

Abstract
Background:
Among high school students, seniors report the highest levels of alcohol use and hazardous drinking. Technology-based interventions are a promising approach for reducing alcohol use among this age group.
Objectives:
This randomized controlled trial investigated the efficacy of the eCHECKUP TO GO, an online personalized feedback intervention, on reducing alcohol use among high school seniors across the academic year (ClinicalTrials.gov Identifier NCT03613818). Drinker risk status, with students classified as high- or low-risk drinkers based on baseline reports binge drinking, was examined as a moderator of intervention effects.
Method:
Participants (N = 311) were recruited from two high schools. Class periods were randomized to the intervention condition or an assessment-only control condition. Participants completed online surveys at baseline, 30-day, and 6-month assessments.
Results:
Intervention effects were moderated by drinker risk status. Among high-risk drinkers, those in the intervention condition reported a significant reduction in weekly drinking quantity and estimated blood alcohol concentration (eBAC) at the 30-day follow-up relative to students in the control condition. By 6 months, reductions in alcohol outcomes among high-risk students in the intervention condition were sustained, but high-risk students in the control condition also reported reductions in weekly drinking. In contrast, for eBAC, intervention effects were significantly greater among students in the intervention condition relative to the control condition at 6 months.
Conclusions:
Results support the efficacy of the eCHECKUP TO GO for decreasing short-term alcohol use among seniors who are high-risk drinkers and provide preliminary evidence that reductions are sustained across the academic year.
Keywords: alcohol, eCHECKUP TO GO, online intervention, personalized feedback, high school seniors
National data indicate that drinking escalates as students progress through high school, with seniors reporting the highest prevalence rates of alcohol use (58.5%) (Johnston et al., 2019). Among seniors, 30.2% report using alcohol in the past 30 days and 42.9% report being drunk at least once in their lifetime (Johnston et al., 2019). Further, 20.9% of seniors report binge drinking, defined as consuming 4/5 (female/male) drinks within a couple of hours on at least one day during the past 30 days (Center for Disease Control and Prevention [CDC], 2017). Additionally, hazardous drinking is more prevalent among older high school students, with the highest rates of risky drinking practices (i.e., drinking games) occurring among 17 – 19 year olds (Borsari et al., 2013; Zamboanga et al., 2016). Despite the need for alcohol interventions for high school seniors, a seminal review of alcohol preventive interventions concluded that the majority of research targets youth ages 10– 15, with limited research conducted with high school students aged 16 and older (Spoth et al., 2008). More recent reviews of the literature parallel these findings, indicating the majority of alcohol intervention research targets students in junior high school (Strøm et al., 2014) or their first two years of high school (Champion et al., 2013). These findings, coupled with the high rates of alcohol use reported by high school seniors, indicate it is important to identify effective alcohol interventions for this age group.
Technology-based alcohol interventions are a promising approach for high school seniors (Schinke et al., 2006). Research indicates likeability ratings on computer-delivered alcohol interventions are associated with decreases in alcohol use outcomes (Fordor et al., 2020). Technology-based interventions can also improve access and treatment fidelity, while reducing implementation costs (Lord & Marsch, 2011; Marsch et al., 2014). The eCHECKUP TO GO (San Diego State University Research Foundation, n.d.) is an online personalized normative feedback intervention categorized in the National Institute on Alcohol Abuse and Alcoholism (NIAAA) CollegeAIM as a highly effective, low cost intervention (NIAAA, 2015). The program was designed to reduce risk factors for alcohol use, increase protective behaviors, and help students make better decisions about their drinking. Because the eCHECKUP TO GO program is brief, can be disseminated to large groups of students within one class period, and is inexpensive ($1,075 per year for unlimited use), the program is well-suited for use as an alcohol intervention for high school seniors.
Although originally developed for college students, research indicates the eCHECKUP TO GO is a promising school-based intervention for high school students (Doumas et al., 2015). Research indicates high school seniors report high levels of program acceptability (i.e., user-friendliness and utility) (Doumas et al., 2020). Further, results from an initial randomized controlled trial examining the short-term (i.e., 6-week) efficacy of the eCHECKUP TO GO in reducing risk factors for alcohol use and alcohol use among high school seniors (drinkers and non-drinkers) indicate that students participating in the program reported a reduction in normative beliefs about peer drinking and positive alcohol expectancies relative to students in an assessment-only control condition (Doumas, Esp, Johnson, Trull, & Shearer, 2017). Further, among students in the same sample, intervention effects were demonstrated for typical drinking and heavy alcohol use, although these effects were limited to students classified as high-risk drinkers (e.g., reporting binge drinking at the baseline assessment) (Doumas, Esp, Flay, & Bond, 2017). Thus, preliminary research demonstrates intervention acceptability and positive short-term outcomes among high school seniors.
Although there is a growing body of literature supporting the efficacy of the eCHECKUP TO GO for high school seniors, studies are limited to short-term changes (i.e., 6-weeks post-intervention) in alcohol use (Doumas, Esp, Flay, & Bond, 2017). This study extends the literature by examining the efficacy of the eCHECKUP TO GO for high school seniors across the academic year (i.e., 30-day and 6-month follow-ups). The eCHECKUP TO GO is often delivered to all students as a universal prevention strategy (http://www.echeckuptogo.com/). Thus, we chose to implement the intervention with all seniors regardless of drinking status. Studies examining the implementation of the eCHECKUP TO GO with low-risk and high-risk drinkers based on reports of baseline binge drinking, demonstrate no adverse effects on students identified as low-risk drinkers, including non-drinkers (Doumas & Anderson, 2009; Doumas et al., 2011; Doumas Esp, Flay, & Bond, 2017; Walters et al., 2007). Further, research with high school students indicates that relative to traditional alcohol education, participation in the eCHECKUP TO GO program is associated with lower rates of drinking initiation (Hausheer et al., 2018). Thus, we also examined drinker risk status as a moderator of intervention effects. We hypothesized that students in the eCHECKUP TO GO condition would report greater reductions in alcohol use than those in the control condition at the 30-day follow-up and that these reductions would be sustained at 6-months. Additionally, we hypothesized intervention effects would be moderated by drinker risk status, with significant intervention effects for high-risk drinkers but not for low-risk drinkers.
Method
Research Design
This study evaluated the efficacy of the eCHECKUP TO GO with high school seniors using a randomized controlled design. Class periods were randomized to the eCHECKUP TO GO intervention condition or assessment-only control condition. We randomized by class period, rather than at the individual level, due to the preference of the schools for this procedure related to ease of implementation of the study procedures. Participants completed baseline, 30-day, and 6-month follow-up assessments online during class time. All study procedures were approved by the University Institutional Review Board and the School District Research Board.
