

Abstract
Aim
The main objective of this paper was to establish types of health status in the group of practicing nurses.
Design
Positive psychology defines human health as the underlying resource for all life activities, including professional work. Practicing nurses are exposed to a variety of professional pressures, most notably high‐stress burden. Long‐term functioning in conditions of work‐related overburden and stress may compromise the health status of nurses and make them vulnerable to somatic or psychosomatic conditions.
Methods
In this study, we used original worksheets for collecting socio‐economic data and health‐related data, Orientation to Life Questionnaire (SOC‐29), General Health Questionnaire (GHQ‐28), Brief COPE Inventory (Mini‐COPE) and the somatic symptom scale. K‐means clustering analysis for cases was used to identify types of health status among the surveyed nurses.
Results
This survey discovered that specific types of health status can be distinguished among practicing nurses. The nurses represented various types of health status, levels of the sense of coherence and the use of stress management strategies.
Keywords: health, nurses, nursing, sense of coherence, stress, type of health condition
1. INTRODUCTION
Human health determines how well individuals function in various spheres of life, including the professional one. Good mental, physical and social status of an employee translates into better performance at work. When performing professional duties, nurses are exposed to various pressures that may negatively affect their health. Strengthening and promoting health is an area of interest for employers. One of key elements of intangible investments in human resources is to take measures aimed at improving employees’ health. Creating a safe working environment is currently an important issue in both Poland and worldwide.
2. BACKGROUND
According to the Ottawa Charter for Health Promotion, health itself is a multifaceted and complex concept (Whitehead, 2018). The contemporary approach to health is based on a definition put forward in the Constitution of the World Health Organization, which reads: “Health is a state of complete physical, mental and social well‐being and not merely the absence of disease or infirmity” (Constitution of The World Health Organization (WHO) 1948, p. 1; Habersack & Luschin, 2013).
By reason of the nature of their professional duties and the risks inherently associated with exposure to noxious and hazardous factors in the working environment, and the psychosocial burdens of their profession, healthcare professionals, including nurses, are intrinsically exposed to multiple health risks. Nursing staff often work in shits and face irregular working hours. This leads to disruptions in the circadian rhythms and sleep disorders; it can have an adverse impact on family and social life and become an additional psychophysical burden accompanied by functional disorders, such as fatigue, headache, irritability, concentration and decision‐making problems (Peplonska et al., 2015). According to the Nurses' Early Exit (NEXT) study conducted in Europe, working night shifts should be considered a contributing factor that can accelerate the development of or aggravate the course of many illnesses and pathological conditions. Shift and night work can be associated with an increased risk of developing cancer (Kamdar et al., 2013). A study by Hansen et al. demonstrated that nurses working night shifts were more likely to develop diabetes. Nurses’ health problems should be analysed in the context of the rapidly ageing nursing workforce. The average age of a Polish nurse in 2019 was 52 years (The Supreme Chamber of Nurses and Midwives, 2020). Obviously, the risk of cardiovascular, musculoskeletal and respiratory conditions increase as the nursing staff becomes older (Andruszkiewicz, 2019). Studies on nurses also reveal that this professional group is particularly exposed to occupational burnout. The moral, emotional and professional demands associated with this profession are not adequately and sufficiently compensated by the level of earnings, social status and the professional prestige. Frustration and dissatisfaction are chronic job stressors. Nursing profession is one of the most stressful occupations today as it involves a specific type of stress arising from everyday interactions with other people. Nursing staff works in multidisciplinary teams and interacts closely with patients and their relatives who are often in very high emotional distress. Nurse is faced by a whole spectrum of problems, some of which are psychological and social in nature and go far beyond health‐related issues; they touch upon experiences of birth, suffering and death (Badu et al., 2020; Kędra & Nowocień, 2015; Kilańska et al., 2016). The subjective stress levels associated with the professional role and the accompanying negative emotions, if they are strong enough and persistent, can lead to a number of permanent negative consequences in cognitive, emotional and behavioural domains and can be manifested by disease symptoms and ultimately lead to health problems. The choice of stress management strategy is important both for the functioning in a profession and for the health of an individual. Taking pro‐active measures to eliminate a stressor or alleviate its negative consequences contribute to maintaining and improving health and well‐being (Basińska, 1998).
