

A 2-year-old female was admitted to the hospital after presenting to the emergency department with a 3-day history of dry cough, one episode of emesis, and low-grade fever. Her medical history was significant for systemic hypertension and polyuric, non-dialysis-dependent stage 5 chronic kidney disease (CKD) related to branchio-oto-renal (BOR) dysplasia syndrome, for which she was active on the deceased donor waiting list for kidney transplant.
Upon initial presentation, she was thin and well-appearing with normal blood pressure and heart rate and increased respiratory rate. Her oxygen saturation was normal in room air. There was no evidence of edema or weight gain from baseline. The cardiovascular and respiratory examinations were remarkable for mild tachypnea without retractions and the presence of a pericardial friction rub.
Initial blood studies showed an elevated CRP of 61.7 mg/L (normal < 8.0), mildly low albumin at 3.3 g/dL (normal 3.5–5), a normal white blood count of 11.7 × 109/L (normal 4.9–13.2), a low hemoglobin of 7.7 g/dL (normal 10.2–12.7), and an elevated platelet count of 570 × 109/L (normal 189–394). Blood chemistry panel showed a high serum creatinine of 7.54 mg/dL (normal 0.19–0.49), high blood urea nitrogen (BUN) of 58 mg/dL (normal 7–22), low total calcium at 7.3 mg/dL (normal 9.3–10.6), and low potassium at 3.0 mEq/L (normal 3.6–5.2). A catheterized urine sample demonstrated more than 300 mg/dL protein with a specific gravity of 1.020 but was otherwise unremarkable, and urine culture was negative. Respiratory pathogen panel and SARS-CoV-2 PCR tests collected by nasopharyngeal swab were negative. A chest radiograph demonstrated new enlargement of the cardiac silhouette compared to the study obtained 1 month prior to presentation (Fig. 1a, b).
Fig. 1.
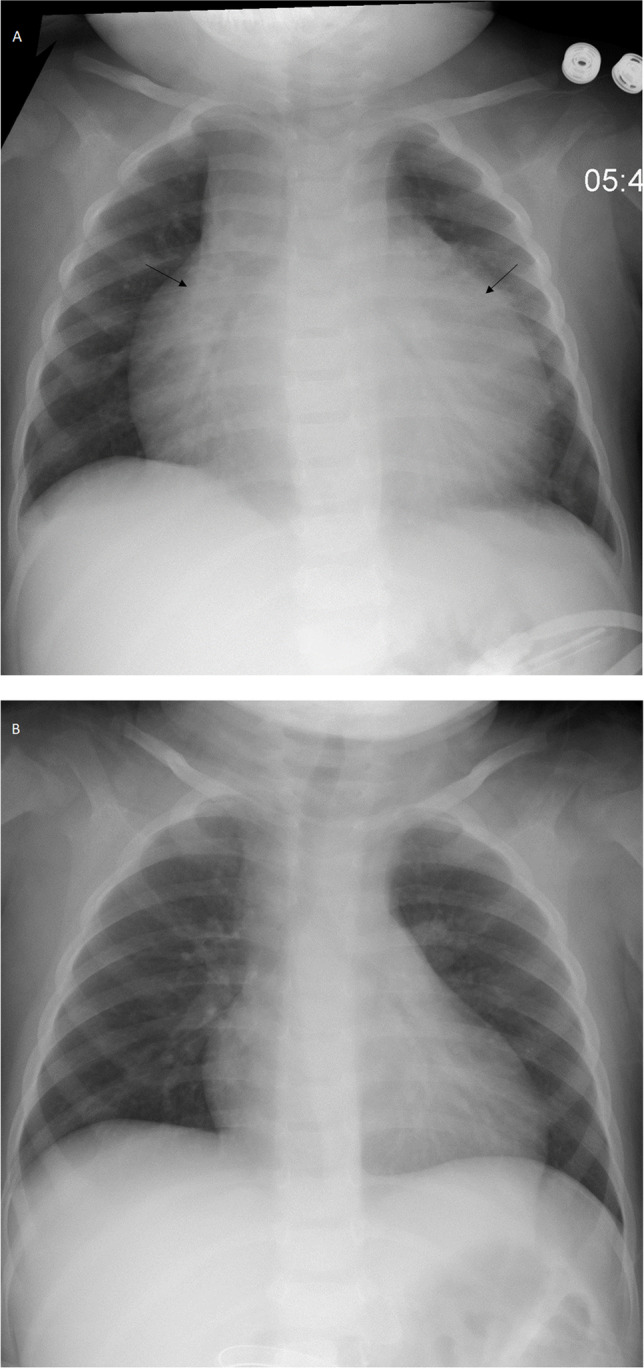
Chest radiograph showing markedly enlarged cardiac silhouette (arrows) (a) compared to the radiograph obtained 1 month prior to admission (b). Lungs are without pulmonary edema, focal consolidation, or pleural effusion
Questions
What would be your differential diagnosis for an enlarged cardiac silhouette in a toddler with advanced CKD?
What additional investigations would you perform?
How would you treat this patient?
Data availability
Not applicable.
Code availability
Not applicable.
Declarations
Conflict of interest
The authors declare no competing interests.
Footnotes
The answers to these questions can be found at 10.1007/s00467-021-05301-7.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.
Not applicable.