | 1167 | .531 | |
| Number of adults in HH | 1.14 | 1167 | .288 | |
| Father highest grade completed | 1.62 | 1167 | .205 | |
| Number of social network members (log transformed) | 0.02 | 1167 | .888 | |
| Target child’s sex is female | 0.77 | 1167 | .382 | |
| Wave | 0.14 | 2167 | .866 | |
| Treatment condition | 0.88 | 1167 | .350 | |
| Wave × treatment condition | 0.17 | 2167 | .846 | |
| Behavior Assessment System for Children (BASC)_depression | ||||
| Father’s age (log transformed) | 0.04 | 1167 | .849 | |
| Number of adults in HH | 0.03 | 1167 | .865 | |
| Father highest grade completed | 1.14 | 1167 | .287 | |
| Number of social network members (log transformed) | 0.04 | 1167 | .845 | |
| Target child’s sex is female | 0.02 | 1167 | .885 | |
| Wave | 0.61 | 2167 | .542 | |
| Treatment condition | 0.02 | 1167 | .902 | |
| Wave × treatment condition | 0.14 | 2167 | .871 | |
| Behavior Assessment System for Children (BASC)_hyperactivity | ||||
| Father’s age (log transformed) | 0.46 | 1167 | .499 | |
| Number of adults in HH | 0.03 | 1167 | .870 | |
| Father highest grade completed | 1.58 | 1167 | .211 | |
| Number of social network members (log transformed) | 1.01 | 1167 | .317 | |
| Target child’s sex is female | 0.35 | 1167 | .554 | |
| Wave | 0.42 | 2167 | .657 | |
| Treatment condition | 0.00 | 1167 | .973 | |
| Wave × treatment condition | 0.01 | 2167 | .986 | |
Moderation Analyses
Analyses testing moderation of treatment effects by intervention participation yielded no significant interaction effects for any of the outcomes. Tables S5 and S6 in the Supplemental Material summarize intervention effects moderated by level of father participation and planned contrasts for moderation analyses.
Discussion
In spite of the high degree of satisfaction among participating fathers, our findings reveal that the BBTF intervention did not significantly impact father or child outcomes. Our endeavor to detect changes in child outcomes as a result of fatherhood intervention participation is seldom attempted. Even so, there are several potential reasons why our results did not meet hypothesized expectations—many of which are related to participant engagement. We discuss challenges associated with conducting intervention research with AA non-resident fathers, describe limitations, and offer recommendations for future research.
In light of the recognized importance of father involvement and the preponderance of AA fathers who do not live in the household with their biological children [13], it is important to address the question of engagement in fatherhood intervention research. We view our ability to screen 495 African American men, identify 251 eligible non-resident fathers, collect 192 baseline interviews, and randomize 178 non-resident African American fathers into the study as a successful step in engaging AA fathers [47]. Even so, we did not meet ongoing targets to enroll 20–30 fathers into each cohort (10–15 per allocated group). Study recruitment was influenced by our initial inclusion criteria, which required maternal consent to participate as data informant prior to fully enrolling fathers into the study. We amended this criterion after experiencing challenges contacting and enrolling mothers in the first three cohorts. The need to amend this inclusion criterion is an important reminder that among couples with fractured relationships, ongoing communication and contact can constrain fathers’ efforts to remain engaged in the lives of their children, and efforts to engage in preventive fatherhood interventions [8]. Fathers interested in bolstering their involvement with their children should not be stymied by maternal-related methodological constraints.
Societal, structural, and family barriers (e.g., structural racism, harsh policing, and potential discord with their child’s mother) can impinge upon AA non-resident fathers’ family relationships and fatherhood intervention engagement [48, 49]. Lemmons and Johnson [49] explore the intersections of race, economics ,and social policy as influencers on AA fatherhood. For example, structural racism has influenced employment opportunities and the current economic environment for AA men, forcing many to prioritize seeking and maintaining employment over preventive fatherhood interventions. Low socioeconomic status as reflected by the low-income and unemployed fathers in the current study can hinder fatherhood intervention engagement [46]. Although we provided monetary incentives in the amount of $50 at each data collection time point, the complexity of fathers’ lives may have outweighed the merits of our monetary incentive.
