

Abstract
Background
In this globalized and high-tech era, the computer has become an integral part of daily life. A constant use of computer for 3 hours and more per day can cause computer vision syndrome (CVS), which is one of the leading occupational hazards of the 21st century. The visual difficulties are the most common health problems associated with excessive computer use. Therefore, this study aimed to assess the prevalence and associated factors of CVS among instructors working in Ethiopian universities.
Methods
A web-based cross-sectional study was conducted among 422 university instructors in Ethiopia from February 02 to March 24, 2021. A structured and self-administered questionnaire prepared by Google Forms was shared among instructors through their e-mail addresses, Facebook, and Telegram accounts. Data cleanup and cross-checking were done before analysis using SPSS version 23. A multivariable logistic regression was applied to identify factors associated with CVS using p value <0.05 and 95% confidence interval.
Results
Of the total 416 participants, about 293 (70.4%) were reported to have CVS (95% CI: 65.9–74.5%), of which 54.6% were aged 24–33 years. Blurred vision, pain in and around the eye, and eye redness were the main symptoms reported. Working in third-established universities (AOR = 8.44, 95% CI: 5.47–21.45), being female (AOR = 2.69, 95% CI: 1.28–5.64), being 44 years old and above (AOR = 2.73, 95% CI: 1.31–5.70), frequently working on the computer (AOR = 5.51, 95% CI: 2.05–14.81), and sitting in bent back position (AOR = 8.10, 95% CI: 2.42–23.45) were the factors associated with computer vision syndrome.
Conclusions
In this study, nearly seven-tenths of instructors in Ethiopian universities reported having symptoms of computer vision syndrome. Working in third-generation universities, being female, age, frequently working on the computer, and sitting in bent back position were statistically significant predictors in computer vision syndrome. Therefore, optimizing exposure time, addressing ergonomic hazards associated with computer usage through on-the-job and off-the-job training, and making the safety guidelines accessible for all university instructors would be critical to address the problem.
1. Background
In this globalized and hi-tech era, the computer has become an integral part of daily life [1]. These devices are deliberated as the necessity of 21st century and being used at workplaces and household level. There has been a rapid increase in computer-related health problems in the current era of prolonged and extensive computer usage [2, 3]. A constant use of computer for 3 hours and more per day can cause computer vision syndrome (CVS), which is defined as a complicated eye and vision difficulty linked to the activities that stress the nearby vision during the use of a computer [4]. This visual difficulty may be caused by a combination of individual visual impediments, poor workstation settings, and insufficient working procedures [5, 6].
Computer vision syndrome is an umbrella term for many eye and environment-related disorders that arise when job-related viewing demands surpass the user's visual capabilities and is characterized by visual symptoms arising from collaboration with a computer monitor and its settings. Ninety percent of the individuals who use the computer for three to four hours daily can develop CVS, and it can be dominant with the symptoms of itching, burning, eye dryness, blurred vision, double vision, and headache that occur during or instantly after the workday [7–10].
Universally, computer vision syndrome is the leading occupational hazard of the 21st century and one of the main public health problems. Global data show that 60 million people are suffering from CVS and one million new cases occur each year. Also, its symptoms affect almost 70% of all computer customers. It is a growing public health concern and contributes significantly to reducing the quality of life and efficiency at the workplace [8, 11, 12]. The economic effect of the visual and musculoskeletal symptoms related to computer usage is great. Underestimating the symptoms that reduce occupational productivity will result in generous financial profit. Visual difficulties are the most frequently occurring health problem related to extreme computer use [13]. Because of barrier inaccessibility and consumption of personal protective equipment, workload, and poor knowledge of ergonomics during computer use, the burden of CVS is high in developing countries such as Ethiopia [14–17].
Earlier studies conducted in different countries showed that the prevalence of CVS ranges from 64% to 90% among computer users [16, 18]. Some of the studies conducted in Ethiopia attempted to figure out the prevalence of CVS and associated factors among computer users in different institutions; however, few individuals are aware of computer vision syndrome, its contributing factors, and simple prevention methods [19, 20]. Factors associated with CVS were commonly categorized as (1) personal factors such as age, poor sitting position, improper viewing distances, medical diseases, taking frequent breaks, and duration of computer usage and (2) the environment which includes improper workstation, poor lighting and computer, imbalance of light between the computer screen and working room surrounding, and poor contrast [21–25].
