

Abstract
The coronavirus disease (COVID-19) pandemic has led to dramatic changes in quality of life, bringing to the forefront of the debate the question of planning and design of pandemic-resilient cities. Using quasi-longitudinal survey data (via a social media campaign) and geospatial data from Greek cities, we evaluate changes in health and well-being during COVID-19 compared to the pre-COVID-19 period, and then explore in detail how specific built environment characteristics in Athens and Thessaloniki relate to health and well-being before and during COVID-19. Results suggest that overall health, life satisfaction, happiness, personal relationships satisfaction, leisure satisfaction, satisfaction with income, and satisfaction with vacations all decreased during COVID-19, while anxiety and back pain increased during COVID-19. The role of the urban built environment in health and well-being was found to differ considerably for the COVID-19 period compared to pre-COVID-19. Proximity to large parks, proximity to numerous local facilities, lower neighborhood density, living further from the city center, and living in a larger dwelling were associated with better health and well-being outcomes during COVID-19. Urban planning and relevant policies that cities adopt should carefully focus on mitigating implications for critical issues such as the quest for sustainable urban development and city forms.
Keywords: Coronavirus disease (COVID-19) pandemic, Compact city, City planning, Quality of life, Urban built environment, Subjective well-being
1. Introduction
It has been well-acknowledged that health and well-being have declined due to the coronavirus disease (COVID-19) pandemic in many countries worldwide (Fiorillo & Gorwood, 2020; Moreno et al., 2020). The COVID-19 pandemic and the related measures to prevent the spread of the disease have caused, among others, stress, anxiety, confusion, anger, depression, food insecurity, unemployment, and loss of economic activity (Brooks et al., 2020; Li et al., 2020; Patrick et al., 2020; Rogowska et al., 2020; Skapinakis et al., 2020; Vatavali et al., 2020; White & Van Der Boor, 2020).
Cities and urban planning can contribute to health and well-being in a variety of ways (Giles-Corti et al., 2016; Hamidi, Ewing, Tatalovich, Grace, & Berrigan, 2018; Litman, 2020b; Mouratidis, 2019a; Stevenson et al., 2016; Wang & Wang, 2016). Recent research has started to explore the links between cities, urban planning, and COVID-19 (Connolly et al., 2020; Hamidi et al., 2020; Honey-Rosés et al., 2020; Litman, 2020a; Sharifi & Khavarian-Garmsir, 2020). However, as the pandemic is still an on-going phenomenon, the role of cities and their built environment characteristics in health and well-being during COVID-19 remains an open question that requires sufficient empirical documentation from a variety of urban environments.
The COVID-19 pandemic has been characterized as the worst health crisis in a century having triggered the worst economic prospects since the Great Depression (UN Habitat, 2020). Historically speaking, urban planning emerged as a response to a series of crises, among which hygiene crises, health, and epidemics played a crucial role (Knox & McKarthy, 2013). Hygeia, the Greek word for health and well-being, was at the heart of modern town planning and many of the utopian planning ideas. Mumford points out in his seminal book The City in History “the counter movement on hygiene provided the most positive contributions to town planning during the nineteenth century” (Mumford, 1961, p. 544). Twentieth-century city planning as an intellectual and professional movement essentially represented a reaction to the “evils” of the nineteenth century, with people's health being one of the more severe consequences. Key urban planning concepts and ideas stemming from the Founders of the early 20th century, and often re-echoed and recycled throughout the contemporary planning history, focused on the ever-worsening urban problems such as urban health crises and health inequalities, unhealthy housing and urban environments, inadequate open spaces, inefficient land use and transportation etc. (Hall, 1988; Mell & Whitten, 2021). The major urban planning questions such as urban densities, urban form and the question of suburban versus compact development, as well as the quality of open and green public spaces have always been directly or indirectly related to the question of public health. Thus, public health was, explicitly or implicitly, at the heart of seeking the ideal urban form and of incorporating the advantages of both built-up and open space in urban growth patterns.
The search for urban sustainability in the past decades gave prominence to planning models and responses that build on the long-term ability of the urban system to reproduce itself. This search enriched some of the most classical urban planning issues, such as urban form, density, integrated land-use transport planning, with new content, connecting them to the issues of environmental and climate change crisis (Yiannakou, 2017). As both urban planning and relevant policies, applied by various cities, paid special attention to the quality of the compact cities and their revitalization, a re-urbanization trend has been monitored during recent years contrary to the decline of the inner-city core which was a common phenomenon in previous decades (Dembski et al., 2019). Many European cities through “green” and other sustainability solutions rediscovered what Hall called “the lost art of urbanism” (Hall, 2013). This shift in favor of urbanity, and therefore of the core compact city, targeted regeneration that improved the quality of urban life and has been characterized as a striking success of urban policy (Dembski et al., 2019).
In a period of ever-increasing rates of urbanization and rapid growth of cities in terms of numbers and size, the current health crisis, with characteristics of another mega-crisis, has influenced people dramatically as well as city routines, and, in a sense, the enduring reality of our social nature (Christakis, 2020). Staying home as a protection from the pandemic practically means staying within the boundaries of a property and its immediate surrounding built-up or natural environment. Proximity and accessibility to healthcare services proved to be critical for timely healthcare provision especially for vulnerable groups such as older adults (Guida & Carpentieri, 2021). Generally speaking, cities have always been and still are considered crucial locations for the transmission of infectious diseases. Early findings from metropolitan counties in the United States showed that connectivity through economic, social, and commuting relationships mattered more than density in the spread of the COVID-19 pandemic (Hamidi et al., 2020). Other research has shown that, due to higher connectedness of denser locations, population density appeared to have affected the impact of COVID-19 only through the timing of outbreaks and not through the rate of subsequent spread (Carozzi et al., 2020). Yet, concerns about some of the classical planning questions, such as lower versus higher density built-up environments or suburban versus compact urban forms, came to the fore once again in the light of the current mega health crisis. Cities represent the physical space of clusters of humans and their interaction and transaction in pursuit of wealth and welfare (Lai et al., 2020). Measures, such as keeping safe distances from other people, meant drastically new routines, which practically questioned the “limits” of urbanity and the availability of open and green public spaces within compact cities against the qualities of living within suburban built-up environments with much lower densities surrounded by natural settings. Close physical proximity, the basis of urbanism – economically, socially, and culturally speaking – has turned to be the opposite of “staying safe” to diminish the risk for individual as well as public health. Experts’ recommendations and public regulations for social distancing were measures that most – if not all – countries undertook to control the spread of the pandemic. These regulations imposed limitations to the proximity of people, a prominent urban factor. Thus, the pandemic turned to also be a cultural challenge and not merely a public health crisis (Davy, 2020).
On the other hand, findings have shown that during lockdowns, cities have been used more for recreation, play, exercise, and pedestrian movement, especially in neighborhoods outside the city center, while walking and cycling became essential forms of mobility (Gehl, 2020). Accordingly, urban open and green public spaces became increasingly important. In fact, lockdown measures sparked interest in some of the more important aspects of sustainable urban planning: open and green spaces as necessary spaces for health and well-being. Social distancing reduced the distance of visited urban green space making thus clear the need for accessible urban green space within the neighborhood radius (Gehl, 2020; Ugolini et al., 2020). Α return to the urban neighborhood as a locus of multiple human activities was the other notable change in the city routine and was observed through multiple ways from journalistic reports in local newspapers to numerous relevant posts in the social media.
Having only just one year of scientific knowledge with regard to the current pandemic, mainly on the health aspects and less on the wider effects or interrelations with the city environments, this paper attempts to contribute to filling the void in knowledge on how cities and built environment characteristics contributed to health and well-being during COVID-19. In early debates and research evidence, some built environment characteristics have been highlighted as fundamental for their potential contribution to health and well-being during COVID-19. These were urban density, public transport, access to facilities, green space, and housing. Urban density has not only been widely debated for its contribution or non-contribution to virus transmission (AbouKorin et al., 2021), but it has also been seen as a key feature during the pandemic as it influences, to a large extent, several other built environment characteristics. For example, denser urban areas can enable better, more frequent public transport services, easier access to facilities, while they are typically characterized by limited green space (especially in the form of private gardens) and by apartment blocks (and not e.g. detached housing) (Mouratidis & Poortinga, 2020; Næss, 2019). Public transport, access to facilities, green space, and housing may contribute to health and well-being via different pathways (Kent & Thompson, 2014; Mouratidis, 2021; Pfeiffer & Cloutier, 2016) but these pathways or their importance seem to have changed during COVID-19. Public transport might have been less safe to use during the COVID-19 pandemic because its enclosed space and the difficulty to maintain social distancing (Zheng et al., 2020) and its use was reduced more than the use of other travel modes (Bucsky, 2020; Jenelius & Cebecauer, 2020; Zhang et al., 2021). Residents who relied on public transport and who had to continue to travel (e.g. to work) during the pandemic might have experienced risk of infection but also stress and other negative feelings while traveling (Shamshiripour et al., 2020). Local facilities (e.g. shops, education, recreation, healthcare) that remained open during the pandemic have allowed residents to participate in activities but also to have access to healthcare services when necessary (Guida & Carpentieri, 2021; Hamidi et al., 2020; Litman, 2020a). Easy access to local facilities typical for mixed-use neighborhoods have also facilitated walking activity during the pandemic (Shaer, Rezaei, Moghani Rahimi, & Shaer, 2021). Therefore, via these different pathways, accessibility to local facilities could have contributed to health and well-being during COVID-19. Green space (including both public and private green space) has been considered particularly important for mitigating the negative impacts of COVID-19 on health and well-being by offering emotional and mental health benefits and a safe open space for activity participation (Douglas et al., 2020; Poortinga et al., 2021; Shoari et al., 2020; Ugolini et al., 2020; Xie et al., 2020). The role of housing has also been highlighted during COVID-19. Overcrowded dwellings may have contributed to more infections since social distances and quarantines are more difficult to maintain in tighter spaces (Hu et al., 2021). Moreover, as people spent more time and performed more daily-life activities in their dwelling during the pandemic, larger dwellings were likely more functional and more pleasant contributing to better health and well-being outcomes (Amerio et al., 2020).
The paper investigates the relationships between cities, health, and well-being before and during COVID-19 using geospatial measures of the urban built environment in combination with quasi-longitudinal data on health and well-being. We address two research questions: (1) How have measures of self-reported health and well-being changed during COVID-19 in comparison with the pre-COVID-19 period? (2) How do built environment characteristics relate to health and well-being before and during COVID-19? The study is based on geospatial data and quasi-longitudinal data from a questionnaire survey carried out all over Greece in April-May 2020. The analysis on cities, health, and well-being focuses on the metropolitan areas of Athens and Thessaloniki. In this paper, “health and well-being” will refer to self-reported measures of health (here measured with overall health, satisfaction with health, anxiety, headache, and back pain) and well-being (here measured with life satisfaction, happiness, personal relationships satisfaction, leisure satisfaction, satisfaction with vacations, and satisfaction with income).
2. Data and methods
2.1. Data sources
Data were collected via a population-based questionnaire survey (Appendix A) and analysis with geographic information systems (GIS). Data collection was carried out in Greece with a particular focus on the metropolitan areas of Athens, the country's capital, and Thessaloniki, the country's second most populous city. As of the 2011 census, the metropolitan area of Athens had a population of approximately 3.8 million residents and the metropolitan area of Thessaloniki had a population of 1 million residents. Fig. 1 shows approximate residential locations of the survey participants living in the metropolitan areas of Athens and Thessaloniki.
Fig. 1.

Maps of the metropolitan areas of Athens (left) and Thessaloniki (right) showing approximate residential locations of survey participants.
The survey was carried out from the end of April until the end of May 2020, a period which coincided with the first round of lockdown measures in Greece due to the COVID-19 pandemic. The final sample of the survey consists of 1201 adult residents of Greece, aged 18-79 years. Among the sample 489 were residents of the Athens metropolitan area, 523 were residents of the Thessaloniki metropolitan area, 185 were residents of other parts of Greece, while 4 were residents of Greece who did not wish to state their place of residence.
