

Abstract
Background
Since three-dimensional segmentation of cardiac region in 123I-metaiodobenzylguanidine (MIBG) study has not been established, this study aimed to achieve organ segmentation using a convolutional neural network (CNN) with 123I-MIBG single photon emission computed tomography (SPECT) imaging, to calculate heart counts and washout rates (WR) automatically and to compare with conventional quantitation based on planar imaging.
Methods
We assessed 48 patients (aged 68.4 ± 11.7 years) with heart and neurological diseases, including chronic heart failure, dementia with Lewy bodies, and Parkinson's disease. All patients were assessed by early and late 123I-MIBG planar and SPECT imaging. The CNN was initially trained to individually segment the lungs and liver on early and late SPECT images. The segmentation masks were aligned, and then, the CNN was trained to directly segment the heart, and all models were evaluated using fourfold cross-validation. The CNN-based average heart counts and WR were calculated and compared with those determined using planar parameters. The CNN-based SPECT and conventional planar heart counts were corrected by physical time decay, injected dose of 123I-MIBG, and body weight. We also divided WR into normal and abnormal groups from linear regression lines determined by the relationship between planar WR and CNN-based WR and then analyzed agreement between them.
Results
The CNN segmented the cardiac region in patients with normal and reduced uptake. The CNN-based SPECT heart counts significantly correlated with conventional planar heart counts with and without background correction and a planar heart-to-mediastinum ratio (R2 = 0.862, 0.827, and 0.729, p < 0.0001, respectively). The CNN-based and planar WRs also correlated with and without background correction and WR based on heart-to-mediastinum ratios of R2 = 0.584, 0.568 and 0.507, respectively (p < 0.0001). Contingency table findings of high and low WR (cutoffs: 34% and 30% for planar and SPECT studies, respectively) showed 87.2% agreement between CNN-based and planar methods.
Conclusions
The CNN could create segmentation from SPECT images, and average heart counts and WR were reliably calculated three-dimensionally, which might be a novel approach to quantifying SPECT images of innervation.
Supplementary Information
The online version contains supplementary material available at 10.1186/s13550-021-00847-x.
Keywords: Artificial intelligence, Myocardial sympathetic imaging, Innervation, Heart-to-mediastinum ratio, Washout rate
Introduction
Estimating sympathetic nervous activity using 123I-metaiodobenzylguanidine (MIBG) is a valuable adjunct for assessing the severity, prognosis, and effects of treatment for heart failure, arrhythmogenic disease, and neurological diseases such as dementia with Lewy bodies and Parkinson's disease [1–8].
The heart-to-mediastinum ratio (HMR) and washout rate (WR) in planar images are common indicators of sympathetic nervous activity [9]. Some studies have shown good reproducibility using 123I-MIBG planar images [9–11]. However, depending on the method of regions of interest (ROI) definition, up to about 40% of results might located lying in a gray zone around the cut-off, through which normal and abnormal innervation are differentiated in the clinical context [12]. In Japan, the HMR and WR have been calculated from planar images using smartMIBG, a semiautomated ROI setting software developed under collaboration with FUJIFILM Toyama Chemical Co. Ltd., Tokyo, Japan [9], whereas ROI has also been set manually according to American Society of Nuclear Cardiology and European recommendations [13–15].
Single-photon emission computed tomography (SPECT) generates three-dimensional (3D) images that are potentially useful to discriminate organ and background activities that overlap the heart. Degrees of segmental defects can also be scored using the 17-segment model applied in myocardial perfusion imaging (MPI) [1]. However, 3D 123I -MIBG distribution seemed to be heterogeneous based on SPECT studies [16]. Besides, segmental uptake differs among 123I-MIBG SPECT images of individuals. The normal database for 123I-MIBG sympathetic imaging shows relatively decreased activity in the inferior wall, and this was more prominent in late images [17]. To set three-dimensional ROI using the conventional method is difficult in practice.
Here, we present an artificial intelligence (AI) method based on convolution neural networks (CNNs) to define cardiac lesions and calculate heart counts without a manual setting. Deep learning algorithms, in particular CNNs, have become the methodology of choice for analyzing medical images [18]. The deep learning approach has been applied to assess conditions such as cardiovascular diseases and prostate cancer using radiology and nuclear medicine [19, 20]. The CNN can directly identify patterns in 3D SPECT images, which allows the classification of each pixel into anatomical components in the image. However, 3D CNN segmentation and automatic calculation of heart counts for 123I-MIBG SPECT have not been reported because cardiac uptake is quite variable and sometimes significantly reduced in patients with severe heart failure and dementia with Lewy bodies.
The present study aimed to create a segmentation method and to calculate heart counts and WR in 123I-MIBG SPECT images using CNN. We also compared this novel approach with conventional quantitation based on planar images.
