

Abstract
Objective
The objective of this study is to provide normative data for a tablet-based dual-task assessment in older adults without cognitive deficits.
Method
In total, 264 participants aged between 60 and 90 years, French and English-speaking, were asked to perform two discrimination tasks, alone and concurrently. The participants had to answer as fast as possible to one or two images appearing in the center of the tablet by pressing to the corresponding buttons. Normative data are provided for reaction time (RT), coefficient of variation, and accuracy. Analyses of variance were performed by trial types (single-pure, single-mixed, dual-mixed), and linear regressions assessed the relationship between performance and sociodemographic characteristics.
Results
The participants were highly educated and a large proportion of them were women (73.9%). The accuracy on the task was very high across all blocks. RT data revealed both a task-set cost and a dual-task cost between the blocks. Age was associated with slower RT and with higher coefficient of variability. Men were significantly slower on dual-mixed trials, but their coefficient of variability was lower on single-pure trials. Education was not associated with performance.
Conclusions
This study provides normative data for a tablet-based dual-task assessment in older adults without cognitive impairment, which was lacking. All participants completed the task with good accuracy in less than 15 minutes and thus, the task is transferable to clinical and research settings.
Keywords: Executive Function, Computerized Assessment, Cognitive Aging, Neuropsychology, Dual-Task Performance
Introduction
Evidence suggests that dual-task performance declines with normal aging. Indeed, several studies have shown that cognitively healthy older adults are slower to perform dual tasks when compared to younger adults (Hartley & Little, 1999; McDowd & Shaw, 2000; Sebastián & Mediavilla, 2017; Verhaeghen & Cerella, 2002; Verhaeghen, Steitz, Sliwinski, & Cerella, 2003). Assessing dual-task performance is of paramount importance given its association with several components of successful aging and quality of life, such as driving performance and risk of car accidents (Cuenen et al., 2015; Hoffman, McDowd, Atchley, & Dubinsky, 2005; Wood, Chaparro, Lacherez, & Hickson, 2012), walking performance, risk of falls (Beauchet et al., 2007; Beauchet et al., 2008; Beauchet et al., 2009), as well as urinary incontinence in women (Chiarelli, Mackenzie, & Osmotherly, 2009; Fraser, Elliott, de Bruin, Bherer, & Dumoulin, 2014; Lussier, Renaud, Chiva-Razavi, Bherer, & Dumoulin, 2013).
However, there are still too few evaluation tools with normative data available to geriatric clinicians who wish to evaluate dual-task performance in older adults. Some battery included dual-task evaluation through paper and pencil tests, but they lack the precision necessary to isolate the costs associated with the dual-tasking paradigm (i.e., Test of Everyday Attention; Robertson, Ward, Ridgeway, & Nimmo-Smith, 1994 and The New Dual-Task Assessment; Della Sala, Foley, Beschin, Allerhand, & Logie, 2010). This is surprising considering the plethora of research done on dual tasking in relation to aging. For example, a meta-analysis has found dual-task (DT) reaction time (RT) to be consistently slower in older adults (Verhaeghen et al., 2003). The study also reported that older adults showed a higher cost associated with performing a dual task than the relative slowing expected with advanced age. Other studies have shown that DT performance might be significantly more impaired in individuals with dementia (Camicioli, Howieson, Lehman, & Kaye, 1997; Foley, Cocchini, Logie, & Della Sala, 2015), and it has been suggested that impaired or inconsistent performance on a DT could identify individuals more likely to convert to Alzheimer's disease (Foley, Kaschel, Logie, & Della Sala, 2011; MacPherson, Parra, Moreno, Lopera, & Della Sala, 2012). In the gait literature, a higher dual-task cost was also associated with a higher rate of progression to dementia (Montero-Odasso et al., 2017).
There are several methods and experimental paradigms to assess dual-task abilities (S. Fraser & Bherer, 2013). In one very simple and common paradigm, participants need to execute two concurrent discrimination tasks (e.g., Tasks A requiring to discriminate between visual stimuli and B to discriminate between two presented sounds). Participants’ performance is assessed in three different types of trials: in isolation (Task A or B performed alone), sequentially (Task A or B trials), and concurrently (Task A and B trials simultaneously) (Schumacher et al., 2001). The advantages of using non-complex discrimination tasks are numerous. First, responses to the tasks performed alone inform on general processing speed. Second, comparing single-task trials alone to the same task performed in random presentation with a second task allows to assess the cost of being in a multi-task setting (often referred as task-set cost). Finally, comparing the performance for a task performed in dual-task condition to the single-task condition can inform on the cost of synchronizing two concurrent tasks (i.e., dual-task cost).
This paradigm has been widely used to evaluate the impact of aging on dual-task performance. What emerges from these studies is that task-set and dual-task costs tend to increase with aging, but that older adults do benefit from a cognitive training regimen, in some cases, to a greater extent than younger adults (Bherer et al., 2005; Bherer et al., 2006; Bherer et al., 2008; Lussier, Brouillard, & Bherer, 2017; Lussier, Bugaiska, & Bherer, 2017; Lussier, Gagnon, & Bherer, 2012; Ruthruff, Van Selst, Johnston, & Remington, 2006; Strobach, Frensch, Soutschek, & Schubert, 2012). Moreover, it has been demonstrated repeatedly that benefits from dual-task training can transfer to dual-tasks involving novel set of stimuli and responses modalities (Bherer et al., 2005, 2008; Lussier et al., 2017; Lussier et al., 2017; Lussier, Gagnon, & Bherer, 2012), and can even transfer to functional abilities, such as gait or driving in a simulator, especially if performing a concurrent task (Cassavaugh & Kramer, 2009; Fraser et al., 2014; Ghai, Ghai, & Effenberg, 2017; Li, Bherer, Mirelman, Maidan, & Hausdorff, 2018; Montero-Odasso et al., 2018; Plummer & Eskes, 2015; Roenker, Cissell, Ball, Wadley, & Edwards, 2003; Schubert & Strobach, 2018; Silsupadol et al., 2009; Smith, Cusack, & Blake, 2016; Wollesen, Schulz, Seydell, & Delbaere, 2017).
