

Abstract
The COVID-19 pandemic has had a substantial and global impact on health care, and has greatly accelerated the adoption of digital technology. One of these emerging digital technologies, blockchain, has unique characteristics (eg, immutability, decentralisation, and transparency) that can be useful in multiple domains (eg, management of electronic medical records and access rights, and mobile health). We conducted a systematic review of COVID-19-related and non-COVID-19-related applications of blockchain in health care. We identified relevant reports published in MEDLINE, SpringerLink, Institute of Electrical and Electronics Engineers Xplore, ScienceDirect, arXiv, and Google Scholar up to July 29, 2021. Articles that included both clinical and technical designs, with or without prototype development, were included. A total of 85 375 articles were evaluated, with 415 full length reports (37 related to COVID-19 and 378 not related to COVID-19) eventually included in the final analysis. The main COVID-19-related applications reported were pandemic control and surveillance, immunity or vaccine passport monitoring, and contact tracing. The top three non-COVID-19-related applications were management of electronic medical records, internet of things (eg, remote monitoring or mobile health), and supply chain monitoring. Most reports detailed technical performance of the blockchain prototype platforms (277 [66·7%] of 415), whereas nine (2·2%) studies showed real-world clinical application and adoption. The remaining studies (129 [31·1%] of 415) were themselves of a technical design only. The most common platforms used were Ethereum and Hyperledger. Blockchain technology has numerous potential COVID-19-related and non-COVID-19-related applications in health care. However, much of the current research remains at the technical stage, with few providing actual clinical applications, highlighting the need to translate foundational blockchain technology into clinical use.
Background
A range of new digital technologies, such as 5G telecommunication networks, the internet of things (IoT), and artificial intelligence (AI) that uses deep learning and big data analytics, has emerged in the past decade. These technologies might have important potential applications and effects in health care.1, 2 The COVID-19 pandemic, which paralysed access to global health-care systems through unprecedented lockdowns and enforced physical distancing, has rapidly accelerated the development of these digital technologies to meet various health-care needs worldwide.3 Coordination of large-scale operations such as population-level mass screening, rapid contact tracing, supply chain management for vaccines and drugs, telemedicine consultations, and e-commerce expansion has prompted the adoption of a wide range of digital technologies.4, 5
Blockchain is a foundational digital technology that integrates multiple other such technologies (appendix pp 2–4).3, 6 In health care, blockchain could serve as a replacement to traditional distributed database management systems, which have generally been client-server databases with Structured Query Language or relational input.7 Although traditional distributed database management systems are an established platform in health-care systems, they have substantial limitations, such as the inability to support peer-to-peer data sharing, susceptibility to external adversaries (eg, hacking), and the absence of an immutable (ie, unchangeable) audit trail.7 With its unique features, such as transparency, traceability, non-repudiation (ie, inability to refute signature validity), disintermediation (ie, removal of intermediaries from a decision-making process), and immutability, blockchain could potentially address these issues, allowing it to deliver important advantages over conventional platforms (eg, distributed database management systems). By incorporating blockchain technology, a decentralised health-care data management system could be created that coordinates on-chain events (transactions that are recorded on the blockchain ledger) and off-chain events (those that occur outside of the blockchain and are generally too large to store on the blockchain; figure 1 ).
Figure 1.

Blockchain-based health-care data management system between multiple stakeholders (nodes) within a health-care ecosystem
Hybrid and private blockchains are maintained by permissioned parties (eg, hospitals and government agencies). Confidential health-care data are saved on-premise and governed by reputable hospitals, laboratories, or similar institutions. High-volume health-care data (eg, radiology image and genomic data) are stored in off-chain data storage (ie, not on the blockchain ledger) for cost savings. Options of on-chain data management can include the logging of Merkle tree roots or designating edge devices as light nodes with storage of a hash function for data integrity verification. Health-care data ownership is returned to patients, who can authorise data use to clinics, research institutes, and insurers during specified time periods. Data access rights and trading transitions are saved and tracked on transparent, immutable, and traceable-distributed ledgers based on a majority agreement consensus protocol. Blockchain-based tokenisation cultivates trustworthy health-care data marketplace and collaboration ecosystem. DNN=deep neural network.
Although widespread adoption of blockchain technology in health care might still be limited by various organisational, technological, and governance barriers, the COVID-19 pandemic has clearly accentuated the need for secure, decentralised, multipurpose platforms for coordination of large-scale transfer of sensitive information, such as contact tracing, vaccination status monitoring, and COVID-19 health certificate issuance.8 These needs provide a strong impetus for a concerted effort to drive greater adoption and eliminate some of these barriers to a general adoption of blockchain technology.
However, to achieve durable and sustained effects, external one-off factors that can push towards adoption of these technologies, such as COVID-19 alone, are unlikely to be sufficient. The health-care community as a whole would need to develop greater understanding, literacy, and targeted research in blockchain technology and its clinical applications.7, 9, 10, 11, 12, 13, 14 Therefore, our aim was to perform a systematic review of the use of blockchain technology in health care, with identified use cases specifically categorised into COVID-19-related and non-COVID-19-related applications (eg, medical supply chain management and contact tracing).
Methods
Systematic review
We conducted a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Our goal was to identify original research articles focused on blockchain applications in health care, with a distinction between COVID-19-related and non-COVID-19-related uses.
We included all publications that matched the following search criteria: original research articles, conference proceedings, or preprints proposing specific health-care applications and blockchain technical design with or without prototype development; in English exclusively; and published between Jan 1, 2016, and April 10, 2021. During the peer review process, we elected to update our search and included articles published up to July 29, 2021. Due to the absence of common standards of reporting of blockchain research (compared with AI publications), we kept the search definition broad, with the specific intention of avoiding the exclusion of relevant publications. We excluded duplicates; reviews, opinions, or surveys; articles without an available full-text; and articles without an English full text. The completed Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist is included in the appendix (pp 5–7).
Search strategy and selection criteria
To identify potentially relevant research articles, we conducted a cross-discipline search of databases from inception to July 29, 2021. We searched in electronic bibliographic databases of published research (PubMed including MEDLINE, Institute of Electrical and Electronics Engineers [IEEE] Xplore, and other databases for research including ScienceDirect, SpringerLink, and arXiv) using the Boolean operators “AND/OR” on July 30, 2021. Search within the medicine-focused PubMed database was performed with the terms “blockchain [title]” OR “distributed ledger [title]”. For non-medicine-focused databases such as arXiv, IEEE Xplore, SpringerLink, and ScienceDirect, the search terms used were (“blockchain [Title]” OR “distributed ledger [title]”) AND (“health [in text]” OR “medical [in text]” OR “healthcare [in text]” OR “COVID [in text]”). In addition, we searched Google Scholar to identify original research articles located in grey literature. Due to the structured search function of Google Scholar, we searched using the “all-text” function with both search strings of “blockchain” AND (“health” OR “medical” OR “healthcare” OR “COVID”); or “distributed ledger” AND (“health” OR “medical” OR “healthcare” OR “COVID”). Health-related search terms were derived and selected on the basis of published literature that previously assessed the robustness of these search terms.9 This search strategy was drafted and refined through discussion between the authors. Due to the increased attention and pace of development of blockchain as a result of the on-going COVID-19 pandemic, we decided to include preprint articles to ensure the relevance of our review. The search results were subsequently exported to Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) for screening.