Methods
Patients
We assessed 51 consecutive patients with heart and neurological diseases by 123I-MIBG planar and SPECT imaging at Kanazawa University Hospital during 2018 and 2019. We selected data from 48 patients with visible lung and liver uptake to evaluate standard organ segmentation of 123I-MIBG images. One patient had low accumulation in the liver parenchyma due to a giant liver cyst, and two others had low accumulation in the lungs partly due to leakage at antecubital injection sites. Table 1 shows the characteristics of the 48 patients (male, n = 32; female, n = 16; average age, 68.4 ± 11.7; range, 26–84 years; weight, 61.1 ± 13.5; range, 28.8–101 kg; body mass index, 23.0 ± 4.1; range, 16–33). Neurological diseases in 27 patients comprised Parkinson's disease (n = 4), dementia with Lewy bodies (n = 2), familial amyloid polyneuropathy (n = 6), and other neurological diseases including progressive supranuclear palsy and related movement disorders (n = 15). Heart diseases in 21 patients comprised chronic heart failure (n = 13), arrhythmia (n = 5), and cardiomyopathy (n = 3). Cardiac 123I-MIBG uptake was considerably reduced to HMR of < 1.5 in 17 patients. The left ventricular ejection fraction (EF) measured by echocardiography (n = 38) was 56.1% ± 17.3% (24–77%), whereas EF was not available in 10 patients with neurological diseases.
Table 1.
Clinical characteristics of the patients
| Patients (n = 48) | |
| Male | 32 (67) |
| Age (years) | 68.4 ± 11.7 |
| Body weight (kg) | 61.1 ± 13.5 |
| Body mass index (kg/m2) | 23.0 ± 4.1 |
| Neurological diseases | 27 (56) |
| Parkinson's disease | 4 |
| Dementia with Lewy bodies | 2 |
| Familial amyloid polyneuropathy | 6 |
| Other neurological diseases including progressive supranuclear palsy | 15 (44) |
| Heart diseases | 21 |
| Chronic heart failure | 13 |
| Arrhythmia | 5 |
| Cardiomyopathy | 3 |
| Reduced cardiac uptake | 17 (35) |
| Left ventricular ejection fraction | 56.1 ± 17.3 |
Data are shown as n, n (%), means ± standard deviation unless otherwise indicated.
123I-MIBG imaging
Anterior planar and SPECT images were acquired using an Anger camera (Siemens Healthcare, Tokyo, Japan) equipped with a low-medium-energy (LME) collimator from 15–20 (early phase) and 180–240 (late phase) min after the patients received an intravenous injection of 123I-MIBG (111 MBq, FUJIFILM Toyama Chemical Co. Ltd., Tokyo, Japan). The 123I energy was centered at 159 keV with a window of 15% or 20%.
Planar images were acquired for 5 min under conditions of a 256 × 256 matrix, 2.4-mm pixels, and zoom factor 1.0, and SPECT images were acquired for 30 s per view under conditions of a 64 × 64 matrix, 6.6-mm pixels, zoom factor 1.45, 60 projections, 360° circular orbit (radius of rotation 24 cm), and rotation radius 24 cm. The SPECT data were reconstructed using filtered back projection (FBP).
Planar image analysis
Early (E) and late (L) average heart counts in planar images (planar HE and HL, unit counts/pixel) and average mediastinal counts (planar ME and ML, unit counts/pixel) were calculated using semiautomated smartMIBG software to set ROI as described in detail elsewhere [9]. In brief, the software algorithm uses a circular heart ROI and a mediastinal ROI that was 10% of the width of the body and a 30% of the height of the mediastinum. After pointing into the center of the heart, all processing is automated, and manual modifications can be added as required.
Early and late heart counts in planar images were calculated using the following formulae for planar HBC, planar H, and planar HMR.
Planar HBC and planar H were divided by a decay correction factor (DCF) and injected dose (MBq)/ kg body weight (BW). The DCF was calculated as 0.5^ (time [h] between early and late imaging/13). If the interval between early and late was 3 h, the DCF was 0.85. The timing of early imaging was then set at zero (namely DCF = 1).
Washout rates (WR, %) were calculated using the following formulae for planar WRBC, planar WRNC, and planar WRHMR as:
Segmentation based on CNN
We used the following two-step model:
Early and late images were registered using uptake in the liver and lungs that is highly visible in both images.
The heart was directly segmented using both images as input and a single volume as output. All models were trained and evaluated using fourfold cross-validation.
Registration
We trained the CNN to segment the lungs and liver on early and late SPECT images using ADAM [21] and a negative log-likelihood loss with an initial learning rate of 0.001. Images in each cross-validation fold were divided 80%/20% into training and validation sets, respectively, using the CNN architecture described in Fig. 1. The batch size was 150 and the model stopped training when the validation loss remained stable for 10 epochs. The resulting segmentations were converted to binary masks and used to register early and late images with Elastix [22]. The advanced mean square metric was used with the full image sampler and 200 iterations of gradient descent.