Given the growing importance of dual-task studies, there is a need to weigh individual performances even when there is no pre-existing baseline performance or a control group comparison available, as it is often the case in clinical setting. Surprisingly, normative data for dual-tasking performance in older adults are still lacking. Over the last decade, our research team has developed a tablet-based dual-task assessment, which has been used in several published articles in older adults’ populations, both for evaluating dual-task performance and for cognitive training. This assessment uses symbols as stimuli so it can be easily used across cultures, except for the instructions that must be translated. Moreover, it is being used in three large registered randomized controlled trials involving multi-domain interventions in older adults and clinical population (Belleville et al., 2019; Montero-Odasso et al., 2018; Pothier et al., 2018). Our dual-task response modality is a touchscreen. Keyboard and mouse control are cumbersome, especially in a clinical setting, and can be hard to use for older adults. Moreover, compared to the classic mouse and keyboard apparatus, touchscreen technology has been shown to decrease age-related deficits in computerized evaluation (Findlater, Froehlich, Fattal, Wobbrock, & Dastyar, 2013). Also, touchscreen devices have been highlighted as suitable for people with dementia due to their intuitive and simple control method (Joddrell & Astell, 2016; Saxton et al., 2009). User-friendly interfaces are especially important when assessing age-related effects and they should be promoted (Parsey & Schmitter-Edgecombe, 2013).
Therefore, the purpose of this study is to provide normative data for a tablet-based dual-task assessment in older adults without cognitive deficits. RT, accuracy, and interindividual variability of RT were analyzed.
Methods
Participants
This study used data from seven studies conducted at various sites in Montreal, Canada (Bherer et al., 2020; Desjardins-Crépeau et al., 2016; Esmail et al., 2020; Lai, Bruce, Bherer, Lussier, & Li, 2017; Lussier, Brouillard, Esmail, & Bherer, 2012; Pothier et al., 2018; Vrinceanu et al., 2019). The institutional ethics review boards at each clinical site approved the protocol and all participants provided written informed consent. All seven study designs were composed of pre-intervention testing, multiple sessions of training (active and control), and post-testing. They differed in their active intervention components. For this project, we used pre-training evaluation data (before any active intervention was assigned to participants). Participants were recruited from newspaper ads, research websites, flyers posted in community centers, universities, and libraries, as well as from existing research participant pools. To be included in this study, participants had to be healthy community-dwelling English- or French-speaking volunteers aged between 60 and 90 years (see Table 1 for demographics data). Lately, several studies have been criticizing the traditional cut-off of 26 as it can be stringent and can often identify normal individuals as cognitively impaired. Therefore, for the French population we used the criteria suggested in Larouche et al. (2016) (i.e., a Z-score > −1.31 based on age, gender, and education). For English-speaking participants, we used the suggested cut-off of 23 (Carson, Leach, & Murphy, 2018; Luis, Keegan, & Mullan, 2009). Exclusion criteria also included having a history of neurological condition, a major surgery requiring general anesthesia in the last 6 months, or any neurodegenerative disorders. Also, all participants had to report no visual or hearing impairment while using their aid devices (e.g., hearing aid and glasses). In total, 10 participants were excluded due to poor performances on the MoCA and two participants due to technical difficulties, leaving a total of 264 valid participants.
Table 1.
Participant characteristics (n = 264)
| Average ± SD | |
|---|---|
| Age | 69.31 ± 6.12 |
| 60–64 years old | n = 60 (22.72%) |
| 65–74 years old | n = 154 (58.33%) |
| ≥75 years old | n = 50 (18.94%) |
| Women | n = 195 (73.90%) |
| Education | 15.12 ± 3.53 |
| Elementary/High school (5–12 years) | n = 68 (25.75%) |
| College (13–14 years) | n = 43 (15.90%) |
| University undergraduate (15–17 years) | n = 90 (34.09%) |
| University graduated (18 + years) | n = 63 (23.86%) |
| MoCA | 27.26 ± 1.78 |
In the present sample, highly educated individuals were overrepresented. When compared with the actual demographics in Quebec, there were less individual with fewer than 12 years of education (no high school diploma) in the current sample (55–64 years old: 1.7% vs. 24.6%, 65–74 years old: 16.9% vs. 42.0%, 75+ years old: 18.0% vs. 54.7%; (Institut de la statistique du Québec, 2006). Women were also overrepresented (73.9% vs. 50.4%; Statistique Canada, 2015).
Material and Procedures
The task was performed on the iPad Air 16 GB Apple (24.6 cm) using Safari. Web browsers were set in full-screen mode; so the on-screen interaction was virtually identical for both tablet devices. A small triangular stand (Ankter™) was used to rest the tablet.
The tablet dual tasks presented here is adapted from a computerized dual task extensively used in several studies involving older adults (Bherer et al., 2005, 2008; Bherer, Erickson, & Liu-Ambrose, 2013; Lussier et al., 2017; Montero-Odasso et al., 2017). The tablet version closely resembles previous computerized version with the main difference being that participants are asked to answer with their two thumbs on the touchscreen instead of both their index and ring fingers on the keyboard. We consider that those modifications do not have an impact on the validity of the task. However, age-related differences could be slightly inferior with the table version.
Stimuli: The dual-task paradigm involves performing two discrimination tasks alone or concurrently. For one task, participants were asked to discriminate animals (dog, snake, or bird) by pressing on the appropriate button with their left thumb. For the other task, they were asked to discriminate celestial bodies (moon, star, or planet) with their right thumb. Stimuli measured 150 pixel2 and were drawn in orange (R-255, G-149, B-0) with a black and a white border to increase contrast with the dark blue background (R-38, G-150, B-71). Stimuli were presented randomly above or below the focus point where the fixation cross appeared (approximately 3.17° from the cross at an arm’s length), to discourage prioritizing one task over the other. Response buttons for the celestial bodies and the animal tasks were drawn in light blue (R-56, G-146, B-219) and were displayed on the screen in a vertical layout, respectively, on the left and right extremities of the tablet. After the participant responded, the accurate response button for that trial went green for 500 ms to indicate the right answer.