Screening and article selection
We selected articles on the basis of the available information in the indexed database (title and abstract). The selection was based on relevance for blockchain use in health care and categorised into COVID-19-related and non-COVID-19-related indications. Screening was done in a stepwise manner by one reviewer knowledgeable in blockchain and health care (Reviewer 1, WYN). First, duplicate articles were excluded. Second, article titles were reviewed, and articles that showed no relevance to blockchain in health care were discarded. Third, review articles, opinions, and surveys were excluded. Fourth, the abstracts of the remaining articles were reviewed. At this stage, only original articles that involved specific use case conceptualisation with description of technical development, proof of concept, or clinical execution were retained; abstracts of previously unidentified editorials, letters, reviews, or opinions were excluded. Finally, the full texts of selected articles were reviewed in entirety to ensure relevance before abstraction of the required information.
Data abstraction
A standardised data abstraction form was developed using Microsoft Excel. A full-text review of the selected articles was done independently by two reviewers (WYN and T-ET). Articles that described any of the following were deemed to fulfil the technical design criterion: description of a blockchain consensus protocol, platform, technical design, or functional prototype. To ensure consistency in data abstraction, a data abstraction pilot was first performed by both reviewers. A list of studies consisting of 10% of all identified full-text reports was created with a computer-generated random sequence. Independent data charting was done by both reviewers for the randomly selected studies, and the results were subsequently discussed. Disagreements were resolved by consensus between the two reviewers. If a consensus could not be reached, a final decision was subsequently made by a third reviewer as tie breaker (AHSF). The data extraction form used is presented in panel 1 , along with a further detailed description of definitions, criteria, and classification. Results were collated and analysed quantitatively. Missing data was handled by pairwise deletion without imputation. The findings were first divided into COVID-19-related and non-COVID-19-related applications, followed by categorisation according to clinical and technical design. Because of the heterogeneity between the studies, all findings were synthesised through a narrative review approach and presented on tables or bar charts. Considering the technical design focus and narrative approach, doing an assessment for potential biases in each individual study or a meta-analysis was deemed infeasible.
Panel 1. Data elements abstracted from selected articles.
Author
Surname of first author
Title
Title of the article
Year
Publication year of the article
Platform name
Name of blockchain platform used in the article (eg, Hyperledger or Ethereum); articles that did not specify the name of the platform used were categorised as not specified
COVID-19-related use
Related to COVID-19 or not related to COVID-19
Indication
-
•
Authentication or authorisation (reports on patients or report authentication or authorisation of accessing personnel)
-
•
Clinical trials and research (reports on the use of blockchain for general research purposes, such as monitoring and managing data access, transfer of clinical data and audit in clinical trials, and data analytics)
-
•
Contact tracing
-
•
Electronic medical records (reports on decentralised sharing, patient-centric access rights control, tamper-proof recording with audit trail, and security and data provenance assessment)
-
•
Epidemic and infection control
-
•
Foundational health-care framework (reports on technical design for an application-agnostic platform for health care)
-
•
Genomics (reports pertaining to control, decentralised sharing, democratisation, or security of genomic information)
-
•
Health and vaccine passports or certificates
-
•
Health-care insurance
-
•
Health-care services (reports pertaining to miscellaneous health-care services including, but not limited to, appointment management, clinical load balancing, or allied health services)
-
•
Medical diagnostics
-
•
Medical education
-
•
Mobile health, remote monitoring, or internet of things applications (reports detailing use of edge or fog devices for clinical monitoring, remote monitoring, and mobile health or research)
-
•
Notarisation
-
•
Pandemic (COVID-19) control and surveillance (reports on movement monitoring, infection monitoring, or aggregation of pandemic information for COVID-19)
-
•
Patient consent
-
•
Reports on artificial intelligence, big data, or federated learning for clinical or research applications
-
•
Supply chain (reports on supply chain monitoring for drugs and medical equipment and addressing issues of manufacturing, logistics, distribution, sales, and fraudulent activities monitoring in the sector)
-
•
Telemedicine
Results
Any simulated or real-world application results:
-
•
Greater weight was applied to studies with executable prototypes and reported simulation results (eg, latency and throughput), which were classified as simulated results
-
•
Studies limited to a working prototype, interface, or demonstration of technical design were classified as nil
Results
The search flow for this systematic review is shown in figure 2 . Our search results retrieved 85 375 initial records, of which 68 901 were unique. All titles and abstract information available in the databases were screened and 68 409 reports were excluded accordingly. The remaining 492 reports were then reviewed in full and assessed for eligibility. A total of 415 reports (31 preprints, 135 conference proceedings papers, and 249 original research articles) were eventually included in this systematic review for data charting and analysis (appendix pp 8–41).
Figure 2.
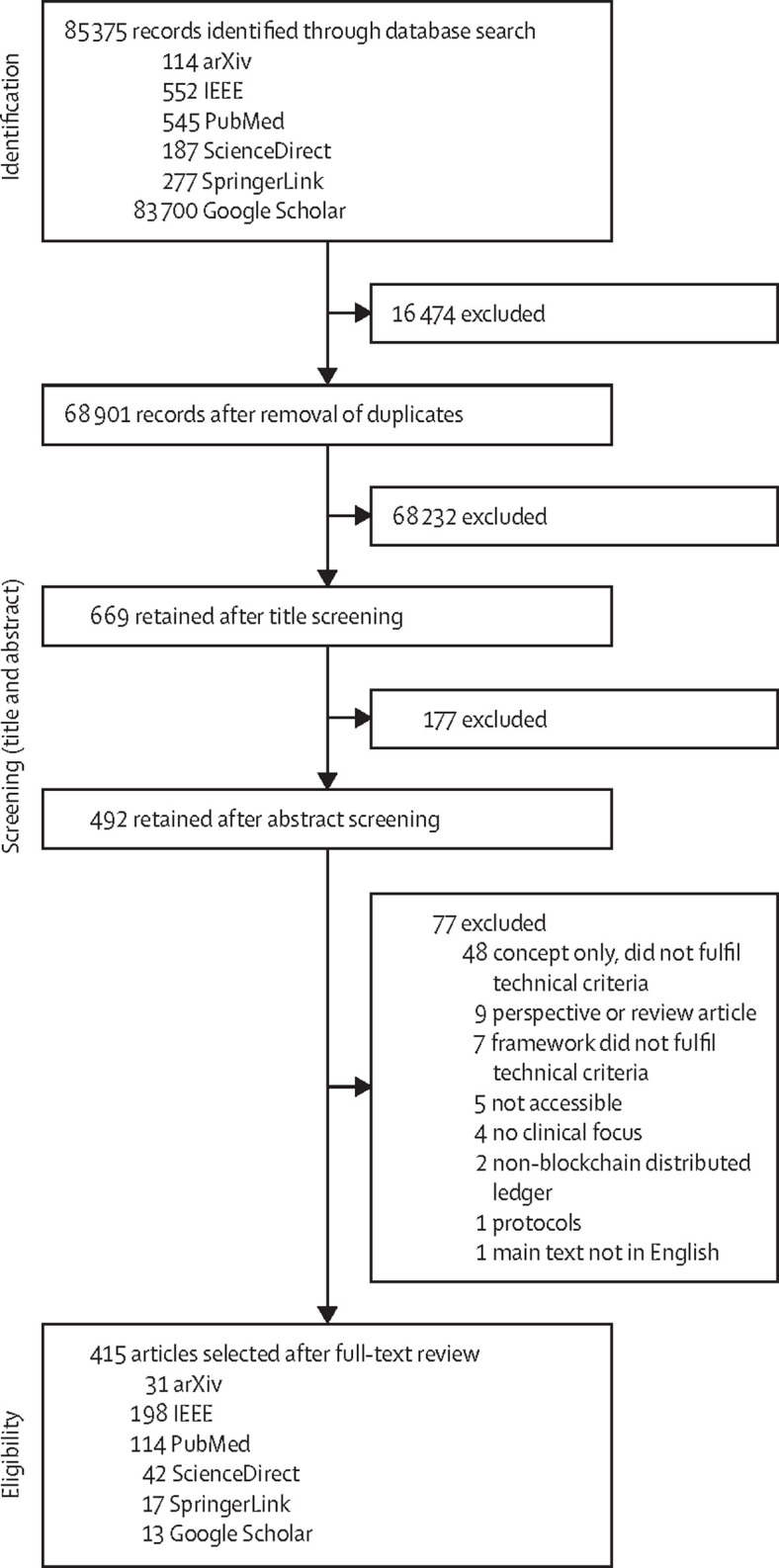
Preferred Reporting Items for Systematic Reviews and Meta-analyses flow diagram of the article selection process
Of a total of 85 375 initial articles, 415 were eligible for data abstraction. The most common sources for the selected articles were IEEE Xplore followed by PubMed. IEEE=Institute of Electrical and Electronics Engineers.