Future researchers focused on fatherhood interventions could consider alternative more flexible delivery modalities to overcome participation barriers or focus on a different subset of AA non-resident fathers. For example, virtual programming via Zoom, delivering intervention content through smartphone technology, collecting follow-up data virtually, and reminding fathers about upcoming sessions and completion of practice assignments could be implemented so as to not interfere with employment and other competing responsibilities [46].
Parent training research has been successful in connecting with maternal participants via child-focused venues that include schools and day care centers. However, organizational, community, or congregational spaces where AA men come together are limited. The barbershop has been proposed as a recruitment venue, but since it is a place of business, it may not be a practical or feasible location for intervention delivery across a diverse group of fathers. In fact, barber shops tend to attract younger fathers, and venues such as restaurants and hardware stores are more feasible for recruiting older fathers [50]. In our engagement approach, we attempted to recruit fathers across a broad array of community locations and employed recognized recruitment and retention strategies [19]. We also rotated our group locations between two areas of the city heavily populated by African Americans (westside and southside of the city), provided meals and transportation costs, and incentivized data collection at $50 per interview. Upon further reflection, it is possible that fathers without social connections to one intervention site and to each other may have been reticent to attend a preventive fatherhood intervention. Health care settings such as Project Brotherhood in Chicago that serve AA men have realized success in establishing trusting relationships that facilitate research participation [51]. In general, AA men may have more distal social connections to potential intervention sites and therefore, require culturally congruent information delivered by trusted providers [51].
Recruitment of fathers while they are expecting through prenatal providers offers some promise for recruitment by focusing on the prenatal triad, which includes mothers, the unborn child, and the father [52]. There could be some limitations with regard to targeting expectant fathers because men with older children could potentially be excluded. Such an approach would require focusing on a different subset of fathers such as fathers who are expectant could capitalize on the initial excitement and engagement of most fathers during pregnancy and early parenthood [53]. This option has the added benefit of engaging mothers who could also benefit from learning about the importance of father involvement to the long-term well-being of their children. For some couples with multiple competing demands, and difficult relationships, preventive intervention participation may also benefit from social support to aid in their transition to parenthood [9].
There were fathers who enrolled in the study who never attended a single group meeting. This phenomenon—pretreatment attrition [46]—is difficult to interpret. More research is needed on fathers’ paternal beliefs and attitudes [54] and motivation to participate in fatherhood interventions that could inform attendance and study retention. Strategies that engage fathers during recruitment to understand how the intervention aligns with their needs and identifies their expectations for content, process, and expected benefits could be helpful. It could also be useful to problem-solve potential obstacles prior to and throughout the study to proactively address attendance and attrition [46].
Motivational interviewing (MI) is a strategy that could facilitate early engagement and potentially sustain engagement for parents enrolled in parent training throughout the duration of the intervention [55]. Motivational interviewing works by supporting intrinsic motivation to change and increasing awareness of internal resources that can facilitate change [56]. MI is a client-focused non-confrontational approach that explores uncertainty about making change and yet is respectful of individuals’ independence; it works particularly well for high-risk individuals [57]. Preliminary findings from prior research conducted on MI in parenting interventions revealed that MI has successfully increased engagement with low-income diverse populations [58].
Finally, qualitative research that engages directly with non-resident fathers [11] can provide much-needed insight into the specific challenges that impede engagement and retention, as well as solutions for overcoming participation barriers. Considerable evidence supports the value of hearing the voices of fathers themselves, which can highlight their strengths as well as their shortcomings [59] and identify strategies to overcome lack of intervention engagement and promote research retention [60].
Limitations
Limitations worth noting in this study include the following. In light of low attendance in the allocated study groups, we were unable to determine whether BBTF is an effective intervention for supporting positive father and child outcomes. Further without additional insight from the fathers themselves, we do not know whether fathers made a conscious decision to sign up for the study and not attend or whether extenuating circumstances precluded their attendance. There were unique challenges in recruiting fathers into the study. Unlike recruitment for other groups of parents who frequently mainstream venues such as schools and daycare, we are limited by incomplete awareness of established locations for recruiting non-resident fathers. We are limited in our ability to analyze cross-informant (maternal and paternal data) because of low maternal participation rates. Finally low retention rates made longitudinal analysis an additional limitation to the study.
