

Abstract
Objective
To evaluate the influence of Nordic walking (NW) on hip joint loads in order to determine whether it can be safely performed during postoperative physiotherapy in patients after orthopeadic surgery of the hip.
Methods
Internal hip joint loads were directly measured in vivo in 6 patients using instrumented hip prostheses during NW and ordinary walking (OW). All patients received training in two different NW techniques (double-poling and the diagonal technique) by a certified NW instructor. Measurements were conducted on a treadmill at a speed of 4 km/h on level ground, at 10% inclination and at 10% slope as well as on a level lawn at a self chosen comfortable speed. Resultant contact force (Fres), bending moment (Mbend) and torsional torque (Mtors) were compared between NW and OW as well as between both NW techniques.
Results
Joint loads showed a double peak pattern during all setups. Neither NW technique significantly influenced hip joint loads at the time of the first load peak during contralateral toe-off (CTO), which was also the absolute load peak, in comparison to OW. Compared to OW, double-poling significantly reduced Fres and Mbend at the time of the second load peak during the contralateral heel strike (CHS) on level ground both on the treadmill (− 6% and − 7%, respectively) and on the lawn (− 7% and − 9%). At 10% inclination, the diagonal technique increased Fres and Mbend at CHS (by + 6% and + 7%), but did not increase the absolute load peak at CTO.
Conclusion
Joint loads during NW are comparable to those of OW. Therefore, NW can be considered a low-impact activity and seems to be safe for patients that are allowed full weight bearing, e.g. during postoperative rehabilitation after THA.
Introduction
Loading of the musculoskeletal system and joints plays a fundamentdal role in a wide variety of orthopaedic conditions, e.g. regarding osteoarthritis, fractures or after orthopaedic surgery [1]. Mechanical stress of the joints is regarded as an important factor contributing to the development of osteoarthritis, and excessive joint loads may increase the risk of complications such as implant failure, aseptic lossening or implant wear after arthroplasty or internal fixation of fractures [1–7].
Osteoarthritis of the hip joint is among the most common orthopaedic conditions and often results in the necessaity of a total hip arthroplasty (THA) for affected patients [8, 9]. The average age of patients receiving THA surgery has been steadily decreasing during the last years and especially for younger patients, the ability to resume sports is one of the key aims after surgery [10–12]. This has lead to an increase in physical activity of the average patient after joint replacement and thereby also to higher functional demands of the THA [13, 14]. However, there are no evidence based guidelines regarding the return to sports after such surgery, and recommendations regarding the adequate amount and type of physical activity diverge [10, 15]. While excessive sport might lead to accelerated wear, loosening or even fractures, a certain level of physical activity certainly improves quality of life, reduces diverse health risks (e.g. obesity) and may strengthen the muscles supporting the hip joint [16–19]. High impact sports are generally considered to bear the highest risks whereas commonly recommended activities are those that ensure a mobility of the joint, but are not suspected to cause high peak loads, such as cycling aquatic excercice, or Nordic walking (NW) [19–24]. NW has been shown to be effective as cardiovascular training, even though it doesn’t cause a perceived difference in exertion rate compared to ordinary walking [25, 26]. Despite the increase in energy consumption during NW, the ground reaction forces, which were used to calculate the acting joint loads indirectly, have even been reported to be reduced in comparison to ordinary walking as the impact disperses when the poles strike the ground [27]. Such combination of effective cardiovascular training and potentially decreased joint loads would make NW an ideal option for patients with osteoarthritis or after orthopaedic surgery like arthroplasty or fracture fixation.
However, available studies investigating the loads on the musculoskeletal system during NW came to conflicting conclusions as to whether NW increases or decreases joint loads and are all based solely on the measurement of the individual ground reaction forces using force plates or instrumented insoles [28–36]. Using such methods, internal joint loads can only be indirectly estimated through musculoskeletal models [37–40]. A novel approach to directly assess the internal forces is the use of instrumented hip implants, which are able to directly measure in vivo forces and moments in the joint [41–43]. This method has already been used successfully to evaluate other methods of hip joint reduction [21, 44].
The aim of the present study was to clarify the influence of NW on hip joint loads using direct in vivo measurements and to evaluate if NW is an appropriate physical activity for patients after orthopedic surgeries of the hip. For this purpose, we used instrumented hip implants to evaluate in vivo hip joint loads during NW and to compare them to joint loads during ordinary walking. Our hypothesis was that NW does not increase hip joint loads in comparison to ordinary walking and is therefore an ideal option for postoperative physiotherapy after orthopaedic surgeries like THA.
Material and methods
Instrumented implants
An already described instrumented hip endoprosthesis was used for in vivo measurements of joint loads [43]. It allows to determine the resultant joint force components Fx, Fy and Fz as well as the moment components Mx, My and Mz with a possible measuring error of 1–2% [44]. These force components were subsequently used to calculate the resultant contact force Fres acting relative to at the femoral head, the bending moment Mbend acting in the middle of the femur neck, which quantifies most of the stress in the implant neck, as well as the torsion torque Mtors in the bone-stem-interface respectively in femur shaft axis, which may influence the initial torsional stability of cementless implants in the femur, based on a coordinate system centered at the head of a right side implant (Fig. 1) [45].
Fig. 1.