The key features of the 415 articles are shown in panel 2 . The majority were published in engineering journals (257 [61·9%] of 415), whereas others were in cross-disciplinary (145 [34·9%] of 415) and medical (13 [3·1%] of 415) journals. A noticeable tendency was an upsurge in relevant research articles published between Jan 1, 2018 (n=50), and Dec 31, 2020 (n=170). COVID-19-related blockchain research accounted for 37 reports since the start of 2020, when SARS-CoV-2 had begun to spread globally. Of these 37 reports, one reported dual applications,10 resulting in a total of 38 applications identified. Within these applications, the majority were related to pandemic control and management of surveillance records (11 [28·9%] of 38), whereas others focused on health, immunity or vaccine passports and certification (9 [23·7%] of 38), or contact tracing (8 [21·1%] of 38). In contrast, non-COVID-19-related research showed clearly different areas of emphasis. Among these papers, the most common clinical application was electronic medical records management (185 [47·2%] of 392), which included a variety of functions, such as decentralised sharing, patient-centric access rights control, tamper-proof recording with audit trail, and security and data provenance assessment. The second most common clinical application was the use of edge or fog devices (ie, pieces of hardware that enable connectivity and control traffic between two networks), such as IoT, for remote monitoring and mobile health (83 [21·2%] of 392). The third largest indication involved drug or equipment supply chain monitoring that addressed manufacturing, logistics, distribution, sales, and surveillance of fraudulent activities within the sector (27 [6·9%] of 392).
Panel 2. Results of reports included in this systematic review.
Total articles selected
415
Publications by year
-
•
2016: three articles
-
•
2017: eight articles
-
•
2018: 50 articles
-
•
2019: 96 articles
-
•
2020: 170 articles
-
•
2021 (up to July 29: 88 articles)
Clinical application
COVID-19-related applications
37* articles, covering:
-
•
Pandemic control and surveillance (11 articles)
-
•
Health and vaccine passport or certificate (nine articles)
-
•
Contact tracing (eight articles)
-
•
Electronic medical records (four articles)
-
•
Artificial intelligence, big data, or federated learning (three articles)
-
•
Supply chain (two articles)
-
•
Clinical trials (one article)
Non-COVID-19-related applications
378† articles, covering:
-
•
Electronic medical records (185 articles)
-
•
Mobile health, remote monitoring, and internet of things (83 articles)
-
•
Supply chain (27 articles)
-
•
Artificial intelligence, big data, or federated learning (16 articles)
-
•
Genomics (15 articles)
-
•
Clinical trials and research (14 articles)
-
•
Telemedicine (11 articles)
-
•
Patient consent (eight articles)
-
•
Health-care services (seven articles)
-
•
Authentication or authorisation (six articles)
-
•
Foundational health-care frameworks (six articles)
-
•
Insurance (six articles)
-
•
Contact tracing (two articles)
-
•
Epidemic and infection control (two articles)
-
•
Medical diagnostics (two articles)
-
•
Notarisation (one article)
-
•
Medical education (one article)
Types of platform used ‡
-
•
Ethereum (150 articles)
-
•
Hyperledger (107 articles)
-
•
MultiChain (eight articles)
-
•
BigchainDB (four articles)
-
•
IOTA (four articles)
-
•
Bitcoin (three articles)
-
•
DAG (three articles)
-
•
RAFT (three articles)
-
•
Tendermint (two articles)
-
•
Gcoin (one article)
-
•
Kaleido (one article)
-
•
KSI Blockchain (one article)
-
•
Modex BCDB (one article)
-
•
Mystiko (one article)
-
•
NEM (one article)
-
•
Oasis (one article)
-
•
Polkadot (one article)
-
•
Quorum (one article)
-
•
RepuCoin (one article)
-
•
Ripple (one article)
-
•
Stellar Consensus Protocol (one article)
-
•
Not specified (126 articles)
Reporting results
COVID-19-related
-
•
Simulated (24 articles)
-
•
Clinical case study (one article)
-
•
Nil (12 articles)
Non-COVID-19-related
-
•
Simulated (253 articles)
-
•
Clinical trial (eight articles; including one reporting mainly on user experience)
-
•
Nil (117 articles)
We further analysed the technical aspects of blockchain use in these reports. Ethereum (150 [35·5%] of 422) was the most frequently used blockchain platform, followed by Hyperledger (107 [25·4%] of 422). However, a substantial proportion of these studies did not specify the platform that their blockchain was designed on (126 [29·9%] of 422). On the other hand, there were seven studies that either made interplatform comparisons or used dual blockchain architecture (such as Ethereum vs Hyperledger, or BigchainDB and Hyperledger as a dual blockchain architecture). Most reports provided evidence of technical simulation and performance indicators, such as latency, throughput, load variation with node participation, and financial cost of transaction (COVID-19-related: 24 [64·9%] of 37; non-COVID-19-related: 253 [66·9%] of 378; figure 3 ).
Figure 3.
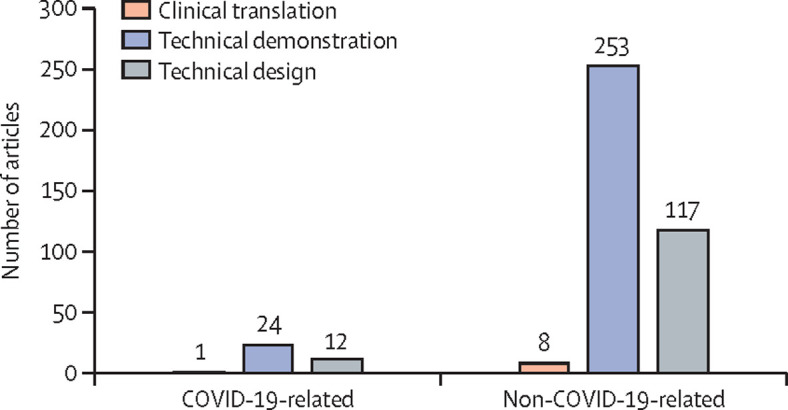
Distribution of studies based on clinical translation, technical demonstration, and technical design
Studies without demonstration of technical results were classified as technical designs. Most studies underwent technical demonstration and reported simulation results including block file sizes, latency, throughput rates, and horizontal scalability.
