

Abstract
Sodium-glucose cotransporter-2 inhibitors (SGLT2i) improve cardiovascular outcomes in patients with type 2 diabetes mellitus (T2D). The comparative efficacy of individual SGLT2i remains unclear. We searched PubMed, www.clinicaltrials.gov and the Cochrane Central Register of Controlled Trials for randomised controlled trials exploring the use of canagliflozin, dapagliflozin, empagliflozin or ertugliflozin in patients with T2D. Comparators included placebo or any other active treatment. The primary endpoint was all-cause mortality. Secondary endpoints were cardiovascular mortality and worsening heart failure (HF). Evidence was synthesised using network meta-analysis (NMA). Sixty-four trials reporting on 74,874 patients were included. The overall quality of evidence was high. When compared with placebo, empagliflozin and canagliflozin improved all three endpoints, whereas dapagliflozin improved worsening HF. When compared with other SGLT2i, empagliflozin was superior for all-cause and cardiovascular mortality reduction. Empagliflozin, canagliflozin and dapagliflozin had similar effects on improving worsening HF. Ertugliflozin had no effect on any of the three endpoints investigated. Sensitivity analyses including extension periods of trials or excluding studies with a treatment duration of < 52 weeks confirmed the main results. Similar results were obtained when restricting mortality analyses to patients included in cardiovascular outcome trials (n = 38,719). Empagliflozin and canagliflozin improved survival with empagliflozin being superior to the other SGLT2i. Empagliflozin, canagliflozin and dapagliflozin had similar effects on improving worsening HF. Prospective head-to-head comparisons would be needed to confirm these results.
Electronic supplementary material
The online version of this article (10.1007/s10741-020-09954-8) contains supplementary material, which is available to authorized users.
Keywords: Sodium-glucose cotransporter-2 inhibitors, Type 2 diabetes, Mortality, Heart failure, Efficacy
Introduction
Sodium-glucose cotransporter-2 inhibitors (SGLT2i) are a new class of oral anti-diabetic drugs (OAD) with a moderate effect on glycaemic control and a low risk of hypoglycaemia and weight gain [1, 2]. Current evidence suggests that SGLT2i improve cardiovascular endpoints including all-cause mortality, cardiovascular mortality, heart failure (HF) and atherosclerotic macrovascular events [3]. The magnitude of cardiovascular risk reduction with SGLT2i, however, differed between trials [3–6]. Furthermore, there is concern regarding the potential cardiovascular safety of some OAD [7]. There is thus remaining uncertainty about the comparative efficacy of individual SGLT2i or whether a class effect can be assumed. To date, there are no prospective or retrospective head-to-head comparisons of individual SGLT2i. Given the required sample size and associated costs, a comparative SGLT2i trial may never be done. We therefore performed a network meta-analysis (NMA) of randomised controlled trials to compare comprehensively the cardiovascular benefits of SGLT2i in patients with type 2 diabetes mellitus (T2D).
Methods
NMA is an extension of pairwise meta-analysis in which multiple treatments are being compared using both direct comparisons of interventions within randomised controlled trials and indirect comparisons across trials based on a common comparator. NMA has advantages over pairwise meta-analysis, such as clarification of inconsistent outcomes from multiple studies including multiple common comparators and indirect effect calculation of missing direct comparisons between important treatments. Also, NMA can provide increased statistical power and cross-validation of the observed treatment effect of weak connections with reasonable network connectivity and sufficient sample sizes. This results in greater precision of treatment effect estimates and the ability to rank all the interventions in a coherent way.
We performed the present review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension statement for reporting systematic reviews incorporating NMAs of health care interventions [8–11]. The protocol of the NMA was prospectively registered at final registration ID at PROSPERO: CRD42020151112.
Identification and selection of studies
We searched electronic databases (PubMed, Cochrane Central Register of Controlled Trials) and websites (www.clinicaltrials.gov) up to August 12, 2019 for randomised controlled trials investigating the use of canagliflozin, dapagliflozin, empagliflozin or ertugliflozin in patients with T2D. Details of the search strategy are provided in the supplemental material. In addition, reviews and meta-analyses of SGLT2i published in PubMed between 2017 and 2019 were screened for additional SGLT2i trials. Two reviewers independently screened citations against the following predefined selection criteria.
Study design
Prospective randomised controlled trials with either parallel-group (all endpoints) or cross-over design (worsening heart failure (HF) only) were included. There were no restrictions regarding date of publication, language or sample size.
Population
We included studies evaluating adults (≥ 18 years) with a diagnosis of T2D and treatment with SGLT2i for at least 24 weeks. There were no restrictions regarding sex, race, background diabetes treatment or dose of SGLT2i.
Interventions
Treatment was with either canagliflozin, dapagliflozin, empagliflozin or ertugliflozin for at least 24 weeks. This arbitrary limit of 24 weeks was chosen to allow a potential survival benefit to become detectable against the overall low short-term baseline mortality in diabetic cohorts. Analyses were restricted to canagliflozin, dapagliflozin, empagliflozin and ertugliflozin since these agents have been approved by both the United States Food and Drug Administration and the European Medicines Agency.
Comparators
Placebo or standard medical care.
Outcomes
Primary outcome was all-cause mortality. Secondary outcomes included cardiovascular mortality and worsening HF.
Data extraction and quality assessment
All relevant articles were independently reviewed by two investigators to assess the eligibility of the article and abstract with standardised data abstraction forms, and disagreement was resolved by a third investigator. For each trial included, details were extracted on study design, patient characteristics, interventions and outcomes. The quality of included trials was assessed using the Cochrane Collaboration Criteria [12].
Statistical analyses
This NMA was conducted with Stata software 15.0 (StataCorp, College Station, TX, USA) using the network family of commands [13, 14]. A random effects model was applied. The NMA was performed to obtain estimates for outcomes of primary and secondary endpoints, presented as relative risks (RR) and 95% confidence intervals (CI) for binary outcomes. The plot of a network of drugs was used as a visual representation of the evidence base and offered a concise description of its characteristics. It consists of nodes representing the drugs being compared and edges representing the available direct comparisons (comparisons evaluated in at least one study) between pairs of drugs [14–16]. The quality of treatment effect estimates was rated following the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach [17, 18]. In order to make the rank of treatments, we used the surface under the cumulative ranking probabilities (SUCRA)—a transformation of the mean rank that accounts both for the location and the variance of all relative treatment effects [19]. SUCRA values range from 0 to 1.0. The higher the SUCRA value, and the closer to 1.0, the higher the likelihood that a therapy is in the top rank or one of the top ranks; the closer to 0 the SUCRA value, the more likely that a therapy is in the bottom rank, or one of the bottom ranks [20]. To check for a publication bias, we designed a funnel plot [14]. Consistency of results was evaluated in each loop by calculation of an inconsistency factor and statistical significance determined via z-test [16, 21].
For trials comprising a core period and an extension period, results of the core period were considered in the main analyses. To test the stability of the results, we performed a sensitivity analysis by including the results of the extension periods of the respective trials, provided that double-blind treatment was continued unchanged during the extension period. If treatment changed during the extension period of a trial, only results from the core period were considered. Additional sensitivity analyses excluded studies with a high risk of bias, studies with a treatment duration < 52 weeks and those not designed as cardiovascular outcome trials. Data on different dosages of active treatments and/or comparators were pooled for each study. Study arms including more than one active treatment (= combination therapy) were excluded from endpoint analyses. All p values were two-tailed with the statistical significance arbitrarily set at < 0.05.
Results
Literature search
The search strategy yielded 73 eligible records reporting on 64 trials [4–6, 22–87]. For three trials (NCT02681094, NCT02630706, NCT00736879), results were not published in a peer-reviewed journal but open to public at www.clinicaltrials.gov. Information on study design and results were thus extracted from www.clinicaltrials.gov. The flowchart of the study selection process is shown in eFig. 1. Agreement between reviewers was excellent (κ = 0.935, 95% CI 0.891–0.980).
No trials directly compared two different SGLT2i. A total of 44 trials compared SGLT2i with placebo, and 18 trials compared SGLT2i with other active treatments. Two trials compared SGLT2i with both placebo and another active treatment. Canagliflozin was studied in 14 trials (n = 22,220 patients), whereas dapagliflozin was studied in 30 trials (n = 31,863 patients). Thirteen trials including 15,716 patients investigated the use of empagliflozin, and seven trials studied ertugliflozin (n = 5074 patients). The corresponding network plots detailing active treatments and endpoints reported are shown in Fig. 1a–c. All but one were multicentre, parallel-group trials and the mean treatment duration of the core trials was 40 weeks. Fifteen trials comprised a core period and an extension period, in which double-blind treatment was continued unchanged. The mean study duration including extension periods was 52 weeks. In total, the 64 trials reported data from 74,874 patients. Of these, 3155 patients were randomised to a combination treatment of more than one study drug and were therefore excluded from endpoint analyses. Outcome data were thus analysed from 71,719 patients. For study characteristics of trials included in the present NMA, please refer to Table 1.
Fig. 1.