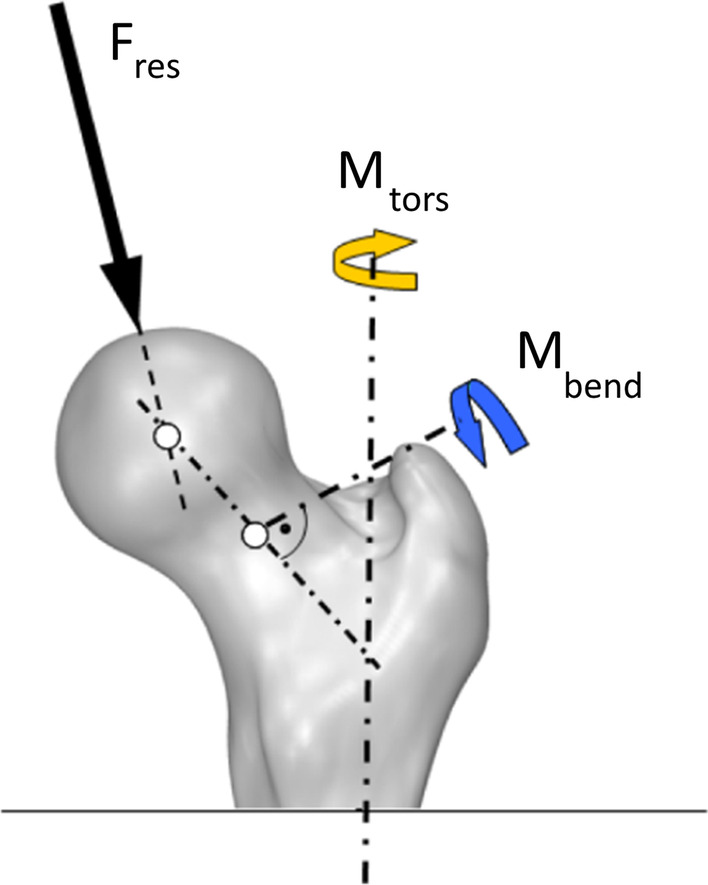
Localisation and direction of the parameters resultant contact force Fres, torsional moment Mtors and bending moment Mbend
Subjects
Six patients with an instrumented hip prosthesis were willing to participate and are included in this study (Table 1). All patients underwent hip replacement surgery using using the direct lateral approach These patients are part of a worldwide unique collective of 10 patients with instrumented implants (all of which were asked to participate in the present study) and have already participated in other previously published studies [21, 24, 45–52]. The measurements were performed between 8 and 32 months after surgery. In all patients, the indication for the THA had been osteoarthritis and all of them were NW novices.
Table 1.
Subjects participating
| Participant | Gender | Age* (years) | Weight* (kg) | Height* (cm) | BMI* (kg/m2) | Time since surgery* (months) | Pole length (cm) |
|---|---|---|---|---|---|---|---|
| H2R | M | 64 | 80 | 172 | 27 | 32 | 118 |
| H5L | W | 64 | 87 | 168 | 30.8 | 24 | 118 |
| H6R | M | 69 | 86 | 176 | 27.8 | 17 | 120 |
| H7R | M | 54 | 92 | 179 | 28.7 | 19 | 123 |
| H8L | M | 56 | 86 | 178 | 27.1 | 14 | 123 |
| H9L | M | 54 | 118 | 181 | 36.3 | 8 | 120 |
| MW ± STD | 60 ± 6 | 91 ± 14 | 176 ± 5 | 30 ± 3 | 19 ± 8 | 120 ± 2 |
*on the day of the measurements
In vivo load measurements
For all in vivo load measurements, the same NW Poles (Flash Vario®, model 2012, Leki, Kirchheim, Germany) were used. The standard length of the poles was 120 cm, but could be individually adapted by ± 5 cm to fit the patients’ proportions (Table 1).
The in vivo load data were collected during walking and NW on a level lawn at self-chosen speed as well as during treadmill walking on level ground with 4 km/h. Furthermore, the in vivo loads were determined at ordinary walking respectively NW with 10% inclination and with 10% slope at 4 km/h. For each measurement two different NW techniques, the diagonal technique and double-poling, were performed (Fig. 2) and the resultant in vivo joint loads were examined in comparison to ordinary walking without poles.
Fig. 2.

Nordic Walking techniques (referring to the right leg)
For the diagonal technique, each arm comes forward together with the contralateral leg and the pole is put onto the ground around the same time as the contralateral heel. For the double-poling technique, both poles come forward together with the same leg and are put onto the ground at the same time, either in a 2:1 or a 3:1 rhythm. In our study, a 2:1 rhythm was performed in which the NW poles always touched the ground at the same time as the heel of the ipsilateral leg.
As none of the participants had prior experience with NW, each received an individual instruction by a licensed NW instructor before the measurements. Additionally, all measurements were performed under the guidance of the same instructor as well. Selected trials of each measurement are published and can be downloaded at the public data base www.OrthoLoad.com. After familiarization, around 30 steps were measured for each setup and patient, which were averaged first individually and then for the whole cohort.
Data collection and evaluation
During the in vivo load measurements, all patients were filmed continually and simultaneously the in vivo data from the instrumented prostheses were stored on the same ditigital video tape. Details regarding the methods and the external measurement system have already been described previously [53].
The in vivo determined time-load patters of each patient were averaged intra-individually and separately for each walking technique using a time warping method [54]. Subsequently, an inter-individual average was calculated for each load component based on the individual averages to determine time load patterns of an average subject for each walking techniques. Peak loads at characteristic time points were determined for each load component. All in vivo measured forces and moments were given as percent of the bodyweight %BW respectively %BWm.
Statistical analysis was performed using IBM SPSS Statistics 20.0/21.0 (New York, USA). Non-parametric Wilcoxon Test was used to compare the mean values with respect to the different setups. The significance level was set to p ≤ 0.05.
Results
Walking on a level lawn
In the first part of the in vivo load measurement the participants walked on a level lawn with and without NW poles at a self-chosen comfortable speed (Table 2). On average, the patients walked faster when using NW poles than when walking without. The difference in walking speed between NW and ordinary walking varied inter-individually between + 1.1 and − 0.26 km/h.
Table 2.
Walking speed during ordinary walking and Nordic walking (NW) on a lawn with two different techniques
| Ordinary walking (km/h) | NW-diagonal (km/h) | NW-double-poling (km/h) | |
|---|---|---|---|
| H2R | 4.06 | 4.54 | 3.80 |
| H5L | 4.73 | 4.60 | 4.81 |
| H6R | 3.71 | 4.81 | 4.79 |
| H7R | 4.62 | 4.75 | 4.47 |
| H8L | 3.97 | 4.00 | 4.35 |
| H9L | 5.04 | 5.25 | 5.55 |
| Mean | 4.35 | 4.66 | 4.63 |
The in vivo measured joint loads Fres and Mbend show a double-peaked pattern that is characteristic for walking (Fig. 3). The first maximum occurs at the time of contralateral toe-off (CTO) and is followed by a second maximum at the time of contralateral heel strike (CHS). Mtors shows a clear maximum corresponding to the first maxima of Fres and Mbend at CTO. Overall the curves show similar patterns for ordinary walking and the two NW techniques.
Fig. 3.

