

Abstract
It has been suggested that self-efficacy specific to parenting or feeding may influence the decisions parents make regarding infant feeding; however, a review of this topic has not been conducted. The purpose of this integrative review is to synthesize the literature regarding the potential role of self-efficacy in infant feeding practices or infant weight gain. A total of 40 articles were used to guide this review, which were classified into three categories examining an association with self-efficacy (1) breastfeeding; (2) infant feeding practices such as parental feeding style and dietary quality; and (3) infant weight gain. Evidence regarding breastfeeding self-efficacy (BFSE) and breastfeeding is extensive; mothers with a higher sense of BFSE more often initiate breastfeeding and breastfeed for longer durations. The evidence regarding self-efficacy and the association with infant feeding practices other than breastfeeding is sparse. However, several studies report that mothers who have a higher sense of self-efficacy are more likely to follow infant feeding practices which align with recommendations. The authors have speculated an association between self-efficacy and infant weight gain; yet, to date, no study has found a significant association. More research is needed on the topic, particularly in diverse populations and with fathers and mothers.
Keywords: Breastfeeding, infant feeding practices, infant weight pain, parental self-efficacy, self-efficacy
Childhood obesity has become epidemic in many developed countries throughout the world (World Health Organization (WHO), 2017). In the United States, approximately 35% of children aged 2–19 years are either overweight or obese (Skinner et al., 2018). Accumulating evidence suggests that factors contributing to childhood obesity begin at the onset of life, if not before, and that modification of risk factors during the prenatal and infancy periods is important to establish healthy dietary practices and prevent obesity (American Academy of Pediatrics (AAP) Committee on Nutrition, 2014; Birch and Doub, 2014; Thompson and Bentley, 2013). One such risk factor is the total amount of weight gained and/or the rate at which the infant gains weight over the first year of life. Infants who exhibit excessive weight gain in comparison to length, or gain weight at a rapid rate, are at risk for childhood obesity (Druet et al., 2012; Ong and Loos, 2006).
Infant weight gain is largely determined by the amount and composition of energy consumed. Given that parents are the primary determinants of infant nutrition, the amount of energy consumed is at least partially attributable to the feeding practices parents choose to employ with their infant. Understanding how parental decisions are made regarding feeding their infant is important to establish healthy dietary practices and growth. It has been suggested that a parent’s sense of self-efficacy may contribute to these decisions (Redsell et al., 2016). For this reason, the influence of self-efficacy on infant feeding practices and/or infant weight gain is worthy of investigation.
Background
Self-efficacy, first conceptualized by Albert Bandura in the 1970s, is defined as ‘beliefs in one’s capabilities to organize and execute the courses of actions required to produce given attainments’ (Bandura, 1997: 3). In other words, self-efficacy is an individual’s belief in his or her ability to accomplish a certain task. Those who believe they have this ability will work hard until task completion. These individuals are considered to have a high sense of self-efficacy. Individuals with a low sense of self-efficacy often give up prematurely because they doubt their ability to successfully complete the task. Factors that contribute to self-efficacy include an individual’s prior experiences (successes and failures); similar experiences of others close to the individual (also known as vicarious experiences); social support; and psychological state (i.e. anxiety, depression, self-esteem) (Bandura, 1997).
Self-efficacy can be applied to roles or tasks. For example, parental self-efficacy (PSE) refers to the belief or confidence parents hold in their ability to accomplish the tasks of parenting (Table 1) (De Montigny and Lacharité, 2005). PSE is associated with parental decision-making during infancy and has been shown to affect parents’ emotions, motivation, cognition, and responses to infant behaviors (Salonen et al., 2009). Additionally, PSE may play a role in infant feeding practices parents choose such as breastfeeding and/or types of foods offered.
Table 1.
Definitions of parental self-efficacy.
| Author/Year | Definition |
|---|---|
| Coleman and Karraker (1997: 58) | ‘one’s perceived ability to exercise positive influence on the behavior and development of one’s children’. |
| De Montigny and Lacharité (2005:390) | ‘Beliefs or judgements a parent holds of their capabilities to organize and execute a set of tasks related to parenting a child’ |
| Grossklaus and Marvicsin (2014: 72) | ‘Self-efficacy is the central cognitive core to parenting competence in which parents look within themselves to decide whether they can influence their child’s well-being’. |
| Teti and Gelfand (1991) | Parent’s expectations about the degree to which he or she is able to perform competently and effectively as a parent |
Infant feeding practices contribute to the amount of weight gained during infancy as well as an individual’s dietary preferences and control mechanisms regarding hunger and satiety (Birch and Doub, 2014; Thompson and Bentley, 2013). Infant feeding practices include the types and quantity of foods offered, the time and setting in which the foods are offered, and the style parents use during feeding (AAP Committee on Nutrition, 2014; Birch and Doub, 2014). Recommendations for feeding infants are provided by organizations such as the American Academy of Pediatrics (AAP) and the WHO. Exclusive breastfeeding is recommended until infants are six months of age, with formula being the alternative if breastfeeding is not possible. Complementary foods (any liquid or food other than breast milk or formula) should be introduced around six months of age. Foods that provide nutrients lacking in breast milk (primarily iron and zinc) should be offered first, followed by other foods with nutritional value yet no added salt or sugar. Food from all groups should be provided by the time an infant is about eight to nine months of age. Juice and sugar-sweetened beverages should be avoided as well as foods that are calorically dense yet lack nutritional value (i.e. desserts) (AAP Committee on Nutrition, 2014; WHO, 2016).
Parental feeding style is included in infant feeding recommendations from all organizations. Parental feeding style is the attitudes and quality of interaction used by parents when feeding (Thompson et al., 2013). A responsive feeding style, in which a parent responds to infant cues regarding hunger and satiety during feeding, is recommended (AAP Committee on Nutrition, 2014; WHO, 2016). Four additional feeding styles are thought to exist (Table 2). Along with the responsive style, Thompson and colleagues (2013) identified the restrictive feeding style to be associated with feeding practices that align with recommendations and healthy growth. In contrast, pressuring/controlling and the indulgent parental feeding styles were associated with feeding practices such as decreased breastfeeding and increased odds of inappropriate feeding (i.e. calorically dense, low nutrient foods) which do not align with recommendations (Thompson et al., 2013).
Table 2.
Parental feeding styles.
| Style | Definition |
|---|---|
| Indulgent | The parent sets no limits on the quantity or quality of the food consumed by the child. |
| Laissez-faire | The parent does not place limits on the quality or quantity of the child’s diet and there is little interaction between parent and child during feeding. |
| Pressuring/controlling | The parent is concerned regarding increases in the amount of food that is taken by the child, demonstrating practices such as adding cereal to a bottle to help with sleep and using food to soothe. |
| Responsive | The parent provides structure yet is attentive to the hunger and satiety cues the child exhibits, the quality of the food is also monitored. |
| Restrictive | The parent is concerned regarding decreasing the amount of food that is taken by the child, and food may be limited to healthful options and quantities. |
Source: From Thompson et al. (2013).
Parental knowledge of infant development, nutrition, and infant feeding recommendations, along with social constraints and other competing time demands, can affect parents’ decisions about what and how to feed their infant (Birch and Doub, 2014; Thompson and Bentley, 2013). Additionally, sociodemographic factors including cultural practices have been identified as contributors to the decisions parents make regarding feeding their infant (Gibbs and Forste, 2014; Taveras et al., 2010). Self-efficacy has also been identified as an important concept in the study of infant feeding practices (Redsell et al., 2016). However, to date, there has been no comprehensive review of research regarding the associations among self-efficacy, infant feeding practices, and infant weight gain. A comprehensive review will identify what is known regarding self-efficacy and infant feeding practices and/or infant weight gain. This knowledge will assist with strategies to implement into clinical practice. Additionally, gaps identified in the review will guide future research. Therefore, the purpose of this integrative review is to synthesize the literature regarding the potential role of self-efficacy in infant feeding practices or infant weight gain.
Methods
Design and search strategy
This integrative review followed the guidelines provided by Whittemore and colleagues (2014). A search was conducted using PubMed, Embase, Cochrane, PsychINFO, and the Cumulative Index to Nursing and Allied Health Library (CINAHL) databases. All searches were conducted using Boolean logic. Search terms included ‘parental self-efficacy’, ‘maternal self-efficacy’, ‘self-efficacy’, ‘breastfeeding self-efficacy’, ‘infant feeding practices’, ‘infant feeding’, ‘feeding practices’, ‘breastfeeding’, ‘formula feeding’, ‘artificial milk’, ‘artificial feeding’, ‘infant weight gain’, ‘infant weight’, ‘weight gain’, and ‘nutrition’. The term ‘nutrition’ was only used when searches using ‘infant feeding practices’ yielded minimal results. With each search, limits were set to examine studies conducted with humans and written in the English language. Limits were also set to only include studies which examined the infancy period (birth to 12 months); in some databases, this included ages up to 23 months. Due to the abundance of literature regarding breastfeeding self-efficacy (BFSE), searches including this term were limited to 2006 to present and excluded dissertations. In the Cochrane database, the search was limited to include only ‘Cochrane Reviews’ and ‘other reviews’. For the remainder of searches, no limit was set on the history of publication date nor the type of article (i.e. review, clinical trial, observational, dissertation). Research examining the association between variables as well as any intervention studies was included. Articles identified were published prior to December 2017.