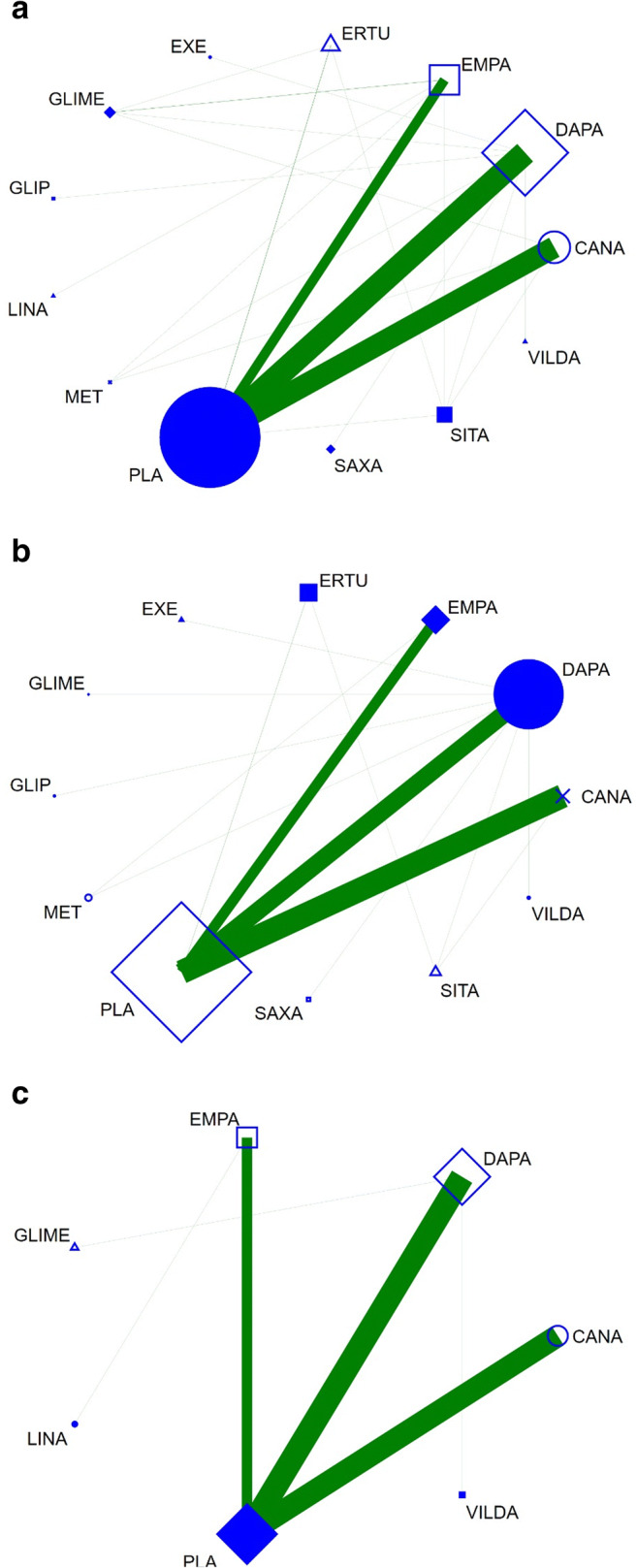
Network plots with respect to a all-cause mortality, b cardiovascular mortality, and c worsening HF. Legend: CANA, canagliflozin; DAPA, dapagliflozin; EMPA, empagliflozin; ERTU, ertugliflozin; EXE, exenatide; GLIME, glimepiride; GLIP, glipizide; LINA, linagliptin; MET, metformin; PLA, placebo; SAXA, saxagliptin; SITA, sitagliptin; VILDA, vildagliptin. Nodes represent the interventions of interest and edges represent available direct comparisons between pairs of interventions. Nodes and edges are weighted according to the number of studies including the respective interventions. Coloured edges are employed to present the risk of bias for each direct comparison in the network, with green, yellow and red colours being used to denote pairwise meta-analyses of low, unclear and high risk of bias
Table 1.
Baseline characteristics of included studies
| Study | NCT number | Year | Sponsor | Active treatment | Comparator | Centres (n) | Patients (n) | Treatment duration (weeks) | |
|---|---|---|---|---|---|---|---|---|---|
| Core period | Extension period | ||||||||
| Bailey [22] | NCT00528879 | 2010 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 80 | 546 | 24 | n.a. |
| Bailey [23] | n.a. | 2012 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 63 | 282 | 24 | n.a. |
| Barnett [24] | NCT01164501 | 2014 | Boehringer Ingelheim, Eli Lilly | Empagliflozin | Placebo | 127 | 738 | 52 | n.a. |
| Bode [25] | NCT01106651 | 2013 | Janssen Research & Development, LLC | Canagliflozin | Placebo | 90 | 716 | 26 | n.a. |
| Bolinder [26, 27] | NCT00855166 | 2012, 2014 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 40 | 182 | 24 | 78 |
| Cefalu [28] | NCT00968812 | 2013 | Janssen Research & Development, LLC | Canagliflozin | Glimepiride | 157 | 1450 | 52 | n.a. |
| Cefalu [29] | NCT01031680 | 2015 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 141 | 922 | 24 | 28 |
| Dagogo-Jack [30] | NCT02036515 | 2018 | Merck & Co., Inc. | Ertugliflozin | Placebo | 104 | 462 | 26 | 26 |
| DeFronzo [31] | NCT01422876 | 2015 | Boehringer Ingelheim, Eli Lilly | Empagliflozin | Linagliptin | 197 | 686 [413] | 24 | 28 |
| Ferdinand [32] | NCT02182830 | 2019 | Boehringer Ingelheim, Eli Lilly | Empagliflozin | Placebo | 92 | 157 | 24 | n.a. |
| Ferrannini [33] | NCT00528372 | 2010 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 85 | 559 | 24 | n.a. |
| Fioretto [34] | NCT02413398 | 2018 | AstraZeneca, National Institutes of Health | Dapagliflozin | Placebo | 88 | 321 | 24 | n.a. |
| Forst [35] | NCT01106690 | 2014 | Janssen Research & Development, LLC | Canagliflozin | Placebo | 74 | 342 | 26 | n.a.a |
| Frias [36], Jabbour [37] | NCT02229396 | 2016, 2018 | AstraZeneca | Dapagliflozin | Exenatide | 134 | 694 [463] | 28 | 25 |
| Grunberger [38] | NCT01986855 | 2018 | Merck Sharp & Dohme Corp., Pfizer Inc. | Ertugliflozin | Placebo | 121 | 467 | 52 | n.a. |
| Hadjadj [39] | NCT01719003 | 2016 | Boehringer Ingelheim, Eli Lilly | Empagliflozin | Metformin | 190 | 1364 [702] | 24 | n.a. |
| Haring [40] | NCT01159600 | 2013 | Boehringer Ingelheim | Empagliflozin | Placebo | 148 | 669 | 24 | n.a. |
| Haring [41] | NCT01159600 | 2014 | Boehringer Ingelheim | Empagliflozin | Placebo | 148 | 637 | 24 | n.a. |
| Henry [42] | NCT00643851 | 2012 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Metformin | 105 | 598 [404] | 24 | n.a. |
| Henry [42] | NCT00859898 | 2012 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Metformin | 131 | 638 [427] | 24 | n.a. |
| Hollander [43, 44] | NCT01999218 | 2018 | Merck & Co., Inc. | Ertugliflozin | Glimepiride | 232 | 1325 | 52 | 52 |
| Inagaki [45] | NCT01413204 | 2014 | Mitsubishi Tanabe Pharma Corporation | Canagliflozin | Placebo | 5 | 272 | 24 | n.a. |
| Jabbour [46] | NCT00984867 | 2014 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 88 | 451 | 24 | 24 |
| Ji [47] | NCT01095653 | 2014 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 40 | 393 | 24 | n.a. |
| Kadowaki [48] | NCT02354235 | 2017 | Mitsubishi Tanabe Pharma Corporation | Canagliflozin | Placebo | 3 | 138 | 24 | n.a. |
| Kaku [49] | NCT01294423 | 2014 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 27 | 261 | 24 | n.a. |
| Kohan [50] | NCT00663260 | 2014 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 111 | 252 | 24 | 70 |
| Kovacs [51, 52] | NCT01210001 | 2014, 2015 | Boehringer Ingelheim | Empagliflozin | Placebo | 69 | 498 | 24 | 52 |
| Lavalle-Gonzalez [53] | NCT01106677 | 2013 | Janssen Research & Development, LLC | Canagliflozin | Placebo | 169 | 1284 | 26 | n.a. |
| Leiter [54] | NCT01042977 | 2014 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 173 | 965 | 24 | 28 |
| Lewin [55] | NCT01422876 | 2015 | Boehringer Ingelheim, Eli Lilly | Empagliflozin | Linagliptin | 197 | 677 [405] | 52 | n.a. |
| Mathieu [56, 57] | NCT01646320 | 2015, 2016 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 67 | 320 | 24 | 26 |
| Matthaei [58] | NCT01392677 | 2015 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 46 | 218 | 24 | n.a. |
| Müller-Wieland [59] | NCT02471404 | 2018 | AstraZeneca | Dapagliflozin | Glimepiride | 194 | 939 [627] | 52 | n.a. |
| Nauck [60] | NCT00660907 | 2011 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Glipizide | 95 | 814 | 52 | n.a. |
| Neal [4] | NCT01032629, NCT01989754 | 2017 | Janssen Research & Development, LLC | Canagliflozin | Placebo | 667 | 10,142 | 188 | n.a. |
| Perkovic [61] | NCT02065791 | 2019 | Janssen Research & Development, LLC | Canagliflozin | Placebo | 690 | 4397 | 136 | n.a. |
| Phrommintikul [62] | NCT03178591 | 2019 | Thailand Research Fund, National Science and Technology Development Agency NSTDA | Dapagliflozin | Vildagliptin | 1 | 49 | 24 | n.a. |
| Pollock [63] | NCT02547935 | 2019 | AstraZeneca | Dapagliflozin | Placebo | 116 | 448 [296] | 24 | n.a. |
| Pratley [64] | NCT02099110 | 2018 | Merck & Co., Inc., Pfizer Inc. | Ertugliflozin | Sitagliptin | 21 | 1232 [745] | 52 | n.a. |
| Ridderstrale [65, 66] | NCT01167881 | 2014, 2018 | Boehringer Ingelheim, Eli Lilly | Empagliflozin | Glimepiride | 173 | 1545 | 104 | 104 |
| Rodbard [67] | NCT02025907 | 2013 | Janssen Research & Development, LLC | Canagliflozin | Placebo | 47 | 216 | 26 | n.a. |
| Roden [68, 69] | NCT01177813, NCT01289990 | 2013, 2015 | Boehringer Ingelheim, Eli Lilly | Empagliflozin | Sitagliptin, placebo | 124 | 899 | 24 | 52 |
| Rosenstock [70] | NCT00683878 | 2012 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 105 | 420 | 48 | n.a. |
| Rosenstock [71] | NCT01606007 | 2015 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Saxagliptin | 139 | 534 [355] | 24 | n.a. |
| Rosenstock [72] | NCT01011868 | 2015 | Boehringer Ingelheim, Eli Lilly | Empagliflozin | Placebo | 97 | 494 | 78 | n.a. |
| Rosenstock [73] | NCT01809327 | 2016 | Janssen Research & Development, LLC | Canagliflozin | Metformin | 158 | 1186 [712] | 26 | n.a. |
| Rosenstock [74] | NCT02033889 | 2018 | Merck Sharp & Dohme Corp., Pfizer | Ertugliflozin | Placebo | ? | 621 | 26 | n.a.a |