Hip joint loads during walking on level lawn
Absolute averaged peak loads for each parameter occurred at CTO with 323%BW for Fres, 4.06%BWm for Mbend and 3.3%BWm for Mtors, whereas joint loads at CHS were lower with 267%BW for Fres and 4.01%BWm for Mbend (values for ordinary walking). For all three examined parameters the overall highest joint loads were observed during NW using the diagonal technique at the time of contralateral toe off (CTO), with on average 343%BW for Fres, 4.22%BWm for Mbend and 3.44%BWm for Mtors. NW with either technique did not have a significant influence on absolute peak joint loads at CTO compared to ordinary walking. Double-poling NW technique resulted in the overall lowest joint loads with 309%BW (CTO) and 248%BW (CHS) for Fres, 3.92%BWm (CTO) and 3.66%BWm (CHS) for Mbend, and 3.32%BWm for Mtors. Double-poling significantly reduced the second (lower) maxima for both Fres and Mbend by − 7% and − 9% compared to ordinary walking (Table 3). The respective first (higher) maxima showed a trend towards a load reduction for double-poling, while Mtors does not change relevantly.
Table 3.
Averaged in vivo measured hip joint loads during ordinary walking and Nordic Walking
| Fres | Mbend | Mtors | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Max (%BW) | Δ (%) | p | 2. Max (%BW) | Δ (%) | p | 1. Max (%BWm) | Δ (%) | p | 2. Max (%BWm) | Δ (%) | p | Abs_max (%BWm) | Δ (%) | p | |
| Ordinary walking | |||||||||||||||
| Level lawn | 323 ± 45 | 267 ± 39 | 4.06 ± 00.8 | 4.01 ± 0.6 | 3.30 ± 0.4 | ||||||||||
| Level ground (treadmill) | 300 ± 39 | 263 ± 35 | 3.89 ± 0.8 | 3.73 ± 0.6 | 2.54 ± 0.4 | ||||||||||
| 10% Inclination | 319 ± 40 | 242 ± 38 | 3.99 ± 0.8 | 3.41 ± 0.5 | 3.32 ± 0.5 | ||||||||||
| 10% Slope | 335 ± 41 | 253 ± 39 | 4.29 ± 0.7 | 3.58 ± 0.6 | 3.38 ± 0.6 | ||||||||||
| Diagonal technique | |||||||||||||||
| Level lawn | 343 ± 52 | + 6 | 0.173 | 276 ± 35 | + 3 | 0.058 | 4.22 ± 0.9 | + 4 | 0.463 | 4.19 ± 0.5 | + 5 | 0.116 | 3.44 ± 0.6 | + 4 | 0.463 |
| Level ground (treadmill) | 308 ± 48 | + 3 | 0.115 | 267 ± 37 | + 1 | 0.463 | 3.91 ± 1 | + 1 | 0.753 | 3.94 ± 0.6 | + 6 | 0.116 | 2.62 ± 0.5 | + 3 | 0.249 |
| 10% Inclination | 328 ± 43 | + 3 | 0.463 | 256 ± 35 | + 6 | 0.028 | 4.03 ± 0.76 | + 1 | 0.917 | 3.64 ± 0.6 | + 7 | 0.026 | 3.12 ± 0.7 | − 6 | 0.173 |
| 10% Slope | 340 ± 45 | + 2 | 0.600 | 259 ± 33 | + 2 | 0.141 | 4.29 ± 0.68 | 0 | 0.753 | 3.63 ± 0.6 | + 1 | 0.463 | 3.46 ± 0.5 | + 2 | 0.600 |
| Double-poling | |||||||||||||||
| Level lawn | 309 ± 50 | − 4 | 0.046 | 248 ± 37 | − 7 | 0.028 | 3.92 ± 0.9 | − 3 | 0.344 | 3.66 ± 0.5 | − 9 | 0.028 | 3.32 ± 0.6 | + 1 | 0.753 |
| Level ground (treadmill) | 297 ± 36 | − 1 | 0.674 | 247 ± 28 | − 6 | 0.043 | 3.83 ± 0.9 | − 1 | 0.463 | 3.48 ± 0.5 | − 7 | 0.046 | 2.69 ± 0.5 | + 6 | 0.400 |
| 10% Inclination | 313 ± 51 | − 2 | 0.600 | 249 ± 46 | + 3 | 0.600 | 3.83 ± 0.86 | − 4 | 0.075 | 3.32 ± 0.6 | − 3 | 0.249 | 3.13 ± 0.8 | − 5 | 0.463 |
| 10% Slope | 325 ± 41 | − 3 | 0.141 | 242 ± 39 | − 4 | 0.249 | 4.15 ± 0.64 | − 3 | 0.345 | 3.38 ± 0.6 | − 6 | 0.116 | 3.44 ± 0.6 | + 2 | 0.832 |
Fres: resultant contact force; Mbend: bending moment; Mtors: torsional moment; Δ: relative difference compared to ordinary walking at the same situation (level, inclination and slope); p: p value for the comparison of joint loads with ordinary walking
Treadmill walking on level ground at 4 km/h
For treadmill walking on level ground at 4 km/h, Fres and Mbend also show the double-peaked pattern that is characteristic for walking. The absolute peak joint loads during ordinary walking on treadmill with 4 km/h were on average 300%BW for Fres, 3.89%BWm for Mbend and 2.54%BWm for Mtors (Table 3). This equals a reduction of joint forces of − 7.1% for Fres, − 4.2% for Mbend and − 23% for Mtors compared to walking on a lawn.
Overall the curves show a similar pattern for ordinary walking and the two NW techniques. Neither of the two NW techniques significantly influenced the absolute peak loads at CTO. NW using the diagonal technique shows a trend towards increased joint loads, which is most pronounced for Mbend at CHS with + 6%, but does not reach significance level (Table 3). Double-poling significantly reduces the second (lower) peak at CHS of Fres by − 6% and Mbend by − 7%, but shows a trend towards an increase in Mtors of + 6%.