Over the past years, a pathogenetic model was the predominant one in medicine and in the analysis of health determinants, focused on identifying the root causes of diseases and somatic dysfunctions. As a counterpoint to the biomedical model, a salutogenic approach emerged as a basis for identifying determinants of good health and well‐being (Behnke et al., 2019; Jażdżewska et al., 2018; Nowicki & Ślusarska, 2011; Wijesinghe & Parshall, 2016). The concept of salutogenesis and the sense of coherence (SOC) as its central construct were coined by Aaron Antonovsky, who argued that a dynamic condition of shaky equilibrium is a normal state in which humans function. Salutogenesis defines health as neither a state nor a permanent resource, but a process of moving on an ease/dis‐ease continuum, and the individual's position on this continuum largely depends on the power of their SOC. Antonovsky claimed that the SOC is the “key to health” or the main determinant through which a human being can stay healthy and avoid diseases or can recover health more quickly (Antonovsky, 1979). Antonovsky defines the SOC as a “global orientation that expresses the extent to which one has a pervasive and enduring, though dynamic, feeling of confidence that the stimuli derived from one's internal and external environments in the course of living are structured, predictable, and explicable; the resources are available to one to meet the demands posed by these stimuli; and these demands are challenges that are worthy of investment and engagement” (Antonovsky, 1987, pp. 34). The SOC is a complex individual variable consisting of three basic components: sense of comprehensibility, sense of manageability and sense of meaningfulness (Antonovsky, 1979; Szcześniak & Strochalska, 2020). The SOC as a trait of personality affects how individuals function in various spheres of life and, as confirmed in research, “it has a positive influence on health, both directly and indirectly, depending on the characteristics and intensity of its components.” (Heszen & Sęk, 2007, pp. 82–83) People characterized by a highly developed SOC are in better physical and mental shape, are more likely to engage into meaningful activities, fulfil their tasks and find it easier to accept the inevitable difficulties of life. They feel much more satisfied with life and enjoy a higher quality of life (Kowitlawkul et al., 2019). Larsson analysed data from five thousand respondents and identified a strong correlation between the SOC and health behaviours, subjective health status and quality of life (Larsson, 2000).
Strengthening and promoting health is an area of interest for employers. One of key elements of intangible investments in human resources is to take measures aimed at improving employees’ health. Nurses are exposed to the risk of health loss in all aspects of their professional activities. Unless the risks are eliminated early enough, they can contribute to the development of occupational diseases, and in consequence, they may trigger a decline in the quality of the nursing services provided. The demands faced by nurses weigh down on their physical and mental health (Rosa et al., 2019). Creating a safe working environment is currently an important issue in both Poland and worldwide. This aspect is particularly relevant in the nursing profession. It may incentivize and encourage students to choose this career path, and as a result, it helps ensure appropriate staffing levels in healthcare establishments. Creating a safe working environment, strengthening health as a meta‐resource and teaching employees how to master constructive stress management strategies should become a central element of investments in human resources.
The main objective of this study was to identify types of health status in a group of practicing nurses who varied in the values of the analysed physical and mental health indicators. It was examined whether nurses representing specific types differ in terms of the level of the SOC and the strategies of coping with stress.
3. METHODOLOGY
The study included 375 women (nurses) aged 22 to 62 years (M = 42, SD = 6.52). The group was diversified in terms of social, demographic and professional variables. The majority of nurses were engaged in a relationship; they mostly had secondary education and the mean work experience in nursing was 21 years (M = 21; SD = 7.21). The vast majority of study subjects worked in a 12‐hr shift system as general nurses.
The following research tools were used in the study:
An original worksheet designed for collecting socio‐economic data and health‐related data. The worksheet included essential data to describe the study group in terms of social and demographic variables, work characteristics and health status (height, body mass, BMI, systolic blood pressure [SBP], diastolic blood pressure [DBP], chronic conditions and subjective health assessment).
Sense of Coherence Questionnaire (SOC‐29) by Antonovsky, adapted version in Polish. This questionnaire is designed to assess the level of the SOC and its three components: comprehensibility, manageability and meaningfulness. The Polish version of SOC‐29 questionnaire proved this to be a valuable research tool. Its internal consistency measured by Cronbach's α was 0.78 (Koniarek et al., 1993).
General Health Questionnaire (GHQ‐28) by Goldberg, adapted version in Polish. This questionnaire is a screening tool to evaluate the mental condition of adults in the general population. GHQ‐28 measures global mental health status and four types of health dimensions: somatic symptoms (GHQ‐A), anxiety and insomnia (GHQ‐B), psychosocial dysfunction (GHQ‐C) and symptoms of depression (GHQ‐D). The internal consistency measured by Cronbach's α ranged from 0.91–0.93 (Makowska & Merecz, 2001).