Participants
Participants in the current study were high school seniors recruited from two urban high school in the Northwest (see Figure 1 for the participant flow diagram). Demographic characteristics for the two schools combined include reported gender of 49.8% female and 50.2% male and reported race/ethnicity of 78.8% White, 10.0% Hispanic, 3.8% African-American, 3.6% Asian, 1.0% American Indian, and 2.8% Other. Demographic information for the sample is provided in Table 1. No significant differences on any participant characteristics were found between the intervention and control conditions at baseline or between those with baseline assessments only compared with those who completed all three assessments.
Figure 1.
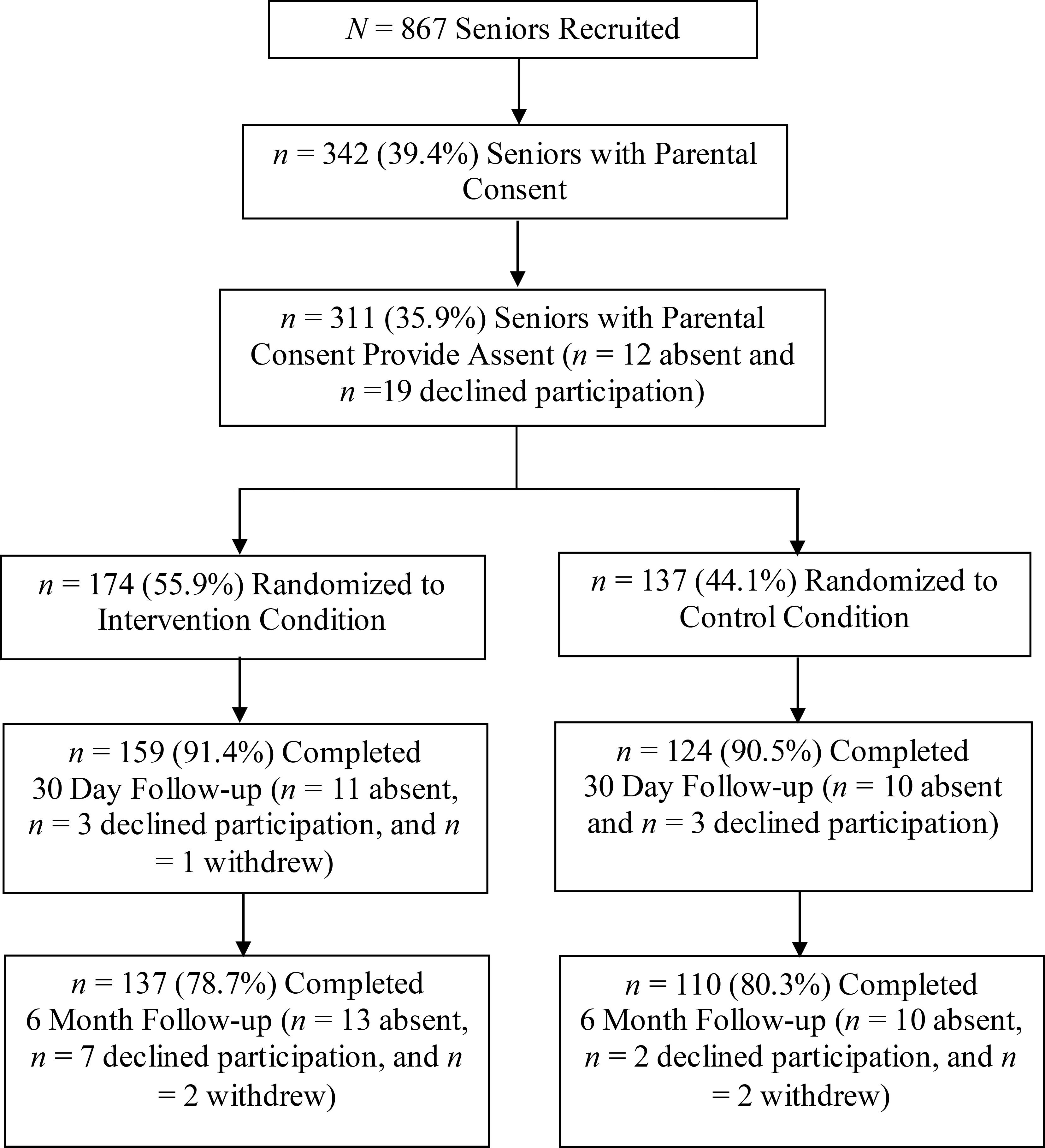
Participant Flow Diagram
Table 1.
Demographics by Study Group
| Demographics | Control Condition (n = 137) |
Intervention Condition (n = 174) |
Total Sample (N = 311) |
|---|---|---|---|
|
| |||
| Age in years, M (SD) | 17.13 (0.45) | 17.13 (0.46) | 17.13 (0.45) |
| Gender | |||
| Male | 46.7% | 42.2% | 44.2% |
| Female | 53.3% | 57.8% | 55.8% |
| Race/Ethnicity | |||
| White | 81.8% | 87.8% | 85.1% |
| Hispanic | 6.6% | 3.5% | 4.9% |
| Asian | 5.1% | 4.1% | 4.5% |
| African-American | 2.9% | 0.6% | 1.6% |
| American Indian/Alaska Native | 1.5% | 1.2% | 1.9% |
| Other | 2.1% | 1.7% | 4.6% |
Procedure
All seniors regardless of alcohol use (e.g., non-drinkers and drinkers) registered at the schools were eligible to participate. Recruitment occurred in the month of September. All parents of seniors were contacted by the schools via letter at their permanent addresses provided by the registrar’s office. A parental consent form and a project-addressed, stamped envelope were enclosed in the letter. Parents were asked to return signed consent forms indicating permission or decling permission for their adolescent to participate in the study. A phone number and email address were also provided for questions. Reminder letters were also sent to the student’s home address and sent home with the student to give to the parent. Due to University Internal Review Board requirements, active parental consent was required by all participants’ parents in order to engage in the study. Participants who received parental consent were recruited during English class, which is a common core course required for all seniors, and were asked to assent prior to participating in the baseline survey.
