

Abstract
The Community Care Outreach Unit (CCO) of the Hawai‘i Emergency Management Medical/Public Health Services Branch conducted a survey to gauge the impact of coronavirus disease 2019 (COVID-19) on the health and social welfare of individuals and families in the state of Hawai‘i. A mixed-methods framework was utilized for survey distribution; 7927 respondents participated in the survey. This article presents key findings for the state's Hawai‘i County (HC). It presents a descriptive analysis of the data to provide a basic overview of the impact of COVID-19 in HC, as assessed in August-September 2020.
A total of 936 participants from HC responded to the survey. Approximately one-third reported that they or their family members experienced reduced work hours, and one-fifth lost their jobs because of COVID-19. Many reported difficulties paying for many types of living essentials and expected these difficulties to increase in the near future. Challenges for the fall school semester included lack of access to funds for school supplies and face-coverings. The majority perceived the severity of COVID-19 to be moderate/very high and most had at least a moderate level of knowledge about risks for developing severe COVID-19. Approximately half reported maintaining social distancing usually/all of the time, and about two-thirds reported wearing a face-covering usually/always when needed. Other barriers for COVID disease prevention and response included a lack of space for quarantine/isolation of family members, not having enough cleaning supplies, low knowledge of how to care for a household member with COVID disease and not having someone available to care for them if they contracted the virus.
The results provide a baseline for understanding the impact, needs, and threats to the health and social welfare of individuals and their families as a result of COVID-19 in HC. Local stakeholders can utilize this information when developing priorities, strategies, and programs to address the pandemic where needed.
Introduction
At the time of this publication the COVID-19 pandemic continues in the state of Hawai‘i and most places across the world. Nearly all communities and countries have been adversely impacted by this historic event. As of July 2, 2021, the state of Hawai‘i has recorded 36 120 cases of coronavirus disease 2019 (COVID-19).1 The County of Hawai‘i (HC), which makes up the entire island of Hawai‘i (also known as the Big Island), has recorded 3204 or 9.0% of the state's COVID-19 cases. This number of cases is low compared to HC's proportion of the state population, which is approximately 14.2%.2 As of July 2, 2021 the HC 14-day average was 8 new cases per day.1 Similar to other neighbor islands, HC experienced surges of COVID-19 cases over the 2020 year. The first surge was in March-April, the second in August–September, and the third in October 2020, when travel restrictions were eased to allow trans-Pacific and interisland travelers via the pre-travel testing program. The last surge of cases occurred during the late December 2020–January 2021 holiday season.
The Community Care Outreach Unit (CCO Unit) of the Hawai‘i Emergency Management (HI-EMA) Medical/Public Health Services Branch conducted an assessment to gauge the impact of COVID-19 on the health and social welfare of individuals and their families in Hawai‘i. The CCO Unit partnered with community leaders from the Native Hawaiian (NH), Pacific Islander (PI), and Filipino communities as well as social and health service organizations that support recognized vulnerable groups (including those who are houseless, aging, and living in rural communities). In doing so, the CCO Unit worked with its community partners to develop, distribute, and analyze a survey that aimed to assess the impact of COVID-19 and identify strategies to provide needed support. Assessment data was collected from individuals (N=7927) across the state during a period of three weeks (August 12–September 5, 2020). During this time the COVID-19 pandemic in the state was at its peak and public officials and citizens were all very concerned for the health and safety for citizens of the state. The findings for the state as a whole are reported elsewhere.3 This report provides findings that are specific to HC.
Methods
The CCO Unit worked closely with its community partners to develop the assessment tool, articulate a participant recruitment and distribution methodology, and analyze the results. The group then used a community-based action programming methodology to identify key challenges and potential solutions for the population at large and vulnerable groups.
The assessment survey tool included 35 questions, which collected information about demographics, household profiles, health and well-being, family finances, social welfare, personal beliefs and behaviors regarding COVID-19, and mental health.3 The survey was distributed August 12, 2020 through September 5, 2020 using a mixed-methods framework that relied on a convenience sample of HC adult citizens, with special outreach to recognized vulnerable populations. Recruitment strategies included snowball sampling via website and social media advertisements, word-of-mouth, and paper surveys along with return postage mailers. Please see State of Hawai‘i - A Report on the Impact of COVID-19 on Individual Health and Social Welfare3 for more details regarding the survey tool. Descriptive analysis of the data is presented here to give a basic overview of the status of the COVID-19 burden in HC.
Results
In HC, 936 individuals responded to the survey. This represents 11.9% of the overall survey respondents. HC has 201 513 residents, which represent 14.2% of the state population.2 Each respondent provided a zip code of residence. To assess the distribution of respondents across the HC, the numbers of respondents were mapped by zip code. Survey respondents came from all populated zip codes in the county (Figure 1).
Figure 1.