Procedure: The procedure followed an ABCCAB structure. First, participants completed a single-pure block of the animal task (A: 12 trials), followed by a single-pure block of the celestial bodies task (B: 12 trials). Then two mixed blocks, combining the two tasks (C: 85 trials each), were performed. Finally, the single-pure blocks were repeated. Four practice trials preceded each first single-pure block and mixed block.
In single-pure condition, participants only had to answer to one type of task (animal task or celestial bodies). Trials within this condition are named single-pure trials. In mixed blocks, participants performed either the two tasks concurrently (dual-mixed trials) or just a single task at a time (single-mixed trials). Sixty percent of trials in the mixed condition were dual-mixed trials. The order of trials within all blocks was randomly generated and was kept the same for all participants. In total, each participant responded to 48 single-pure trials, 68 single-mixed trials, and 102 dual-mixed trials (Figs 1–3).
Fig. 1.

Visualization of a dual-mixed trial.
Fig. 3.
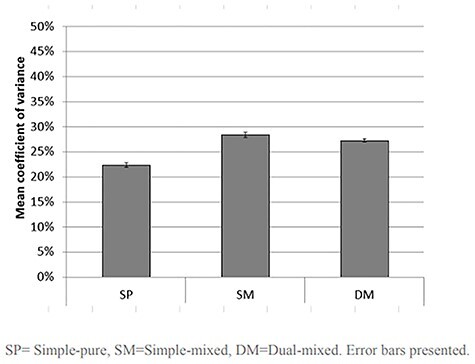
Dual-task mean coefficient of variation by type of trials.
Fig. 2.
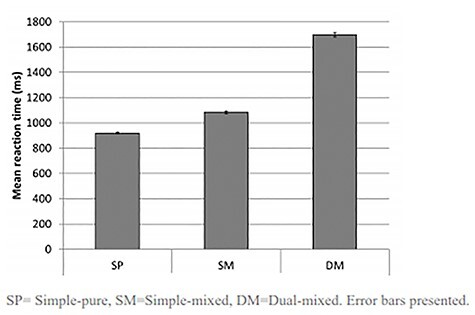
Dual-task mean reaction time by type of trials.
After appearing on the screen, stimuli remained for as long as needed for the participant to answer. Once all stimuli were answered, they immediately disappeared from the screen, leading to a one-second pause before the next trial appears.
The computerized dual task was designed to minimalize the impact of language. Although instructions were provided in one of the two languages, during the task, only symbols were presented on screen. The instructions were given verbally by the tester, and very simple sentences were presented on the screen at the beginning to instruct the participant.
The reliability of computerized RT paradigms has been shown to be adequate if the task has enough trials (Saville et al., 2011). Although test–retest reliability could not be evaluated with the available data, the correlation between the first and the second half of the task design (i.e., ABCCAB) was over .85 for all trial types (simple-pure: .85, simple-mixed: .88, dual-mixed: .90). This suggests that the task has an adequate reliability and that the number of trials administered was sufficient.
Statistical analyses
Measures:
Three variables of interest were examined: RT means (or RT, in milliseconds [ms]), coefficient of variation of RT (or COV in %), and accuracy (in % of correct responses) for each participant. Interindividual variability of RT is sometimes considered as a proxy for inefficient neural processing. COV entails making intra-individual variability proportional to the mean (standard deviation/mean RT × 100) and, in a way, weighing high variability in a fast performance context more heavily. Incorrect responses were not included in the RT and COV analyses, and trials were also rejected if RT was shorter than 200 ms or longer than 4000 ms. None of the variables of interest interacted with hand preference (task associated with the right hand vs. task associated with the left hand), and the values were averaged as it is common in this case. This is a common procedure and was also used in several previous dual-task studies (Bherer et al., 2005, 2008; Lussier et al., 2017; Lussier, Gagnon, & Bherer, 2012). In our sample, analyses of variance (ANOVAs) showed differences in age and education between men and women. Also, there was no performance difference on the dual task between the anglophones and francophones.
Cost: The difference in performance between single-pure and single-mixed trials provides a task-set cost, which is assumed to reflect the ability to maintain many response alternatives in working memory and to prepare to answer multiple tasks. A second performance index, the dual-task cost, is observed by contrasting performances in single-mixed trials and dual-mixed trials. Dual-task cost reflects the additional cost due to the synchronization of two concurrent tasks originally proposed by Schumacher et al. (2001) and is widely used in dual-task studies with older adults (Bherer et al., 2005, 2008; Lussier et al., 2017, 2017; Lussier, Gagnon, & Bherer, 2012; Strobach et al., 2012).
Analyses: Statistical analyses were run with SPSS 20. Data were examined for normality, skewness, and kurtosis. First, to confirm the presence of task-set and dual-task cost, ANOVAs were performed by trial types (single-pure (SP), single-mixed (SM), dual-mixed (DM)) as within-subject factors. The Greenhouse–Geisser-corrected degrees of freedom was reported when the assumption of sphericity was violated (Mauchly’s test). Effect sizes (η2) were also reported. Repeated contrasts were used in the case of a significant interaction with more than two levels of a repeated-measures factor. Second, linear regressions were performed to assess the relationship between participant’s sociodemographic characteristics (age, sex, and years of education) and performance for each of the three types of trials (sinple-pur, single-mixed and dual-mixed). Sociodemographic characteristics were included in the predictive model, when a minimum of 5% explained variance (r2) with the main outcome was observed.
Results
The mean RT, COV, and accuracy for each condition (SP, SM, DM) for the normative and validation samples are provided in Table 2. Based on the results from the regression model, the equation to calculate the expected score given the age and sex of the participants is reported in Table 2.
Table 2.