Inventory to Measure Coping Strategies with Stress (Mini‐COPE) by Carver, Scheier and Weintraub, adapted version in Polish. This questionnaire investigates the strategies of coping with stress and consists of 28 statements addressing 14 different stress management strategies. The internal consistency measured by Cronbach's α was 0.78 for the overall scale and ranged from 0.92–0.66 for subscales (Ogińska‐Bulik & Juczyński, 2009).
The scale of somatic symptoms by Basińska was based on the somatic scale of the Minnesota Multiphasic Personality Inventory (MMPI‐2). It was designed to evaluate the tendency to report somatic complaints in adults. Internal consistency measured by Cronbach's α was 0.86 (Basińska, not published).
K‐means clustering analysis for cases was used to identify different types of health status among the surveyed nurses. The health data obtained (BMI, systolic pressure—SBP; diastolic pressure—DBP, chronic disease burden, global mental health status, tendency to complain about somatic symptoms) were analysed in various variants—from two–five clusters. After analysing the results, the partition into three clusters was found to be most logical and to provide the best diversification of cases. The analysis only included results for the global health status (total of GHQ) excluding subscales.
3.1. Ethical considerations
The study also included nurses who participated in postgraduate vocational training programmes. The study was conducted according to the principles laid down in the Declaration of Helsinki. It was approved by the Ethics Committee of the University (KB 666/2015).
4. RESULTS
The first stage of analysis was intended to determine whether the health status indicators of the surveyed group of nurses are sufficient to extract internally diversified types of health status among the study subjects. Another objective was to make clear whether individuals belonging to specific types of health status differ in terms of somatic health indicators, global mental health status and the tendency to complain about somatic symptoms. The question of whether individuals belonging to the identified types of health status statistically significantly differ in terms of the SOC and its components (comprehensibility, manageability and meaningfulness) and the strategies of coping with stress was also identified as relevant.
Three clusters were derived from the results obtained:
No abnormalities in terms of objective somatic health indicators were observed in the first group of nurses surveyed—BMI was within normal range, systolic blood pressure and diastolic blood pressure were normal, and the respondents rarely reported any chronic conditions, and they represented good mental health and had no tendency to complain about somatic symptoms. This group was referred to as “healthy.”
Abnormalities in terms of objective somatic health indicators were revealed in the second group of the nurses surveyed (BMI—overweight, slightly elevated systolic blood pressure, normal diastolic blood pressure)—these nurses suffered from chronic conditions and had a moderate mental health status and a lower tendency to complain about somatic symptoms compared to the “healthy” cluster. This group was referred to as “with disorders.”
Abnormalities in BMI (overweight), slightly elevated systolic blood pressure, and normal diastolic blood pressure were revealed in the third group of the nurses surveyed; these nurses suffered from chronic conditions and had a poor mental health and an increased tendency to complain about somatic symptoms. This group was referred to as “malcontents with health problems” (Table 1).
TABLE 1.
Health status indicators of the surveyed nurses
| Health status indicators | “healthy” cluster (N = 146) | “with disorders” cluster (N = 132) | “malcontents with health problems” cluster (N = 64) | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |
| BMI | 23.71 | 3.041 | 25.70 | 4.732 | 25.50 | 4.800 |
| Systolic blood pressure (SBP) | 103.90 | 8.396 | 125.91 | 9.189 | 121.61 | 9.835 |
| Diastolic blood pressure (DBP) | 63.00 | 6.742 | 79.51 | 6.707 | 77.12 | 7.653 |
| Chronic disease burden | 0.33 | 0.520 | 0.52 | 0.736 | 0.71 | 0.736 |
| Global mental health status | 22.72 | 8.344 | 19.41 | 5.776 | 41.11 | 8.634 |
| Tendency to report somatic complaints | 6.81 | 3.625 | 5.40 | 3.682 | 9.70 | 3.673 |
The next stage of analysis was intended to find out whether individuals belonging to specific types of health status significantly differed in terms of each of the specified health status indicators. An analysis of variance revealed statistically significant differences in each of the identified health status indicators (Table 2; Figure 1).
TABLE 2.