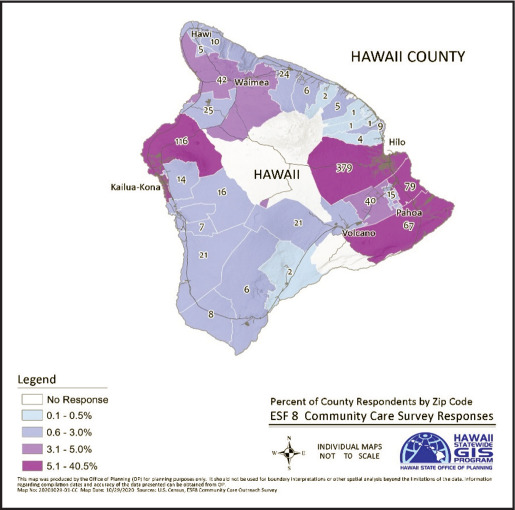
Hawai‘i County Survey Response by Zip Code
Demographics
In HC, as across the state, more females (72.3%) completed the survey than males (21.8%), with 5.9% responding as other gender individuals. This pattern is consistent with females being more apt to make healthcare decisions for the family and single-parent households are more often led by a woman.4
About one-third of respondents were young adults (18–34 years of age), one-third were middle-aged (35–54), and one-third were older (≥55 years). This closely aligns with the age distribution in the state.
Of the 936 respondents from HC who answered the questions about which race/ethnicity they identify with, 38% reported identity with more than 1 race/ethnicity group; Caucasian, Japanese, NH, Filipino, and Chinese were the most frequent groups reported.
When asked which 1 group they most closely identified with, the percentages changed for multiple groups; however, the order of frequency remained the same for the top 4 in HC: Caucasian (44.6%), NH (18.6%), Japanese (13.1%) and Filipino (8.2%). Three percent reported most close identification as a PI. When combining groups into more general categories, Caucasian, Asian, NH, and Filipino remained as the most predominant groups in HC. Table 1 illustrates the comparison of HC to state respondents in terms of gender, age group, and race/ethnicity group.
Table 1.
Characteristics of Hawai‘i County Respondents (N=936) Compared to All Respondents in Hawai‘i (N=7927)
| Hawai‘i County Respondents | Statewidea | ||
|---|---|---|---|
| nb | %c | % | |
| Gender | |||
| Female | 673 | 71.9 | 25.4 |
| Male | 203 | 21.6 | 69.3 |
| Non-binaryd | 55 | 5.9 | 5.3 |
| Age | |||
| 18–24 | 136 | 14.7 | 14.9 |
| 25–34 | 140 | 15.1 | 16.7 |
| 35–44 | 173 | 18.6 | 20.2 |
| 45–54 | 153 | 16.5 | 17.7 |
| 55–64 | 175 | 18.9 | 16.8 |
| 65+ | 151 | 16.3 | 13.8 |
| Race/Ethnicity | |||
| Caucasian | 411 | 44.6 | 34.8 |
| Filipino | 76 | 8.3 | 11.6 |
| Japanese | 121 | 13.1 | 19.4 |
| Chinese | 15 | 1.6 | 5.7 |
| Other Asian | 13 | 1.4 | 3.8 |
| Native Hawaiian | 172 | 18.7 | 14.3 |
| Pacific Islander | 28 | 3 | 3.4 |
| African American | 4 | 0.4 | 0.8 |
| Hispanic | 31 | 3.4 | 2.8 |
| Other | 50 | 5.4 | 3.5 |
All respondents in Hawai‘i.3
Totals may not equal to 936 due to unanswered/missing data.
Percentages may not equal 100% due to unanswered/missing data.
Non-binary refers to the self-reported sexual identity of the survey respondent.
Household Profile
The vast majority of respondents in HC reported having others living in their home (87.1%) as opposed to living alone; the mean number of people living in each household was 2.6. About one-third (30.7%) reported at least 1 older person ≥ 65 years (mean number of elders in each household 1.4), and a little more than one-third (36%) reported 1 or more child younger than 18 in their household (mean number of children in each household 1.8).
Digital Connectivity
The vast majority of HC respondents reported having internet access in the home or work, and less than 1% reported having no internet access at all. The vast majority (99.1%) also reported having access to a working cell phone. The residents of HC who responded to the survey have good connectivity that is comparable to the rest of the state.
Housing
More than half of HC respondents who answered the annual family income question reported a family income of $75 000 or less. The median annual household income in HC is $66 420.5 It should be noted that 110 respondents (11.8%) chose not to answer this question. Sixty percent (60.9%) reported that their family income decreased due to COVID-19, and about one-third (37.7%) reported the decrease as being moderate or large.
Approximately one-third (33.3%) of HC respondents reported that they or their family members experienced reduced work hours, and one-fifth lost their jobs (21.2%) because of COVID-19. A little more than one-third (37.4%) reported no change in work hours, and 8.1% reported an increase in work hours. The impact on employment in HC was significant, but also comparable to that of the state. Table 2 displays the data on household income and impact of COVID-19 on employment for HC as well as the statewide respondents.
Table 2.