Data extraction and synthesis
After duplicates were removed, and titles and abstracts screened for relevance to self-efficacy and infant feeding practices or infant weight gain, 120 articles remained. Studies focused on infancy and those that followed infants into the second year, as relevant, were included. Articles were excluded if the focus was on children beyond the age of 24 months with no inclusion of the infancy period, infants born prematurely, development or validation of tools, an aspect of parenting other than self-efficacy, or maternal mental health (Figure 1). Following the method of data analysis suggested by Whittemore and colleagues (2014), categories were identified and articles sorted based on these categories. Additionally, the articles were appraised and the level of evidence and grade of each was assigned based on the recommendations provided by the Joanna Briggs Institute (Joanna Briggs Institute, 2014).
Figure 1.
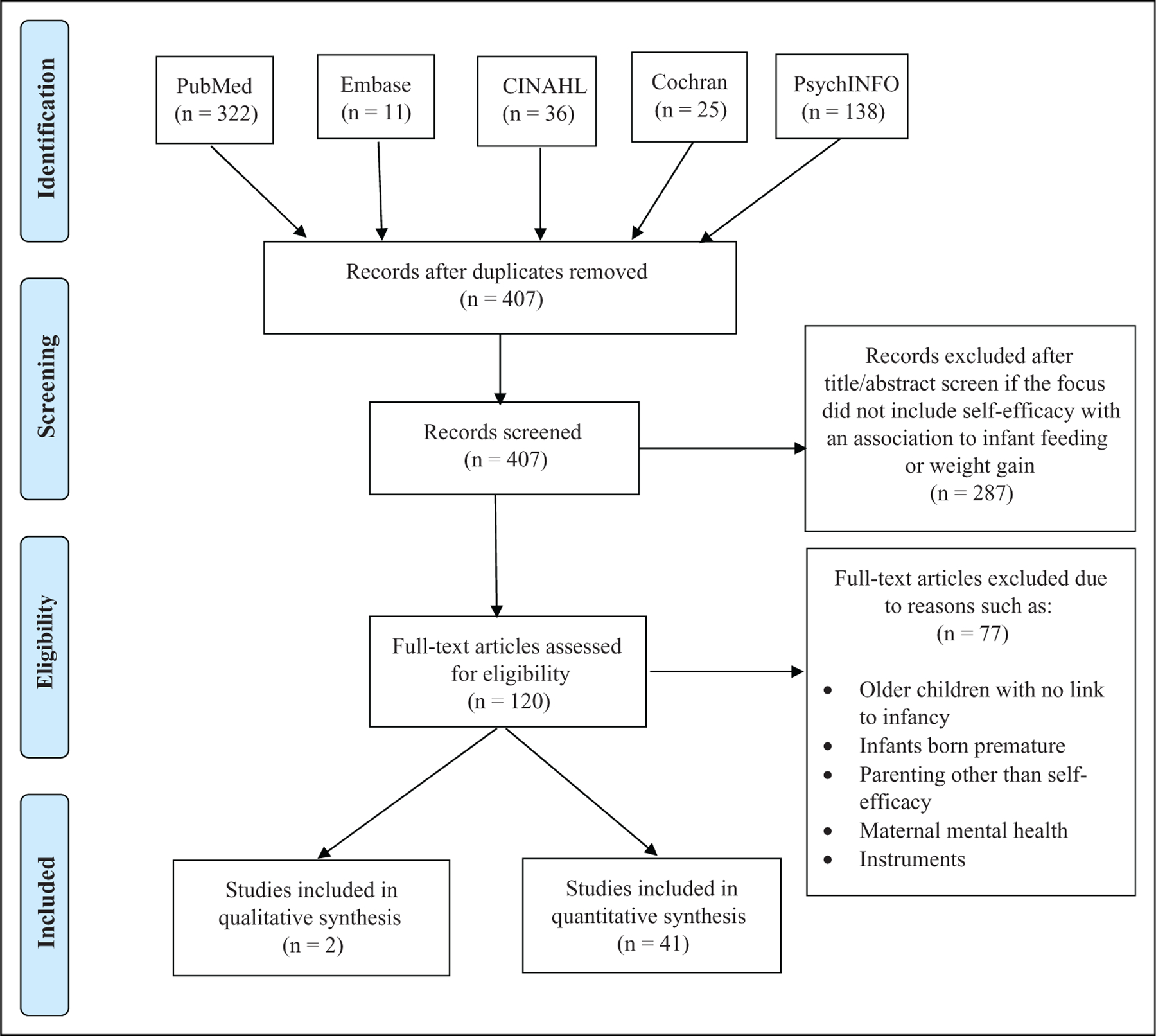
PRISMA flow diagram of search. From: Moher et al. (2009).
Results
A total of 43 articles were included to guide this review (Tables 3–7). These studies used populations from a variety of geographic areas including the United States, Australia, Canada, Brazil, Turkey, Europe, and Asia. Articles were included if the topic of self-efficacy and infant feeding practices or infant weight gain was addressed regardless of the race, ethnicity, or socio-demographics of the population studied including both first-time and experienced parents. Self-efficacy was measured in a variety of ways: self-efficacy in general, self-efficacy specific to parenting, self-efficacy specific to breastfeeding, and self-efficacy specific to maternal feeding. Results of this review are classified into three categories of articles that examined an association with self-efficacy: (1) breastfeeding; (2) infant feeding practices such as parental feeding style and dietary quality; and (3) infant weight gain. A limited number of the articles addressed associations of self-efficacy with more than one category. The following sections provide an overview of findings.
Table 3.
Breastfeeding self-efficacy and breastfeeding.
| First author (year) | Study design and location | Variables (tools) | Sample size and participants | Findings | Level of evidence | Grade |
|---|---|---|---|---|---|---|
| Baghurst (2007) | Cohort study (followed from late pregnancy to 6 months PP) Adelaide, Australia |
IV: BF Self-efficacy (BFSE Short Form) DV: BF Duration |
N = 317 primiparous mothers and infants 88% Caucasian |
BFSE at 1 week PP was an important predictor for BF duration | 3.e | A |
| Barbosa et al. (2017) | Qualitative, focus groups Richmond, Virginia, USA |
NA |
N = 25 mothers (any parity) Low-income, African-American |
Group of mothers who breastfed for longer than 4 months exhibited higher levels of general self-efficacy as well as BFSE | 3* | A |
| Bartle (2017) | Prospective questionnaire study England |
IV: BF Self-efficacy (BFSE Short Form) (32 weeks Gestation) DV: BF initiation and any BF at 6 weeks PP |
N = 149 mothers (n = 77 primiparous, n = 72 multiparous) 87% Caucasian |
BFSE associated with BF at 6 weeks only in the multiparous group of mothers (r = .36, p < .01). No association in primiparous mothers (r = .09, p > .05) | 3.e | A |
| Furman et al. (2013) | Qualitative, focus groups Cleveland, Ohio, USA |
NA |
N = 20 pregnant or PP women Inner city African-American |
Themes of self-efficacy and self-esteem identified as barriers or facilitators to BF | 3* | A |
| Gercek et al. (2017) | Cross-sectional, descriptive Turkey | IV: BF Self-efficacy (BFSE Short Form) DV: BF success (LATCH BF Assessment Tool) |
N = 303 mothers and infants (any parity) Primarily Turkish |
High BFSE was associated with higher LATCH scores PP | 4.b | A |
| Glassman (2014) | Prospective cohort study New York City |
IV: BF Self-efficacy (BFSE Short Form) DV: Initiation and continuation of BF through 1 month PP |
N = 209 (156 at 1 month) mothers and infants (any parity) Low income, Latina |
Higher BFSE resulted in higher rates of BF at 1 month PP Only BFES was associated with exclusive BF |
3.e | A |
| Henshaw et al. (2015) | Prospective cohort study Ohio |
IV: BF Self-efficacy (BFSE Short Form) DV:BF exclusivity |
N = 142 primiparous mothers and infants 85% Caucasian, 10% African-American |
BFSE at 2 days PP was significant predictor of BF exclusivity at 6 months PP but not 6 weeks PP | 3.e | A |
| Karall et al. (2015) | Prospective cohort study (followed first 24 months of infant’s life) Tyrol, Austria |
IV: Open-ended questions regarding reason for weaning (no tool provided) DV: BF duration |
N = 555 mothers and infants (any parity) Primarily Austrian |
Low BFSE is risk for early weaning | 3.e | B |
| Ku (2010) | Non-experimental, cross-sectional design Hong Kong |
IV: BF Self-efficacy (BFSE Scale) DV: BF patterns and exclusivity |
N = 82 primiparous mothers and infants Primarily Chinese |
Higher BFSE is associated with higher odds of exclusive BF (OR 1.104, p < .001) | 4.b | A |
| Loke (2013) | Descriptive, correlation study Hong Kong |
IV: BF Self-efficacy (BFSE Scale) DV: BF duration and exclusivity |
N = 199 mothers (any parity) Primarily Chinese |
High BFSE was associated with exclusive BF at 6 weeks PP (OR 7.776, p < .001) | 3.e | A |
| McCarter-Spaulding (2009) | Descriptive, longitudinal cohort study New England |
IV: BF Self-efficacy (BFSE Scale) DV: BF duration and pattern |
N = 125 mothers (any parity) African decent (32% African-American, 25% Caribbean, 10% African, 8% Cape Verdean, 25% Other) |
Higher BFSE associated with longer duration and more exclusive BF at 1 and 6 months PP (p < .01) | 3.e | A |
| McQueen (2015) | Prospective Cohort study Ontario, Canada |