Walking with inclination and slope on a treadmill at 4 km/h
Walking with inclination and slope showed the same double-peaked pattern for Fres and Mbend as walking on level ground, both for ordinary walking and for NW. However, the first maximum (at CTO) increased for both parameters by up to + 11.7% (ordinary walking, Fres) and + 10.3% (ordinary walking, Mbend) at a 10% slope compared to walking on a level treadmill. For all three examined parameters (Fres, Mbend and Mtors), the highest joint loads were observed at the time of CTO using the diagonal technique at 10% slope with 340%BW for Fres, 4.29%BWm for Mbend and 3.46%BWm for Mtors. NW with either technique did not significantly change absolute peak joint loads at CTO compared to ordinary walking. Using the diagonal technique at 10% inclination significantly increased the second maxima (at CHS) of both Fres by + 6% and Mbend by + 7%, compared to ordinary walking with 10% inclination. For a slope of 10%, the in vivo hip joint loads for the diagonal technique did not significantly differ from ordinary walking with the same slope. Double-poling did not significantly change any of the examined joint loads at 10% inclination or at 10% slope in comparison to ordinary walking.
Comparison of joint loads between diagonal technique and double-poling (all setups)
When comparing in vivo joint loads between both NW techniques, diagonal versus double poling, Fres and Mbend show a general trend towards higher values for the diagonal technique (Table 4). The highest differences were observed during walking on a level lawn, where double-poling significantly reduced the absoluted peak of Fres at CTO compared to the diagonal technique. Additionally, it significantly reduced Fres at CHS by − 10% and Mbend at CHS by − 13% on a level lawn. There were no significant differences between both techniques regarding Mtors.
Table 4.
Percentual differences in hip joint loads between diagonal technique and double-poling
| Fres | Mbend | Mtors | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Max | 2. Max | 1. Max | 2. Max | Absolute maximum | ||||||
| Δ (%) | p | Δ (%) | p | Δ (%) | p | Δ (%) | p | Δ (%) | p | |
| Level ground | − 4 | 0.141 | − 7 | 0.028 | − 2 | 0.345 | − 12 | 0.028 | − 3 | 0.600 |
| 10% Inclination | − 5 | 0.249 | − 3 | 0.345 | − 5 | 0.046 | − 9 | 0.028 | 0 | 0.600 |
| 10% Slope | − 4 | 0.116 | − 7 | 0.075 | − 3 | 0.172 | − 7 | 0.046 | − 1 | 0.345 |
| Lawn | − 10 | 0.028 | − 10 | 0.028 | − 7 | 0.116 | − 13 | 0.028 | − 3 | 0.753 |
Differences are presented in relation to the values of the diagonal technique. Fres: resultant contact force; Mbend: bending moment; Mtors: torsional moment
Discussion
In this study we examined hip joint loads in vivo during ordinary walking and NW at different inclinations and using two different NW techniques. The aim was to clarify the influence of NW on hip joint loads and to determine in vivo whether NW is an appropriate physical activity during postoperative rehabilitation in patients after orthopaedic surgery of the hip. For this purpose, we used instrumented implants to conduct direct measurements of the respective joint loads during NW in vivo. It should be noted that this is an important difference to most existing studies we compare our data to, as the majority of them calculate internal forces from external measurement using the musculoskeletal models [28–36]. Such mathematical models may come to different results since they rely on the measurement of external instead of intrinsicly generated forces.
Regarding the influence of NW on in vivo joint loads during level treadmill walking, neither of the two NW techniques lead to a significant increase in joint loads. The double poling technique resulted in a slight but significant decrease of joint contact Force Fres (− 6%) as well as the bending moment Mbend on the femur neck (− 7%) at the time of the contralateral heel strike respectively the second (lower) peak of the typical load pattern, while absolute peak loads at CTO were not significantly influenced. Similar results were observed for walking on a level lawn at self chosen velocity, where double poling also slightly, yet significantly reduced the second (lower) peak of both Fres and Mbend by − 7% and − 9%, respectively. The diagonal technique on the other hand showed a trend towards higher joint loads of + 3% for the absolute peak loads of Fres and Mtors, which however did not reach significance. It should be noted that the average walking velocity was 0.31 km/h (+ 7.1%) faster than for normal walking. This might explain the trend towards higher joint loads, as an increase of up to + 6% should be expected merely due to the higher walking speed [55]. From these results we conclude that NW on a level lawn using the diagonal technique does not relevantly increase hip joint loads. These results are in line with those from two previous studies, that reported either a slight reduction of joint forces or no difference in joint loads for NW on level ground [36, 56]. One study with 15 patients reported siginificantly higher lower extremity joint loads for NW compared to ordinary walking [57]. However, this study focused on the knee instead of the hip and was performed at a much higher walking speed than our study (7.2 km/h versus 4.4–4.7 km/h) [57].
Similar to walking on level ground, NW with either technique at 10% slope or 10% inclination did not significantly influence hip joint loads in vivo compared to ordinary walking under the same conditions. Our results showed an increase of the second (lower) peak (CHS) for Fres and Mbend at 10% inclination for the diagonal technique. However, the increases were overall moderate (≤ + 7%) and hardly affected the absolute peak loads, which occurred at the first maximum for both Fres and Mbend and only showed a trend towards an increase of ≤ + 3%. Since the peak loads were hardly influenced by NW, an elevated risk due to NW using the diagonal rechnique after orthopaedic surgery seems rather unlikely. To the best of our knowledge, this is the first study to examine the influence of NW on hip joint forces at inclined surfaces in vivo, so that a comparison to existing studies is difficult. The influence of NW on lower extremity joint forces during walking downhill has been examined by one other study so far, which used 3:1 double-poling at a slope of 25% [58]. This study reported a reduction of ground reaction forces and calculated knee joint loads of 12–25% for NW. Although we did not observe a significant reduction of joint forces for NW at 10% slope, our results confirm that NW does not lead to increased joint loads at 10% slope and can therefore safely be performed after THA. When comparing the two techniques, double-poling showed overall lower joint loads for both Fres and Mbend, ranging up to a difference of − 13% for Mbend at CHS and − 10% for Fres at CTO and CHS on a level lawn. Mtors did not significantly differ between the two techniques. These results suggest that in situations where the avoidance of elevated loads is particularly important, e.g. in the early postoperative phase after orthopaedic surgery, double-poling may be preferred over the diagonal technique. However, it needs to be kept in mind that we only examined forces of the ipsilateral leg, which is put onto the ground at the same time as the poles. No conclusion can be drawn regarding the influence of double-poling on the contralateral leg.