To the best of our knowledge, the magnitude of CVS and associated factors among instructors in Ethiopia University was not well studied. Therefore, this study was designed to assess the prevalence of CVS and associated factors among instructors working in Ethiopian universities in 2021.
2. Materials and Methods
2.1. Study Designs, Period, and Settings
A web-based cross-sectional survey was conducted among instructors working in Ethiopian universities from February 02, 2021, to March 24, 2021. Ethiopia is a large, landlocked, and diverse country with more than 90 ethnic and linguistic groups with a population of over 99 million. In Ethiopia, there are ten administrative regions and more than 80 percent of the population lives in rural areas, although there is increased urbanization as workers move from agriculture towards more productive manufacturing and services jobs. A total of 45 universities with 14 first, 23 second, and 8 third established universities are currently giving service in Ethiopia, respectively. The number of academic staff/instructors in Ethiopian universities is estimated to be 32000 [26].
2.2. Sampling and Population
The target population was all the instructors working in Ethiopian universities. The study population was all the instructors who use e-mail or social media during the data collection period. The sample size was figured out using a single population proportion formula. Considering 50% proportion, 95% level of confidence, 5% margin of error, and 10% nonresponse rate, we finally obtained 422 sample sizes.
2.3. Data Collection Tool
Data were collected through a structured, web-based, and self-administered questionnaire. First, the questionnaires were prepared in English using Google Forms by reviewing earlier studies [23, 25, 27]. The data collection tool includes sociodemographic, ergonomic practice during computer use, and computer vision syndrome items/questions.
2.4. Data Collection Methods and Procedures
The prepared Google Form link was shared with the instructors working in Ethiopian universities through their e-mail addresses, Facebook, and Telegram accounts. The Google Form was shared on official social media pages and diverse groups of Ethiopian university instructors' associations/unions to ensure equal representation of participants during the data collection process. The questionnaire became accessible after accepting the terms and conditions of the study. The link to the online Google Form is found at https://docs.google.com/forms/d/e/1FAIpQLSfv5rN6cUJxy6EGp0tW4yUdTuqE8amwi190i7dqCW9htmg5PA/viewform?vc=0&c=0&w=1&flr=0&usp=mail_form_link.
2.5. Data Processing and Analysis
The responses of Google Forms were transferred to an Excel sheet and then exported to SPSS 23. Data cleanup and cross-checking were done before analysis using SPSS 23. The frequency, cross-tabulation, charts were used in descriptive analysis. All required assumptions were checked to apply multivariable logistic regression to identify factors associated with computer vision syndrome. In this regard, Hosmer and Lemeshow's model fitness test was used and multicollinearity of independent variables was checked using variance inflation factor (VIF). The variables with a p value of <0.20 in the bivariable analysis can be a candidate for the multivariable binary logistic regression. All variables in the multivariable analysis were considered as statistically significant if p value is <0.05 with 95% confidence level.
2.6. Operational Definitions
2.6.1. Presence of Computer Vision Syndrome (CVS)
In the past one year, if the respondents select at least one of the CVS symptoms such as headache, pain in and around the eye, blurred vision, dry eyes, eye redness, burning sensation, and double vision, the presence of CVS was coded as “yes = 1” if CVS symptoms were reported and “no = 0” if CVS symptoms have not been reported [19, 28].
2.6.2. 20-20-20 Rule for the Eye
After 20 minutes of computer usage, look at something 20 feet away for 20 seconds [29].
2.6.3. First/Second/Third Established University
The 1st, 2nd, and 3rd oldest universities established in Ethiopia were selected, respectively.
3. Results
3.1. Sociodemographic Characteristics
A total of 416 respondents have completed the online survey questionnaire with a participation rate of 98.6%. Of these participants, about 144 (34.6%) were from the Oromia region and 219 (52.6%) were from second established universities. The majority (72.4%) of respondents were males, and 227 (54.6%) were within the age group of 24–33 years. Concerning educational status, around 317 (76.2%) of respondents attained up to the second degree or masters and 150 (36.1%) of them were within the 1–5 service years' category (Table 1).
Table 1.