Fig. 1.

Architecture of CNN used to segment lungs and liver. Convolution layers do not use padding. Input shape to network is 72 × 72 × 72 pixel cube; output shape is 8 × 8 × 8 pixel cube.
Heart segmentation
To create a target segmentation for a given early and late image pair, manual heart segmentation masks were aligned using the transformation computed above. The result was fractional labeling with heart probabilities between 0 and 1 depending on whether or not the two aligned segmentations agreed. Using this target volume, the CNN was trained taking the two aligned SPECT volumes as input. We used the same training pipeline as described [23], but to avoid excluding uptake from the heart due to under-segmentation, the background loss was set to 0 for all pixels within 1.2 cm (2 pixels) from the heart that did not overlap with lungs or the liver in either of the aligned masks.
CNN-based calculation of average heart counts and WR
We calculated SPECT early and late average heart counts per pixel (Early HCNN and Late HCNN) and SPECT washout rate (WRCNN) using CNN-based heart segmentation. The SPECT HCNN and WRCNN were determined by taking the average counts in the heart VOI from early and late images without background or reference volumes. The SPECT HCNN and WRCNN were calculated as:
Comparison of CNN-based and conventional quantitation
We investigated correlations between SPECT HCNN and planar HBC, planar H, and planar HMR for each early and late image. We also investigated correlations between SPECT WRCNN and planar WRBC, planar WRNC, and planar WRHMR. Cutoff values for planar WR parameters to distinguish normal from abnormal determined from standard values created using JSNM working group databases (n = 62) were: planar WRBC 34.0%, planar WRNC 30.1%, planar WRHMR = 14.2% [24]. The cutoff for SPECT WRCNN was determined from linear regression lines determined by the relationship between planar and SPECT WR. We divided images into normal and abnormal groups, according to the cutoff values for SPECT WRCNN and planar WR parameters, and then analyzed agreement between them.
Statistical analysis
Data are expressed as means and standard deviation (SD). Differences in average heart counts and WR between SPECT and planar images regarding were analyzed using t tests and two-way analysis of variance. Differences among WR were also analyzed by Bland–Altman plot [25]. Relationships between SPECT and planar methods were assessed by linear regression analysis. Agreement between automated and manual segmentations was estimated using the Sørensen–Dice (Dice) index as numbers of overlapping voxels. All data were statistically analyzed using JMP version 14 (SAS Institute Inc., Cary, NC, USA). Values with p ≤ 0.05 were considered statistically significant.
Results
Segmentation on images using CNN
