

Abstract
Introduction
Peyronie's Disease is a deformity of the penis. Surgical procedure options for Peyronie's disease treatment include grafting (curvature >60°) or plication (curvature <60°). This case report emphasizes the curvature degree and therapy options chosen, such as tunica albuginea plication instead of grafting.
Case presentation
A 55-year-old male complains about a curved penis during erection. Examination shows penile bending 70° ventrally with ±15 cm length and 2x4cm size. The patient underwent Ducket-Baskin tunica albuginea placation (TAP). Postoperative unbent penis size decrement of ±3 cm, neither pain nor erectile dysfunction felt.
Clinical discussion
Tunica plication is usually recommended in Peyronie's disease patients with curvature less than 60°, without an hourglass or hinge if grafting is not available. This technique is more simple, safe, the higher success rate of curvature correction (> 80%), low recurrency, low complication rate of penile hypoesthesia (approximately 10%), as well as low risk for postoperative erectile dysfunction.
Conclusion
In our case, the tunica albuginea plication technique gives a good outcome in Peyronie's disease reconstruction.
Keywords: Peyronie disease, Penile deformity, Tunica albuginea plication, Penile curvature, Ducket-Baskin
Highlights
-
•
The curvature degree as a factor affecting therapy option, including tunica albuginea plication instead of grafting.
-
•
The penis was bent around 70° ventrally and the patient underwent Ducket-Baskin tunica albuginea placation (TAP).
-
•
Tunica albuginea plication technique gives a good outcome.
1. Introduction
Peyronie's disease, or induration penis plastica, is a deformity in the penis, described as “rosary beads of scar” that causes curvature of the penis during erection. The disease is one of the conditions often seen in men aged 55 to 60 years old, with a prevalence of 0.4% to 9%. Patients with erectile dysfunction and diabetes have a higher risk of Peyronie's disease [1], [2].
Peyronie's disease is characterized by the development of fibrous or nodule plaques in the tunica layer of the penile albuginea, which causes scar formation following penile trauma that activates abnormal tissue healing responses. Scar of plaque inelasticity may cause deformities in the penis, including curvature, indentation, shortening, and sometimes erectile dysfunction. One of the most important characteristics of the wound healing disorder is once a scar is formed, it will not undergo normal remodeling, and the scar and deformity will persist [1], [2].
Peyronie's disease with a large degree of curvature may cause intercourse disturbance and is often thought to have a spontaneous resolution, but we found that spontaneous resolution seldom happens from recent studies. We also found that 50% of patients' conditions will be worsen if not treated within the first 12–18 months [3]. According to the latest guideline, therapies of Peyronie's disease are conservative, including drugs or surgery. Surgery can be done by grafting procedure if the curvature is >60°, and a plication procedure would be preferred if the curvature is <60o. But instead, in this report, we emphasize the preference of tunica albuginea plication in Peyronie's Disease with curvature >60° for a patient referred to Persahabat Hospital, Jakarta.
2. Case presentation
A 55-years-old male patient came in with a complaint of penile bending during an erection in the last six months prior to admission. Initially, the patient complained about a hard palpable nodule-like encircle of half penis circumference on the ventral skin of the penis, close to the penile gland. When erects, the area feels tender, and the penis bends downward. The bending is worsened, but the pain is lessened in time. The patient still had regular sexual intercourse but was bothered by the complaint. He had no history of trauma or scars on the penis, no history of urinary tract infections. The patient claimed that this was the first symptom. He had a history of smoking, hypertension, and diabetes mellitus. The patient was married and had two kids. The patient went to see a doctor in Bekasi, who then referred him to Persahabatan Hospital Jakarta.
Physical examination was done and within normal limit with the blood pressure of 140/90 mmHg. The penis length was ±15 cm, the penis was bending around 70° ventrally. The plaque was palpable on the ventral shaft encircle the half of penis circumference, proximal to the gland, with the size of 2 × 4 cm and hard on consistency (Fig. 1). Hourglass and hinge not found. Ultrasound examination was done and showed plaque of the corpus cavernosum. A clinical diagnosis of Peyronie Disease was made.
Fig. 1.