Sociodemographic characteristics of instructors in Ethiopian universities, 2021 (n = 416).
| Variables | Frequency | Percent |
|---|---|---|
| Regions | ||
| Harari | 3 | .7 |
| Sidama Zone | 4 | 1.0 |
| Gambella | 9 | 2.2 |
| Somali | 10 | 2.4 |
| Dire Dawa | 12 | 2.9 |
| Tigrai | 20 | 4.8 |
| Benishangul-Gumuz | 21 | 5.0 |
| SNNP | 56 | 13.5 |
| Oromia | 144 | 34.6 |
|
| ||
| Stage of university | ||
| First generation | 133 | 32.0 |
| Second generation | 219 | 52.6 |
| Third generation | 64 | 15.4 |
|
| ||
| Sex | ||
| Male | 301 | 72.4 |
| Female | 115 | 27.6 |
|
| ||
| Educational status | ||
| First degree (BSc or BA) | 52 | 12.5 |
| Second degree (Master's) | 317 | 76.2 |
| Third degree (PhD) | 47 | 11.3 |
|
| ||
| Age | ||
| 24–33 years | 227 | 54.6 |
| 34–43 years | 162 | 38.9 |
| 44 years and above | 27 | 6.5 |
|
| ||
| Service years | ||
| 1–5 | 150 | 36.1 |
| 6–10 | 129 | 31.0 |
| 11–15 | 102 | 24.5 |
| 16 and above | 35 | 8.4 |
3.2. Ergonomic Practices during Computer Utilization
In this study, about 228 (54.8%) respondents were reported to use laptop only. During computer utilization, around 327 (78.6%) respondents adjust the brightness of their computer. About 43% and 83.4% of respondents work on their computer frequently and take regular breaks of 20–60 minutes per day, respectively. Concerning regular sitting position, 159 (38.2%) respondents reported the frequent sitting position with the bent back (Table 2).
Table 2.
Ergonomic practices and awareness during computer use among instructors in Ethiopian universities, 2021 (n = 416).
| Items/questions | Frequency | Percent |
|---|---|---|
| Types of computer used | ||
| Laptop only | 258 | 62.0 |
| Laptop and desktop | 153 | 36.8 |
| Desktop only | 5 | 1.2 |
|
| ||
| Currently use eyeglass | ||
| Yes | 228 | 54.8 |
| No | 188 | 45.2 |
|
| ||
| Do you know the 20-20-20 rule for eyes? | ||
| Yes | 175 | 42.1 |
| I do not know | 241 | 57.9 |
|
| ||
| Is your institution having workplace safety guideline? | ||
| Yes | 158 | 38.0 |
| No | 211 | 50.7 |
| I do not know | 47 | 11.3 |
|
| ||
| Do you always adjust the brightness of your computer? | ||
| Yes | 327 | 78.6 |
| No | 89 | 21.4 |
|
| ||
| How often do you work on your computer? | ||
| Rarely | 22 | 5.3 |
| Sometimes | 57 | 13.7 |
| Often | 179 | 43.0 |
| Always | 158 | 38.0 |
|
| ||
| How often is your sitting position upright with bending back? | ||
| Never | 21 | 5.0 |
| Rarely | 61 | 14.7 |
| Sometimes | 137 | 32.9 |
| Often | 159 | 38.2 |
| Always | 38 | 9.1 |
|
| ||
| Health break per day | ||
| 20–60 minutes | 347 | 83.4 |
| 61–120 minutes | 69 | 16.6 |
3.3. Prevalence of Computer Vision Syndrome (CVS)
Among the total participants involved in the study, about 293 (70.4%) were reported to have computer vision syndrome (95% CI: 65.9–74.5%). Commonly reported computer vision syndrome was blurred vision (9.9%), pain in and around the eye (11.1%), and eye redness (8.9%). 134 (32.2%) and 163 (39.2%) respondents reported moderate and severe computer vision syndrome, respectively (Figures 1 and 2).
Figure 1.
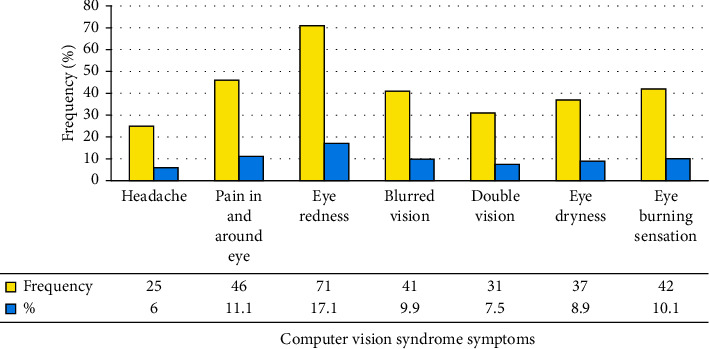
The symptoms of computer vision syndrome mentioned by university instructors in Ethiopia, 2021.