Estimated Income and Impact on Employment and Work HoursAmong Hawai‘i County Respondents (N=936) Compared to All Respondents in Hawai‘i (N=7927) After COVID-19
| Hawai‘i County Respondents | Statewidea | ||
|---|---|---|---|
| nb | %c | % | |
| Income range | |||
| Less than $40,000 | 247 | 26.4 | 17.2 |
| $41,000 – $75,000 | 244 | 26.0 | 20.7 |
| $76,000 – $125,000 | 218 | 23.3 | 26.3 |
| $126,000+ | 117 | 12.5 | 22.1 |
| Choose not to answer | 110 | 11.8 | 13.7 |
| Impact on employment or work hours | |||
| No effect | 365 | 39.1 | 37.0 |
| Increased work hours | 217 | 23.2 | 11.2 |
| Reduced work hours | 161 | 17.2 | 32.2 |
| Lost job | 191 | 20.5 | 19.6 |
| Impact on income | |||
| No | 155 | 26.6 | 39.9 |
| Yes, a little | 137 | 23.5 | 24.4 |
| Yes, a moderate amount | 136 | 23.4 | 18.1 |
| Yes, a large amount | 154 | 26.46 | 17.6 |
All respondents in Hawai‘i.3
Totals may not equal to 936 due to unanswered/missing data.
Percentages may not equal 100% due to unanswered/missing data.
Chronic Disease Burden
More than one-half (56.3%) of HC respondents reported that at least 1 person in the household had at least 1 chronic disease. Consistent with statewide respondents, asthma, diabetes, obesity, mental health, and heart disease are prevalent in HC respondents’ households (Table 3).
Table 3.
Chronic Disease Burden Among Hawai‘i County Respondents (N=936) Compared to All Respondents in Hawai‘i (N=7927)
| Hawai‘i County Respondents | Statewidea | ||
|---|---|---|---|
| n | % | % | |
| Chronic disease | |||
| Diabetes | 149 | 16.2 | 19.1 |
| Heart disease | 111 | 12.0 | 12.5 |
| Asthma | 243 | 26.3 | 25.5 |
| Lung disease | 32 | 3.5 | 3.3 |
| Kidney disease | 24 | 2.6 | 3.8 |
| Mental health illness | 150 | 16.3 | 15.0 |
| Obesity | 187 | 20.3 | 18.9 |
| Cancer | 35 | 3.8 | 5.3 |
All respondents in Hawai‘i.3
Usual Source of Health Care
The majority of HC respondents (68.8%) reported that they went to a family doctor's office for health care, followed by a community health center (CHC; 22.0%) and hospital-based clinic (8.5%). Ten percent (10.1%) reported that they either used the emergency department (ED) as their usual source of healthcare or had no usual source of healthcare. In HC, a larger percentage of people use CHCs for health care compared to statewide respondents. These findings highlight the importance of CHCs in this rural county of the state. Table 4 includes the data on usual source of health care for HC respondents and all respondents in Hawai‘i.
Table 4.
Usual Source of Health Care Among Hawai‘i County Respondents (N=936) Compared to All Respondents in Hawai‘i (N=7927)
| Hawai‘i County Respondents | Statewidea | ||
|---|---|---|---|
| n | % | % | |
| Usual source of health care | |||
| Family doctor office | 642 | 68.8 | 70.9 |
| Community Health Center/ or Community | 203 | 22.1 | 12.4 |
| Hospital based clinic | 78 | 8.5 | 17.6 |
| Emergency Department | 47 | 5.1 | 4.0 |
| Have no usual source of health care | 46 | 5 | 4.4 |
| Other | 57 | 6.2 | 4.8 |
Mental Health
The survey tool included the 4 questions from the Patient Health Questionnaire-4 (PHQ-4) to assess emotions related to mental health (emotion level).6 A score was computed by assigning points for the level of each emotion, the stronger the negative emotion, the higher the score. Factors included nervous/anxious on edge, not able to stop/control worrying, little interest/pleasure, feel down/depressed.
More than half of HC respondents (54.7%) reported feeling nervous more than half of days or nearly every day in the past 2 weeks, and about one-fourth (26.8%) reported feeling worried more than half of days or nearly every day in the past 2 weeks.
A mental health score was computed via assigning points for the level of each emotion. Severe negative emotions were reported by a larger percentage of HC respondents (15.2%) compared with statewide respondents (11.5%; Table 5).
Table 5.
Mental Health Scores Among Hawai‘i County Respondents (N=936) Compared to All Respondents in Hawai‘i (N=7927)
| Hawai‘i County Respondents | Statewidea | ||
|---|---|---|---|
| nb | %c | % | |
| PHQ-4 Score | |||
| Normal (0–2) | 421 | 45.2 | 45.5 |
| Mild (3–5) | 226 | 24.3 | 27.6 |
| Moderate (6–8) | 141 | 15.2 | 15.5 |
| Severe (9–12) | 143 | 15.3 | 11.5 |
All respondents in Hawai‘i.3
Totals may not equal to 936 due to unanswered/missing data.
Percentages may not equal 100% due to unanswered/missing data.