Participant dual-task performance (n = 264)
| 55–64 (n = 60) | 65–74 (n = 154) | 75+ (n = n = 50) | All (n = 264) | Equation for Z-score (n = 264) | |
|---|---|---|---|---|---|
| Dual-task RT | |||||
| Simple-pure trials | 871 ms (118) | 914 ms (103) | 996 ms (98) | 920 ms (113) | (410.39 + Age × 7.35)/113.09 |
| Simple-mixed trials | 1033 ms (143) | 1077 ms (163) | 1171 ms (178) | 1084 ms (168) | (474.15 + Age × 8.81)/167.51 |
| Dual-mixed trials | 1632 ms (246) | 1689 ms (269) | 1798 ms (271) | 1697 ms (269) | (979.62 + Age × 10.02 + Sex × 88.90)/269.22 |
| Dual-task COV | |||||
| Simple-pure trials | 22% (6.1) | 22% (5.8) | 25% (8.4) | 23% (6.6) | (5.77% + Age × 0.25 + Sex × -2.50)/6.55 |
| Simple-mixed trials | 28% (6.9) | 28% (8.3) | 29% (7.3) | 28% (7.7) | 28.04%/7.74 |
| Dual-mixed trials | 27 (5.1) | 26% (4.7) | 30% (4.4) | 28% (5.0) | (17.76% + Age × 0.14)/4.95 |
| Dual-task Accuracy | 5th percentile cut-off (n participants) | ||||
| Simple-pure trials | 97% (2.4) | 97% (4.8) | 97% (4.9) | 97% (4.5) | 93.56% (n = 38) |
| Simple-mixed trials | 98.% (1.6) | 98.% (2.6) | 98.% (3.0) | 98% (2.7) | 92.46% (n = 15) |
| Dual-mixed trials | 98% (2.0) | 98% (2.4) | 97% (4.4) | 98% (2.9) | 93.25% (n = 13) |
Reaction Time
A significant main effect of condition was observed, F(2, 526) = 3083.85, p<.001, η2 = .92. Repeated contrasts revealed the presence of both a task-set cost (mean of 164 ms), F(1, 263) = 504.04, p<.001, η2 = .66, and a dual-task cost (mean of 613 ms), F(1, 263) = 3964.87, p<.001, η2 = .94.
For SP trials, the predictive model, F(2, 262) = 49.32, p < .001, R2adjusted = .16), included age which was associated with slower RT (β = 7.35, SE = 1.05, p < .001). For SM trials, the predictive model, F(2, 262) = 30.29, p < .001, R2adjusted = .10), also included age which was associated with slower RT (β = 8.81, SE = 1.60, p < .001). Finally, for DM trials, the predictive model included both age and sex, F(2, 261) = 10.16, p < .001, R2adjusted = .07. Older adults’ performances were slower (β = 10.02, SE = 2.62, p < .001) and men were significantly slower than women (β = 89.00, SE = 36.47, p < .001).
Coefficient of Variance
As with RT, a significant main effect of condition was observed in COV, F(1, 526) = 58.67, p<.001, η2 = .21. Repeated contrasts showed the presence of a task-set cost (+6.08%), F(1, 263) = 86.34, p<.001, η2 = .28.
For SP trial, the predictive model, F(2, 257) = 9.62, p < .001, R2 adjusted = .07), included age as it was associated with higher COV (SP: β = .25, SE = .07) and sex because women COV were slightly lower than men (β = −2.50, SE = 1.00). SM trial did not interact with age, sex, or education. Finally, the predictive model of DM trial, F(2, 261) = 6.96, p < .01, R2adjusted = .02, included age as it was associated with higher COV (SP: β = 0.13, SE = .05).
Accuracy
Regarding accuracy, performance was quite high suggesting a ceiling effect, especially for single-pure (mean: 98.55%, median: 100%) and single-mixed trials (mean: 98.89%, median: 100%), but also for dual-mixed trials (mean: 96.44%, median: 99.02%). A large proportion of participants made one error or less resulting in a strongly non-parametric distribution. Therefore, the 5th percentile was selected as a cut-off of poor performance. Table 1 presents the 5th percentile for each type of trial.
Discussion
The main objective of this study was to provide normative data for a computerized touchscreen dual-task in older adults without cognitive deficits, which previously have been unavailable in the literature. Additionally, performance cost differences associated with single- and dual-task paradigms were examined, and an innovative measure for the dual-task paradigm, the COV, was explored. Participants were recruited from the greater region of Montreal (Canada), and their age ranged from 60 to 90 years, were highly educated, and consisted of 73.9% women. As it can be observed from the very high accuracy rates (over 97.25%), the participants understood and were able to correctly perform the task. The RTs were, as expected, slower in the DM (1697.51 ± 269.22 ms) and SM trials (1084.20± 167.51 ms), and fastest in the SP trials (920.20 ± 113.09 ms). With respect to performance costs, findings revealed an effect of task-set cost for COV and both task-set and dual-task cost effects for RT. This is consistent with several previous studies, which reported these costs on RT performances in older adults (Bherer et al., 2005, 2008; Erickson et al., 2005; Erickson et al., 2007; Laguë-Beauvais et al., 2015; Leone et al., 2017; Lussier et al., 2017; Verhaeghen et al., 2003). Finally, results revealed that women slightly outperformed men in the dual task, consistent with previous studies using the same task (Castonguay, Lussier, Bugaiska, Lord, & Bherer, 2015). However, it is important to keep in mind that women were overrepresented in the sample.
The present study used a tablet-based dual-task assessment. The tablet version closely resembles previous computerized version using computer and keyboard, so we do not expect that this modification could have impact on the validity of the task. However, we hypothesized that the responding with a keyboard may exacerbate age-related effects in task-set cost because it is more taxing on working memory (i.e., each stimulus is associated with an arbitrary key, which must be pressed by an arbitrary finger). In contrast, the tablet-based version is more intuitive and straightforward, especially for individuals with less computer experience (Fanning & McAuley, 2014; Findlater et al., 2013; Holzinger, 2002). As expected, the task-set cost appeared to be smaller than what was observed in older adults in previous studies (e.g., approx. 400 ms in Bherer et al. (2005, 2008) vs. 164 ms in the present study), whereas dual-task cost was roughly comparable. Further analyses are required, but we believe that the present tablet-based dual-task assessment is less likely to overestimate age-related differences by removing the arbitrary load of key mapping.