Figure 2.
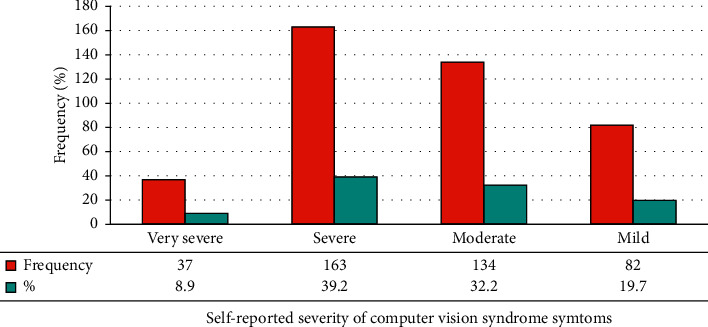
Self-reported severity of computer vision syndrome symptoms among instructors working in Ethiopia universities, 2021.
3.4. Factors Associated with Computer Vision Syndrome
The respondents who were working in second and third established Ethiopian universities were nearly seven and eight times more likely to develop computer vision syndrome (CVS) than those working in the first established universities (AOR = 7.34, 95% CI: 5.36–17.54 and AOR = 8.44, 95% CI: 5.47–21.45), respectively. The odds of developing CVS among females were nearly three times higher than males (AOR = 2.69, 95% CI: 1.28–5.64). The instructors within the age category of 44 years old and above were nearly 3 times more likely to develop CVS than their counterparts (AOR = 2.73, 95% CI: 1.31–5.70). The respondents more frequently (always/often) working on their computer were 5.5 times more likely to develop CVS when compared to those working on their computer less frequently (rarely/sometimes) (AOR = 5.51, 95% CI: 2.05–14.81). Regarding ergonomic practices, the instructors who more frequently sit in bent back positions were eight times more likely to report CVS than their counterparts (AOR = 8.10, 95% CI: 2.42–23.45). The odds of having CVS among instructors who did not use eyeglass were 68% less likely than eyeglass users (AOR = 0.32, 95% CI: 0.15–0.67). The instructors who do not know the presence of workplace safety guidelines were nearly six times more likely to develop CVS than their counterparts (AOR = 6.37, 95% CI: 1.68–14.34) (Table 3).
Table 3.
Bivariable and multivariable logistic regression analysis for computer vision syndrome among instructors in Ethiopian universities, 2021 (n = 416).
| Variables | Presence of CVS | COR (95% CI) | AOR (95% CI) | |
|---|---|---|---|---|
| Yes (%) | No (%) | |||
| Sex | ||||
| Male | 213 (70.8) | 88 (29.2) | 1 | 1 |
| Female | 80 (69.6) | 35 (30.4) | 1.99 (1.04–3.80)∗ | 2.69 (1.28–5.64)∗∗ |
|
| ||||
| Stage of university | ||||
| First generation | 42 (31.6) | 91 (68.4) | 1 | 1 |
| Second generation | 158 (72.1) | 61 (27.9) | 7.34 (5.45–20.16)∗ | 6.14 (2.45–19.16)∗∗ |
| Third generation | 44 (68.8) | 20 (31.3) | 6.56 (4.78–18.47)∗ | 5.46 (3.78–16.47)∗∗ |
|
| ||||
| Educational status | ||||
| First degree (BSc or BA) | 31 (59.6) | 21 (40.4) | 1 | |
| Second degree (Master's) | 230 (72.6) | 87 (27.4) | 3.24 (1.36–7.69)∗ | |
| Third degree (PhD) | 32 (68.1) | 15 (31.9) | 2.71 (0.86–8.58) | |
|
| ||||
| Age | ||||
| 24–33 years | 157 (69.2) | 70 (30.8) | 1 | 1 |
| 34–43 years | 121 (74.7) | 41 (25.3) | 0.36 (0.11–1.16) | 0.62 (0.16–2.41) |
| 44 years and above | 121 (74.7) | 41 (25.3) | 2.35 (1.25–4.38)∗ | 2.73 (1.31–5.70)∗∗ |
|
| ||||
| Currently use eyeglass | ||||
| Yes | 162 (71.1) | 66 (28.9) | 1 | 1 |
| No | 131 (69.7) | 57 (30.3) | 0.41 (0.23–0.73)∗ | 0.32 (0.15–0.67)∗ |
|
| ||||
| Types of computer used | ||||
| Laptop only | 183 (70.9) | 75 (29.1) | 1 | 1 |