Types of health status versus health status indicators (significant differences between individuals who belong to various types of health status) in the surveyed group of nurses
| Types of health status | F | p | Significant differences |
|---|---|---|---|
| BMI | 9 | <.001 | "healthy"—"with disorders" |
| Systolic blood pressure (SBP) | 224.40 | <.001 |
"malcontents with health problems"—"healthy" "malcontents with health problems"—"with disorders" "healthy"—"with disorders" |
| Diastolic blood pressure (DBP) | 219.41 | <.001 |
"malcontents with health problems"—"healthy" "healthy"—"with disorders" |
| Chronic disease burden | 6.11 | .003 |
"healthy"—"malcontents with health problems" "healthy"—"with disorders" |
| Global mental health status | 189.72 | <.001 |
"malcontents with health problems"—"healthy" "malcontents with health problems"—"with disorders" "healthy"—"with disorders" |
| Tendency to report somatic complaints | 29.62 | <.001 |
"malcontents with health problems"—"healthy" "malcontents with health problems"—"with disorders" "healthy"—"with disorders" |
FIGURE 1.
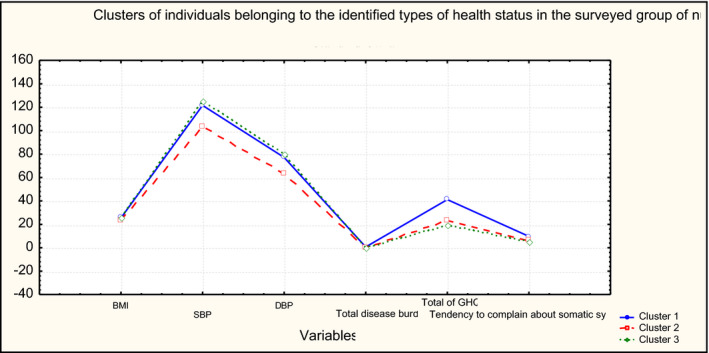
Clusters of individuals belonging to the identified types of health status in the surveyed group of nurses. Cluster 1—“malcontents with health problems”, Cluster 2—“healthy”, Cluster 3—“with disorders”
In the next step of analysis, individuals belonging to the identified types of health status were examined for differences in the SOC and its components. Nurses classified as “with disorders” were SOC 136.15, “healthy individuals”—133.69 and “malcontents with health problems”—114.18. The Kruskal–Wallis test was used, and multiple post hoc comparisons were performed to determine the significance of the differences between the types of health status. The findings confirmed that individuals belonging to the identified types of health status differed significantly in the SOC and its components (Table 3).
TABLE 3.
Significance of differences in the sense of coherence among individuals belonging to the identified types of health status in the surveyed group of nurses
| Types of health status | “malcontents with health problems” | "healthy" | "with disorders" |
|---|---|---|---|
| Mean rank | 90.847 | 179.46 | 188.62 |
| “malcontents with health problems” | <0.001 | <0.001 | |
| "healthy" | <0.001 | 1 | |
| "with disorders" | <0.001 | 1 |
The multiple comparison post hoc test revealed that “malcontents with health problems” statistically significantly differed from nurses belonging to the other two types of health status. These nurses were characterized by the lowest SOC. No significant differences in the SOC were found between individuals classified as “healthy individuals” and “with disorders.” The differences in the SOC are illustrated in Figure 2. The SOC is an example used to present the research findings; “malcontents with health problems” also exhibited the lowest sense of comprehensibility, manageability and meaningfulness.
FIGURE 2.
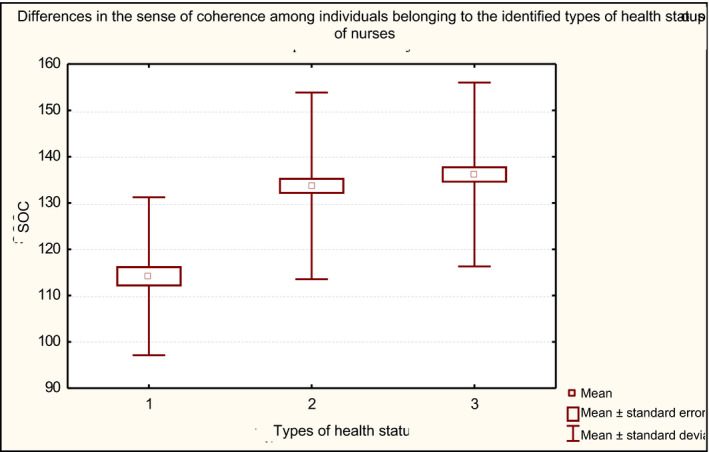
Differences in the sense of coherence among individuals belonging to the identified types of health status in the surveyed group of nurses. Cluster 1—“malcontents with health problems”, Cluster 2—“healthy”, Cluster 3—“with disorders”
In the next steps, the Kruskal–Wallis test was performed to check for differences in the strategies of coping with stress among individuals belonging to the identified types of health status. The findings confirmed that individuals assigned to the identified types of health status differed significantly in the strategies of coping with stress, including denial, venting, behavioural disengagement, and self‐blame. “Malcontents with health problems” most often used the enumerated non‐adaptive strategies of stress management. The findings are presented with the example of the denial strategy (Tables 4 and 5).