Housing Situation
Fewer HC respondents, compared to statewide respondents, who currently own or rent a house or condo expected to be living in the same place in 3 months. The percentage who reported they expected to change their residence within the next 3 months is higher in HC compared to the state overall. Table 6 illustrates the magnitude of this expected change.
Table 6.
Housing Situation Today and Likely in 3 Months Hawai‘i County Respondents (N=936) Compared to All Respondents in Hawai‘i (N=7927)
| Housing arrangement | Hawai‘i County Respondents | Statewidea | ||
|---|---|---|---|---|
| TODAY where do you live | Where are you most likely tolive in 3 MONTHS? | TODAY where do you live | Where are you most likely tolive in 3 MONTHS? | |
| nb (%)c | nb (%)c | n (%) | n (%) | |
| A home, condo, or apartment that you OWN. | 610 (65.5) | 491 (52.7) | 4588 (58.2) | 3803 (48.2) |
| A home, condo, or apartment that you RENT. | 289 (31.3) | 255 (27.6) | 3005 (38.1) | 2578 (32.8) |
| Houseless, live with others that you know, in their home or apartment. | 34 (3.7) | 43 (4.7) | 272 (3.5) | 317 (4.0) |
| Houseless, live in a public shelter. | 2 (0.2) | 1 (0.1) | 22 (0.3) | 32 (0.4) |
| Houseless, live in a tent, car, or outside. | 3 (0.3) | 13 (1.4) | 13 (0.2) | 70 (0.9) |
All respondents in Hawai‘i.3
Totals may not equal to 936 due to unanswered/missing data.
Percentages may not equal 100% due to unanswered/missing data.
Daily Essentials
HC respondents reported difficulty paying for most of the essentials required for daily living at the time of the survey. This difficulty was expected to increase to more than 25% within the next 3 months for most categories, including food, rent/mortgage, utility bills, cell phone expenses, childcare, healthcare, transportation and other debts. See Table 7 for current and expected future difficulties with having enough money to pay for essentials among the HC respondents compared to all respondents in Hawai‘i.
Table 7.
Current and Expected Future Difficulties with Having Enough Money to Pay for Essentials Among the Hawai‘i County Respondents (N=936) Compared to All Respondents in Hawai‘i (N=7927)
| Hawai‘i County Respondents | Statewidea | |||
|---|---|---|---|---|
| Today n (%) | In 3 months n (%) | Today n (%) | In 3 months n (%) | |
| Essential | ||||
| Food | 136 (14.8) | 262 (28.3) | 979 (12.5) | 1821 (23.1) |
| Rent or mortgage | 140 (15.2) | 267 (28.9) | 1142 (14.5) | 2222 (28.2) |
| Auto expenses (e.g., gas, insurance, car payments) | 168 (18.2) | 280 (30.3) | 1099 (14.0) | 1942 (24.7) |
| Medicines | 79 (8.6) | 140 (15.2) | 657 (8.4) | 1206 (15.4) |
| Utility bills (e.g., electric, water, cable, internet) | 148 (16.0) | 248 (26.8) | 1090 (13.9) | 1839 (23.4) |
| Cell phone, internet, cable bill | 150 (16.2) | 245 (26.4) | 1055 (13.4) | 1741 (22.1) |
| Childcare/ elder care | 51 (5.6) | 82 (8.9) | 416 (5.3) | 720 (9.2) |
| Healthcare | 113 (12.3) | 189 (20.5) | 816 (10.4) | 1437 (18.3) |
| Public transportation | 23 (2.5) | 51 (5.6) | 312 (4.0) | 536 (6.8) |
| Other debts | 166 (18.0) | 264 (28.6) | 1244 (15.8) | 1966 (25.0) |
All respondents in Hawai‘i.3
Challenges with School
More than one-half (n=514; 54.9%) of HC respondents expected to have someone in their household physically return to school in fall 2020. Expected challenges included lack of funds to purchase school supplies (n=137; 14.9%), lack of face-covering (n=43; 4.7%), and language barrier (n=12; 1.3%).
Language Spoken Mostly in the Home and Translation Needs
The majority of respondents (n=872; 95%) reported English as the language most spoken in the home. Translation needs that were not met were reported by 10 respondents, most were for health (n=6), educational services (n=6), and social services (n=3).
Use of Statewide Assistance Hotline Number (211)7
Only 3% (n=25) of HC respondents reported that they ever called 211 for social service assistance. Of these 25 individuals, only 20% (n=5) reported that they received the assistance that they requested. When asked about specifics, 36.0% (n=9) reported they did not receive the assistance that they requested, and 56% (n=14) reported that they were only directed to an internet website.
Attempt at Applying for Assistance Benefits
Most of the HC individuals who applied for assistance benefits were able to complete the application for financial hardship relief, food stamps, and health insurance and health benefits. Application for rental assistance was the most challenging; only two-thirds were able to complete the application. The most common reasons for application challenges were related to difficulty with navigating the form, lack of proper documents, or trying to call on the phone but could not get through. These challenges are consistent with what others in the state reported. Table 8 provides a detailed summary of the percent of respondents who were able versus unable to complete each type of application and reasons for not having success.