Notably, there were very few reports that involved real-world clinical implementation, with either clinical trial results or user experience assessments. Only nine reports provided clinical results, of which only one article focused on user experience. This particular article proposed a medical document monitoring system that alerted patients to any changes made to their medical documents, with patients showing strong interest in this blockchain application.
We found inconsistencies and poor standardisation on the disclosure of the underlying blockchain consensus mechanisms, which can be problematic because inference of the consensus mechanism based on the identified blockchain platform alone (eg, Ethereum) can be misleading in light of technological improvements, such as the switch from Proof of Work to Proof of Stake between Ethereum 1.0 and Ethereum 2.0.11
Finally, we looked for year-over-year trends in the foci of non-COVID-related research between Jan 1, 2018, and July 29, 2021 (figure 4 ). Before 2018, the absolute numbers of reports were small, which precluded a meaningful analysis of research foci. For every year from 2018 onwards, the top three research foci have consistently been: electronic medical records; mobile health, remote monitoring, or IoT usage; and supply chain monitoring. Electronic medical records research has seen the most substantial year-over-year increase (70·0% in 2018–19 [from 30 papers, in 2018, to 51 papers, in 2019], and 39·2% in 2019–20 [from 51 papers, in 2019, to 71 papers, in 2020]). Beyond these top three applications, we have also observed increasing research interest in the use of blockchain to facilitate the management of genomics, telemedicine, AI, big data, and federated learning.
Figure 4.
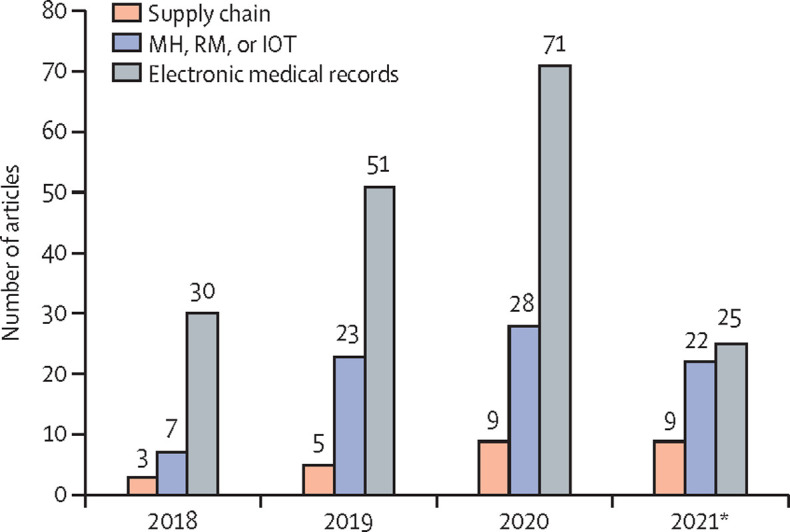
Trends in non-COVID-19 blockchain research over the past 4 years for the three most common clinical applications
The top three most common applications are supply chain monitoring; mobile health, remote clinical and research monitoring, and internet of things for eHealth; and electronic medical records monitoring, storage, sharing, and access control. MH=mobile health. RM=remote monitoring. IoT=internet of things. *Up to July 29, 2021.
Discussion
Our systematic review provides a summary of the current state of research with blockchain technology for both COVID-19-related and non-COVID-19-related applications in health care. Key findings are, first, that COVID-19-related research clearly has different areas of emphasis compared with non-COVID-19-related research, and focuses predominantly on pandemic control and surveillance, contact tracing, and immunity or vaccine passports. Although some reported applications (eg, vaccine supply chain monitoring) could be considered extensions from non-COVID-19-related indications, most applications (eg, COVID-19 immunity certificates or movement monitoring and control) are quite distinct.12, 13 Second, electronic medical records are the most common focus of blockchain research, but the scope of research has been substantially expanded to include other applications in the past 4 years. These applications include areas of blockchain application such as telemedicine14, 15, 16, 17 and supply chain monitoring.16, 17 These differences in the applications of blockchain technology are illustrated in the appendix (p 42). Third, the majority of the studies reviewed demonstrated technical simulation results, but only a few were actually trialled in clinical settings. Finally, most of the blockchain platforms were designed either on Ethereum or Hyperledger. However, an important proportion of studies did not specify the exact platform used, which might be due to an absence of standardised reporting guidelines.
COVID-19-related applications of blockchain
The COVID-19 pandemic has necessitated the coordination and management of large amounts of data. First, these data are usually sensitive, but need to be easily verifiable and managed transparently.8, 18 However, if these data management platforms were to grant full access of the data to central authorities, important privacy concerns could be raised, which might in turn be counter-productive.19, 20 To address these concerns, Garg and colleagues21 developed a blockchain-based movement pass that relies on smart contracts and tokens (tokens-based movement passes) that dispense the need for personal particulars for verification purposes. Separately, Xu and colleagues22 demonstrated a viable blockchain platform (with data acquisition via IoT) that can desensitise a user's identity and location information through its hash function, thereby ensuring the protection of the identity of patients with COVID-19 and the privacy of the public in a decentralised environment. These examples highlight how blockchain solutions can overcome the challenge of collating verifiable, yet de-identified, tracking data.
Second, the implementation of rapid, widespread testing and vaccination strategies might also require the introduction of health and immunity certificates. Blockchain technology can provide a secure and decentralised environment for cross-border verification of COVID-negative or immunity status.23, 24, 25 Eisenstadt and colleagues23 used a consortium, Ethereum-based blockchain architecture combined with a mobile application to achieve instant verification of tamper-proof test results, achieved through the use of public or private key pairs generalised to avoid restrictive ownership of sensitive keys or data. In a separate, unique study by Chaudhari and colleagues,26 the authors stored COVID-19 vaccination details of each recipient on-chain on a publicly readable platform, and authenticated users and anonymously located vaccination records with an iris extraction technique, which allowed them to hide the input and avoid leakage of any personal identifiable information. Concerns about scalability, latency, and storage were also addressed in a separate study, where Hyperledger Fabric architecture and a distributed system for file storage and access (Interplanetary File Storage)27 were adopted in a simulated, high-travel volume European Member State environment, achieving satisfactory results at a peak of 100 transactions per s.28
Third, there is greater scrutiny over the management of supply chains for vital supplies, such as personal protective equipment, essential medications, and COVID-19 vaccines.29, 30, 31, 32, 33 Precise monitoring can be done at a granular level with IoT, oracles, and Application Programming Interfaces for each individual vial or package. In a study by Antal and colleagues,34 IoT sensor devices were combined with self-enforcing smart contracts on an Ethereum blockchain platform to achieve end-to-end tracking and visibility, thereby ensuring the veracity of COVID-19 vaccine distribution data. In addition, the proposed system also addressed a major concern about such vaccines, by also supporting on-chain recording of side-effects. Ahmad and colleagues35 instead demonstrated the use of blockchain to manage an entire forward supply chain and waste management of COVID-19-related medical equipment and supplies. Similarly, their blockchain was designed with Ethereum architecture in combination with smart contracts, highlighting the versatility of Ethereum.