| Laptop and desktop | 108 (70.6) | 45 (29.4) | 0.81 (0.44–1.50) | 0.54 (0.27–1.07) |
| Desktop only | 2 (40.0) | 3 (60.0) | 0.56 (0.36–0.64)∗ | 0.42 (0.16–0.81)∗∗ |
|
| ||||
| Health break per day | ||||
| 20–60 minutes | 242 (69.7) | 105 (30.3) | 1 | |
| 61–120 minutes | 51 (73.9) | 18 (26.1) | 1.69 (0.80–3.57) | |
|
| ||||
| Know the 20-20-20 rule | ||||
| Yes | 118 (67.4) | 57 (32.6) | 1 | |
| I do not know | 118 (67.4) | 57 (32.6) | 1.29 (0.84–1.96) | |
|
| ||||
| Presence of workplace safety guideline | ||||
| Yes | 107 (67.7) | 51 (32.3) | 1 | 2.58 (1.10–6.06)∗∗ |
| No | 151 (71.6) | 60 (28.4) | 0.99 (0.54–1.84) | 6.37 (1.68–14.37)∗∗ |
| I do not know | 12 (25.5) | 35 (74.5) | 2.07 (0.71–6.07) | 2.58 (1.10–6.06)∗∗ |
|
| ||||
| Adjust the brightness of the computer | ||||
| Yes | 229 (70.0) | 98 (30.0) | 1 | |
| No | 64 (71.9) | 25 (28.1) | 1.57 (0.79–3.13) | 0.199 |
|
| ||||
| Duration of working on the computer | ||||
| Rarely | 9 (40.9) | 13 (59.1) | 1 | 1 |
| Sometimes | 33 (57.9) | 24 (42.1) | 0.68 (0.12–1.35) | 1.20 (0.44–3.31) |
| Often | 132 (73.7) | 47 (26.3) | 2.06 (1.24–6.54)∗ | 3.35 (1.89–8.95)∗∗ |
| Always | 119 (75.3) | 39 (24.7) | 3.97 (1.65–9.55)∗ | 5.51 (2.05–14.81)∗∗ |
|
| ||||
| Sitting position with bending back | ||||
| Never | 13 (61.9) | 8 (38.1) | 1 | 1 |
| Rarely | 39 (63.9) | 22 (36.1) | 0.85 (0.30–2.42) | 0.76 (0.29–1.99) |
| Sometimes | 90 (65.7) | 47 (34.3) | 0.25 (0.04–1.44) | 0.81 (0.15–4.35) |
| Often | 121 (76.1) | 38 (23.9) | 2.23 (1.13–4.41)∗ | 1.97 (0.90–4.32) |
| Always | 30 (78.9) | 8 (21.1) | 5.52 (1.83–16.60)∗ | 8.11 (2.42–23.45)∗∗ |
∗ p < 0.05, crude odds ratio; ∗∗p < 0.05, adjusted odds ratio.
4. Discussion
Computer vision syndrome (CVS) is a public health problem associated with computer use. Occupational health and safety regrettably take a backseat most of the time in developing countries such as Ethiopia [29, 30]. This study was designed to assess the prevalence of CVS and associated factors among instructors in Ethiopian universities. In this study, seven out of ten respondents (70.4%) had computer vision syndrome (CVS), with 32.2% moderate and 39.2% severe symptoms, respectively. This finding was similar to that of study conducted in Debre Tabor town, Ethiopia, 69.5% [31], and Malaysia, 68.1% [27]. This consistency might be due to similar characteristics of respondents in computer use. These findings were less than those of a study from Chennai, India, which showed 80.3% [32]. The probable reason for the discrepancy might be either due to sociodemographic variation, study settings, and different duration of exposure to computer electromagnetic radiation. In our study, the most frequent CVS symptoms reported by instructors were redness of the eye and pain in and around the eye, followed by eye burning sensation. These study findings are found to be lower than the findings from Debre Tabor, Ethiopia [31], and India [33]. This discrepancy might be due to sampling size, study participants' age groups, and computer work duration differences.