Table 8.
Summary of Outcomes When Applying for Assistance Among Hawai‘i County Respondents (N=936)
| Type of Assistancea | If YES, applied for assistance, were you able to complete the application? | If you could not complete the application: Reason(s) [Check all that apply] | |||||
|---|---|---|---|---|---|---|---|
| Yes | No | No internet access | Could not figure out how to navigate the form | Did not have all the documents | Do not understand questions in English | Tried to call on phone but could not get through | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Prequalification for financial hardship relief | 97 (91.5) | 9 (8.5) | 1 (11.1) | 5 (55.6) | 2 (22.2) | 0 (0) | 4 (44.4) |
| Rental assistance | 19 (65.5) | 10 (34.5) | 1 (10.0) | 1 (10.0) | 2 (20.0) | 0 (0) | 2 (20) |
| Food | 118 (88.7) | 15 (11.3) | 1 (6.7) | 4 (26.7) | 6 (40.0) | 0 (0) | 2 (13.3) |
| Health insurance | 171 (95.0) | 9 (5.0) | 2 (22.2) | 2 (22.2) | 2 (22.2) | 0 (0) | 4 (44.4) |
| Healthcare benefits (e.g., Quest or WIC) | 136 (93.8) | 9 (6.2) | 2 (22.2) | 3 (33.3) | 2 (22.2) | 0 (0) | 2 (22.2) |
Abbreviation: WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Type of assistance applied for in Hawai‘i between August 12, 2020, and September 5, 2020.
Personal Beliefs and Activities Regarding COVID-19 Prevention
Participants were asked a series of questions about COVID-19 to assess their beliefs, knowledge, behaviors, and resources related to the pandemic. See Table 9 for factors that influence COVID-19 preparedness and response among HC respondents compared to statewide respondents.
Table 9.
Factors for COVID-19 Preparedness and Response Among Hawai‘i County Respondents (N=936) Compared to All Respondents in Hawai‘i (N=7927)
| Hawai‘i County Respondents | Statewidea | ||
|---|---|---|---|
| na | % | % | |
| Attitude Question | |||
| Perceived Severity of COVID-19 | |||
| Not serious | 20 | 2.1 | 1.7 |
| Low level | 42 | 4.5 | 3.7 |
| Moderate level | 136 | 14.6 | 12.4 |
| High level | 277 | 29.6 | 29.9 |
| Very high level | 459 | 49.2 | 52.4 |
| Knowledge Questions | |||
| Know vulnerable populations (elderly and chronic disease) | 579 | 61.9 | 66.3 |
| Know where to go for COVID-19 testing | 665 | 71.4 | 64.8 |
| Know how to provide medical care for someone at home with COVID-19 | 369 | 39.6 | 38.7 |
| Able to recognize when a family member with COVID-19 would need to go to the hospital | 637 | 68.4 | 69.4 |
| Behaviors Questions | |||
| Usually or Always practice social distancing by staying at least 6 feet away from others when not at home | 511 | 55 | 96.1 |
| Usually or Always wear a face-covering when outside of your home | 646 | 69.5 | 97.1 |
| Family members wash hands the same frequency or More frequently since COVID-19 | 835 | 89.6 | 99.8 |
| Have a thermometer that works at home | 658 | 70.5 | 75.8 |
| Resources Questions | |||
| Problems would face if someone lives with had COVID-19 | |||
| Lack of space for isolation | 489 | 52.5 | 55.6 |
| NO face mask | 24 | 2.6 | 2.4 |
| NO hand sanitizer | 56 | 6.1 | 5.7 |
| Not enough cleaning supplies | 285 | 30.8 | 31.2 |
| Have someone be available to care for you if you got COVID-19 | 460 | 49.5 | 53.8 |
Totals may not equal to 936 due to unanswered/missing data.
The majority of respondents from HC considered COVID-19 to be quite serious (78.8% consider it highly or very highly serious). There was a moderate to low level of knowledge about which groups are more at risk for contracting severe COVID-19; 61.8% knew it is the elderly and those with chronic disease, and 68.3% reported the ability to recognize if a family member with COVID-19 needed to go to the hospital. Seventy-one percent reported knowing where to go for COVID-19 testing but only 39.6% reported knowing how to provide care at home for someone in their family (or home) that has contracted COVID-19.
About half (54.9%) of HC respondents reported that they usually or always practice social distancing, and 69.3% said they wear a face covering usually or all of the time. The majority (89.5%) reported that their family members wash their hands the same or more often since the COVID-19 pandemic began. Seventy percent (70.5%) report having a working thermometer at home.
Multiple barriers for caring for a family member with COVID-19 in HC were reported. More than half (55.5%) reported a lack of space in their home for isolation or quarantine, and 30% reported they would not have enough cleaning supplies. About half (49.5%) reported that if they got COVID-19 there would be a family member available to care for them.