Figure 2 shows examples of CNN-based segmentation. The CNN method correctly identified cardiac regions in patients with normal and reduced uptake. Additionally, the heart, liver, and lungs were appropriately segmented in a natural anatomical form as the original organs. The CNN method did not generate sub-diaphragmatic artifacts, and liver and heart segmentation did not overlap in any patients. However, the CNN did not appropriately segment these organs due to high accumulation in an expanding renal pelvis in one patient, and these data were excluded from further statistical analysis. The automatic segmentation had a Sørensen–Dice (Dice) index for early and late SPECT images of 0.63 ± 0.15, recall of 0.82 ± 0.15, and precision of 0.54 ± 0.19.
Fig. 2.
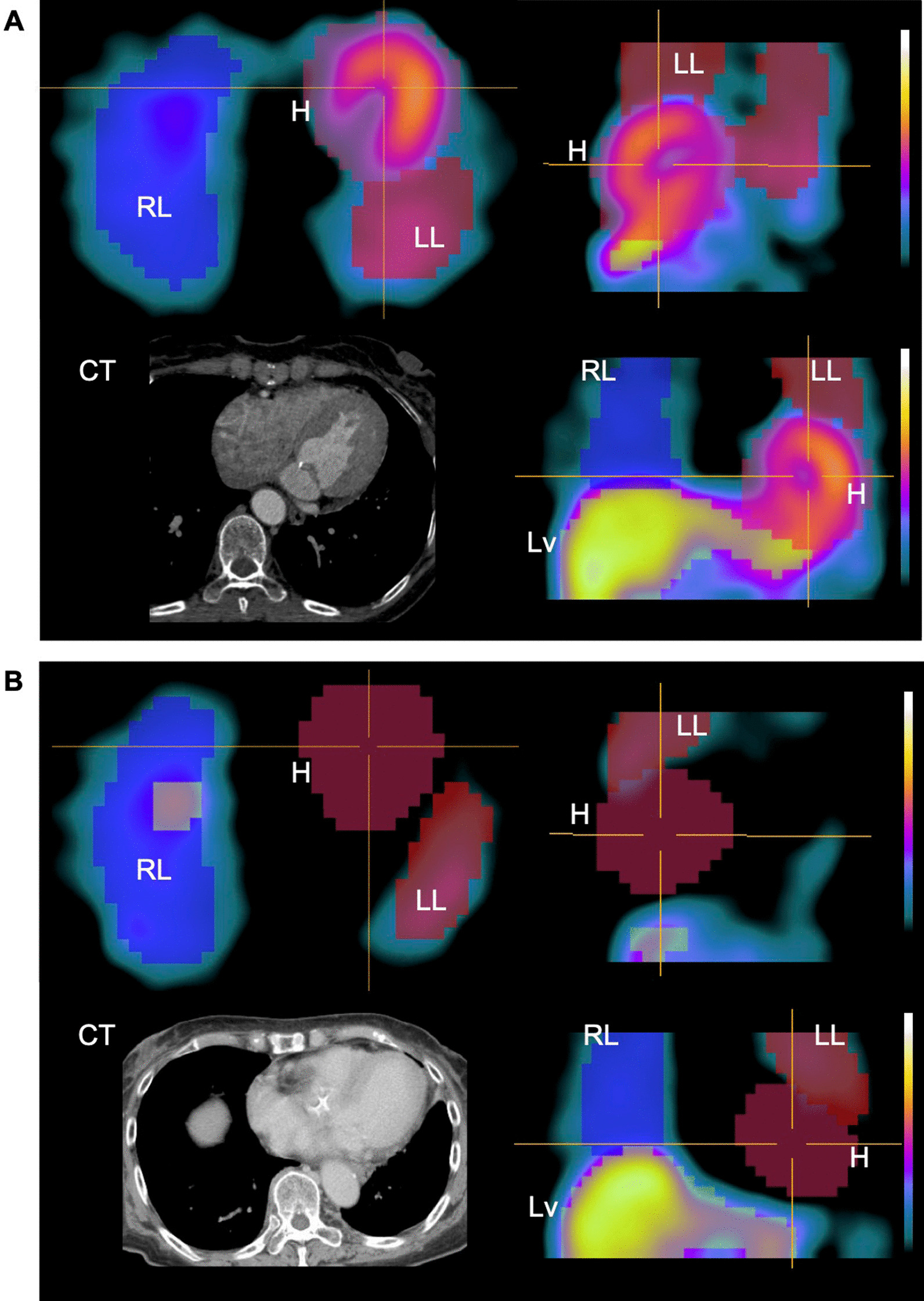
CNN-based segmentation images with 123I-MIBG SPECT data. Patients with normal (A) and reduced (B) uptake. Heart segmentation is correctly identified without anatomical CT images. Liver and lungs are naturally segmented as original organs. Contrast-enhanced X-ray CT images, which were performed for different purposes, are shown as an anatomical reference. H, heart; LL, left lung; Lv, liver; RL, right lung.
SPECT HCNN versus planar HBC, planar H, and planar HMR
The average heart counts were compared between SPECT images using CNN and planar images using the conventional method for early and late imaging. The correlation between SPECT HCNN and planar HBC with background correction was close (SPECT HCNN = 10.3 + 4.25 × planar HBC; R2 = 0.862, p < 0.0001; Fig. 3A). Correlations were also good between SPECT HCNN and planar H without background correction, and between SPECT HCNN and planar HMR (R2 = 0.827 and 0.729, p < 0.0001, respectively; Fig. 3B and C). Correlations were positive between SPECT HCNN and the planar parameters HBC, H, and HMR even in patients with reduced myocardial 123I-MIBG uptake with HMR < 1.5, (R2 = 0.460–0.498, p < 0.0001 for all; Additional file 1: Figure S1).
Fig. 3.

Relationship of average heart counts calculated from SPECT images using CNN and from conventional early and late planar images. SPECT HCNN vs. planar HBC (A), planar H (B), and planar HMR (C). Red circles and blue squares, early and late images, respectively. Shaded area, confidence of fit.
SPECT WRCNN versus planar WRBC, planar WRNC, and planar WRHMR
We compared washout rates in SPECT images determined using CNN and in planar images determined using the conventional method. Correlations were significant between SPECT WRCNN and planar WR parameters (R2 = 0.584, 0.568 and 0.507, p < 0.0001; Fig. 4). The systematic error between SPECT WRCNN and planar WRBC was on the borderline of significance as shown in Bland–Altman plots (p = 0.052). The SPECT WRCNN showed systematically higher values compared with planar WRNC and planar WRHMR (p = 0.006 and p < 0.0001, respectively). The cutoff value of SPECT WRCNN determined by linear regression with the upper limit of the normal range (34%) by the planar WR [24], was 30%. We assigned the patients to groups with normal and abnormal WR based on these cutoff values of SPECT WRCNN and planar WR parameters (Table 2). Although six outliers remained, agreement between SPECT WRCNN and planar WRBC was good at 41 (87.2%) of 47 (Table 2A). The agreement rates between SPECT WRCNN and planar WRNC and planar WRHMR were 78.7% and 72.3%, respectively (Table 2B and C).