Overall, our results show that NW on level ground does not lead to a relevant increase in hip joint forces. Therefore, we suggest that NW can be safely performed on level ground or at moderate inclinations and slopes by any patient who is allowed ordinary walking with the same walking velocity, e.g. during postoperative rehabilitation after THA. The exact time at which full weight bearing is allowed depends on the circumstances of the surgery (e.g. primary THA vs. revision THA) and is usually decided by the surgeon. For routine primary THA, early full weight bearing has been reported to be safe and is becoming increasingly popular, so that NW could already be introduced in early postoperative stages as soon as patients are able to walk comfortably without crutches [59]. This is of particular interest as NW has been shown to be a good stimulus for the circulation through the use of upper body musculature [60]. Despite the resulting increase in energy expenditure, NW has been reported to cause no perceived difference in exertion rate, which may offer a very convenient way to start sports again after surgery or injury [26]. This is supported by the observations in our study as well as in published literature, where the patients’ self-chosen comfortable walking speed was faster for NW than for ordinary walking [27]. One study even reported NW to be superior to both strength training and home-based exercises for improving function in patients with hip osteoarthritis [61]. Therefore, NW also seems like an ideal option for younger patients that desire a fast return to physical activity after THA. Furthermore, NW has been shown to improve gait asymmetry [62]. Gait asymmetry occurs in patients with lower extremity osteoarthritis, often persists after THA and is suspected to be associated with accelerated implant wear, making its correction an important aim [63–65]. Even though NW seems generally safe, it should be noted that it might still lead to an elevated risk through postoperative disturbances of balance or the increase in walking speed that we observed compared to ordinary walking. A higher walking speed directly increases hip joint loads and might also increase the risk of falls [55]. Therefore, it seems advisable to only recommend NW once patients are able to comfortably walk without crutches and to remind them to carefully consider their walking speed.
Sports that are typically recommended for early postoperative physiotherapy include low-impact activities such as cycling and aquatic exercises [10, 15]. For dynamic aquatic exercises, a previous in vivo study using instrumented implants reported resultant joint forces in the hip joint of 280%BW [21]. These values are similar to those we observed for double-poling on a treadmill with level ground, where Fres was 297%BW. However, joint loads during aquatic exercises could be lowered considerably if only non-weight-bearing or weight-bearing activities were performed, with values of 106–155%BW. The effect of cycling on hip joint loads has been examined by another study, which reported resultant hip joint forces of 118%BW for an ergometer at 110 W [24]. Consequently, cycling on an ergometer as well aquatic exercises using non-weight-bearing and weight-bearing activities might be more suitable for patients with load reductions, whereas NW and dynamic aquatic exercises seem to be safe as soon as full weight-bearing is allowed.
Despite our efforts for a rigorous methodology, there are some limitations to our study. The patient cohort is rather small with six participants, five of them male. Larger studies with a more equal representation of male and female patients would be desirable to confirm our results, but are be difficult to realize due to the highly complex methodology. For the measurements on a level lawn, walking velocities were not standardized and each patient chose an individual comfortable walking velocity instead. However, the individual walking velocities only differed by up to − 0.8 or + 0.9 km/h from the respective average. Yet, we would like to underline that the walking speed only differed between the participants during walking on the lawn, while all other measurements were performed at the same fixed walking speed of 4 km/h for all participants. Treadmill walking at a defined walking velocity on the other hand may have been unfamiliar for some of the participants. All patients in this study were NW novices. This ensures a good applicability to patients looking for allowed activies after orthopedic surgeries, as the majority of these may not have previous NW experience. However, it is possible that joint loads would differ in a more experienced cohort. We suspect joint loads to rather decrease than increase in such patients, as more experience will likely lead to a more efficient technique. Furthermore, due to the use of instrumented implants for the in vivo load measurements, only patients with previous THA could be included. Even though it seems likely that the effects of NW on joint loads are similar in healthy patient, no definite conclusions can be drawn from our study.
Conclusion
The study presents for the first time in vivo hip joint loads during NW with two different techniques. These unique in vivo data suggest that NW on level ground and at moderate inclinations or slopes does not relevantly change hip joint loads compared to normal walking at the same conditions. Thus, NW at normal walking speed can be considered a low-impact sport and seems to be a safe postoperative activity for patients that are allowed full weight bearing. However, it should be kept in mind that NW is often performed at a higher walking speed than ordinary walking, which may cause increased joint loads.
Acknowledgements
This work is based on the master thesis of Simone Schuster at the Julius Wolff Institute. The study was supported by German Research Society (DA 1786/5-1), the German Federal Ministry of Education and Research (BMBF 01EC1905D, BMBF—workHealth, Subproject 3) and the OrthoLoadClub. Dr. Palmowski is participant in the BIH-Charité Junior Clinician Scientist Program funded by the Charité—Universitätsmedizin Berlin and the Berlin Institute of Health.
Authors’ Contributions
YP participated in the analysis and interpretation of data, drafted the manuscript, approved the submitted version and agrees both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work. SP participated in the interpretation of data, critically revised the manuscript, approved the submitted version and agrees both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work. SGS participated in the design of the work, acquisition, analysis and interpretation of data, critically revised the manuscript, approved the submitted version and agrees both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work. SH participated in the interpretation of data, critically revised the manuscript, approved the submitted version and agrees both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work. PD participated in the design of the work, the acquisition, analysis and interpretation of data, substantially revised the work, approved the submitted version and agrees both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work. All authors read and approved the final manuscript.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work was supported by German Research Society (DA 1786/5–1)) and the OrthoLoadClub.
Availability of data and materials
Selected trials of each measurement are published and can be downloaded at the public data base www.OrthoLoad.com.
Declarations
Ethics approval and consent to participate
The implantation and the study protocols were approved by the institutional review board of the Charité – Universitätsmedizin Berlin (EA2/057/09) and registered at the ‘German Clinical Trials Register’ (DRKS00000563). All patients gave written informed consent prior to participation in these studies, in which they agreed to implantation of the instrumented implants, in vivo load measurements and the publication of their images. All methods were performed in accordance with the relevant guidelines and regulations. The funders played no role in the design, conduct, or reporting of this study.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Yannick Palmowski, Email: yannick.palmowski@charite.de.
Srdan Popovic, Email: srdan.popovic@charite.de.
Simone G. Schuster, Email: simone_schuster@gmx.de
Sebastian Hardt, Email: sebastian.hardt@charite.de.