IV: BF Self-efficacy (BFSE Short Form) DV: BF outcomes at 4 and 8 weeks PP |
N = 130 mothers and infants (any parity) Aboriginals of North America (Indians (First Nations), Metis, and Inuit) |
Higher BFSE in the immediate PP period associated with higher probability of any BF for at least 8 weeks | 3.e | A |
| Nommsen-Rivers (2010) | Cross-sectional (prenatally) California, USA |
IV: BF Self-efficacy (BFSE Short Form) DV: BF intention |
N = 532 primiparous mothers White non-Hispanic 41%, Hispanic 26.7%, African-American 14.1%, Asian 12%, Other 6.2% |
Higher BFSE positively associated with BF intention (p < .0001) Higher comfort with formula feeding inversely associated with BF intention (p < .0001) |
4.b | A |
| Otsuka (2008) | Cross-sectional Japan (Tokyo and Kusatsu) |
IV: BF Self-efficacy (BFSE Short Form) DV: Perception of breast milk supply (Perception of Insufficient Milk Questionnaire) |
N = 262 mothers and infants (any parity) Primarily Japanese |
BFSE and perception of insufficient breast milk supply were negatively correlated (r = −.45, p <.001) BFSE explained 21% of variance in maternal perception of breast milk supply |
4.b | A |
| Robinson (2011) | Mixed Methods Midwest US | IV: BF Self-efficacy (BFSE Short Form) DV: Intention to BF |
N = 59 (quantitative portion), 17 (qualitative portion) mothers and infants (any parity) African-American |
BFSE was different between those intending to BF and those not (p = .001), higher BFSE associated with higher intention to BF | 4.b | A |
| Semenic (2008) | Prospective, correlational (followed from birth to 6 months PP) Montreal, Quebec, Canada |
IV: BF self-efficacy (BFSE Short Form) DV: Exclusive BF at 6 months |
N = 189 primiparous mothers intending to BF English Canadians, French Canadians, and immigrants |
Higher BFSE associated with longer duration of exclusive BF (p = .03) | 3.e | A |
| Tsai (2015) | Prospective, longitudinal design Taiwan (Taipei and Yi-Lan) |
IV: BF self-efficacy (BFSE Scale) DV: BF practice |
N = 300 Primiparous mothers Primarily Taiwanese | BFSE was significantly associated with exclusive BF in the immediate PP period as well as 1 month and 3 months PP | 3.e | A |
| Yang et al. (2016) | Cross-sectional descriptive Guangzhou, China |
IV: Network Support for Breastfeeding Scale DV: BF Self-efficacy (BFSE Short Form) |
N = 571 mothers (any parity) Chinese | Six predictors of BFSE in the immediate PP period: intention to BF, husband support, nurse/midwife support, attendance of prenatal BF classes, time from birth to initiation of BF, and previous BF experience | 4.b | A |
Table 7.
Self-efficacy and feeding practices, feeding style, or weight gain intervention studies.
| First author (year) | Study design and location | Variables (tools) | Sample size and participants | Findings | Level of evidence | Grade |
|---|---|---|---|---|---|---|
| Shah et al. (2016) | 2-year follow-up of a RCT, retrospective chart review New Haven, CT |
IV: Intervention—Group well care (focus on maternal/infant relationships and PSE) for the infant’s first year; Control—Standard individualized care for the infant’s first year DV: Nutrition Behaviors, Child weight at 24, 30, and 36 months |
N = 63 mother-infant dyads (n = 40 intervention, n = 23 control) (any parity) African-American, Caucasian, Hispanic (percentage of each not provided) |
No statistical differences in nutrition or weight between groups; however, a trend seen in the intervention group for ever being overweight | 1.c | A |
| Willis et al. (2014) | Pre/post test experimental study (not control group) England |
IV: Heath, Exercise, Nutrition for the Really Young (HENRY) 8-week program DV: PSE (Parenting Self-Agency Measure), Family dietary habits (Food Frequency Questionnaire, Family Eating & Activity Habits Questionnaire) |
N = 60 parents and children (average age 3.3 years, 22% had an infant) (any parity) 86.7% Caucasian |
PSE significantly increased after the program and remained high at the 8-week follow time point (p < .001) Children’s intake of vegetables, fruit, and legumes all showed a significant increase |
2.d | A |
| Zhang et al. (2009) | Cluster-randomized control trial, blinded Beijing, China |
IV: Intervention—Education sessions and home visits every 3 months on infant nutrition; Control—Routine counseling on infant feeding DV: Maternal knowledge of infant feeding, attitudes, subjective norms, self-efficacy on feeding, intention to adopt optimal feeding practices (tool developed by researchers) |
N = 485 mother-infant dyads (n = 251 intervention, n = 234 control) (enrolled at infant age of 2–4 months) (any parity) Primarily Chinese (Han) |
Maternal feeding self-efficacy significant rose post-intervention (p < .001) and significantly differed from control group (p < .001) Maternal feeding self-efficacy was also associated with mothers’ intention to use optimal feeding behaviors at baseline (p = .002) and post-intervention (p < .001) |
1.c | A |
Breastfeeding
Evidence suggests that women with a higher sense of BFSE have higher rates of breastfeeding initiation, longer durations of any breastfeeding, and longer durations of exclusive breastfeeding, as compared to women who report a lower sense of BFSE (Table 3) (Gercek et al., 2017; Henshaw et al., 2015; Karall et al., 2015). Additionally, two qualitative studies that examined mothers’ decisions to breastfeed identified self-efficacy as an important theme (Barbosa et al., 2017; Furman et al., 2013). From these findings, several interventions have been developed and tested to determine the impact on a mother’s sense of BFSE (Table 5) (Abbass-Dick et al., 2017; Dodt et al., 2015; Joshi et al., 2016; Liu et al., 2017).
Table 5.
Breastfeeding self-efficacy intervention studies.