Conclusion
The importance of fatherhood intervention research and the advances made in developing and implementing culturally and contextually relevant fatherhood programs is well established. Even so, more research is needed to inform research methods, recruitment, and retention strategies. Based on lessons learned through the current study, we recommend that research investigators continue collaborating with AA non-resident fathers as knowledgeable allies in this work. Tailored engagement strategies, designed explicitly for this population, are needed in order to keep pace with the circumstances that impugn research participation. The field of fatherhood intervention research would be strengthened by ongoing examination of engagement from study conceptualization to actualization. Finally, agreements about standardizing data collection and reporting on research engagement in this population would allow for greater visualization of findings across research studies.
Supplementary Information
(DOCX 40 kb)
Acknowledgements
This research was funded by The National Institutes of Health/National Institute of Nursing Research Grant #2R01NR011182.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Yogman M, Garfield CF. Committee on Psychosocial Aspects of Child and Family Health. Fathers’ roles in the care and development of their children: the role of pediatricians. Pediatrics. 2016;138(1) 10.1542/peds.2016-1128. [DOI] [PubMed]
- 2.Livingston G. About one third of US children are living with an unmarried parent. Pew Research Center, April. 2018;27
- 3.Higgs E, Gomez-Vidal C, Austin MJ. Low-income nonresident fatherhood: a literature review with implications for practice and research. Fam Soc. 2018;99(2):110–120. doi: 10.1177/1044389418767826. [DOI] [Google Scholar]
- 4.Castillo J, Welch G, Sarver C. Fathering: the relationship between fathers’ residence, fathers’ sociodemographic characteristics, and father involvement. Matern Child Health J. 2011;15(8):1342–1349. doi: 10.1007/s10995-010-0684-6. [DOI] [PubMed] [Google Scholar]
- 5.Fagan J, Iglesias A. Father involvement program effects on fathers, father figures, and their head start children: a quasi-experimental study. Early Child Res Q. 1999;14(2):243–269. doi: 10.1016/S0885-2006(99)00008-3. [DOI] [Google Scholar]
- 6.Cheadle JE, Amato PR, King V. Patterns of nonresident father contact. Demography. 2010;47(1):205–225. doi: 10.1353/dem.0.0084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Davis RN, Caldwell CH, Clark SJ, Davis MM. Depressive symptoms in nonresident African American fathers and involvement with their sons. Pediatrics. 2009;124(6):1611–1618. doi: 10.1542/peds.2009-0718. [DOI] [PubMed] [Google Scholar]
- 8.Carlson MJ, McLanahan SS, Brooks-Gunn J. Coparenting and nonresident fathers’ involvement with young children after a nonmarital birth. Demography. 2008;45(2):461–488. doi: 10.1353/dem.0.0007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Castillo JT, Sarver CM. Nonresident fathers’ social networks: the relationship between social support and father involvement. Pers Relat. 2012;19(4):759–774. doi: 10.1111/j.1475-6811.2011.01391.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Paulson JF, Dauber SE, Leiferman JA. Parental depression, relationship quality, and nonresident father involvement with their infants. J Fam Issues. 2011;32(4):528–549. doi: 10.1177/0192513X10388733. [DOI] [Google Scholar]
- 11.Coates EE, Phares V. Predictors of paternal involvement among nonresidential, Black fathers from low-income neighborhoods. Psychol Men Masculinity. 2014;47(1):205–225. [Google Scholar]