Computer vision syndrome expressively damages workstation productivity and moderates the quality of life by assigning uncommon strain on the human physical well-being. Regrettably, in this study, some important variables such as duration of university establishment, sex, age, using eyeglass, frequent working, and sitting with bent back position during computer use were factors associated with computer vision syndrome. The instructors working in Ethiopian universities established at the second and third stage were more likely to develop CVS than those working in the first established universities. This observed difference might be due to differences in the implementation of workplace safety guidelines; the most senior universities may have proper infrastructures, services, and supplies that enable instructors to minimize CVS.
The odds of having CVS among females were higher compared to males. This finding was comparable with the study finding in Malaysia, which shows that females have higher odds for CVS when compared to males [27]. This higher rate could be explained by the fact that women more frequently work on the computer and sit in inappropriate positions than males [34]. Our study has revealed that using the eyeglass was significantly associated with CVS; the odds of having CVS among instructors who did not use eyeglass were 68% less likely than eyeglass users. A potential explanation of decreased odds of CVS among those not using eyeglass might be that computer tasks are a type of near work that looks at letters on the screen without shaped tiny dots called pixels.
On the contrary, when the eyeglass is used, it is a little harder to retain the focus images while consistently working on the computer [10]. The respondents within the age category of 44 years and above were nearly 3 times more likely to develop CVS than younger participants. This might be explained by that as age increases, the probability of developing CVS also increases. This finding is inconsistent with the study finding in Malaysia, which shows that the younger age groups were at higher risk of developing CVS [27]. The respondents who were more frequently working on their computers were more likely to develop CVS when compared to those working on their computers less frequently. This might be because a computer emanates electromagnetic radiation or high-energy blue light, which stresses the ciliary muscle in the eye; eventually, a continued exposure to a computer screen causes eye stress. Thus, minimizing the duration of exposure to a computer is important to reduce CVS [10]. This study finding was comparable with that in Debre Tabor, Ethiopia [31], and elsewhere [16, 27].
Regarding ergonomic practices, the respondents who had frequent sitting positions with bending back were more likely to report CVS than their counterparts. This type of practice may reduce the distance between the eye and computer, which exposes them to more electromagnetic radiation emitting from the computer. This study finding was comparable to study findings in Gondar, Ethiopia [25]. The instructors who do not know the presence of workplace safety guidelines were more likely to develop CVS than their counterparts. This might be because they have no probability of using/reading safety guidelines to understand ergonomic hazards and their prevention measures.
4.1. Limitation of the Study
This study has a few limitations, such as the ophthalmic checkup was not performed to measure CVS, but was based only on the self-reported symptoms. Since the study used a web-based survey, the respondents were limited to social media and Internet users. The study findings might not reveal the whole country's actual condition due to the underrepresentation of certain universities. The study might not reveal the cause-effect association between dependent and independent variables due to the study's cross-sectional nature.
5. Conclusion
Regardless of the above limitation, this study revealed that seven-tenth of instructors in Ethiopian universities reported symptoms of CVS. The most frequent symptoms of CVS reported by instructors were redness of eyes, pain in and around the eye, and burning sensation of the eye. The factors such as university's establishment, sex, age, eyeglass use, types of computer used, workplace safety guidelines, duration of working on the computer, and sitting in bent back position at the computer were identified as associated factors of CVS. Therefore, optimizing the exposure time and minimizing the ergonomic hazards related to computer use through proper job training by developing workplace safety guidelines and making them accessible to all instructors are essential to tackle the problem.
Acknowledgments
The authors would like to thank all study participants and Madda Walabu University for their helpful participation in this study.
Abbreviations
- CVS:
Computer vision syndrome
- AOR:
Adjusted odds ratio
- COR:
Crude odds ratio.
Data Availability
Data will be made available from the primary author upon reasonable request.
Ethical Approval
The online survey was conducted in accordance with Helsinki Declaration after ethical clearance was obtained from the Ethical Review Board of the Madda Walabu University Goba Referral Hospital. Participants were informed to fill the online self-administered questionnaire voluntarily with a full right not to respond to all or any of the questions. The online survey has no personal identifier, so that anonymity was kept. The first online pages for the self-administered questionnaire could be accessed by the participants and have information to go ahead to the next page if they fully consent to take part.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Authors' Contributions
DZ participated in conception and design, acquisition of data, or analysis and interpretation of data and took part in drafting the article. BS, YT, MB, and JA participated in the sequence alignment and design of the study and performed the statistical analysis. VC conceived the study and participated in its design and coordination and helped in editing English language. All authors read and approved the final manuscript.