Fig. 4.

Relationships between washout rates calculated from SPECT images using CNN and planar images using conventional methods: linear regression lines (upper panels) and Bland–Altman plots (lower panels). SPECT WR vs. planar WRBC (A), planar WRNC (B), and planar WRHMR (C). Shaded area, confidence of fit; dotted lines, 95% confidence intervals
Table 2.
Washout rates determined from SPECT and planar images using CNN-based and standard methods, respectively
| Planar WRBC | Total | ||
|---|---|---|---|
| < 34% | ≥ 34% | ||
| (A) | |||
| SPECT WRCNN | |||
| ≤ 30% | 23 (48.9%) | 1 (2.1%) | 24 (51.1%) |
| > 30% | 5 (10.6%) | 18 (38.3%) | 23 (48.9%) |
| Total | 28 (59.6%) | 19 (40.4%) | 47 |
| Planar WRNC | Total | ||
|---|---|---|---|
| < 30.1% | ≥ 30.1% | ||
| (B) | |||
| SPECT WRCNN | |||
| ≤ 30% | 18 (38.3%) | 1 (2.1%) | 19 (40.4%) |
| > 30% | 9 (19.2%) | 19 (40.4%) | 28 (59.6%) |
| Total | 27 (57.5%) | 20 (42.5%) | 47 |
| Planar WRHMR | Total | ||
|---|---|---|---|
| < 14.2% | ≥ 14.2% | ||
| (C) | |||
| SPECT WRCNN | |||
| ≤ 30% | 18 (38.3%) | 1 (2.1%) | 19 (40.4%) |
| > 30% | 12 (25.5%) | 16 (34.0%) | 28 (59.6%) |
| Total | 30 (63.8%) | 17 (36.2%) | 47 |
Planar WRBC, planar washout rate with background correction; Planar WRHMR, planar washout rate heart-to-mediastinum ratio; Planar WRNC, planar washout rate without background correction; SPECT WRCNN, SPECT washout rate using CNN.
Discussion
While 3D quantitation for sympathetic nerve imaging is potentially useful, the feasibility of artificial intelligence for 123I-MIBG studies has not been verified. Therefore, the present study aimed to achieve segmentation and accurate quantitative values using CNN. The CNN segmented organs in 3D and calculated heart counts even when cardiac accumulation was low. The method presented herein could serve as a good foundation for 3D quantitative assessments.
Advantages of SPECT over planar image acquisition
Although sympathetic nervous activity associated with 123I-MIBG has usually been estimated using planar imaging, the usefulness of HMR for diagnosis and prognosis has been confirmed. However, since HMR is a crude parameter based simply on cardiac and mediastinal regions, the planar method has inherently limited objectivity. Since anatomical structures including the heart are three-dimensional, the data obtained from two-dimensional images cannot perfectly separate these structures. In contrast, the 3D approach is fundamentally more appropriate for evaluating actual myocardial activity because it avoids organ overlap, and the myocardial wall excluding the LV cavity can be identified. We compared the new approach using SPECT images with conventional planar quantitation, but we could not strictly define myocardial walls. Since perfusion studies with 99mTc-labeled tracers and X-ray CT studies were not included in the protocol for this study, the whole heart was segmented by the CNN algorithm. Further development will be required to strictly segment the myocardial wall.
The SPECT approach is also feasible as more institutions now have cadmium-zinc telluride SPECT cameras. Solid-state SPECT is capable of 3D evaluation with high-resolution and sensitivity, image acquisition is rapid, and radiation exposure is low due to a low injected dose, whereas planar images are not readily available. Therefore, the determination of total tracer uptake in organs using 3D images is an essential step and might lead to improved objectivity and diagnostic accuracy.
Comparison with literature
Chen et al. assessed global quantitation of cardiac uptake using 123I-MIBG SPECT [26]. They calculated the SPECT HMR using a ratio of mean counts between cardiac and mediastinal volumes of interest (VOI), determined on transaxial images, and then compared them with the planar HMR. However, defining heart VOI using the SPECT quantitation tool includes some manual procedures. The shape of the heart VOI is an oval that does not precisely reflect the contour of the heart under examination. Here, we did not use a predefined heart model but automatically segmented the location of the heart and measured counts using the CNN. Since the CNN was trained on manual organ segmentation, the heart VOI was determined in a naturally shaped heart. Although the shape of heart cannot be traced in patients with extremely low cardiac activity, the CNN-segmented heart was placed on the approximate location of the cardiac region, and the average counts would not have significantly differed from those determined using a manually traced heart region.
Heart segmentation and quantitation
The most crucial issue with heart segmentation using only SPECT images is the prevalence of low cardiac uptake in early images. We used a two-step approach to overcome this. Registration and final segmentation can be achieved using different methods, but we believe the two-step approach makes the model more robust and ensures consistent heart volumes for the two images.