Fourth, a secure, decentralised, peer-to-peer network could also be used for telemedicine initiatives, including test kit management14 and medical data sharing amongst trusted stakeholders.36, 37 In a study by Kumar and Tripathi,36 a consortium network blockchain was created for the sharing of COVID-19-related reports (eg, chest CT scans). The blockchain was designed to identify and validate these reports before they were stored on-chain, by comparing the similarity of the perceptual hash of each report with existing on-chain perceptual hashes, thereby filtering out non-COVID-19-related reports. Lee and colleagues38 created a global International Patient Summary electronic medical record system using Proof of Authority consensus. The system supported real-time uploading from clinic electronic medical records systems using a combination of open Application Programming Interface and Fast Healthcare Interoperability Resources. This way, they could provide timely public updates on the pandemic, assist authorities with dynamic adjustment of health-care policies, and support pandemic research.
Non-COVID-19-related applications of blockchain
Apart from the immediate focus on COVID-19, blockchain applications in digital health have been described in several other key health-care domains: authentication and electronic medical records management;39, 40 clinical trial research and consent management;41, 42 health-care insurance claims processing;43 research data transfer and AI model development;44, 45 genomics;46 supply chain encryption for medical supplies;16, 47 and mobile health and IoT.46, 48
First, blockchain technology is an effective digital technology to manage electronic medical records, with the ability to assign controlling rights to patients.49 Such studies identified in this systematic review varied in their approach, with strategies including the use of shared keys in the event of the death of the patient (key-holder);50 electronic medical records maintenance in a unified viewpoint;51 secure cloud-based electronic medical records;52 enhanced interoperability;53 fine-grained access;54 and privacy-preservation techniques.50, 55, 56 In one of the few clinically trialled blockchain platforms we found, Lo and colleagues57 integrated medical data from the National Medical Record system in Taiwan with clinic electronic medical records to create an alliance-based medical referral system. They also used a patient-centric approach by further developing an additional blockchain-based decentralised application to grant access rights and data control to patients, which allowed them to demonstrate a viable decentralised referral system and strong patient interest in accessing their own medical data.
Second, application of blockchain has been explored for the management of clinical trials to potentially improve transparency and auditability. Benchoufi and colleagues58 used the automatic execution of blockchain to monitor clinical trial events, including voluntary consent, in a pre-set chronological order. This automatic execution could be further extrapolated for use in the context of clinical consent for procedures or treatment to combat medicolegal fraud.59 In health-care insurance, a distributed ledger could improve the claims process by enhancing security and decreasing the overall time taken to reach settlement.60 When insurance claims are recorded immutably on-chain, the required transparency to deter fraudulent activities might be reached.61 However, as highlighted by Mackey and colleagues,61 the feasibility of such systems is likely to hinge on their ability to establish interoperability with off-chain databases.
Third, blockchain technology could facilitate medical research collaboration, especially in the field of AI development with privacy-preserving technologies. Several of the studies identified combined federated learning with blockchain technology to improve AI development and generalisability.62, 63 Kumar and colleagues,64 however, suggested that local model weights be distributed on a decentralised blockchain network. Tan and colleagues44 showed proof of concept through a permissioned blockchain platform to allow secure data transfer, transparent reporting of AI model performance, and model transfer and testing on an external dataset, which might provide health regulators (eg, the US Food and Drug Administration) with a means to effectively audit and verify future diagnostic performance of AI algorithms for regulatory approval. To further enhance privacy-preservation and decentralisation of AI training, Warnat-Herresthal and colleagues65 proposed a combination of blockchain and swamp learning as the next evolution beyond federated learning, in which way the central custodian is dispensed with and the data and parameters are kept at the edge.
Fourth, another area of blockchain research interest is the class of so-called omics technologies (eg, genomics, proteomics, and metabolomics) and genetics. This interest in blockchain technology stems from concerns about the ability of centralised databases to manage such highly confidential data.66, 67, 68, 69 In one of the few studies to use commercially available blockchain platforms, Jin and colleagues46 described the use of genomic blockchain Life Code, which is designed with the Ethereum architecture. The platform facilitated access to genomic data by establishing a secure trading system through the use of tokens. Separately, Glicksberg and colleagues70 conducted a prospective cohort study for dissemination of de-identified clinical and genomic data of patients with late-stage cancer and reported two key findings. The completeness of the electronic medical records extracted by the blockchain platform was comparable with registry reports, which allowed rapid dissemination of real-world data. Furthermore, they reported that patients with cancer were increasingly willing to share their data for the development of medical knowledge.
Fifth, the medical supply chain, especially for pharmaceutical drugs, is particularly complex, with widely distributed geographical networks. During the assessment of blockchain viability, Tseng and colleagues47 also noted that the use of traditional devices, such as barcodes and radiofrequency identification, have so far failed to prevent counterfeit drug fiascos, even in high-income regions, such as Taiwan. They instead showed the viability of a Proof of Work consensus using a commercial blockchain platform (GCoin) and further suggested the development of a smart-contract-based open-governance surveillance net. Lower-income countries, such as the Philippines, also face similar drug safety concerns. To address this issue, Sylim and colleagues17 embarked on the development of a pharmacological surveillance blockchain system to support information sharing along the official drug distribution network, using either delegated Proof of Stake or Practical Byzantine Fault Tolerance to achieve scalability and adaptability. In these examples, blockchain technology serves to create a trust mechanism to track and authenticate pharmaceuticals while protecting the supply chain from malicious attacks.
Finally, patient-centric care requires close monitoring. Advances in IoT technology supported by edge or fog computing serve to bring blockchain functionality to the patient level. Ali and colleagues71 combined blockchain with medical IoT to deliver remote patient monitoring, such as cardiac monitoring, sleep apnoea testing, and electroencephalogram monitoring. In their study, they addressed inherent blockchain and IoT issues, such as privacy and scalability, by adopting a hybrid of on-chain (public blockchain for authentication and record keeping) and off-chain solutions (Tor hidden services for data transfer). Although most of the studies included in this Review were designed with either Ethereum or Hyperledger, Brogan and colleagues72 explored the use of the IOTA protocol (open-source distributed ledger technology), which is an inexpensive platform specifically designed for computationally light-weight IoT. With this blockchain platform, they were able to broadcast and receive authenticated, encrypted activity data from a wearable device. In a broader setting, such functionality might enable remote monitoring and mobile health for clinical or research purposes in the future.