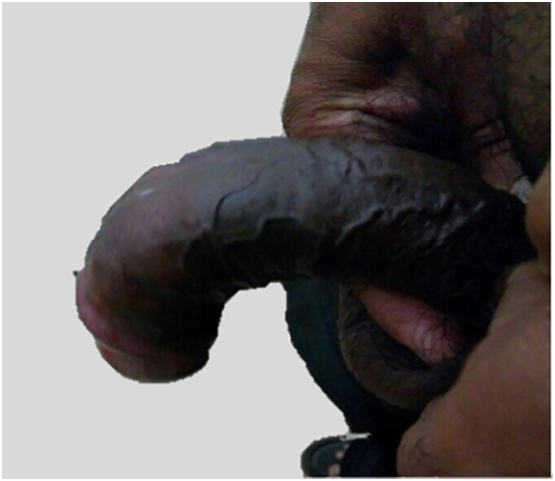
Patient's penis pre-operative.
The patient underwent the Ducket-Baskin tunica albuginea plication (TAP) technique. During operation, we performed an erection test; although the degree of curvature was >60o, we chose to perform tunica albuginea placation (TAP). Because the plaque's location was on the ventral side of the penis, we had to perform neurovascular bundle (NVB) mobilization by opening the buck fascia on the dorsal side. Then, we performed another erection test. The penis was straight and no longer bent (Fig. 2). The patient was hospitalized for 5 days. One month after surgery, the follow-up examination showed the penis was no longer bent, but we found a size decrement of the penis around 3 cm (Fig. 3). The patient had no complaints regarding pain or erectile dysfunction.
Fig. 2.

Tunica albuginea plication process.
Fig. 3.

Tunica albuginea plication post-operation, length decrement of the penis appeared.
3. Discussion
We reported the case of Peyronie disease in a 55-year-old man with a history of uncontrolled diabetes; this correlates with the theory that this disease would happen in men ranging from ages of 55 to 60 years old, and the prevalence would increase in populations with diabetes mellitus and erectile dysfunction [5].
There are two phases of Peyronie's disease, the active (acute) phase in which is generally related to pain during erection and penile deformity, and the stable (chronic) phase in which is characterized by the stable deformation and the disappearance of pain during erection [1], [6], [8]. The patient had achieved the stable phase of Peyronie's disease. No complaint of erectile dysfunction, but the patient felt bothered with the bending penis.
Even though conservative therapy in Peyronie's disease could lessen or even eliminate pain during erection, improvement in the deformity of the penis is only seen in few cases. Surgery is still the gold standard for Peyronie's disease, primarily to reduce the deformity [1], [2].
An operative technique that is recommended in penile curvature >60° is the Grafting procedure. Unfortunately, the ideal grafting material has yet to be identified in Indonesia [1]. Tunica plication is usually recommended in patients with curvature less than 60°, without hourglass or hinge, and in patients presumed to have a length decrement of 20% during erection [1]. Single or multiple longitudinal incisions were made on the convex side of the penis closed horizontally to shorten the longer (or convex) side of the tunica albuginea to match the length to the shorter side. Advantages of these approaches include shorter surgical time, good cosmetic outcomes, minimal rigidity effect, and relatively safe and effective surgery. Disadvantages of this approach include shortening of the penis and failure to correct an hourglass or hinge [2]. All plication procedures would decrease the length of the penis 1—1.5 cm, but in a patient with ventral curvature greater than 60 degrees to have the most significant potential loss of penile length [9], [10], [11]. Plication variation includes Levine modification of the Duckett-Baskin tunica albuginea plication (TAP), originally used for children with congenital curvature. In this technique, a partial-thickness incision was made transversely on the contralateral side to the point of maximum curvature. A pair of transverse parallel incisions sized 1 to 1.5 cm in length were made through the longitudinal fibers but should not damage the inner circular fibers of the tunica. If the underlying cavernosal tissue were still intact, it would decrease the likelihood of postoperative ED. These incisions are separated by 0.5 to 1.0 cm depending on the desired amount of shortening. The longitudinal fibers between the two transverse incisions are excised to reduce the bulk of the plication. This procedure is now done with a single central permanent suture (2–0 Tevdek suture®, Teleflex Medical®, Research Triangle Park®, NC®, or TiCron suture®, Medline®, Mundelein®, IL®), placed an inverting vertical mattress to let the knot seamless and with choosing the absorbable suture (3–0 polydioxanone [PDS]®, Ethicon®, Somerville®, NJ®) placed in a Lembert technique to make the plication and knots unpalpable. In this case, we use prolane® as a monofilament suture non-absorbable as a permanent suture because all earlier materials are not available in Indonesia [2]. There is no evidence that one surgical approach provides better outcomes than another, but curvature correction is projected to increase ED risk compared with grafting procedures [4].