The survey distribution method was based on a campaign in social media and social networks. An invitation to participate in an online survey together with a weblink to the survey were distributed. The campaign included four main distribution channels: (1) social media campaign in Facebook groups, (2) snowball sampling via social networks, (3) project webpage, and (4) article in an online magazine focusing on city issues. Most survey participants were recruited via Facebook groups (N = 762), followed by those recruited by snowball sampling (N = 404). The rest of the participants (N = 35) were recruited via the project webpage and the online article which redirected to the project webpage. For the social media campaign in Facebook groups, the survey invitation was posted in 112 Facebook groups of Athens, 77 Facebook groups of Thessaloniki, and 27 general Facebook groups in Greece. Various residents’ Facebook groups of all neighborhoods in Athens and Thessaloniki were covered. Moreover, the survey invitation was posted in a wide range of Facebook groups that focused on topics including daily news, sports, culture, politics, urban life, travel, history, philosophy, psychology, disabled citizens, parenthood, and childcare. Snowball sampling was performed using a wide range of social networks of the authors. Colleagues were excluded from this process to reduce biases. The survey invitation was distributed to social networks in Greece who in turn distributed it to their own social networks. The distribution was conducted mainly via email and Facebook.
The survey distribution resulted in a sample that covers residential locations (requested with relevant questions in the survey) all over Greece, but mainly the metropolitan areas of Athens and Thessaloniki, where the analysis on the built environment focuses on. As seen in Fig. 1, a high representation of diverse urban forms (high density, medium density, low density), locations (urban, suburban, peripheral, rural), and socioeconomic profiles (richer versus poorer areas) was achieved in these two metropolitan areas. The survey was pilot-tested and revised before its final distribution. No monetary or other incentives were offered to study participants. The invitation letter and the survey questions were only in the Greek language, so this might have hindered the participation of residents who did not speak Greek. As survey participants were not selected from a sampling frame, other sources of biases might be relevant for the study's sample. Table 1 presents the sample's sociodemographic characteristics. The sample is subject to biases common in questionnaire surveys including higher representation of well-educated citizens and lower representation of immigrants. These discrepancies from the population are similar for the samples of Athens, Thessaloniki, and other cities in Greece. However, because the sample size from the other cities in Greece is small, the analysis on how the built environment relates to health and well-being is performed only for Athens and Thessaloniki.
Table 1.
Descriptive statistics of independent variables.
| Variables | N | Min/Max | Athens (N = 489) |
Thessaloniki (N = 523) |
Other parts of Greece (N = 185) |
|||
|---|---|---|---|---|---|---|---|---|
| Mean | s.d. | Mean | s.d. | Mean | s.d. | |||
| Built environment | ||||||||
| Distance to city center (km) | 999 | 0.2/56.6 | 9.39 | (6.72) | 8.56 | (8.68) | N/A | N/A |
| Neighborhood density (persons/ha within 1 km radius) | 1159 | 1/247 | 110.23 | (63.39) | 98.06 | (61.93) | 39.58 | (21.06) |
| Public transport (number of stops within 1 km radius) | 1158 | 0/410 | 149.71 | (72.04) | 31.07 | (26.59) | 12.33 | (27.23) |
| Local facilities (number of facilities within 1 km radius) | 1158 | 0/2278 | 293.18 | (358.08) | 351.70 | (388.78) | 150.99 | (185.03) |
| Park area (square meters within 1 km radius) | 1128 | 499/1094705 | 222,590.06 | (205,995.87) | 118,976.33 | (88,829.30) | 102,899.51 | (92,776.75) |
| Tree cover (% within 1 km radius) | 1158 | 0/28.98 | 1.00 | (2.63) | 0.84 | (2.25) | 1.22 | (2.25) |
| Apartment (1 = apartment; 0 = other) | 1197 | 0/1 | 0.66 | (0.47) | 0.73 | (0.44) | 0.56 | (0.50) |
| Dwelling size (square meters) | 1177 | 11/800 | 110.00 | (64.90) | 105.00 | (52.03) | 104.62 | (53.04) |
| Area socioeconomic status | ||||||||
| Mean annual household income (Euros) | 1173 | 7128/24574 | 16,350.40 | (3762.32) | 13,444.58 | (1507.165) | 11,263.51 | (1205.00) |
| Immigrant residents (%) | 1173 | 0.7/17.4 | 9.54 | (4.96) | 6.26 | (1.89) | 4.66 | (1.71) |
| Unemployment rate (%) | 1173 | 2.1/15.4 | 5.14 | (1.03) | 6.22 | (0.85) | 5.94 | (1.37) |
| Individual sociodemographic variables | ||||||||
| Age (years) | 1200 | 18/79 | 43.81 | (12.81) | 41.74 | (13.85) | 39.21 | (14.04) |
| Female | 1201 | 0/1 | 0.52 | (0.50) | 0.56 | (0.50) | 0.65 | (0.48) |
| Unemployed | 1201 | 0/1 | 0.19 | (0.40) | 0.21 | (0.41) | 0.11 | (0.32) |
| Living with partner/spouse | 1201 | 0/1 | 0.63 | (0.48) | 0.62 | (0.49) | 0.54 | (0.50) |
| Immigrant | 1201 | 0/1 | 0.01 | (0.08) | 0.02 | (0.12) | 0.01 | (0.07) |
| Income (personal net monthly income in Euros) | 1201 | 0/4250 | 1336.20 | (987.31) | 1062.14 | (855.11) | 1014.86 | (910.15) |
| College degree or higher | 1201 | 0/1 | 0.73 | (0.45) | 0.70 | (0.46) | 0.68 | (0.47) |
| Household with children | 1201 | 0/1 | 0.44 | (0.50) | 0.41 | (0.49) | 0.39 | (0.49) |
| Religious | 1196 | 0/1 | 0.52 | (0.50) | 0.47 | (0.50) | 0.58 | (0.49) |
| Disability (or longstanding health issue) | 1201 | 0/1 | 0.15 | (0.35) | 0.14 | (0.34) | 0.19 | (0.39) |
Notes: N/A = Not applicable. Median income for Athens sample = 1100 Euros. Median income for Thessaloniki sample = 900 Euros. Median income for sample in other parts of Greece = 900 Euros.
2.2. Variable descriptions
Built environment characteristics are presented in Table 1. These characteristics were selected for their potential contribution to health and well-being during COVID-19, as explained in Section 1. Distance to city center and neighborhood density are measures relevant to urban density; with distance to city center capturing residential locations in relation to the city center and thus being relevant to overall urban density, while neighborhood density is a measure of local-level density (Næss, 2019). Access to public transport and to local facilities were measured to analyze the role of public transport and local facilities respectively. To capture the role of green space we used two variables: park area and tree cover. Park area captures public green space while tree cover captures any type of area with the presence of trees. To assess the role of housing, we used two variables: dwelling type and dwelling size. Dwelling type is relevant not only to interior living space but also to exterior spaces such as private garden or balcony since detached houses or duplexes are more likely to have a private garden than apartments.
Two characteristics were captured via the survey while the rest of the data were obtained with analysis in GIS. The type of residence that the respondent lives in was asked in the survey and was later coded for this analysis as: 1 = apartment and 0 = other (e.g. detached house, duplex). The size of the respondents’ dwelling in square meters was also asked in the survey. The GIS analysis for the rest of the built environment characteristics was conducted based on the residential location that participants filled in when completing the survey. Participants were asked to fill in the residential address. Since some people may not be comfortable with sharing such information, this question was optional. The majority of participants, however, filled in this information; N = 832 filled in their full address, while N = 354 filled in only their postal code. The residential locations were first georeferenced and then GIS analysis was conducted as described below. The following built environment characteristics were measured: distance to city center, neighborhood density, public transport, local facilities, park area, and tree cover. These characteristics were measured for each survey participant individually. Distance to city center was measured only for residents of the metropolitan areas of Athens and Thessaloniki and assessed the location of each participant's residence in relation to the city center of Athens or Thessaloniki. It was calculated in kilometers along walking routes. Neighborhood density was measured in persons per hectare as the population density within a 1000 m radius from each participant's residence using data from high-resolution population density maps (FCL & CIESIN, 2020). Public transport accessibility was measured as the number of public transport stops (bus, tram, metro, train, trolley bus) within a 1000 m radius from each participant's residence. OpenStreetMap data were used for this analysis. Local facilities were measured as the number of facilities within a 1000 m radius from each participant's residence. This analysis used data from OpenStreetMap on the “amenity” category. All different types of facilities in this category were included in the analysis, for example: school, cinema, theater, post office, café, restaurant, bank, library, and hospital. Park area was measured as the total area of parks within a 1000 m radius from each participant's residence. This variable was measured in meters and was based on OpenStreetMap data. Tree cover was calculated as the mean percentage of tree canopy cover within a 1000 m radius from each participant's residence using updated 2019 data by Hansen et al. (2013).
Area socioeconomic status indicators are presented in Table 1. These indicators were obtained with analysis in GIS using geospatial data processed by Kalogirou (2010) based on census data from Hellenic Statistical Authority (EL.STAT.) and the General Secretariat of Information Systems in Greece. Area refers to the municipality that each respondent's residence was located in. Area socioeconomic status was measured with three indicators: mean annual household income in Euros, percentage of people who do not have Greek citizenship, and unemployment rate.
Table 1 shows descriptive statistics for individual sociodemographic variables, measured via the survey. Sociodemographic variables included: age, gender, cohabitation status (living with partner or spouse), citizenship, household income, presence of children in the household, employment status, religiosity, and level of education. Having a disability or important health issue is used as a control variable in the study and was measured with the question: “Are you hampered in your daily activities in any way by any longstanding illness, or disability, infirmity or mental health problem?”
Quasi-longitudinal data on health and well-being were obtained via the survey (Table 2 ). For the questions on health and well-being, the following guidelines were given to participants: “Consider your life during the coronavirus pandemic (COVID-19) (During COVID-19). Also consider your life right before the COVID-19 pandemic (Before COVID-19).” All variables on health and well-being were evaluated for both “before COVID-19” and “during COVID-19”. Measurement of health and well-being is largely based on guidelines by OECD (2013) and the European Social Survey (2012). Single-item measures of well-being were used. These are stable and reliable (Lucas & Brent Donnellan, 2012). Participants were asked: “How satisfied are/were you with your...?” on a scale from “extremely dissatisfied” (0) to “extremely satisfied” (10). The question was asked in order to evaluate “life as a whole”, “personal relationships”, “leisure activities”, “health status”, “vacations”, and “personal income”. Overall health (self-reported health) was assessed by asking participants to describe their general health on a scale from “extremely poor” (0) to “extremely good” (10). Participants were also asked to evaluate the frequency of feelings of happiness and anxiety on a scale from “very rarely or never” (1) to “very often or always” (5). The same scale was also used to evaluate the frequency of headache and back pain.
Table 2.