Accuracy was quite high, which suggests that the touchscreen format was intuitive enough for older adults. High accuracy is an interesting quality of this dual-task assessment because errors can be a great source of anxiety and can be detrimental to performance, especially in older adults (Nieuwenhuis et al., 2002). Moreover, if future studies were to demonstrate that older adults with mild cognitive impairment or dementia do make several errors, it would be a clear indicator of cognitive decline as near-perfect accuracy is to be expected in cognitively healthy older adults (Hultsch, MacDonald, & Dixon, 2002). Interestingly, variability of RT in dual-task condition does not significantly interact with age in healthy older adults. Again, it remains to be seen how COV in dual tasking could interact with cognitive deficits, as intraindividual variability in cognitive performance can be a behavioral indicator of compromised neurological mechanisms (Hultsch et al., 2002). One limitation to generalization of the present results is that participants are highly healthy educated volunteers from an urban community.
As a result, the normative data presented in this paper might not be representative of the general population but might represent specific characteristics of the aging population interested in participating in research studies. The higher percentage of women in our sample is another limitation. Future studies should seek to further validate this task by comparing the DT performance of different population samples (e.g., participants from different regions in Quebec, sample with more participants having fewer years of education) to the reported normative data. Also, we could assess DT performance in a sample of older adults with diagnosed cognitive deficits to determine whether the tablet-based dual-task is sensitive enough to identify cognitive decline. Studies should also compare the shared variance between performances on the present tablet-based dual-task and performances on other paper–pencil assessment of dual tasking available to clinicians to further validate the measures (e.g., Test of Everyday Attention, The New Dual-Task Assessment).
Overall, the results of the present study are consistent with the current literature on dual-tasking performance in older adults. This evaluation uses touchscreen technology that might be more suited for evaluating age-related deficits. Indeed, the tasks were well understood and used by older adults with various degrees of computer skills and education levels, which offers great potential use of standardized and computerized dual-task evaluation in both clinical and research settings. Also, we believe that the portability and the practical size of the hardware required (iPad) is an advantage for clinical settings. Already, many clinicians have shown great interest in this tablet-based dual task, but many have mentioned that a shorter task duration would prove to be useful considering the limited time available for formal neuropsychological evaluations. We are currently working on a version of the task that could easily and securely be shared in clinical and academic settings. At the moment, both the computerized task and calculator sheet for the normative data can be acquired by contacting Dr. Lussier or Dr. Bherer. Now that a large sample of cognitively older adults has been tested, the next step should be to gather data from populations with mild cognitive impairment and dementia to determine and expand the sample to older adults living in senior retirement homes, whether this tablet-based dual-task evaluation could be used to detect cognitive decline.
Funding
This work was supported in part by a fellowship from the Fonds de recherche du Québec—Santé and the Fonds de recherche du Québec—Nature et technologies (ML), the Canada research Chair program (LB) and the Natural Sciences and Engineering Research Council of Canada (ML and LB) and the Canadian Institutes of Health Research (LB).
Conflict of Interest
The authors declare that there is no conflict of interest.
Acknowledgments
The authors thank Vanessa Tabry, Louis Nascan Gill, Kristina Aurousseau, Kristell Pothier, David Predovan, Anne Julien, Florence St-Onge, Ramzi Houdeib, and Michele Dolla for their help on this project.
Contributor Information
Maxime Lussier, Department of Medicine, Université de Montréal, Montréal H3C 3J7, Canada; Centre de Recherche de l’Institut Universitaire de Gériatrie de Montréal, Montréal H3W 1W5, Canada.
Kathia Saillant, Centre de Recherche de l’Institut Universitaire de Gériatrie de Montréal, Montréal H3W 1W5, Canada; Department of Psychologie, Université du Québec à Montréal, Montréal H3C 3P8, Canada; EPIC Center, Montreal Heart Institute, Montreal H1T 1N6, Canada.
Tudor Vrinceanu, Centre de Recherche de l’Institut Universitaire de Gériatrie de Montréal, Montréal H3W 1W5, Canada; Department of Psychologie, Université du Québec à Montréal, Montréal H3C 3P8, Canada; EPIC Center, Montreal Heart Institute, Montreal H1T 1N6, Canada.
Carol Hudon, School of Psychology, Université Laval, Québec G1V 0A6, Canada; CERVO Brain Research Centre, Québec G1J 2G3, Canada.
Louis Bherer, Department of Medicine, Université de Montréal, Montréal H3C 3J7, Canada; Centre de Recherche de l’Institut Universitaire de Gériatrie de Montréal, Montréal H3W 1W5, Canada; EPIC Center, Montreal Heart Institute, Montreal H1T 1N6, Canada.