Class periods were randomly assigned to the eCHECKUP TO GO intervention or assessment-only control condition using a computer generated randomization table. Across the two schools, there were 14 periods; 7 periods were randomized to the intervention condition (56% of participants) and 7 periods were randomized to the control condition (44% of participants). Students with parental consent were taken to the school’s computer lab in the library to participate in the study in early October. A member of the research team described the research study and invited the students to participate. Students were given a unique personal identification number (PIN) to maintain confidentiality and a URL to access the baseline survey. Students then logged onto the survey website where they read a welcome screen explaining the research and were asked for their assent to participate. Once students gave assent by clicking “Agree”, they were taken to a screen that asked them to enter their PIN and were then directed to begin the baseline survey, which took approximately 20 minutes. Students without parental consent remained in their classroom with their teacher. Students with parental consent who did not provide assent were sent back to their classroom. After survey completion, students randomly assigned to class periods in the intervention condition completed the 30-minute online intervention; students randomly assigned to class periods in the control condition completed the 20 minute survey and then were sent back to their classrooms for the remaining 30 minutes of the period. All participants who completed the baseline survey were invited to participate in the 30-day and the 6-month follow-up surveys. Follow-up surveys took approximately 20 minutes to complete. We did not contact students who were absent from school on data collection days to complete surveys at any of the assessment points. Incentives included $100 deposited to the teachers’ school accounts for supplies and a bagel or pizza party after completion of the follow-up survey for classrooms that achieved a 60% or greater parental consent return rate. As parents were given the choice to agree or not agree to their teen’s participation on the consent form, the incentive was for the rate of return of the consent forms, not the rate of parents agreeing to their teen’s participation.
Measures
Demographics.
A brief demographic questionnaire designed for this study included basic participant characteristics (e.g., gender, race/ethnicity, age).
Weekly Drinking Quantity.
Weekly drinking quantity use was assessed using the Daily Drinking Questionnaire (DDQ; Collins et al., 1985). Participants were asked the question “Given that it is a typical week, please write the number of drinks you probably would have each day.” A response scale was provided for each day of the week (e.g., Monday__, Tuesday__, etc.). A drink was defined as “a 12-ounce can or bottle of beer, a 4-ounce glass of wine, a shot of distilled spirits or a shot in a mixed drink.” Weekly drinking was calculated by combining the reports for the seven days of the week.
Estimated Peak Blood Alcohol Concentration.
To assess estimated peak blood alcohol concentration (eBAC), we used the Widmark (1932/1981) formula which takes into account alcohol volume, hours of alcohol consumption, participant sex, and participant weight. Peak alcohol volume was assessed using the Quantity ⁄Frequency ⁄Peak Questionnaire (QFP; Dimeff et al., 1999; Marlatt et al., 1998). Participants were asked the questions “Think of the occasion when you drank the most in the past month. How much did you drink?” and “Think of the occasion you drank the most in the past month. How many hours did you spend drinking on this occasion?” We used participants’ report of peak alcohol volume and number of hours over which those drinks were consumed to calculate eBAC.
Classification of High-Risk vs. Low-Risk Drinkers.
We also asked participants to report on the frequency of binge drinking defined as having 3 or more drinks in a row for females and 5 or more for males in the past month. Although binge drinking is often defined as having 4 or more drinks in a row for females and 5 or more for males, the number of drinks used in this study to measure binge drinking was based on research by Donovan (2009) establishing cut-points for children and adolescents. Participants who reported one or more episodes of binge drinking in the past month (33.5%; 34.3% male and 32.9% female) were classified as high-risk drinkers. Of those classified as low-risk drinkers, 73.8% reported drinking no alcohol within the past month.
The eCHECKUP TO GO
The eCHECKUP TO GO is a 30-minute personalized normative feedback (PNF) intervention available through the San Diego State University Research Foundation (http://www.echeckuptogo.com/). The program is customized for the participating school, including providing school-specific normative data, referrals to the school counselor and the local community, and designing the website using school colors and logos. School-specific normative data was derived from surveys collected biennially by a local drug-free community coalition. The program consists of an online assessment followed by personalized feedback. The online assessment includes questions regarding basic demographic information and information on alcohol consumption, drinking behavior, alcohol-related consequences, and knowledge and beliefs about alcohol. Once all questions are completed, personalized feedback is given to participants via text, graphs, and video recordings embedded in the program. Feedback is provided in the following domains.
Drinking profile.
This section provides a summary of the student’s quantity and frequency of drinking. Personalized normative feedback is also provided for amount of drinking and blood alcohol concentration (BAC) relative to peers. A description of BAC is also provided, including how long it takes to sober up at the student’s BAC level and things that do not work to speed up the processing of alcohol. A personal BAC chart is also provided.
Cost of alcohol and tobacco.
This section includes pie graphs depicting the cost of alcohol and cigarettes. Comparisons are made to what other items could have been purchased with that money.
Physical costs of alcohol.
Feedback of the number of cheeseburgers that are equivalent to alcohol calories consumed is depicted graphically. The time it would take to “run off” the calories is also presented. The student’s responses and correct responses to a True/False “quiz” on physical performance (e.g., alcohol takes effect more quickly when mixed with carbonated/caffeinated beverages or mixers; drinking alcohol has little or no effect on the body’s ability to build muscle strength) are also presented.
Personal risk factors.
Graphical feedback is provided for the student’s personal risk score. The student’s risk of blackout, based on their estimated BAC, is also presented. Charts for tolerance level, family risk, and risk related to age of initiation of alcohol use are also graphically depicted. Other risks, such as drinking and driving consequences, are reported.
Normative comparisons.
Pie graph comparisons of perceptions of peer drinking and tobacco use to actual peer use are presented. Additionally, the percentage of students drinking more than the student respondent is also provided.
Strategies to reduce drinking.
During the feedback portion of the program, students are asked to respond whether or not they would be willing to engage in potential strategies to reduce drinking. Students are then given a list of strategies (e.g. avoid drinking games, space my drinks out over time, alternate alcoholic and non-alcoholic drinks) they have selected that they can use as steps to change their drinking.
Goals and aspirations.
A list of goals and ways to meet those goals are presented in the areas of health and fitness (e.g., spend more time at the gym, exercising or playing sports), relationships (e.g., feel more comfortable talking to people), career and life goals (e.g., spend more time studying), and self-esteem (e.g., feel more confident).
To ensure the standardized delivery of the eCHECKUP TO GO, a member of the research team followed an instruction script to read to the participants. A minimum of three research team members were present throughout the intervention to assist participants and serve as monitors, ensuring participants completed the program, kept their eyes on their own screens, and that there was no discussion among the participants.
Data Analyses
We examined all variables for outliers at baseline and follow-up assessments and outliers. Data points were considered outliers if they were greater than 3.3 SD above the mean for the whole sample and were adjusted downward to the value corresponding to 3.3 SD above the mean before conducting analyses (Tabachnik & Fidell, 2007). Across the two outcome variables and three time points, we adjusted less than 2% of the data points. One student was dropped from the intervention condition due to extreme responses that suggested non-compliance with the study. We examined differences in demographics and baseline outcomes between the intervention and control conditions and among those who completed all three assessments and less than three assessments, using t-tests for continuous variables and chi-square tests for categorical variables.