The accumulation of 123I-MIBG is usually high in scintigraphy of the liver and heart, and moderate in the lungs. Since the distribution profile of 123I-MIBG is similar regardless of camera types, the CNN constructed herein will probably be applicable to other vendors, but further study will be required for confirmation.
Automated segmentation failed for one of our patients due to high tracer retention in an expanding renal pelvis. Unusually high or low accumulation in other locations, for example, the renal pelvis, large liver defects, extraordinary anatomical structures, can result in segmentation error. Although we already confirmed useful segmentation methods in most situations, adjustments might be required to minimize the frequency of errors. Training models on patients with atypical distribution might also improve performance. That is, the results will become more stable when the CNN is trained more on the anatomical locations of organs, as well as variations including regions of high accumulation outside the liver and heart.
The correlation of heart counts between CNN-based SPECT and conventional planar images was good (r2 = 0.73–0.86), whereas the correlation between CNN-based WR and planar WR parameters was lower than the CNN-based SPECT and planar heart counts (r2 = 0.51–0.58). Since WR is calculated as the subtraction and ratio of small values in reduced myocardial 123I-MIBG uptake, fluctuations in quantitation might have occurred at the higher range of WR. This variation resulted in the lower correlations between the CNN-based WR and planar WR parameters compared with normal 123I-MIBG uptake. However, the patients were separated well into normal and abnormal groups according to cutoff values for CNN-based WR and planar WR parameters.
Future directions for 123I-MIBG imaging
Since the data obtained from this study are relative quantitation, an absolute quantitation method using CNN should be established. For example, the standardized uptake value (SUV) can be calculated if data can be acquired with SPECT-CT and appropriate reconstruction method. To obtain better segmentation, additional anatomical information incorporating X-ray computed tomography with SPECT might be useful. Thereafter, a new three-dimensional index for globally measuring the total amount of 123I-MIBG might be developed. Such a novel quantitative approach will improve the uncertainty of the conventional method regarding two-dimensional quantitation and could be the next step towards absolute quantitation using the CNN. Including data from different cameras and reconstruction methods in CNN training would also improve the accuracy of segmentation.
Limitations
This study had some limitations. Since we included a relatively small patient cohort, further investigations of larger patient cohorts are needed to develop more accurate segmentation. This study included patients with cardiac and neurological diseases, and some of them have yet to be finally diagnosed and/or their prognoses have yet to be confirmed. Clinical 123I-MIBG innervation studies in Japan have included both neurological and cardiac diseases. The present study aimed to create a methodology for 3D heart segmentation and the quantitation of both types of diseases. Therefore, consecutive patients with various backgrounds were selected to ensure that the CNN methods are broadly applicable, although disease-specific analyses, final diagnoses, and prognoses could not be included. To create the CNN architecture, three patients with indistinguishable lungs and liver were not included because the method relies on visualizing the contours of organs. Poor segmentation in one patient was due to excessive accumulation at another location. Such circumstances might be addressed by fusing SPECT-CT imaging with novel CNN-based segmentation. However, since X-ray CT has not been routinely applied for sympathetic nerve imaging at our institution, modifications of the study protocol will be required for further investigation.
Conclusions
The CNN can be trained to determine organ contours and to automatically calculate heart counts and washout rates in 123I-MIBG SPECT images. Average SPECT heart counts calculated by CNN significantly correlated with those determined by conventional quantitation of planar images in patients with cardiac and neurological diseases. Washout rates also significantly correlated between SPECT with CNN segmentation and planar parameters. Automatic quantitation with CNN might have excellent potential and provide a foundation for the development of an absolute quantitative method.
Supplementary Information
Additional file 1. Relationship of heart counts in patients with reduced uptake between CNN and conventional methods.
Acknowledgements
We appreciate Hiroto Yoneyama and Takahiro Konishi, Department of Radiological Technology, and Takayuki Shibutani, Department of Quantum Medical Technology, for technical assistance. The authors thank Norma Foster for editorial assistance.
Abbreviations
- CNN
Convolutional neural network
- HBC
Average heart counts with background correction
- HCNN
Average heart counts using CNN-based segmentation
- HMR
Heart-to-mediastinum ratio
- MIBG
Metaiodobenzylguanidine
- SPECT
Single-photon emission computed tomography
- WR
Washout rates
- WRBC
Washout rates with background correction
- WRCNN
Washout rates using CNN-based segmentation
- WRNC
Washout rates without background correction
Authors' contributions
SS and KN designed and summarized the study. LE, OE, and JU created the CNN architecture for automatic heart segmentation. SS statistically analyzed the data, and KN confirmed the statistical outcomes. SS drafted, and KN, LE, OE, and JU revised the manuscript. SK supervised the study. All authors read and approved the final manuscript.