| Schernthaner [75] | NCT01137812 | 2013 | Janssen Research & Development, LLC | Canagliflozin | Sitagliptin | 140 | 755 | 52 | n.a. |
| Scott [76] | NCT02532855 | 2018 | Merck & Co., Inc. | Dapagliflozin | Sitagliptin | 185 | 614 | 24 | n.a. |
| Softeland [77] | NCT01734785 | 2017 | Boehringer Ingelheim, Eli Lilly | Empagliflozin | Placebo | 90 | 332 | 24 | n.a. |
| Stenlof [78] | NCT01081834 | 2013 | Janssen Research & Development, LLC | Canagliflozin | Placebo | 79 | 584 | 26 | n.a.a |
| Strojek [79, 80] | NCT00680745 | 2011, 2014 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 84 | 596 | 24 | 24 |
| Terra [81] | NCT01958671 | 2017 | Pfizer, Inc., Merck & Co., Inc. | Ertugliflozin | Placebo | 67 | 461 | 26 | n.a. a |
| Wilding [82, 83] | NCT00673231 | 2012, 2014 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 126 | 807 | 24 | 80 |
| Wilding [84] | NCT01106625 | 2013 | Janssen Research & Development, LLC | Canagliflozin | Placebo | 85 | 469 | 26 | 26 |
| Wiviott [5] | NCT01730534 | 2019 | AstraZeneca | Dapagliflozin | Placebo | 882 | 17,160 | 218 | n.a. |
| Yale [85] | NCT01064414 | 2013 | Janssen Research & Development, LLC | Canagliflozin | Placebo | 89 | 269 | 26 | n.a. |
| Yang [86] | NCT01095666 | 2016 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 32 | 444 | 24 | n.a. |
| Yang [87] | NCT02096705 | 2018 | AstraZeneca | Dapagliflozin | Placebo | 28 | 272 | 24 | n.a. |
| Zinman [6] | NCT01131676 | 2015 | Boehringer Ingelheim, Eli Lilly | Empagliflozin | Placebo | 590 | 7020 | 164 | n.a. |
| AstraZeneca | NCT00736879 | Bristol-Myers Squibb, AstraZeneca | Dapagliflozin | Placebo | 62 | 282 | 24 | n.a. | |
| AstraZeneca | NCT02681094 | AstraZeneca | Dapagliflozin | Saxagliptin | 119 | 883 [590] | 24 | n.a. | |
| Merck Sharp & Dohme Corp. | NCT02630706 | Merck Sharp & Dohme Corp., Pfizer | Ertugliflozin | Placebo | 50 | 506 | 26 | n.a. | |
aDuring the extension period of the trial, patients on placebo or active control changed their treatment. Therefore, only the core period of the respective trial was considered for analyses. n.a., not available. Numbers in brackets show the number of patients available for endpoint analyses (if different to the total number of patients included in the respective trial)
Patient characteristics
Patients were on average between 52 and 69 years old and baseline HbA1c varied between 7.2% and 9.3%. The majority of patients had preserved renal function. The prevalence of cardiovascular disease was reported in 15 trials and varied between 26.1% and 100%, totalling 26,360 patients. A total of 7534 patients from 14 trials was treatment-naïve, whereas 67,340 patients received background treatment for diabetes with OADs and/or insulin. For details, please see eTable 1.
Risk of bias
The overall risk of bias was low. With respect to the individual items of the risk of bias assessment (eFig. 2), the majority of studies provided adequate random sequence generation with good group balance at baseline. All-cause mortality could be retrieved for all but one trial, whereas cardiovascular mortality was reported in 46 (71.9%) trials (n = 59,168 patients). Data on HF outcomes were available for 42,683 patients included in 12 trials. There was no systematic association between type or size of the trial or the publication date and any pattern of missing endpoint information. The comparison adjusted funnel plot for all-cause mortality (eFig. 3) was symmetrical, suggesting the absence of small-study effects and publication bias.
Outcomes
For all endpoints including the respective outcome numbers per trial arm, please refer to eTable 2.
All-cause mortality
The predictive interval plot summarizing the relative mean effects along with the impact of heterogeneity on the respective confidence interval (= the predictive interval) of each (network) comparison is shown in Fig. 2. Canagliflozin, dapagliflozin and empagliflozin all had a beneficial effect on all-cause mortality compared with placebo. In head-to-head comparisons, the analysis suggests that empagliflozin is superior to both canagliflozin and dapagliflozin. No other head-to-head comparison of any pair of treatments (including non-SGLT2 treatments) found a significant difference between agents, though for most of these comparisons, the 95% CI was wide. SUCRA values are presented in Table 2. The graphical display of the ranking based on the SUCRA values is shown in eFig. 4. The inconsistency within the respective closed loops for each comparison was overall low (eFig. 5) and did not reach statistical significance for any of the loops.
Fig. 2.

Predictive interval plot for all-cause mortality. Legend: The predictive interval plot represents a forest plot of the joint estimated summary effects from both direct and indirect comparisons along with their confidence intervals. Significant results are shown in read colour
Table 2.
Surface under the cumulative ranking curve (SUCRA) values for all endpoints
| SUCRA | All-cause mortality | Cardiovascular mortality | Worsening HF |
|---|---|---|---|
| Canagliflozin | 0.519 | 0.533 | 0.754 |
| Dapagliflozin | 0.437 | 0.414 | 0.537 |
| Empagliflozin | 0.684 | 0.697 | 0.677 |
| Ertugliflozin | 0.385 | 0.659 | n.a. |
| Placebo | 0.335 | 0.374 | 0.285 |
HF, heart failure; n.a., not available. SUCRA is a transformation of the mean rank that accounts both for the location and the variance of all relative treatment effects. SUCRA would be 1 when a treatment is certain to be the best and 0 when a treatment is certain to be the worst [19]
Cardiovascular mortality
The predictive interval plot (Fig. 3) showed that empagliflozin was again superior to placebo, canagliflozin and dapagliflozin in reducing cardiovascular mortality. Canagliflozin also reduced cardiovascular mortality compared with placebo. No other head-to-head comparison of any pair of treatments (including non-SGLT2 treatments) found a significant difference between agents, though again for most of these comparisons, the 95% CI was wide. SUCRA values are presented in Table 2. The graphical display of the ranking based on the SUCRA values is shown in eFig. 6. The inconsistency within the respective closed loops for each comparison was overall low (eFig. 7) and again did not reach statistical significance for any of the loops.
Fig. 3.

Predictive interval plot for cardiovascular mortality. Legend: The predictive interval plot represents a forest plot of the joint estimated summary effects from both direct and indirect comparisons along with their confidence intervals. Significant results are shown in red colour
Worsening HF
The predictive interval plot (Fig. 4) showed that canagliflozin, dapagliflozin and empagliflozin all reduced the endpoint of worsening HF when compared with placebo. There were no further significant differences in HF outcomes between individual SGLT2i. SUCRA values are presented in Table 2. The graphical display of the ranking based on the SUCRA values is shown in eFig. 8. No closed loops were formed and consequently no inconsistency could be derived.
Fig. 4.