| First author (year) | Study design and location | Variables (tools) | Sample size and participants | Findings | Level of evidence | Grade |
|---|---|---|---|---|---|---|
| Abbass-Dick et al. (2017) | Pre/post test experimental study (phase 2 of the study) Ontario, Canada |
IV: Intervention—An eHealth breastfeeding and co-parenting resource, interactive with multimodal delivery of information (developed based on feedback from Phase I) DV: BF Self-efficacy (BFSE Short Form) |
N = 31 mothers and N = 35 fathers (primiparous) Race/ethnicity not provided |
Maternal and paternal BF self-efficacy scores rose posttest | 2.d | A |
| Chan (2016) | Experimental design with random assignment Hong Kong |
IV: Intervention—2 hour BF workshop prenatally and 30–60 minute telephone session at 2 weeks PP. Control—standard care DV: BF exclusivity, BF Self-efficacy (BFSE Short Form) |
N = 71 primiparous mothers (35 intervention, 36 control) 95% Chinese |
BFSE scores significantly higher in intervention group from prenatal to 2 weeks PP (p < .01) and higher than control group at 2 weeks PP (p < .01) Exclusive BF in intervention group higher at each time point to 6 months, on significant at 8 weeks PP (p = .02) |
1.d | A |
| Dodt et al. (2015) | Experimental, pre/post-test design, interventional and control groups Brazil |
IV: Intervention—flip chart containing education on BFSE during PP period in hospital (between 6 hours PP and hospital discharge). Control—no flip chart DV: BF Self-efficacy (BFSE Short Form), BF rates |
N = 201 mothers (100 intervention, 101 control) (any parity) Primarily Brazilian |
Intervention group had higher change in BFSE scores from immediate PP period to 2 months PP (p = .032). Exclusive BF at 2 months PP: intervention group, 100%, control group 41% |
2.d | A |
| Hauck et al. (2007) | Experimental study Australia | IV: Intervention—Breastfeeding journal with education material provided at approximately 36-week gestation. Control—No journal provided DV: BF Self-efficacy (BFSE Scale) |
N = 276 primiparous mothers (136 intervention, 140 control) Primarily Australian *Both groups attended a prenatal BF workshop |
No statistically significant differences between the intervention and control groups in BFSE during the immediate PP period (p = .23) or the 12 weeks PP period (p = .75) | 2.c | B |
| Joshi et al. (2016) | Two-group, repeated measures quasi-experimental study Nebraska |
IV: Intervention—Computer based BF educational support program administered last 6 weeks of pregnancy. Control—printed educational material on BF. DV: BF exclusivity, BF Self-efficacy (BFSE Short Form) |
N = 46 mothers (any parity) Rural, Hispanic |
Intervention group at higher intent to BF 1 week PP Not significant but BFSE scores decreased from 6 weeks to 6 months in the control group, and increased in the intervention group |
2.c | A |
| Liu et al. (2017) | Comparative, quasi-experimental study China |
IV: Intervention—1 hour prenatal BF workshop and 1-hour BF counseling session within 24 hours of birth. Control—standard care. DV: BF exclusivity at 8 weeks PP, BF Self-efficacy (BFSE Short Form) |
N = 130 (65 each group) primiparous mothers Primarily Chinese |
Intervention group had significantly higher BFSE scores at 4 weeks PP (p < .0001) & 8 weeks PP (p < .0001) than the control group At 8 weeks PP 24.6% of intervention infants were exclusively BF, compared to 1.5% of control group infants (p < .0001) |
2.c | A |
| McQueen et al. (2011) | RCT (pilot study) Ontario, Canada |
IV: Intervention—Individual BFSE enhancing sessions, 2 PP in hospital and 1 a week after birth. Control—standard care. Provided third trimester. DV: BF Self-efficacy (BFSE Short Form), BF duration and exclusivity. 4 weeks PP |
N = 150 (69 intervention, 81 control) primiparous mothers 81% Caucasian, 14% Aboriginals of North America |
Mothers in the intervention group had higher rates of BF self-efficacy, duration, and exclusivity at 4 and 8 weeks PP, but not significant Intervention was feasible |
1.c | A |
| Nichols (2009) | Experimental study Queensland, Australia |
IV: Intervention—BFSE interactive workbook. Control—Workbook on parenting, no mention of BF. DV: BF duration and exclusivity, BF self-efficacy (BFSE Scale) |
N = 90 (number in each group not provided) mothers (any parity) Primarily Australian |
Mothers in the intervention group at higher BFSE (p = .03) | 2.c | A |
| Noel-Weiss (2006) | RCT Canada | IV: Intervention—delivered prenatally, after 34 weeks gestation, a 2.5 hour BF workshop based on Bandura’s self-efficacy theory and adult learning. Control—standard care DV: BF Self-efficacy (BFSE Short Form), duration of BF |
N = 110 primiparous mothers Race/ethnicity not provided |
BFSE higher in intervention group Exclusive BF higher in intervention group at 4 and 8 weeks PP |
1.c | A |
| Wu (2014) | Experimental, pre/post test, 2 group design Wuhan, China |
IV: Intervention—3 phase (2 face-to-face in the immediate PP period, 1 via telephone 1-week after hospital discharge) individual sessions focused on self-efficacy and BF. Control—Standard care. DV: BF self-efficacy (BFSE Short Form), |
N = 74 primiparous mothers (37 each group) Primarily Chinese |
Intervention group had significantly higher BFSE at 4 weeks (R2 = .74, p < .001) and 8 weeks PP (R2 = .74, p < .001) | 2.d | A |
Interventions targeting BFSE have been varied. Some have included BFSE as a part of the intervention (Dodt et al., 2015; McQueen et al., 2011) and others have tested an intervention on a mother’s sense of BFSE (Abbass-Dick et al., 2017; Liu et al., 2017). Interventions included electronically accessible resources, face-to-face sessions, or workbooks, offered prenatally and/or postnatally, in groups or individual sessions (Table 5). Regardless of the type of intervention, most studies found that the intervention increased a mother’s sense of BFSE and contributed to higher rates of either breastfeeding initiation or duration of any or exclusive breastfeeding. Only one study found no difference in BFSE between the intervention and control groups in a cohort of Australian mothers; however, all of the participants (intervention and control group) attended a prenatal breastfeeding workshop (Hauck et al., 2007). Recognizing that BFSE is an important predictor for breastfeeding success, Yang and colleagues (2016) identified six constructs which increase a mother’s sense of BFSE: breastfeeding intention, partner support, nurse/midwife support, attending a prenatal breastfeeding class, time to initiation of breastfeeding in the immediate postpartum period, and prior experiences of breastfeeding. Additionally, Bartle and Harvey (2017) found that prior personal and vicarious experiences influenced a mother’s sense of BFSE, as well as the decision to breastfeed or provide formula.
General self-efficacy or PSE and the association with breastfeeding have also been examined, though to a lesser extent (Table 4). General self-efficacy (not specific to breastfeeding or parenting) was examined in a group of mothers from rural China finding that those with higher reported self-efficacy were more likely to exclusively breastfeed (Shi et al., 2008). Separate systematic reviews examining support for breastfeeding suggest that interventions that increase a mother’s sense of self-efficacy, while being tailored to individual needs, are most beneficial to successful breastfeeding (Demirtas, 2012; Hannula et al., 2008). The researchers did not indicate whether this was general self-efficacy, PSE, or BFSE. Hernandez’s study (2014) is the only one identified which examined an association between PSE and breastfeeding. This study was conducted in the United States in a population of Mexican-American women (N = 110) using the Parent’s Expectation Survey to measure PSE. PSE was measured in the 48 hours postpartum and negatively correlated (r = −.23, p = .01) with breastfeeding at infant age of six weeks. The negative correlation between PSE and breastfeeding is contradictory to most findings examining BFSE; however, three observations were noted by the researchers: (1) cultural differences in the Mexican-American population could influence feeding practices; (2) 80% of the mothers were experienced, and there was no differentiation with first-time mothers; and (3) this study was the first time the Parent’s Expectation Survey was translated to Spanish for use in a study.
Table 4.
Self-efficacy and breastfeeding.
| First author (year) | Study design and location | Variables (tools) | Sample size and participants | Findings | Level of evidence | Grade |
|---|---|---|---|---|---|---|
| Hernandez (2014) | Prospective, cross-sectional study (unpublished dissertation) Tampa, FL, USA |
IV: PSE (Parent’s Expectation Survey), measured at birth, General Self-efficacy (General Self-Efficacy Scale) DV: Exclusive BF at 6 weeks PP (breastfeeding index) |
N = 110 mothers (80% multiparous, 20% primiparous) Mexican-American (Hispanic) |
Higher PSE significantly associated with decreased BF intensity (p = .01). General self-efficacy not associated with BF |
4.b | B |
| Shi et al. (2008) | Cross-sectional survey Rural China |
IV: General self-efficacy (4 questions developed by researchers for use in the study) DV: BF exclusivity or fully BF (breast milk plus small quantity of other liquids) |
N = 599 mothers–infant dyads (parity not provided) Primarily Chinese (Han) |
Higher self-efficacy associated with mothers being more likely to fully breastfeed (OR 1.06, p <.01) | 4.b | B |
Infant feeding practices
Self-efficacy and infant feeding other than breastfeeding have also been examined (Table 6). Barrett and colleagues (2016) reported that PSE is associated with parental feeding styles. PSE was measured using the Parenting Sense of Competence Scale and found to be positively associated (r = .20, p < .05) with the restrictive feeding style in a sample of first-time African-American mother–infant dyads. Mothers who reported a higher sense of PSE tended to demonstrate the restrictive feeding style, which has previously been linked with lower caloric intake, increased breastfeeding, and decreased inappropriate feeding (i.e. using food to soothe or providing foods with low nutrient value) (Thompson et al., 2013). The pressuring feeding style has been associated with inappropriate infant feeding (Stifter and Moding, 2015; Thompson et al., 2013), but no significant correlation with PSE was seen in the study by Barrett and colleagues (2016). The researchers conclude that strengthening of PSE along with maternal self-esteem may be targets for future intervention studies (Barrett et al., 2016).
Table 6.