TABLE 4.
The denial strategy used by nurses belonging to specific types of health status
| Types of health status | M | H | p |
|---|---|---|---|
| Mean rank | 1.43 | 21.46 | <.001 |
| “malcontents with health problems” | 0.90 | ||
| "healthy" | 0.93 | ||
| "with disorders" |
TABLE 5.
Significance of differences in the use of denial strategy by nurses belonging to specific types of health status
| Types of health status | “malcontents with health problems” | "healthy" | "with disorders" |
|---|---|---|---|
| Mean rank | 221.23 | 157.51 | 161.50 |
| “malcontents with health problems” | <0.001 | <0.001 | |
| "healthy" | <0.001 | 1 | |
| "with disorders" | <0.001 | 1 |
It was important to examine whether the nurses assigned to the identified types of health status differ in terms of age. “Healthy nurses” were shown to statistically significantly differ from individuals belonging to the other two types of health status in terms of age. They were the youngest, although all nurses were middle‐aged, that is around 40 years old.
5. DISCUSSION
Research findings show that specific types of health status can be identified among practicing nurses. In this study, three specific types of health status have been distinguished. “Healthy individuals” are nurses with the best somatic health status who reported the lowest burden of chronic diseases. Nurses “with disorders” represented a poor somatic health status but the best global mental health status. Despite somatic disorders, these nurses enjoyed good physical well‐being. “Malcontents with health problems” was a group of nurses in whom the highest number of risk factors in physical and mental well‐being were identified. These nurses reported the highest burden of chronic diseases and a stronger tendency to report somatic complaints. Health risks in this group can be traced back to a poor global mental health status as compared to other respondents. In addition, nurses in this group opted for the least adaptive strategies of coping with stress. Nurses “with disorders” were characterized by the highest SOC, as opposed to “malcontents with health problems,” whose SOC was the lowest.
The analysis of data from surveys conducted by Andruszkiewicz demonstrated a clear distinction between how the identified types of nurses functioned at work, as evidenced in the cluster analysis. These findings were also confirmed in our own surveys.
In a group of 1,141 practicing nurses, Andruszkiewicz identified three types of health status: “poor health status,” “fair health status” and “good health status. The largest group of respondents were classified as the “fair health status” type. These individuals were characterized by optimum somatic health indicators, good physical condition, medium levels of fatigue, medium burden of chronic diseases and a tendency to use offensive strategies of coping with stress. Nurses having this type of health status did not feel significantly mentally burdened, did not experience excessive stress levels associated with their professional duties and were able to distance themselves from work and come to terms with failure. The author presented interesting points concerning behavioural patterns that the nurses qualified to the two opposite types of health status were using when faced by challenges at work. Nurses enjoying “good health status” openly confronted with difficulties and burdens. They were focused on important issues and priorities. In contrast, individuals with “poor health status” used evasive strategies which failed to promote problem‐solving. The degree to which these personal traits prevail shapes the individual strategy of confronting with professional challenges and creates a kind of protective factor which promotes the mental health of an individual. Individuals with “poor health status” were shown to function according to plan B—characterized by signs of professional burnout, lack of motivation, negative emotions and reduced mental resilience. These nurses should be included in support programmes for healthcare workers. The three types of health status confirm that the level of available resources and individual coping strategies (Andruszkiewicz, 2019) is the source of differences between the groups, which were also confirmed in this study. Ogińska‐Bulik published a similar analysis focused on the structure of health dimensions. This study was conducted on representatives of professional groups delivering specific categories of social services, including paramedics. The working environment of nurses and paramedics bears many similarities and involves similar factors of distress that is often caused by strong emotions arising from interactions with patients, shift work and physical burdens. Ogińska‐Bulik distinguished two types of clusters: 58.6% of paramedics belonged to a better health status cluster, and 41.4% belonged to a cluster characterized by a poorer health status. Individuals with poorer health experienced higher stress levels but had a lower level of personal and social resources; they more often used evasive strategies of coping with stress (denial, distraction, doing nothing, taking psychoactive substances; Ogińska‐Bulik, 2006).