Descriptive statistics of dependent variables.
| Variables | N | Min/Max | Athens (N = 489) |
Thessaloniki (N = 523) |
Other parts of Greece (N = 185) |
|||
|---|---|---|---|---|---|---|---|---|
| Mean | s.d. | Mean | s.d. | Mean | s.d. | |||
| Health and well-being | ||||||||
| Life satisfaction before COVID-19 | 1201 | 0/10 | 7.26 | (1.68) | 7.35 | (1.71) | 7.28 | (1.92) |
| Life satisfaction during COVID-19 | 1201 | 0/10 | 5.74 | (2.22) | 5.55 | (2.42) | 5.56 | (2.42) |
| Personal relationships satisfaction before COVDI-19 | 1201 | 0/10 | 7.42 | (1.73) | 7.61 | (1.72) | 7.52 | (1.78) |
| Personal relationships satisfaction during COVID-19 | 1201 | 0/10 | 5.90 | (2.49) | 5.83 | (2.56) | 5.30 | (2.62) |
| Leisure satisfaction before COVID-19 | 1201 | 0/10 | 6.95 | (2.01) | 7.23 | (1.93) | 7.15 | (2.15) |
| Leisure satisfaction during COVID-19 | 1201 | 0/10 | 5.38 | (2.78) | 5.37 | (2.72) | 5.34 | (2.99) |
| Satisfaction with income before COVID-19 | 1201 | 0/10 | 6.64 | (2.11) | 6.40 | (2.28) | 6.49 | (2.33) |
| Satisfaction with income during COVID-19 | 1201 | 0/10 | 5.33 | (2.94) | 4.88 | (2.98) | 5.28 | (2.97) |
| Satisfaction with vacations before COVID-19 | 1201 | 0/10 | 7.27 | (2.25) | 7.30 | (2.14) | 7.19 | (2.32) |
| Satisfaction with vacations during COVID-19 | 1201 | 0/10 | 3.36 | (2.76) | 3.24 | (2.83) | 3.71 | (2.99) |
| Satisfaction with health before COVID-19 | 1201 | 0/10 | 8.12 | (1.71) | 8.19 | (1.66) | 8.15 | (1.76) |
| Satisfaction with health during COVID-19 | 1201 | 0/10 | 7.85 | (2.11) | 7.72 | (2.28) | 7.59 | (2.30) |
| Overall health before COVID-19 | 1201 | 0/10 | 7.92 | (1.65) | 7.99 | (1.60) | 7.97 | (1.56) |
| Overall health during COVID-19 | 1201 | 0/10 | 7.72 | (1.72) | 7.62 | (1.90) | 7.65 | (1.90) |
| Happiness before COVID-19 | 1201 | 1/5 | 3.77 | (0.76) | 3.82 | (0.77) | 3.72 | (0.82) |
| Happiness during COVID-19 | 1201 | 1/5 | 3.20 | (0.95) | 3.18 | (0.94) | 3.14 | (0.93) |
| Anxiety before COVID-19 | 1201 | 1/5 | 3.14 | (0.92) | 3.11 | (0.96) | 3.34 | (0.97) |
| Anxiety during COVID-19 | 1201 | 1/5 | 3.42 | (1.02) | 3.38 | (1.06) | 3.55 | (1.12) |
| Headache before COVID-19 | 1201 | 1/5 | 2.06 | (0.93) | 2.05 | (1.04) | 2.25 | (1.08) |
| Headache during COVID-19 | 1201 | 1/5 | 2.15 | (1.09) | 2.09 | (1.08) | 2.35 | (1.28) |
| Back pain before COVID-19 | 1201 | 1/5 | 2.10 | (1.07) | 2.13 | (1.10) | 2.23 | (1.13) |
| Back pain during COVID-19 | 1201 | 1/5 | 2.25 | (1.22) | 2.28 | (1.23) | 2.44 | (1.27) |
As seen in Table 2, sample size N = 1201 for all dependent variables while as seen in Table 1, sample size varies for different independent variables. Distance to city center is measured only for Athens and Thessaloniki – for which the analysis on the built environment and health/well-being is applied – so the sample size for this variable is considerably smaller. The sample size for the other independent variables slightly varies due to missing data: missing geospatial data, missing area socioeconomic data, and missing or invalid responses to certain survey questions.
2.3. Data analysis
To address the research questions of the paper, we performed two main types of analysis. First, we compared mean values of health and well-being before and during COVID-19. Second, we examined how built environment characteristics relate to health and well-being before and during COVID-19.
For the first analysis, we conducted Wilcoxon signed-rank tests to test for significant differences in the values of each health/well-being variable before and during COVID-19. Wilcoxon signed-rank tests are tests suitable for comparing variables in two dependent groups such as the ones in this study (before and during COVID-19). They are non-parametric tests suitable for ordinal variables and non-normal distributions of the differences between pairs of data. Since we perform before-during COVID-19 comparisons on 11 different dependent variables, we applied the Bonferroni Correction to reduce the likelihood of type I error. We therefore consider significant differences those with a p-value smaller than 0.00455.
For the second analysis, we used multiple linear regression, in which built environment characteristics, sociodemographic characteristics, and area socioeconomic status were treated as independent variables, and health and well-being measures were treated as the dependent variable. Measures of health and well-being represent ordinal variables but can be used as an approximation of continuous variables, and parametric analyses including linear regression are considered robust (Ferrer-i-Carbonell & Frijters, 2004; Norman, 2010). In fact, research has shown that using linear regression or ordinal regression in models with well-being as the dependent variable makes little difference (Ferrer-i-Carbonell & Frijters, 2004), therefore using linear models that treat health or well-being variables (measured on scales such as 1-5 or 0-10) as continuous is common practice (Cao, 2016; Poortinga et al., 2021). A preliminary analysis with multilevel models – considering area socioeconomic status on level-2 – was also performed but results showed that there was no between-cluster variance when level-1 variables were added, so this method was eventually not appropriate. Linear regression analyses were performed independently for Athens and Thessaloniki due to differences in urban structure, size, and socioeconomic characteristics. Independent analyses for these two main metropolitan areas of Greece were conducted for comparative purposes since preliminary analyses showed that results differed for the two regions. Built environment variables were included in the models in two steps based on relevant theoretical considerations (Mouratidis & Poortinga, 2020; Næss, 2019). The first step includes the variables “distance to city center” and “neighborhood density”, while the second step additionally includes the variables “public transport”, “local facilities”, “park area”, “tree cover”, “apartment”, and “dwelling size” all of which might be influenced by distance to city center and neighborhood density. In models of the second step, distance to city center and neighborhood density play the role of control variables. Variables on health and well-being that were examined as dependent variables in regression models are: “life satisfaction”, “personal relationships satisfaction”, “leisure satisfaction”, “overall health”, “happiness”, “anxiety”, “headache”, and “back pain”. The other three health and well-being variables in our dataset were considered less relevant to the built environment so were not included in this analysis in order to reduce complexity. The analysis was conducted for health and well-being: before COVID-19, during COVID-19, and for the change before-during COVID-19. For the dependent variables that decreased during COVID-19, the change was calculated by subtracting the value of the variable during COVID-19 from the value of the variable before COVID-19. For the dependent variables that increased during COVID-19, the change was calculated by subtracting the value of the variable before COVID-19 from the value of the variable during COVID-19. Independent analyses for the urban regions of Athens and Thessaloniki are presented in each table. All the analyses control for individual sociodemographic variables and area socioeconomic status(their coefficients are not presented here to reduce the size of the tables).
3. Results
3.1. Health and well-being before-during COVID-19
This analysis compares health and well-being variables before and during COVID-19 (Fig. 2 and Fig. 3 ). Wilcoxon signed-rank tests were performed. The results show that almost all health and well-being variables became significantly less positive during COVID-19 compared to before COVID-19. The values of the following variables decreased during COVID-19: life satisfaction, personal relationships satisfaction, leisure satisfaction, satisfaction with income, satisfaction with vacations, satisfaction with health, overall health, and happiness. Anxiety and the frequency of back pain increased during COVID-19. The increase in the frequency of headache was not significant when applying the Bonferroni Correction (p-value less than 0.00455). The most substantial changes are observed for well-being variables: life satisfaction (23% decrease), happiness (16% decrease), personal relationships satisfaction (23% decrease), leisure satisfaction (24% decrease), satisfaction with income (21% decrease), and satisfaction with vacations (54% decrease). The changes in physical and mental health measures – overall health (4% decrease), satisfaction with health (5% decrease), anxiety (9% increase), and back pain (8% increase) – were considerably smaller, but still statistically significant. Descriptive statistics on health and well-being in Athens, Thessaloniki, and other parts of Greece (Table 2) indicate that trends in changes before-during COVID-19 are similar for these different geographical areas.
Fig. 2.

Mean values of health and well-being variables before and during COVID-19. Notes: Variables are measured on a scale from 0 to 10. Sample size is N = 1201. Wilcoxon signed-rank tests show significant differences at * p < 0.001.
Fig. 3.
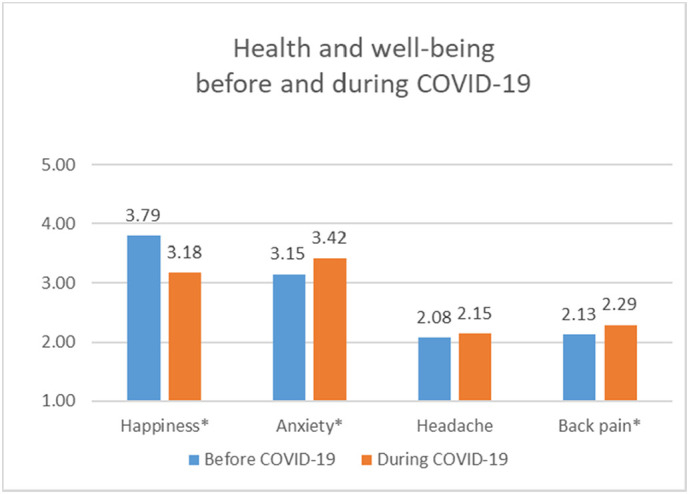
Mean values of health and well-being variables before and during COVID-19. Notes: Variables are measured on a scale from 1 to 5. Sample size is N = 1201. Wilcoxon signed-rank tests show significant differences at * p < 0.001.
3.2. Urban built environment, health, and well-being before-during COVID-19
The regression models presented in Table 3, Table 4, Table 5, Table 6, Table 7, Table 8, Table 9, Table 10 examine how built environment characteristics relate to health and well-being, with each table focusing on a different health or well-being variable.
Table 3.
Regression models examining how the built environment relates to life satisfaction before and during COVID-19.
| Variables | Life satisfaction (Athens) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (Before – During COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | 0.008 | 0.059 | 0.087 | 0.171⁎ | −0.081 | −0.125 |
| Neighborhood density | −0.105 | −0.087 | −0.032 | −0.053 | −0.047 | −0.012 |
| Public transport | −0.048 | 0.049 | −0.084 | |||
| Local facilities | 0.067 | 0.131 | −0.080 | |||
| Park area | 0.112a | 0.057 | 0.027 | |||
| Tree cover | −0.007 | −0.054 | 0.049 | |||
| Apartment | 0.054 | −0.084a | 0.124⁎ | |||
| Dwelling size | 0.095a | 0.041 | 0.031 | |||
| Summary statistics | ||||||
| N | 470 | 465 | 470 | 465 | 470 | 465 |
| Adjusted R-squared | 0.112 | 0.118 | 0.137 | 0.146 | 0.038 | 0.046 |
| Variables | Life satisfaction (Thessaloniki) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (Before – During COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | 0.012 | 0.065 | -0.095 | -0.087 | 0.106 | 0.136 |
| Neighborhood density | −0.058 | −0.219a | −0.140a | −0.119 | 0.101 | -0.037 |
| Public transport | 0.194a | −0.044 | 0.186 | |||
| Local facilities | −0.017 | 0.001 | -0.013 | |||
| Park area | 0.149⁎ | 0.119a | -0.014 | |||
| Tree cover | 0.004 | −0.026 | 0.029 | |||
| Apartment | -0.008 | −0.042 | 0.037 | |||
| Dwelling size | 0.129⁎ | 0.077 | 0.014 | |||
| Summary statistics | ||||||
| N | 510 | 504 | 510 | 504 | 510 | 504 |
| Adjusted R-squared | 0.101 | 0.116 | 0.058 | 0.059 | −0.002 | −0.007 |
All coefficients shown are standardized. The models are adjusted for individual sociodemographic variables: age, age squared, gender, unemployment, cohabitation status, citizenship, income, education level, presence of children in household, religiosity, and disability. The models are also adjusted for area socioeconomic status: mean household income, proportion of immigrants, and unemployment rate. ⁎⁎ p < 0.01. ⁎⁎⁎ p < 0.001.
p < 0.10.
p < 0.05.
Table 4.