Self-efficacy and feeding practices, feeding style, or weight gain studies.
| First author (year) | Study design and location | Variables (tools) | Sample size and participants | Findings | Levels of evidence | Grade |
|---|---|---|---|---|---|---|
| Anzman-Frasca et al. (2013) | Correlational study Pennsylvania | IV: PSE (Parenting Sense of Competence Scale), Infant Temperament (Infant Behavior Questionnaire-Revised) DV: Infant Weight (measured at 1 year BMIz and residual weight gain from 1–3 years) |
N = 110 mother-toddlers (1 year of age) (primiparous), subset n = 75 mother–toddlers (3 years of age) 91% Caucasian |
Low PSE and negative infant temperature predicted greater weight gain from 1 to 3 years of age (β = −.35, p < .01), the relationship was opposite when mothers had high PSE | 3.e | B |
| Barrett et al. (2016) | Secondary data analysis of the Infant Care, Feeding, and Risk of Obesity Study; correlational study Chapel Hill, NC |
IV: PSE (Parenting Sense of Competence Scale) DV: Maternal Feeding Style (Infant Feeding Style Questionnaire) |
N = 160 mother–infant dyads (primiparous) African-American |
Self-efficacy was correlated with the restricted feeding style (r = .20, p < .05) | 3.e | B |
| Campbell et al. (2010) | Cross-sectional study Sydney, Australia |
IV: Maternal Feeding Self-efficacy (9 item questionnaire developed by the researchers) DV: Child dietary habits at 1 and 5 years of age (Eating and Physical Activity Questionnaire) |
N = 140 mother–child dyads (n = 60 at 1 years, n = 80 at 5 years) (parity not provided) Primarily Australian |
Maternal feeding self-efficacy associated with vegetable intake in 1-year old children (r = .31, p < .05), inversely associated with cake intake (r = −.34, p < .0005) | 4.b | B |
| Koh et al. (2014) | Cross-sectional study, first time point of the South Australian Infants Dietary Intake study South Australia |
IV: Maternal Feeding Self-efficacy (5 items from the self-efficacy questionnaire used in the Nutrition Education Aimed at Toddlers) DV: Dietary intake (dietary recalls and food records |
N = 277 mother-infant dyads (infant age 6–7 months) (any parity) Primarily Australian |
Maternal feeding self-efficacy was significantly related to vegetable variety (β = .61, p < .05) and was influenced by maternal confidence (β = .36, p < .01), how often mothers offered new foods (β = .26, p < .05), frequency a new food was offered before deciding a child doesn’t like it (β = .40, p < .01), and child willingness to eat new food (β = .70, p < .01) | 4.b | B |
| Spence et al. (2014) | Secondary data analysis of the Melbourne Infant Feeding Activity and Nutrition Trial (InFANT) Program; correlational study (tested mediation affect on the intervention arm) Melbourne, Australia |
IV: Maternal Feeding Self-efficacy (same tool used by Campbell et al., 2010) DV: Child Diet (Comprehensive Feeding Practices Questionnaire and dietary recalls) |
N = 528 mother-child dyads (child age 18 months) (primiparous) Primarily Australian |
Maternal feeding self-efficacy associated with child diet quality, but was not a mediator to the intervention arm of the InFANT Program | 3.e | B |
| Stifter and Moding (2015) | Cohort, correlational study Pennsylvania | IV: PSE (Parenting Self-efficacy Questionnaire) DV: Use of food to soothe (at 6 months, question asked of the mother, at 12 and 18 months the Food to Soothe Questionnaire; also observed in the lab) |
N = 160 mother–infant/toddler dyads (infants from 6 to 18 months) (any parity) 95% Caucasian |
PSE associated with using food to soothe the infant at 6 months, parent report (β = .21, R2 = .31, p < .05) and lab findings (β = 1.61, OR = 5, p < .01) Using food to soothe at 6 months was associated with increased weight gain from 6 to 18 months (β = .3, R2 = .15, p < .001) |
3.e | B |
| Stifter et al. (2011) | Cohort, correlational study Pennsylvania | IV: PSE (Parenting Self-efficacy Questionnaire) DV Use of food to soothe (Baby Basic Needs Questionnaire); Infant weight and length (BMIz) |
N = 78 mother–infant/toddler dyads (ages 3 to 34 months) (any parity) Caucasian |
PSE associated with using food to soothe the infant (r = −.29, p = .04) PSE not associated with child weight status (r = .2, p > .05) |
3.e | B |
| Xu et al. (2013) | Cross-sectional study, secondary analysis from the Health Beginnings Trial control group Sydney, Australia |
IV: PSE (Used questions from the ‘Growing up in Australia: The Longitudinal Study of Australian Children’) DV: Child dietary habits (questions from the NSW Child Health Survey 2011) |
N = 242 mother–toddler dyads (age 2 years) (primiparous) Primarily Australian |
PSE associated with fruit (p = .002) and vegetable (p = .003) consumption in toddlers, and inversely associated with soft drink consumption (p = .003). | 4.b | B |
Three studies conducted in Australia examined mothers’ sense of self-efficacy and dietary preferences in toddlers. All indicated that mothers who reported a higher sense of self-efficacy had toddlers with greater intake of fruit and vegetables and less intake of soft drinks and sweets (Campbell et al., 2010; Spence et al., 2014; Xu et al., 2013). Koh and colleagues (2014) examined maternal feeding self-efficacy, maternal psychological symptoms, parenting confidence, and infant feeding behavior in a group of Australian mother–infant dyads at infant age of six months. Similar to the findings above with mother–toddler dyads, mothers who reported a higher sense of self-efficacy offered an increased variety of vegetables to their infant compared to mothers who reported a lower sense of self-efficacy (R2 = .14, p < .05). Maternal feeding self-efficacy was also positively correlated with how often the mother offered new foods (r = .64, p < .001) and the frequency of offering a food (r = .52, p < .001). The authors concluded that a higher sense of self-efficacy contributes to healthy infant feeding practices and dietary habits of infants and that modification of the antecedents to maternal feeding self-efficacy, such as familial feeding practices, may be important interventions to target (Koh et al., 2014).
An intervention study conducted in China demonstrates that enhancing PSE may contribute to infant feeding practices that better align with recommendations (Zhang et al., 2009). Mother–infant dyads were enrolled in this study at infant age of two to four months (Table 7). The intervention group received training on child nutrition and infant feeding practices every three months. PSE was measured at baseline and again at study completion when the infants were 10–11 months of age. Post-intervention, mothers in the intervention group had higher PSE scores (M = 11.3 (SD = 5.6) vs M = 6.0 (SD = 5.7), p < .001), higher intentions to adopt recommended infant feeding practices (M = 6.7 (SD = 1.7) vs M = 4.0 (SD = 2.0), p < .001), and PSE was positively correlated with intention to adopt recommended infant feeding practices (standardized β = .21, p < .001) (Zhang et al., 2009). Additionally, the infants in the intervention group were breastfed longer and received complementary foods around six months of age, consistent with infant feeding recommendations (Zhang et al., 2009). A separate study conducted in the United Kingdom had similar findings with parents of children (infants through preschoolers) (Willis et al., 2014). These parents received eight weeks of educational sessions regarding health, exercise, and nutrition; PSE scores rose significantly (Cohen’s d = .6, p < .001) from baseline to study completion as did family dietary practices such as eating as a family and increased consumption of fruits and vegetables (Willis et al., 2014). This research provides examples of how impacting PSE may have a positive influence on infant and child feeding practices.
Infant weight gain
Studies examining the association between self-efficacy and infant weight gain are lacking. Stifter and colleagues (2011) examined the correlation between PSE and infant and toddler weight status; a positive, yet non-significant correlation was seen (r = .20, p > .05). This study was conducted in the northeastern region of the United States in a sample of Caucasian mother–child dyads (ages 3–34 months) with 49% of families having an income of at least $60,000 and mothers who were primarily well educated (65% with a college degree). Child weight status at a single visit was calculated by body mass index (BMI) z-score using WHO standards (Stifter et al., 2011). Despite this null finding, researchers suggest that the practice of using food to soothe an infant may mediate the relationship between PSE and infant weight gain (Stifter et al., 2011; Stifter and Moding, 2015). Mothers who reported a low sense of PSE were more likely to use food to soothe their infant, which in turn was associated with a higher BMI z-score (Stifter et al., 2011) or a rapid rate of infant weight gain (Stifter and Moding, 2015).
Infant temperament may also mediate or moderate the relationship between PSE and infant weight gain. Infants reported as having a negative temperament were more likely to exhibit a higher BMI z-score (Stifter et al., 2011) or rapid weight gain through infancy (Anzman-Frasca et al., 2013). Anzman-Frasca and colleagues (2013) found that this association between negative infant temperament and rapid weight gain was only seen when mothers reported a low sense of PSE; the relationship was opposite in mothers reporting a high sense of PSE. Further exploration is needed, but these findings imply that low PSE and/or negative infant temperament may work independently or together to trigger a mother to use food to soothe her infant, and thereby inadvertently promoting increased weight gain.