Future directions of research in blockchain
The COVID-19 pandemic has potentially lowered barriers to the entry of new and innovative digital technologies into health care by altering mindsets in favour of such technologies. This change can be inferred from the greater numbers of COVID-19-specific blockchain applications evaluated in response to the global pandemic. What is required, as shown by our findings, is to successfully bridge the divide between simulation and actual clinical implementation. For this bridging to occur, several issues need to be addressed. First, interoperability using open standards such as Fast Healthcare Interoperability Resources will be required. Next, transactional costs and efficiency will need to be deliberated. For example, platforms that use Ethereum would incur ether gas fees, whereas others built on Hyperledger would not. Also, the real-world transactional efficiency of health-care blockchain platforms is likely be inferior to that of distributed database management systems, which has to be weighed against the tangible (eg, cybersecurity cost savings) and non-tangible (eg, consequences of security breaches) benefits of a blockchain platform. Third, blockchain technology does not entirely eliminate risks related to data privacy. Theft of private keys by malicious agents could still compromise secure data transfer and patient confidentiality. Furthermore, there are governance concerns due to the small number of nodes involved in consortium or private health-care blockchains. Comprehensive cybersecurity assessments, such as penetration tests, will be required to minimise the risks of such flaws. Finally, storing large-scale medical data on a blockchain is impractical. On-chain storage would require these data to be stored on every node, which would impose high costs on a decentralised network and severely limit health-care applications (which frequently involve large files, such as medical images). To address this problem, off-chain storage options such as a centralised database or decentralised storage, including cloud or distributed storage systems (Interplanetary File Storage or Neo File Storage),73 would need to be considered.
Strengths and weaknesses
We herein provide a comprehensive, up-to-date systematic review of active blockchain research in various health-care domains, which helps to provide a perspective on the current research landscape on this topic, including the state of research and overall direction. Hopefully, this systematic review will allow the identification of areas that require greater attention or that might hold strong potential for real-world implementation. In addition, we explored COVID-19-specific applications, which are currently key drivers for the adoption of blockchain into the otherwise traditionally conservative health-care system. Furthermore, our systematic review described both COVID-19-related and non-COVID-19-related health-care blockchain applications. A substantial proportion of these COVID-19-specific use cases is likely to find durable relevance in the post-pandemic world, such as in vaccine and pharmaceutical supply chain management, contact tracing, and telemedicine recording (of the notes documented during consultation or the off-chain storage locations of large files). This work is thus the first to provide a comprehensive review of the development of blockchain in health care, and of how the evolving pandemic continues to shape the role of this technology. The little availability of original studies that show clinical implementation provides an indication of the relative infancy of blockchain technology in health care and of barriers toward widespread acceptance. Because of time limitations, we were not able to conduct a further exhaustive search across other bibliographical database that might provide additional valuable information. In addition, non-peer-reviewed literature was included in our evaluation, which could affect the robustness of the data. Finally, the absence of standardised research reporting for crucial technical components, such as blockchain consensus protocols and platforms, limits the generalisability of this systematic review, which might contribute to a disconnection between the early-stage championing of blockchain and validated, real-world research progress. Nevertheless, we believe that the literature assessed in this systematic review represents a strong foundation for blockchain as an enabling platform for a broad spectrum of health-care applications, both during and beyond the COVID-19 pandemic.
Data sharing
All data collected are publicly available and all selected articles have been tabulated in the appendix (pp 8–41). All study protocols detailed in this systematic review will be made available upon request and without time, user, or purpose of use restrictions. This systematic review was pre-registered in the Open Science Framework at https://osf.io/7fm3p/?view_only=c9cb23866c4c4a78b7e63a745cba1ca1.
Declaration of interests
We declare no competing interests.
Contributors
All authors conceptualised this systematic review, researched for contents, determined the methods, wrote the manuscript, and revised all versions. WYN and T-ET were involved in the verification of underlying data. All authors had access to the data presented in this manuscript.
Footnotes
37 COVID-19-related blockchain articles covering a total of 38 applications. 36 articles explored a single application whereas one article involved two applications (contact tracing and pandemic control and surveillance).
378 non-COVID-19-related blockchain articles covering a total of 392 applications. 365 articles explored a single application, 12 articles covered dual applications (eg, artificial intelligence, big data, and federated learning with mobile health, remote monitoring, or internet of things), and one article described triple applications (electronic medical records, mobile health, remote monitoring, or internet of things, and epidemic and infection control).
Some studies used multiple blockchain platforms.
Supplementary Material
References
- 1.Ting DSW, Lin H, Ruamviboonsuk P, Wong TY, Sim DA. Artificial intelligence, the internet of things, and virtual clinics: ophthalmology at the digital translation forefront. Lancet Digit Health. 2020;2:e8–e9. doi: 10.1016/S2589-7500(19)30217-1. [DOI] [PubMed] [Google Scholar]
- 2.Gunasekeran DV, Tseng RMWW, Tham Y-C, Wong TY. Applications of digital health for public health responses to COVID-19: a systematic scoping review of artificial intelligence, telehealth and related technologies. NPJ Digit Med. 2021;4:40. doi: 10.1038/s41746-021-00412-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gunasekeran DV, Tseng RMWW, Tham YC, Wong TY. Applications of digital health for public health responses to COVID-19: a systematic scoping review of artificial intelligence, telehealth and related technologies. NPJ Digit Med. 2021;4:40. doi: 10.1038/s41746-021-00412-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Whitelaw S, Mamas MA, Topol E, Van Spall HGC. Applications of digital technology in COVID-19 pandemic planning and response. Lancet Digit Health. 2020;2:e435–e440. doi: 10.1016/S2589-7500(20)30142-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sharma A, Adhikary A, Borah SB. Covid-19's impact on supply chain decisions: strategic insights from NASDAQ 100 firms using Twitter data. J Bus Res. 2020;117:443–449. doi: 10.1016/j.jbusres.2020.05.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Iansiti M, Lakhani KR. The truth about blockchain. 2017. https://hbr.org/2017/01/the-truth-about-blockchain