Funding
This study was partly funded by JSPS Grants-in-Aid for Scientific Research (C) in Japan (PI: K. Nakajima, No. 20K07990), the Fund for Basic Research 2020–2021 from Kanazawa University Hospital, Kanazawa, Japan, and Takeda Japan Medical Office Funded Research Grant 2020.
Availability of data and materials
The image datasets generated and/or analyzed during the current study are not publicly distributed, which is not approved by the Ethics Committees at Kanazawa University, but can be available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
The Ethics Committees at Kanazawa University approved the present study. The need for written informed consent from each patient was waived because of the retrospective design.
Consent for publication
Informed consent including publication was obtained from all patients in the form of opt-out.
Competing interests
KN is in a research collaboration with FUJIFILM Toyama Chemical Co. Ltd., Tokyo, Japan, which supplied the 123I-MIBG in Japan. No other authors have any competing interests to declare.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Shintaro Saito, Email: shintaro1515@stu.kanazawa-u.ac.jp.
Kenichi Nakajima, Email: nakajima@med.kanazawa-u.ac.jp.
References
- 1.Nakajima K, Nakata T, Doi T, Kadokami T, Matsuo S, Konno T, et al. Validation of 2-year 123I-meta-iodobenzylguanidine-based cardiac mortality risk model in chronic heart failure. Eur Heart J Cardiovasc Imaging. 2018;19:749–56. [DOI] [PMC free article] [PubMed]
- 2.Nakata T, Nakajima K, Yamashina S, Yamada T, Momose M, Kasama S, et al. A pooled analysis of multicenter cohort studies of 123I-mIBG imaging of sympathetic innervation for assessment of long-term prognosis in heart failure. JACC Cardiovasc Imaging. 2013;6:772–784. doi: 10.1016/j.jcmg.2013.02.007. [DOI] [PubMed] [Google Scholar]
- 3.Travin MI, Henzlova MJ, van Eck-Smit BLF, Jain D, Carrio I, Folks RD, et al. Assessment of 123I-mIBG and 99mTc-tetrofosmin single-photon emission computed tomographic images for the prediction of arrhythmic events in patients with ischemic heart failure: Intermediate severity innervation defects are associated with higher arrhythmic risk. J Nucl Cardiol. 2017;24:377–391. doi: 10.1007/s12350-015-0336-8. [DOI] [PubMed] [Google Scholar]
- 4.Nakajima K, Nakata T, Yamada T, Yamashina S, Momose M, Kasama S, et al. A prediction model for 5-year cardiac mortality in patients with chronic heart failure using 123I-metaiodobenzylguanidine imaging. Eur J Nucl Med Mol Imaging. 2014;41:1673–1682. doi: 10.1007/s00259-014-2759-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Orimo S, Suzuki M, Inaba A, Mizusawa H. 123I-MIBG myocardial scintigraphy for differentiating Parkinson's disease from other neurodegenerative parkinsonism: a systematic review and meta-analysis. Parkinsonism Relat Disord. 2012;18:494–500. doi: 10.1016/j.parkreldis.2012.01.009. [DOI] [PubMed] [Google Scholar]
- 6.Nakajima K, Nakata T, Doi T, Tada H, Maruyama K. Machine learning-based risk model using 123I-metaiodobenzylguanidine to differentially predict modes of cardiac death in heart failure. J Nucl Cardiol. 2020 doi: 10.1007/s12350-020-02173-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.McKeith IG, Boeve BF, Dickson DW, Halliday G, Taylor JP, Weintraub D, et al. Diagnosis and management of dementia with Lewy bodies: fourth consensus report of the DLB Consortium. Neurology. 2017;89:88–100. doi: 10.1212/WNL.0000000000004058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yamada M, Komatsu J, Nakamura K, Sakai K, Samuraki-Yokohama M, Nakajima K, et al. Diagnostic criteria for dementia with lewy bodies: updates and future directions. J Mov Disord. 2020;13:1–10. doi: 10.14802/jmd.19052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Okuda K, Nakajima K, Hosoya T, Ishikawa T, Konishi T, Matsubara K, et al. Semi-automated algorithm for calculating heart-to-mediastinum ratio in cardiac Iodine-123 MIBG imaging. J Nucl Cardiol. 2011;18:82–89. doi: 10.1007/s12350-010-9313-4. [DOI] [PubMed] [Google Scholar]
- 10.Owenius R, Zanette M, Cella P. Variability in heart-to-mediastinum ratio from planar 123I-MIBG images of a thorax phantom for 6 common gamma-camera models. J Nucl Med Technol. 2017;45:297–303. doi: 10.2967/jnmt.117.196055. [DOI] [PubMed] [Google Scholar]