Regression models examining how the built environment relates to personal relationships satisfaction before and during COVID-19.
| Variables | Personal relationships satisfaction (Athens) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (Before – During COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | −0.017 | −0.047 | 0.108 | 0.125 | −0.127a | −0.167a |
| Neighborhood density | −0.048 | −0.045 | 0.130 | 0.168 | −0.173a | −0.212a |
| Public transport | −0.104 | −0.104 | 0.034 | |||
| Local facilities | −0.024 | 0.148a | −0.175a | |||
| Park area | 0.021 | −0.008 | 0.024 | |||
| Tree cover | −0.038 | −0.110⁎ | 0.089 | |||
| Apartment | 0.049 | −0.080 | 0.121⁎ | |||
| Dwelling size | −0.019 | 0.055 | −0.072 | |||
| Summary statistics | ||||||
| N | 470 | 465 | 470 | 465 | 470 | 465 |
| Adjusted R-squared | 0.082 | 0.078 | 0.090 | 0.096 | 0.029 | 0.047 |
| Variables | Personal relationships satisfaction (Thessaloniki) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (Before – During COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| 0.5 | ||||||
| Built environment | ||||||
| Distance to city center | 0.042 | 0.042 | −0.091 | −0.058 | 0.116 | 0.084 |
| Neighborhood density | -0.035 | −0.127 | −0.167⁎ | −0.147 | 0.142a | 0.062 |
| Public transport | 0.158 | −0.002 | 0.103 | |||
| Local facilities | 0.008 | 0.050 | -0.043 | |||
| Park area | 0.050 | 0.036 | -0.003 | |||
| Tree cover | −0.043 | 0.024 | -0.051 | |||
| Apartment | −0.113a | -0.022 | -0.052 | |||
| Dwelling size | 0.095a | 0.059 | 0.003 | |||
| Summary statistics | ||||||
| N | 510 | 504 | 510 | 504 | 510 | 504 |
| Adjusted R-squared | 0.039 | 0.051 | 0.046 | 0.038 | 0.005 | -0.002 |
All coefficients shown are standardized. The models are adjusted for individual sociodemographic variables: age, gender, unemployment, cohabitation status, citizenship, income, education level, presence of children in household, religiosity, and disability. The models are also adjusted for area socioeconomic status: mean household income, proportion of immigrants, and unemployment rate. ⁎⁎ p < 0.01. ⁎⁎⁎ p < 0.001.
p < 0.10.
p < 0.05.
Table 5.
Regression models examining how the built environment relates to leisure satisfaction before and during COVID-19.
| Variables | Leisure satisfaction (Athens) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (Before – During COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | −0.038 | −0.003 | −0.005 | 0.084 | −0.019 | −0.071 |
| Neighborhood density | −0.047 | −0.105 | −0.040 | −0.078 | 0.005 | 0.001 |
| Public transport | 0.010 | 0.072 | −0.054 | |||
| Local facilities | −0.002 | 0.137 | −0.116 | |||
| Park area | 0.084 | 0.027 | 0.028 | |||
| Tree cover | −0.061 | −0.042 | −0.002 | |||
| Apartment | −0.027 | −0.085 | 0.054 | |||
| Dwelling size | −0.031 | −0.021 | −0.001 | |||
| Summary statistics | ||||||
| N | 470 | 465 | 470 | 465 | 470 | 460 |
| Adjusted R-squared | 0.041 | 0.038 | 0.040 | 0.048 | 0.042 | 0.040 |
| Variables | Leisure satisfaction (Thessaloniki) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (Before – During COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | 0.048 | 0.073 | −0.042 | −0.071 | 0.059 | 0.096 |
| Neighborhood density | −0.015 | −0.054 | −0.136a | −0.098 | 0.099 | 0.047 |
| Public transport | 0.058 | −0.070 | 0.087 | |||
| Local facilities | 0.039 | −0.008 | 0.028 | |||
| Park area | 0.010 | 0.047 | −0.031 | |||
| Tree cover | −0.037 | −0.071 | 0.035 | |||
| Apartment | 0.028 | −0.067 | 0.068 | |||
| Dwelling size | 0.149⁎ | 0.021 | 0.066 | |||
| Summary statistics | ||||||
| N | 510 | 504 | 510 | 504 | 510 | 504 |
| Adjusted R-squared | 0.015 | 0.019 | 0.043 | 0.040 | 0.019 | 0.013 |
All coefficients shown are standardized. The models are adjusted for individual sociodemographic variables: age, gender, unemployment, cohabitation status, citizenship, income, education level, presence of children in household, religiosity, and disability. The models are also adjusted for area socioeconomic status: mean household income, proportion of immigrants, and unemployment rate. ⁎⁎ p < 0.01. ⁎⁎⁎ p < 0.001.
p < 0.10.
p < 0.05.
Table 6.
Regression models examining how the built environment relates to overall health before and during COVID-19.
| Variables | Overall health (Athens) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (Before – During COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | 0.029 | 0.083 | 0.064 | 0.064 | −0.067 | 0.030 |
| Neighborhood density | −0.016 | −0.036 | 0.055 | 0.077 | −0.132 | −0.208a |
| Public transport | 0.019 | −0.058 | 0.142 | |||
| Local facilities | 0.037 | 0.020 | 0.031 | |||
| Park area | 0.077 | 0.048 | 0.049 | |||
| Tree cover | −0.025 | −0.022 | −0.003 | |||
| Apartment | 0.036 | −0.010 | 0.082 | |||
| Dwelling size | 0.055 | 0.027 | 0.049 | |||
| Summary statistics | ||||||
| N | 470 | 465 | 470 | 465 | 470 | 465 |
| Adjusted R-squared | 0.116 | 0.111 | 0.109 | 0.100 | 0.015 | 0.017 |
| Variables | Overall health (Thessaloniki) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (Before – During COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | 0.045 | 0.150 | −0.029 | −0.043 | 0.099 | 0.250⁎ |
| Neighborhood density | 0.011 | −0.148 | −0.016 | −0.092 | 0.038 | −0.047 |
| Public transport | 0.230⁎ | 0.128 | 0.095 | |||
| Local facilities | 0.050 | −0.038 | 0.119a | |||
| Park area | 0.084 | 0.036 | 0.050 | |||
| Tree cover | −0.007 | −0.013 | 0.011 | |||
| Apartment | −0.015 | 0.014 | −0.039 | |||
| Dwelling size | 0.088a | 0.141⁎⁎ | −0.101a | |||
| Summary statistics | ||||||
| N | 510 | 504 | 510 | 504 | 510 | 504 |
| Adjusted R-squared | 0.181 | 0.185 | 0.203 | 0.204 | 0.035 | 0.045 |
All coefficients shown are standardized. The models are adjusted for individual sociodemographic variables: age, gender, unemployment, cohabitation status, citizenship, income, education level, presence of children in household, religiosity, and disability. The models are also adjusted for area socioeconomic status: mean household income, proportion of immigrants, and unemployment rate. ⁎⁎⁎ p < 0.001.
p < 0.10.
p < 0.05.
p < 0.01.
Table 7.
Regression models examining how the built environment relates to happiness before and during COVID-19.
| Variables | Happiness (Athens) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (Before – During COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | 0.096 | 0.050 | 0.128a | 0.185⁎ | -0.052 | −0.147a |
| Neighborhood density | 0.024 | 0.091 | 0.068 | 0.045 | -0.049 | 0.028 |
| Public transport | −0.089 | 0.070 | −0.142 | |||
| Local facilities | 0.032 | 0.121 | −0.096 | |||
| Park area | −0.058 | −0.064 | 0.018 | |||
| Tree cover | 0.053 | −0.054 | 0.097a | |||
| Apartment | 0.002 | −0.067 | 0.069 | |||
| Dwelling size | −0.030 | −0.029 | 0.005 | |||
| Summary statistics | ||||||
| N | 470 | 465 | 470 | 465 | 470 | 465 |
| Adjusted R-squared | 0.057 | 0.050 | 0.084 | 0.089 | 0.042 | 0.055 |
| Variables | Happiness (Thessaloniki) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (Before – During COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | 0.023 | −0.072 | −0.092 | −0.096 | 0.108 | 0.042 |
| Neighborhood density | −0.057 | −0.225a | −0.130 | −0.020 | 0.081 | −0.108 |
| Public transport | 0.144 | −0.045 | 0.134 | |||
| Local facilities | −0.125a | −0.056 | −0.046 | |||
| Park area | 0.044 | 0.094 | −0.052 | |||
| Tree cover | −0.121⁎ | 0.016 | −0.110⁎ | |||
| Apartment | −0.037 | −0.051 | 0.018 | |||
| Dwelling size | 0.011 | 0.063 | −0.058 | |||
| Summary statistics | ||||||
| N | 510 | 504 | 510 | 504 | 510 | 504 |
| Adjusted R-squared | 0.069 | 0.077 | 0.079 | 0.076 | −0.005 | −0.001 |
All coefficients shown are standardized. The models are adjusted for individual sociodemographic variables: age, age squared, gender, unemployment, cohabitation status, citizenship, income, education level, presence of children in household, religiosity, and disability. The models are also adjusted for area socioeconomic status: mean household income, proportion of immigrants, and unemployment rate. ⁎⁎ p < 0.01. ⁎⁎⁎ p < 0.001.
p < 0.10.
p < 0.05.
Table 8.
Regression models examining how the built environment relates to anxiety before and during COVID-19.
| Variables | Anxiety (Athens) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (During – Before COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | 0.021 | 0.092 | −0.073 | −0.018 | 0.084 | −0.094 |
| Neighborhood density | 0.172a | 0.154 | 0.062 | 0.078 | 0.087 | −0.057 |
| Public transport | 0.063 | −0.007 | −0.059 | |||
| Local facilities | 0.081 | 0.088 | 0.013 | |||
| Park area | 0.038 | 0.030 | −0.004 | |||
| Tree cover | 0.040 | 0.113⁎ | 0.070 | |||
| Apartment | −0.027 | 0.044 | 0.063 | |||
| Dwelling size | −0.086 | −0.151⁎⁎ | −0.067 | |||
| Summary statistics | ||||||
| N | 470 | 465 | 470 | 465 | 470 | 465 |
| Adjusted R-squared | 0.083 | 0.085 | 0.017 | 0.032 | 0.030 | 0.028 |
| Variables | Anxiety (Thessaloniki) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (During – Before COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | −0.100 | −0.159 | −0.010 | −0.043 | −0.077 | 0.097 |
| Neighborhood density | −0.070 | 0.004 | −0.017 | −0.111 | −0.044 | −0.111 |
| Public transport | −0.118 | 0.089 | 0.190a | |||
| Local facilities | 0.000 | −0.025 | −0.025 | |||
| Park area | −0.107a | −0.046 | 0.049 | |||
| Tree cover | −0.033 | −0.087 | −0.056 | |||
| Apartment | 0.024 | 0.021 | 0.000 | |||
| Dwelling size | −0.049 | 0.024 | 0.066 | |||
| Summary statistics | ||||||
| N | 510 | 504 | 510 | 504 | 510 | 504 |
| Adjusted R-squared | 0.053 | 0.047 | 0.035 | 0.036 | 0.004 | 0.006 |
All coefficients shown are standardized. The models are adjusted for individual sociodemographic variables: age, gender, unemployment, cohabitation status, citizenship, income, education level, presence of children in household, religiosity, and disability. The models are also adjusted for area socioeconomic status: mean household income, proportion of immigrants, and unemployment rate. ⁎⁎⁎ p < 0.001.
p < 0.10.
p < 0.05.
p < 0.01.
Table 9.
Regression models examining how the built environment relates to headache before and during COVID-19.
| Variables | Headache (Athens) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (During - Before COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | 0.003 | 0.020 | −0.015 | −0.001 | 0.025 | −0.025 |
| Neighborhood density | −0.016 | −0.101 | −0.033 | −0.053 | 0.027 | 0.046 |
| Public transport | 0.182a | 0.010 | −0.199a | |||
| Local facilities | −0.081 | 0.053 | 0.169a | |||
| Park area | −0.020 | −0.034 | −0.023 | |||
| Tree cover | 0.018 | −0.020 | −0.048 | |||
| Apartment | −0.030 | −0.022 | 0.004 | |||
| Dwelling size | −0.016 | −0.031 | −0.025 | |||
| Summary statistics | ||||||
| N | 470 | 465 | 470 | 465 | 470 | 465 |
| Adjusted R-squared | 0.069 | 0.064 | 0.064 | 0.056 | 0.009 | 0.005 |
| Variables | Headache (Thessaloniki) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (During – Before COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | 0.008 | −0.038 | −0.007 | 0.045 | 0.018 | 0.101 |
| Neighborhood density | −0.026 | −0.052 | 0.021 | −0.078 | −0.056 | −0.036 |
| Public transport | 0.044 | 0.176 | 0.169 | |||
| Local facilities | 0.006 | 0.078 | 0.090 | |||
| Park area | −0.091 | −0.064 | 0.026 | |||
| Tree cover | −0.056 | −0.035 | 0.023 | |||
| Apartment | −0.093 | −0.109a | −0.028 | |||
| Dwelling size | −0.067 | −0.038 | 0.030 | |||
| Summary statistics | ||||||
| N | 510 | 504 | 510 | 504 | 510 | 504 |
| Adjusted R-squared | 0.088 | 0.084 | 0.061 | 0.071 | −0.002 | 0.000 |
All coefficients shown are standardized. The models are adjusted for individual sociodemographic variables: age, gender, unemployment, cohabitation status, citizenship, income, education level, presence of children in household, religiosity, and disability. The models are also adjusted for area socioeconomic status: mean household income, proportion of immigrants, and unemployment rate. ⁎ p < 0.05. ⁎⁎ p < 0.01. ⁎⁎⁎ p < 0.001.
p < 0.10.