Study outcomes were fit with a linear mixed model with fixed effects of Time (baseline, 30-day, 6-months), Condition (intervention, control), and Risk Status (high, low). This approach is robust to incomplete data and uses all available data, complete or incomplete, provided data are missing at random (Stroup, 2013). Random effects were selected from the set of within-participants, within-period, and within-school (i.e., correlation of outcome measures within individual participants across time, participants within class periods, and participants within schools) using AICc under the restricted maximum likelihood algorithm (Burnham & Anderson, 1998), resulting in inclusion of within-participant and within-period as random effects in the analyses. Models were assessed for appropriateness using residual plots. While the data distribution was skewed due to the non-drinkers and low-risk drinkers in the sample, the inclusion of the risk status moderator allowed the model residuals to meet the key requirement of homoscedasticity. We did observe a larger variance for observations at baseline, so we included different overall variance components by time, which also improved AICc (Stroup, 2013).
Because our interest was in risk status as a moderator over time, we used the model to explicitly estimate the Time x Condition interaction separately for each risk status for each outcome from baseline to the 30-day follow-up and from baseline to the 6-month follow-up. Thus, prior to modeling, we identified specific contrasts of interest including the Time x Condition interaction for high-risk and low-risk drinkers from baseline to the 30-day follow-up and from baseline to the 6-month follow-up, regardless of the significance of the Time x Condition x Risk Status interaction. Because these were pre-planned comparisons, we did not adjust these p-values (Pagano, 2013; Sheskin 2011). We calculated model-based means and their differences after establishing significance, and used a Bonferroni step-up procedure (Hochberg, 1988) to control for the family-wise error rate for multiple comparisons. Specifically, we examined differences in pairs of means for the outcome variables between time points within the intervention and control conditions for high-risk and low-risk drinkers. These p-values are presented as padj. Analyses were considered significant at p < 0.05 and were conducted in SPSS version 25.0 and SAS version 9.4. R libraries tidyverse (Wickham et. al, 2019) and ggplot2 (Wickham, 2016) in RStudio (RStudio Team, 2020) were used to produce plots and present descriptive statistics.
Results
Preliminary Analyses
Descriptive statistics for the outcome variables by condition and risk status are presented in Table 2. Although there were no significant baseline differences between the intervention and control condition on weekly drinking, t(308) = −1.43, p = .15, students in the intervention condition reported significantly higher levels of eBAC, t(308) = −3.32, p = .001, compared to the control condition. Additionally, the percentage of high-risk drinkers was higher in the intervention condition than the control condition, χ2(1) = 9.86, p = .002. Baseline levels of weekly drinking, t(102) = 0.53, p = .60, and eBAC, t(102) = −0.88, p = .38, however, did not differ between students in the intervention or control condition among student in the high risk group. Regarding attrition, those who completed all three assessments did not differ from those who completed less than three assessments on eBAC, t (308) = 0.77, p = .44. However, for weekly drinking quantity, those who completed all three assessments reported significantly lower levels of weekly drinking compared to those who completed less than three assessments, t(308) = 2.22, p = .03.
Table 2.
Alcohol Use at Baseline and Follow-Ups by Study Condition and Drinker Risk-Status
| Drinker Risk-Status |
||||
|---|---|---|---|---|
| Low-Riska | High-Riskb | Total Samplec | ||
|
| ||||
| Outcomes | M (SD) | M (SD) | M(SD) | |
|
| ||||
| Weekly Drinking Quantityd | ||||
| Control | Baseline | 0. 98 (3.87) | 9.88 (7.86) | 3.06 (6.39) |
| 30-Day | 0.58 (2.04) | 9.29 (7.30) | 2.55 (5.32) | |
| 6-Month | 0.32 (1.14) | 7.76 (7.66) | 2.14 (5.04) | |
| Intervention | Baseline | 0.66 (1.86) | 9.14 (7.98) | 4.14 (6.74) |
| 30-Day | 0.59 (1.73) | 6.34 (6.02) | 2.92 (4.94) | |
| 6-Month | 0.51 (1.50) | 5.05 (4.97) | 2.23 (3.94) | |
| eBACe | ||||
| Control | Baseline | 0.01 (0.03) | 0.21 (0.13) | 0.06 (0.11) |
| 30-Day | 0.01 (0.03) | 0.18 (0.15) | 0.05 (0.11) | |
| 6-Month | 0.02 (0.05) | 0.22 (0.24) | 0.07 (0.15) | |
| Intervention | Baseline | 0.02 (0.03) | 0.24 (0.17) | 0.11 (0.16) |
| 30-Day | 0.02 (0.04) | 0.15 (0.12) | 0.07 (0.11) | |
| 6-Month | 0.03 (0.08) | 0.18 (0.18) | 0.09 (0.15) | |
Control Condition n = 104; Intervention Condition n = 102.
Control Condition n = 33; Intervention Condition n = 71.
Control Condition n = 137; Intervention Condition n = 173.
Range for weekly drinking is 0 – 26; 84.5% Low-Risk and 11.5% High-Risk score = 0.
Range for eBAC is 0 – .62; 76.3% Low-Risk and 0% High-Risk score = 0.
Alcohol Outcomes
Results from the overall statistical models and the specific comparisons for 30-day and 6-month follow-ups for high-risk and low-risk drinkers for weekly drinking quantity and eBAC are displayed in Table 3.
Table 3.