Shah and colleagues (2016) conducted an intervention study that examined whether dietary behaviors and/or infant/toddler weight differed in a group of mother–infant dyads who received infant well care in a group setting (experimental) versus an individual setting (control). The experimental arm received infant well care (over the first year of life) focused on maternal–infant attachment and PSE in a group setting with other mothers and infants. In this sample, no statistically significant differences were observed between groups regarding dietary practices or child weight up to 36 months of age; however, the experimental group had less incidence of ever being overweight (Shah et al., 2016). A limitation of the study was that PSE of the mothers was not measured; therefore, differences between groups could not be examined nor pre-/post-intervention differences. However, these findings lend further support to the need for future investigation of the association of PSE and infant weight gain.
Discussion
This review has outlined the literature regarding the association of self-efficacy with infant feeding practices and infant weight gain. In sum, mothers who exhibit a higher sense of self-efficacy engage in infant feeding practices that better align with recommendations, such as breastfeeding and providing nutrient dense foods to infants. Research regarding BFSE and the association with breastfeeding initiation and duration is abundant. However, the dearth of literature regarding other feeding practices is evident. Specifically, there are minimal studies that examine an association between self-efficacy and parental feeding style or types and quality of foods offered. Additionally, the majority of research has been conducted in Caucasian mothers and fathers, and mothers of other racial and ethnic groups have not often been studied. Finally, only one study examined the association between self-efficacy and infant weight gain limiting conclusions.
Mothers who reported a higher sense of BFSE had higher rates of breastfeeding initiation and a longer duration of any breastfeeding including exclusive breastfeeding (Gercek et al., 2017; Henshaw et al., 2015; Karall et al., 2015). The association of self-efficacy with breastfeeding was also supported by studies describing how interventions that increase a mother’s sense of BFSE are successful at increasing the duration and exclusivity of breastfeeding (Abbass-Dick et al., 2017; Liu et al., 2017). Joshi and colleagues (2016) found that six weeks and three months postpartum were key time points when breastfeeding intervention and support was needed. The association between BFSE and breastfeeding is important as breastfeeding has been associated with a lower rate of weight gain during infancy compared with formula fed infants (Li et al., 2012). Rapid weight gain during infancy is associated with pediatric obesity, therefore an important modifier to consider during infancy (Druet et al., 2012; Ong and Loos, 2006). Additionally, breastfeeding has been associated with healthy dietary practices later in childhood, such as increased intake of fruits and vegetables and less intake of sugar-sweetened beverages (Perrine et al., 2014).
Despite the abundance of literature showing an association between BFSE and breastfeeding, there were some contradictory findings. Bartle and Harvey (2017) found the association between BFSE and breastfeeding to be significant in experienced mothers only, not in first-time mothers. The additional finding regarding the influence of vicarious experiences on BFSE and breastfeeding practices may contribute to the differences seen between the experienced and first-time mothers (Bartle and Harvey, 2017). Vicarious experience is known to contribute to the development of one’s self-efficacy (Bandura, 1997); however, the study by Bartle and Harvey (2017 may be the first to examine this association in the context of breastfeeding. Additional research is needed to elucidate the role of vicarious experiences on BFSE and breastfeeding.
Hernandez (2014) is the only study identified in this review that did not support an association of self-efficacy with improved breastfeeding in a cohort of primarily experienced mothers. Although the reasons for this discrepancy are unknown, the study was conducted in a cohort of Mexican-American women, which raises the possibility that there may be cultural influences on the association of self-efficacy with breastfeeding that have yet to be fully explored. Consequently, it would be useful for future research to explore cultural, social, and economic influences on the association of self-efficacy with breastfeeding among more diverse mother–infant dyads.
The evidence regarding an association between self-efficacy and infant feeding practices other than breastfeeding is minimal. However, findings from existing studies are concordant; mothers who reported a higher sense of self-efficacy tended to choose infant feeding practices that aligned with infant feeding recommendations resulting in a better quality of dietary intake (i.e. more fruits and vegetables, less sugar-sweetened beverages) (Koh et al., 2014; Zhang et al., 2009). Additionally, these mothers were more likely to use a restrictive or responsive parental feeding style when self-efficacy was high (Barrett et al., 2016; Koh et al., 2014) and less likely to use food to soothe their infant (Stifter and Moding, 2015). Consequently, it is possible that self-efficacy could impact infant weight gain via infant feeding practices, but these studies did not address this question. Additionally, the studies examining self-efficacy and infant feeding did not follow the cohorts beyond infancy to know whether the associations between self-efficacy and feeding practices were persistent or whether there was an association with childhood weight status. Examining infants during the first year of life is important for establishing healthy dietary practices; however, without following the cohorts longitudinally, the findings cannot be extrapolated to older ages.
There is also a lack of intervention studies to examine whether self-efficacy plays a causal role in infant feeding practices. Only one study was identified in which self-efficacy was a focus in the intervention (Shah et al., 2016). Of note, there are two intervention studies reported in the literature (Paul et al., 2014; Wasser et al., 2017) that measure self-efficacy as an outcome following interventions aimed at reducing infants’ risk for obesity, but neither has reported self-efficacy results as of the date of this review. While not conclusive, findings to date indicate that self-efficacy, specifically PSE or self-efficacy for infant feeding, is important to include in further research.
Weight gain during infancy has important implications for future childhood weight status (Druet et al., 2012). Therefore, it is vital for research to examine modifiable contributors to the rate at which infants gain weight. To date, few studies have examined this association despite evidence that PSE could be a mediator or moderator of the association between infant feeding practices and weight gain (Anzman-Frasca et al., 2013; Barrett et al., 2016; Furman et al., 2013; Shah et al., 2016; Stifter and Moding, 2015). It is plausible that an association between self-efficacy and infant weight gain may exist, but further research is needed.
Conclusion
Additional findings from this review must be noted. First, the majority of populations studied were Caucasian. In the United States, African-American and/or Hispanic infants are at greatest risk for rapid weight gain and feeding practices that do not align with infant feeding recommendations (Gibbs and Forste, 2014; Taveras et al., 2010). As cited above, studies of breastfeeding included a diverse group of populations from across the world including African-American and Hispanic mother–infant dyads; however, these groups are underrepresented in the other studies. The cohort studied by Barrett and colleagues (2016) was a group of African-American mothers and their infants; otherwise, all studies were conducted primarily with Caucasian participants. Second, the inconsistent measurement of self-efficacy based on whether it relates to BFSE, PSE, or maternal feeding self-efficacy in these studies impairs our ability to make direct comparisons of findings. As a result, the question arises whether general self-efficacy or PSE is an adequate measurement or whether a tool that assessed self-efficacy specific to infant feeding practices is needed. Individual researchers have developed tools to measure self-efficacy specific to infant feeding for use in specific studies (Campbell et al., 2010; Koh et al., 2014; Spence et al., 2014; Zhang et al., 2009). Although some of these tools have been used in multiple studies, little is known about the validity of these instruments. Additionally, due to the impact of vicarious experiences identified by Bartle and Harvey (2017), the researchers suggest the development of a self-efficacy tool which addresses formula feeding to be used in addition to the BFSE Scale. Consequently, there is a need to develop a tool to measure self-efficacy specifically with respect to infant feeding practices, and preferably that can be applied across diverse populations.
Limitations
There are limitations to this review that should be noted. The literature search was conducted by a single author, which could impact the totality of the review. Using the Boolean method, many search terms and a variety of databases were used in an effort to conduct a thorough search; however, the possibility remains that articles were missed. Additionally, not all search terms were Medical Subject Heading (MeSH) vocabulary; for example, ‘self-efficacy’ is a MeSH term but neither ‘parental self-efficacy’ nor ‘breastfeeding self-efficacy’ is a MeSH term. This could have resulted in overlooking articles in the PubMed database. There is also a limitation of generalizability. Due to the limited number of articles published on the topic of self-efficacy and infant feeding practices, articles from all over the world, in populations of various race, ethnicity, socioeconomic status, and culture, were included. This makes it difficult to generalize the findings to a particular population.
Implications for practice
Clinicians who care for infants and their parents should be aware of the role self-efficacy may have in parent decisions regarding infant feeding practices, particularly breastfeeding. The abundance and quality of evidence demonstrating the benefit of BFSE in successful initiation and longer durations of breastfeeding is such that clinicians can feel confident in using these findings in practice. BFSE can be screened by clinicians in the prenatal and/or postnatal periods using the self-report Breastfeeding Self-Efficacy Scale—Short Form. Identification of mothers with low BFSE is important to assist clinicians in providing additional education and support to these mothers who are at risk for low breastfeeding initiation and/or short duration of breastfeeding, and hence, whose infants are at increased risk for rapid weight gain.