References to the authors’ own research can be found in numerous surveys conducted with the use of AVEM (Arbeitsbesorgenes Verhaltens und Erlebenmuster) questionnaire to test individual behaviour patterns and experiences related to work (Andruszkiewicz, 2010; Hager & Seibt, 2018; Mroczek et al., 2017, 2018; Schulz et al., 2011). Andruszkiewicz concluded that the nurses characterized by a higher SOC were more likely to use type G [healthy] and type S [economic] patterns of behaviour in their professional life, both of which promote better health. Nurses with a low SOC, on the other hand, were more likely to behave according to type B—burnout, which does not foster health (Andruszkiewicz, 2010). Type B (burnout) pattern of behaviour was found to prevail in a study by Mroczek on a group of 160 nurses (Mroczek et al., 2017). In a study of German nurses, Wollesen concluded that type B prevailed among geriatric nurses and was one of the key drivers of stress at work (Wollesen et al., 2019). Schaarschmidt et al. explained that the high tendency to give up in the face of failure, a low level of offensive problem‐solving strategies, a low level of inner comfort and balance and the lack of sense of professional achievement are the distinctive individual patterns of those who are particularly exposed to professional burnout. Individuals who follow this pattern of behaviour exhibit lower levels of readiness to exert themselves, subjective importance of their work and occupational ambitions. They also have limited ability to distance themselves from job and reduced resistance to stress. Functioning according to type B pattern of behaviour was suggested to play a significant role in the development of stress, and inconsequence, it affects the physical and mental well‐being (Burmeister et al., 2019).
The study revealed that the SOC acted as a buffer and was very strongly correlated with the state of somatic and mental health of nurses. Nurses “with disorders,” despite having a poor somatic health status, enjoyed the best global mental health status and the highest SOC. Despite the somatic disorders, these nurses remained in a good mental health and actively responded to challenges at work. These findings suggest the need to educate nurses in order to strengthen their SOC, especially those who use less adaptive strategies of coping with stress. It is important to note that the nursing staff should be viewed as individuals rather than a collectivity. This study demonstrated that nurses differ in terms of health status. Importantly, the well‐being of nurses is not solely determined by somatic disorders. In essence, a good mental health status was largely determined by the SOC—a high SOC translated into better mental health, correct functioning in the working environment, and using adaptive strategies of coping with stress. Differences in health status and mental health of nurses are the determinants of individual adjustments in training programmes. The rationale for psychoeducational programmes for individuals who work in professions involving high levels of stress seems uncontested, both at the level of graduate and postgraduate education, in order to eliminate risky behaviours and to help them develop the ability to cope with them.
5.1. Limitations
As limitations of the conducted study, we consider a small group of surveyed nurses. In the future, in order to obtain a greater generalization of the results, it would be worth re‐examining a larger group. We also see that it would be interesting to compare nurses with other medical professionals, such as doctors or paramedics, in terms of types of health condition, the level of the SOC and coping with stress strategies.
6. CONCLUSIONS
Specific types of health status can be distinguished among practicing nurses; the nursing staff varies in terms of health status, the SOC and the use of stress management strategies.
Psychoeducational training programmes dedicated to the nursing staff should be individually adapted to address the differences in the types of health status.
6.1. Implications for nursing
Practicing nurses differ in terms of health status. Importantly, the well‐being of nurses is not solely determined by somatic disorders. In essence, a good mental health status is largely determined by the SOC—a high SOC translates into better mental health, correct functioning in the working environment and adaptive strategies of coping with stress. Differences in health status and mental health of nurses are the determinants of individual adjustments in training programmes. The rationale for psychoeducational programmes for individuals who work in professions involving high levels of stress seems uncontested, both at the level of graduate education and at the level of postgraduate education, in order to eliminate risky behaviours and to help them develop the ability to cope with them. This manuscript identifies specific types of health status in a group of practicing nurses and demonstrates that the nursing staff differs in terms of the prevalence of the analysed dimensions of physical and mental health, and the levels of the SOC and strategies of coping with stress. The conclusions from the research and carried out analyses have practical consequences. They allow to conclude that employers should supervise psychosocial risk factors in the daily work of nurses so that it constitutes an important element of the analysis of the changing work environment. The role of decision‐makers should also be to create a positive and safe work environment and to influence the factors related to the functioning of nurses while performing their professional tasks. The development of policies, work‐related stress prevention programmes and mental health promotion are current challenges for nursing decision‐makers.
CONFLICT OF INTEREST
No conflict of interest has been declared by the author(s).
ETHICAL APPROVAL
The study was approved by the Ethics Committee of the Nicolaus Copernicus University in Toruń, Ludwik Rydygier Collegium Medicum in Bydgoszcz 2015/10/20 (KB 666/2015).