In this patient, a plaque was identified at the central part of the penis, which resulted in 70 degrees curvature to the ventral when erect. There were no hourglass and hinge. The patient has already been informed and understood about the risk of post-operation penile decrement. Due to the graft materials are not available in Indonesia, the tunica albuginea plication technique was chosen. Another consideration in selecting this technique was because the method is more simple, safe, the higher success rate of curvature correction (> 80%), low recurrency, low complication rate of penile hypoesthesia (approximately 10%), as well as low risk for postoperative erectile dysfunction [1], [2]. The postoperative condition showed that the penis was no longer bent, with the length of the penis ±12 cm or decreased ±3 cm, with neither pain nor erectile dysfunction during sexual intercourse.
4. Conclusion
In this case, the tunica albuginea plication (TAP) technique gives a relatively safe and effective alternative for curvature correction, in case the grafting method is not readily available.
Ethics approval and consent to participate
This case report has been exempted from ethical approval by Universitas Indonesia Ethical Committee.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available on demand.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
CRediT authorship contribution statement
Hendy Mirza: Conceptualization, Methodology, Writing Original-Draft, Investigation, Resources.
Rio Rahmadi: Conceptualization, Methodology, Writing Original-Draft, Investigation.
Research registration
Not applicable.
Guarantor
Hendy Mirza.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Other relevant information
The case report is in compliance with SCARE Guidelines [12].
Declaration of competing interest
The authors declare that they have no competing interests.
Acknowledgment
The authors would like to thank everyone who supported this study. Special thanks are given to Universitas Indonesia which fully supported the authors during writing period.
References
- 1.Salonia A., Bettochi C., Carvalho J., Corona G., Jones T.H., Kadioglu A., Martinez-Salamanca J.I. Eur Urol. EAU Guidelines Office; Arnhem, The Netherlands: 2021 March. European Association of Urology Guidelines on Sexual and Reproductive Health: 2021 Update. [Google Scholar]
- 2.Wein A.J., Kavoussi L.R., Partin A.W., Peters C. 2016. Campbell-Walsh Urology. [Google Scholar]
- 3.Mirza M., Saria M., Mumtaz T. Peyronie’s disease. J. Ayub Med. Coll. Abbottabad. 2006;18:66–67. [PubMed] [Google Scholar]
- 4.Ralph D., Gonzalez-Cadavid N., Mirone V., Perovic S., Sohn M., Usta M. The management of Peyronie’s disease: evidence-based 2010 guidelines. J. Sex. Med. 2010 Jul;7(7):2359–2374. doi: 10.1111/j.1743-6109.2010.01850.x. [DOI] [PubMed] [Google Scholar]
- 5.Dibenedetti D.B., Nguyen D., Zografos L., Ziemiecki R., Zhou X. A population-based study of Peyronie's disease: prevalence and treatment patterns in the United States. Adv Urol. 2011;2011 doi: 10.1155/2011/282503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pryor J.P., Ralph D.J. Clinical presentations of Peyronie’s disease. Int. J. Impot. Res. 2002;14(5):414–417. doi: 10.1038/sj.ijir.3900877. [DOI] [PubMed] [Google Scholar]
- 8.Chung E., Clendinning E., Lessard L., Brock G. Five-year follow-up of Peyronie's graft surgery: outcomes and patient satisfaction. J. Sex. Med. 2011;8(2):594–600. doi: 10.1111/j.1743-6109.2010.02102.x. [DOI] [PubMed] [Google Scholar]
- 9.Greenfield J.M., Lucas S., Levine L.A. Factors affecting the loss of length associated with Tunica albuginea plication for correction of penile curvature. J. Urol. 2006;175(1):238–241. doi: 10.1016/S0022-5347(05)00063-7. [DOI] [PubMed] [Google Scholar]
- 10.Mulhall J., Anderson M., Parker M. A surgical algorithm for men with combined Peyronie’s disease and erectile dysfunction: functional and satisfaction outcomes. J. Sex. Med. 2005;2(1):132–138. doi: 10.1111/j.1743-6109.2005.20113.x. [DOI] [PubMed] [Google Scholar]
- 11.Rybak J., Papagiannopoulos D., Levine L. A retrospective comparative study of traction therapy vs. no traction following Tunica albuginea plication or partial excision and grafting for Peyronie’s disease: measured lengths and patient perceptions. J. Sex. Med. 2012 Sep;9(9):2396–2403. doi: 10.1111/j.1743-6109.2012.02849.x. [DOI] [PubMed] [Google Scholar]
- 12.Agha R.A., Franchi T., Sohrabi C., Mathew G., for the SCARE Group The SCARE 2020 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int. J. Surg. 2020;84:226–230. doi: 10.1016/j.ijsu.2020.10.034. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available on demand.