To assess overall household preparedness for COVID-19, scores were computed for each factor (attitude, knowledge, behavior, and resources). Overall, for HC there was a high level of positive attitude/belief regarding the seriousness of COVID-19, a moderate to low level of knowledge about COVID-19 disease, and a moderate to high level of positive behaviors for COVID-19 prevention and management (Table 10). Clear needs in the areas of space for isolation and someone in the home to provide COVID-19 care were identified. Most of these needs reported were similar to that of respondents from other counties in the state with the exception that more people in HC knew where to go for COVID-19 testing but a smaller percentage reported use of face coverings all of the time.
Table 10.
Overall Household Preparedness for COVID-19 Among Hawai‘i County Respondents (N=936)
| na | %b | |
|---|---|---|
| Attitude - Perceived Severity of COVID-19 (total 1 question) | ||
| Low (none-low) | 62 | 6.6 |
| Moderate (mod) | 136 | 14.6 |
| High level (high-very high) | 736 | 78.8 |
| Knowledge (total 4 questions) | ||
| Low level of knowledge (0–2) | 468 | 50 |
| Moderate level of knowledge (3) | 278 | 29.7 |
| High level of knowledge (4) | 190 | 20.3 |
| Behaviors – compliance with measures (total 4 questions) | ||
| Low level of compliance (0–1) | 116 | 12.4 |
| Moderate level of compliance (2–3) | 512 | 54.8 |
| High level of compliance (4) | 306 | 32.8 |
| Resources Needed (total 6 questions) | ||
| None (0) | 209 | 22.4 |
| Low level of needs (1) | 289 | 30.9 |
| Moderate level of needs (2–3) | 357 | 38.2 |
| High level of needs (4–6) | 80 | 8.6 |
Totals may not equal to 936 due to unanswered/missing data.
Percentages may not equal 100% due to unanswered/missing data.
Best Source of Accurate Information
While many sources of information were reported, the majority of respondents from HC reported that they used the Centers for Disease Control and Prevention (CDC) website (50.7%), followed by the Hawai‘i State Department of Health website (19.0%), television news reports (7.0%), and local community-based sources for reliable information about COVID-19. This is consistent with respondents from other counties in the state.
Burden of Challenges by Race/Ethnicity
The reported COVID-19 household preparedness and challenges were sorted by racial/ethnic group for each county. Across HC, PIs, NHs, and Filipinos carry a higher burden of challenges in multiple areas. Greater disparities were found for NH, PI, and Filipinos in the areas of burden of chronic disease and challenges with preparing students to return to school (Table 11).
Table 11.
Challenges for Special Groups Among Hawai‘i County Respondents (N=936)
| Caucasian n (%) | Filipino n (%) | Asian n (%) | Native Hawaiian n (%) | Pacific Islander n (%) | Other n (%) | |
|---|---|---|---|---|---|---|
| Connectivity | ||||||
| NO access to internet | 3 (0.73) | 1 (1.4) | 0 (0) | 1 (0.6) | 0 (0) | 0 (0) |
| NO working cell phone | 4 (1.0) | 0 (0) | 2 (1.4) | 2 (1.2) | 0 (0) | 0 (0) |
| Household chronic disease | ||||||
| Household has one or more people living with chronic disease | 202 (49.2) | 51 (67.1) | 84 (56.4) | 109 (63.4) | 19 (67.9) | 54 (63.6) |
| Challenges going back to school | ||||||
| Language barrier | 6 (1.5) | 2 (2.8) | 1 (0.7) | 1 (0.6) | 1 (3.9) | 0 (0) |
| Lack of face-covering | 8 (2.0) | 11 (15.3) | 2 (14.9) | 12 (7.2) | 1 (3.9) | 7 (8.3) |
| Lack of funds to buy school supplies | 40 (9.8) | 24 (33.3) | 16 (11.1) | 33 (19.3) | 5 (19.2) | 14 (16.7) |
| Other – computer, internet | 77 (18.8) | 23 (32.4) | 39 (26.9) | 58 (34.1) | 11 (42.3) | 27 (31.7) |
| Emotional Stress Level | ||||||
| Normal | 189 (46.2) | 35 (46.7) | 73 (49.3) | 71 (41.5) | 15 (53.6) | 31 (36.5) |
| Mild | 98 (24.0) | 24 (32.0) | 36 (24.3) | 45 (26.3) | 6 (21.4) | 13 (15.3) |
| Moderate | 57 (13.9) | 11 (14.7) | 15 (10.2) | 30 (17.5) | 3 (10.7) | 22 (25.9) |
| Severe | 65 (16.0) | 5 (6.7) | 24 (16.2) | 25 (14.6) | 4 (14.3) | 19 (22.4) |
Discussion
Demographics and Household Profile
With the exception of gender, the respondents from HC closely approximated the demographic distribution for the county. Compared to the statewide participants, HC households entered the pandemic with lower incomes in general.5 Tourism is a key industry in HC, and as a consequence of the higher restrictions on incoming travelers, the economy experienced a negative financial impact because of COVID-19. Many hotels and travel industry businesses suffered greatly as visitor arrivals by air dropped by 69.4% in the third quarter of 2020 as compared to 2019.8 Additionally, unemployment in HC increased to 11.9% in third quarter 2020, from 3.5% in the same time period in 2019.8
However, HC reported lower unemployment and economic impact from COVID-19 compared to the other neighbor islands of Maui and Kaua‘i (but still higher than the City and County of Honolulu). This may be due to a more diversified economy in HC that includes aquaculture, agriculture, natural energy, and ocean technology research and activities.9
Housing Situation
When asked if they expected to be in the same housing situation in 3 months, the percentage of participants who reported that they expected to be living in the same house or condominium dropped by 16.4% in HC. The assessment team projected that this number will increase once the Order under Section 261 of the Public Health Service Act to halt any evictions is allowed to expire on August 6, 2021.10
Daily Essentials
In HC, respondents across the board reported having problems paying for essentials at the time of the survey and expected the problems to increase in the coming 3 months. Almost one-third of the HC participants expected to have problems paying for food, rent/mortgage, auto expenses, utility bills, and cell/internet costs. Almost one-fifth of the HC participants reported that they expected to experience problems with paying for health care and medicines. These problems will likely be further exacerbated by the fact that many specialty health care resources are sparse in HC and may be available only on the island of O‘ahu. The need for transportation to O’ahu for healthcare reduces access and increases costs.