References
- Beauchet, O., Annweiler, C., Allali, G., Berrut, G., Herrmann, F. R., & Dubost, V. (2008). Recurrent falls and dual task–related decrease in walking speed: Is there a relationship? Journal of the American Geriatrics Society, 56(7), 1265–1269. [DOI] [PubMed] [Google Scholar]
- Beauchet, O., Annweiler, C., Dubost, V., Allali, G., Kressig, R. W., Bridenbaugh, S.et al. (2009). Stops walking when talking: A predictor of falls in older adults? European Journal of Neurology, 16(7), 786–795. [DOI] [PubMed] [Google Scholar]
- Beauchet, O., Dubost, V., Allali, G., Gonthier, R., Hermann, F. R., & Kressig, R. W. (2007). ‘Faster counting while walking’as a predictor of falls in older adults. Age and Ageing, 36(4), 418–423. [DOI] [PubMed] [Google Scholar]
- Belleville, S., Moussard, A., Ansaldo, A. I., Belchior, P., Bherer, L., Bier, N.et al. (2019). Rationale and protocol of the ENGAGE study: A double-blind randomized controlled preference trial using a comprehensive cohort design to measure the effect of a cognitive and leisure-based intervention in older adults with a memory complaint. Trials, 20(1), 282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bherer, L., Erickson, K. I., & Liu-Ambrose, T. (2013). A review of the effects of physical activity and exercise on cognitive and brain functions in older adults. Journal of Aging Research, 2013, 657508. 10.1155/2013/657508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bherer, L., Gagnon, C., Langeard, A., Lussier, M., Desjardins-Crépeau, L., Berryman, N.et al. (2020). Synergistic effects of cognitive training and physical exercise on dual-task performance in older adults. The Journals of Gerontology: Series B, 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bherer, L., Kramer, A. F., Peterson, M. S., Colcombe, S., Erickson, K., & Becic, E. (2005). Training effects on dual-task performance: Are there age-related differences in plasticity of attentional control? Psychology and Aging, 20(4), 695. [DOI] [PubMed] [Google Scholar]
- Bherer, L., Kramer, A. F., Peterson, M. S., Colcombe, S., Erickson, K., & Becic, E. (2006). Testing the limits of cognitive plasticity in older adults: Application to attentional control. Acta Psychologica, 123(3), 261–278. [DOI] [PubMed] [Google Scholar]
- Bherer, L., Kramer, A. F., Peterson, M. S., Colcombe, S., Erickson, K., & Becic, E. (2008). Transfer effects in task-set cost and dual-task cost after dual-task training in older and younger adults: Further evidence for cognitive plasticity in attentional control in late adulthood. Experimental Aging Research, 34(3), 188–219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carson, N., Leach, L., & Murphy, K. J. (2018). A re-examination of Montreal cognitive assessment (MoCA) cutoff scores. J International Journal of Geriatric Psychiatry: A Journal of the Psychiatry of Late Life Allied Sciences, 33(2), 379–388. [DOI] [PubMed] [Google Scholar]
- Cassavaugh, N. D., & Kramer, A. F. (2009). Transfer of computer-based training to simulated driving in older adults. Applied Ergonomics, 40(5), 943–952. [DOI] [PubMed] [Google Scholar]
- Castonguay, N., Lussier, M., Bugaiska, A., Lord, C., & Bherer, L. (2015). Executive functions in men and postmenopausal women. Journal of Clinical and Experimental Neuropsychology, 37(2), 193–208. [DOI] [PubMed] [Google Scholar]
- Chiarelli, P. E., Mackenzie, L. A., & Osmotherly, P. G. (2009). Urinary incontinence is associated with an increase in falls: A systematic review. The Australian Journal of Physiotherapy, 55(2), 89–95. [DOI] [PubMed] [Google Scholar]
- Cuenen, A., Jongen, E. M., Brijs, T., Brijs, K., Lutin, M., Van Vlierden, K., & Wets, G. (2015). Does attention capacity moderate the effect of driver distraction in older drivers?. Accident Analysis & Prevention, 77, 12–20. [DOI] [PubMed] [Google Scholar]
- Della Sala, S., Foley, J. A., Beschin, N., Allerhand, M., & Logie, R. H. (2010). Assessing dual-task performance using a paper-and-pencil test: Normative data. Archives of Clinical Neuropsychology, 25(5), 410–419. [DOI] [PubMed] [Google Scholar]
- Desjardins-Crépeau, L., Berryman, N., Fraser, S. A., Vu, T. T. M., Kergoat, M.-J., Li, K. Z. H.et al. (2016). Effects of combined physical and cognitive training on fitness and neuropsychological outcomes in healthy older adults. Clinical Interventions in Aging, 11, 1287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Erickson, K. I., Colcombe, S. J., Wadhwa, R., Bherer, L., Peterson, M. S., Scalf, P. E.et al. (2007). Training-induced plasticity in older adults: Effects of training on hemispheric asymmetry. Neurobiology of Aging, 28(2), 272–283. [DOI] [PubMed] [Google Scholar]
- Erickson, K. I., Colcombe, S. J., Wadhwa, R., Bherer, L., Peterson, M. S., Scalf, P. E.et al. (2005). Neural correlates of dual-task performance after minimizing task-preparation. NeuroImage, 28(4), 967–979. [DOI] [PubMed] [Google Scholar]
- Esmail, A., Vrinceanu, T., Lussier, M., Predovan, D., Berryman, N., Houle, J.et al. (2020). Effects of dance/movement training vs. aerobic exercise training on cognition, physical fitness and quality of life in older adults: A randomized controlled trial. Journal of Bodywork and Movement Therapies, 24(1), 212–220. [DOI] [PubMed] [Google Scholar]
- Fanning, J., & McAuley, E. (2014). A comparison of tablet computer and paper-based questionnaires in healthy aging research. JMIR research protocols, 3(3), e38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Findlater, L., Froehlich, J. E., Fattal, K., Wobbrock, J. O., & Dastyar, T. (2013). Age-related differences in performance with touchscreens compared to traditional mouse input. In Paper presented at the Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Montréal, Québec, Canada.