Predictive interval plot for worsening HF. Legend: The predictive interval plot represents a forest plot of the joint estimated summary effects from both direct and indirect comparisons along with their confidence intervals. Significant results are shown in red colour
Sensitivity analyses
Sensitivity analyses essentially confirmed our main results. When we included the results of study extension periods to the outcome analyses, empagliflozin was again more effective in reducing all-cause and cardiovascular mortality than all other agents, while there was no difference between the individual SGLT2i in reducing worsening HF (eFig. 9, 10 and 11). Results were similar after excluding trials with a treatment duration < 52 weeks (eFig. 12, 13 and 14) or when restricting our analyses to patients included in cardiovascular outcome trials (n = 38,719; eFig. 15, 16 and 17). As we did not identify any trials with a high risk of bias, the corresponding sensitivity analysis was not appropriate.
Discussion
SGLT2i belong to a new class of OAD that confer benefits on cardiovascular endpoints in patients with T2D. To date, there is no randomised controlled trial (RCT) or retrospective head-to-head comparison of any available SGLT2i. NMA is an increasingly popular tool for comparative effectiveness research. The integration of direct (head-to-head) and indirect (transitively derived via a common comparator) evidence allows for comparisons that otherwise elude conventional (aggregate) analysis while increasing precision in the estimates along the way. The present analysis is thus the first to provide evidence of the comparative cardiovascular effects of different SGLT2i in patients with T2D.
In a comprehensive analysis of almost 75,000 patients derived from 64 trials, we found that while empagliflozin, canagliflozin and dapagliflozin reduce all-cause mortality compared with placebo, empagliflozin appears more effective than the latter two. These results were essentially mirrored for cardiovascular mortality, while all three appear of similar efficacy with respect to worsening HF. Ertugliflozin had no effect on any of the three endpoints investigated.
The mortality advantage of empagliflozin reflects the results of four recently published large-scale placebo-controlled cardiovascular outcome trials, since these trials contribute more than 90% of mortality events to the present analysis. In the EMPA-REG-OUTCOME trial, empagliflozin significantly reduced all-cause and cardiovascular mortality in 7020 patients with T2D at high cardiovascular risk [6]. In contrast, dapagliflozin had a neutral effect on survival in 17,160 patients included in the DECLARE-TIMI 58 trial [5]. Similarly, canagliflozin did not affect overall survival or cardiovascular death both in 10,142 patients enrolled in the CANVAS programme and in 4401 patients enrolled in the CREDENCE trial [4, 61], though in all cases, the 95% CI of the effect measure just touched the null-effect line.
Our findings may reflect features of trial designs or actual differences between the agents. Although molecules of dapagliflozin and canagliflozin are very similar to those of empagliflozin, small differences in the molecular structure can potentially lead to critical differences. For example, the molecular differences between the hormones testosterone and estradiol are substantially smaller than the differences between the empagliflozin molecule and the other two members of the class [88]. However, individual SGLT2i share their mode of action as well as important pharmacological characteristics including bioavailability, receptor selectivity, metabolism, elimination half-life and excretion [89, 90]. In addition, they have comparable effects on blood glucose, body weight and blood pressure, which are the suggested mediators of the anti-atherosclerotic effects of SGLT2i.
The difference in survival benefit between individual SGLT2i may potentially be explained by differences in trial populations. For example, the number of patients with established atherosclerotic cardiovascular disease in EMPA-REG-OUTCOME was significantly higher than in the other trials. The mortality rate in the placebo group of the EMPA-REG-OUTCOME trial was higher than in the other SGLT2i cardiovascular outcome trials, highlighting the differences between populations. An additional factor is that the number of patients with concomitant chronic kidney disease varied between trials. As patients with impaired renal function may gain a greater benefit from SGLT2i therapy, exclusion of these patients from the DECLARE-TIMI 58 trial may have limited mortality benefits [91].
To date, data on the cardiovascular effects of ertugliflozin are scarce. The present NMA includes seven trials totalling 4740 patients treated with ertugliflozin; however, these trials reported only 17 deaths. Due to the low number of events, mortality analyses result in wide confidence intervals and should therefore be interpreted with caution. The cardiovascular efficacy and safety of ertugliflozin in patients with T2D is currently being evaluated in the VERTIS-CV trial. The trial completed enrolment in 2017 and the results are expected to be published in 2020 [92].
The present NMA shows a clear reduction in HF events with canagliflozin, dapagliflozin and empagliflozin, with no significant difference between individual SGLT2i. Again, these results are mainly driven by the four large-scale cardiovascular outcome trials, which reported a relative 30–40% risk reduction for worsening HF for each agent [4–6, 61]. Notably, the benefit was independent of baseline cardiovascular risk or a history of HF [93–95]. The benefits with SGLT2i for HF outcomes may be secondary to a reduction in circulating volume and other haemodynamic effects with a reduction of myocardial loading [93–95]. Natriuresis [96], systemic blood pressure lowering [97], modification of the intrarenal renin angiotensin axis [98] and reduction in arterial stiffness [99] may all contribute to the protection afforded [94]. These effects have been reported for all the different SGLT2i, consistent with the comparable HF efficacy of individual SGLT2i.
In the present NMA, no significant differences in mortality or HF efficacy were found when comparing individual SGLT2i to other active treatments. This contrasts to two recently published meta-analyses in which the use of SGLT2 inhibitors was associated with lower mortality and a lower risk of HF compared with dipeptidyl peptidase 4 inhibitors [100, 101]. The meta-analyses, however, compared classes of drugs, whereas the present NMA presents comparisons of individual agents. As the number of events included in each analysis is low, comparisons of individual SGLT2i with other active treatments need to be interpreted with caution.
Limitations
The present NMA includes all the available evidence regarding the effects of SGLT2i on commonly accepted endpoints in patients with T2D. It deliberately excludes the recently published DAPA-HF trial [102]. This is because all trials (except DAPA-HF) included T2D patients—of whom some had chronic HF—while DAPA-HF included only chronic HF patients—of whom some had T2D. This would substantially skew baseline characteristics between DAPA-HF and all other studies. The ensuing violation of the transitivity assumption would thus invalidate the entire NMA. Several other potential study limitations should be considered.
First, most trials in the present NMA included a relatively small number of patients, with four trials contributing almost half of the study population.
Second, the mean follow-up duration of the core trials was 40 weeks, which limits mortality analyses. However, our results were confirmed in a sensitivity analysis restricted to trials with a treatment duration of at least 52 weeks.
Third, the majority of studies included were not designed as cardiovascular outcome trials. They were therefore not powered to detect differences in survival between active treatments and comparators. However, aggregation of individual trial data in a (network) meta-analysis is an appropriate tool to increase the power and validity of individual study results. In addition, we confirmed the results of our NMA in a sensitivity analysis that excluded non-cardiovascular outcome trials.
Fourth, baseline cardiovascular risk—if reported at all—varied substantially between trials, with a significantly higher number of patients with established atherosclerotic cardiovascular disease included in empagliflozin trials. As patients at high cardiovascular risk may gain a greater benefit from SGLT2i therapy, differences between trial populations may have biased the results. In addition, differences in background anti-diabetic and/or cardiovascular treatment may have affected the number of cardiovascular endpoints.
Fifth, statistically significant results from a (network) meta-analysis do not necessarily imply clinically meaningful differences in efficacy. The findings of the present study should therefore be interpreted cautiously.
Conclusion
We found similar reductions in worsening HF with empagliflozin, canagliflozin and dapagliflozin. However, empagliflozin was associated with a greater reduction in all-cause and cardiovascular mortality. Due to the low number of events reported from ertugliflozin trials, no reliable conclusions on cardiovascular outcomes may be drawn from ertugliflozin analyses. Although the differences in the efficacy of individual SGLT2i might reflect different trial designs, clinicians may prefer empagliflozin over other SGLT2i until more evidence on the comparative efficacy of SGLT2i is available.
Electronic supplementary material
(PDF 2994 kb)
Acknowledgements
Open Access funding provided by Projekt DEAL.
Authors’ contribution
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Tobias Täger, Hanna Fröhlich and Lutz Frankenstein. The first draft of the manuscript was written by Tobias Täger and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Compliance with ethical standards
Conflict of interest
Prof. Agewall and Prof. Atar report personal fees from Boehringer Ingelheim (outside the submitted work). Prof. Cleland reports grants and personal fees from Abbott, Amgen, Bayer, Bristol-Myers Squibb, and Torrent Pharmaceuticals; personal fees from AstraZeneca and Myokardia; grants, personal fees and non-financial support from Medtronic, Novartis, and Vifor; grants and non-financial support from Pharmacosmos and PharmaNord (outside the submitted work). Prof. Katus reports personal fees from AstraZeneca, Boehringer Ingelheim, Roche Diagnostics, Bayer Vital, and Daiichi Sankyo (outside the submitted work).