References
- 1.Mani K. Ergonomics education for office computer workers: an evidence-based strategy. In: Korhan O., editor. Anatomy, Posture, Prevalence, Pain, Treatment and Interventions of Musculoskeletal Disorders . First. London, UK: InTech; 2018. [Google Scholar]
- 2.Singh H., Tigga M. J., Laad S., Khan N. Prevention of ocular morbidity among medical students by prevalence assessment of asthenopia and its risk factors. Journal of Evidence Based Medicine and Healthcare . 2016;3(15):532–536. doi: 10.18410/jebmh/2016/122. [DOI] [Google Scholar]
- 3.Bali J., Navin N., Thakur B. Computer vision syndrome: a study of the knowledge, attitudes and practices in Indian ophthalmologists. Indian Journal of Ophthalmology . 2007;55(4):p. 289. doi: 10.4103/0301-4738.33042. [DOI] [PubMed] [Google Scholar]
- 4.Sen A., Richardson S. A study of computer-related upper limb discomfort and computer vision syndrome. Journal of Human Ergology . 2007;36(2):45–50. [PubMed] [Google Scholar]
- 5.Millodot M. Dictionary of Optometry and Visual Science E-Book . Philadelphia, PA, USA: Elsevier Health Sciences; 2014. [Google Scholar]
- 6.Logaraj M., Madhupriya V., Hegde S. Computer vision syndrome and associated factors among medical and engineering students in Chennai. Annals of Medical and Health Sciences Research . 2014;4(2):179–185. doi: 10.4103/2141-9248.129028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gangamma M., Poonam M. R., Rajagopala M. A clinical study on “Computer vision syndrome” and its management with Triphala eye drops and Saptamrita Lauha. AYU (An International Quarterly Journal of Research in Ayurveda) . 2010;31(2):p. 236. doi: 10.4103/0974-8520.72407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Charpe N. A., Kaushik V. Computer vision syndrome (CVS): recognition and control in software professionals. Journal of Human Ecology . 2009;28(1):67–69. doi: 10.1080/09709274.2009.11906219. [DOI] [Google Scholar]
- 9.Akinbinu T. R., Mashalla Y. Knowledge of computer vision syndrome among computer users in the workplace in Abuja, Nigeria. Journal of Physiology and Pathophysiology . 2013;4(4):58–63. [Google Scholar]
- 10.Louis S. American optometric association (AOA) the association. 2013. https://wwwaoaorg/2013 Oct 30 .
- 11.Wimalasundera S. Computer vision syndrome. Galle Medical Journal . 2009;11(1) doi: 10.4038/gmj.v11i1.1115. [DOI] [Google Scholar]
- 12.Tadesse S., Kelaye T., Assefa Y. Utilization of personal protective equipment and associated factors among textile factory workers at Hawassa Town, Southern Ethiopia. Journal of Occupational Medicine and Toxicology . 2016;11(1):1–6. doi: 10.1186/s12995-016-0096-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Portello J. K., Rosenfield M., Bababekova Y., Estrada J. M., Leon A. Computer-related visual symptoms in office workers. Ophthalmic and Physiological Optics . 2012;32(5):375–382. doi: 10.1111/j.1475-1313.2012.00925.x. [DOI] [PubMed] [Google Scholar]
- 14.Hayes J. R., Sheedy J. E., Stelmack J. A., Heaney C. A. Computer use, symptoms, and quality of life. Optometry and Vision Science . 2007;84(8):E738–E755. doi: 10.1097/opx.0b013e31812f7546. [DOI] [PubMed] [Google Scholar]
- 15.Shantakumari N., Eldeeb R., Sreedharan J., Gopal K. Computer use and vision-related problems among university students in Ajman, United Arab Emirate. Annals of Medical and Health Sciences Research . 2014;4(2):258–263. doi: 10.4103/2141-9248.129058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ranasinghe P., Wathurapatha W. S., Perera Y. S., et al. Computer vision syndrome among computer office workers in a developing country: an evaluation of prevalence and risk factors. BMC Research Notes . 2016;9(1):150–159. doi: 10.1186/s13104-016-1962-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Anshel J. Visual Ergonomics Handbook . Boca Raton, FL, USA: CRC Press; 2005. [Google Scholar]
- 18.Bali J., Neeraj N., Bali R. Computer vision syndrome: a review. Journal of clinical ophthalmology and research . 2014;2(1):p. 61. doi: 10.4103/2320-3897.122661. [DOI] [Google Scholar]