Philipp Damm, Email: philipp.damm@charite.de.
References
- 1.Buckwalter JA, Anderson DD, Brown TD, Tochigi Y, Martin JA. The roles of mechanical stresses in the pathogenesis of osteoarthritis: implications for treatment of joint injuries. Cartilage. 2013;4(4):286–294. doi: 10.1177/1947603513495889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dangsheng X. Friction and wear properties of UHMWPE composites reinforced with carbon fiber. Mater Lett. 2005;59(2–3):175–179. doi: 10.1016/j.matlet.2004.09.011. [DOI] [Google Scholar]
- 3.Mazzucucco D, Spector M. Effects of contact area and stress on the volumetric wear of ultrahigh molecular weight polyethylene. Wear. 2003;254(5–6):514–522. doi: 10.1016/S0043-1648(03)00135-2. [DOI] [Google Scholar]
- 4.Pietrabissa R, Raimondi M, Di Martino E. Wear of polyethylene cups in total hip arthroplasty: a parametric mathematical model. Med Eng Phys. 1998;20(3):199–210. doi: 10.1016/S1350-4533(98)00004-6. [DOI] [PubMed] [Google Scholar]
- 5.Seedhom BB, Wallbridge NC. Walking activities and wear of prostheses. Ann Rheum Dis. 1985;44(12):838–843. doi: 10.1136/ard.44.12.838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shen G, Zhang J, Fang F. In vitro evaluation of artificial joints: a comprehensive review. Adv Manuf. 2019;7(1):1–14. doi: 10.1007/s40436-018-00244-z. [DOI] [Google Scholar]
- 7.Phillips TW, Nguyen LT, Munro SD. Loosening of cementless femoral stems: a biomechanical analysis of immediate fixation with loading vertical, femur horizontal. J Biomech. 1991;24(1):37–48. doi: 10.1016/0021-9290(91)90324-G. [DOI] [PubMed] [Google Scholar]
- 8.Maradit Kremers H, Larson DR, Crowson CS, Kremers WK, Washington RE, Steiner CA, et al. Prevalence of total hip and knee replacement in the United States. J Bone Joint Surg Am. 2015;97(17):1386–1397. doi: 10.2106/JBJS.N.01141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. Lancet. 2007;370(9597):1508–1519. doi: 10.1016/S0140-6736(07)60457-7. [DOI] [PubMed] [Google Scholar]
- 10.Vu-Han T, Hardt S, Ascherl R, Gwinner C, Perka C. Recommendations for return to sports after total hip arthroplasty are becoming less restrictive as implants improve. Arch Orthop Trauma Surg. 2020;141:497–507. doi: 10.1007/s00402-020-03691-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Klug A, Gramlich Y, Hoffmann R, Pfeil J, Drees P, Kutzner KP. Trends in total hip arthroplasty in Germany from 2007 to 2016: What has changed and where are we now? Z Orthop Unfall. 2019;159:173–180. doi: 10.1055/a-1028-7822. [DOI] [PubMed] [Google Scholar]
- 12.Hoorntje A, Janssen KY, Bolder SBT, Koenraadt KLM, Daams JG, Blankevoort L, et al. The effect of total hip arthroplasty on sports and work participation: a systematic review and meta-analysis. Sports Med. 2018;48(7):1695–1726. doi: 10.1007/s40279-018-0924-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Crowninshield RD, Rosenberg AG, Sporer SM. Changing demographics of patients with total joint replacement. Clin Orthop Relat Res. 2006;443:266–272. doi: 10.1097/01.blo.0000188066.01833.4f. [DOI] [PubMed] [Google Scholar]
- 14.Meek RMD, Treacy R, Manktelow A, Timperley JA, Haddad FS. Sport after total hip arthroplasty: undoubted progress but still some unknowns. Bone Joint J. 2020;102-B(6):661–663. doi: 10.1302/0301-620X.102B6.BJJ-2020-0208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vogel LA, Carotenuto G, Basti JJ, Levine WN. Physical activity after total joint arthroplasty. Sports Health. 2011;3(5):441–450. doi: 10.1177/1941738111415826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kilgus DJ, Dorey FJ, Finerman GA, Amstutz HC. Patient activity, sports participation, and impact loading on the durability of cemented total hip replacements. Clin Orthop Relat Res. 1991;269:25–31. [PubMed] [Google Scholar]
- 17.Huch K, Muller KA, Sturmer T, Brenner H, Puhl W, Gunther KP. Sports activities 5 years after total knee or hip arthroplasty: the Ulm osteoarthritis study. Ann Rheum Dis. 2005;64(12):1715–1720. doi: 10.1136/ard.2004.033266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wylde V, Blom A, Dieppe P, Hewlett S, Learmonth I. Return to sport after joint replacement. J Bone Joint Surg Br. 2008;90(7):920–923. doi: 10.1302/0301-620X.90B7.20614. [DOI] [PubMed] [Google Scholar]
- 19.Kuster MS. Exercise recommendations after total joint replacement. Sports Med. 2002;32:433–445. doi: 10.2165/00007256-200232070-00003. [DOI] [PubMed] [Google Scholar]
- 20.Thiele K, Hube R. Hip arthroplasty with increased expectancy. Z Orthop Unfall. 2019;159:91–97. doi: 10.1055/a-1019-8053. [DOI] [PubMed] [Google Scholar]
- 21.Kutzner I, Richter A, Gordt K, Dymke J, Damm P, Duda GN, et al. Does aquatic exercise reduce hip and knee joint loading In vivo load measurements with instrumented implants. PLoS ONE. 2017;12(3):e0171972. doi: 10.1371/journal.pone.0171972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Berry DJ, Bozic KJ. Current practice patterns in primary hip and knee arthroplasty among members of the American Association of Hip and Knee Surgeons. J Arthroplast. 2010;25(6 Suppl):2–4. doi: 10.1016/j.arth.2010.04.033. [DOI] [PubMed] [Google Scholar]