Mixed Model Analysis of Variance Results for Outcomes
| Source | Weekly Drinking Quantity | eBAC | ||
|---|---|---|---|---|
|
| ||||
| Random Effects (Variance Component Estimate) | ||||
| Student | 11.02 | 0.00 | ||
| Period | <.001 | <.001 | ||
| Residual Baseline | 14.67 | 0.01 | ||
| Residual 30-Days | 3.80 | 0.00 | ||
| Residual 6-Months | 6.44 | 0.01 | ||
| Fixed Effects | F-Value | Pr > F | F-Value | Pr > F |
| Condition | 4.30 | 0.09 | 0.09 | 0.78 |
| Time | 13.41 | <.001*** | 11.01 | <.001*** |
| Risk Status | 233.71 | <.001*** | 302.03 | <.001*** |
| Condition * Risk Status | 3.59 | 0.06 | 1.66 | 0.20 |
| Time * Risk Status | 8.57 | <.001*** | 11.41 | <.001*** |
| Time * Condition | 1.29 | 0.28 | 4.26 | 0.02* |
| Time * Condition * Risk Status | 2.02 | 0.13 | 4.48 | 0.01** |
| Specific Comparisons | F-Value | Pr > F | F-Value | Pr > F |
| Baseline to 30-Day | ||||
| Time * Condition * Risk Status | 4.03 | 0.05* | 7.30 | 0.007* |
| High-Risk Status: Time * Condition | 4.61 | 0.03* | 10.53 | <.001*** |
| Low-Risk Status: Time * Condition | 0.15 | 0.70 | 0.00 | 0.97 |
| Baseline to 6-Month | ||||
| Time * Condition * Risk Status | 2.31 | 0.13 | 5.42 | 0.02* |
| High-Risk Status: Time * Condition | 2.14 | 0.14 | 6.98 | 0.009** |
| Low-Risk Status: Time * Condition | 0.29 | 0.59 | 0.00 | 0.83 |
p < .05.
p < .01.
p < .001.
Weekly Drinking Quantity.
As seen in Table 3, for the overall model, the Time x Condition interaction effect (p = .28) and the Time x Condition x Risk Status interaction effect (p = .13) were not significant. Specific comparisons, however, revealed a significant Time x Condition x Risk Status interaction from baseline to the 30-day follow-up (p = .05) but not from baseline to the 6-month follow-up (p = .13). As seen in Figure 2, for high-risk drinkers, the Time x Condition interaction was significant from baseline to the 30-day follow-up (p = .03), demonstrating significantly greater reductions in weekly drinking in the intervention condition relative to the control condition. We did not, however, find a significant Time x Condition interaction effect from baseline to the 6-month follow-up (p = .14). Further comparisons examining pairs of means revealed that high-risk drinkers in the intervention condition reported significant reductions in weekly drinking from baseline to the 30-day follow-up (padj < .001) and from baseline to the 6-month follow-up (padj < .001), suggesting initial changes were sustained for students in the intervention condition. Those in the control condition, however, also demonstrated a decrease in weekly drinking from baseline to the 6-month follow-up (padj = .05), leading to non-significant interactions from baseline to the 6-month follow-up. For low-risk drinkers, the Time x Condition interaction was not significant from baseline to either the 30-day follow-up (p = .70) or the 6-month follow-up (p = .59), demonstrating no differences between low-risk drinkers in the intervention and control conditions over time (see Figure 2).
Figure 2. Weekly Drinking Quantity by Intervention Condition and Risk-Status.
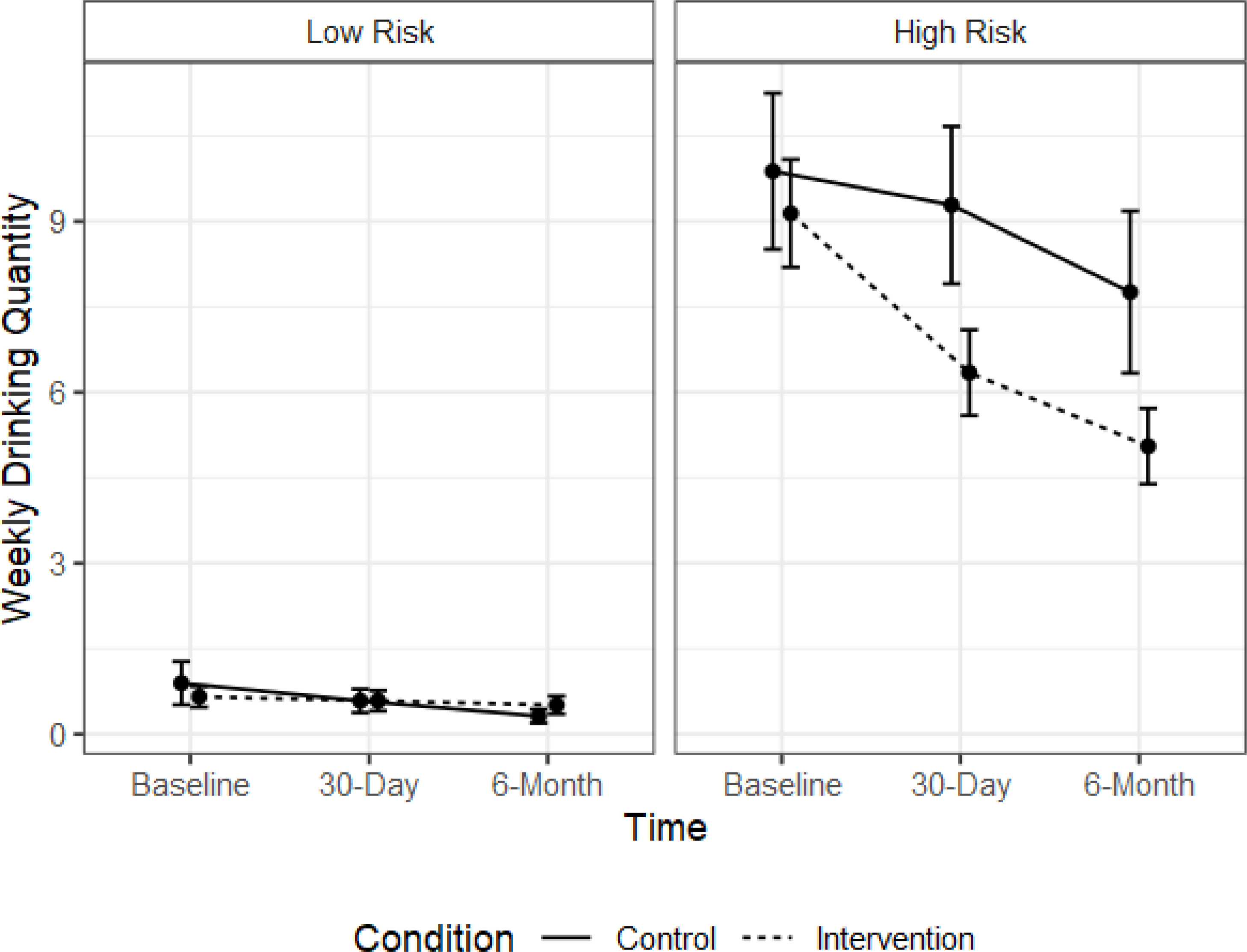
Note. This figure demonstrates model-based means (± 1 model-based standard error) for weekly drinking quantity. There are no significant differences in weekly drinking among low-risk participants. Among high-risk participants, students in the intervention condition reported greater reduction in weekly drinking compared to students in the control condition from baseline to the 30-day follow-up (p = .03), but not from baseline to the 6-month follow-up (p = .14). Follow-up analyses indicated that participants in the intervention condition reported significant reductions in weekly drinking from baseline to the 30-day follow-up (padj < .001) and from baseline to the 6-month follow-up (padj < .001). Participants in the control condition also reported significant reductions in weekly drinking from baseline to the 6-month follow-up (padj =.05).
eBAC.