- 19.Alemayehu M., Nega A., Tegegne E., Mule Y. Prevalence of self reported computer vision syndrome and associated factors among secretaries and data processors who are working in University of Gondar, Ethiopia. Journal of Biology, Agriculture and Healthcare . 2014;4(15) [Google Scholar]
- 20.Harris M. G., Sheedy J. E., Gan C. M. Vision and task performance with monovision and diffractive bifocal contact lenses. Optometry and Vision Science: Official Publication of the American Academy of Optometry . 1992;69(8):609–614. doi: 10.1097/00006324-199208000-00003. [DOI] [PubMed] [Google Scholar]
- 21.Agarwal S., Goel D., Sharma A. Evaluation of the factors which contribute to the ocular complaints in computer users. Journal of Clinical and Diagnostic Research: Journal of Clinical and Diagnostic Research . 2013;7(2):331–5. doi: 10.7860/JCDR/2013/5150.2760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Galinsky T. L., Swanson N. G., Sauter S. L., Hurrell J. J., Schleifer L. M. A field study of supplementary rest breaks for data-entry operators. Ergonomics . 2000;43(5):622–638. doi: 10.1080/001401300184297. [DOI] [PubMed] [Google Scholar]
- 23.Chiemeke S. C., Akhahowa A. E., Ajayi O. B., editors. Evaluation of vision-related problems amongst computer users: a case study of University of Benin, Nigeria. Proceedings of the World Congress on Engineering; July 2007; London, UK. [Google Scholar]
- 24.Ihemedu C. O., Omolase C. O. The level of awareness and utilization of computer shields among computer users in a Nigerian community. Asian Journal of Medical Sciences . 2010;1(2):49–52. [Google Scholar]
- 25.Assefa N. L., Weldemichael D. Z., Alemu H. W., Anbesse D. H. Prevalence and associated factors of computer vision syndrome among bank workers in Gondar City, northwest Ethiopia, 2015. Clinical Optometry . 2017;9:p. 67. doi: 10.2147/OPTO.S126366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Salmi J., Sursock A., Olefir A. Improving the Performance of Ethiopian Universities in Science and Technology . Washington, DC, USA: World Bank; 2017. [Google Scholar]
- 27.Rahman Z. A., Sanip S. Computer user: demographic and computer related factors that predispose user to get computer vision syndrome. International Journal of Business, Humanities and Technology . 2011;1(2):84–91. [Google Scholar]
- 28.Bhanderi D., Choudhary S., Doshi V. A community-based study of asthenopia in computer operators. Indian Journal of Ophthalmology . 2008;56(1):p. 51. doi: 10.4103/0301-4738.37596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Gyawali R., Toomey M., Stapleton F., et al. Quality of 2019 American optometric association clinical practice guideline for diabetic eye care. Ophthalmic and Physiological Optics . 2021;41(1):165–170. doi: 10.1111/opo.12763. [DOI] [PubMed] [Google Scholar]
- 30.Akinbinu T. R. M. Y. Impact of computer technology on health: computer vision syndrome (CVS) Medical Practice and Reviews . 2016;5(3):20–30. [Google Scholar]
- 31.Dessie A., Adane F., Nega A., Wami S. D., Chercos D. H. Computer vision syndrome and associated factors among computer users in Debre Tabor town, Northwest Ethiopia. Journal of environmental and public health . 2018;2018:p. 4107590. doi: 10.1155/2018/4107590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Logaraj M., Priya V. M., Seetharaman N., Hedge S. K. Practice of ergonomic principles and computer vision syndrome (CVS) among under graduates students in Chennai. National Journal of Medical Research . 2013;3(2):111–116. [Google Scholar]
- 33.Talwar R., Kapoor R., Puri K., Bansal K., Singh S. A study of visual and musculoskeletal health disorders among computer professionals in NCR Delhi. Indian Journal of Community Medicine . 2009;34(4):p. 326. doi: 10.4103/0970-0218.58392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rahman Z. A., Atiya A. S. Prevalence of work-related upper limbs symptoms (WRULS) among office workers. Asia-Pacific Journal of Public Health . 2009;21(3):252–258. doi: 10.1177/1010539509341423. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data will be made available from the primary author upon reasonable request.