Chronic Disease Burden
Compared to the rest of the state, the HC participants reported a slightly higher percentage of having someone in the household with asthma and obesity, and a slightly lower percentage reported having a household member with diabetes. A general concern for the HC population is the ability to obtain timely health care. In particular, neighbor island patients need financial and logistical support when they require a higher level of care and need to travel off-island to Honolulu. However due to COVID-19, additional possible access barriers may include changes in work schedules, lack of health insurance due to reduced work hours, no primary care physician, inability to make time due to overlapping needs of the workplace/childcare/elderly parent care, government restrictions on movement, and cutbacks in transportation options.
Usual Source of Health Care
More than one-fifth of HC respondents reported that they obtain their primary care services at a local CHC, and 10.2% either have no source of health care or use the ED for such services. This illustrates the important role that the CHCs can provide in HC, which has a dispersed population that is spread across a large geographical area. Readily access to a reliable source of healthcare is essential during a pandemic.
Personal Beliefs, and Activities Regarding COVID-19 Prevention
Overall, there was a high level of knowledge among HC participants about the severity of COVID-19 and which groups are considered to be most at-risk. However, of concern is the fact that less than half of the HC participants reported knowing how to provide care for a family member if they get sick with COVID-19, and only about half (49.5%) reported that they would have someone who could care for them if they contracted the disease. This lack of capacity for COVID-19 care in the home was further exacerbated by the lack of space for social isolation. Also of concern is the COVID-19 preparedness behavior response by HC participants: Only slightly more than half of the HC respondents reported that they practice social distancing all of the time, and about one-third reported not wearing a face-covering all of the time. These actions may have been encouraged by a false sense of security perpetuated by the extensive travel restrictions of inter-island or transpacific travel and low daily average of COVID-19 cases. However, HC was and still remains at risk. COVID-19 has been shown to be unpredictable in the spread and mutation of the virus. As of July, 2021 HC has a lower COVID-19 vaccination rate compared to the Hawaii state as a whole.11 This is a concern. For HC, even before the pandemic, health care access has been a concern for this population with high rates of chronic disease. Strained resources during this pandemic may put the population at further risk for poor health outcomes.
Education on the prevention and care for those who have become ill is important in keeping the HC population safe, and there are many sources for gathering information on COVID-19. To facilitate increased access to culturally tailored information, public messaging that is targeted toward different groups must be crafted and delivered through relevant methods for each ethnic group. Individuals need specific instructions and the necessary tools to reduce the spread of COVID-19 and care for those who become ill. Locally based community health workers are likely to be an effective strategy to support COVID-19 disease prevention, detection and response activities. The Hawaii Department of Health initiated efforts to translate and develop special COVID-19 information materials that were culturally appropriate for the rural populations of HC, and its Public Health Nursing Branch developed a simple to read booklet to teach about homecare for a person with COVID-19 disease. Many of the county agencies in HC also developed specific programs to support the HC population during the pandemic. These efforts must continue in order to mitigate the risks and consequences of COVID-19 in HC.
Burden of Challenges by Race/Ethnicity
Consistent with the rest of the state, NH, PI, and Filipino respondents in HC reported higher burdens of chronic disease among their households, and challenges with preparing to return to school in the fall 2020. This is understandable, as these groups entered the COVID-19 pandemic less prepared to withstand the social and economic impact of the disease. This underscores the need to address the social determinants of health for all groups before such events occur in order to better prepare all groups to respond, thrive, and survive.
Limitations
A convenience-sampling frame was used; all responders were self-selected and there is no way to determine an actual response rate. Therefore, the report results must be viewed within the context of potential self- selection bias. In addition, while the survey was available in both paper form and online, the vast majority of respondents participated online. Thus, there is a chance that those with no access to the internet and hidden groups, such as the houseless, may not be adequately represented in the sample. In addition, all data were self-reported and not verified. However, there are consistent trends in responses across respondents from all of Hawai‘i counties, which lends credence to the findings. To mitigate some of these concerns, the community partners reviewed and corroborated the results.