Although more research is needed regarding the impact of self-efficacy on other infant feeding practices, the few studies to date suggest that feeding practices are healthier and more likely to align with recommendations if parents have a high sense of self-efficacy. Strategies to increase a parent’s sense of self-efficacy could be incorporated into clinic visits and parenting classes, with the ultimate goal of improving an overall sense of self-efficacy which may improve infant nutrition and wellness. Self-report questionnaires to measure a parent’s sense of PSE are available. A review by Wittkowski and colleagues (2017) identified 34 such instruments. The Karitane Parenting Confidence Scale (KPCS) and Perceived Maternal Parenting Self-Efficacy Scale received the highest overall scores in this review. However, the authors caution that no tool received a perfect score and with so many tools, a practitioner should consider the tool in the context of the population and setting to determine the most appropriate for the circumstances (Wittkowski et al., 2017). The KPCS is available free of charge for use in clinical and research settings.
Future research
The positive outcomes of interventions to address BFSE support the importance of self-efficacy for infant feeding practices in general. However, there is a dearth of research regarding other feeding practices such as the age of complementary food introduction, types of complementary foods offered during infancy, formula feeding, and the parental feeding style used. There is also a lack of longitudinal research examining self-efficacy and a child’s dietary habits and growth. Research has shown that a parent’s sense of PSE increases over time (De Montigny and Lacharité, 2005; Salonen et al., 2009), but it is unknown whether PSE changes as a child becomes independent with eating. In addition, most research to date has examined a maternal sense of self-efficacy, but research of fathers and other caregivers is warranted. In the United States, approximately 59% of mothers with infants work outside the home (Bureau of Labor Statistics, 2017) with fathers and grandmothers being the most common non-maternal familial caregivers. It is also important to recognize that despite their high risk for childhood obesity (Taveras et al., 2010), minority populations are often understudied, warranting more study of diverse populations. Finally, despite the abundance of tools available to measure PSE, none specific to self-efficacy to infant feeding are available for use. Researchers should consider the need for a tool to measure self-efficacy specific to feeding practices other than breastfeeding.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Abbass-Dick J, Xie F, Koroluk J, et al. (2017) The development and piloting of an eHealth breastfeeding resource targeting fathers and partners as co-parents. Midwifery 50: 139–147. [DOI] [PubMed] [Google Scholar]
- American Academy of Pediatrics Committee on Nutrition (2014) Pediatric Nutrition. Grove Village: American Academy of Pediatrics. [Google Scholar]
- Anzman-Frasca S, Stifter CA, Paul IM, et al. (2013) Infant temperament and maternal parenting self-efficacy predict child weight outcomes. Infant Behaviour & Development 36: 494–497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baghurst P, Pincombe J, Peat B, et al. (2007) Breast feeding self-efficacy and other determinants of the duration of breast feeding in a cohort of first-time mothers in Adelaide, Australia. Midwifery 23: 382–391. [DOI] [PubMed] [Google Scholar]
- Bandura A (1997) Self-efficacy: The Exercise of Control. New York: W. H. Freeman and Company. [Google Scholar]
- Barbosa CE, Masho SW, Carlyle KE, et al. (2017) Factors distinguishing positive deviance among low-income African American women: a qualitative study on infant feeding. Journal of Human Lactation 33: 368–378. [DOI] [PubMed] [Google Scholar]
- Barrett KJ, Thompson AL and Bentley ME (2016) The influence of maternal psychosocial characteristics on infant feeding styles. Appetite 103: 396–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bartle NC and Harvey K (2017) Explaining infant feeding: The role of previous personal and vicarious experience on attitudes, subjective norms, self-efficacy, and breastfeeding outcomes. British Journal of Health Psychology 22: 763–785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birch LL and Doub AE (2014) Learning to eat: birth to age 2 y. American Journal of Clinical Nutrition 99: 723S–728S. [DOI] [PubMed] [Google Scholar]
- Bureau of Labor Statistics USDoL (2017) Employment characteristics of families - 2016. Available at: https://www.bls.gov/news.release/pdf/famee.pdf (accessed 17 October 2017).
- Campbell KJ, Hesketh K, Silverii A, et al. (2010) Maternal self-efficacy regarding children’s eating and sedentary behaviours in the early years: associations with children’s food intake and sedentary behaviours. International Journal of Pediatric Obesity 5: 501–508. [DOI] [PubMed] [Google Scholar]
- Chan MY, Ip WY and Choi KC (2016) The effect of a self-efficacy-based educational programme on maternal breast feeding self-efficacy, breast feeding duration and exclusive breast feeding rates: A longitudinal study. Midwifery 36: 92–98. [DOI] [PubMed] [Google Scholar]
- Coleman PK and Karraker KH (1997) Self-efficacy and parenting quality: Findings and future applications. Developmental Review 18: 47–85. [Google Scholar]
- De Montigny F and Lacharité C (2005) Perceived parental efficacy: concept analysis. Journal of Advanced Nursing 49: 387–396. [DOI] [PubMed] [Google Scholar]
- Demirtas B (2012) Strategies to support breastfeeding: a review. International Nursing Review 59: 474–481. [DOI] [PubMed] [Google Scholar]
- Dodt RC, Joventino ES, Aquino PS, et al. (2015) An experimental study of an educational intervention to promote maternal self-efficacy in breastfeeding. Revista Latino-Americana De Enfermagem 23: 725–732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Druet C, Stettler N, Sharp S, et al. (2012) Prediction of childhood obesity by infancy weight gain: an individual-level meta-analysis. Paediatric&Perinatal Epidemiology 26: 19–26. [DOI] [PubMed] [Google Scholar]
- Furman LM, Banks EC and North AB (2013) Breastfeeding among high-risk inner-city African-American mothers: A risky choice? Breastfeed Medicine 8: 58–67. [DOI] [PubMed] [Google Scholar]
- Gercek E, Sarikaya Karabudak S, Ardic Celik N, et al. (2017) The relationship between breastfeeding self-efficacy and LATCH scores and affecting factors. Journal of Clinical Nursing 26: 994–1004. [DOI] [PubMed] [Google Scholar]
- Gibbs BG and Forste R (2014) Socioeconomic status, infant feeding practices and early childhood obesity. Pediatric Obesity 9: 135–146. [DOI] [PubMed] [Google Scholar]
- Glassman ME, McKearney K, Saslaw M, et al. (2014) Impact of breastfeeding self-efficacy and sociocultural factors on early breastfeeding in an urban, predominantly Dominican community. Breastfeeding Medicine 9: 301–307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grossklaus H and Marvicsin D (2014) Parenting efficacy and its relationship to the prevention of childhood obesity. Pediatric Nursing 40: 69–86. [PubMed] [Google Scholar]
- Hannula L, Kaunonen M and Tarkka MT (2008) A systematic review of professional support interventions for breastfeeding. Journal of Clinical Nursing 17: 1132–1143. [DOI] [PubMed] [Google Scholar]
- Hauck Y, Hall WA and Jones C (2007) Prevalence, self-efficacy and perceptions of conflicting advice and self-management: effects of a breastfeeding journal. Journal of Advanced Nursing 57: 306–317. [DOI] [PubMed] [Google Scholar]
- Henshaw EJ, Fried R, Siskind E, et al. (2015) Breastfeeding self-efficacy, mood, and breastfeeding outcomes among primiparous women. Journal of Human Lactation 31: 511–518. [DOI] [PubMed] [Google Scholar]
- Hernandez IF (2014) Acculturation, Self-efficacy and Breastfeeding Behavior in a Sample of Hispanic Women. Tampa: University of South Florida. [Google Scholar]
- Joanna Briggs Institute (2014) The JBI approach. Available at: http://joannabriggs.org/jbi-approach.html#tabbed-nav=JBI-approach (accessed 8 April 2018).