Footnotes
Hanna Fröhlich and Lutz Frankenstein shared last authorship
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Liu XY, Zhang N, Chen R, Zhao JG, Yu P. Efficacy and safety of sodium-glucose cotransporter 2 inhibitors in type 2 diabetes: a meta-analysis of randomized controlled trials for 1 to 2years. J Diabetes Complicat. 2015;29(8):1295–1303. doi: 10.1016/j.jdiacomp.2015.07.011. [DOI] [PubMed] [Google Scholar]
- 2.Donnan JR, Grandy CA, Chibrikov E, Marra CA, Aubrey-Bassler K, Johnston K, Swab M, Hache J, Curnew D, Nguyen H, Gamble JM. Comparative safety of the sodium glucose co-transporter 2 (SGLT2) inhibitors: a systematic review and meta-analysis. BMJ Open. 2019;9(1):e022577. doi: 10.1136/bmjopen-2018-022577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Furtado RHM, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Sabatine MS. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019;393(10166):31–39. doi: 10.1016/S0140-6736(18)32590-X. [DOI] [PubMed] [Google Scholar]
- 4.Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, Shaw W, Law G, Desai M, Matthews DR. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–657. doi: 10.1056/NEJMoa1611925. [DOI] [PubMed] [Google Scholar]
- 5.Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Silverman MG, Zelniker TA, Kuder JF, Murphy SA, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Ruff CT, Gause-Nilsson IAM, Fredriksson M, Johansson PA, Langkilde AM, Sabatine MS, Investigators D-T. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–357. doi: 10.1056/NEJMoa1812389. [DOI] [PubMed] [Google Scholar]
- 6.Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–2128. doi: 10.1056/NEJMoa1504720. [DOI] [PubMed] [Google Scholar]
- 7.Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med. 2007;356(24):2457–2471. doi: 10.1056/NEJMoa072761. [DOI] [PubMed] [Google Scholar]
- 8.Hutton B, Catala-Lopez F, Moher D. The PRISMA statement extension for systematic reviews incorporating network meta-analysis: PRISMA-NMA. Med Clin (Barc) 2016;147(6):262–266. doi: 10.1016/j.medcli.2016.02.025. [DOI] [PubMed] [Google Scholar]
- 9.Moher D, Stewart L, Shekelle P. Implementing PRISMA-P: recommendations for prospective authors. Syst Rev. 2016;5:15. doi: 10.1186/s13643-016-0191-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA, Group P-P Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;349:g7647. doi: 10.1136/bmj.g7647. [DOI] [PubMed] [Google Scholar]
- 11.Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA, Group P-P Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1. doi: 10.1186/2046-4053-4-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Higgins J, Green S (eds) Cochrane handbook for systematic reviews of interventions version 5.1.0 [updated March 2011]
- 13.Higgins JP, Jackson D, Barrett JK, Lu G, Ades AE, White IR. Consistency and inconsistency in network meta-analysis: concepts and models for multi-arm studies. Res Synth Methods. 2012;3(2):98–110. doi: 10.1002/jrsm.1044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chaimani A, Higgins JP, Mavridis D, Spyridonos P, Salanti G. Graphical tools for network meta-analysis in STATA. PLoS One. 2013;8(10):e76654. doi: 10.1371/journal.pone.0076654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Salanti G. Indirect and mixed-treatment comparison, network, or multiple-treatments meta-analysis: many names, many benefits, many concerns for the next generation evidence synthesis tool. Res Synth Methods. 2012;3(2):80–97. doi: 10.1002/jrsm.1037. [DOI] [PubMed] [Google Scholar]
- 16.Salanti G, Marinho V, Higgins JP. A case study of multiple-treatments meta-analysis demonstrates that covariates should be considered. J Clin Epidemiol. 2009;62(8):857–864. doi: 10.1016/j.jclinepi.2008.10.001. [DOI] [PubMed] [Google Scholar]
- 17.Salanti G, Del Giovane C, Chaimani A, Caldwell DM, Higgins JP. Evaluating the quality of evidence from a network meta-analysis. PLoS One. 2014;9(7):e99682. doi: 10.1371/journal.pone.0099682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Puhan MA, Schunemann HJ, Murad MH, Li T, Brignardello-Petersen R, Singh JA, Kessels AG, Guyatt GH, Group GW A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2014;349:g5630. doi: 10.1136/bmj.g5630. [DOI] [PubMed] [Google Scholar]
- 19.Salanti G, Ades AE, Ioannidis JP. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J Clin Epidemiol. 2011;64(2):163–171. doi: 10.1016/j.jclinepi.2010.03.016. [DOI] [PubMed] [Google Scholar]
- 20.Mbuagbaw L, Rochwerg B, Jaeschke R, Heels-Andsell D, Alhazzani W, Thabane L, Guyatt GH. Approaches to interpreting and choosing the best treatments in network meta-analyses. Syst Rev. 2017;6(1):79. doi: 10.1186/s13643-017-0473-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Song F, Harvey I, Lilford R. Adjusted indirect comparison may be less biased than direct comparison for evaluating new pharmaceutical interventions. J Clin Epidemiol. 2008;61(5):455–463. doi: 10.1016/j.jclinepi.2007.06.006. [DOI] [PubMed] [Google Scholar]
- 22.Bailey CJ, Gross JL, Pieters A, Bastien A, List JF. Effect of dapagliflozin in patients with type 2 diabetes who have inadequate glycaemic control with metformin: a randomised, double-blind, placebo-controlled trial. Lancet. 2010;375(9733):2223–2233. doi: 10.1016/S0140-6736(10)60407-2. [DOI] [PubMed] [Google Scholar]
- 23.Bailey CJ, Iqbal N, T'Joen C, List JF. Dapagliflozin monotherapy in drug-naive patients with diabetes: a randomized-controlled trial of low-dose range. Diabetes Obes Metab. 2012;14(10):951–959. doi: 10.1111/j.1463-1326.2012.01659.x. [DOI] [PubMed] [Google Scholar]
- 24.Barnett AH, Mithal A, Manassie J, Jones R, Rattunde H, Woerle HJ, Broedl UC, investigators E-RRt Efficacy and safety of empagliflozin added to existing antidiabetes treatment in patients with type 2 diabetes and chronic kidney disease: a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2014;2(5):369–384. doi: 10.1016/S2213-8587(13)70208-0. [DOI] [PubMed] [Google Scholar]
- 25.Bode B, Stenlof K, Sullivan D, Fung A, Usiskin K. Efficacy and safety of canagliflozin treatment in older subjects with type 2 diabetes mellitus: a randomized trial. Hosp Pract (1995) 2013;41(2):72–84. doi: 10.3810/hp.2013.04.1020. [DOI] [PubMed] [Google Scholar]
- 26.Bolinder J, Ljunggren O, Kullberg J, Johansson L, Wilding J, Langkilde AM, Sugg J, Parikh S. Effects of dapagliflozin on body weight, total fat mass, and regional adipose tissue distribution in patients with type 2 diabetes mellitus with inadequate glycemic control on metformin. J Clin Endocrinol Metab. 2012;97(3):1020–1031. doi: 10.1210/jc.2011-2260. [DOI] [PubMed] [Google Scholar]
- 27.Bolinder J, Ljunggren O, Johansson L, Wilding J, Langkilde AM, Sjostrom CD, Sugg J, Parikh S. Dapagliflozin maintains glycaemic control while reducing weight and body fat mass over 2 years in patients with type 2 diabetes mellitus inadequately controlled on metformin. Diabetes Obes Metab. 2014;16(2):159–169. doi: 10.1111/dom.12189. [DOI] [PubMed] [Google Scholar]
- 28.Cefalu WT, Leiter LA, Yoon KH, Arias P, Niskanen L, Xie J, Balis DA, Canovatchel W, Meininger G. Efficacy and safety of canagliflozin versus glimepiride in patients with type 2 diabetes inadequately controlled with metformin (CANTATA-SU): 52 week results from a randomised, double-blind, phase 3 non-inferiority trial. Lancet. 2013;382(9896):941–950. doi: 10.1016/S0140-6736(13)60683-2. [DOI] [PubMed] [Google Scholar]
- 29.Cefalu WT, Leiter LA, de Bruin TW, Gause-Nilsson I, Sugg J, Parikh SJ. Dapagliflozin’s effects on glycemia and cardiovascular risk factors in high-risk patients with type 2 diabetes: a 24-week, multicenter, randomized, double-blind, placebo-controlled study with a 28-week extension. Diabetes Care. 2015;38(7):1218–1227. doi: 10.2337/dc14-0315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Dagogo-Jack S, Liu J, Eldor R, Amorin G, Johnson J, Hille D, Liao Y, Huyck S, Golm G, Terra SG, Mancuso JP, Engel SS, Lauring B. Efficacy and safety of the addition of ertugliflozin in patients with type 2 diabetes mellitus inadequately controlled with metformin and sitagliptin: the VERTIS SITA2 placebo-controlled randomized study. Diabetes Obes Metab. 2018;20(3):530–540. doi: 10.1111/dom.13116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.DeFronzo RA, Lewin A, Patel S, Liu D, Kaste R, Woerle HJ, Broedl UC. Combination of empagliflozin and linagliptin as second-line therapy in subjects with type 2 diabetes inadequately controlled on metformin. Diabetes Care. 2015;38(3):384–393. doi: 10.2337/dc14-2364. [DOI] [PubMed] [Google Scholar]