- 12.Henry JB, Julion WA, Bounds DT, Sumo JN. Fatherhood matters: an integrative review of fatherhood intervention research. The Journal of School Nursing. 2020;36(1):19–32. [DOI] [PubMed]
- 13.Adamsons K, Johnson SK. An updated and expanded meta-analysis of nonresident fathering and child well-being. J Fam Psychol. 2013;27(4):589–599. doi: 10.1037/a0033786. [DOI] [PubMed] [Google Scholar]
- 14.Knox V, Cowan PA, Pape Cowan C, Bildner E. Policies that strengthen fatherhood and family relationships: what do we know and what do we need to know? Ann Am Acad Pol Soc Sci. 2011;635(1):216–239. doi: 10.1177/0002716210394769. [DOI] [Google Scholar]
- 15.Cowan PA, Cowan CP, Pruett MK, Pruett K, Wong JJ. Promoting fathers’ engagement with children: preventive interventions for low-income families. J Marriage Fam Couns. 2009;71(3):663–679. doi: 10.1111/j.1741-3737.2009.00625.x. [DOI] [Google Scholar]
- 16.Cowan PA, Cowan CP, Pruett MK, Pruett K, Gillette P. Evaluating a couples group to enhance father involvement in low-income families using a benchmark comparison. Fam Relat. 2014;63(3):356–370. doi: 10.1111/fare.12072. [DOI] [Google Scholar]
- 17.Rienks SL, Wadsworth ME, Markman HJ, Einhorn L, Moran EE. Father involvement in urban low-income fathers: baseline associations and changes resulting from preventive intervention. Fam Relat. 2011;60(2):191–204. doi: 10.1111/j.1741-3729.2010.00642.x. [DOI] [Google Scholar]
- 18.Bayley J, Wallace LM, Choudhry K. Fathers and parenting programmes: barriers and best practice. Community Pract. 2009;82(4):28–31. [PubMed] [Google Scholar]
- 19.Stahlschmidt MJ, Threlfall J, Seay KD, Lewis EM, Kohl PL. Recruiting fathers to parenting programs: advice from dads and fatherhood program providers. Child Youth Serv Rev. 2013;35(10):1734–1741. doi: 10.1016/j.childyouth.2013.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Panter-Brick C, Burgess A, Eggerman M, McAllister F, Pruett K, Leckman JF. Practitioner review: engaging fathers--recommendations for a game change in parenting interventions based on a systematic review of the global evidence. J Child Psychol Psychiatry. 2014;55(11):1187–1212. doi: 10.1111/jcpp.12280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Block S, Brown CA, Barretti LM, Walker E, Yudt M, Fretz R. A mixed-method assessment of a parenting program for incarcerated fathers. Journal of Correctional Education (1974-) 2014;65(1):50–67. [Google Scholar]
- 22.DeGarmo DS, Jones J, Rains LA. A pilot study evaluation of Marte Meo for divorced fathers. J Fam Ther. 2019;41(2):232–250. doi: 10.1111/1467-6427.12221. [DOI] [Google Scholar]
- 23.Ferguson S, Morley P. Improving engagement in the role of father for homeless, noncustodial fathers: a program evaluation. J Poverty. 2011;15(2):206–225. doi: 10.1080/10875549.2011.563175. [DOI] [Google Scholar]
- 24.Bunston W. “What about the fathers?” Bringing “Dads on BoardTM” with their infants and toddlers following violence. J Fam Stud. 2013;19(1):70–79. doi: 10.5172/jfs.2013.19.1.70. [DOI] [Google Scholar]
- 25.Houghton LJ, O’Dwyer M, Foweather L, Watson P, Alford S, Knowles ZR. An impact and feasibility evaluation of a six-week (nine hour) active play intervention on fathers’ engagement with their preschool children: a feasibility study. Early Child Dev Care. 2015;185(2):244–266. doi: 10.1080/03004430.2014.919495. [DOI] [Google Scholar]
- 26.Concha M, Villar ME, Tafur-Salgado R, Ibanez S, Azevedo L. Fatherhood education from a cultural perspective: evolving roles and identities after a fatherhood intervention for Latinos in South Florida. Journal of Latinos and Education. 2016;15(3):170–9.