- Foley, J. A., Cocchini, G., Logie, R. H., & Della Sala, S. (2015). No dual-task practice effect in Alzheimer's disease. Memory, 23(4), 518–528. [DOI] [PubMed] [Google Scholar]
- Foley, J. A., Kaschel, R., Logie, R. H., & Della Sala, S. (2011). Dual-task performance in Alzheimer's disease, mild cognitive impairment, and normal ageing. Journal of Archives of Clinical Neuropsychology, 26(4), 340–348. [DOI] [PubMed] [Google Scholar]
- Fraser, S., & Bherer, L. (2013). Age-related decline in divided-attention: From theoretical lab research to practical real-life situations. Wiley Interdisciplinary Reviews: Cognitive Science, 4(6), 623–640. [DOI] [PubMed] [Google Scholar]
- Fraser, S. A., Elliott, V., deBruin, E. D., Bherer, L., & Dumoulin, C. (2014). The effects of combining videogame dancing and pelvic floor training to improve dual-task gait and cognition in women with mixed-urinary incontinence. Games for Health: Research, Development, and Clinical Applications, 3(3), 172–178. [DOI] [PubMed] [Google Scholar]
- Ghai, S., Ghai, I., & Effenberg, A. O. (2017). Effects of dual tasks and dual-task training on postural stability: A systematic review and meta-analysis. Clinical Interventions in Aging, 12, 557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hartley, A. A., & Little, D. M. (1999). Age-related differences and similarities in dual-task interference. Journal of Experimental Psychology: General, 128(4), 416. [DOI] [PubMed] [Google Scholar]
- Hoffman, L., McDowd, J. M., Atchley, P., & Dubinsky, R. (2005). The role of visual attention in predicting driving impairment in older adults. Psychology and aging, 20(4), 610. [DOI] [PubMed] [Google Scholar]
- Holzinger, A. (2002). Finger instead of mouse: touch screens as a means of enhancing universal access. In Paper presented at the ERCIM Workshop on User Interfaces for All, Paris, France.
- Hultsch, D. F., MacDonald, S. W. S., & Dixon, R. A. (2002). Variability in reaction time performance of younger and older adults. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 57(2), P101–P115. [DOI] [PubMed] [Google Scholar]
- Institut de la statistique du Québec (2006). Population de 25 ans et plus, selon le degré de scolarité atteint, le sexe et le groupe d’âge, Québec 2006 Canadien Census, Gouvernement of Québec. https://www.stat.gouv.qc.ca/statistiques/education/niveau-scolarite/tab1_niv_sco_2006.htm.
- Joddrell, P., & Astell, A. J. (2016). Studies involving people with dementia and touchscreen technology: A literature review. JMIR Rehabilitation and Assistive Technologies, 3(2), e10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laguë-Beauvais, M., Fraser, S. A., Desjardins-Crépeau, L., Castonguay, N., Desjardins, M., Lesage, F.et al. (2015). Shedding light on the effect of priority instructions during dual-task performance in younger and older adults: A fNIRS study. Brain and Cognition, 98, 1–14. [DOI] [PubMed] [Google Scholar]
- Lai, L., Bruce, H., Bherer, L., Lussier, M., & Li, K. Z. H. (2017). Comparing the transfer effects of simultaneously and sequentially combined aerobic exercise and cognitive training in older adults. Journal of Cognitive Enhancement, 1(4), 478–490. [Google Scholar]
- Larouche, E., Tremblay, M.-P., Potvin, O., Laforest, S., Bergeron, D., Laforce, R.et al. (2016). Normative data for the Montreal cognitive assessment in middle-aged and elderly Quebec-French people. Archives of Clinical Neuropsychology, 31(7), 819–826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leone, C., Feys, P., Moumdjian, L., D’Amico, E., Zappia, M., & Patti, F. (2017). Cognitive-motor dual-task interference: A systematic review of neural correlates. Neuroscience & Biobehavioral Reviews, 75, 348–360. [DOI] [PubMed] [Google Scholar]
- Li, K. Z. H., Bherer, L., Mirelman, A., Maidan, I., & Hausdorff, J. M. (2018). Cognitive involvement in balance, gait and dual-tasking in aging: A focused review from a neuroscience of aging perspective. Frontiers in Neurology, 9, 913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luis, C. A., Keegan, A. P., & Mullan, M. (2009). Cross validation of the Montreal cognitive assessment in community dwelling older adults residing in the Southeastern US. International Journal of Geriatric Psychiatry: A Journal of the Psychiatry of Late Life Allied Sciences, 24(2), 197–201. [DOI] [PubMed] [Google Scholar]
- Lussier, M., Brouillard, P., & Bherer, L. (2017). Limited benefits of heterogeneous dual-task training on transfer effects in older adults. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 72(5), 801–812. [DOI] [PubMed] [Google Scholar]
- Lussier, M., Brouillard, P., Esmail, A., & Bherer, L. (2012). Investigation of an assessment tool on a tablet for divided attention in an elderly population: Preliminary data. Non-Pharmacological Therapies in Dementia, 3(2), 173–176. [Google Scholar]
- Lussier, M., Bugaiska, A., & Bherer, L. (2017). Specific transfer effects following variable priority dual-task training in older adults. Restorative Neurology and Neuroscience, 35(2), 237–250. [DOI] [PubMed] [Google Scholar]
- Lussier, M., Gagnon, C., & Bherer, L. (2012). An investigation of response and stimulus modality transfer effects after dual-task training in younger and. Training-Induced Cognitive and Neural Plasticity, 118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lussier, M., Renaud, M., Chiva-Razavi, S., Bherer, L., & Dumoulin, C. (2013). Are stress and mixed urinary incontinence associated with impaired executive control in community-dwelling older women? Journal of Clinical and Experimental Neuropsychology, 35(5), 445–454. [DOI] [PubMed] [Google Scholar]
- MacPherson, S. E., Parra, M. A., Moreno, S., Lopera, F., & Della Sala, S. (2012). Dual task abilities as a possible preclinical marker of Alzheimer's disease in carriers of the E280A presenilin-1 mutation. Journal of the International Neuropsychological Society, 18(2), 234–241. [DOI] [PubMed] [Google Scholar]