- 32.Ferdinand KC, Izzo JL, Lee J, Meng L, George J, Salsali A, Seman L (2019) Antihyperglycemic and blood pressure effects of empagliflozin in African Americans with type 2 diabetes and hypertension. Circulation. 10.1161/CIRCULATIONAHA.118.036568 [DOI] [PubMed]
- 33.Ferrannini E, Ramos SJ, Salsali A, Tang W, List JF. Dapagliflozin monotherapy in type 2 diabetic patients with inadequate glycemic control by diet and exercise: a randomized, double-blind, placebo-controlled, phase 3 trial. Diabetes Care. 2010;33(10):2217–2224. doi: 10.2337/dc10-0612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Fioretto P, Del Prato S, Buse JB, Goldenberg R, Giorgino F, Reyner D, Langkilde AM, Sjostrom CD, Sartipy P, Investigators DS. Efficacy and safety of dapagliflozin in patients with type 2 diabetes and moderate renal impairment (chronic kidney disease stage 3A): the DERIVE Study. Diabetes Obes Metab. 2018;20(11):2532–2540. doi: 10.1111/dom.13413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Forst T, Guthrie R, Goldenberg R, Yee J, Vijapurkar U, Meininger G, Stein P. Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes on background metformin and pioglitazone. Diabetes Obes Metab. 2014;16(5):467–477. doi: 10.1111/dom.12273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Frias JP, Guja C, Hardy E, Ahmed A, Dong F, Ohman P, Jabbour SA. Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with type 2 diabetes inadequately controlled with metformin monotherapy (DURATION-8): a 28 week, multicentre, double-blind, phase 3, randomised controlled trial. Lancet Diabetes Endocrinol. 2016;4(12):1004–1016. doi: 10.1016/S2213-8587(16)30267-4. [DOI] [PubMed] [Google Scholar]
- 37.Jabbour SA, Frias JP, Hardy E, Ahmed A, Wang H, Ohman P, Guja C. Safety and efficacy of exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with type 2 diabetes inadequately controlled with metformin monotherapy: 52-week results of the DURATION-8 randomized controlled trial. Diabetes Care. 2018;41(10):2136–2146. doi: 10.2337/dc18-0680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Grunberger G, Camp S, Johnson J, Huyck S, Terra SG, Mancuso JP, Jiang ZW, Golm G, Engel SS, Lauring B. Ertugliflozin in patients with stage 3 chronic kidney disease and type 2 diabetes mellitus: the VERTIS RENAL randomized study. Diabetes Ther. 2018;9(1):49–66. doi: 10.1007/s13300-017-0337-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Hadjadj S, Rosenstock J, Meinicke T, Woerle HJ, Broedl UC. Initial combination of empagliflozin and metformin in patients with type 2 diabetes. Diabetes Care. 2016;39(10):1718–1728. doi: 10.2337/dc16-0522. [DOI] [PubMed] [Google Scholar]
- 40.Haring HU, Merker L, Seewaldt-Becker E, Weimer M, Meinicke T, Woerle HJ, Broedl UC, Investigators E-RMT. Empagliflozin as add-on to metformin plus sulfonylurea in patients with type 2 diabetes: a 24-week, randomized, double-blind, placebo-controlled trial. Diabetes Care. 2013;36(11):3396–3404. doi: 10.2337/dc12-2673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Haring HU, Merker L, Seewaldt-Becker E, Weimer M, Meinicke T, Broedl UC, Woerle HJ, Investigators E-RMT. Empagliflozin as add-on to metformin in patients with type 2 diabetes: a 24-week, randomized, double-blind, placebo-controlled trial. Diabetes Care. 2014;37(6):1650–1659. doi: 10.2337/dc13-2105. [DOI] [PubMed] [Google Scholar]
- 42.Henry RR, Murray AV, Marmolejo MH, Hennicken D, Ptaszynska A, List JF. Dapagliflozin, metformin XR, or both: initial pharmacotherapy for type 2 diabetes, a randomised controlled trial. Int J Clin Pract. 2012;66(5):446–456. doi: 10.1111/j.1742-1241.2012.02911.x. [DOI] [PubMed] [Google Scholar]
- 43.Hollander P, Liu J, Hill J, Johnson J, Jiang ZW, Golm G, Huyck S, Terra SG, Mancuso JP, Engel SS, Lauring B. Ertugliflozin compared with glimepiride in patients with type 2 diabetes mellitus inadequately controlled on metformin: the VERTIS SU randomized study. Diabetes Ther. 2018;9(1):193–207. doi: 10.1007/s13300-017-0354-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hollander P, Liu J, Hill J, Johnson J, Jiang ZW, Wang D, Golm G, Huyck S, Terra S, Mancuso JP et al (2018) Safety and efficacy of ertugliflozin compared with glimepiride after 104 weeks in patients with type 2 diabetes inadequately controlled on metformin: VERTIS SU extension. Diabetologia Conference: 54th annual meeting of the European association for the study diabetes, EASD 2018 Germany 61 (Supplement 1):S304-S305. 10.1007/s00125-018-4693-0
- 45.Inagaki N, Kondo K, Yoshinari T, Takahashi N, Susuta Y, Kuki H. Efficacy and safety of canagliflozin monotherapy in Japanese patients with type 2 diabetes inadequately controlled with diet and exercise: a 24-week, randomized, double-blind, placebo-controlled, phase III study. Expert Opin Pharmacother. 2014;15(11):1501–1515. doi: 10.1517/14656566.2014.935764. [DOI] [PubMed] [Google Scholar]
- 46.Jabbour SA, Hardy E, Sugg J, Parikh S, Study G Dapagliflozin is effective as add-on therapy to sitagliptin with or without metformin: a 24-week, multicenter, randomized, double-blind, placebo-controlled study. Diabetes Care. 2014;37(3):740–750. doi: 10.2337/dc13-0467. [DOI] [PubMed] [Google Scholar]
- 47.Ji L, Ma J, Li H, Mansfield TA, T'Joen CL, Iqbal N, Ptaszynska A, List JF. Dapagliflozin as monotherapy in drug-naive Asian patients with type 2 diabetes mellitus: a randomized, blinded, prospective phase III study. Clin Ther. 2014;36(1):84–100.e109. doi: 10.1016/j.clinthera.2013.11.002. [DOI] [PubMed] [Google Scholar]
- 48.Kadowaki T, Inagaki N, Kondo K, Nishimura K, Kaneko G, Maruyama N, Nakanishi N, Iijima H, Watanabe Y, Gouda M. Efficacy and safety of canagliflozin as add-on therapy to teneligliptin in Japanese patients with type 2 diabetes mellitus: results of a 24-week, randomized, double-blind, placebo-controlled trial. Diabetes Obes Metab. 2017;19(6):874–882. doi: 10.1111/dom.12898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Kaku K, Kiyosue A, Inoue S, Ueda N, Tokudome T, Yang J, Langkilde AM. Efficacy and safety of dapagliflozin monotherapy in Japanese patients with type 2 diabetes inadequately controlled by diet and exercise. Diabetes Obes Metab. 2014;16(11):1102–1110. doi: 10.1111/dom.12325. [DOI] [PubMed] [Google Scholar]
- 50.Kohan DE, Fioretto P, Tang W, List JF. Long-term study of patients with type 2 diabetes and moderate renal impairment shows that dapagliflozin reduces weight and blood pressure but does not improve glycemic control. Kidney Int. 2014;85(4):962–971. doi: 10.1038/ki.2013.356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Kovacs CS, Seshiah V, Swallow R, Jones R, Rattunde H, Woerle HJ, Broedl UC, investigators E-RPt Empagliflozin improves glycaemic and weight control as add-on therapy to pioglitazone or pioglitazone plus metformin in patients with type 2 diabetes: a 24-week, randomized, placebo-controlled trial. Diabetes Obes Metab. 2014;16(2):147–158. doi: 10.1111/dom.12188. [DOI] [PubMed] [Google Scholar]
- 52.Kovacs CS, Seshiah V, Merker L, Christiansen AV, Roux F, Salsali A, Kim G, Stella P, Woerle HJ, Broedl UC, investigators E-REP Empagliflozin as add-on therapy to pioglitazone with or without metformin in patients with type 2 diabetes mellitus. Clin Ther. 2015;37(8):1773–1788. doi: 10.1016/j.clinthera.2015.05.511. [DOI] [PubMed] [Google Scholar]
- 53.Lavalle-Gonzalez FJ, Januszewicz A, Davidson J, Tong C, Qiu R, Canovatchel W, Meininger G. Efficacy and safety of canagliflozin compared with placebo and sitagliptin in patients with type 2 diabetes on background metformin monotherapy: a randomised trial. Diabetologia. 2013;56(12):2582–2592. doi: 10.1007/s00125-013-3039-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Leiter LA, Cefalu WT, de Bruin TW, Gause-Nilsson I, Sugg J, Parikh SJ. Dapagliflozin added to usual care in individuals with type 2 diabetes mellitus with preexisting cardiovascular disease: a 24-week, multicenter, randomized, double-blind, placebo-controlled study with a 28-week extension. J Am Geriatr Soc. 2014;62(7):1252–1262. doi: 10.1111/jgs.12881. [DOI] [PubMed] [Google Scholar]
- 55.Lewin A, DeFronzo RA, Patel S, Liu D, Kaste R, Woerle HJ, Broedl UC. Initial combination of empagliflozin and linagliptin in subjects with type 2 diabetes. Diabetes Care. 2015;38(3):394–402. doi: 10.2337/dc14-2365. [DOI] [PubMed] [Google Scholar]