- 27.Julion WA, Breitenstein SM, Waddell D. Fatherhood intervention development in collaboration with African American non‐resident fathers. Research in Nursing & Health. 2012;35(5):490–506. [DOI] [PMC free article] [PubMed]
- 28.Lyons AC, Scherpf E. Moving from unbanked to banked: Evidence from the Money Smart program. FINANCIAL SERVICES REVIEW-GREENWICH. 2004;13(3):215–232. [Google Scholar]
- 29.Resnick B, Inguito P, Orwig D, Yahiro JY, Hawkes W, Werner M, Zimmerman S, Magaziner J. Treatment fidelity in behavior change research: a case example. Nurs Res. 2005;54(2):139–143. doi: 10.1097/00006199-200503000-00010. [DOI] [PubMed] [Google Scholar]
- 30.Breitenstein SM, Fogg L, Garvey C, Hill C, Resnick B, Gross D. Measuring implementation fidelity in a community-based parenting intervention. Nursing Research. 2010;59(3):158. [DOI] [PMC free article] [PubMed]
- 31.Sarason IG, Sarason BR, Shearin EN. A brief measure of social support: practical and theoretical implications. Journal of social and. Published online 1987. https://journals.sagepub.com/doi/abs/10.1177/0265407587044007?casa_token=RxM_EAQkcmsAAAAA:IRqk_9ZIFadp63QuJ75f0bTkC-fnKAy0mZxMgC15lYC-hLP61RA1smvtUemqC4Rg_j6DCRdYI2mHvg
- 32.Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. doi: 10.1177/014662167700100306. [DOI] [Google Scholar]
- 33.Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi: 10.2307/2136404. [DOI] [PubMed] [Google Scholar]
- 34.Taylor J, Tomasic MN. Taylor’s measures of dysphoria, anxiety, anger, and self esteem. In Jones, R. (Ed.). Handbook of Tests and Measurements for Black Populations (Vol. 2). Hampton (VA): Cobb & Henry Publishers 1996;2:297–9.
- 35.Teven JJ, McCroskey JC, Richmond VP. Measurement of tolerance for disagreement. Commun Res Rep. 1998;15(2):209–217. doi: 10.1080/08824099809362115. [DOI] [Google Scholar]
- 36.Maydeu-Olivares A, D’Zurilla TJ. The factor structure of the problem solving inventory. Eur J Psychol Assess. 1997;13(3):206–215. doi: 10.1027/1015-5759.13.3.206. [DOI] [Google Scholar]
- 37.Pierce GR, Sarason IG, Sarason BR, Solky-Butzel JA, Nagle LC. Assessing the quality of personal relationships. J Soc Pers Relat. 1997;14(3):339–356. doi: 10.1177/0265407597143004. [DOI] [Google Scholar]
- 38.Fox RA. Development of an instrument to measure the behaviors and expectations of parents of young children. J Pediatr Psychol. 1992;17(2):231–239. doi: 10.1093/jpepsy/17.2.231. [DOI] [PubMed] [Google Scholar]
- 39.Johnston C, Mash EJ. A measure of parenting satisfaction and efficacy. J Clin Child Psychol. 1989;18(2):167–175. doi: 10.1207/s15374424jccp1802_8. [DOI] [Google Scholar]
- 40.Julion WA, Sumo JN, Bounds DT. A tripartite model for recruiting African‐Americans into fatherhood intervention research. Public Health Nursing. 2018;35(5):420–426. [DOI] [PMC free article] [PubMed]
- 41.Reichman NE, Teitler JO, Garfinkel I, McLanahan SS. Fragile families: sample and design. Child Youth Serv Rev. 2001;23(4):303–326. doi: 10.1016/S0190-7409(01)00141-4. [DOI] [Google Scholar]
- 42.Reynolds CR, Kamphaus RW, Vannest KJ. BASC3: behavior assessment system for children. PscyhCorp; 2015.
- 43.van Buuren S. Multiple imputation of discrete and continuous data by fully conditional specification. Stat Methods Med Res. 2007;16(3):219–242. doi: 10.1177/0962280206074463. [DOI] [PubMed] [Google Scholar]
- 44.SAS Institute Inc. (2019). SAS® 9.4 and SAS® Viya® 3.3 Programming Documentation, SAS Institute Inc, Cary, NC.