As seen in Table 3, for the overall model, the Time x Condition interaction effect (p = .02) and the Time x Condition x Risk Status interaction effect (p = .01) were significant. Specific comparisons revealed a statistically significant interaction effect for Time x Condition x Risk Status interaction from baseline to the 30-day follow-up (p = .007) and from baseline to the 6-month follow-up (p = .02). As seen in Figure 3, for high-risk drinkers, the Time x Condition interaction was significant from baseline to the 30-day follow-up (p = .001) and from baseline to the 6-month follow-up (p = .009), demonstrating greater reductions in eBAC in the intervention condition relative to the control condition at both time points. Further comparisons examining pairs of means revealed that among high-risk drinkers, participants in the intervention condition had significant reductions in eBAC at the 30-day follow-up (padj < .001) and at the 6-month follow-up (padj = .002), indicating a sustained decrease in eBAC. There were no significant reductions in eBAC for the control condition from baseline to either the 30-day or 6-month follow-ups. For low-risk drinkers, the Time x Condition interaction was not significant from baseline to either the 30-day follow-up (p = .97) or the 6-month follow-up (p = .83), demonstrating no differences between low-risk drinkers in the intervention and control conditions over time (see Figure 3).
Figure 3. eBAC by Intervention Group and Risk-Status.
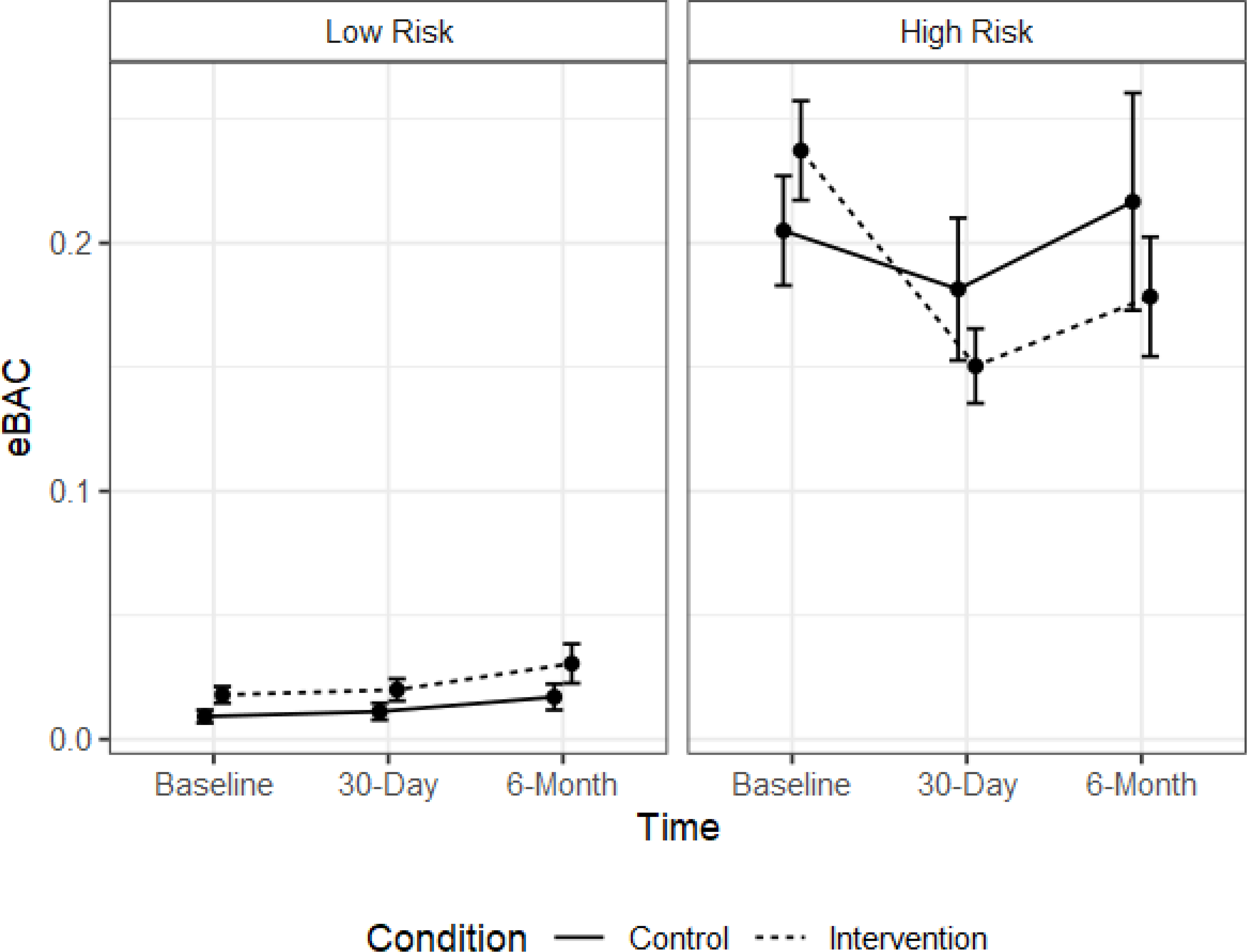
Note. This figure demonstrates model-based means (± 1 model-based standard error) for eBAC. There are no significant differences in eBAC among low-risk participants. Among high-risk participants, students in the intervention condition reported greater reduction in eBAC compared to students in the control condition from baseline to the 30-day follow-up (p = .001) and from baseline to the 6-month follow-up (p = .009). Follow-up analyses indicated participants in the intervention condition reported significant reductions in eBAC from baseline to the 30-day follow-up (padj < 0.001) and from baseline to the 6-month follow-up (padj = 0.002). There are no significant changes in eBAC among participants in the control condition.
Discussion
Results demonstrated several positive findings for students receiving the eCHECKUP TO GO intervention relative to those in the control condition. As hypothesized, intervention effects were moderated by risk status, such that high-risk students in the intervention condition reported a greater reduction in alcohol use relative to students in the control condition. These findings are consistent with studies demonstrating the short-term efficacy of the eCHECKUP TO GO in reducing alcohol use among high school seniors (Doumas, Esp, Flay, & Bond, 2017). Further, findings from the current study extend the literature by providing preliminary evidence for the efficacy of the e-CHECKUP TO GO for high school students across the academic year.