ACKNOWLEDGEMENTS
We would like to extend our sincere appreciation to the nurses who participated in the study. The corresponding author would like to thank research supervisors for their guidance, support and feedback throughout all aspects of this study.
Betke K, Basińska MA, Andruszkiewicz A. Nurses’ sense of coherence and stress management strategies against the types of health status. Nurs Open. 2021;8:3403–3410. 10.1002/nop2.886
Funding information
This research did not receive any specific grant from funding agencies in the public, commercial or not‐for‐profit sectors.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Andruszkiewicz, A. (2010). Typy zachowań w pracy i wpływ na zdrowie psychiczne pielęgniarek. Problemy Pielęgniarstwa, 18(2), 91–96. [Google Scholar]
- Andruszkiewicz, A. (2019). Wybrane psychospołeczne aspekty funkcjonowania zawodowego pielęgniarek a ich stan zdrowia. Wydawnictwo Naukowe Uniwersytetu Mikołaja Kopernika. [Google Scholar]
- Antonovsky, A. (1979). Health, stress, and coping. [Google Scholar]
- Antonovsky, A. (1987). Unraveling the mystery of health. San Francisco, p. 175. [Google Scholar]
- Badu, E. , O’Brien, A. P. , Mitchell, R. , Rubin, M. , James, C. , McNeil, K. , Nguyen, K. , & Giles, M. (2020). Workplace stress and resilience in the Australian nursing workforce: A comprehensive integrative review. International Journal of Mental Health Nursing, 29(1), 5–34. 10.1111/inm.12662 [DOI] [PubMed] [Google Scholar]
- Basińska, M. A. (1998). Factors triggering stress in a nurse's work. Psychological Forum, 3(2), 166–180. [Google Scholar]
- Behnke, A. , Conrad, D. , Kolassa, I. T. , & Rojas, R. (2019). Higher sense of coherence is associated with better mental and physical health in emergency medical services: Results from investigations on the revised sense of coherence scale (SOC‐R) in rescue workers. European Journal of Psychotraumatology, 10(1), 1606628. 10.1080/20008198.2019.1606628 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burmeister, E. A. , Kalisch, B. J. , Xie, B. , Doumit, M. A. A. , Lee, E. , Ferraresion, A. , Terzioglu, F. , & Bragadóttir, H. (2019). Determinants of nurse absenteeism and intent to leave: An international study. Journal of Nursing Management, 27(1), 143–153. 10.1111/jonm.12659 [DOI] [PubMed] [Google Scholar]
- Habersack, M. , & Luschin, G. (2013). WHO‐definition of health must be enforced by national law: A debate. BMC Medical Ethics, 14(1), 1–3. 10.1186/1472-6939-14-24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hager, M. , & Seibt, T. (2018). The relationship between work‐related behavior and experience patterns and organizational commitment. In Bilgin M., Danis H., Demir E. & Can U. (Eds.), Eurasian business perspectives (pp. 291–303). Springer. [Google Scholar]
- Heszen, I. , & Sęk, H. (2007). Psychologia zdrowia. Wydawnictwo Naukowe PWN, Warszawa, 10, 160–176. [Google Scholar]
- Jażdżewska, N. , Kretowicz, K. , & Żuralska, R. (2018). Hope for success and a sense of coherence in the nurses' professional group. Nursing Problems, 26(1), 9–14. [Google Scholar]
- Kamdar, B. B. , Tergas, A. I. , Mateen, F. J. , Bhayani, N. H. , & Oh, J. (2013). Night‐shift work and risk of breast cancer: A systematic review and meta‐analysis. Breast Cancer Research and Treatment, 138(1), 291–301. 10.1007/s10549-013-2433-1 [DOI] [PubMed] [Google Scholar]
- Kędra, E. , & Nowocień, M. (2015). Czynniki stresogenne a ryzyko wypalenia zawodowego w pracy pielęgniarek. Pielęgniarstwo Polskie, 3(57), 293–306. [Google Scholar]
- Kilańska, D. , Gorzkowicz, B. , Sienkiewicz, Z. , Lewandowska, M. , Dominiak, I. , & Bielecki, W. (2016). Evaluation of chosen determinants of the positive practice environments (PPE) at Polish nursing wards. Medycyna Pracy, 67(1), 11–19. [DOI] [PubMed] [Google Scholar]
- Koniarek, J. , Dudek, B. , Makowska, Z. , & Życiowej, K. O. (1993). Adaptacja the Sense Coherence Questionnaire (SOC) A. Antonovsky Ego. Przegląd Psychologiczny, 36(4), 98–120. [Google Scholar]