Table 10.
Regression models examining how the built environment relates to back pain before and during COVID-19.
| Variables | Back pain (Athens) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (During – Before COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | −0.097 | −0.059 | −0.126a | −0.086 | 0.060 | −0.050 |
| Neighborhood density | −0.184⁎ | −0.271⁎ | −0.207⁎ | −0.226⁎ | 0.066 | 0.017 |
| Public transport | 0.164 | 0.019 | −0.181 | |||
| Local facilities | −0.036 | 0.087 | 0.172a | |||
| Park area | −0.005 | 0.000 | 0.008 | |||
| Tree cover | −0.004 | −0.057 | −0.078 | |||
| Apartment | −0.086a | −0.046 | 0.043 | |||
| Dwelling size | −0.103a | 0.030 | 0.175⁎⁎ | |||
| Summary statistics | ||||||
| N | 470 | 465 | 470 | 465 | 470 | 465 |
| Adjusted R-squared | 0.101 | 0.108 | 0.081 | 0.078 | 0.008 | 0.025 |
| Variables | Back pain (Thessaloniki) |
|||||
|---|---|---|---|---|---|---|
| Before COVID-19 |
During COVID-19 |
Change (During – Before COVID-19) |
||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Built environment | ||||||
| Distance to city center | −0.046 | 0.003 | −0.116 | −0.082 | 0.106 | −0.119 |
| Neighborhood density | −0.011 | 0.018 | −0.038 | −0.116 | 0.039 | −0.184 |
| Public transport | −0.008 | 0.192a | 0.277⁎ | |||
| Local facilities | 0.031 | −0.004 | −0.044 | |||
| Park area | 0.056 | −0.004 | −0.075 | |||
| Tree cover | 0.035 | 0.085 | 0.074 | |||
| Apartment | −0.082 | −0.138⁎ | −0.089 | |||
| Dwelling size | −0.048 | −0.081 | −0.053 | |||
| Summary statistics | ||||||
| N | 510 | 504 | 510 | 504 | 510 | 504 |
| Adjusted R-squared | 0.076 | 0.068 | 0.093 | 0.101 | 0.004 | 0.015 |
All coefficients shown are standardized. The models are adjusted for individual sociodemographic variables: age, gender, unemployment, cohabitation status, citizenship, income, education level, presence of children in household, religiosity, and disability. The models are also adjusted for area socioeconomic status: mean household income, proportion of immigrants, and unemployment rate. ⁎⁎⁎ p < 0.001.
p < 0.10.
p < 0.05.
p < 0.01
Table 3 displays models on life satisfaction. Results indicate that neighborhood density is negatively associated with life satisfaction in Thessaloniki during COVID-19. Park area is positively associated with life satisfaction in both Athens and Thessaloniki before COVID-19. This association persists in Thessaloniki during COVID-19, with park area being positively related to life satisfaction in Thessaloniki during COVID-19. Dwelling size is positively associated with life satisfaction in both Athens and Thessaloniki before COVID-19, but not during COVID-19. Living in an apartment is negatively associated with life satisfaction in Athens during COVID-19. Public transport is positively associated with life satisfaction in Thessaloniki before COVID-19, but not during COVID-19.
Table 4 presents models on personal relationships satisfaction. Neighborhood density is found to be negatively associated with personal relationships satisfaction in Thessaloniki during COVID-19. Living in an apartment is negatively related to personal relationships satisfaction in Thessaloniki before COVID-19. Local facilities are positively associated with personal relationships satisfaction in Athens during COVID-19. Tree cover is negatively associated with personal relationships satisfaction in Athens during COVID-19.
Table 5 presents models on leisure satisfaction. Findings indicate a negative association between neighborhood density and leisure satisfaction in Thessaloniki during COVID-19. Dwelling size is positively associated with leisure satisfaction in Thessaloniki before COVID-19. The other built environment characteristics did not yield significant associations with leisure satisfaction.
Tables 6 presents models on overall health. Dwelling size is found to be positively associated with overall health in Thessaloniki before COVID-19, and this positive association became stronger during COVID-19. Public transport is positively associated with overall health in Thessaloniki before COVID-19. The other built environment characteristics did not yield significant associations with overall health.
Table 7 displays models on happiness. Living further away from the city center of Athens is found to be positively associated with happiness during COVID-19. Local facilities are negatively associated with happiness in Thessaloniki before COVID-19. Tree cover is negatively associated with happiness in Thessaloniki before COVID-19. The other built environment characteristics did not yield significant associations with happiness.
Table 8 displays models on anxiety. Findings indicate that higher neighborhood density is associated with higher anxiety in Athens before COVID-19. A negative relationship between dwelling size and anxiety in Athens during COVID-19 is found, suggesting the larger dwellings are linked to lower anxiety in Athens during COVID-19. Park area is associated with lower anxiety in Thessaloniki before COVID-19. Tree cover is related to higher anxiety in Athens during COVID-19. The other built environment characteristics did not yield significant associations with anxiety.
Table 9 and Table 10 present models on the frequency of headache and back pain respectively. Public transport accessibility is associated with more frequent headache in Athens before COVID-19. Living in an apartment is associated with less frequent headache in Thessaloniki during COVID-19. Living further from the city center of Athens was associated with less frequent back pain during COVID-19. Higher neighborhood density is related to less frequent back pain in Athens both before and during COVID-19. Living in an apartment is associated with less frequent back pain in Athens before COVID-19 and in Thessaloniki during COVID-19, whereas larger dwelling size is linked to less frequent back pain in Athens before COVID-19. Public transport accessibility is associated with more frequent back pain in Thessaloniki during COVID-19. The other built environment characteristics are not found to be significantly associated with back pain.
4. Synthesis and discussion of results
To answer the first research question of this study, we analyzed trends in health and well-being before and during the COVID-19 pandemic. Comparisons before versus during COVID-19 suggest that health and well-being outcomes naturally worsened due to the pandemic. The following indicators declined during COVID-19: overall health, satisfaction with health, life satisfaction, happiness, personal relationships satisfaction, leisure satisfaction, satisfaction with income, and satisfaction with vacations. Anxiety and back pain increased during COVID-19. More substantial changes were observed for well-being variables than for health variables. Specifically, life satisfaction, happiness, personal relationships satisfaction, leisure satisfaction, satisfaction with income, and satisfaction with vacations all substantially declined during COVID-19, according to the study's findings. We could infer that these changes in health and well-being are mainly due to the direct and indirect impacts of COVID-19. This is because health and well-being outcomes were evaluated for the same participants before and during COVID-19 and the time period between the two measurements is very short, so no other major changes are expected to have affected the large majority of participants. The decline in health and well-being outcomes because of COVID-19 found in our study supports earlier results from other geographical areas (Fiok et al., 2021; Li et al., 2020; Moreno et al., 2020; Patrick et al., 2020; White & Van Der Boor, 2020). Our results also support those from a recent study in Greece suggesting a decline in personal circumstances and an increase in stress due to COVID-19 (Vatavali et al., 2020). It should be noted that results from this study represent the first wave of the COVID-19 pandemic (spring 2020). The impact of the pandemic on health and well-being has fluctuated but it is expected that in general health and well-being outcomes have remained worse than pre-COVID-19 times throughout the pandemic (Sønderskov et al., 2021). As COVID-19 continued in 2020 and 2021, well-being levels for certain individuals might have improved (e.g. getting used to lockdowns, social distancing, and new lifestyles) but might have worsened for others (e.g. infection with the virus, economic impacts of continuous pandemic might have caused unemployment or loss of income). Continuous study of health and well-being throughout the pandemic is needed to obtain the full picture of the impacts of COVID-19.
To answer the second research question of this study, we analyzed relationships between built environment characteristics and health and well-being before and during COVID-19. Independent analyses were performed for Athens and Thessaloniki. The observed differences in findings before and during COVID-19 indicate that the role of the urban built environment in health and well-being differs for the COVID-19 period compared to pre-COVID-19. The differences in findings for the two cities suggest that the particularities of each city contributed to the relationship between built environment and health and well-being in diverse ways. Findings are mostly modest in size as commonly observed in studies on objectively measured built environment characteristics, health, and well-being. Statistically significant findings are summarized in Table 11 and are discussed as follows.
Table 11.
How built environment relates to health and well-being before and during COVID-19: a summary of findings.
| Built environment characteristics | Positive health/well-being outcomes | Negative health/well-being outcomes | Overall health/well-being outcome during COVID-19 |
|---|---|---|---|
| Longer distance to city center | Higher happiness (Athens during COVID-19); less frequent back pain (Athens during COVID-19) | Positive | |
| Higher neighborhood density | Less frequent back pain (Athens before and during COVID-19) | Lower life satisfaction, lower personal relationships satisfaction, and lower leisure satisfaction (Thessaloniki during COVID-19); higher anxiety (Athens before COVID-19) | Mostly negative |
| Public transport accessibility | Higher life satisfaction and better overall health (Thessaloniki before COVID-19) | More frequent headache (Athens before COVID-19); more frequent back pain (Thessaloniki during COVID-19) | Negative |
| Numerous local facilities | Higher personal relationships satisfaction (Athens during COVID-19) | Lower happiness (Thessaloniki before COVID-19) | Positive |
| Large park area | Higher life satisfaction (Athens and Thessaloniki before COVID-19; Thessaloniki during COVID-19); lower anxiety (Thessaloniki before COVID-19) | Positive | |
| Higher tree cover | Lower personal relationships satisfaction (Athens during COVID-19); higher anxiety (Athens during COVID-19); lower happiness (Thessaloniki before COVID-19) | Negativea | |
| Living in an apartment | Less frequent back pain (Athens before COVID-19 and Thessaloniki during COVID-19); less frequent headache (Thessaloniki during COVID-19) | Lower life satisfaction (Athens during COVID-19); lower personal relationships satisfaction (Thessaloniki before COVID-19) | Mixed |
| Living in a larger dwelling | Higher life satisfaction (Athens and Thessaloniki before COVID-19); higher leisure satisfaction (Thessaloniki before COVID-19); better overall health (Thessaloniki before and during COVID-19 – more significant during COVID-19); lower anxiety (Athens during COVID-19); less frequent back pain (Athens before COVID-19) | Positive |
Longer distance to the city center of Athens was found to be related to higher happiness and less frequent back pain during COVID-19, suggesting that residents of suburban locations were happier and suffered less often from back pain problems than their inner-city counterparts during COVID-19. These findings concern Athens but not Thessaloniki, and this difference is possibly due to the substantially larger size of Athens as well as due to differences in city morphology such as the proximity of their city core to the seafront. Inner-city residents of Athens may have had fewer opportunities to avoid stressors found in the dense urban core, while it was likely easier for inner-city residents of Thessaloniki to access the city's waterfront and surrounding forest. On the other hand, distance to the city center, in general, may have had indirect contributions to well-being due to its links to the other built environment characteristics. For both cities in the study, neighborhoods located closer to the city center are characterized by higher population densities, greater public transport accessibility, more and larger parks, more local facilities, more apartments and fewer detached houses, and smaller dwellings.