For weekly drinking quantity, intervention effects were limited to the baseline to 30-day follow-up period. Specifically, among high-risk students, at the 30-day follow-up we found a significant decrease in weekly drinking in the intervention condition relative to the control condition. However, intervention effects from baseline to the 6-month follow-up were not significant. Examination of the means suggests that within-condition changes in weekly drinking among students in the intervention condition were sustained, but students in the control condition also reported significant decreases in weekly drinking from baseline to the 6-month follow-up such that differences between the conditions were no longer significant. The pattern of means suggests that the eCHECKUP TO GO was effective in reducing weekly drinking, with reductions sustained at 6-months, but that students in the control condition seemed to “catch up” over the course of the academic year. One explanation for this finding is that there is a natural decrease in alcohol use from the fall to spring semester in high school students. Although national statistics suggest that alcohol use escalates through high school, peaking in the senior year (Johnston et al., 2019), we could find no study examining changes in alcohol use within the senior year. Thus, it is unclear if reductions in weekly drinking among the control condition represent a natural shift in alcohol use or if there is another explanation. For example, reductions in weekly drinking among control students may be related to contamination effects, such that as intervention students decreased their drinking, they created new drinking norms, thereby influencing alcohol use among students in the control condition.
For eBAC, intervention effects were evident at the 30-day follow-up and were sustained at the 6-month follow-up. Specifically, among high-risk students, we found a significant decrease in eBAC relative to the control condition at both the 30-day and 6-month follow-up assessments. Thus, short-term intervention effects between the two conditions were sustained across the academic year. It is unclear why we found sustained intervention effects for eBAC but not for weekly drinking. It is possible that even though students in the control condition reported a reduction in typical weekly drinking quantity at the 6-month follow-up, these students may continue to drink in a hazardous manner (i.e., high eBAC) when they do drink.
Similarly to the findings from prior research on the efficacy of the eCHECKUP TO GO with college students (Doumas & Anderson, 2009; Doumas et al., 2011) and high school seniors (Doumas Esp, Flay, & Bond, 2017), we did not find significant intervention effects for low-risk drinkers. Although this finding is likely due to a floor effect, results from the current study add to the existing literature demonstrating that students who do not drink or who are low-risk drinkers are not adversely affected by personalized normative feedback interventions. That is, we did not find evidence that low-risk drinkers increase their drinking in response to the intervention. This finding is important as the eCHECKUP TO GO intervention is often used as a universal prevention strategy, with schools disseminating the program to all students, including non-drinkers (http://www.echeckuptogo.com/).
Although this study adds to the literature by providing support for the efficacy of the eCHECKUP TO GO intervention for high school seniors, there are limitations. First, generalizability of the results is limited due to a relatively small sample with a predominantly White demographic makeup recruited from one region of the US. Future research with larger, more diverse samples is recommended. Second, our response rate of 35.8% is at the lower end of the 30% – 60% response rates typical of other studies using active parental consent (Smith et al., 2009). Research suggests that active parental consent yields lower response rates (Smith et al., 2009) and results in an underrepresentation of diverse students and male students (Unger et al., 2004) relative to passive parental consent. White participants and female participants were slightly over-represented in the study sample relative to the demographic make-up of the schools, suggesting that the demographic make-up of our sample may have been influenced by parental consent procedures. Adolescent self-reported alcohol use is also a limitation of this study. The reliability and validity of self-reported use for this age group, however, have been demonstrated, and self-report is common practice used in studies examining adolescent alcohol use (Flisher et al., 2004; Lintonen et al., 2004). Finally, we used an assessment-only control condition in this study. Because research indicates effect sizes are larger when brief interventions are tested against assessment-only control conditions rather than active comparison conditions (Carey et al., 2009), future research with high school seniors should examine the efficacy of the eCHECKUP TO GO using an active comparison condition that includes alcohol content.
Results of this study have important implications for providing intervention programs to reduce alcohol use among high school seniors. This study replicates earlier findings supporting the short-term efficacy of the eCHECKUP TO GO for high school seniors and suggests reduction in drinking are sustained throughout the academic year. Because high school seniors report the highest rates of alcohol use among high school students, identifying evidence-based programing for this age group is essential. Further, online programs are well-suited for school-based programs for this age group. The eCHECKUP TO GO is inexpensive, requires no training for intervention delivery, and is easy to disseminate to large groups of students within a class period. Thus, even schools with few resources can easily adopt the eCHECKUP TO GO and sustain program delivery.
Acknowledgments
The authors wish to thank Andrea Pikes, April Watts, Beverly Glouser, and Dayna Showalter for assistance with participant recruitment and data collection.
Declaration of Interest Statement: This study was registered with ClinicalTrials.gov (Identifier NCT03613818). We have no conflicts of interest to declare. This work was supported by the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health under Grant Number R21AA023880; Institutional Development Awards (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under Grants #P20GM103408 and P20GM109095. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We also acknowledge support from The Biomolecular Research Center at Boise State with funding from the National Science Foundation, Grants Number 0619793 and Number 0923535, the MJ Murdock Charitable Trust, and the Idaho State Board of Education.