- 45.Eisner M, Meidert U. Stages of parental engagement in a universal parent training program. J Prim Prev. 2011;32(2):83–93. doi: 10.1007/s10935-011-0238-8. [DOI] [PubMed] [Google Scholar]
- 46.Chacko A, Jensen SA, Lowry LS, Cornwell M, Chimklis A, Chan E, Lee D, Pulgarin B. Engagement in behavioral parent training: review of the literature and implications for practice. Clin Child Fam Psychol Rev. 2016;19(3):204–215. doi: 10.1007/s10567-016-0205-2. [DOI] [PubMed] [Google Scholar]
- 47.Julion WA, Sumo JN, Bounds DT. A tripartite model for recruiting African‐Americans into fatherhood intervention research. Public Health Nursing. 2018;35(5):420–426. [DOI] [PMC free article] [PubMed]
- 48.Watkins DC, Walker RL, Griffith DM. A meta-study of black male mental health and well-being. J Black Psychol. 2010;36(3):303–330. doi: 10.1177/0095798409353756. [DOI] [Google Scholar]
- 49.Lemmons BP, Johnson WE. Game changers: a critical race theory analysis of the economic, social, and political factors impacting black fatherhood and family formation. Soc Work Public Health. 2019;34(1):86–101. 10.1080/19371918.2018.1562406. [DOI] [PubMed]
- 50.Moore N, Wright M, Gipson J, Jordan G, Harsh M, Reed D, et al. A survey of African American men in Chicago barbershops: implications for the effectiveness of the barbershop model in the health promotion of African American men. J Community Health. 2016;41(4):772–9. [DOI] [PubMed]
- 51.Murray M, Campbell C, Kendall L, Whitt-Glover MC, Watson KS. Perspectives from project brotherhood: facilitating engagement of African American Men in research. Prog Community Health Partnersh. 2019;13(5):137–142. doi: 10.1353/cpr.2019.0047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Varga S, Mackert M, Mandell DJ. The prenatal triad: The importance of provider-patient communication with expectant fathers throughout the prenatal care process. Patient Educ Couns Published online November. 2020;6 10.1016/j.pec.2020.11.005. [DOI] [PubMed]
- 53.Lee JY, Knauer HA, Lee SJ, MacEachern MP, Garfield CF. Father-inclusive perinatal parent education programs: a systematic review. Pediatrics. 2018;142(1) 10.1542/peds.2018-0437. [DOI] [PubMed]
- 54.Volker J, Gibson C. Paternal involvement: A review of the factors influencing father involvement and outcomes. TCNJ Journal of Student Scholarship. 2014;15:1–8. [Google Scholar]
- 55.Nock MK, Kazdin AE. Randomized controlled trial of a brief intervention for increasing participation in parent management training. J Consult Clin Psychol. 2005;73(5):872–879. doi: 10.1037/0022-006X.73.5.872. [DOI] [PubMed] [Google Scholar]
- 56.Arkowitz H, Miller WR, Rollnick S. Motivational interviewing in the treatment of psychological problems. Second Edition: Guilford Publications; 2015. [Google Scholar]
- 57.Shepard S, Armstrong LM, Silver RB, Berger R, Seifer R. Embedding the family check-up and evidence-based parenting programmes in Head Start to increase parent engagement and reduce conduct problems in young children. Adv School Ment Health Promot. 2012;5(3):194–207. doi: 10.1080/1754730X.2012.707432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Stormshak EA, De Garmo D, Garbacz SA, LL MI, Caruthers A. Using motivational interviewing to improve parenting skills and prevent problem behavior during the transition to kindergarten. Prev Sci. Published online February. 2020;8 10.1007/s11121-020-01102-w. [DOI] [PMC free article] [PubMed]
- 59.Stover CS, Morgos D. Fatherhood and intimate partner violence: bringing the parenting role into intervention strategies. Prof Psychol Res Pr. 2013;44(4):247–256. doi: 10.1037/a0031837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Smith TK, Tandon SD, Bair-Merritt MH, Hanson JL. Parenting Needs of Urban, African American Fathers. Am J Mens Health. 2015;9(4):317–331. doi: 10.1177/1557988314545380. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX 40 kb)