Higher neighborhood densities were associated with lower life satisfaction, lower personal relationships satisfaction, and lower leisure satisfaction in Thessaloniki during COVID-19, indicating a negative link between urban compactness and well-being during COVID-19 for the case of Thessaloniki. Higher neighborhood density was also associated with more frequent anxiety in Athens before COVID-19, supporting previous related evidence (Lederbogen et al., 2011; Mouratidis, 2019b). On the other hand, residents of denser neighborhoods of Athens reported less frequent back pain both before and during COVID-19. This finding is probably due to increased walking of residents of denser neighborhoods (Fiok et al., 2021) as research has shown that high density is linked to more walking (Durand et al., 2011; Mouratidis, 2019a; Saelens & Handy, 2008), and more walking is linked to less frequent back pain (Sitthipornvorakul et al., 2018; Vanti et al., 2019).
Public transport accessibility was related to better overall health and higher life satisfaction in Thessaloniki before COVID-19. This outcome is in accordance with earlier studies suggesting that cities providing easy access to convenient public transportation may promote happiness, physical activity, and related health benefits (Eisenberg-Guyot et al., 2019; Freeland et al., 2013; Leyden et al., 2011). It is important to note that public transport accessibility is enabled and accompanied by urban forms of short distances and higher density (Næss, 2019). Altogether these characteristics may provide accessibility benefits. The positive relationship between public transport accessibility and health and well-being disappeared during COVID-19, which might be due to the high risk of infection when using public transport during the pandemic and the associated decline in public transport use (Bucsky, 2020; Hadjidemetriou et al., 2020; Jenelius & Cebecauer, 2020; Teixeira & Lopes, 2020). Public transport accessibility was also found to be associated with more frequent headache in Athens before COVID-19. The use of public transport especially during rush hours or the exposure to noise generated by public transport might contribute to more frequent headache. The reduced use of public transport during COVID-19 may explain the observed insignificance of this association for the COVID-19 period. The observed association between public transport accessibility and frequency of back pain in Thessaloniki during COVID-19 is difficult to interpret and requires more detailed investigation.
Numerous local facilities were associated with higher personal relationships satisfaction in Athens during COVID-19. Local facilities – those that remained open during the pandemic – including educational, commercial, and recreational facilities may have allowed residents to perform activities without disruption and without the risk of infection associated with the use of several motorized travel modes, since local facilities are typically accessed by active travel modes. By allowing residents to participate in some activities, local facilities may have enabled in-person social interaction thus contributing to satisfaction with personal relationships. This positive link between local facilities and well-being during COVID-19 found in the study is in line with claims about the positive role of facilities and services during pandemic crises (Douglas et al., 2020; Hamidi et al., 2020; Litman, 2020a). On the other hand, the observed negative link between local facilities and happiness in Thessaloniki before COVID-19 is difficult to interpret. It might be coincidental or could be attributed to noise or other factors generated by urban vibrancy and numerous local facilities.
Large parks in close proximity were associated with higher life satisfaction in Athens before COVID-19 and in Thessaloniki before and during COVID-19 as well as lower anxiety in Thessaloniki before COVID-19. These findings are in line with evidence on the well-being benefits of urban nature (Gascon et al., 2015; Markevych et al., 2017). The positive link between park area and life satisfaction during COVID-19 in Thessaloniki supports recent studies finding a positive relationship between green space and well-being during the pandemic (Ugolini et al., 2020; Xie et al., 2020) and claims about the role of green space in mitigating COVID-19 effects on health and well-being (Slater et al., 2020). Parks and other types of green space allow people to perform several activities including physical and social activities (Markevych et al., 2017). Since other arenas for physical and social activities have been restricted due to COVID-19, the importance of large parks within walkable distance has been highlighted during the pandemic.
Tree cover had some unexpected negative associations with health and well-being outcomes. Residents of neighborhoods with higher tree cover in Athens were found to have lower personal relationships satisfaction and higher anxiety in Athens during COVID-19. Residents of neighborhoods with higher tree cover in Thessaloniki were found to have lower happiness before COVID-19. These negative links between tree cover and well-being are difficult to interpret and are in contrast with the well-established benefits of trees in cities (Ulmer et al., 2016) and urban nature in general (Gascon et al., 2015; Markevych et al., 2017). These findings might be attributed to particularities in neighborhoods with high tree cover in the case cities or to some unseen factor not captured by the independent variables in the models, for example, particularly remote or deprived areas that happen to have high tree cover. Such cases might not be completely captured by the variables on distance to city center and area socioeconomic status. Further research is needed to understand the pathways behind these unexpected observed outcomes.
Living in an apartment – rather than living in a detached house or duplex – was associated with lower life satisfaction in Athens during COVID-19. Detached or duplex houses with attached private green spaces and outdoor areas might have been more functional and pleasant during the pandemic. Private outdoor spaces might have fostered leisure activities such as gardening (Corley et al., 2021) and social interaction with a lower risk of infection. Living in an apartment was also found to be negatively linked to personal relationships satisfaction in Thessaloniki before COVID-19. One possible explanation behind this finding is the lower local social cohesion typically observed for residents of apartment blocks compared to residents of detached or duplex houses. Moreover, living in an apartment was related to less frequent back pain in Athens before COVID-19 and in Thessaloniki during COVID-19. This finding is probably due to the relationship between high-density living and back pain explained above. Residents of apartments typically found in denser areas tend to walk more (Durand et al., 2011; Mouratidis, 2019a) and this may improve back pain problems (Sitthipornvorakul et al., 2018; Vanti et al., 2019). Finally, living in an apartment was associated with less frequent headache in Thessaloniki during COVID-19. This association is difficult to interpret and requires further research.
Living in a larger dwelling was linked to several health and well-being benefits both before and during COVID-19. Specifically, living in a larger dwelling was associated with lower anxiety in Athens during COVID-19, better overall health in Thessaloniki before but even more so during COVID-19, higher life satisfaction in Athens and Thessaloniki before COVID-19, higher leisure satisfaction in Thessaloniki before COVID-19, and less frequent back pain in Athens before COVID-19. Overall, these findings support links between housing and well-being (Mouratidis, 2020). Living in cramped dwellings – which is more prevalent among socioeconomically deprived households – is conducive to lower well-being outcomes (Hu & Coulter, 2016) and has been linked to a higher risk of depression during COVID-19 (Amerio et al., 2020). Residents spent large parts, if not most, of their days at home during the pandemic and performed a wide range of home-based activities and teleactivities (de Haas et al., 2020; Marcucci et al., 2021; Pierce et al., 2020; Shamshiripour et al., 2020; Wijesooriya et al., 2020). Those who lived in larger dwellings might have had more opportunities to perform activities at home without disruption and stress.
This study enhances the literature reviewed in Section 1 in several ways. First, it provides an overview on how a wide a range of health and well-being indicators changed due to COVID-19. Few studies so far have collectively assessed such measures. Quasi-longitudinal data used in the study, despite their limitations, clearly indicate trends on how health and well-being worsened due to the pandemic. The second and most important contribution is the study's investigation of the relationships between built environment characteristics and health/well-being before and during COVID-19. Most studies so far have focused on specific characteristics (e.g. green space) but not on how different built environment characteristics collectively relate to health/well-being before and during COVID-19. This is, to our knowledge, one of the first studies using geospatial and survey (before and during COVID-19) data to investigate this topic. Such evidence may provide important insights for urban planning and policy during pandemics but also under normal circumstances.
Our study has certain limitations that should be considered. The trends in health and well-being before and during the COVID-19 pandemic are analyzed for the context of Greece. Similar studies from other contexts will enrich the current findings. Future studies measuring health and well-being trends during later COVID-19 lockdowns would be particularly useful. Pathways between built environment characteristics and health and well-being outcomes need to be investigated in more detail in future research to provide insights into possible causal links. This study has used self-reported measures of health and well-being. In future studies, objective health and well-being indicators could be assessed for their relation to the built environment in cities during COVID-19. The sample of the study is subject to biases common for questionnaire surveys and non-probability sampling. Health and well-being indicators were evaluated with univariate variables representing distinct concepts, thus a composite measure of health and/or well-being is not possible. These univariate variables are stable and reliable (Lucas & Brent Donnellan, 2012); datasets with latent variables might have nevertheless produced even more reliable estimates. This study has assessed separate models for each health and well-being variable, while future studies could also explore connections between these health and well-being variables with more complex statistical techniques. The study was based on retrospective quasi-longitudinal data on health and well-being outcomes before and during COVID-19. Individual recall might be imprecise and subject to biases compared to prospective longitudinal designs. Furthermore, due to the short interval between the before and during COVID-19 time points, individual sociodemographic characteristics were assessed only once. Measurements of these variables in two time points might have provided greater accuracy to the results.
5. Conclusions
This is one of the first studies to investigate relationships between cities, health, and well-being before and during COVID-19 using GIS-derived measures of the built environment in combination with quasi-longitudinal data on health and well-being. The study contributes to knowledge on COVID-19 and quality of life in cities by assessing changes in health and well-being before and during COVID-19 and by examining how urban planning and built environment characteristics in specific may have contributed to these changes.
Findings from Greek cities suggest that health and well-being outcomes worsened due to the COVID-19 pandemic. Overall health, satisfaction with health, life satisfaction, happiness, personal relationships satisfaction, leisure satisfaction, satisfaction with income, and satisfaction with vacations all declined during COVID-19 compared to the pre-COVID-19 period, while anxiety and back pain problems increased during the pandemic. More substantial changes were observed for well-being outcomes than for health outcomes. Our analysis on cities, health, and well-being indicates that the role of the urban built environment in health and well-being differs considerably for the COVID-19 period compared to pre-COVID-19. Accessibility to numerous local facilities, proximity to large parks, lower neighborhood density, and living further away from the city center were all associated with better well-being outcomes during COVID-19, while living in a larger dwelling was associated with better overall health and lower anxiety during COVID-19.
Perhaps the most crucial outcome of this study concerns the implications for urban planning and policies to mitigate the negative impacts of a mega health crisis such as the COVID-19 pandemic and future pandemics on health and well-being in cities. These impacts can be observed in relation to other major changes that were accelerated due to this pandemic, such as remote working, e-shopping, distant learning etc. This pandemic is expected to have an impact on how we reflect on denser urban areas that seem to be more vulnerable during the COVID-19 crisis when it comes to living conditions and quality of life. This is especially the case in older high-density inner-city parts of certain urban regions. These compact parts might have the advantages of short distances and mixed-use development; however, they are, for the case of Greek cities but also in other contexts, often characterized by poorer living conditions such as an old building stock; lack of open public spaces; lack of parks, gardens, and vegetation; poor infrastructure; noise; air pollution; and lack of direct sunlight in dwellings due to building density.
Therefore, urban planning recommendations should focus on the qualities as well as the major needs of cities. Key issues for urban planning are the type and quality of housing provision; the density and local services heterogeneity; the location of destinations and accessibility; the quality of public transport; and the availability, size, variety of open and green spaces. Easy access to inclusive, large, well-maintained parks, gardens, and other open public spaces; easy access to nearby nature and in general contact with greenery; focus on short distances and the neighborhood level along with the provision of multiple, diverse facilities and services and available space for walking in the surroundings; avoidance of cramped dwellings and housing support for vulnerable groups; communal, outdoor spaces attached to apartment blocks; improvements in walkability and cyclability; provision of frequent, well-ventilated, and safe public transport; and affordable and accessible new mobility options are some measures that could ensure and strengthen the capacities of cities to deal with the effects of a public health crisis and improve the health and well-being of their citizens.
CRediT authorship contribution statement
Kostas Mouratidis: Conceptualization, Methodology, Investigation, Formal analysis, Visualization, Writing – original draft, Writing – review & editing, Funding acquisition, Project administration. Athena Yiannakou: Investigation, Writing – original draft, Writing – review & editing, Supervision.
Acknowledgements
This research is co-financed by Greece and the European Union (European Social Fund- ESF) through the Operational Programme “Human Resources Development, Education and Lifelong Learning” in the context of the project “Reinforcement of Postdoctoral Researchers - 2nd Cycle” (MIS-5033021), implemented by the State Scholarships Foundation (ΙΚΥ). We thank the anonymous reviewers for their insightful comments.
Appendix A. Survey questions (translated from Greek)
In which type of residence do you live?
-
•
Apartment in an apartment block
-
•
Detached single-family house
-
•
Duplex house
-
•
Other (you can write here):
Please write the address of your present dwelling:
The purpose of collecting these data is to analyze the characteristics of each residential area and understand their influence on quality of life so that we can make suitable recommendations for improvement according to the type of residential area.