- Kowitlawkul, Y. , Yap, S. F. , Makabe, S. , Chan, S. , Takagai, J. , Tam, W. W. S. , & Nurumal, M. S. (2019). Investigating nurses’ quality of life and work‐life balance statuses in Singapore. International Nursing Review, 66(1), 61–69. 10.1111/inr.12457 [DOI] [PubMed] [Google Scholar]
- Larsson, G. (2000). Quality of life and health: Impact of sense of coherence and view of‐life. In 8th Conference of the European Health Psychology Society on Quality of life & Health Psychology, Alicate, Spain. [Google Scholar]
- Makowska, Z. , & Merecz, D. (2001). Ocena Zdrowia Psychicznego na podstawie badań Kwestionariuszami Davida Goldberga. Podręcznik dla użytkowników Kwestionariuszy GHQ‐12 i GHQ‐28. Prof. J. Nofera. [Google Scholar]
- Mroczek, B. , Kotwas, A. , Karpeta‐Pawlak, I. E. , WoliÅ, W. , Rudnicki, J. , Bikowska, M. , & Kurpas, D. (2017). Relationships between the level of social competence and work‐related behaviors in a group of physicians, nurses, and paramedics. International Journal of Psychotherapy Practice and Research, 1(1), 15. 10.14302/issn.2574-612X.ijpr-17-1634 [DOI] [Google Scholar]
- Mroczek, B. , Wolińska, W. , Kotwas, A. , Karpeta‐Pawlak, I. , & Kurpas, D. (2018). The risk of job burnout among medical workers on the basis of their work‐related behaviors. Family Medicine & Primary Care Review, 1, 28–35. 10.5114/fmpcr.2018.73701 [DOI] [Google Scholar]
- Nowicki, G. , & Ślusarska, B. (2011). Determinanty społeczno‐demograficzne wartościowania zdrowia wśród pracujących osób dorosłych. Hygeia Public Health, 46(2), 280–285. [Google Scholar]
- Ogińska‐Bulik, N. (2006). Stres zawodowy w zawodach usług społecznych [Professional stress in social services occupations: Sources, consequences, prevention]. Difin. [Google Scholar]
- Ogińska‐Bulik, N. , & Juczyński, Z. (2009). Narzędzia pomiaru stresu i radzenia sobie ze stresem [Stress and coping measures]. Pracownia Testów Psychologicznych. [Google Scholar]
- Peplonska, B. , Bukowska, A. , & Sobala, W. (2015). Association of rotating night shift work with BMI and abdominal obesity among nurses and midwives. PLoS One, 10(7), e0133761. 10.1371/journal.pone.0133761 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosa, D. , Terzoni, S. , Dellafiore, F. , & Destrebecq, A. (2019). Systematic review of shift work and nurses’ health. Occupational Medicine, 69(4), 237–243. 10.1093/occmed/kqz063 [DOI] [PubMed] [Google Scholar]
- Schulz, M. , Damkröger, A. , Voltmer, E. , Löwe, B. , Driessen, M. , Ward, M. , & Wingenfeld, K. (2011). Work‐related behaviour and experience pattern in nurses: Impact on physical and mental health. Journal of Psychiatric and Mental Health Nursing, 18(5), 411–417. 10.1111/j.1365-2850.2011.01691.x [DOI] [PubMed] [Google Scholar]
- Szcześniak, M. , & Strochalska, K. (2020). Temperament and sense of coherence: Emotional intelligence as a mediator. International Journal of Environmental Research and Public Health, 17(1), 219. 10.3390/ijerph17010219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Supreme Chamber of Nurses and Midwives in Poland (2020). https://nipip.pl/ (Last accessed 15 03 2020).
- Whitehead, D. (2018). Exploring health promotion and health education in nursing. Nursing Standard, 33(8), 38–44. 10.7748/ns.2018.e11220 [DOI] [PubMed] [Google Scholar]
- Wijesinghe, S. , & Parshall, M. B. (2016). Impermanence and sense of coherence: Lessons learned from the adaptive behaviors of Sri Lankan Buddhist nuns with a chronic illness. Journal of Transcultural Nursing, 27(2), 157–165. 10.1177/1043659614545402 [DOI] [PubMed] [Google Scholar]
- Wollesen, B. , Hagemann, D. , Pabst, K. , Schlüter, R. , Bischoff, L. L. , Otto, A.‐K. , Hold, C. , & Fenger, A. (2019). Identifying individual stressors in geriatric nursing staff—a cross‐sectional study. International Journal of Environmental Research and Public Health, 16(19), 3587. 10.3390/ijerph16193587 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.