- 23.Cherian JJ, Jauregui JJ, Banerjee S, Pierce T, Mont MA. What host factors affect aseptic loosening after THA and TKA? Clin Orthop Relat Res. 2015;473(8):2700–2709. doi: 10.1007/s11999-015-4220-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Damm P, Dymke J, Bender A, Duda G, Bergmann G. In vivo hip joint loads and pedal forces during ergometer cycling. J Biomech. 2017;60:197–202. doi: 10.1016/j.jbiomech.2017.06.047. [DOI] [PubMed] [Google Scholar]
- 25.Cebula A, Tyka AK, Tyka A, Palka T, Pilch W, Luty L, et al. Physiological response and cardiorespiratory adaptation after a 6-week Nordic walking training targeted at lipid oxidation in a group of post-menopausal women. PLoS ONE. 2020;15(4):e0230917. doi: 10.1371/journal.pone.0230917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Church TS, Earnest CP, Morss GM. Field testing of physiological responses associated with Nordic walking. Res Q Exerc Sport. 2002;73(3):296–300. doi: 10.1080/02701367.2002.10609023. [DOI] [PubMed] [Google Scholar]
- 27.Willson J, Torry MR, Decker MJ, Kernozek T, Steadman JR. Effects of walking poles on lower extremity gait mechanics. Med Sci Sports Exerc. 2001;33(1):142–147. doi: 10.1097/00005768-200101000-00021. [DOI] [PubMed] [Google Scholar]
- 28.Stief F, Kleindienst FI, Wiemeyer J, Wedel F, Campe S, Krabbe B. Inverse dynamic analysis of the lower extremities during Nordic walking, walking, and running. J Appl Biomech. 2008;24(4):351–359. doi: 10.1123/jab.24.4.351. [DOI] [PubMed] [Google Scholar]
- 29.Kleindienst FI, Michel KJ, Schwarz J, Krabbe B. Vergleich von kinematischen und kinetischen parameters zwischen den Bewegungsformen Nordic Walking, Walking und Laufen. Sportverletz Sportschaden. 2006;20:25–30. doi: 10.1055/s-2006-926592. [DOI] [PubMed] [Google Scholar]
- 30.Kleindienst FI, Stief F, Wedel F, Campe S, Krabbe B. Joint loading of lower extremities during Nordic walking compared to walking based on kinetic and kinematic data. In: Proceedings of the XXIV international symposium on biomechanics in sports. 2006.
- 31.Kleindienst FI, Michel KJ, Stief F, Wedel F, Campe S, Krabbe B. Vergleich der gelenkbelastung der unteren extremitäten zwischen den bewegungsformen Nordic walking, walking und Laufen mittels inverser dynamik. Dtsch Z Sportmed. 2007;58(4):105–111. [Google Scholar]
- 32.Hagen M, Hennig EM, Stieldorf P. Ground reaction forces, rearfoot motion and wrist acceleration in Nordic walking. In: Proceedings of the XXIV international symposium on biomechanics in sports. 2006. pp. 139–42.
- 33.Thorwesten L, Overhaus N, Rudack P, Völker K. Vergleichende plantare Druckverteilungsmessung beim Nordic Walking und Walking. Deutsche Zeitschrift für Sportmedizin. 2005;56(7/8):215. [Google Scholar]
- 34.Jöllenbeck T, Leyser D, Classen C, Mull M, Grüneberg C. Biomechanical loading of the lower extremities during Nordic walking—a field study. In: Proceedings of the XXIV international symposium on biomechanics in sports. 2006. pp. 624–7.
- 35.Jöllenbeck T, Leyser D, Classen C, Mull M, Grüneberg C. Nordic walking. Eine feldstudie über den mythos gelenkentlastung. Prävention und Rehabilitation. 2007;Symposiumsbericht Bad Sassendorf. 2006. pp. 399–405.
- 36.Koizumi T, Tsujiuchi N, Takeda M, Fujikura R, Kojima T. Load dynamics of joints in Nordic walking. Procedia Eng. 2011;13:544–551. doi: 10.1016/j.proeng.2011.11.2750. [DOI] [Google Scholar]
- 37.Delp SL, Anderson FC, Arnold AS, Loan P, Habib A, John CT, et al. OpenSim: open-source software to create and analyze dynamic simulations of movement. IEEE Trans Biomed Eng. 2007;54(11):1940–1950. doi: 10.1109/TBME.2007.901024. [DOI] [PubMed] [Google Scholar]
- 38.Seth A, Hicks JL, Uchida TK, Habib A, Dembia CL, Dunne JJ, et al. OpenSim: Simulating musculoskeletal dynamics and neuromuscular control to study human and animal movement. PLoS Comput Biol. 2018;14(7):e1006223. doi: 10.1371/journal.pcbi.1006223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Stansfield BW, Nicol AC, Paul JP, Kelly IG, Graichen F, Bergmann G. Direct comparison of calculated hip joint contact forces with those measured using instrumented implants. An evaluation of a three-dimensional mathematical model of the lower limb. J Biomech. 2003;36(7):929–936. doi: 10.1016/S0021-9290(03)00072-1. [DOI] [PubMed] [Google Scholar]
- 40.Moisio KC, Sumner DR, Shott S, Hurwitz DE. Normalization of joint moments during gait: a comparison of two techniques. J Biomech. 2003;36(4):599–603. doi: 10.1016/S0021-9290(02)00433-5. [DOI] [PubMed] [Google Scholar]
- 41.Bergmann G, Graichen F, Rohlmann A, Westerhoff P, Bender A, Gabel U, et al. Loads acting on orthopaedic implants. Measurements and practical applications. Orthopade. 2007;36(3):195–196. doi: 10.1007/s00132-007-1055-x. [DOI] [PubMed] [Google Scholar]
- 42.Bergmann G, Graichen F, Rohlmann A, Westerhoff P, Heinlein B, Bender A, et al. Design and calibration of load sensing orthopaedic implants. J Biomech Eng. 2008;130(2):021009. doi: 10.1115/1.2898831. [DOI] [PubMed] [Google Scholar]
- 43.Damm P, Graichen F, Rohlmann A, Bender A, Bergmann G. Total hip joint prosthesis for in vivo measurement of forces and moments. Med Eng Phys. 2010;32(1):95–100. doi: 10.1016/j.medengphy.2009.10.003. [DOI] [PubMed] [Google Scholar]
- 44.Damm P, Schwachmeyer V, Dymke J, Bender A, Bergmann G. In vivo hip joint loads during three methods of walking with forearm crutches. Clin Biomech (Bristol, Avon) 2013;28(5):530–535. doi: 10.1016/j.clinbiomech.2012.12.003. [DOI] [PubMed] [Google Scholar]