Conclusion
The HC results revealed several areas of need that are consistent with statewide findings. The geographical distance from the other neighbor islands, suffering economy, and health care access challenges have placed the population of HC in a unique situation. This population was somewhat protected by the restrictions and isolation, however, it remained vulnerable due to limited access to care and COVID-19 fatigue, as evidenced by the lack of social distancing by many. Findings also highlight how the vulnerable populations (PI, NH, and Filipino groups) have been further challenged by the pandemic.
Overall, the statewide assessment was designed to identify the impact of COVID-19 on the health and social welfare of the peoples in Hawai‘i. After completion of the survey, the CCO Unit came together with its community partners to analyze and interpret the findings, and to compose a full report.2 This report was distributed widely to constituent groups, policy makers, and organizations that serve the health and social needs of the state's residents in order to inform decisions regarding allocation of resources to mitigate the effects of COVID-19 on the population. These findings will continue to be used to inform policies and programs that aim to mitigate the effects of COVID-19 on the people of HC.
Acronyms
- CCO Unit
Community Care Outreach Unit
- CDC
Centers for Disease Control and Prevention
- CHC
community health centers
- COVID-19
coronavirus disease 2019
- ED
Emergency Department
- HC
Hawai‘i County
- HI-EMA
Hawai‘i Emergency Management Agency
- ICS
incident command system
- NH
Native Hawaiian
- PHQ-4
Patient Health Questionnaire-4
- PI
Pacific Island
Conflict of Interest
None of the authors identify a conflict of interest.
References
- 1.Hawai‘i COVID-19 data. State of Hawai‘i – Department of Health Disease Outbreak Control Division | COVID-19 website. Available from: https://health.hawaii.gov/coronavirusdisease2019/what-you-should-know/current-situation-in-hawaii. Updated January 28, 2021. Accessed January 29, 2021.
- 2.County population facts for the state of Hawaii: July 1, 2010 through July 1, 2019. Department of Business, Economic Development & Tourism Census website. Available from: https://census.hawaii.gov/home/data-products/. Published March 26, 2020. Accessed January 2, 2021.
- 3.Qureshi K, Buenconsejo-Lum LE, Palafox N, et al. A report on the impact of COVID-19 on the health and social welfare in the state of Hawai‘i. Hawai’i J Health Soc Welf. 2021. In press. [PMC free article] [PubMed]
- 4.Matoff-Stepp S, Applebaum B, Pooler J, Kavanagh E. Women as health care decision-makers: implications for health care coverage in the United States. Journal of Health Care for the Poor and Underserved. 2014;25((4)):1507–1513. doi: 10.1353/hpu.2014.0154. [DOI] [PubMed] [Google Scholar]
- 5.Census data highlights. Department of Business, Economic Development & Tourism Census website. Available from: https://census.hawaii.gov/wp-content/uploads/2020/10/acs2019_1-yr_DBEDT-highlights.pdf. Published September 17, 2020. Accessed January 2, 2021.
- 6.Kroenke K, Spitzer RL, Williams JB, Löwe B. An ultra-brief screening scale for anxiety and depression: The PHQ-4. Psychosomatics. 2009;50((6)):613–621. doi: 10.1176/appi.psy.50.6.6137. [DOI] [PubMed] [Google Scholar]
- 7.Aloha United Way 211. Aloha United Way website. Available from: https://www.auw211.org/s/. Accessed January 12, 2021.
- 8.County economic conditions, 4th quarter 2020 Report. Department of Business, Economic Development and Tourism website. Available from: http://dbedt.hawaii.gov/economic/qser/county/. Published 2020. Accessed January 21, 2021.
- 9.Hasslinger T. Big Island economy is ‘Getting By’ as the pandemic persists. Honolulu Civil Beat Website. Available from: https://www.civilbeat.org/2020/12/big-island-economy-is-getting-byas-the-pandemic-persists/. Published December 21, 2020. Accessed February 18, 2021.
- 10.Temporary halt in residential evictions to prevent the further spread of COVID-19. National Archives website. Available from: https://www.federalregister.gov/documents/2020/09/04/2020-19654/temporary-halt-in-residential-evictions-to-prevent-the-further-spread-of-covid-19. Published September 4, 2020. Accessed January 3, 2021.
- 11.Hawaii DOVID-19 data. Hawaii Department of Health, Disease Outbreak Control Division Website. 2021. Jun 23, https://health.hawaii.gov/coronavirusdisease2019/current-situationin-hawaii/ Accessed July 12, 2021l.
- 12.Hawaii emergency management agency community based organizational capacity and needs for COVID-19 response and recovery survey full report. State of Hawaii Department of Defense website. Available from: https://dod.hawaii.gov/hiema/files/2020/06/ESF-8-CCO-Unit-Survey.pdf. Published June 12, 2020. Accessed February 5, 2021.