- 7.Kuo TT, Kim HE, Ohno-Machado L. Blockchain distributed ledger technologies for biomedical and health care applications. J Am Med Inform Assoc. 2017;24:1211–1220. doi: 10.1093/jamia/ocx068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ting DSW, Carin L, Dzau V, Wong TY. Digital technology and COVID-19. Nat Med. 2020;26:459–461. doi: 10.1038/s41591-020-0824-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Agbo CC, Mahmoud QH, Eklund JM. Blockchain technology in healthcare: a systematic review. Healthcare (Basel) 2019;7:56. doi: 10.3390/healthcare7020056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Klaine PV, Zhang L, Zhou B, Sun Y, Xu H, Imran M. Privacy-preserving contact tracing and public risk assessment using blockchain for COVID-19 pandemic. IEEE Internet Things Mag. 2020;3:58–63. [Google Scholar]
- 11.No authors listed Proof-of-stake (POS) https://ethereum.org/en/developers/docs/consensus-mechanisms/pos
- 12.Shamsi K, Khorasani KE, Shayegan MJ. A secure and efficient approach for issuing KYC token as COVID-19 health certificate based on stellar blockchain network. arXiv. 2020 doi: 10.22133/ijwr.2020.250275.1070. published online Oct 5. (preprint). [DOI] [Google Scholar]
- 13.Alsamhi SH, Lee B, Guizani M, Kumar N, Qiao Y, Liu X. Blockchain for decentralized multi-drone to combat COVID-19. arXiv. 2021 https://arxiv.org/abs/2102.00969v1 published online Feb 1. (preprint). [Google Scholar]
- 14.Celesti A, Ruggeri A, Fazio M, Galletta A, Villari M, Romano A. Blockchain-based healthcare workflow for tele-medical laboratory in federated hospital IoT clouds. Sensors (Basel) 2020;20:2590. doi: 10.3390/s20092590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lin H, Zhang H, Yan H, et al. A secure online treatment blockchain service. Wirel Pers Commun. 2021;117:1773–1795. [Google Scholar]
- 16.Qiu Z, Zhu Y. A Novel structure of blockchain applied in vaccine quality control: double-chain structured blockchain system for vaccine anticounterfeiting and traceability. J Healthc Eng. 2021;2021:6660102. doi: 10.1155/2021/6660102. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 17.Sylim P, Liu F, Marcelo A, Fontelo P. Blockchain technology for detecting falsified and substandard drugs in distribution: pharmaceutical supply chain intervention. JMIR Res Protoc. 2018;7:e10163. doi: 10.2196/10163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mahmood S, Hasan K, Colder Carras M, Labrique A. Global preparedness against COVID-19: we must leverage the power of digital health. JMIR Public Health Surveill. 2020;6:e18980. doi: 10.2196/18980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bay J, Kek J, Tan A, Hau CS. BlueTrace: a privacy-preserving protocol for community-driven contact tracing across borders. 2020. https://bluetrace.io/static/bluetrace_whitepaper-938063656596c104632def383eb33b3c.pdf
- 20.Idrees SM, Nowostawski M, Jameel R. Blockchain-based digital contact tracing apps for COVID-19 pandemic management: issues, challenges, solutions, and future directions. JMIR Med Inform. 2021;9:e25245. doi: 10.2196/25245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Garg C, Bansal A, Padappayil RP. COVID-19: prolonged social distancing implementation strategy using blockchain-based movement passes. J Med Syst. 2020;44:165. doi: 10.1007/s10916-020-01628-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Xu H, Zhang L, Onireti O, Fang Y, Buchanan WB, Imran MA. BeepTrace: blockchain-enabled privacy-preserving contact tracing for COVID-19 pandemic and beyond. arXiv. 2020 doi: 10.1109/JIOT.2020.3025953. published online May 20. (preprint). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Eisenstadt M, Ramachandran M, Chowdhury N, Third A, Domingue J. COVID-19 antibody test/vaccination certification: there's an app for that. IEEE Open J Eng Med Biol. 2020;1:148–155. doi: 10.1109/OJEMB.2020.2999214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hasan HR, Salah K, Jayaraman R, et al. Blockchain-based solution for COVID-19 digital medical passports and immunity certificates. TechRxiv. 2020 doi: 10.36227/techrxiv.12800360.v1. published online Aug 14. (preprint). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bansal A, Garg C, Padappayil RP. Optimizing the implementation of COVID-19 “immunity certificates” using blockchain. J Med Syst. 2020;44:140. doi: 10.1007/s10916-020-01616-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chaudhari S, Clear M, Bradish P, Tewari H. Framework for a DLT based COVID-19 passport. arXiv. 2020 https://arxiv.org/abs/2008.01120v7 (preprint). published online Aug 3. [Google Scholar]
- 27.No authors listed What is IPFS? https://docs.ipfs.io/concepts/what-is-ipfs/
- 28.Hernández-Ramos JL, Karopoulos G, Geneiatakis D, Martin T, Kambourakis G, Fovino IN. Sharing pandemic vaccination certificates through blockchain: case study and performance evaluation. arXiv. 2021 published online Jan 12. https://arxiv.org/abs/2101.04575v1 (preprint). [Google Scholar]
- 29.Alexander GC, Qato DM. Ensuring access to medications in the US during the COVID-19 pandemic. JAMA. 2020;324:31–32. doi: 10.1001/jama.2020.6016. [DOI] [PubMed] [Google Scholar]
- 30.Gordon DE, Jang GM, Bouhaddou M, et al. A SARS-CoV-2 protein interaction map reveals targets for drug repurposing. Nature. 2020;583:459–468. doi: 10.1038/s41586-020-2286-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ho D. Addressing COVID-19 drug development with artificial intelligence. Adv Intell Syst. 2020 doi: 10.1002/aisy.202000070. published online April 27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Khurshid A. Applying blockchain technology to address the crisis of trust during the COVID-19 pandemic. JMIR Med Inform. 2020;8:e20477. doi: 10.2196/20477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kovács G, Falagara Sigala I. Lessons learned from humanitarian logistics to manage supply chain disruptions. J Supply Chain Manag. 2020;57:41–49. [Google Scholar]
- 34.Antal CD, Cioara T, Antal M, Anghel I. Blockchain platform for COVID-19 vaccine supply management. arXiv. 2021 https://arxiv.org/abs/2101.00983v1 published online Jan 4. (preprint). [Google Scholar]
- 35.Ahmad RW, Salah K, Jayaraman R, Yaqoob I, Omar M, Ellahham S. Blockchain-based forward supply chain and waste management for COVID-19 medical equipment and supplies. IEEE Access. 2021;9:44905–44927. doi: 10.1109/ACCESS.2021.3066503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kumar R, Tripathi R. A Secure and distributed framework for sharing COVID-19 patient reports using consortium blockchain and IPFS. 6th International Conference on Parallel, Distributed and Grid Computing; online; 6–8 Nov, 2020: 231–36.
- 37.Christodoulou K, Christodoulou P, Zinonos Z, Carayannis EG, Chatzichristofis SA. Health information exchange with blockchain amid Covid-19-like pandemics. 16th International Conference on Distributed Computing in Sensor Systems; Marina del Rey, CA, USA; May 25–27, 2020: 412–17.