- 45.Bergmann G, Bender A, Dymke J, Duda G, Damm P. Standardized loads acting in hip implants. PLoS ONE. 2016;11(5):e0155612. doi: 10.1371/journal.pone.0155612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Angelini L, Damm P, Zander T, Arshad R, Di Puccio F, Schmidt H. Effect of arm swinging on lumbar spine and hip joint forces. J Biomech. 2018;70:185–195. doi: 10.1016/j.jbiomech.2017.09.011. [DOI] [PubMed] [Google Scholar]
- 47.Bergmann G, Bender A, Dymke J, Duda GN, Damm P. Physical activities that cause high friction moments at the cup in hip implants. J Bone Joint Surg Am. 2018;100(19):1637–1644. doi: 10.2106/JBJS.17.01298. [DOI] [PubMed] [Google Scholar]
- 48.Bergmann G, Kutzner I, Bender A, Dymke J, Trepczynski A, Duda GN, et al. Loading of the hip and knee joints during whole body vibration training. PLoS ONE. 2018;13(12):e0207014. doi: 10.1371/journal.pone.0207014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Damm P, Bender A, Duda G, Bergmann G. In vivo measured joint friction in hip implants during walking after a short rest. PLoS ONE. 2017;12(3):e0174788. doi: 10.1371/journal.pone.0174788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Damm P, Kutzner I, Bergmann G, Rohlmann A, Schmidt H. Comparison of in vivo measured loads in knee, hip and spinal implants during level walking. J Biomech. 2017;51:128–132. doi: 10.1016/j.jbiomech.2016.11.060. [DOI] [PubMed] [Google Scholar]
- 51.Damm P, Zonneveld J, Brackertz S, Streitparth F, Winkler T. Gluteal muscle damage leads to higher in vivo hip joint loads 3 months after total hip arthroplasty. PLoS ONE. 2018;13(1):e0190626. doi: 10.1371/journal.pone.0190626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Damm P, Bender A, Bergmann G. Postoperative changes in in vivo measured friction in total hip joint prosthesis during walking. PLoS ONE. 2015;10(3):e0120438. doi: 10.1371/journal.pone.0120438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Graichen F, Arnold R, Rohlmann A, Bergmann G. Implantable 9-channel telemetry system for in vivo load measurements with orthopedic implants. IEEE Trans Biomed Eng. 2007;54(2):253–261. doi: 10.1109/TBME.2006.886857. [DOI] [PubMed] [Google Scholar]
- 54.Bender A, Bergmann G. Determination of typical patterns from strongly varying signals. Comput Methods Biomech Biomed Eng. 2012;15(7):761–769. doi: 10.1080/10255842.2011.560841. [DOI] [PubMed] [Google Scholar]
- 55.Giarmatzis G, Jonkers I, Wesseling M, Van Rossom S, Verschueren S. Loading of hip measured by hip contact forces at different speeds of walking and running. J Bone Miner Res. 2015;30(8):1431–1440. doi: 10.1002/jbmr.2483. [DOI] [PubMed] [Google Scholar]
- 56.Hansen L, Henriksen M, Larsen P, Alkjaer T. Nordic walking does not reduce the loading of the knee joint. Scand J Med Sci Sports. 2008;18(4):436–441. doi: 10.1111/j.1600-0838.2007.00699.x. [DOI] [PubMed] [Google Scholar]
- 57.Kleindienst FI, Stief F, Wedel F, Campe S, Krabbe B. Joint loading of lower extremities during Nordic walking compared to walking based on kinetic and kinematic data 24. In: International symposium on biomechanics in sports 2006.
- 58.Schwameder H, Roithner R, Muller E, Niessen W, Raschner C. Knee joint forces during downhill walking with hiking poles. J Sports Sci. 1999;17(12):969–978. doi: 10.1080/026404199365362. [DOI] [PubMed] [Google Scholar]
- 59.Tian P, Li ZJ, Xu GJ, Sun XL, Ma XL. Partial versus early full weight bearing after uncemented total hip arthroplasty: a meta-analysis. J Orthop Surg Res. 2017;12(1):31. doi: 10.1186/s13018-017-0527-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Kukkonen-Harjula K, Hiilloskorpi H, Manttari A, Pasanen M, Parkkari J, Suni J, et al. Self-guided brisk walking training with or without poles: a randomized-controlled trial in middle-aged women. Scand J Med Sci Sports. 2007;17(4):316–323. doi: 10.1111/j.1600-0838.2006.00585.x. [DOI] [PubMed] [Google Scholar]
- 61.Bieler T, Siersma V, Magnusson SP, Kjaer M, Christensen HE, Beyer N. In hip osteoarthritis, Nordic walking is superior to strength training and home-based exercise for improving function. Scand J Med Sci Sports. 2017;27(8):873–886. doi: 10.1111/sms.12694. [DOI] [PubMed] [Google Scholar]
- 62.Kato N, Fukusaki C, Leetawesup K, Kadokura Y, Ishii N. Improvement in gait asymmetry during Nordic walking in patients with lower extremity osteoarthritis. J Phys Fitness Sports Med. 2020;9(2):65–73. doi: 10.7600/jpfsm.9.65. [DOI] [Google Scholar]
- 63.Hodt-Billington C, Helbostad JL, Vervaat W, Rognsvag T, Moe-Nilssen R. Criteria of gait asymmetry in patients with hip osteoarthritis. Physiother Theory Pract. 2012;28(2):134–141. doi: 10.3109/09593985.2011.574783. [DOI] [PubMed] [Google Scholar]
- 64.Mendiolagoitia L, Rodriguez MA, Crespo I, Del Valle M, Olmedillas H. Kinematic gait analysis after primary total hip replacement: a systematic review: gait after total hip replacement: a systematic review. Indian J Orthop. 2020;54(6):767–775. doi: 10.1007/s43465-020-00101-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Ardestani MM, Amenabar Edwards PP, Wimmer MA. Prediction of polyethylene wear rates from gait biomechanics and implant positioning in total hip replacement. Clin Orthop Relat Res. 2017;475(8):2027–2042. doi: 10.1007/s11999-017-5293-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Selected trials of each measurement are published and can be downloaded at the public data base www.OrthoLoad.com.