- Joshi A, Amadi C, Meza J, et al. (2016) Evaluation of a computer-based bilingual breastfeeding educational program on breastfeeding knowledge, self-efficacy and intent to breastfeed among rural Hispanic women. International Journal of Medical Informatics 91: 10–19. [DOI] [PubMed] [Google Scholar]
- Karall D, Ndayisaba JP, Heichlinger A, et al. (2015) Breast-feeding duration: Early weaning-do we sufficiently consider the risk factors? Journal of Pediatric Gastroenterology and Nutrition 61: 577–582. [DOI] [PubMed] [Google Scholar]
- Koh GA, Scott JA, Woodman RJ, et al. (2014) Maternal feeding self-efficacy and fruit and vegetable intakes in infants. Results from the SAIDI study. Appetite 81: 44–51. [DOI] [PubMed] [Google Scholar]
- Ku CM and Chow SK (2010) Factors influencing the practice of exclusive breastfeeding among Hong Kong Chinese women: A questionnaire survey. Journal of Clinical Nursing 19: 2434–2445. [DOI] [PubMed] [Google Scholar]
- Li R, Magadia J, Fein SB, et al. (2012) Risk of bottle-feeding for rapid weight gain during the first year of life. Archives of Pediatrics and Adolescent Medicine 166: 431–436. [DOI] [PubMed] [Google Scholar]
- Liu L, Zhu J, Yang J, et al. (2017) The effect of a perinatal breastfeeding support program on breastfeeding outcomes in primiparous mothers. Western Journal of Nursing Research 39: 906–923. [DOI] [PubMed] [Google Scholar]
- Loke AY and Chan LK (2013) Maternal breastfeeding self-efficacy anNd the breastfeeding behaviors of newborns in the practice of exclusive breastfeeding. Journal of Obstetric, Gynecologic, and Eonatal Nursing 42: 672–684. [DOI] [PubMed] [Google Scholar]
- McCarter-Spaulding D and Gore R (2009) Breastfeeding self-efficacy in women of African descent. Journal of Obstetric, Gynecologic, and Neonatal Nursing 38: 230–243. [DOI] [PubMed] [Google Scholar]
- McQueen KA, Dennis CL, Stremler R, et al. (2011) A pilot randomized controlled trial of a breastfeeding self-efficacy intervention with primiparous mothers. Journal of Obstetrics, Gynecologic, and Neonatal Nursing: JOGNN 40: 35–46. [DOI] [PubMed] [Google Scholar]
- McQueen KA, Sieswerda LE, Montelpare W, et al. (2015) Prevalence and factors affecting breastfeeding among Aboriginal women in Northwestern Ontario. Journal of Obstetric, Gynecologic, and Neonatal Nursing 44: 51–68. [DOI] [PubMed] [Google Scholar]
- Moher D, Liberati A, Tetzlaff J, et al. (2009) Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6: e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nichols J, Schutte NS, Brown RF, et al. (2009) The impact of self-efficacy intervention on short-term breastfeeding outcomes. Health Education & Behavior 36: 250–258. [DOI] [PubMed] [Google Scholar]
- Noel-Weiss J, Rupp A, Cragg B, et al. (2006) Randomized controlled trial to determine effects of prenatal breastfeeding workshop on maternal breastfeeding self-efficacy and breastfeeding duration. Journal of Obstetric, Gynecologic, and Neonatal Nursing 35: 616–624. [DOI] [PubMed] [Google Scholar]
- Nommsen-Rivers LA, Chantry CJ, Cohen RJ, et al. (2010) Comfort with the idea of formula feeding helps explain ethnic disparity in breastfeeding intentions among expectant first-time mothers. Breastfeeding Medicine 5: 25–33. [DOI] [PubMed] [Google Scholar]
- Ong KK and Loos RJ (2006) Rapid infancy weight gain and subsequent obesity: systematic reviews and hopeful suggestions. Acta Paediatrica 95: 904–908. [DOI] [PubMed] [Google Scholar]
- Otsuka K, Dennis C, Tatsuoka H, et al. (2008) The relationship between breastfeeding self-efficacy and perceived insufficient milk among Japanese mothers. Journal of Obstetric, Gynecologic & Neonatal Nursing 37: 546–555. [DOI] [PubMed] [Google Scholar]
- Paul IM, Williams JS, Anzman-Frasca S, et al. (2014) The intervention nurses start infants growing on healthy trajectories (INSIGHT) study. BMC Pediatrics 14: 184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perrine CG, Galuska DA, Thompson FE, et al. (2014) Breastfeeding duration is associated with child diet at 6 years. Pediatrics 134: S50–S55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Redsell SA, Edmonds B, Swift JA, et al. (2016) Systematic review of randomised controlled trials of interventions that aim to reduce the risk, either directly or indirectly, of overweight and obesity in infancy and early childhood. Maternal & Child Nutrition 12: 24–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson KM and VandeVusse L (2011) African American women’s infant feeding choices: Prenatal breastfeeding self-efficacy and narratives from a black feminist perspective. Journal of Perinatal and Neonatal Nursing 25: 320–330. [DOI] [PubMed] [Google Scholar]
- Salonen AH, Kaunonen M, Astedt-Kurki P, et al. (2009) Parenting self-efficacy after childbirth. Journal of Advanced Nursing 65: 2324–2336. [DOI] [PubMed] [Google Scholar]
- Semenic S, Loiselle C and Gottlieb L (2008) Predictors of the duration of exclusive breastfeeding among first-time mothers. Research in Nursing & Health 31: 428–441. [DOI] [PubMed] [Google Scholar]
- Shah NB, Fenick AM and Rosenthal MS. (2016) A healthy weight for toddlers? Two-year follow-up of a randomized controlled trial of group well-child care. Clinical Pediatrics 55: 1354–1357. [DOI] [PubMed] [Google Scholar]
- Shi L, Zhang J, Wang Y, et al. (2008) Breastfeeding in rural China: association between knowledge, attitudes, and practices. Journal of Human Lactation 24: 377–385. [DOI] [PubMed] [Google Scholar]
- Skinner AC, Ravanbakht SN, Skelton JA, et al. (2018) Prevalence of obesity and severe obesity in US children, 1999–2016. Pediatrics 141: e20173459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spence AC, Campbell KJ, Crawford DA, et al. (2014) Mediators of improved child diet quality following a health promotion intervention: the Melbourne InFANT program. International Journal of Behavior Nutrition and Physical Activity 11: 137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stifter CA, Anzman-Frasca S, Birch LL, et al. (2011) Parent use of food to soothe infant/toddler distress and child weight status. An exploratory study. Appetite 57: 693–699. [DOI] [PubMed] [Google Scholar]
- Stifter CA and Moding KJ (2015) Understanding and measuring parent use of food to soothe infant and toddler distress: a longitudinal study from 6 to 18 months of age. Appetite 95: 188–196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taveras EM, Gillman MW, Kleinman K, et al. (2010) Racial/ethnic differences in early-life risk factors for childhood obesity. Pediatrics 125: 686–695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teti DM and Gelfand DM (1991) Behavioral competence among mothers of infants in the first year: The mediational role of maternal self-efficacy. Child Development 62: 918–929. [DOI] [PubMed] [Google Scholar]
- Thompson AL, Adair LS and Bentley ME (2013) Pressuring and restrictive feeding styles influence infant feeding and size among a low-income African-American sample. Obesity 21: 562–571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thompson AL and Bentley ME (2013) The critical period of infant feeding for the development of early disparities in obesity. Social Science & Medicine 97: 288–296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tsai TI, Huang SH and Lee SY (2015) Maternal and hospital factors association with first-time mothers’ breastfeeding practice: A prospective study. Breastfeeding Medicine 10: 334–340. [DOI] [PubMed] [Google Scholar]
- Wasser HM, Thompson AL, Suchindran CM, et al. (2017) Family-based obesity prevention for infants: design of the “Mothers & Others” randomized trial. Contemporary Clinical Trials 60: 24–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whittemore R, Chao A, Jang M, et al. (2014) Methods for knowledge synthesis: an overview. Heart &Lung 43: 453–461. [DOI] [PubMed] [Google Scholar]
- Willis TA, George J, Hunt C, et al. (2014) Combating child obesity: impact of HENRY on parenting and family lifestyle. Pediatric Obesity 9: 339–350. [DOI] [PubMed] [Google Scholar]
- Wittkowski A, Garrett C, Calam R, et al. (2017) Self-report measures of parental self-efficacy: a systematic review of the current literature. Journal of Child &Family Studies 26: 2960–2978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization (2016) Infant and young child feeding. Available at: http://who.int/mediacentre/factsheets/fs342/en/ (accessed 18 October 2017).
- World Health Organization (2017) Childhood overweight and obesity. Available at: http://www.who.int/dietphysicalactivity/childhood/en/ (accessed 15 December 2017).
- Wu DS, Hu J, McCoy TP, et al. (2014) The effects of breastfeeding self-efficacy intervention on short-term breastfeeding outcomes among primiparous mothers in Wuhan, China. Journal of Advanced Nursing 70: 1837–1879. [DOI] [PubMed] [Google Scholar]
- Xu H, Wen LM, Rissel C, et al. (2013) Parenting style and dietary behaviour of young children. Findings from the Healthy Beginnings Trial. Appetite 71: 171–177. [DOI] [PubMed] [Google Scholar]
- Yang X, Gao LL, Ip WY, et al. (2016) Predictors of breast feeding self-efficacy in the immediate postpartum period: a cross-sectional study. Midwifery 41: 1–8. [DOI] [PubMed] [Google Scholar]
- Zhang J, Shi L, Chen D, et al. (2009) Using the theory of planned behavior to examine effectiveness of an educational intervention on infant feeding in China. Preventative Medicine 49: 529–534. [DOI] [PubMed] [Google Scholar]