- 11.Bateman TM, Ananthasubramaniam K, Berman DS, Gerson M, Gropler R, Henzlova M, et al. Reliability of the 123I-mIBG heart/mediastinum ratio: results of a multicenter test-retest reproducibility study. J Nucl Cardiol. 2019;26:1555–1565. doi: 10.1007/s12350-017-1183-6. [DOI] [PubMed] [Google Scholar]
- 12.Klene C, Jungen C, Okuda K, Kobayashi Y, Helberg A, Mester J, et al. Influence of ROI definition on the heart-to-mediastinum ratio in planar 123I-MIBG imaging. J Nucl Cardiol. 2018;25:208–216. doi: 10.1007/s12350-016-0708-8. [DOI] [PubMed] [Google Scholar]
- 13.Flotats A, Carrio I, Agostini D, Le Guludec D, Marcassa C, Schafers M, et al. Proposal for standardization of 123I-metaiodobenzylguanidine (MIBG) cardiac sympathetic imaging by the EANM Cardiovascular Committee and the European Council of Nuclear Cardiology. Eur J Nucl Med Mol Imaging. 2010;37:1802–1812. doi: 10.1007/s00259-010-1491-4. [DOI] [PubMed] [Google Scholar]
- 14.Soman P, Travin MI, Gerson M, Cullom SJ, Thompson R. I-123 MIBG cardiac imaging. J Nucl Cardiol. 2015;22:677–685. doi: 10.1007/s12350-015-0108-5. [DOI] [PubMed] [Google Scholar]
- 15.Tilkemeier PL, Bourque J, Doukky R, Sanghani R, Weinberg RL. ASNC imaging guidelines for nuclear cardiology procedures: standardized reporting of nuclear cardiology procedures. J Nucl Cardiol. 2017;24:2064–2128. doi: 10.1007/s12350-017-1057-y. [DOI] [PubMed] [Google Scholar]
- 16.Momose M, Tyndale-Hines L, Bengel FM, Schwaiger M. How heterogeneous is the cardiac autonomic innervation? Basic Res Cardiol. 2001;96:539–546. doi: 10.1007/s003950170004. [DOI] [PubMed] [Google Scholar]
- 17.Nakajima K. Normal values for nuclear cardiology: Japanese databases for myocardial perfusion, fatty acid and sympathetic imaging and left ventricular function. Ann Nucl Med. 2010;24:125–135. doi: 10.1007/s12149-009-0337-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Litjens G, Kooi T, Bejnordi BE, Setio AAA, Ciompi F, Ghafoorian M, et al. A survey on deep learning in medical image analysis. Med Image Anal. 2017;42:60–88. doi: 10.1016/j.media.2017.07.005. [DOI] [PubMed] [Google Scholar]
- 19.Al'Aref SJ, Anchouche K, Singh G, Slomka PJ, Kolli KK, Kumar A, et al. Clinical applications of machine learning in cardiovascular disease and its relevance to cardiac imaging. Eur Heart J. 2019;40:1975–1986. doi: 10.1093/eurheartj/ehy404. [DOI] [PubMed] [Google Scholar]
- 20.Polymeri E, Sadik M, Kaboteh R, Borrelli P, Enqvist O, Ulen J, et al. Deep learning-based quantification of PET/CT prostate gland uptake: association with overall survival. Clin Physiol Funct Imaging. 2020;40:106–113. doi: 10.1111/cpf.12611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kingma DP, Ba J. Adam: a method for stochastic optimization. The 3rd international conference for learning representations. 2015. https://arxiv.org/abs/1412.6980.
- 22.Klein S, Staring M, Murphy K, Viergever MA, Pluim JP. elastix: a toolbox for intensity-based medical image registration. IEEE Trans Med Imaging. 2010;29:196–205. doi: 10.1109/TMI.2009.2035616. [DOI] [PubMed] [Google Scholar]
- 23.Tragardh E, Borrelli P, Kaboteh R, Gillberg T, Ulen J, Enqvist O, et al. RECOMIA-a cloud-based platform for artificial intelligence research in nuclear medicine and radiology. EJNMMI Phys. 2020;7:51. doi: 10.1186/s40658-020-00316-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nakajima K, Okuda K, Matsuo S, Wakabayashi H, Kinuya S. Is 123I-metaiodobenzylguanidine heart-to-mediastinum ratio dependent on age? From Japanese Society of Nuclear Medicine normal database. Ann Nucl Med. 2018;32:175–181. doi: 10.1007/s12149-018-1231-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–310. doi: 10.1016/S0140-6736(86)90837-8. [DOI] [PubMed] [Google Scholar]
- 26.Chen J, Folks RD, Verdes L, Manatunga DN, Jacobson AF, Garcia EV. Quantitative I-123 mIBG SPECT in differentiating abnormal and normal mIBG myocardial uptake. J Nucl Cardiol. 2012;19:92–99. doi: 10.1007/s12350-011-9438-0. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1. Relationship of heart counts in patients with reduced uptake between CNN and conventional methods.
Data Availability Statement
The image datasets generated and/or analyzed during the current study are not publicly distributed, which is not approved by the Ethics Committees at Kanazawa University, but can be available from the corresponding author on reasonable request.