- 38.Lee HA, Kung HH, Lee YJ, et al. Global infectious disease surveillance and case tracking system for COVID-19: development study. JMIR Med Inform. 2020;8:e20567. doi: 10.2196/20567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Hylock RH, Zeng X. A blockchain framework for patient-centered health records and exchange (HealthChain): evaluation and proof-of-concept study. J Med Internet Res. 2019;21:e13592. doi: 10.2196/13592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Mohsin AH, Zaidan AA, Zaidan BB, et al. Based blockchain-PSO-AES techniques in finger vein biometrics: a novel verification secure framework for patient authentication. Comput Stand Interfaces. 2019;66:103343. [Google Scholar]
- 41.Zhuang Y, Sheets LR, Shae Z, Chen YW, Tsai JJP, Shyu CR. Applying blockchain technology to enhance clinical trial recruitment. AMIA Annu Symp Proc. 2020;2019:1276–1285. [PMC free article] [PubMed] [Google Scholar]
- 42.Zhuang Y, Sheets L, Shae Z, Tsai JJP, Shyu CR. Applying blockchain technology for health information exchange and persistent monitoring for clinical trials. AMIA Annu Symp. 2018;2018:1167–1175. [PMC free article] [PubMed] [Google Scholar]
- 43.Zhou L, Wang L, Sun Y. Mistore: a blockchain-based medical insurance storage system. J Med Syst. 2018;42:149. doi: 10.1007/s10916-018-0996-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Tan TE, Anees A, Chen C, et al. Retinal photograph-based deep learning algorithms for myopia and a blockchain platform to facilitate artificial intelligence medical research: a retrospective multicohort study. Lancet Digit Health. 2021;3:e317–e329. doi: 10.1016/S2589-7500(21)00055-8. [DOI] [PubMed] [Google Scholar]
- 45.Kuo TT, Gabriel RA, Cidambi KR, Ohno-Machado L. EXpectation Propagation LOgistic REgRession on permissioned blockCHAIN (ExplorerChain): decentralized online healthcare/genomics predictive model learning. J Am Med Inform Assoc. 2020;27:747–756. doi: 10.1093/jamia/ocaa023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Jin XL, Zhang M, Zhou Z, Yu X. Application of a blockchain platform to manage and secure personal genomic data: a case study of LifeCODE.ai in China. J Med Internet Res. 2019;21:e13587. doi: 10.2196/13587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Tseng JH, Liao YC, Chong B, Liao SW. Governance on the drug supply chain via Gcoin blockchain. Int J Environ Res Public Health. 2018;15:1055. doi: 10.3390/ijerph15061055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Dwivedi AD, Srivastava G, Dhar S, Singh R. A decentralized privacy-preserving healthcare blockchain for IoT. Sensors (Basel) 2019;19:326. doi: 10.3390/s19020326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Chenthara S, Ahmed K, Wang H, Whittaker F, Chen Z. Healthchain: a novel framework on privacy preservation of electronic health records using blockchain technology. PLoS One. 2020;15:e0243043. doi: 10.1371/journal.pone.0243043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Tian H, He J, Ding Y. Medical data management on blockchain with privacy. J Med Syst. 2019;43:26. doi: 10.1007/s10916-018-1144-x. [DOI] [PubMed] [Google Scholar]
- 51.Roehrs A, da Costa CA, da Rosa Righi R. OmniPHR: a distributed architecture model to integrate personal health records. J Biomed Inform. 2017;71:70–81. doi: 10.1016/j.jbi.2017.05.012. [DOI] [PubMed] [Google Scholar]
- 52.Wang H, Song Y. Secure cloud-based EHR system using attribute-based cryptosystem and blockchain. J Med Syst. 2018;42:152. doi: 10.1007/s10916-018-0994-6. [DOI] [PubMed] [Google Scholar]
- 53.Jin H, Xu C, Luo Y, Li P, Cao Y, Mathew J. Toward secure, privacy-preserving, and interoperable medical data sharing via blockchain. IEEE 25th International Conference on Parallel and Distributed Systems; Tianjin; Dec 4–6, 2019: 852–61.
- 54.Malamas V, Kotzanikolaou P, Dasaklis TK, Burmester M. A hierarchical multi blockchain for fine grained access to medical data. IEEE Access. 2020;8:134393–134412. [Google Scholar]
- 55.Liu H, Crespo RG, Martínez OS. Enhancing privacy and data security across healthcare applications using blockchain and distributed ledger concepts. Healthcare (Basel) 2020;8:243. doi: 10.3390/healthcare8030243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Zhang A, Lin X. Towards secure and privacy-preserving data sharing in e-health systems via consortium blockchain. J Med Syst. 2018;42:140. doi: 10.1007/s10916-018-0995-5. [DOI] [PubMed] [Google Scholar]
- 57.Lo YS, Yang CY, Chien HF, Chang SS, Lu CY, Chen RJ. Blockchain-enabled iWellChain framework integration with the National Medical Referral System: development and usability study. J Med Internet Res. 2019;21:e13563. doi: 10.2196/13563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Benchoufi M, Porcher R, Ravaud P. Blockchain protocols in clinical trials: transparency and traceability of consent. F1000 Res. 2017;6:66. doi: 10.12688/f1000research.10531.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Velmovitsky PE, Miranda PADSES, Vaillancourt H, Donovska T, Teague J, Morita PP. A blockchain-based consent platform for active assisted living: modeling study and conceptual framework. J Med Internet Res. 2020;22:e20832. doi: 10.2196/20832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Thenmozhi M, Dhanalakshmi R, Geetha S, Valli R. Implementing blockchain technologies for health insurance claim processing in hospitals. Mater Today Proc. 2021 doi: 10.1016/j.matpr.2021.02.776. published online March 24. [DOI] [Google Scholar]
- 61.Mackey TK, Miyachi K, Fung D, Qian S, Short J. Combating health care fraud and abuse: conceptualization and prototyping study of a blockchain antifraud framework. J Med Internet Res. 2020;22:e18623. doi: 10.2196/18623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Rahman MA, Hossain MS, Islam MS, Alrajeh NA, Muhammad G. Secure and provenance enhanced internet of health things framework: a blockchain managed federated learning approach. IEEE Access. 2020;8:205071–205087. doi: 10.1109/ACCESS.2020.3037474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Polap D, Srivastava G, Yu K. Agent architecture of an intelligent medical system based on federated learning and blockchain technology. J Inf Secur Appl. 2021;58:102748. [Google Scholar]
- 64.Kumar R, Wang W, Kumar J, et al. An integration of blockchain and AI for secure data sharing and detection of CT images for the hospitals. Comput Med Imaging Graph. 2021;87:101812. doi: 10.1016/j.compmedimag.2020.101812. [DOI] [PubMed] [Google Scholar]
- 65.Warnat-Herresthal S, Schultze H, Shastry KL, et al. Swarm Learning for decentralized and confidential clinical machine learning. Nature. 2021;594:265–270. doi: 10.1038/s41586-021-03583-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Ozercan HI, Ileri AM, Ayday E, Alkan C. Realizing the potential of blockchain technologies in genomics. Genome Res. 2018;28:1255–1263. doi: 10.1101/gr.207464.116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Aiello M, Cavaliere C, D'Albore A, Salvatore M. The challenges of diagnostic imaging in the era of big data. J Clin Med. 2019;8:316. doi: 10.3390/jcm8030316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Ngiam KY, Khor IW. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. 2019;20:e262–e273. doi: 10.1016/S1470-2045(19)30149-4. [DOI] [PubMed] [Google Scholar]
- 69.Kruse CS, Goswamy R, Raval Y, Marawi S. Challenges and opportunities of big data in health care: a systematic review. JMIR Med Inform. 2016;4:e38. doi: 10.2196/medinform.5359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Glicksberg BS, Burns S, Currie R, et al. Blockchain-authenticated sharing of genomic and clinical outcomes data of patients with cancer: a prospective cohort study. J Med Internet Res. 2020;22:e16810. doi: 10.2196/16810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Ali MS, Vecchio M, Putra GD, Kanhere SS, Antonelli F. A decentralized peer-to-peer remote health monitoring system. Sensors (Basel) 2020;20:1656. doi: 10.3390/s20061656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Brogan J, Baskaran I, Ramachandran N. Authenticating health activity data using distributed ledger technologies. Comput Struct Biotechnol J. 2018;16:257–266. doi: 10.1016/j.csbj.2018.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Fang HSA, Tan TH, Tan YFC, Tan CJM. Blockchain personal health records: systematic review. J Med Internet Res. 2021;23:e25094. doi: 10.2196/25094. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
All data collected are publicly available and all selected articles have been tabulated in the appendix (pp 8–41). All study protocols detailed in this systematic review will be made available upon request and without time, user, or purpose of use restrictions. This systematic review was pre-registered in the Open Science Framework at https://osf.io/7fm3p/?view_only=c9cb23866c4c4a78b7e63a745cba1ca1.