-
•
Street and number:
-
•
Postal code:
-
•
City:
What is the size of your dwelling in square meters (approximately)?
The purpose of collecting these data is to analyze the characteristics of the residence and understand their influence on quality of life, so that we can make suitable recommendations for improvement according to the type of residence.
-
•
Square meters:
For the following questions:
Consider your life during the lockdown due to the coronavirus pandemic (Covid-19) (during Covid-19).
Also consider your life before the Covid-19 pandemic (before Covid-19).
How satisfied are/were you with your…?
Extremely dissatisfied 0 1 2 3 4 5 6 7 8 9 10 Extremely satisfied
-
•
Life as a whole (during Covid-19)
-
•
Life as a whole (before Covid-19)
-
•
Personal relationships (during Covid-19)
-
•
Personal relationships (before Covid-19)
-
•
Leisure activities (during Covid-19)
-
•
Leisure activities (before Covid-19)
-
•
Health (during Covid-19)
-
•
Health (before Covid-19)
-
•
Vacations (during Covid-19)
-
•
Vacations (before Covid-19)
-
•
Personal income (during Covid-19)
-
•
Personal income (before Covid-19)
Please tell us how much of the time you felt…
Very rarely or never, Rarely, Sometimes, Often, Very often or always
-
•
Happy (during Covid-19)
-
•
Happy (before Covid-19)
-
•
Anxious (during Covid-19)
-
•
Anxious (before Covid-19)
-
•
Pain in your head (during Covid-19)
-
•
Pain in your head (before Covid-19)
-
•
Pain in your back (during Covid-19)
-
•
Pain in your back (before Covid-19)
How would you describe your health in general…?
Extremely poor 0 1 2 3 4 5 6 7 8 9 10 Extremely good
-
•
Overall health (during Covid-19)
-
•
Overall health (before Covid-19)
Are you hampered in your daily activities in any way by any longstanding illness, or disability, infirmity or mental health problem?
-
•
Yes a lot
-
•
Yes to some extent
-
•
No
What is your current employment status?
-
•
Work (full time or part time)
-
•
Student
-
•
Recently fired or stopped working
-
•
Temporary suspension from work
-
•
Out of work (for other reasons)
-
•
Retired
-
•
Other (you can write here):
Year of birth:
Gender:
-
•
Female
-
•
Male
-
•
Other
Citizenship:
-
•
Greek
-
•
Other
What is the highest level of education you have completed?
-
•
Elementary school
-
•
High school (or professional secondary school)
-
•
Technical education (e.g. vocational school)
-
•
Bachelor's degree or similar
-
•
Master's degree or doctoral degree
Do you live with a spouse/partner?
-
•
No
-
•
Yes
How many children live regularly within your household?
-
•
0
-
•
1
-
•
2
-
•
3
-
•
4 or more
Including yourself, how many people live regularly within your household in total?
-
•
1
-
•
2
-
•
3
-
•
4
-
•
5
-
•
6
-
•
7 or more
Would you consider yourself religious?
-
•
No
-
•
Yes somewhat
-
•
Yes
What is your personal monthly net income (approximately)? Please consider the income from all possible sources and subtract possible additional taxes, insurance, and pension.
-
•
No income
-
•
Lower than 200 Euro
-
•
200–400 Euro
-
•
401–600 Euro
-
•
601–800 Euro
-
•
801–1000 Euro
-
•
1001–1200 Euro
-
•
1201–1400 Euro
-
•
1401–1600 Euro
-
•
1601–1800 Euro
-
•
1801–2000 Euro
-
•
2001–2200 Euro
-
•
2201–2400 Euro
-
•
2401–2600 Euro
-
•
2601–2800 Euro
-
•
2801–3000 Euro
-
•
3001–3500 Euro
-
•
3501–4000 Euro
-
•
Higher than 4000 Euro
References
- AbouKorin S.A.A., Han H., Mahran M.G.N. Role of urban planning characteristics in forming pandemic resilient cities – case study of Covid-19 impacts on European cities within England, Germany and Italy. Cities. 2021;118 doi: 10.1016/j.cities.2021.103324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amerio A., Brambilla A., Morganti A., Aguglia A., Bianchi D., Santi F., Capolongo S. COVID-19 lockdown: Housing built environment’s effects on mental health. International Journal of Environmental Research and Public Health. 2020;17(16) doi: 10.3390/ijerph17165973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks S.K., Webster R.K., Smith L.E., Woodland L., Wessely S., Greenberg N., Rubin G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet. 2020;395(10227):912–920. doi: 10.1016/S0140-6736(20)30460-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bucsky P. Modal share changes due to COVID-19: The case of Budapest. Transportation Research Interdisciplinary Perspectives. 2020;8 doi: 10.1016/j.trip.2020.100141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cao X. How does neighborhood design affect life satisfaction? Evidence from twin cities. Travel Behaviour and Society. 2016;5:68–76. doi: 10.1016/j.tbs.2015.07.001. [DOI] [Google Scholar]
- Carozzi F., Provenzano S., Roth S. CEP discussion paper no 1711: Urban density and Covid-19. 2020. https://cep.lse.ac.uk/pubs/download/dp1711.pdf Retrieved from London:
- Christakis N.A. Little, Brown Spark; New York: 2020. Apollo's arrow: The profound and enduring impact of coronavirus on the way we live. [Google Scholar]
- Connolly C., Keil R., Ali S.H. Extended urbanisation and the spatialities of infectious disease: Demographic change, infrastructure and governance. Urban Studies. 2020 doi: 10.1177/0042098020910873. 0042098020910873. [DOI] [Google Scholar]
- Corley J., Okely J.A., Taylor A.M., Page D., Welstead M., Skarabela B., Russ T.C. Home garden use during COVID-19: Associations with physical and mental wellbeing in older adults. Journal of Environmental Psychology. 2021;73 doi: 10.1016/j.jenvp.2020.101545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davy B. Social distancing and cultural bias. Journal of the American Planning Association. 2020;1–8 doi: 10.1080/01944363.2020.1824617. [DOI] [Google Scholar]
- de Haas M., Faber R., Hamersma M. How COVID-19 and the dutch ‘intelligent lockdown’ change activities, work and travel behaviour: Evidence from longitudinal data in the Netherlands. Transportation Research Interdisciplinary Perspectives. 2020;6 doi: 10.1016/j.trip.2020.100150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dembski S., Sykes O., Couch C., Desjardins X., Evers D., Osterhage F., Zimmermann K. Reurbanisation and suburbia in Northwest Europe: A comparative perspective on spatial trends and policy approaches. Progress in Planning. 2019;100462 doi: 10.1016/j.progress.2019.100462. [DOI] [Google Scholar]
- Douglas M., Katikireddi S.V., Taulbut M., McKee M., McCartney G. Mitigating the wider health effects of covid-19 pandemic response. BMJ. 2020;369 doi: 10.1136/bmj.m1557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Durand C.P., Andalib M., Dunton G.F., Wolch J., Pentz M.A. A systematic review of built environment factors related to physical activity and obesity risk: Implications for smart growth urban planning. Obesity Reviews. 2011;12(5):e173–e182. doi: 10.1111/j.1467-789X.2010.00826.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg-Guyot J., Moudon A.V., Hurvitz P.M., Mooney S.J., Whitlock K.B., Saelens B.E. Beyond the bus stop: Where transit users walk. Journal of Transport & Health. 2019;14 doi: 10.1016/j.jth.2019.100604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- European Social Survey . Centre for Comparative Social Surveys, City University London; London: 2012. ESS round 6 source questionnaire. [Google Scholar]
- FCL, CIESIN . Columbia University; 2020. Facebook Connectivity Lab and Center for International Earth Science Information Network - CIESIN. 2016. High Resolution Settlement Layer (HRSL). Source imagery for HRSL © 2016 DigitalGlobe. [Google Scholar]
- Ferrer-i-Carbonell A., Frijters P. How important is methodology for the estimates of the determinants of happiness? The Economic Journal. 2004;114(497):641–659. [Google Scholar]
- Fiok K., Karwowski W., Gutierrez E., Saeidi M., Aljuaid A.M., Davahli M.R., Sawyer B.D. A study of the effects of the COVID-19 pandemic on the experience of back pain reported on Twitter® in the United States: A natural language processing approach. International Journal of Environmental Research and Public Health. 2021;18(9) doi: 10.3390/ijerph18094543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fiorillo A., Gorwood P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. European Psychiatry. 2020;63(1) doi: 10.1192/j.eurpsy.2020.35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freeland A.L., Banerjee S.N., Dannenberg A.L., Wendel A.M. Walking associated with public transit: Moving toward increased physical activity in the United States. American Journal of Public Health. 2013;103(3):536–542. doi: 10.2105/AJPH.2012.300912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gascon M., Triguero-Mas M., Martínez D., Dadvand P., Forns J., Plasència A., Nieuwenhuijsen M. Mental health benefits of long-term exposure to residential green and blue spaces: A systematic review. International Journal of Environmental Research and Public Health. 2015;12(4):4354. doi: 10.3390/ijerph120404354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gehl Public Space & Public Life during COVID-19. 2020. https://covid19.gehlpeople.com/files/report.pdf Retrieved from:
- Giles-Corti B., Vernez-Moudon A., Reis R., Turrell G., Dannenberg A.L., Badland H., Stevenson M. City planning and population health: A global challenge. The Lancet. 2016;388(10062):2912–2924. doi: 10.1016/S0140-6736(16)30066-6. [DOI] [PubMed] [Google Scholar]
- Guida C., Carpentieri G. Quality of life in the urban environment and primary health services for the elderly during the Covid-19 pandemic: An application to the city of Milan (Italy) Cities. 2021;110 doi: 10.1016/j.cities.2020.103038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hadjidemetriou G.M., Sasidharan M., Kouyialis G., Parlikad A.K. The impact of government measures and human mobility trend on COVID-19 related deaths in the UK. Transportation Research Interdisciplinary Perspectives. 2020;6 doi: 10.1016/j.trip.2020.100167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall P. Blackwell; Oxford: 1988. Cities of tomorrow. [Google Scholar]
- Hall P. Routledge; London: 2013. Good cities, better lives: How Europe discovered the lost art of urbanism. [Google Scholar]
- Hamidi S., Ewing R., Tatalovich Z., Grace J.B., Berrigan D. Associations between urban sprawl and life expectancy in the United States. International Journal of Environmental Research and Public Health. 2018;15(5) doi: 10.3390/ijerph15050861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamidi S., Sabouri S., Ewing R. Does density aggravate the COVID-19 Pandemic? Journal of the American Planning Association. 2020;86(4):495–509. doi: 10.1080/01944363.2020.1777891. [DOI] [Google Scholar]
- Hansen M.C., Potapov P.V., Moore R., Hancher M., Turubanova S.A., Tyukavina A., Townshend J.R.G. High-resolution global maps of 21st-century forest cover change. Science. 2013;342(6160):850–853. doi: 10.1126/science.1244693. [DOI] [PubMed] [Google Scholar]
- Honey-Rosés J., Anguelovski I., Chireh V.K., Daher C., Konijnendijk van den Bosch C., Litt J.S., Nieuwenhuijsen M.J. The impact of COVID-19 on public space: An early review of the emerging questions – Design, perceptions and inequities. Cities & Health. 2020;1–17 doi: 10.1080/23748834.2020.1780074. [DOI] [Google Scholar]
- Hu M., Roberts J.D., Azevedo G.P., Milner D. The role of built and social environmental factors in Covid-19 transmission: A look at America’s capital city. Sustainable Cities and Society. 2021;65 doi: 10.1016/j.scs.2020.102580. [DOI] [Google Scholar]
- Hu Y., Coulter R. Living space and psychological well-being in urban China: Differentiated relationships across socio-economic gradients. Environment and Planning A: Economy and Space. 2016;49(4):911–929. doi: 10.1177/0308518X16680213. [DOI] [Google Scholar]
- Jenelius E., Cebecauer M. Impacts of COVID-19 on public transport ridership in Sweden: Analysis of ticket validations, sales and passenger counts. Transportation Research Interdisciplinary Perspectives. 2020;8 doi: 10.1016/j.trip.2020.100242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kalogirou S. Spatial inequalities in income and post-graduate educational attainment in Greece. Journal of Maps. 2010;6(1):393–400. doi: 10.4113/jom.2010.1095. [DOI] [Google Scholar]