- McDowd, J. M., & Shaw, R. J. (2000). Attention and aging: A functional perspective. In F. I. M. Craik & T. A. Salthouse (Eds.), The handbook of aging and cognition (p. 221–292). Lawrence Erlbaum Associates Publishers. [Google Scholar]
- Montero-Odasso, M., Almeida, Q. J., Burhan, A. M., Camicioli, R., Doyon, J., Fraser, S.et al. (2018). Synergic trial (SYNchronizing exercises, remedies in gait and cognition) a multi-Centre randomized controlled double blind trial to improve gait and cognition in mild cognitive impairment. BMC Geriatrics, 18(1), 1–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Montero-Odasso, M., Sarquis-Adamson, Y., Speechley, M., Borrie, M. J., Hachinski, V. C., Wells, J.et al. (2017). Association of dual-task gait with incident dementia in mild cognitive impairment: Results from the gait and brain study. JAMA Neurology, 74(7), 857–865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nieuwenhuis, S., Ridderinkhof, K. R., Talsma, D., Coles, M. G. H., Holroyd, C. B., Kok, A.et al. (2002). A computational account of altered error processing in older age: Dopamine and the error-related negativity. Cognitive, Affective, & Behavioral Neuroscience, 2(1), 19–36. [DOI] [PubMed] [Google Scholar]
- Parsey, C. M., & Schmitter-Edgecombe, M. (2013). Applications of technology in neuropsychological assessment. The Clinical Neuropsychologist, 27(8), 1328–1361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plummer, P., & Eskes, G. (2015). Measuring treatment effects on dual-task performance: A framework for research and clinical practice. Frontiers in Human Neuroscience, 9, 225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pothier, K., Gagnon, C., Fraser, S. A., Lussier, M., Desjardins-Crépeau, L., Berryman, N.et al. (2018). A comparison of the impact of physical exercise, cognitive training and combined intervention on spontaneous walking speed in older adults. Aging Clinical and Experimental Research, 30(8), 921–925. [DOI] [PubMed] [Google Scholar]
- Robertson, I. H., Ward, T., Ridgeway, V., & Nimmo-Smith, I. (1994). The test of everyday attention (TEA) (, pp. 197–221). Bury St. Edmunds, UK: Thames Valley Test Company. [Google Scholar]
- Roenker, D. L., Cissell, G. M., Ball, K. K., Wadley, V. G., & Edwards, J. D. (2003). Speed-of-processing and driving simulator training result in improved driving performance. Human Factors, 45(2), 218–233. [DOI] [PubMed] [Google Scholar]
- Ruthruff, E., Van Selst, M., Johnston, J. C., & Remington, R. (2006). How does practice reduce dual-task interference: Integration, automatization, or just stage-shortening? Psychological Research, 70(2), 125–142. [DOI] [PubMed] [Google Scholar]
- Saville, C. W., Pawling, R., Trullinger, M., Daley, D., Intriligator, J., Klein, C. J. P.et al. (2011). On the stability of instability: Optimising the reliability of intra-subject variability of reaction times. Personality and Individual Differences, 51(2), 148–153. [Google Scholar]
- Saxton, J., Morrow, L., Eschman, A., Archer, G., Luther, J., & Zuccolotto, A. (2009). Computer assessment of mild cognitive impairment. Postgraduate Medicine, 121(2), 177–185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schubert, T., & Strobach, T. (2018). Practice-related optimization of dual-task performance: Efficient task instantiation during overlapping task processing. Journal of Experimental Psychology: Human Perception and Performance, 44(12), 1884. [DOI] [PubMed] [Google Scholar]
- Schumacher, E. H., Seymour, T. L., Glass, J. M., Fencsik, D. E., Lauber, E. J., Kieras, D. E.et al. (2001). Virtually perfect time sharing in dual-task performance: Uncorking the central cognitive bottleneck. Psychological Science, 12(2), 101–108. [DOI] [PubMed] [Google Scholar]
- Sebastián, M. V., & Mediavilla, R. (2017). Does dual-task coordination performance decline in later life? Psicothema, 29(2), 223–228. [DOI] [PubMed] [Google Scholar]
- Silsupadol, P., Shumway-Cook, A., Lugade, V., vanDonkelaar, P., Chou, L.-S., Mayr, U.et al. (2009). Effects of single-task versus dual-task training on balance performance in older adults: A double-blind, randomized controlled trial. Archives of Physical Medicine and Rehabilitation, 90(3), 381–387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith, E., Cusack, T., & Blake, C. (2016). The effect of a dual task on gait speed in community dwelling older adults: A systematic review and meta-analysis. Gait & Posture, 44, 250–258. [DOI] [PubMed] [Google Scholar]
- Statistique Canada, A. (2015). Population selon le sexe, Canada, 1921 à 2061. Retrieved fromhttps://www150.statcan.gc.ca/n1/pub/89-503-x/2015001/article/14152/tbl/tbl1-fra.htm
- Strobach, T., Frensch, P. A., Soutschek, A., & Schubert, T. (2012). Investigation on the improvement and transfer of dual-task coordination skills. Psychological Research, 76(6), 794–811. [DOI] [PubMed] [Google Scholar]
- Verhaeghen, P., & Cerella, J. (2002). Aging, executive control, and attention: A review of meta-analyses. Neuroscience & Biobehavioral Reviews, 26(7), 849–857. [DOI] [PubMed] [Google Scholar]
- Verhaeghen, P., Steitz, D. W., Sliwinski, M. J., & Cerella, J. (2003). Aging and dual-task performance: A meta-analysis. Psychology and Aging, 18(3), 443–460. doi: 10.1037/0882-7974.18.3.443. [DOI] [PubMed] [Google Scholar]
- Vrinceanu, T., Esmail, A., Berryman, N., Predovan, D., Vu, T. T. M., Villalpando, J. M.et al. (2019). Dance your stress away: Comparing the effect of dance/movement training to aerobic exercise training on the cortisol awakening response in healthy older adults. Stress, 22(6), 687–695. [DOI] [PubMed] [Google Scholar]
- Wollesen, B., Schulz, S., Seydell, L., & Delbaere, K. (2017). Does dual task training improve walking performance of older adults with concern of falling? BMC Geriatrics, 17(1), 213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wood, J. M., Chaparro, A., Lacherez, P., & Hickson, L. (2012). Useful field of view predicts driving in the presence of distracters. Optometry and Vision Science, 89(4), 373–381. [DOI] [PubMed] [Google Scholar]