- 56.Mathieu C, Ranetti AE, Li D, Ekholm E, Cook W, Hirshberg B, Chen H, Hansen L, Iqbal N. Randomized, double-blind, phase 3 trial of triple therapy with dapagliflozin add-on to saxagliptin plus metformin in type 2 diabetes. Diabetes Care. 2015;38(11):2009–2017. doi: 10.2337/dc15-0779. [DOI] [PubMed] [Google Scholar]
- 57.Mathieu C, Herrera Marmolejo M, Gonzalez Gonzalez JG, Hansen L, Chen H, Johnsson E, Garcia-Sanchez R, Iqbal N. Efficacy and safety of triple therapy with dapagliflozin add-on to saxagliptin plus metformin over 52 weeks in patients with type 2 diabetes. Diabetes Obes Metab. 2016;18(11):1134–1137. doi: 10.1111/dom.12737. [DOI] [PubMed] [Google Scholar]
- 58.Matthaei S, Bowering K, Rohwedder K, Grohl A, Parikh S, Study G Dapagliflozin improves glycemic control and reduces body weight as add-on therapy to metformin plus sulfonylurea: a 24-week randomized, double-blind clinical trial. Diabetes Care. 2015;38(3):365–372. doi: 10.2337/dc14-0666. [DOI] [PubMed] [Google Scholar]
- 59.Muller-Wieland D, Kellerer M, Cypryk K, Skripova D, Rohwedder K, Johnsson E, Garcia-Sanchez R, Kurlyandskaya R, Sjostrom CD, Jacob S, Seufert J, Dronamraju N, Csomos K. Efficacy and safety of dapagliflozin or dapagliflozin plus saxagliptin versus glimepiride as add-on to metformin in patients with type 2 diabetes. Diabetes Obes Metab. 2018;20(11):2598–2607. doi: 10.1111/dom.13437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Nauck MA, Del Prato S, Meier JJ, Duran-Garcia S, Rohwedder K, Elze M, Parikh SJ. Dapagliflozin versus glipizide as add-on therapy in patients with type 2 diabetes who have inadequate glycemic control with metformin: a randomized, 52-week, double-blind, active-controlled noninferiority trial. Diabetes Care. 2011;34(9):2015–2022. doi: 10.2337/dc11-0606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, Edwards R, Agarwal R, Bakris G, Bull S, Cannon CP, Capuano G, Chu PL, de Zeeuw D, Greene T, Levin A, Pollock C, Wheeler DC, Yavin Y, Zhang H, Zinman B, Meininger G, Brenner BM, Mahaffey KW. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–2306. doi: 10.1056/NEJMoa1811744. [DOI] [PubMed] [Google Scholar]
- 62.Phrommintikul A, Wongcharoen W, Kumfu S, Jaiwongkam T, Gunaparn S, Chattipakorn S, Chattipakorn N. Effects of dapagliflozin vs vildagliptin on cardiometabolic parameters in diabetic patients with coronary artery disease: a randomised study. Br J Clin Pharmacol. 2019;85(6):1337–1347. doi: 10.1111/bcp.13903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Pollock C, Stefansson B, Reyner D, Rossing P, Sjostrom CD, Wheeler DC, Langkilde AM, Heerspink HJL. Albuminuria-lowering effect of dapagliflozin alone and in combination with saxagliptin and effect of dapagliflozin and saxagliptin on glycaemic control in patients with type 2 diabetes and chronic kidney disease (DELIGHT): a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2019;7(6):429–441. doi: 10.1016/S2213-8587(19)30086-5. [DOI] [PubMed] [Google Scholar]
- 64.Pratley RE, Eldor R, Raji A, Golm G, Huyck SB, Qiu Y, Sunga S, Johnson J, Terra SG, Mancuso JP, Engel SS, Lauring B. Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with type 2 diabetes mellitus inadequately controlled with metformin: the VERTIS FACTORIAL randomized trial. Diabetes Obes Metab. 2018;20(5):1111–1120. doi: 10.1111/dom.13194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Ridderstrale M, Andersen KR, Zeller C, Kim G, Woerle HJ, Broedl UC, investigators E-RHHSt Comparison of empagliflozin and glimepiride as add-on to metformin in patients with type 2 diabetes: a 104-week randomised, active-controlled, double-blind, phase 3 trial. Lancet Diabetes Endocrinol. 2014;2(9):691–700. doi: 10.1016/S2213-8587(14)70120-2. [DOI] [PubMed] [Google Scholar]
- 66.Ridderstrale M, Rosenstock J, Andersen KR, Woerle HJ, Salsali A, investigators E-RHHSt Empagliflozin compared with glimepiride in metformin-treated patients with type 2 diabetes: 208-week data from a masked randomized controlled trial. Diabetes Obes Metab. 2018;20(12):2768–2777. doi: 10.1111/dom.13457. [DOI] [PubMed] [Google Scholar]
- 67.Rodbard HW, Seufert J, Aggarwal N, Cao A, Fung A, Pfeifer M, Alba M. Efficacy and safety of titrated canagliflozin in patients with type 2 diabetes mellitus inadequately controlled on metformin and sitagliptin. Diabetes Obes Metab. 2016;18(8):812–819. doi: 10.1111/dom.12684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Roden M, Weng J, Eilbracht J, Delafont B, Kim G, Woerle HJ, Broedl UC, investigators E-RMt Empagliflozin monotherapy with sitagliptin as an active comparator in patients with type 2 diabetes: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Diabetes Endocrinol. 2013;1(3):208–219. doi: 10.1016/S2213-8587(13)70084-6. [DOI] [PubMed] [Google Scholar]
- 69.Roden M, Merker L, Christiansen AV, Roux F, Salsali A, Kim G, Stella P, Woerle HJ, Broedl UC, investigators E-REM Safety, tolerability and effects on cardiometabolic risk factors of empagliflozin monotherapy in drug-naive patients with type 2 diabetes: a double-blind extension of a phase III randomized controlled trial. Cardiovasc Diabetol. 2015;14:154. doi: 10.1186/s12933-015-0314-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Rosenstock J, Vico M, Wei L, Salsali A, List JF. Effects of dapagliflozin, an SGLT2 inhibitor, on HbA(1c), body weight, and hypoglycemia risk in patients with type 2 diabetes inadequately controlled on pioglitazone monotherapy. Diabetes Care. 2012;35(7):1473–1478. doi: 10.2337/dc11-1693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Rosenstock J, Hansen L, Zee P, Li Y, Cook W, Hirshberg B, Iqbal N. Dual add-on therapy in type 2 diabetes poorly controlled with metformin monotherapy: a randomized double-blind trial of saxagliptin plus dapagliflozin addition versus single addition of saxagliptin or dapagliflozin to metformin. Diabetes Care. 2015;38(3):376–383. doi: 10.2337/dc14-1142. [DOI] [PubMed] [Google Scholar]
- 72.Rosenstock J, Jelaska A, Zeller C, Kim G, Broedl UC, Woerle HJ, investigators E-RBt Impact of empagliflozin added on to basal insulin in type 2 diabetes inadequately controlled on basal insulin: a 78-week randomized, double-blind, placebo-controlled trial. Diabetes Obes Metab. 2015;17(10):936–948. doi: 10.1111/dom.12503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Rosenstock J, Chuck L, Gonzalez-Ortiz M, Merton K, Craig J, Capuano G, Qiu R. Initial combination therapy with canagliflozin plus metformin versus each component as monotherapy for drug-naive type 2 diabetes. Diabetes Care. 2016;39(3):353–362. doi: 10.2337/dc15-1736. [DOI] [PubMed] [Google Scholar]
- 74.Rosenstock J, Frias J, Pall D, Charbonnel B, Pascu R, Saur D, Darekar A, Huyck S, Shi H, Lauring B, Terra SG. Effect of ertugliflozin on glucose control, body weight, blood pressure and bone density in type 2 diabetes mellitus inadequately controlled on metformin monotherapy (VERTIS MET) Diabetes Obes Metab. 2018;20(3):520–529. doi: 10.1111/dom.13103. [DOI] [PubMed] [Google Scholar]
- 75.Schernthaner G, Gross JL, Rosenstock J, Guarisco M, Fu M, Yee J, Kawaguchi M, Canovatchel W, Meininger G. Canagliflozin compared with sitagliptin for patients with type 2 diabetes who do not have adequate glycemic control with metformin plus sulfonylurea: a 52-week randomized trial. Diabetes Care. 2013;36(9):2508–2515. doi: 10.2337/dc12-2491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Scott R, Morgan J, Zimmer Z, Lam RLH, O'Neill EA, Kaufman KD, Engel SS, Raji A. A randomized clinical trial of the efficacy and safety of sitagliptin compared with dapagliflozin in patients with type 2 diabetes mellitus and mild renal insufficiency: the CompoSIT-R study. Diabetes Obes Metab. 2018;20(12):2876–2884. doi: 10.1111/dom.13473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Softeland E, Meier JJ, Vangen B, Toorawa R, Maldonado-Lutomirsky M, Broedl UC. Empagliflozin as add-on therapy in patients with type 2 diabetes inadequately controlled with linagliptin and metformin: a 24-week randomized, double-blind, parallel-group trial. Diabetes Care. 2017;40(2):201–209. doi: 10.2337/dc16-1347. [DOI] [PubMed] [Google Scholar]