- Kent J.L., Thompson S. The three domains of urban planning for health and well-being. Journal of Planning Literature. 2014;29(3):239–256. doi: 10.1177/0885412214520712. [DOI] [Google Scholar]
- Knox P., McKarthy L. Pearson; London: 2013. Urbanization: An introduction to urban geography. [Google Scholar]
- Lai K.Y., Webster C., Kumari S., Sarkar C. The nature of cities and the Covid-19 pandemic. Current Opinion in Environmental Sustainability. 2020;46:27–31. doi: 10.1016/j.cosust.2020.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lederbogen F., Kirsch P., Haddad L., Streit F., Tost H., Schuch P., Deuschle M. City living and urban upbringing affect neural social stress processing in humans. Nature. 2011;474(7352):498–501. doi: 10.1038/nature10190. [DOI] [PubMed] [Google Scholar]
- Leyden K.M., Goldberg A., Michelbach P. Understanding the pursuit of happiness in ten major cities. Urban Affairs Review. 2011;47(6):861–888. doi: 10.1177/1078087411403120. [DOI] [Google Scholar]
- Li J., Yang Z., Qiu H., Wang Y., Jian L., Ji J., Li K. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry. 2020;19(2):249–250. doi: 10.1002/wps.20758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Litman T. Pandemic-resilient community planning. 2020. https://www.vtpi.org/PRCP.pdf Retrieved from Victoria, Canada:
- Litman T. Urban sanity: Understanding urban mental health impacts and how to create saner, happier cities. 2020. https://www.vtpi.org/urban-sanity.pdf Retrieved from Victoria, Canada:
- Lucas R.E., Brent Donnellan M. Estimating the reliability of single-item life satisfaction measures: Results from four National Panel Studies. Social Indicators Research. 2012;105(3):323–331. doi: 10.1007/s11205-011-9783-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marcucci E., Gatta V., Le Pira M., Chao T., Li S. Bricks or clicks? Consumer channel choice and its transport and environmental implications for the grocery market in Norway. Cities. 2021;110 doi: 10.1016/j.cities.2020.103046. [DOI] [Google Scholar]
- Markevych I., Schoierer J., Hartig T., Chudnovsky A., Hystad P., Dzhambov A.M., Fuertes E. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environmental Research. 2017;158:301–317. doi: 10.1016/j.envres.2017.06.028. [DOI] [PubMed] [Google Scholar]
- Mell I., Whitten M. Access to nature in a post Covid-19 world: Opportunities for green infrastructure financing, distribution and equitability in urban planning. International Journal of Environmental Research and Public Health. 2021;18(4):1527. doi: 10.3390/ijerph18041527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moreno C., Wykes T., Galderisi S., Nordentoft M., Crossley N., Jones N., Arango C. How mental health care should change as a consequence of the COVID-19 pandemic. The Lancet Psychiatry. 2020;7(9):813–824. doi: 10.1016/S2215-0366(20)30307-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mouratidis K. Built environment and leisure satisfaction: The role of commute time, social interaction, and active travel. Journal of Transport Geography. 2019;80 doi: 10.1016/j.jtrangeo.2019.102491. [DOI] [Google Scholar]
- Mouratidis K. Compact city, urban sprawl, and subjective well-being. Cities. 2019;92:261–272. doi: 10.1016/j.cities.2019.04.013. [DOI] [Google Scholar]
- Mouratidis K. Commute satisfaction, neighborhood satisfaction, and housing satisfaction as predictors of subjective well-being and indicators of urban livability. Travel Behaviour and Society. 2020;21:265–278. doi: 10.1016/j.tbs.2020.07.006. [DOI] [Google Scholar]
- Mouratidis K. Urban planning and quality of life: A review of pathways linking the built environment to subjective well-being. Cities. 2021;115 doi: 10.1016/j.cities.2021.103229. [DOI] [Google Scholar]
- Mouratidis K., Poortinga W. Built environment, urban vitality and social cohesion: Do vibrant neighborhoods foster strong communities? Landscape and Urban Planning. 2020;204 doi: 10.1016/j.landurbplan.2020.103951. [DOI] [Google Scholar]
- Mumford L. Penguin Books; London: 1961. The City in history: Its origins, its transformations and its prospects. [Google Scholar]
- Næss P. Meta-analyses of built environment effects on travel: No new platinum standard. 2019. (0739456X19856425) [DOI] [Google Scholar]
- Norman G. Likert scales, levels of measurement and the “laws” of statistics. Advances in Health Sciences Education. 2010;15(5):625–632. doi: 10.1007/s10459-010-9222-y. [DOI] [PubMed] [Google Scholar]
- OECD . OECD Better Life Initiative; Washington, DC: 2013. OECD guidelines on measuring subjective well-being. [PubMed] [Google Scholar]
- Patrick S.W., Henkhaus L.E., Zickafoose J.S., Lovell K., Halvorson A., Loch S., Davis M.M. Well-being of parents and children during the COVID-19 pandemic: A National Survey. Pediatrics. 2020;146(4) doi: 10.1542/peds.2020-016824. [DOI] [PubMed] [Google Scholar]
- Pfeiffer D., Cloutier S. Planning for happy neighborhoods. Journal of the American Planning Association. 2016;82(3):267–279. doi: 10.1080/01944363.2016.1166347. [DOI] [Google Scholar]
- Pierce B.S., Perrin P.B., Tyler C.M., McKee G.B., Watson J.D. The COVID-19 telepsychology revolution: A national study of pandemic-based changes in U.S. mental health care delivery. American Psychologist. 2020 doi: 10.1037/amp0000722. [DOI] [PubMed] [Google Scholar]
- Poortinga W., Bird N., Hallingberg B., Phillips R., Williams D. The role of perceived public and private green space in subjective health and wellbeing during and after the first peak of the COVID-19 outbreak. Landscape and Urban Planning. 2021;211 doi: 10.1016/j.landurbplan.2021.104092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogowska A.M., Kuśnierz C., Bokszczanin A. Examining anxiety, life satisfaction, general health, stress and coping styles during COVID-19 pandemic in Polish sample of university students. Psychology Research and Behavior Management. 2020;13:797–811. doi: 10.2147/PRBM.S266511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saelens B.E., Handy S.L. Built environment correlates of walking: A review. Medicine and Science in Sports and Exercise. 2008;40(7 Suppl):S550. doi: 10.1249/MSS.0b013e31817c67a4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaer A., Rezaei M., Moghani Rahimi B., Shaer F. Examining the associations between perceived built environment and active travel, before and after the COVID-19 outbreak in Shiraz city, Iran. Cities. 2021;115 doi: 10.1016/j.cities.2021.103255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shamshiripour A., Rahimi E., Shabanpour R., Mohammadian A. How is COVID-19 reshaping activity-travel behavior? Evidence from a comprehensive survey in Chicago. Transportation Research Interdisciplinary Perspectives. 2020;7 doi: 10.1016/j.trip.2020.100216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sharifi A., Khavarian-Garmsir A.R. The COVID-19 pandemic: Impacts on cities and major lessons for urban planning, design, and management. Science of the Total Environment. 2020;749 doi: 10.1016/j.scitotenv.2020.142391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shoari N., Ezzati M., Baumgartner J., Malacarne D., Fecht D. Accessibility and allocation of public parks and gardens in England and Wales: A COVID-19 social distancing perspective. PLOS ONE. 2020;15(10) doi: 10.1371/journal.pone.0241102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sitthipornvorakul E., Klinsophon T., Sihawong R., Janwantanakul P. The effects of walking intervention in patients with chronic low back pain: A meta-analysis of randomized controlled trials. Musculoskeletal Science and Practice. 2018;34:38–46. doi: 10.1016/j.msksp.2017.12.003. [DOI] [PubMed] [Google Scholar]
- Skapinakis P., Bellos S., Oikonomou A., Dimitriadis G., Gkikas P., Perdikari E., Mavreas V. Depression and its relationship with coping strategies and illness perceptions during the COVID-19 lockdown in Greece: A cross-sectional survey of the population. Depression Research and Treatment. 2020;2020:3158954. doi: 10.1155/2020/3158954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slater S.J., Christiana R.W., Gustat J. Recommendations for keeping parks and green space accessible for mental and physical health during COVID-19 and other pandemics. Preventing Chronic Disease. 2020;17:E59. doi: 10.5888/pcd17.200204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sønderskov K.M., Dinesen P.T., Vistisen H.T., Østergaard S.D. Variation in psychological well-being and symptoms of anxiety and depression during the COVID-19 pandemic: Results from a three-wave panel survey. Acta Neuropsychiatrica. 2021;33(3):156–159. doi: 10.1017/neu.2020.47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stevenson M., Thompson J., de Sá T.H., Ewing R., Mohan D., McClure R., Woodcock J. Land use, transport, and population health: estimating the health benefits of compact cities. The Lancet. 2016;388(10062):2925–2935. doi: 10.1016/S0140-6736(16)30067-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teixeira J.F., Lopes M. The link between bike sharing and subway use during the COVID-19 pandemic: The case-study of New York's citi bike. Transportation Research Interdisciplinary Perspectives. 2020;6 doi: 10.1016/j.trip.2020.100166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ugolini F., Massetti L., Calaza-Martínez P., Cariñanos P., Dobbs C., Ostoić S.K., Sanesi G. Effects of the COVID-19 pandemic on the use and perceptions of urban green space: An international exploratory study. Urban Forestry & Urban Greening. 2020;56 doi: 10.1016/j.ufug.2020.126888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ulmer J.M., Wolf K.L., Backman D.R., Tretheway R.L., Blain C.J.A., O’Neil-Dunne J.P.M., Frank L.D. Multiple health benefits of urban tree canopy: The mounting evidence for a green prescription. Health & Place. 2016;42:54–62. doi: 10.1016/j.healthplace.2016.08.011. [DOI] [PubMed] [Google Scholar]
- UN Habitat World cities report 2020. The value of sustainable urbanization. 2020. https://unhabitat.org/sites/default/files/2020/10/wcr_2020_report.pdf Retrieved from:
- Vanti C., Andreatta S., Borghi S., Guccione A.A., Pillastrini P., Bertozzi L. The effectiveness of walking versus exercise on pain and function in chronic low back pain: A systematic review and meta-analysis of randomized trials. Disability and Rehabilitation. 2019;41(6):622–632. doi: 10.1080/09638288.2017.1410730. [DOI] [PubMed] [Google Scholar]
- Vatavali F., Gareiou Z., Kehagia F., Zervas E. Impact of COVID-19 on urban everyday life in Greece. Perceptions, experiences and practices of the active population. Sustainability. 2020;12(22):9410. [Google Scholar]
- Wang F., Wang D. Mobility, sociability and well-being of urban living. Springer; Berlin: 2016. Place, geographical context and subjective well-being: State of art and future directions; pp. 189–230. [Google Scholar]
- White R.G., Van Der Boor C. Impact of the COVID-19 pandemic and initial period of lockdown on the mental health and well-being of adults in the UK. BJPsych Open. 2020;6(5) doi: 10.1192/bjo.2020.79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wijesooriya N.R., Mishra V., Brand P.L.P., Rubin B.K. COVID-19 and telehealth, education, and research adaptations. Paediatric Respiratory Reviews. 2020;35:38–42. doi: 10.1016/j.prrv.2020.06.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xie J., Luo S., Furuya K., Sun D. Urban parks as green buffers during the COVID-19 pandemic. Sustainability. 2020;12(17):6751. [Google Scholar]
- Yiannakou A. In conversation with Klaus R. kunzmann: Athena yiannakou — Challenges for spatial development and planning in Europe. disP. The Planning Review. 2017;53(2):92–93. doi: 10.1080/02513625.2017.1341184. [DOI] [Google Scholar]
- Zhang N., Jia W., Wang P., Dung C.-H., Zhao P., Leung K., Li Y. Changes in local travel behaviour before and during the COVID-19 pandemic in Hong Kong. Cities. 2021;112 doi: 10.1016/j.cities.2021.103139. [DOI] [PMC free article] [PubMed] [Google Scholar]