References
- Carey KB, Scott-Sheldon LA, Elliott JC, Bolles JR, & Carey MP (2009). Computer-delivered interventions to reduce college student drinking: A meta-analysis. Addiction, 104(11), 1807–1819. 10.1111/j.1360-0443.2009.02691.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2017). Youth Risk Behavior Surveillance System (YRBSS). https://www.cdc.gov/healthyyouth/data/yrbs/index.htm
- Champion KE, Newton NC, Barrett EL, & Teesson M (2013). A systematic review of school-based alcohol and other drug prevention programs facilitated by computers or the Internet. Drug and Alcohol Review, 32(2), 115–123. 10.1111/j.1465-3362.2012.00517.x [DOI] [PubMed] [Google Scholar]
- Dimeff LA, Baer JS, Kivlahan DR, & Marlatt GA (1999). Brief Alcohol Screening and Intervention for College Students (BASICS): A harm reduction approach. New York: Guilford Press. [Google Scholar]
- Donovan JE (2009). Estimated blood alcohol concentrations for child and adolescent drinking and their implications for screening instruments. Pediatrics, 123(6), 975–981. 10.1542/peds.2008-0027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Doumas DM, & Anderson L (2009). Reducing alcohol use in first-year university students: Evaluation of a web-based personalized feedback program. Journal of College Counseling, 18(1), 18–32. 10.1002/j.2161-1882.2009.tb00037.x [DOI] [Google Scholar]
- Doumas DM, Esp S, Flay B, & Bond L (2017). A randomized controlled trial testing the efficacy of a brief online alcohol intervention for high school seniors. Journal of Studies on Alcohol and Drugs, 78(5), 706–715. 10.15288/jsad.2017.78.706 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Doumas DM, Esp S, Turrisi R, Bond L, Porchia S, & Flay B (2020). Sex differences in the acceptability and short-term outcomes of a web-based personalized feedback alcohol intervention for high school seniors. Psychology in the Schools, 57(11), 1724–1740. 10.1002/pits.22422 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Doumas DM, Esp S, Johnson J, Trull R, & Shearer K (2017). The eCHECKUP TO GO for High School: Impact on risk factors and protective behaviors for alcohol use. Addictive Behaviors, 64, 93–100. 10.1016/j.addbeh.2016.08.030 [DOI] [PubMed] [Google Scholar]
- Doumas DM, Esp S, Turrisi R, & Schottelkorb A (2015). Adopting a brief, web-based feedback approach to counter high school drinking: Considerations for professional school counselors. Professional School Counseling, 18(1), 148–157. 10.1177/2156759X0001800105 [DOI] [Google Scholar]
- Doumas DM, Kane CM, Navarro T, & Roman J (2011). Decreasing heavy drinking in first year students: Evaluation of a web-based personalized feedback program administered during orientation. Journal of College Counseling, 14(1), 5–20. 10.1002/j.2161-1882.2011.tb00060.x [DOI] [Google Scholar]
- Flisher AJ, Evans J, Muller M, & Lombard C (2004). Brief report: Test-retest reliability of self-reported adolescent risk behaviour. Journal of Adolescence, 27(2), 207–212. 10.1016/j.adolescence.2001.10.001 [DOI] [PubMed] [Google Scholar]
- Fodor MC, Grekin ER, Beatty JR, McGoron L, & Ondersma SJ (2020). Participant satisfaction with computer-delivered intervention components and its relation to alcohol outcomes. Substance Use & Misuse, 55(14), 2332–2340. 10.1080/10826084.2020.1811343 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hausheer R, Doumas DM, & Esp S (2018). Evaluation of a web-based alcohol program alone and in combination with a parent-based intervention for 9th grade students. Journal of Addictions and Offender Counseling, 39, 15–30. 10.1002/jaoc.12038 [DOI] [Google Scholar]
- Hochberg Y (1988). A sharper Bonferroni procedure for multiple significance testing. Biometrika, 75(4), 800–802. 10.2307/2336325 [DOI] [Google Scholar]
- Johnston LD, Miech RA, O’Malley PM, Bachman JG, Schulenberg JE, & Patrick ME (2019). Monitoring the Future national survey results on drug use 1975–2018: Overview, key findings on adolescent drug use. Ann Arbor: Institute for Social Research, The University of Michigan. http://www.monitoringthefuture.org/pubs/monographs/mtf-overview2018.pdf [Google Scholar]
- Lintonen T, Ahlstrom S, & Metso L (2004). The reliability of self-reported drinking in adolescence. Alcohol and Alcoholism, 39(4), 362–368. 10.1093/alcalc/agh071 [DOI] [PubMed] [Google Scholar]
- Lord S, & Marsch L (2011). Emerging trends and innovations in the identification and management of drug use among adolescents and young adults. Adolescent Medicine: State of the Art Reviews, 22(3), 649–669. [PMC free article] [PubMed] [Google Scholar]
- Marlatt GA, Baer JS, Kivlahan DR, Dimeff LA, Larimer ME, Quigley LA, Somers JM, & Williams E (1998). Screening and brief intervention for high-risk college student drinkers: Results from a 2-year follow-up assessment. Journal of Consulting and Clinical Psychology, 66(4), 604–615. 10.1037/0022-006X.66.4.604 [DOI] [PubMed] [Google Scholar]
- Marsch LA, Carroll KM, & Kiluk BD (2014). Technology-based interventions for the treatment and recovery management of substance use disorders: A JSAT special issue. Journal of Substance Abuse Treatment, 46(1), 1–4. 10.1016/j.jsat.2013.08.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism (2015). Planning alcohol interventions using NIAAA’s college aim alcohol intervention matrix. https://www.niaaa.nih.gov/
- Pagano RR (2013). Understanding statistics in the behavioral sciences (10th ed.). Cengage. [Google Scholar]
- Sheskin D (2011). Handbook of parametric and nonparametric statistical procedures (5th ed.). Chapman & Hall. [Google Scholar]
- San Diego State University Research Foundation (n.d.). http://www.echeckuptogo.com/
- Smith DC, Boel-Studt S, & Cleeland L (2009). Parental consent in adolescent substance abuse treatment outcome studies. Journal of Substance Abuse Treatment, 37(3), 298–306. 10.1016/j.jsat.2009.03.007 [DOI] [PubMed] [Google Scholar]
- Spoth R, Greenberg M, & Turrisi R (2008). Preventive interventions addressing underage drinking: State of the evidence and steps toward public health impact. Pediatrics, 121, 311–336. 10.1542/peds.2007-2243E [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strøm HK, Adolfsen F, Fossum S, Kaiser S, & Martinussen M (2014). Effectiveness of school-based preventive interventions on adolescent alcohol use: A meta-analysis of randomized controlled trials. Substance Abuse Treatment, Prevention, and Policy, 9(1), Article 48. 10.1186/1747-597X-9-48 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stroup WW (2013). Generalized linear mixed models: Modern concepts, methods, and applications. CRC Press. [Google Scholar]
- Tabachnick BG, & Fidell LS (2007). Using multivariate statistics (5th ed.). Allyn and Bacon. [Google Scholar]
- Unger JB, Gallaher P, Palmer PH, Baezconde-Garbanati L, Trinidad DR, Cen S, & Johnson CA (2004). No news is bad news: Characteristics of adolescents who provide neither parental consent nor refusal for participation in school-based survey research. Evaluation Review, 28(1), 52–63. 10.1177/0193841X03254421 [DOI] [PubMed] [Google Scholar]
- Walters ST, Vader AM, & Harris TR (2007). A controlled trial of web-based feedback for heavy drinking college students. Prevention Science, 8(1), 83–88. 10.1007/s11121-006-0059-9 [DOI] [PubMed] [Google Scholar]
- Widmark EMP (1932/1981). Principles and applications of medicolegal alcohol determination (Die theoretischen Grundlagen und die praktische Verwendbarkeit der gerichtlich-medizinischen Alkoholbestimmung— German). Biomedical Publications. [Google Scholar]