- 78.Stenlof K, Cefalu WT, Kim KA, Alba M, Usiskin K, Tong C, Canovatchel W, Meininger G. Efficacy and safety of canagliflozin monotherapy in subjects with type 2 diabetes mellitus inadequately controlled with diet and exercise. Diabetes Obes Metab. 2013;15(4):372–382. doi: 10.1111/dom.12054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Strojek K, Yoon KH, Hruba V, Elze M, Langkilde AM, Parikh S. Effect of dapagliflozin in patients with type 2 diabetes who have inadequate glycaemic control with glimepiride: a randomized, 24-week, double-blind, placebo-controlled trial. Diabetes Obes Metab. 2011;13(10):928–938. doi: 10.1111/j.1463-1326.2011.01434.x. [DOI] [PubMed] [Google Scholar]
- 80.Strojek K, Yoon KH, Hruba V, Sugg J, Langkilde AM, Parikh S. Dapagliflozin added to glimepiride in patients with type 2 diabetes mellitus sustains glycemic control and weight loss over 48 weeks: a randomized, double-blind, parallel-group, placebo-controlled trial. Diabetes Ther. 2014;5(1):267–283. doi: 10.1007/s13300-014-0072-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Terra SG, Focht K, Davies M, Frias J, Derosa G, Darekar A, Golm G, Johnson J, Saur D, Lauring B, Dagogo-Jack S. Phase III, efficacy and safety study of ertugliflozin monotherapy in people with type 2 diabetes mellitus inadequately controlled with diet and exercise alone. Diabetes Obes Metab. 2017;19(5):721–728. doi: 10.1111/dom.12888. [DOI] [PubMed] [Google Scholar]
- 82.Wilding JP, Woo V, Soler NG, Pahor A, Sugg J, Rohwedder K, Parikh S, Dapagliflozin 006 Study G Long-term efficacy of dapagliflozin in patients with type 2 diabetes mellitus receiving high doses of insulin: a randomized trial. Ann Intern Med. 2012;156(6):405–415. doi: 10.7326/0003-4819-156-6-201203200-00003. [DOI] [PubMed] [Google Scholar]
- 83.Wilding JP, Woo V, Rohwedder K, Sugg J, Parikh S, Dapagliflozin 006 Study G Dapagliflozin in patients with type 2 diabetes receiving high doses of insulin: efficacy and safety over 2 years. Diabetes Obes Metab. 2014;16(2):124–136. doi: 10.1111/dom.12187. [DOI] [PubMed] [Google Scholar]
- 84.Wilding JP, Charpentier G, Hollander P, Gonzalez-Galvez G, Mathieu C, Vercruysse F, Usiskin K, Law G, Black S, Canovatchel W, Meininger G. Efficacy and safety of canagliflozin in patients with type 2 diabetes mellitus inadequately controlled with metformin and sulphonylurea: a randomised trial. Int J Clin Pract. 2013;67(12):1267–1282. doi: 10.1111/ijcp.12322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Yale JF, Bakris G, Cariou B, Yue D, David-Neto E, Xi L, Figueroa K, Wajs E, Usiskin K, Meininger G. Efficacy and safety of canagliflozin in subjects with type 2 diabetes and chronic kidney disease. Diabetes Obes Metab. 2013;15(5):463–473. doi: 10.1111/dom.12090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Yang W, Han P, Min KW, Wang B, Mansfield T, T'Joen C, Iqbal N, Johnsson E, Ptaszynska A. Efficacy and safety of dapagliflozin in Asian patients with type 2 diabetes after metformin failure: a randomized controlled trial. J Diabetes. 2016;8(6):796–808. doi: 10.1111/1753-0407.12357. [DOI] [PubMed] [Google Scholar]
- 87.Yang W, Ma J, Li Y, Zhou Z, Kim JH, Zhao J, Ptaszynska A (2018) Dapagliflozin as add-on therapy in Asian patients with type 2 diabetes inadequately controlled on insulin with or without oral antihyperglycemic drugs: a randomized controlled trial. J Diabetes(no pagination). 10.1111/1753-0407.12634 [DOI] [PubMed]
- 88.Schernthaner G, Khunti K, Lotan C, Burnier M, Drexel H, Prazny M. Relevance of positive cardiovascular outcome trial results in clinical practice: perspectives from the Academy for Cardiovascular Risk, Outcomes and Safety Studies in Type 2 Diabetes (ACROSS T2D) Ther Clin Risk Manag. 2017;13:1569–1576. doi: 10.2147/tcrm.s144362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Scheen AJ. Pharmacodynamics, efficacy and safety of sodium-glucose co-transporter type 2 (SGLT2) inhibitors for the treatment of type 2 diabetes mellitus. Drugs. 2015;75(1):33–59. doi: 10.1007/s40265-014-0337-y. [DOI] [PubMed] [Google Scholar]
- 90.Scheen AJ. Evaluating SGLT2 inhibitors for type 2 diabetes: pharmacokinetic and toxicological considerations. Expert Opin Drug Metab Toxicol. 2014;10(5):647–663. doi: 10.1517/17425255.2014.873788. [DOI] [PubMed] [Google Scholar]
- 91.Bloomgarden Z. The kidney and cardiovascular outcome trials. J Diabetes. 2018;10(2):88–89. doi: 10.1111/1753-0407.12616. [DOI] [PubMed] [Google Scholar]
- 92.Cannon CP, McGuire DK, Pratley R, Dagogo-Jack S, Mancuso J, Huyck S, Charbonnel B, Shih WJ, Gallo S, Masiukiewicz U, Golm G, Cosentino F, Lauring B, Terra SG. Design and baseline characteristics of the eValuation of ERTugliflozin effIcacy and Safety CardioVascular outcomes trial (VERTIS-CV) Am Heart J. 2018;206:11–23. doi: 10.1016/j.ahj.2018.08.016. [DOI] [PubMed] [Google Scholar]
- 93.Fitchett D, Butler J, van de Borne P, Zinman B, Lachin JM, Wanner C, Woerle HJ, Hantel S, George JT, Johansen OE, Inzucchi SE. Effects of empagliflozin on risk for cardiovascular death and heart failure hospitalization across the spectrum of heart failure risk in the EMPA-REG OUTCOME(R) trial. Eur Heart J. 2018;39(5):363–370. doi: 10.1093/eurheartj/ehx511. [DOI] [PubMed] [Google Scholar]
- 94.Radholm K, Figtree G, Perkovic V, Solomon SD, Mahaffey KW, de Zeeuw D, Fulcher G, Barrett TD, Shaw W, Desai M, Matthews DR, Neal B. Canagliflozin and heart failure in type 2 diabetes mellitus. Circulation. 2018;138(5):458–468. doi: 10.1161/circulationaha.118.034222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Kato ET, Silverman MG, Mosenzon O, Zelniker TA, Cahn A, Furtado RHM, Kuder J, Murphy SA, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Bonaca MP, Ruff CT, Desai AS, Goto S, Johansson PA, Gause-Nilsson I, Johanson P, Langkilde AM, Raz I, Sabatine MS, Wiviott SD. Effect of dapagliflozin on heart failure and mortality in type 2 diabetes mellitus. Circulation. 2019;139(22):2528–2536. doi: 10.1161/circulationaha.119.040130. [DOI] [PubMed] [Google Scholar]
- 96.Fitchett D, Zinman B, Wanner C, Lachin JM, Hantel S, Salsali A, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE, investigators E-ROt Heart failure outcomes with empagliflozin in patients with type 2 diabetes at high cardiovascular risk: results of the EMPA-REG OUTCOME(R) trial. Eur Heart J. 2016;37(19):1526–1534. doi: 10.1093/eurheartj/ehv728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Psaty BM, Lumley T, Furberg CD, Schellenbaum G, Pahor M, Alderman MH, Weiss NS. Health outcomes associated with various antihypertensive therapies used as first-line agents: a network meta-analysis. JAMA. 2003;289(19):2534–2544. doi: 10.1001/jama.289.19.2534. [DOI] [PubMed] [Google Scholar]
- 98.Staels B. Cardiovascular protection by sodium glucose cotransporter 2 inhibitors: potential mechanisms. Am J Med. 2017;130(6S):S30–S39. doi: 10.1016/j.amjmed.2017.04.009. [DOI] [PubMed] [Google Scholar]
- 99.Marti CN, Gheorghiade M, Kalogeropoulos AP, Georgiopoulou VV, Quyyumi AA, Butler J. Endothelial dysfunction, arterial stiffness, and heart failure. J Am Coll Cardiol. 2012;60(16):1455–1469. doi: 10.1016/j.jacc.2011.11.082. [DOI] [PubMed] [Google Scholar]
- 100.Zheng SL, Roddick AJ, Aghar-Jaffar R, Shun-Shin MJ, Francis D, Oliver N, Meeran K. Association between use of sodium-glucose cotransporter 2 inhibitors, glucagon-like peptide 1 agonists, and dipeptidyl peptidase 4 inhibitors with all-cause mortality in patients with type 2 diabetes: a systematic review and meta-analysis. JAMA. 2018;319(15):1580–1591. doi: 10.1001/jama.2018.3024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Yang DY, He X, Liang HW, Zhang SZ, Zhong XB, Luo CF, Du ZM, He JG, Zhuang XD, Liao XX. Comparative outcomes of heart failure among existent classes of anti-diabetic agents: a network meta-analysis of 171,253 participants from 91 randomized controlled trials. Cardiovasc Diabetol. 2019;18(1):47. doi: 10.1186/s12933-019-0853-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.McMurray JJV, Solomon SD, Inzucchi SE, Kober L, Kosiborod MN, Martinez FA, Ponikowski P, Sabatine MS, Anand IS, Belohlavek J, Bohm M, Chiang CE, Chopra VK, de Boer RA, Desai AS, Diez M, Drozdz J, Dukat A, Ge J, Howlett JG, Katova T, Kitakaze M, Ljungman CEA, Merkely B, Nicolau JC, O'Meara E, Petrie MC, Vinh PN, Schou M, Tereshchenko S, Verma S, Held C, DeMets DL, Docherty KF, Jhund PS, Bengtsson O, Sjostrand M, Langkilde AM, Committees D-HT, Investigators (2019) Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 10.1056/NEJMoa1911303
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(PDF 2994 kb)